Surgical Management of Pulmonary Metastases. Dr AG Jacobs Principal Specialist Dept Cardiothoracic Surgery Steve Biko Academic Hospital
|
|
|
- Merry Owen
- 6 years ago
- Views:
Transcription
1 Surgical Management of Pulmonary Metastases Dr AG Jacobs Principal Specialist Dept Cardiothoracic Surgery Steve Biko Academic Hospital


2 Introduction Lungs 2 nd most common site of metastatic deposition 2 main forms recognised: Haematogenous Lymphatic
3 Introduction Most common primaries resulting in pulmonary metastases: Breast carcinoma Colorectal carcinoma Renal cell carcinoma Uterine leiomyosarcoma Head and neck squamous cell carcinoma

4 Introduction Less common tumours resulting in pulmonary metastases: Choriocarcinoma Ewing sarcoma Malignant melanoma Osteosarcoma Testicular tumours Thyroid carcinoma




5 Symptoms Present in 15-20% of patients Cough Dyspnoea Haemoptysis Spontaneous pneumothorax
6 Criteria for resection Primary tumour controlled Metastases resectable Absence of extra pulmonary disease Adequate cardiopulmonary reserve
 Number of metastases Tumour")
7 Prognostic Determinants No universal criteria which predict longterm survival 1990-International registry of lung metastases (IRLM) 5206 cases from Identified 4 major prognostic factors Complete resection Disease-free Interval (DFI) Number of metastases Tumour Doubling Time
8 Prognostic Determinants Complete Resection Data from International registry: Complete Resection Incomplete Resection Median Survival 35 months 15 months 5 year survival 36% 13%
9 Prognostic Determinants COMPLETE RESECTION Overall actuarial survival after lung metastasectomy: complete resection versus incomplete resection.



10 Prognostic Determinants TUMOR DOUBLING TIME Morton, Joseph et al Studied patients with variety of tumour types TDT < 40 days all died within 2-5 years By comparison: TDT > 40days 63% 5yr survival post resection.
11 Prognostic Determinants TUMOR DOUBLING TIME Ollila et al (1998) Largest series of melanoma patients. Median Survival TDT < 60 days 16 mo 0 TDT > 60 days yr survival

12 Prognostic Determinants Disease-free interval (DFI) Important prognostic factor: Pastorino U, et al 1997 Todd TR, et al 1997 Kandiolar, et al 1998 Others: DFI not an important factor - no influence on outcome: Robert JH, et al 1997

13 Prognostic Determinants Disease-free interval IRLM: Survival of the complete resection according to DFI
14 Prognostic Determinants Number and distribution of pulmonary metastases IRLM Series:
15 Recurrent Pulmonary Metastases Controversy regarding efficacy of metastasectomy. Studies examining survival of patient with recurrent pulmonary mets: Series from University of Vienna 5 year survival 48% 35 patients Landmark IRLM report 5 year survival 44% 10 year survival 29% DFI strongly associated with improved survival
16 PRE-OP EVALUATION OF PATIENTS

17 CHEST X-RAY

18 CHEST X-RAY

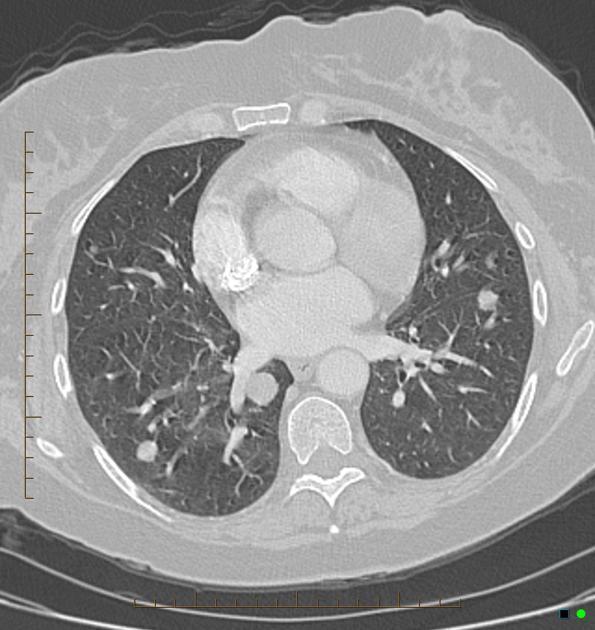
19 CT-SCAN
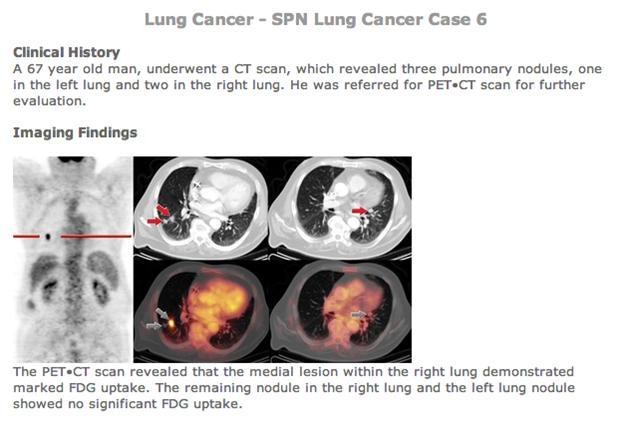
20 PET SCAN
21 MALIGNANT MELANOMA Aggressive and unpredictable tumour. Pulmonary nodule first sign of metastatic disease in 40% patients with melanoma. 7 months survival post diagnosis of pulmonary mets.
22 MALIGNANT MELANOMA A number of studies have reported their results of surgical resection: Mathis et al (1979): - Mean survival 10.5 months in unresectable patients - Mean survival 12 months in patients rendered disease free in the lungs. Morrow et al (1980): - 12% - 5 year survival. Pogrebniak et al (no. 77): - 13 months mean survival. - 7%, 5 year survival.

23 MALIGNANT MELANOMA Initial report by JWCI: , 5 year survival 25%. - mean survival 19 months - 5 year survival 31.6% - Results reflect strict selection criteria: - TDT > 40 days - Limited number of pulmonary mets - Long DFI






24 More recently: MALIGNANT MELANOMA JWCI investigators: 106 patients undergoing resection Control group 878 patients - were matched - managed non-operatively Results: - Surgical patients: 27%, 5 year survival. - Non-surgical patients 3%, 5 year survival. - Highest survival (39%) occurred in patients with single mets


25 MALIGNANT MELANOMA Kolodziejski et al (1999) : reported on 93 patients undergoing pulmonary metastasectomy from various primaries. 28%, 5 year survival in patients with cutaneous melanoma.
 reported only 0.4% incidence of metastatic disease to the lungs.")
26 PULMONARY METASTASECTOMY FOR BREAST CANCER Metastatic Breast Cancer (BC) known to be a systemic disease even in early stages. Frequently spreads to multiple organ sites. Very infrequently spreads only to the lungs. Mayo Clinic (96) reported only 0.4% incidence of metastatic disease to the lungs. Question: Is there a significant role for pulmonary resection in breast cancer?
 50% - Mayo Clinic Group (1994) 37.")
27 PULMONARY METASTASECTOMY FOR BREAST CANCER Studies: 5 year survival: - Mountain et al 14% - McCormack + Martini 30% - Lanza et al (more recently) 50% - Mayo Clinic Group (1994) 37.8%
28 PULMONARY METASTASECTOMY FOR BREAST CANCER Prognostic factors: Complete resection Long DFI Number of metastasis Positive hormone receptor Complete resection: Most studies no survival difference concerning complete and incomplete resection. McDonald et al (1994) - better 5 year survival for patients having incomplete resection (42.1%) vs. 35.6% after complete resection.

29 PULMONARY METASTASECTOMY FOR BREAST CANCER Disease free interval (DFI) Long DFI seems to be of prognostic relevance. Interval reaching significance 1 year or longer. Seems to represent: - Slowly growing tumour - Long effective antihormone therapy - Minor tumour burden
30 PULMONARY METASTASECTOMY Number of metastases: FOR BREAST CANCER An important prognostic factor in other tumours IR: included various histological types: - single mets 43% survival at 5 years - > 4 mets 27% survival at 5 years This difference does however not reach significance in most publications concerning MBC. Tanaka, F (2005) Rena O (2007) Planchard D (2004)
31 PULMONARY METASTASES OF Oestrogen Receptor Status (ERS) BREAST CANCER Only a small number of studies examined ERS for it s prognostic relevance. Welter 3 (2008) in E.J.C T Surgery Demonstrated a survival benefit for patients with ER positive metastasis on a significant level. 5 year survival 70% in receptive positive status and 12.1% in receptor negative ones. A similar survival difference was found for the status of the Her 2 neu receptor. Rahman et al (1999) 1581 MBC cases Median survival difference of 28.6 mo for positive versus 18.1 mo for receptor negative patients.

 To find and")
 To prove the histology and investigate grading, hormone")
32 PULMONARY METASTASES OF BREAST CANCER In conclusion thoracotomy for MBC should not be routinely done except for solitary pulmonary lesions. Other indications for surgery include: (1) To find and resect primary lung cancer and rule out benign lesions. (2) To prove the histology and investigate grading, hormone receptor status in order to adapt medical treatment.
33 SOFT TISSUE SARCOMA Preferentially spreads to the lungs. Resection yields 20-30% rate of prolonged survival: Mc Cormack & Martini (51) (Memorial Sloane Kettering) Creagan et al (83) Roth et al (84) European Organization for Research and Treatment of Cancer-Soft Tissue and Bone Sarcoma Group 25%, 5 year survival 29%, 5 year survival 30%, 3 year survival patients - 38%, 5 year survival
34 SOFT TISSUE SARCOMA Memorial Sloane Kettering 779 patients Complete mestastasectomy associated with: Median survival 33 mo 5 yr actuarial survival rate of 37%
35 SOFT TISSUE SARCOMA Recurrence: Rate high 80% will recur in lung Weiser et al (2000) Re-explore 86 patients Median disease specific survival 42.8mo. Identified 3 independent prognostic factors which were associated with poor outcomes: >3 nodules Largest metastases > 2cm High-grade primary tumour histology
36 OSTEOGENIC SARCOMA Primary tumour spreads directly to lungs where it may be initially restricted before metastasizing to other visceral organs. Prognosis particularly good McCormack and Martini (1979) 5yr survival of 25% Huth et al (1980) 4yr survival of 40% (soft tissue + osteogenic sarcoma) NCI study 43 patients Actuarial 5yr survival rate of 40%
37 Mountain & colleagues (1984) Antunes and colleagues (1999) 50.7%, 5yr survival in review of patients presenting with metastatic osteogenic sarcoma. 3yr overall survival rate of 61% - patients who had chemotherapy post resection.


38 COLORECTAL CANCER Metastatic lesions rarely limited to the lungs. Patients thus infrequent candidates for pulmonary metastasectomy. However if extra pulmonary disease excluded, results of resection similar to those of pulmonary metastases from other sites.
39 Outcome of patients undergoing surgical resection of Pulmonary Metastases from CRC Author, yr No. patients 5yr survival, % - Mansel et al, Goya et al McAfee et al McCormack et al Five year survival ranges from 20-40%

40 COLORECTAL CANCER At least 3 larger series address the issue of long-term outcome after pulmonary metastases from CRC (1) Japanese series (1989): * 62 patients * 5yr survival 42% 10yr survival 22% * Highest survival rate solitary metastasis < 3.0cm * Survival not influenced by: - Gender - Age - DFI - Extent of resection

41 COLORECTAL CANCER (2) Mayo Clinic (1986, 1992): * 139 patients undergoing pulmonary resection for metastatic CRC between * 30.5% alive at 5 years 16.2% at 20 years * 5 year survival rate: - solitary met % - 2 mets % - >2 mets - 7.7% * Elevated CEA had significant effect on survival
42 COLORECTAL CANCER (3) MSKCC group: * Results similar to Mayo Clinic * 144 patients undergoing resection for pulmonary mets between 1960 & 1988 * 5 year survival 40% 10 year survival 30% * Majority of patients (80 of 144) presented with solitary Pulmonary nodule. - Had a slightly but not statistically significant, better survival than patients who had > 1 nodule. Both Mayo Clinic & MSKCC series: - Found that patients could experience long-term survival after multiple sequential resections for pulmonary metastases.


43 Carcinoembryonic antigen (CEA) A 70kDa protein with 3 conserved repeat domains Member of adhesion molecule family Expressed on the apical surface of colon epithelial cells CEA expression is associated with progression of colorectal cancers Maintained in more than 95% of colorectal cancers and their metastases.


44 CARCINO-EMBRYONIC ANTIGEN (CEA) Two recent retrospective studies (1) Phillip Girard (Paris): - Found pre-op CEA a statistically significant factor in 86 colorectal patients undergoing pulmonary metastasectomy. - Overall 5 year probability of survival 24%. - Estimated 5 year survival rate reached 60% for those with a normal prethoracotomy CEA level - Conclusion except for resectability not a single prognostic factor (including no. of mets) has been found so far to be as effective as CEA for predicting survival after pulmonary metastasectomy.
45 CARCINO-EMBRYONIC ANTIGEN (CEA) (2) Mark Allen Normal CEA pre-op Raised CEA pre-op - 28 patients % 5 year survival - in 24 patients - 16%, 5year survival (Found a very similar predictive value with CEA in their patients with resectable colon mets to the lung) Conclusion - CEA an important marker - Does show statistical significance as far as survivability - However one should not refuse pulmonary resection based only on an increased CEA level
46 COLORECTAL CARCINOMA Liver 33% and lung 22% most common sites of metastases from CRC. Surgical resection or isolated: Liver mets 5yr survival range from 25-42% Lung mets 5yr survival range from 21-43% James Headrick of Mayo Clinic (2001): Retrospective review all patients who underwent both hepatic and pulmonary resection for metastatic CRC between Pulmonary metastasectomy Liver resection 58 - Resection of both lung and liver mets Concluded that resection of hepatic & pulmonary secondary to colon cancer safe and results in long term survival. Robinson et al (1999) 48 patients Found longer survival after resection at both locations

47 SUMMARY Pulmonary metastasectomy can improve survival of cancer patients. Mandatory criteria for resection are complete logoregional control of the tumor and complete resection of the metastases. Long disease-free interval, few metastases and small size of the dominant nodule are favourable prognostic factors. Contra indication to surgery include incomplete resection, no logoregional control of the primary tumor, widespread metastatic cancer, inadequate pulmonary reserve and a medical condition not allowin lung surgery.
Surgical Approaches to Pulmonary Metastases
 Surgical Approaches to Pulmonary Metastases Raja M Flores MD Professor and Chief Thoracic Surgery Mount Sinai School of Medicine New York, New York History of Lung Metastasectomy 1882 Weinlechner +CW 1926
Surgical Approaches to Pulmonary Metastases Raja M Flores MD Professor and Chief Thoracic Surgery Mount Sinai School of Medicine New York, New York History of Lung Metastasectomy 1882 Weinlechner +CW 1926
sarcoma Reprint requests: Dr M H Robinson, YCRC Senior Lecturer Clinical Oncology, Weston Park Hospital, Whitham Road, Sheffield S10 2SJ.
 1994, The British Journal of Radiology, 67, 129-135 Lung metastasectomy sarcoma in patients with soft tissue 1 M H ROBINSON, MD, MRCP, FRCR, 2 M SHEPPARD, FRCPATH, 3 E MOSKOVIC, MRCP, FRCR and 4 C FISHER,
1994, The British Journal of Radiology, 67, 129-135 Lung metastasectomy sarcoma in patients with soft tissue 1 M H ROBINSON, MD, MRCP, FRCR, 2 M SHEPPARD, FRCPATH, 3 E MOSKOVIC, MRCP, FRCR and 4 C FISHER,
VATS Metastasectomy. Inderpal (Netu) S. Sarkaria, MD, FACS
 S. Sarkaria, MD, FACS") VATS Metastasectomy Inderpal (Netu) S. Sarkaria, MD, FACS Vice Chairman, Clinical Affairs Director, Robotic Thoracic Surgery Co-Director, Esophageal and Lung Surgery Institute Disclosures Speaking & Education:
VATS Metastasectomy Inderpal (Netu) S. Sarkaria, MD, FACS Vice Chairman, Clinical Affairs Director, Robotic Thoracic Surgery Co-Director, Esophageal and Lung Surgery Institute Disclosures Speaking & Education:
After primary tumor treatment, 30% of patients with malignant
 ESTS METASTASECTOMY SUPPLEMENT Alberto Oliaro, MD, Pier L. Filosso, MD, Maria C. Bruna, MD, Claudio Mossetti, MD, and Enrico Ruffini, MD Abstract: After primary tumor treatment, 30% of patients with malignant
ESTS METASTASECTOMY SUPPLEMENT Alberto Oliaro, MD, Pier L. Filosso, MD, Maria C. Bruna, MD, Claudio Mossetti, MD, and Enrico Ruffini, MD Abstract: After primary tumor treatment, 30% of patients with malignant
PET IMAGING (POSITRON EMISSION TOMOGRAPY) FACT SHEET
 FACT SHEET") Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Positron Emission Tomography (PET) When calling Anthem (1-800-533-1120) or using the Point of Care authorization system for a Health Service Review, the following clinical information may be needed to
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Pulmonary Resection for Metastases from Colorectal Cancer
 ORIGINAL ARTICLE Pulmonary Resection for Metastases from Colorectal Cancer Paul M. van Schaik, MD,* Ewout A. Kouwenhoven, MD, PhD,* Robert J. Bolhuis, MD,* Bonne Biesma, MD, PhD, and Koop Bosscha, MD,
ORIGINAL ARTICLE Pulmonary Resection for Metastases from Colorectal Cancer Paul M. van Schaik, MD,* Ewout A. Kouwenhoven, MD, PhD,* Robert J. Bolhuis, MD,* Bonne Biesma, MD, PhD, and Koop Bosscha, MD,
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Pulmonary laser resections: Technical aspects and results in colorectal cancer
 Pulmonary laser resections: Technical aspects and results in colorectal cancer Bernward Passlick Professor of Thoracic Surgery Dept. of Thoracic Surgery University of Freiburg Germany Pulmonary laser resections
Pulmonary laser resections: Technical aspects and results in colorectal cancer Bernward Passlick Professor of Thoracic Surgery Dept. of Thoracic Surgery University of Freiburg Germany Pulmonary laser resections
Pulmonary metastases of breast cancer. When is resection indicated?
 European Journal of Cardio-thoracic Surgery 34 (2008) 1228 1234 www.elsevier.com/locate/ejcts Pulmonary metastases of breast cancer. When is resection indicated? Stefan Welter a, *, Jan Jacobs a, Thomas
European Journal of Cardio-thoracic Surgery 34 (2008) 1228 1234 www.elsevier.com/locate/ejcts Pulmonary metastases of breast cancer. When is resection indicated? Stefan Welter a, *, Jan Jacobs a, Thomas
PATHWAY FOR INVESTIGATION OF ADULTS PRESENTING WITH ASCITES. U/S Abdo/pelvis shows ascites without obvious evidence of 1 liver disease
 PATHWAY FOR INVESTIGATION OF ADULTS PRESENTING WITH ASCITES U/S Abdo/pelvis shows ascites without obvious evidence of 1 liver disease Refer back to original requester with this paperwork and review previous
PATHWAY FOR INVESTIGATION OF ADULTS PRESENTING WITH ASCITES U/S Abdo/pelvis shows ascites without obvious evidence of 1 liver disease Refer back to original requester with this paperwork and review previous
came from a carcinoma and in 12 from a sarcoma. Ninety lesions were intrapulmonary and the as the chest wall and pleura. Details of the primary
 Thorax 1982;37:366-370 Thoracic metastases MARY P SHEPHERD From the Thoracic Surgical Unit, Harefield Hospital, Harefield ABSTRACI One hundred and four patients are reviewed who were found to have thoracic
Thorax 1982;37:366-370 Thoracic metastases MARY P SHEPHERD From the Thoracic Surgical Unit, Harefield Hospital, Harefield ABSTRACI One hundred and four patients are reviewed who were found to have thoracic
Pulmonary resection for metastatic colorectal carcinoma was first performed
 General Thoracic Surgery Pulmonary metastasectomy for 165 patients with colorectal carcinoma: A prognostic assessment Yukihito Saito, MD, a Hideyasu Omiya, MD, a Keijiro Kohno, MD, b Takanobu Kobayashi,
General Thoracic Surgery Pulmonary metastasectomy for 165 patients with colorectal carcinoma: A prognostic assessment Yukihito Saito, MD, a Hideyasu Omiya, MD, a Keijiro Kohno, MD, b Takanobu Kobayashi,
CASE REPORT. Introduction. Case series reports. J Thorac Dis 2012;4(S1): DOI: /j.issn s003
: DOI: /j.issn s003") CASE REPORT Lost in time pulmonary metastases of renal cell carcinoma: complete surgical resection of metachronous metastases, 18 and 15 years after nephrectomy Kosmas Tsakiridis 1, Aikaterini N Visouli
CASE REPORT Lost in time pulmonary metastases of renal cell carcinoma: complete surgical resection of metachronous metastases, 18 and 15 years after nephrectomy Kosmas Tsakiridis 1, Aikaterini N Visouli
BJUI. Solitary, isolated metastatic disease to the kidney: Memorial Sloan-Kettering Cancer Center experience
 ; 2010 Urological Oncology SOLITARY, ISOLATED METASTATIC DISEASE TO THE KIDNEY ADAMY ET AL. BJUI Solitary, isolated metastatic disease to the kidney: Memorial Sloan-Kettering Cancer Center experience Ari
; 2010 Urological Oncology SOLITARY, ISOLATED METASTATIC DISEASE TO THE KIDNEY ADAMY ET AL. BJUI Solitary, isolated metastatic disease to the kidney: Memorial Sloan-Kettering Cancer Center experience Ari
Risk Adapted Follow-Up
 Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Risk Adapted Follow-Up Individualizing Follow- Up Strategies R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine Weill Medical College
Pulmonary metastasectomy in uterine malignancies: outcome and prognostic factors
 Original Article Pulmonary metastasectomy in uterine malignancies: outcome and prognostic factors Marco Anile, Sara Mantovani, Ylenia Pecoraro, Carolina Carillo, Lorenzo Gherzi, Andreina Pagini, Erino
Original Article Pulmonary metastasectomy in uterine malignancies: outcome and prognostic factors Marco Anile, Sara Mantovani, Ylenia Pecoraro, Carolina Carillo, Lorenzo Gherzi, Andreina Pagini, Erino
Clinical Study Clinical Outcomes of Stereotactic Body Radiotherapy for Patients with Lung Tumors in the State of Oligo-Recurrence
 Pulmonary Medicine Volume 2012, Article ID 369820, 5 pages doi:10.1155/2012/369820 Clinical Study Clinical Outcomes of Stereotactic Body Radiotherapy for Patients with Lung Tumors in the State of Oligo-Recurrence
Pulmonary Medicine Volume 2012, Article ID 369820, 5 pages doi:10.1155/2012/369820 Clinical Study Clinical Outcomes of Stereotactic Body Radiotherapy for Patients with Lung Tumors in the State of Oligo-Recurrence
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
pulmonary metastasis 80EE4727C6037E7F69A9981B7E55A238 Pulmonary Metastasis 1 / 6
 Pulmonary Metastasis 1 / 6 2 / 6 3 / 6 Pulmonary Metastasis Metastatic tumors in the lungs are cancers that developed at other places in the body (or other parts of the lungs). They then spread through
Pulmonary Metastasis 1 / 6 2 / 6 3 / 6 Pulmonary Metastasis Metastatic tumors in the lungs are cancers that developed at other places in the body (or other parts of the lungs). They then spread through
Tumour Markers. For these reasons, only a handful of tumour markers are commonly used by most doctors.
 Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Tumour Markers What are Tumour Markers? Tumour markers are substances that can be found in the body when cancer is present. They are usually found in the blood or urine. They can be products of cancer
Adjuvant therapy for thyroid cancer
 Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Carcinoma of the thyroid Adjuvant therapy for thyroid cancer John Hay Department of Radiation Oncology Vancouver Cancer Centre Department of Surgery UBC 1% of all new malignancies 0.5% in men 1.5% in women
Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer
 Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer Jai Sule 1, Kah Wai Cheong 2, Stella Bee 2, Bettina Lieske 2,3 1 Dept of Cardiothoracic and Vascular Surgery, University Surgical Cluster,
Indeterminate Pulmonary Nodules in Patients with Colorectal Cancer Jai Sule 1, Kah Wai Cheong 2, Stella Bee 2, Bettina Lieske 2,3 1 Dept of Cardiothoracic and Vascular Surgery, University Surgical Cluster,
More than half of the patients undergoing resection for colorectal
 General Thoracic Surgery Pfannschmidt et al Prognostic factors and survival after complete resection of pulmonary metastases from colorectal carcinoma: Experiences in 167 patients Joachim Pfannschmidt,
General Thoracic Surgery Pfannschmidt et al Prognostic factors and survival after complete resection of pulmonary metastases from colorectal carcinoma: Experiences in 167 patients Joachim Pfannschmidt,
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Multidisciplinary management of retroperitoneal sarcomas
 Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Dr Sneha Shah Tata Memorial Hospital, Mumbai.
 Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
Dr Sneha Shah Tata Memorial Hospital, Mumbai. Topics covered Lymphomas including Burkitts Pediatric solid tumors (non CNS) Musculoskeletal Ewings & osteosarcoma. Neuroblastomas Nasopharyngeal carcinomas
NEOPLASIA. 3. Which of the following tumour is benign a. Chondrosarcoma b. Osteochondroma c. Chondroblastoma d. Ewing s tumour e.
 NEOPLASIA 1. malignant neoplasms a. are independent of hormonal influence b. are always composed of homogenous cell lines c. arise from differentiated cells by a process of anaplasia d. display abnormal
NEOPLASIA 1. malignant neoplasms a. are independent of hormonal influence b. are always composed of homogenous cell lines c. arise from differentiated cells by a process of anaplasia d. display abnormal
Surgical Treatment for Pulmonary Me. Tsunehisa; Kugimiya, Toshiyasu. Citation Acta medica Nagasakiensia. 1983, 28
 NAOSITE: Nagasaki University's Ac Title Author(s) Surgical Treatment for Pulmonary Me Ayabe, Hiroyoshi; Tomita, Masao; Na Katsunobu; Nakao, Susumu; Eguchi, M Tsunehisa; Kugimiya, Toshiyasu Citation Acta
NAOSITE: Nagasaki University's Ac Title Author(s) Surgical Treatment for Pulmonary Me Ayabe, Hiroyoshi; Tomita, Masao; Na Katsunobu; Nakao, Susumu; Eguchi, M Tsunehisa; Kugimiya, Toshiyasu Citation Acta
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Thoracic Recurrences. Soft tissue recurrence
 Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Stereotactic body radiotherapy for thoracic and soft malignancies Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of
Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer
 Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer Gabriela M. Vargas, MD Kristin M. Sheffield, PhD, Abhishek Parmar, MD, Yimei Han, MS, Kimberly M. Brown,
Physician Follow-Up and Guideline Adherence in Post- Treatment Surveillance of Colorectal Cancer Gabriela M. Vargas, MD Kristin M. Sheffield, PhD, Abhishek Parmar, MD, Yimei Han, MS, Kimberly M. Brown,
UK Musculoskeletal Oncology: Something for All Ages. Lars Wagner, MD Pediatric Hematology/Oncology University of Kentucky
 UK Musculoskeletal Oncology: Something for All Ages Lars Wagner, MD Pediatric Hematology/Oncology University of Kentucky Pediatric-Type Sarcomas of Bone and Soft Tissue The incidence of sarcoma continues
UK Musculoskeletal Oncology: Something for All Ages Lars Wagner, MD Pediatric Hematology/Oncology University of Kentucky Pediatric-Type Sarcomas of Bone and Soft Tissue The incidence of sarcoma continues
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Specialist Referral Service Willows Information Sheets. Cancer in cats and dogs: Assessment of the patient
 Specialist Referral Service Willows Information Sheets Cancer in cats and dogs: Assessment of the patient Cancer in cats and dogs: Assessment of the patient Cancer is common in human and veterinary medicine.
Specialist Referral Service Willows Information Sheets Cancer in cats and dogs: Assessment of the patient Cancer in cats and dogs: Assessment of the patient Cancer is common in human and veterinary medicine.
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Koebner Phenomenon in Radiation Associated Angiosarcoma of the Breast: Linear Metastasis in Split Skin Graft Donor Site
 ISPUB.COM The Internet Journal of Surgery Volume 9 Number 2 Koebner Phenomenon in Radiation Associated Angiosarcoma of the Breast: Linear Metastasis in Split Skin Graft Donor Site A Chhabra, A Goyal, R
ISPUB.COM The Internet Journal of Surgery Volume 9 Number 2 Koebner Phenomenon in Radiation Associated Angiosarcoma of the Breast: Linear Metastasis in Split Skin Graft Donor Site A Chhabra, A Goyal, R
Cancer Prevention & Control in Adolescent & Young Adult Survivors
 + Cancer Prevention & Control in Adolescent & Young Adult Survivors NCPF Workshop July 15-16, 2013 Patricia A. Ganz, MD UCLA Schools of Medicine & Public Health Jonsson Comprehensive Cancer Center + Overview
+ Cancer Prevention & Control in Adolescent & Young Adult Survivors NCPF Workshop July 15-16, 2013 Patricia A. Ganz, MD UCLA Schools of Medicine & Public Health Jonsson Comprehensive Cancer Center + Overview
Surgical Metabolism Section, Surgery Branch, NCI, Bethesda, MD Division of Surgical Oncology, University of Maryland, Baltimore, MD
 High Dose Intra-Arterial Melphalan Delivered via Percutaneous Hepatic Perfusion (PHP) for Patients with Unresectable Hepatic Metastases from Primary Neuroendocrine Tumors. James F. Pingpank, Richard E.
High Dose Intra-Arterial Melphalan Delivered via Percutaneous Hepatic Perfusion (PHP) for Patients with Unresectable Hepatic Metastases from Primary Neuroendocrine Tumors. James F. Pingpank, Richard E.
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
Lung Cancer-a primer. Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo
 Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
Lung Cancer-a primer Sai Yendamuri, MD Professor and Chair, Dept of Thoracic Surgery,RPCI,Buffalo CLINICAL CATEGORIES THE SOLITARY PULMONARY NODULE MULTIPLE PULMONARY NODULES Differential Diagnosis Malignant
TUMOR M ARKERS MARKERS
 TUMOR MARKERS M.Shekarabi IUMS Definition Many cancers are associated with the abnormal production of some molecules l which h can be measured in plasma. These molecules are known as tumor markers. A good
TUMOR MARKERS M.Shekarabi IUMS Definition Many cancers are associated with the abnormal production of some molecules l which h can be measured in plasma. These molecules are known as tumor markers. A good
New Visions in PET: Surgical Decision Making and PET/CT
 New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
New Visions in PET: Surgical Decision Making and PET/CT Stanley J. Goldsmith, MD Director, Nuclear Medicine Professor, Radiology & Medicine New York Presbyterian Hospital- Weill Cornell Medical Center
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON
 Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Colon cancer is still one of the leading causes of
 Long-Term Survival After Repeated Resection of Pulmonary Metastases From Colorectal Cancer Stefan Welter, MD, Jan Jacobs, MD, Thomas Krbek, MD, Bettina Krebs, MD, and Georgios Stamatis, MD Department of
Long-Term Survival After Repeated Resection of Pulmonary Metastases From Colorectal Cancer Stefan Welter, MD, Jan Jacobs, MD, Thomas Krbek, MD, Bettina Krebs, MD, and Georgios Stamatis, MD Department of
Malignant Cardiac Tumors Rad-Path Correlation
 Malignant Cardiac Tumors Rad-Path Correlation Vincent B. Ho, M.D., M.B.A. 1 Jean Jeudy, M.D. 2 Aletta Ann Frazier, M.D. 2 1 Uniformed Services University of the Health Sciences 2 University of Maryland
Malignant Cardiac Tumors Rad-Path Correlation Vincent B. Ho, M.D., M.B.A. 1 Jean Jeudy, M.D. 2 Aletta Ann Frazier, M.D. 2 1 Uniformed Services University of the Health Sciences 2 University of Maryland
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Carcinoma of unknown primary origin (CUP) Faculty of Clinical Radiology www.rcr.ac.uk Contents Carcinoma of
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Carcinoma of unknown primary origin (CUP) Faculty of Clinical Radiology www.rcr.ac.uk Contents Carcinoma of
ORIGINAL RESEARCH. International Journal of Surgery
 International Journal of Surgery 11 (2013) 244e248 Contents lists available at SciVerse ScienceDirect International Journal of Surgery journal homepage: www.theijs.com Original research Pulmonary metastasectomy
International Journal of Surgery 11 (2013) 244e248 Contents lists available at SciVerse ScienceDirect International Journal of Surgery journal homepage: www.theijs.com Original research Pulmonary metastasectomy
Prognostic factors for resection of isolated pulmonary metastases in breast cancer patients: a systematic review and meta-analysis
 Original Article Prognostic factors for resection of isolated pulmonary metastases in breast cancer patients: a systematic review and meta-analysis Jun Fan, Dali Chen, Heng Du, Cheng Shen, Guowei Che Department
Original Article Prognostic factors for resection of isolated pulmonary metastases in breast cancer patients: a systematic review and meta-analysis Jun Fan, Dali Chen, Heng Du, Cheng Shen, Guowei Che Department
Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication for Repeat Metastasectomy
 Respiratory Medicine Volume 2015, Article ID 570314, 5 pages http://dx.doi.org/10.1155/2015/570314 Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication
Respiratory Medicine Volume 2015, Article ID 570314, 5 pages http://dx.doi.org/10.1155/2015/570314 Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication
F NaF PET/CT in the Evaluation of Skeletal Malignancy
 F NaF PET/CT in the Evaluation of Skeletal Malignancy Andrei Iagaru, MD September 26, 2013 School of of Medicine Ø Introduction Ø F NaF PET/CT in Primary Bone Cancers Ø F NaF PET/CT in Bone Metastases
F NaF PET/CT in the Evaluation of Skeletal Malignancy Andrei Iagaru, MD September 26, 2013 School of of Medicine Ø Introduction Ø F NaF PET/CT in Primary Bone Cancers Ø F NaF PET/CT in Bone Metastases
Dynamic Risk Stratification:
 Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
Dynamic Risk Stratification: Using Risk Estimates to Guide Initial Management R Michael Tuttle, MD Clinical Director, Endocrinology Service Memorial Sloan Kettering Cancer Center Professor of Medicine
SECONDARIES: A PRELIMINARY REPORT
 HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO)
") North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO) UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Original Prepared by NMcL April 2016
North of Scotland Cancer Network Clinical Management Guideline for Metastatic Malignancy of Undefined Primary Origin (MUO) UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Original Prepared by NMcL April 2016
RFA of Tumors of the Lung: How and Why. Radiofrequency Ablation. Radiofrequency Ablation. RFA of pulmonary metastases. Radiofrequency Ablation of Lung
 RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation
RFA of Tumors of the Lung: How and Why Radiofrequency Ablation of Lung Ernest Scalzetti MD SUNY Upstate Medical University Syracuse NY FDA WARNING: Off-label use of a medical device Radiofrequency Ablation
Non-Small Cell Lung Cancer: Disease Spectrum and Management in a Tertiary Care Hospital
 Non-Small Cell Lung Cancer: Disease Spectrum and Management in a Tertiary Care Hospital Muhammad Rizwan Khan,Sulaiman B. Hasan,Shahid A. Sami ( Department of Surgery, The Aga Khan University Hospital,
Non-Small Cell Lung Cancer: Disease Spectrum and Management in a Tertiary Care Hospital Muhammad Rizwan Khan,Sulaiman B. Hasan,Shahid A. Sami ( Department of Surgery, The Aga Khan University Hospital,
In the past, pulmonary metastases (PM) were considered
 were considered") Original Article The Role of Extended Pulmonary Metastasectomy Monica Casiraghi, MD,* Patrick Maisonneuve, Eng, Daniela Brambilla, Msc,* Francesco Petrella, MD,* Piergiorgio Solli, MD,* Juliana Guarize,
Original Article The Role of Extended Pulmonary Metastasectomy Monica Casiraghi, MD,* Patrick Maisonneuve, Eng, Daniela Brambilla, Msc,* Francesco Petrella, MD,* Piergiorgio Solli, MD,* Juliana Guarize,
Accepted Manuscript. Preoperative CEA in Patients with Colorectal Metastases Matters. Benny Weksler, MBA, MD
 Accepted Manuscript Preoperative CEA in Patients with Colorectal Metastases Matters Benny Weksler, MBA, MD PII: S0022-5223(19)30068-6 DOI: https://doi.org/10.1016/j.jtcvs.2019.01.016 Reference: YMTC 14019
Accepted Manuscript Preoperative CEA in Patients with Colorectal Metastases Matters Benny Weksler, MBA, MD PII: S0022-5223(19)30068-6 DOI: https://doi.org/10.1016/j.jtcvs.2019.01.016 Reference: YMTC 14019
Oncology 101. Cancer Basics
 Oncology 101 Cancer Basics What Will You Learn? What is Cancer and How Does It Develop? Cancer Diagnosis and Staging Cancer Treatment What is Cancer? Cancer is a group of more than 100 different diseases
Oncology 101 Cancer Basics What Will You Learn? What is Cancer and How Does It Develop? Cancer Diagnosis and Staging Cancer Treatment What is Cancer? Cancer is a group of more than 100 different diseases
Update on management of metastatic brain disease. Peter Hoskin Mount Vernon Cancer Centre Northwood UK
 Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Update on management of metastatic brain disease Peter Hoskin Mount Vernon Cancer Centre Northwood UK Incidence 15-30% of patients with solid tumours will develop brain metastases Most common primary sites
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy
 Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 PET Scanning: Oncologic Applications Page 1 of 42 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Positron Emission Tomography (PET) Scanning: Oncologic
PET Scanning: Oncologic Applications Page 1 of 42 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: See also: Positron Emission Tomography (PET) Scanning: Oncologic
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Value of Systematic Mediastinal Lymph Node Dissection During Pulmonary Metastasectomy
 Value of Systematic Mediastinal Lymph Node Dissection During Pulmonary Metastasectomy Florian Loehe, MD, Sonja Kobinger, MD, Rudolf A. Hatz, MD, Thomas Helmberger, MD, Udo Loehrs, MD, and Heinrich Fuerst,
Value of Systematic Mediastinal Lymph Node Dissection During Pulmonary Metastasectomy Florian Loehe, MD, Sonja Kobinger, MD, Rudolf A. Hatz, MD, Thomas Helmberger, MD, Udo Loehrs, MD, and Heinrich Fuerst,
Introduction. Results. Discussion. Histopathologic and immunohistochemical findings. Results. conclusions,
 1/5 2/5 Carcinoma distinctive carcinoma. form erysipeloides (CE), metastasis. which clinically Itfrom has resembles been termed erysipelas, is an uncommon, but may extend It164 toclassically back, presents
1/5 2/5 Carcinoma distinctive carcinoma. form erysipeloides (CE), metastasis. which clinically Itfrom has resembles been termed erysipelas, is an uncommon, but may extend It164 toclassically back, presents
Leiomyosarcoma of the inferior vena cava: 1 case. B. Bancel, A. Rode, C. Ducerf. Hôpital CROIX ROUSSE LYON. Case report
 Leiomyosarcoma of the inferior vena cava: 1 case B. Bancel, A. Rode, C. Ducerf Hôpital CROIX ROUSSE LYON Bucharest Nov 2011 Case report 34 yr-old woman, no antecedent Sept 2004: Abdominal upper right quadrant
Leiomyosarcoma of the inferior vena cava: 1 case B. Bancel, A. Rode, C. Ducerf Hôpital CROIX ROUSSE LYON Bucharest Nov 2011 Case report 34 yr-old woman, no antecedent Sept 2004: Abdominal upper right quadrant
UPDATE ON RADIOTHERAPY
 1 Miriam Kleiter UPDATE ON RADIOTHERAPY Department for Companion Animals and Horses, Plattform Radiooncology and Nuclear Medicine, University of Veterinary Medicine Vienna Introduction Radiotherapy has
1 Miriam Kleiter UPDATE ON RADIOTHERAPY Department for Companion Animals and Horses, Plattform Radiooncology and Nuclear Medicine, University of Veterinary Medicine Vienna Introduction Radiotherapy has
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer
 Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
Pre-operative Ultrasound of Lymph Nodes in Thyroid Cancer AACE - Advances in Medical and Surgical Management of Thyroid Cancer - 2018 Robert A. Levine, MD, FACE, ECNU Thyroid Center of New Hampshire Geisel
The Frequency and Significance of Small (15 mm) Hepatic Lesions Detected by CT
 Hepatic Lesions Detected by CT") 535 Elizabeth C. Jones1 Judith L. Chezmar Rendon C. Nelson Michael E. Bernardino Received July 22, 1991 ; accepted after revision October 16, 1991. Presented atthe annual meeting ofthe American Aoentgen
535 Elizabeth C. Jones1 Judith L. Chezmar Rendon C. Nelson Michael E. Bernardino Received July 22, 1991 ; accepted after revision October 16, 1991. Presented atthe annual meeting ofthe American Aoentgen
Mauricio Camus Appuhn Associate Professor Chief, Department of Surgical Oncology, Pontificia Universidad Católica de Chile
 May 18-20, 2017 18 a 20 de Maio / 2017 Castro's Park Hotel Surgery for metastatic breast cancer: the controversy of local surgery for metastatic breast cancer Cirurgia em câncer de mama metastático: a
May 18-20, 2017 18 a 20 de Maio / 2017 Castro's Park Hotel Surgery for metastatic breast cancer: the controversy of local surgery for metastatic breast cancer Cirurgia em câncer de mama metastático: a
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Page: 1 of 29. For this policy, PET scanning is discussed for the following 4 applications in oncology:
 Emission Tomography Scanning Page: 1 of 29 Last Review Status/Date: June 2015 Description Positron emission tomography (PET) scans are based on the use of positron-emitting radionuclide tracers coupled
Emission Tomography Scanning Page: 1 of 29 Last Review Status/Date: June 2015 Description Positron emission tomography (PET) scans are based on the use of positron-emitting radionuclide tracers coupled
Classification of Neoplasms
 Classification of Neoplasms ICD-10 Chapter 2, Neoplasms Codes C00-D48 Notes at beginning of Chapter 2 Classified by behaviour and site Correct use of Alphabetic index required Main terms Modifiers Table
Classification of Neoplasms ICD-10 Chapter 2, Neoplasms Codes C00-D48 Notes at beginning of Chapter 2 Classified by behaviour and site Correct use of Alphabetic index required Main terms Modifiers Table
Zurich, January 19, 2018
 Brain metastases as first presentation of malignancy: Immediate management, differential diagnosis; prevalence of primaries and suggested work-up Symposium on Brain Metastasis Cancer Center Zurich Zurich,
Brain metastases as first presentation of malignancy: Immediate management, differential diagnosis; prevalence of primaries and suggested work-up Symposium on Brain Metastasis Cancer Center Zurich Zurich,
Pulmonary Resection for Metastatic Adrenocortical Carcinoma: The National Cancer Institute Experience
 Pulmonary Resection for Metastatic Adrenocortical Carcinoma: The National Cancer Institute Experience Clinton D. Kemp, MD,* R. Taylor Ripley, MD,* Aarti Mathur, MD, Seth M. Steinberg, PhD, Dao M. Nguyen,
Pulmonary Resection for Metastatic Adrenocortical Carcinoma: The National Cancer Institute Experience Clinton D. Kemp, MD,* R. Taylor Ripley, MD,* Aarti Mathur, MD, Seth M. Steinberg, PhD, Dao M. Nguyen,
Editorial commentary: Size and margin do matter, but is it the whole story? Paul A.J. Beckers, MD, Lawek Berzenji, MD,, Paul E. Van Schil, MD, PhD
 Accepted Manuscript Editorial commentary: Size and margin do matter, but is it the whole story? Paul A.J. Beckers, MD, Lawek Berzenji, MD,, Paul E. Van Schil, MD, PhD PII: S0022-5223(18)33135-0 DOI: https://doi.org/10.1016/j.jtcvs.2018.11.036
Accepted Manuscript Editorial commentary: Size and margin do matter, but is it the whole story? Paul A.J. Beckers, MD, Lawek Berzenji, MD,, Paul E. Van Schil, MD, PhD PII: S0022-5223(18)33135-0 DOI: https://doi.org/10.1016/j.jtcvs.2018.11.036
Outline. WBRT field. Brain Metastases. Whole Brain RT Prophylactic WBRT Stereotactic radiosurgery (SRS) 1 fraction Stereotactic frame
 1 fraction Stereotactic frame") Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
Radiation Therapy for Advanced NSC Lung Ca Alexander Gottschalk, M.D., Ph.D. Associate Professor Director of CyberKnife Radiosurgery Department of Radiation Oncology University of California San Francisco
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A fatal case of an adrenal gland melanoma with a mysterious primary lesion
 ISPUB.COM The Internet Journal of Urology Volume 6 Number 2 A fatal case of an adrenal gland melanoma with a mysterious primary lesion A Adam, M Engelbrecht, I van Heerden Citation A Adam, M Engelbrecht,
ISPUB.COM The Internet Journal of Urology Volume 6 Number 2 A fatal case of an adrenal gland melanoma with a mysterious primary lesion A Adam, M Engelbrecht, I van Heerden Citation A Adam, M Engelbrecht,
T tases in patients with soft-tissue sarcomas is well
 Response to Chemotherapy Does Not Predict Survival After Resection of Sarcomatous Pulmonary etastases Louis A. Lanza, D, Joe B. Putnam, Jr, D, Robert S. Benjamin, D, and Jack A. Roth, D Departments of
Response to Chemotherapy Does Not Predict Survival After Resection of Sarcomatous Pulmonary etastases Louis A. Lanza, D, Joe B. Putnam, Jr, D, Robert S. Benjamin, D, and Jack A. Roth, D Departments of
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP
 Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
Lung Cancer in Women: A Different Disease? James J. Stark, MD, FACP Medical Director, Cancer Program and Director of Palliative Care Maryview Medical Center Professor of Medicine Eastern Virginia Medical
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Histopathologic Prognostic Factors in Resected Colorectal Lung Metastases
 Histopathologic Prognostic Factors in Resected Colorectal Lung Metastases Satoshi Shiono, MD, Genichiro Ishii, MD, Kanji Nagai, MD, Junji Yoshida, MD, Mitsuyo Nishimura, MD, Yukinori Murata, MT, Koji Tsuta,
Histopathologic Prognostic Factors in Resected Colorectal Lung Metastases Satoshi Shiono, MD, Genichiro Ishii, MD, Kanji Nagai, MD, Junji Yoshida, MD, Mitsuyo Nishimura, MD, Yukinori Murata, MT, Koji Tsuta,
The prognostic importance of the number of metastases in pulmonary metastasectomy of colorectal cancer
 Cho et al. World Journal of Surgical Oncology (2015) 13:222 DOI 10.1186/s12957-015-0621-7 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Open Access The prognostic importance of the number of metastases in
Cho et al. World Journal of Surgical Oncology (2015) 13:222 DOI 10.1186/s12957-015-0621-7 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Open Access The prognostic importance of the number of metastases in
Master Class: Fundamentals of Lung Cancer
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Pulmonary Metastasectomy for Pulmonary Metastases of Head and Neck Squamous Cell Carcinomas
 ORIGINAL ARTICLES: SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must have either an STS
ORIGINAL ARTICLES: SURGERY: The Annals of Thoracic Surgery CME Program is located online at http://cme.ctsnetjournals.org. To take the CME activity related to this article, you must have either an STS
Update on Sarcomas of the Head and Neck. Kevin Harrington
 Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
R. F. Falkenstern-Ge, 1 S. Bode-Erdmann, 2 G. Ott, 2 M. Wohlleber, 1 and M. Kohlhäufl Introduction. 2. Histology
 Case Reports in Oncological Medicine Volume 2013, Article ID 167585, 4 pages http://dx.doi.org/10.1155/2013/167585 Case Report Late Lung Metastasis of a Primary Eccrine Sweat Gland Carcinoma 10 Years after
Case Reports in Oncological Medicine Volume 2013, Article ID 167585, 4 pages http://dx.doi.org/10.1155/2013/167585 Case Report Late Lung Metastasis of a Primary Eccrine Sweat Gland Carcinoma 10 Years after
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
The Importance of One-Stage Median Stemotomy and Retroperitoneal Node Dissection in Disseminated Testicular Cancer
 The Importance of One-Stage Median Stemotomy and Retroperitoneal Node Dissection in Disseminated Testicular Cancer Isidore Mandelbaum, M.D., Peter B. Yaw, M.D., Lawrence H. Einhorn, M.D., Stephen D. Williams,
The Importance of One-Stage Median Stemotomy and Retroperitoneal Node Dissection in Disseminated Testicular Cancer Isidore Mandelbaum, M.D., Peter B. Yaw, M.D., Lawrence H. Einhorn, M.D., Stephen D. Williams,
UK CAA Oncology Certification Charts
 UK CAA Oncology Certification Charts 1. Colorectal 2. Malignant Melanoma 3. Germ Cell Tumour of Testis 4. Renal Cell Carcinoma 5. Breast Carcinoma 6. Non-small Cell Lung Cancer Note: All Class 1 cases
UK CAA Oncology Certification Charts 1. Colorectal 2. Malignant Melanoma 3. Germ Cell Tumour of Testis 4. Renal Cell Carcinoma 5. Breast Carcinoma 6. Non-small Cell Lung Cancer Note: All Class 1 cases
Cancer of Unknown Primary (CUP) Protocol
 Protocol") 1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
1 Department of Oncology. Cancer of Unknown Primary (CUP) Protocol Version: Document type: Document sponsor Designation Document author [ s] Designation[s] Approving committee / Group Ratified by: Date
Canadian Scientific Journal. Intraoperative color detection of lymph nodes metastases in thyroid cancer
 Canadian Scientific Journal 2 (2014) Contents lists available at Canadian Scientific Journal Canadian Scientific Journal journal homepage: Intraoperative color detection of lymph nodes metastases in thyroid
Canadian Scientific Journal 2 (2014) Contents lists available at Canadian Scientific Journal Canadian Scientific Journal journal homepage: Intraoperative color detection of lymph nodes metastases in thyroid