Lung 8/7/14. Collecting Cancer Data: Lung NAACCR Webinar Series. August 7, 2014
|
|
|
- Norah Cross
- 6 years ago
- Views:
Transcription

1 Collecting Cancer Data: Lung NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar at your site, please collect their names and s. We will be distributing a Q&A document in about one week. This document will fully answer questions asked during the webinar and will contain any corrections that we may discover after the webinar. NAACCR Webinar Series 1


2 Fabulous Prizes 3 Agenda Overview Quiz 1 Staging Quiz 2 Treatment Quiz 3 Case Scenarios NAACCR Webinar Series 2

3 Key Statistics 5 Survival 2014, American Cancer Society, Inc. 6 NAACCR Webinar Series 3
4 Risk Factors Smoking Approximately 85 to 90% of lung cancer cases are caused by smoking Radon Asbestos 7 Histology Non Small Cell Lung Cancer (NSLC) (8046/3) Adenocarcinoma (8140/3) 40% of lung cancers Usually found in the peripheral parts of the lung Large Cell Carcinoma (8012/3) Squamous Cell Carcinoma (8070/3) 25 30% of all lung cancers Usually originate in cells lining the inside of the lung airways. Tend to be more centrally located. 8 NAACCR Webinar Series 4
5 Histology Small Cell Lung Cancer (8041/3) 10 15% of all lung cases Starts in the bronchi near the center of the chest Tends to spread widely to other parts of the body prior Patients often present with regional or distant disease Lung carcinoid tumors (8240/3) 5% of all lung cases Tend to be slow growing 9 Thyroid transcription factor 1 (TTF 1) Adenocarcinoma TTF 1 positive Squamous cell carcinoma TTF 1 negative and p63 positive TTF 1 helps distinguish primary lung adenocarcinoma from metastatic adenocarcinoma 10 NAACCR Webinar Series 5
 Diaphragm http://en.")
6 Biomarkers Predictive biomarkers Epidermal growth factor receptor (EGFR) Anaplastic lymphoma kinase (ALK) Prognostic biomarker KRAS KRAS mutational status is prognostic of survival Currently not targeted therapy for KRAS positive patients 11 Anatomy Thoracic Cavity Mediastinum Superior vena cava Trachea Thymus Heart etc Two Pleural Cavities (where the lungs are housed) Diaphragm viewer/file:blausen_0458_heart_thoraciccavity.png 12 NAACCR Webinar Series 6



7 C33.9 C34.1 C34.1 C34.2 C34.0 C34.3 C34.3 Bronchial Tree 14 NAACCR Webinar Series 7



8 1-Oblique Fissure 2- Lower Lobe Lung 3-Hilum 7- Apex (C34.1) 4-Cardiac Notch 6-Lingula (C34.1) 5-Diaphragmatic Surface Thoracic Cavity NAACCR Webinar Series 8




9 Lung 8/7/14 17 Lymph Node Stations Single digit stations are N2 Double digit stations are N1 18 NAACCR Webinar Series 9
10 Pancoast Tumor Form in the extreme apex of the lung in the superior sulcus Tend to involve the chest wall structures rather than the underlying lung tissue Pancoast syndrome is characterized by pain in the shoulder and along the inner side of the arm or hand Atelectasis The collapse of part or (much less commonly) all of a lung Caused by a blockage of the air passages (bronchus or bronchioles) or by pressure on the outside of the lung. NAACCR Webinar Series 10

11 Obstructive Pneumonitis Combination of atelectasis, bronchiectasis with mucous plugging, and parenchymal inflammation that develops distal to an obstructing endobronchial lesion. Pleural Effusion Caused by excess fluid accumulation between the two layers of the pleura Consider malignant unless multiple cytopathologic examinations of pleural and/or pericardial fluid are negative for tumor, and the fluid is non bloody and is not an exudates NAACCR Webinar Series 11
12 Quiz 23 Staging Systems Lung NAACCR Webinar Series 12
13 Collaborative Stage Data Collection System V02.05 Lung 25 CS Tumor Size: Lung Do not code size of hilar mass unless stated to be hilum primary Tumor size is a determinant in AJCC T1, T2, and T3 NAACCR Webinar Series 13
14 CS Extension: Lung Do NOT code bronchopneumonia as obstructive pneumonitis Code invasion of pleura Code 410: Extension to but not into pleura, including invasion of elastic layer BUT not through the elastic layer Code 420: Invasion of pleura, including invasion through the elastic layer Code 430: Invasion of pleura NOS Code 600: Direct extension to parietal pleura Do NOT code pleural or pericardial effusion in CS Extension Assign code 700 for vocal cord paralysis from involvement of recurrent branch of vagus nerve 27 CS Extension: Lung CS Extension = , , , 730, and T category is based on value of CS Tumor Size, CS Extension, and SSF1 CS Extension = , 740, and Summary Stage 2000 is based on CS Extension and SSF1 28 NAACCR Webinar Series 14
15 Pop Quiz CT of Chest: There is a 3.8 x 4.7 cm mass with spiculated margins in the central portion of the left lower lung lobe that abuts the pericardium overlying the left ventricle. The linear opacity extending inferolateral to the mass represents atelectasis. There is no pleural effusion and no definite adenopathy. FNA biopsy left lower lung lobe: Malignant tissue consistent with non small cell carcinoma. 29 Pop Quiz What is the code for CS Tumor Size? a. 038 b. 047 c. 997: Diffuse (entire lobe) d. 999: Unknown What is the code for CS Extension? a. 400: Atelectasis/obstructive pneumonitis that extends to the hilar region but does not involve the entire lung OR atelectasis/obstructive pneumonitis NOS b. 550: Atelectasis/obstructive pneumonitis involving entire lung c. 560: Parietal pericardium or pericardium NOS d. 999: Unknown 30 NAACCR Webinar Series 15
16 CS Lymph Nodes: Lung Code adenopathy, enlargement, or mass of lymph nodes named in codes 100 and 200 as lymph node involvement Assign code 600 for bilateral adenopathy, enlargement, or mass Assign code 200 (mediastinal node involvement) for vocal cord paralysis from involvement of recurrent branch of vagus nerve if primary tumor is peripheral and unrelated to vocal cord paralysis Pop Quiz PET scan: 3.8 X 2.1 mass of middle lobe of right lung, consistent with malignancy; enlarged mediastinal nodes. Bronchoscopic biopsy: Brushing of right middle lobe negative for malignancy. Fine needle aspiration of multiple lymph node stations negative for malignancy. Wedge resection of right middle lobe of lung and lymph node dissection: 3.4 cm squamous cell carcinoma surrounded by intact visceral pleura; 0/12 malignant nodes (3 right and 3 left peribronchial LN, 3 right and 3 left mediastinal LN). 32 NAACCR Webinar Series 16
17 Pop Quiz What is the code for CS Lymph Nodes? a. 000: No regional lymph node involvement b. 200: Ipsilateral mediastinal lymph node(s) c. 600: Contralateral/bilateral mediastinal lymph node(s) d. 999: Unknown 33 CS Mets at DX: Lung Code pleural and pericardial effusion as distant metastasis UNLESS multiple cytopathologic exams and clinical judgment indicate effusion is not related to tumor Code separate tumor nodules in contralateral lung and pleural tumor foci or nodules on contralateral lung as distant metastasis (code 23) Code direct extension of structures considered M1 as distant metastasis Extension to contralateral lung or mainstem bronchus (code 23) Extension to sternum, skeletal muscle, skin of chest (code 37) NAACCR Webinar Series 17
18 Pop Quiz CT Chest: RLL lung mass, 4.5cm, with contiguous extension superiorly to right hilar and perihilar region and hilar lymphadenopathy. No contralateral nodal activity. Suspect metastatic disease to lower thoracic and lumbar spine. Chest x ray: Accentuated interstitial markings with hazy opacity in RUL lung. Bilateral pulmonary nodules in LUL lung. FNA biopsy RLL lung mass: Non small cell carcinoma. MRI & Bone scan: Negative for metastasis. 35 Pop Quiz What is the code for CS Mets at DX? a. 00: No distant metastasis b. 23: Separate tumor nodule(s) in contralateral lung c. 40: Distant metastasis d. 41: NAACCR Webinar Series 18
19 SSF1: Separate Tumor Nodules Ipsilateral Lung Code Description 000 No separate tumor nodules noted 010 Separate tumor nodules in ipsilateral lung, same lobe 020 Separate tumor nodules in ipsilateral lung, different lobe Separate tumor nodules, ipsilateral lung, unknown if same or different lobe 988 Not applicable: Information not collected for this case 999 Unknown if separate tumor nodules Separate tumor nodules cannot be assessed Not documented in patient record 37 Pop Quiz Left upper lung lobe biopsy: Adenocarcinoma. Chest CT scan: Multiple lung nodules are present; LUL 2.1cm, RML 2.0cm, RML less than 4 mm, LLL less than 4mm; bilateral mediastinal lymphadenopathy; metastatic nodules in right ribs. Discharge summary final diagnosis: Left lung carcinoma with metastasis. 38 NAACCR Webinar Series 19
20 Pop Quiz What is the code for SSF1? a. 000: No separate tumor nodules noted b. 010: Separate tumor nodules in ipsilateral lung, same lobe c. 020: Separate tumor nodules in ipsilateral lung, different lobe d. 030: e. 040: Separate tumor nodules, ipsilateral lung, unknown if same or different lobe 39 SSF2: Pleural/Elastic Layer Invasion (PL) by H and E or Elastic Stain Code level of pleural layer (PL) invasion as documented on path report Assign code 998 if no histologic exam of pleura FNA is not adequate to assess PL invasion 40 NAACCR Webinar Series 20
21 SSF2: Pleural/Elastic Layer Invasion (PL) by H and E or Elastic Stain PL0: Tumor does not completely traverse elastic layer PL1: Tumor extends through elastic layer PL2: Tumor extends to surface of visceral pleura PL3: Tumor extends to parietal pleura 41 Pop Quiz Wedge resection of right middle lobe of lung and lymph node dissection: Histologic tumor type: Squamous cell carcinoma Histologic tumor grade: 2 of 4 Tumor focality: Single tumor Tumor size: 3.4 cm Visceral pleura involvement: Tumor extends to but not through the elastic layer Margins: Negative Lymph node status: 0/12 42 NAACCR Webinar Series 21
22 Pop Quiz What is the code for SSF2? a. 000: PL0 b. 010: PL1 c. 020: PL2 d. 030: PL3 e. 040: Invasion of pleura NOS 43 AJCC Cancer Stage Lung: Chapter NAACCR Webinar Series 22
23 AJCC Cancer Stage: Lung Classification Clinical staging Evidence acquired prior to treatment Physical exam, imaging studies, lab tests, and staging procedures Pathologic staging Evidence acquired prior to treatment + evidence acquired during and after surgery, particularly from pathologic exam Resection of primary tumor sufficient to evaluate highest pt Removal of sufficient number of lymph nodes to evaluate highest pn 45 AJCC Cancer Stage: Lung ICD O 3 Topography Codes C34.0, C34.1, C34.2, C34.3, C34.8, C34.9 ICD O 3 Histology Code Ranges NAACCR Webinar Series 23
24 AJCC Cancer Stage: Lung T Category TX: Primary tumor cannot be assessed OR tumor proven by presence of malignant cells in sputum or bronchial washings but not visualized by imaging or bronchoscopy T0: No evidence of primary tumor Tis: Carcinoma in situ 47 AJCC Cancer Stage: Lung T Category T1: Tumor 3 cm or less surrounded by lung or visceral pleura without bronchoscopic evidence of invasion more proximal than the lobar bronchus T1a: Tumor 2 cm or less T1b: Tumor more than 2 cm but 3 cm or less 48 NAACCR Webinar Series 24
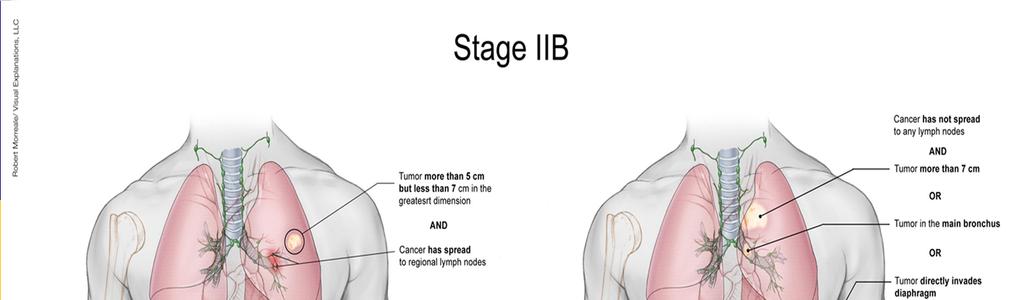
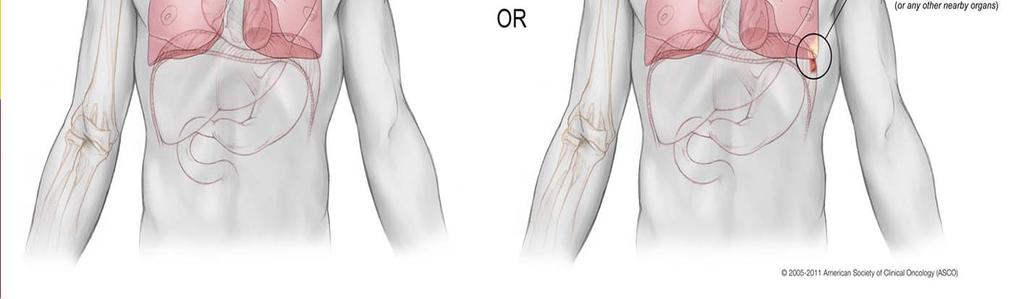
25 AJCC Cancer Stage: Lung T Category T2 Tumor more than 3 cm but 7 cm or less OR Any of the following features Involves main bronchus 2 cm or more distal to carina Invades visceral pleura (PL1 or PL2) Associated with atelectasis or obstructive pneumonitis that extends to hilar region but does not involve entire lung T2 tumors with above features are T2a if 5 cm or less T2a: Tumor more than 3 cm but 5 cm or less T2b: Tumor more than 5 cm but 7 cm or less 49 AJCC Cancer Stage: Lung T Category T3 Tumor more than 7cm OR Directly invades any of the following: parietal pleura (PL3) chest wall (including superior sulcus tumors), diaphragm, phrenic nerve, mediastinal pleura, parietal pericardium OR Tumor in main bronchus less than 2 cm distal to carina but without involvement of carina OR Associated atelectasis or obstructive pneumonitis of entire lung OR Separate tumor nodule(s) in same lobe 50 NAACCR Webinar Series 25
26 AJCC Cancer Stage: Lung T Category T4: Tumor of any size invades Mediastinum, heart, great vessels, trachea, recurrent laryngeal nerve, esophagus, vertebral body, and/or carina Separate tumor nodule(s) in different ipsilateral lobe 51 AJCC Cancer Stage: Lung N Category NX: Regional lymph nodes cannot be assessed N0: No regional lymph node metastasis N1: Metastasis in ipsilateral peribronchial and/or ipsilateral hilar lymph nodes and intrapulmonary nodes including involvement by direct extension N2: Metastasis in ipsilateral mediastinal and/or subcarinal lymph nodes N3: Metastasis in contralateral mediastinal, contralateral hilar, ipsilateral or contralateral scalene, or supraclavicular lymph nodes 52 NAACCR Webinar Series 26
27 AJCC Cancer Stage: Lung M Category M0: No distant metastasis M1: Distant metastasis M1a Separate tumor nodule(s) in contralateral lobe tumor with pleural nodules OR Malignant pleural or pericardial effusion M1b: Distant metastasis (in extrathoracic organs) 53 AJCC Cancer Stage: Lung Stage T N M 0ccult carcinoma X is NAACCR Webinar Series 27


28 55 56 NAACCR Webinar Series 28


29 57 58 NAACCR Webinar Series 29

30 59 60 NAACCR Webinar Series 30


31 61 Pop Quiz CT/PET: 6 cm mass in right middle and upper lung lobe, most likely malignant, with tumor associated obstructive pneumonitis in the upper lobe. No lymphadenopathy or metastasis observed. Right middle and upper lung lobectomies: Moderately differentiated squamous cell carcinoma, 6 x 5 x 4.5 cm, of upper and middle lobes obliterates the fissure. No evidence of any mass lesions within the bronchial tree. Tumor is confined within the lung parenchyma with no invasion of the visceral pleura. Margins clear. 19 lymph nodes dissected; microscopic focus of metastasis in 1 ipsilateral hilar node. 62 NAACCR Webinar Series 31
32 Pop Quiz What is the AJCC clinical stage? ct2b cn0 cm0 c stage group IIA What is the AJCC pathologic stage? pt2b pn1 cm0 p stage group IIB 63 Summary Stage Lung 64 NAACCR Webinar Series 32
33 Summary Stage In situ Noninvasive; intraepithelial 1 Localized Confined to carina Confined to hilus of lung Confined to main stem bronchus >2.0 cm from carina Confined to main stem bronchus NOS Extension from other parts of lung to main stem bronchus >2.0 cm from carina Extension from other parts of lung to main stem bronchus NOS Single tumor confined to 1 lung Localized NOS Summary Stage Regional by direct extension only Extension to major blood vessels, brachial plexus from superior sulcus, carina from lung, chest wall, diaphragm, esophagus, main stem bronchus < 2 cm from carina, mediastinum (extrapulmonary or NOS), nerves (cervical sympathetic, phrenic, recurrent laryngeal, vagus), pancoast tumor, parietal pleura, parietal pericardium, pericardium NOS, pleura NOS, pulmonary ligament, trachea, visceral pleura Separate tumor nodule(s) in same lobe Separate tumor nodule(s) in main stem bronchus Tumor of main stem bronchus < 2 cm from carina 66 NAACCR Webinar Series 33
34 Summary Stage Regional IPSILATERAL lymph nodes(s) involved only Aortic NOS, peri/para aortic, subaortic, bronchial, carinal, hilar, intrapulmonary, mediastinal, pericardial, peri/parabronchial, peri/paraesophageal, peri/paratracheal, pre and retrotracheal, pulmonary ligament, subcarinal Regional lymph nodes NOS 4 Regional by BOTH direct extension AND IPSILATERAL regional lymph node(s) involved Summary Stage 2000 codes Regional NOS 67 Summary Stage Distant site(s)/lymph node(s) involved Distant lymph nodes Cervical, contralateral/bilateral hilar, contralateral/bilateral mediastinal, scalene (ipsilateral or contralateral), supraclavicular (ipsilateral or contralateral), other distant lymph nodes Extension to Abdominal organs, adjacent rib, contralateral lung, contralateral main stem bronchus, heart, pericardial effusion, pleural effusion, skeletal muscle, skin of chest, sternum, vertebra(e), visceral pericardium Separate tumor nodule(s) in different lobe Separate tumor nodule(s) in contralateral lung Metastasis 68 NAACCR Webinar Series 34
35 Pop Quiz CT Chest: 8.3 cm left lung upper lobe mass. Left hilar adenopathy, most likely malignant. 1.9 cm left adrenal mass consistent with adrenal adenoma. Small left sided pleural effusion. Left upper lobe lung biopsy: Poorly differentiated adenocarcinoma. Patient deemed inoperable and referred to oncology for treatment plan. 69 Pop Quiz What is the Summary Stage 2000? a. 0 In situ b. 1 Localized c. 2 Regional by direct extension only d. 3 Regional ipsilateral regional lymph node(s) involved only e. 4 Regional by both extension and ipsilateral regional lymph node(s) involved f. 5 Regional NOS g. 7 Distant site(s)/node(s) involved 70 NAACCR Webinar Series 35

36 Quiz 71 Diagnostic and Staging Procedures MRI CT Scan PET Scan Bronchoscopy Mediastinoscopy Lymph Node Sampling 72 NAACCR Webinar Series 36
37 Treatment 73 NSCLC Surgery provides the best chance of cure for patients with Stage I or Stage II 74 NAACCR Webinar Series 37
38 Surgical Procedures Lobectomy (30) Removal of an entire lobe Sleeve Lobectomy (30) Removes a lobe of the lung plus part of the airway and then reattaches the airway Pneumonectomy (55) Removal of entire lung 75 Surgical Procedures Sublobar resection Segmentectomy (22) Wedge resection (21) 76 NAACCR Webinar Series 38

39 Lymph Node Dissection Lymph node sampling is appropriate for patients with N0 disease having pulmonary resection Right side primary 2R, 4R, 7, 8, and 9 Left side primary 4L, 5, 6, 7, 8, and 9 77 NSCLC Stage IIIA N2 Patients with a single positive N2 node less than 3cm, may be eligible for surgery after neoadjuvant treatment 78 NAACCR Webinar Series 39
40 Radiation (RT) May be given as Adjuvant treatment for patients with resectable disease Primary local treatment Palliative treatment CT Planned 3D conformal RT is now considered minimum standard 4D conformal, intensity modulated RT/ volumetric modulated arc (IMRT/VMAT), image guided RT, motion management strategies, and proton therapy have been shown to reduce toxicity and improve survival 79 RT Recommended for early stage NSCLC patients that are medically inoperable or refuse surgery. Definitive chemoradiation is recommended for patients who are stage II III 80 NAACCR Webinar Series 40
41 RT Stereotactic Ablative Radiotherapy (SABR) Uses short courses of very high dose RT that are precisely delivered to the target. Improved 3 year survival in patients with stage I disease. Whole Brain RT and Stereotactic Radiosurgery 81 Chemotherapy May be given as Neoadjuvant Adjuvant therapy Chemoradiation Usually platinum based Cisplatin May be targeted therapy Erlotinib Crizotinib 82 NAACCR Webinar Series 41
42 Small Cell Lung Cancer Limited Stage Any AJCC stage I III (any T, any N, M0) that can be treated with definitive radiation Unless there are multiple lung nodules Extensive stage is a stage 4 (any T, any N, M1a or M1b) of T3 4 with multiple nodules or a tumor too big to be treated by radiation. 83 Surgery Patients with stage I disease are surgical candidates Less than 5% of patients present with stage I disease Patients should have a thorough staging evaluation prior to resection Adjuvant chemotherapy is required 84 NAACCR Webinar Series 42
43 Chemotherapy Adjuvant chemotherapy for patients who are surgical candidates Chemotherapy is the primary treatment for patients with extensive disease Concurrent chemotherapy and radiation is recommended for patients with limited stage disease that are not surgical candidates Etoposide and cisplatin (EP) is a common regimen 85 RT For limited stage disease concurrent RT with chemotherapy is preferred to sequential RT and chemotherapy. For extensive stage thoracic RT may be beneficial for selected patients. Prophylactic Cranial Irradiation in patients with good responses to initial therapy decreases brain mets and increases overall survival. 86 NAACCR Webinar Series 43
44 Quiz 87 Coming Up Coding Pitfalls September 11, 2014 Registration is open for Cancer Registry & Surveillance Webinar Series NAACCR Webinar Series 44
45 And the winners are.. 89 CE Certificate Quiz/Survey Phrase Link NAACCR Webinar Series 45
46 Thank You!!!! Please send any questions to: Jim Hofferkamp Shannon Vann NAACCR Webinar Series 46
NAACCR Webinar Series 1
 Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung 2013 2014 NAACCR Webinar Series August 7, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Lung
 Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Collecting Cancer Data: Lung NAACCR 2011 2012 Webinar Series 2/2/2012 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this
Lung /1/16. Please submit all questions concerning webinar content through the Q&A panel. Reminder:
 1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
1 NAACCR 2015-2016 Webinar Series Collecting Cancer Data: Lung NAACCR 2015 2016 Webinar Series Presented by: Angela Martin amartin@naaccr.org Jim Hofferkamp jhofferkamp@naaccr.org Q&A Please submit all
AJCC-NCRA Education Needs Assessment Results
 AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
AJCC-NCRA Education Needs Assessment Results Donna M. Gress, RHIT, CTR Survey Tool 1 Survey Development, Delivery, Analysis THANKS to NCRA for the following work Developed survey with input from partners
Collaborative Stage. Site-Specific Instructions - LUNG
 Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Slide 1 Collaborative Stage Site-Specific Instructions - LUNG In this presentation, we are going to review the AJCC Cancer Staging criteria for the lung primary site. Slide 2 Reading Assignments As each
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Lung /4/18. Please submit all questions concerning the webinar content through the Q&A panel.
 Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
The 8th Edition Lung Cancer Stage Classification
 The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
The 8th Edition Lung Cancer Stage Classification Elwyn Cabebe, M.D. Medical Oncology, Hematology, and Hospice and Palliative Care Valley Medical Oncology Consultants Director of Quality, Medical Oncology
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
Role of Surgery in Management of Non Small Cell Lung Cancer. Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City
 Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
B REAST STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi c a b c d TUMOR SIZE:
FDG PET/CT in Lung Cancer Read with the experts. Homer A. Macapinlac, M.D.
 FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
FDG PET/CT in Lung Cancer Read with the experts Homer A. Macapinlac, M.D. Patient with suspected lung cancer presents with left sided chest pain T3 What is the T stage of this patient? A) T2a B) T2b C)
B REAST STAGING FORM. PATHOLOGIC Extent of disease through completion of definitive surgery. CLINICAL Extent of disease before any treatment
 B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
B REAST STAGING FORM Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery (DCIS) (LCIS) (Paget s) mi a b c a b c d TUMOR SIZE: S TAGE
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Lung. 10/24/13 Chest X-ray: 2.9 cm mass like density in the inferior lingular segment worrisome for neoplasm. Malignancy cannot be excluded.
 Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Lung Case Scenario 1 A 54 year white male presents with a recent abnormal CT of the chest. The patient has a history of melanoma, kidney, and prostate cancers. 10/24/13 Chest X-ray: 2.9 cm mass like density
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer. Doug Rahn 6/1/12
 Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
Case Conference: Post-Operative Radiotherapy for Non-Small Cell Lung Cancer Doug Rahn 6/1/12 Outline I. Presentation of Case II. Epidemiology III. Staging IV. Review of Literature V. Recommendations VI.
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
Lung Cancer Imaging. Terence Z. Wong, MD,PhD. Department of Radiology Duke University Medical Center Durham, NC 9/9/09
 Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
Lung Cancer Imaging Terence Z. Wong, MD,PhD Department of Radiology Duke University Medical Center Durham, NC 9/9/09 Acknowledgements Edward F. Patz, Jr., MD Jenny Hoang, MD Ellen L. Jones, MD, PhD Lung
6 th Reprint Handbook Pages AJCC 7 th Edition
 6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
6 th Reprint Handbook Pages AJCC 7 th Edition AJCC 7 th Edition Errata for 6 th Reprint Table 1 Handbook No Significant Staging Clarifications for 6 th Reprint AJCC 7 th Edition Errata for 6 th Reprint
Non small cell Lung Cancer
 Non small cell Lung Cancer The 13th refresher course for residents in radiation oncology Jiraporn Setakornnukul, M.D. Radiation oncology division, Radiology department Siriraj Hospital, Mahidol University
Non small cell Lung Cancer The 13th refresher course for residents in radiation oncology Jiraporn Setakornnukul, M.D. Radiation oncology division, Radiology department Siriraj Hospital, Mahidol University
Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer. Quick Reference Chart and Diagrams
 CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
CHEST Special Features Seventh Edition of the Cancer Staging Manual and Stage Grouping of Lung Cancer Quick Reference Chart and Diagrams Omar Lababede, MD ; Moulay Meziane, MD ; and Thomas Rice, MD, FCCP
Histopathology of NSCLC, IHC markers and ptnm classification
 ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
ESMO Preceptorship on Non-Small Cell Lung Cancer November 15 th & 16 th 2017 Singapore Histopathology of NSCLC, IHC markers and ptnm classification Prof Keith M Kerr Department of Pathology, Aberdeen University
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Surgical management of lung cancer
 Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Surgical management of lung cancer Nick Roubos FRACS Cardiothoracic Surgeon Box Hill Hospital, Epworth Eastern Thoracic Oncology Non Small Cell Lung Cancer (NSCLC) Small Cell Lung Cancer Mesothelioma Pulmonary
Chest X-ray Interpretation
 Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
Chest X-ray Interpretation Introduction Routinely obtained Pulmonary specialist consultation Inherent physical exam limitations Chest x-ray limitations Physical exam and chest x-ray provide compliment
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Testicular Malignancies /8/15
 Collecting Cancer Data: Testis 2014-2015 NAACCR Webinar Series January 8, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Testis 2014-2015 NAACCR Webinar Series January 8, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL
 LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
and Strength of Recommendations
 ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
THORACIC MALIGNANCIES
 THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
THORACIC MALIGNANCIES Summary for Malignant Malignancies. Lung Ca 1 Lung Cancer Non-Small Cell Lung Cancer Diagnostic Evaluation for Non-Small Lung Cancer 1. History and Physical examination. 2. CBCDE,
The International Association for the Study of Lung Cancer (IASLC) Lung Cancer Staging Project, Data Elements
 Lung Cancer Staging Project, Data Elements") Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Page 1 Contents 1.1. Registration... 2 1.2. Patient Characteristics... 3 1.3. Laboratory Values at Diagnosis... 5 1.4. Lung Cancers with Multiple Lesions... 6 1.5. Primary Tumour Description... 10 1.6.
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
WHITE PAPER - SRS for Non Small Cell Lung Cancer
 WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
WHITE PAPER - SRS for Non Small Cell Lung Cancer I. Introduction This white paper will focus on non-small cell lung carcinoma with sections one though six comprising a general review of lung cancer from
ACRIN NLST 6654 Primary Lung Cancer. F1/F2 Interval: to (mm-dd-yyyy) 1. Date of diagnosis: (mm-dd-yyyy)
 1. Date of diagnosis: (mm-dd-yyyy)") No. F1/F2 Interval: - - 20 to - - 20 (mm-dd-yyyy) 1. Date of diagnosis: - - 20 (mm-dd-yyyy) 2. Samples recorded: ZP Number S-Number 1) 2) 3) 4) (Refer to Form PX, Column 1. In the rare instance of a diagnosis
No. F1/F2 Interval: - - 20 to - - 20 (mm-dd-yyyy) 1. Date of diagnosis: - - 20 (mm-dd-yyyy) 2. Samples recorded: ZP Number S-Number 1) 2) 3) 4) (Refer to Form PX, Column 1. In the rare instance of a diagnosis
LUNG CANCER. Agnieszka Słowik, MD. Department of Oncology, University Hospital in Cracow Jagiellonian University
 LUNG CANCER Agnieszka Słowik, MD Department of Oncology, University Hospital in Cracow Jagiellonian University Epidemiology Most common malignancy worldwide Place of lung cancer among other malignancies
LUNG CANCER Agnieszka Słowik, MD Department of Oncology, University Hospital in Cracow Jagiellonian University Epidemiology Most common malignancy worldwide Place of lung cancer among other malignancies
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Thyroid and Adrenal Gland
 Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Thyroid and Adrenal Gland NAACCR 2011 2012 Webinar Series 12/1/11 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Mediastinal Mysteries: What can be solved with EBUS?
 Mediastinal Mysteries: What can be solved with EBUS? W. Graham Carlos MD Pulmonary & Critical Care Fellow Indiana University School of Medicine Disclosures None Objectives Introduce you to the technique
Mediastinal Mysteries: What can be solved with EBUS? W. Graham Carlos MD Pulmonary & Critical Care Fellow Indiana University School of Medicine Disclosures None Objectives Introduce you to the technique
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
FDG PET/CT STAGING OF LUNG CANCER. Dr Shakher Ramdave
 FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
FDG PET/CT STAGING OF LUNG CANCER Dr Shakher Ramdave FDG PET/CT STAGING OF LUNG CANCER FDG PET/CT is used in all patients with lung cancer who are considered for curative treatment to exclude occult disease.
Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!!
 The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
The lateral chest radiograph: Challenging area around the thoracic aorta!!! Do you want to be an excellent Radiologist? - Focus on the thoracic aorta on lateral chest image!!! Dong Yoon Han 1, So Youn
NAACCR Webinar Series 1
 Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Chief Complain. For chemotherapy
 Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Chief Complain For chemotherapy Present Illness 93.12 Progressive weakness of R t arm for 1 year X-ray: peneative lesion over right proximal humorous Bone scan: multiple increased intake Biopsy of distal
Lung Cancer. Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD
 Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
Lung Cancer Current Therapy JEREMIAH MARTIN MBBCh FRCSI MSCRD Objectives Describe risk factors, early detection & work-up of lung cancer. Define the role of modern treatment options, minimally invasive
Lung cancer forms in tissues of the lung, usually in the cells lining air passages.
 Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
Scan for mobile link. Lung Cancer Lung cancer usually forms in the tissue cells lining the air passages within the lungs. The two main types are small-cell lung cancer (usually found in cigarette smokers)
Coding Pitfalls 9/11/14
 Coding Pitfalls 2013 2014 NAACCR Webinar Series September 11, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Coding Pitfalls 2013 2014 NAACCR Webinar Series September 11, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Boot Camp Case Scenarios
 Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Boot Camp Case Scenarios Case Scenario 1 Patient is a 69-year-old white female. She presents with dyspnea on exertion, cough, and right rib pain. Patient is a smoker. 9/21/12 CT Chest FINDINGS: There is
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Lung Carcinoid Tumor Early Detection, Diagnosis, and Staging
 Lung Carcinoid Tumor Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can
Lung Carcinoid Tumor Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can
LungStage. Bringing machine learning to Nuclear Medicine and Lung Cancer using Big Data, Machine Learning and Multicenter Studies
 LungStage Bringing machine learning to Nuclear Medicine and Lung Cancer using Big Data, Machine Learning and Multicenter Studies Medical Team: Bram Stieltjes, MD PhD; Alex Sauter, MD; Gregor Sommer, MD;
LungStage Bringing machine learning to Nuclear Medicine and Lung Cancer using Big Data, Machine Learning and Multicenter Studies Medical Team: Bram Stieltjes, MD PhD; Alex Sauter, MD; Gregor Sommer, MD;
Educational Objectives. Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach.
 Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Managing Lung Cancer From the Solitary Pulmonary Nodule to Complex Cases: A Multidisciplinary Approach Robert A. Meguid, MD, MPH, FACS Assistant Professor of Cardiothoracic Surgery Surgical Director, Surgical
Summary Stage 2018 (SS2018)
") Summary Stage 2018 (SS2018) NAACCR October Webinar October 24, 2018 General Information 2 Summary Stage 2018 1 General Summary Stage is ANATOMICALLY based Unlike AJCC, it does not use the following in
Summary Stage 2018 (SS2018) NAACCR October Webinar October 24, 2018 General Information 2 Summary Stage 2018 1 General Summary Stage is ANATOMICALLY based Unlike AJCC, it does not use the following in
3/30/2009 Lung Cancer Deaths 2008 Lung Cancer Deaths Lung Cancer Deaths--Males Males 5
 LUNG CANCER 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Very common Very lethal Lung Cancer Median age of diagnosis approximately 70 years, but affects all ages(even pediatric!) Advances in
LUNG CANCER 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Very common Very lethal Lung Cancer Median age of diagnosis approximately 70 years, but affects all ages(even pediatric!) Advances in
Lung Cancer Incidence 2008 Lung Cancer Deaths-Males 2008 Incidence Total U.S.(all types): 1,437,180 Lung Cancer Deaths-Females Lung cancer 215,000(15%
: 1,437,180 Lung Cancer Deaths-Females Lung cancer 215,000(15%") Multidisciplinary approach 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Neurology Neurosurgery Orthopedic surgery General surgery Vascular surgery Gastroenterology Cardiology Lung Cancer Very
Multidisciplinary approach 2009 Mark B. Stoopler, M.D. Division of Medical Oncology Neurology Neurosurgery Orthopedic surgery General surgery Vascular surgery Gastroenterology Cardiology Lung Cancer Very
Small Cell Lung Cancer Early Detection, Diagnosis, and Staging
 Small Cell Lung Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that
Small Cell Lung Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that
Liver 6/5/14. Collecting Cancer Data: Liver NAACCR Webinar Series. June 5, 2014
 Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Liver 2013 2014 NAACCR Webinar Series June 5, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
2018 Implementation: SEER Summary Stage 2018
 2018 Implementation: SEER Summary Stage 2018 PRESENTED BY JENNIFER RUHL OCTOBER 24, 2018 10/23/2018 1 Q&A Please submit all questions concerning the content of the webinar through the Q&A panel Submit
2018 Implementation: SEER Summary Stage 2018 PRESENTED BY JENNIFER RUHL OCTOBER 24, 2018 10/23/2018 1 Q&A Please submit all questions concerning the content of the webinar through the Q&A panel Submit
NAACCR Webinar Series 11/2/2017
 COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: LARYNX 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Lung cancer LUNG CANCER. Box 1 Clinical signs
 22 LUNG CANCER Lung cancer Bronchial carcinoma refers to two distinct clinical entities small cell and non-small cell carcinoma. Although these conditions have much in common, with broadly similar presenting
22 LUNG CANCER Lung cancer Bronchial carcinoma refers to two distinct clinical entities small cell and non-small cell carcinoma. Although these conditions have much in common, with broadly similar presenting
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Lung Cancer Very common Very lethal Median age of diagnosis i approximately 70 years, but affects all ages In the United States, the highest incidence
 LUNG CANCER 2010 Mark B. Stoopler, M.D. Division of Medical Oncology Lung Cancer Very common Very lethal Median age of diagnosis i approximately 70 years, but affects all ages In the United States, the
LUNG CANCER 2010 Mark B. Stoopler, M.D. Division of Medical Oncology Lung Cancer Very common Very lethal Median age of diagnosis i approximately 70 years, but affects all ages In the United States, the
Case 1: Early Stage NSCLC. Dr. Dhar Dr. Coughlin Dr. Kay Dr. Hirmiz
 Case 1: Early Stage NSCLC Dr. Dhar Dr. Coughlin Dr. Kay Dr. Hirmiz 62M with 2 months of worsening cough, productive of white sputum. No significant dyspnea. ROS otherwise negative. PMHx: Hypertension,
Case 1: Early Stage NSCLC Dr. Dhar Dr. Coughlin Dr. Kay Dr. Hirmiz 62M with 2 months of worsening cough, productive of white sputum. No significant dyspnea. ROS otherwise negative. PMHx: Hypertension,
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma [Based on WOSCAN SCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED WHEN PRINTED Document
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Mesothelioma [Based on WOSCAN SCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED WHEN PRINTED Document
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Non-Small Cell Lung Cancer Early Detection, Diagnosis, and Staging
 Non-Small Cell Lung Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
Non-Small Cell Lung Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
The Itracacies of Staging Patients with Suspected Lung Cancer
 The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
The Itracacies of Staging Patients with Suspected Lung Cancer Gerard A. Silvestri, MD,MS, FCCP Professor of Medicine Medical University of South Carolina Charleston, SC silvestri@musc.edu Staging Lung
Adam J. Hansen, MD UHC Thoracic Surgery
 Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Adam J. Hansen, MD UHC Thoracic Surgery Sometimes seen on Chest X-ray (CXR) Common incidental findings on computed tomography (CT) chest and abdomen done for other reasons Most lung cancers discovered
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
OBJECTIVES. Solitary Solid Spiculated Nodule. What would you do next? Case Based Discussion: State of the Art Management of Lung Nodules.
 Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Organ Imaging : September 25 2015 OBJECTIVES Case Based Discussion: State of the Art Management of Lung Nodules Dr. Elsie T. Nguyen Dr. Kazuhiro Yasufuku 1. To review guidelines for follow up and management
Imaging of Lung Cancer: A Review of the 8 th TNM Staging System
 Imaging of Lung Cancer: A Review of the 8 th TNM Staging System Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco
Imaging of Lung Cancer: A Review of the 8 th TNM Staging System Travis S Henry, MD Associate Professor of Clinical Radiology Cardiac and Pulmonary Imaging Section University of California, San Francisco
Thoracic Surgery; An Overview
 Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Thoracic Surgery What we see Thoracic Surgery; An Overview James P. Locher, Jr, MD Methodist Cardiovascular and Thoracic Surgery Lung cancer Mets Fungus and TB Lung abcess and empyema Pleural based disease
Special Treatment Issues in Non-small Cell Lung Cancer
 CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Special Treatment Issues in Non-small Cell Lung Cancer Diagnosis and Management of Lung Cancer, 3rd ed: American College
CHEST Supplement DIAGNOSIS AND MANAGEMENT OF LUNG CANCER, 3RD ED: ACCP GUIDELINES Special Treatment Issues in Non-small Cell Lung Cancer Diagnosis and Management of Lung Cancer, 3rd ed: American College
Lung & Pleura. The Topics :
 Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Lung & Pleura The Topics : The Trachea. The Bronchi. The Brochopulmonary Segments. The Lungs. The Hilum. The Pleura. The Surface Anatomy Of The Lung & Pleura. The Root & Hilum. - first of all, the lung
Lung Cancer Resection
 Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
Lung Cancer Resection Introduction The occurrence of lung cancer has increased dramatically over the last 50 years. Your health care provider may have recommended an operation to remove your lung cancer.
NAACCR Webinar Series 1
 Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Lip and Oral 2013 2014 NAACCR Webinar Series October 3, 2013 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013
 Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Lecturer: Ms DS Pillay ROOM 2P24 25 February 2013 Thoracic Wall Consists of thoracic cage Muscle Fascia Thoracic Cavity 3 Compartments of the Thorax (Great Vessels) (Heart) Superior thoracic aperture
Thursday, August 16, :30 AM - 4:30 PM and Friday, August 17, :30 AM 12:00 PM Crowne Plaza 830 Phillips Lane Louisville, KY 40209
 KCR newsletter March 2018 KCR 2018 Fall Workshop/Regional Meeting 2018 Tri-State Regional Cancer Registrars Meeting Presented by: Kentucky Cancer Registry, Indiana Cancer Consortium, and Ohio Cancer Incidence
KCR newsletter March 2018 KCR 2018 Fall Workshop/Regional Meeting 2018 Tri-State Regional Cancer Registrars Meeting Presented by: Kentucky Cancer Registry, Indiana Cancer Consortium, and Ohio Cancer Incidence
9/17/2013. Presentation Outline. Overview
 FCDS 2013 Educational Webcast Series September 19, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff Presentation Outline Overview of Lung Cancer Signs, Symptoms and Risk Factors Anatomy
FCDS 2013 Educational Webcast Series September 19, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff Presentation Outline Overview of Lung Cancer Signs, Symptoms and Risk Factors Anatomy
FCDS 2013 Educational Webcast Series September 19, Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff
 FCDS 2013 Educational Webcast Series September 19, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff Presentation Outline Overview of Lung Cancer Signs, Symptoms and Risk Factors Anatomy
FCDS 2013 Educational Webcast Series September 19, 2013 Mayra Espino, BA, RHIT, CTR Steven Peace, BS, CTR FCDS QC Staff Presentation Outline Overview of Lung Cancer Signs, Symptoms and Risk Factors Anatomy
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Lung Cancer Clinical Guidelines: Surgery
 Lung Cancer Clinical Guidelines: Surgery 1 Scope of guidelines All Trusts within Manchester Cancer are expected to follow this guideline. This guideline is relevant to: Adults (18 years and older) with
Lung Cancer Clinical Guidelines: Surgery 1 Scope of guidelines All Trusts within Manchester Cancer are expected to follow this guideline. This guideline is relevant to: Adults (18 years and older) with
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Non-Small Cell Lung Cancer Early Detection, Diagnosis, and Staging
 Non-Small Cell Lung Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
Non-Small Cell Lung Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
PLACE LABEL HERE. Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form. RTOG Study No.
 Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form RTOG Study No. 0813 Case # Name RTOG Patient ID INSTRUCTIONS: Submit this form at the appropriate followup
Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form RTOG Study No. 0813 Case # Name RTOG Patient ID INSTRUCTIONS: Submit this form at the appropriate followup
Dr. Andres Wiernik. Lung Cancer
 Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional