CANCER IN TASMANIA INCIDENCE AND MORTALITY 1999
|
|
|
- Aubrie Simpson
- 6 years ago
- Views:
Transcription
1 CANCER IN TASMANIA INCIDENCE AND MORTALITY 1999
2
3 CANCER IN TASMANIA INCIDENCE AND MORTALITY 1999 Menzies Centre for Population Health Research University of Tasmania Tasmanian Cancer Registry 17 Liverpool Street Hobart Tasmania Australia 7000 Postal address: GPO Box Hobart Tasmania Australia 7001 Telephone (03) Facsimile (03) URL: Editors: Pavlides S, Venn A, Blizzard L, Dwyer T. Publication date: July 2002
4 Acknowledgments The Tasmanian Cancer Registry is funded by the Tasmanian Department of Health and Human Services (DHHS), through its Health Advancement Program, and by the Menzies Centre. Additional funds are raised from the community and research funding bodies. This report has been made possible through the collaboration of various people and organisations within Tasmania and across Australia. The Registry s work would not be possible without the assistance of the staff of the State s pathology laboratories, hospital medical records departments, the WP Holman Clinics, the office of the Registrar of Births, Deaths and Marriages, the medical community, the Coroner s Office, the Australian Bureau of Statistics and the interstate cancer registries; their support is greatly appreciated. The adminstrative staff and volunteers of the Registry are commended for their commitment and efforts towards achieving accurate and complete data upon which this report is based. In addition, the voluntary assistance provided by the Advisory Committee and the Data Release Committee is greatly appreciated by the Registry. We thank other Menzies Centre staff for their assistance with statistical, computing, administrative, financial, media and editorial matters. Citation The following citation is suggested in referring to this report: The Tasmanian Cancer Registry, Menzies Centre for Population Health Research Cancer in Tasmania: Incidence and Mortality Hobart: Menzies Centre for Population Health Research, University of Tasmania 2
5 Contents The Tasmanian Cancer Registry Introduction Sources of data Data handling Data collection and coding practices Data control and quality assurance Publication of reports All Cancers All cancers combined, incidence and mortality, All cancers combined, time trends, Common Cancers Common cancers diagnosed in males, Common cancer-related deaths in males, Common cancers diagnosed in females, Common cancer-related deaths in females, Regional Distribution of Cancers Female Breast Cancer Tumour size Lymph node involvement Cancer Incidence and Mortality Table, Appendices Appendix A: Cancer codes and specific coding practices Appendix B: Statistical methods and calculations Appendix C: Population data Appendix D: Indices of data quality Appendix E: Use of cancer registry data Appendix F: Cancer registry staff, volunteers and committee members Appendix G: Incidence summary and mortality summary,
6 The Tasmanian Cancer Registry Introduction The Tasmanian Cancer Registry was established in 1977 as a population-based registry covering the State. The Registry was set up for the purpose of providing the State Government with accurate cancer incidence and mortality statistics and to provide the capacity to monitor cancer trends. In July 1988 the responsibility for the operation of the Cancer Registry was transferred from the Department of Health Services to the Menzies Centre for Population Health Research, University of Tasmania. Cancers were proclaimed as notifiable diseases in December 1992 and cancer registration since then has had a legislative basis. The Registry is assisted by an Advisory Committee and a Data Release Committee. The Registry staff currently comprises a Director, Registrar, Administrative Assistant, Medical Coder and a Clerical Assistant. Volunteers also assist with the paper data handling. The Registry has access to biostatisticians and a database administrator. The Tasmanian Cancer Registry is a full member of the Australasian Association of Cancer Registries (AACR) and the International Association of Cancer Registries (IACR). Sources of data All pathology laboratories in the State provide the Registry with copies of histopathology, cytology and cell marker reports of cancer. Notification of cancer forms are supplied by the two radiation oncology clinics. Private and public hospitals notify diagnoses of cancer to the Registry upon discharge of patients or provide a computerised listing of cancer cases periodically. Death certificates of Tasmanian people are reviewed for mention of cancer as a cause of death. Since 1994 breast and cervical cancer screening programs have been undertaken in Tasmania and listings from these sources are available to check against Registry records. Interstate registries supply data to the Tasmanian Cancer Registry on Tasmanian residents who seek treatment interstate or who move interstate at some time after cancer diagnosis. Data handling Paper copies of all data are retained. Paper records for persons deceased are archived two years after death. Data are entered into software provided by the South Australian Cancer Registry. Only one tumour per ICD-9 site can be recorded. The Tasmanian Cancer Registry collects and stores all pathology reports of non-melanoma skin cancers (NMSC) but these are not routinely entered onto the database. Incidence is not regularly reported due to resource considerations. Deaths from NMSC are reported annually. Data collection and coding practices Data collected by the Registry include demographic and clinical data for the cancer patient. Additional tumour data are collected for melanoma, lymphomas, unknown primaries, breast and bladder cancers. The Tasmanian Cancer Registry records multiple primary cancers in the same person, of which only some are counted for incidence purposes according to the rules of the International Agency for Research on Cancer (IARC) and IACR. The primary site of cancer is coded according to the International Classification of Diseases, ninth edition (ICD-9) and morphology according to the International Classification of Diseases for Oncology, second edition (ICD-O-2). Coding practices specific to the Tasmanian Cancer Registry are detailed in Appendix A. Data control and quality assurance The quality of information provided by the Registry depends on the quality of data received as well as the processing of data by the Registry. The indices used to measure the quality of the 1999 data are provided in Appendix D. The accuracy of data entry at the Tasmanian Cancer Registry is monitored by a case flagging system that is used to identify data that are entered in error. Data matching programs enable the identification and amendment of duplicate entries by identifying incorrect spellings, name changes upon marriage and 4
7 date of birth inconsistencies. In addition, the National Cancer Statistics Clearing House (NCSCH) collates all State and Territory data and checks for duplicate registrations across two or more States. To help achieve high data quality and case ascertainment, data are obtained from multiple sources such as pathology laboratories, hospitals and the Registrar of Births, Deaths and Marriages. Most registered cases include data from both a pathology laboratory and a hospital service (inpatient or radiation oncology clinic). Where insufficient information is received to enable complete registration, active follow-up is undertaken by contacting treating doctors and hospital medical records departments. Publication of reports The incidence and mortality data in this report are based on cancer registrations for 1999, and for in trend analysis, completed by 7 June Despite intensive efforts to ensure the completeness of incidence data, the database is continually updated by previously unregistered cases and new information for registered cases. This improves the quality of data but future publications and responses to requests for data will reflect any subsequent revisions to the data and may not exactly correspond to the figures in this report. Notifications of cancer are received and dealt with in a timely manner at the Tasmanian Cancer Registry. On average, the Registry receives cancer notifications once or twice a week from pathology laboratories, quarterly and ad hoc from hospitals, and monthly from the Registrar of Births, Deaths and Marriages. The cases are registered within two months of notification and cases that are incomplete are followed up over the next 18 months. 5
8 All Cancers All cancers combined, incidence and mortality, 1999 There were 2,235 new cases of cancer (excluding non-melanocytic skin cancers) diagnosed among Tasmanian residents during 1999 (1,203 males and 1,032 females). The overall age standardised incidence 1 was 344 per 100,000 in males and 278 per 100,000 in females. The risk of developing any cancer by the age of 75 years was approximately 1 in 3. This risk estimate does not include the risk of developing non-melanocytic skin cancer. Cancer incidence generally increased with age (Figure 1). Male rates exceeded female rates for Tasmanians aged 60 years or over. Prostate cancer and lung cancer were responsible for the greater male cancer incidence at these ages. Breast cancer accounted for the slightly higher female rates among younger adults. Figure 1: Age-specific incidence and mortality for all cancers (excluding non-melanocytic skin cancers), Male Incidence Female Incidence Male Mortality Female Mortality 3000 Age specific rates per 100, Age (years) 1 Age standardised rates were calculated using the World Standard Population. 6
9 There were 995 (550 males and 445 females) cancer related deaths among Tasmanian residents in Nine deaths were due to non-melanocytic skin cancer. The overall age standardised mortality was 149 per 100,000 for males and 104 per 100,000 for females. The risk of dying of cancer by age 75 years was 1 in 6 for males and 1 in 9 for females. All cancers combined, time trends, The age standardised incidence of all cancers combined (excluding non-melanocytic skin cancers) increased by more than 30% during the 22-year period (comparing with , the increase was 33.7% for males and 37.4% for females). Some of the largest increases were observed for prostate cancer in men and breast cancer in women. Those increases in incidence coincided with the greater use of PSA testing for prostate cancer in men and the introduction of mammography screening for breast cancer in women. Whilst incidence has been increasing, mortality rates have declined marginally. As can be seen from Figure 2, the difference between incidence and death rates has widened in consequence. Figure 2: Trends in age standardised incidence and mortality of all cancers (excluding non-melanocytic skin cancers), Male Incidence Female Incidence Male Mortality Female Mortality Age standardised rates per 100,000 Year 7
10 Common Cancers The five most common cancers (other than non-melanocytic skin cancer) diagnosed in 1999 accounted for 63% of all cancers in males and 59% of all cancers in females. Cancers of unknown primary site accounted for 3.8% of all cancers for males and 5.1% of all cancers for females. Common cancers diagnosed in males, 1999 The most common cancer in males was prostate cancer (23%), followed by colorectal cancer (15%), lung cancer (12%), melanoma skin cancer (7%) and bladder cancer (6%). While the number of prostate cancer cases was much greater than any other cancer, prostate cancer numbers have continued to decline since the peak in 1994 when 420 new prostate cancer cases were reported. Figure 3: Common cancers, 1999: males Prostate 276 Colorectal 180 Lung 143 Melanoma 87 Bladder Number of new cancer cases Common cancer-related deaths in males, 1999 Lung cancer accounted for 24% of all cancer-related deaths in male Tasmanian residents in 1999, followed by colorectal cancer (14%) and prostate cancer (13%). The next most common causes of cancer deaths were lymphomas (5%) and stomach cancer (4%). Figure 4: Common causes of cancer-related deaths, 1999: males Lung 130 Colorectal 78 Prostate 71 All Lymphomas 28 Stomach Number of new cancer cases 8
11 Common cancers diagnosed in females, 1999 The most common cancer in females was breast cancer, accounting for 24% of all cancers in females, followed by colorectal cancer (14%), melanoma skin cancer (10%), lung cancer (7%) and lymphomas (5%). Figure 5: Common cancers, 1999: females Breast 244 Colorectal 146 Melanoma 103 Lung 70 All Lymphomas Number of new cancer cases Common cancer-related deaths in females, 1999 The most common causes of cancer-related deaths in female Tasmanian residents in 1999 were breast cancer (20%), colorectal cancer (17%), lung cancer (12%), pancreatic cancer (6%), ovarian cancer (4%) and lymphomas (4%). Figure 6: Common causes of cancer related deaths, 1999: females Breast 87 Colorectal 74 Lung 52 Pancreas 26 Ovary All Lymphomas Number of new cancer cases 9
12 Regional Distribution of Cancers The regional distribution for each cancer site is shown as the number of cases and the percentage of cases for each cancer site in each statistical division (Table 1). This information is based on recorded postcode of residence. On the basis of population numbers in each of the statistical divisions, the distribution of cancers would be expected to be 49% in the south, 28% in the north and 23% in the Mersey-Lyell division. Variation around that distribution can be expected due to chance occurrences and differences in the age distribution between the regional populations. Table 1: Regional distribution of cancer incidence for all sites with a minimum of 50 new cases, 1999 ICD-9 Site Southern Northern Mersey-Lyell Total 229,119 (49%) 133,169 (28%) 108,515 (23%) 470,803* (100%) Colorectal 152 (47%) 91 (28%) 83 (25%) Prostate 133 (48%) 77 (28%) 66 (24%) Breast 118 (48%) 69 (28%) 59 (24%) Lung 103 (48%) 57 (27%) 53 (25%) Melanoma 108 (57%) 42 (22%) 40 (21%) All lymphomas 47 (44%) 23 (21%) 37 (35%) Bladder 47 (46%) 34 (33%) 21 (21%) Unspecified site 45 (48%) 31 (33%) 18 (19%) Kidney 39 (56%) 21 (30%) 10 (14%) Total new cases 1,120 (50%) 604 (27%) 511 (23%) 2,235 * Estimated Resident Population at June 1999 (ABS) 10
13 Female Breast Cancer Breast cancer tumour size and lymph node involvement were first recorded by the Tasmanian Cancer Registry in 1997 when funding was provided to all Australian cancer registries for this purpose. Tumour size In 1999, 97% of the 244 primary breast cancer cases (female) were histologically examined. Information about tumour size was available for 224 (92%) of these cases. For these tumours, 45 (20%) were less than 10mm in diameter, 95 (42%) were between 10 and 19mm, 68 (30%) were between 20 and 49mm, and 16 (7%) were greater than 50mm in diameter. Figure 7 compares categories of tumour size from 1997 to Figure 7: Breast cancer, : size of histologically-confirmed tumours Percentage of cases mm mm mm 50+ mm Tumour size Lymph node involvement Of the 224 tumours that were histologically examined and measured in 1999, lymph nodes were investigated in 163 (73%) of cases. Where nodal status was examined, 104 (64%) cases were classified as lymph node negative. Figure 8 compares categories of lymph node involvement from 1997 to Figure 8: Breast cancer, : lymph node involvement Percentage of cases nodes 1 3 nodes 4 6 nodes 7+ nodes Number of nodes involved 11
14 12
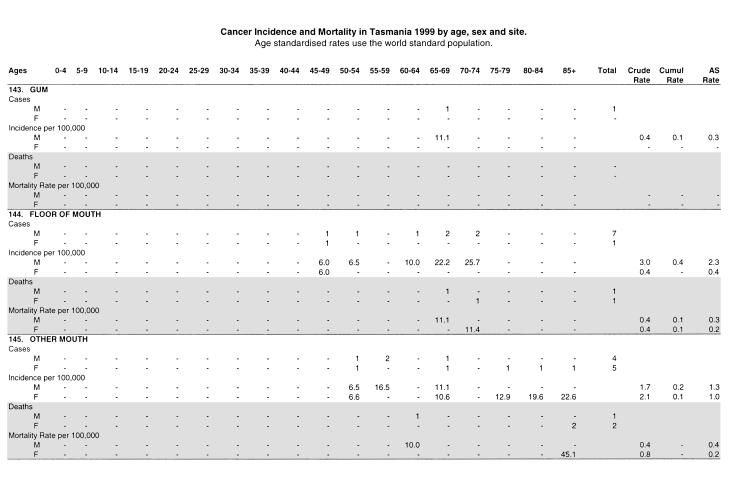
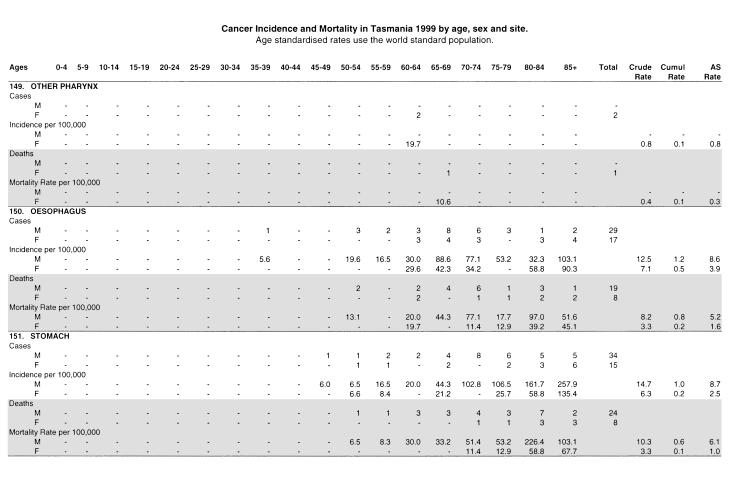
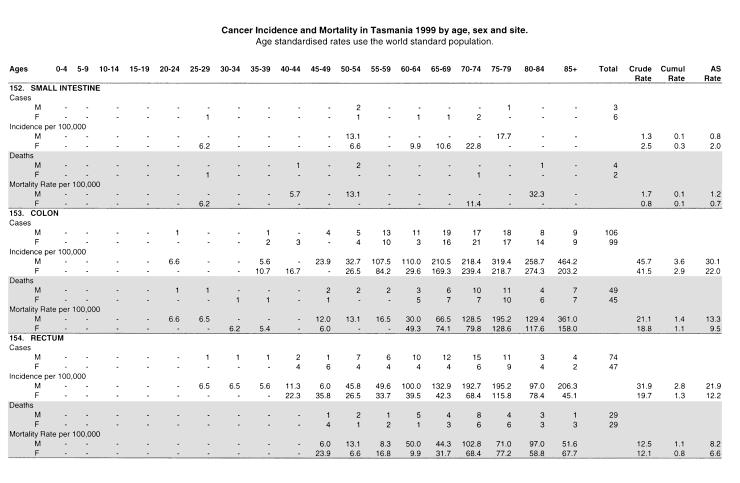
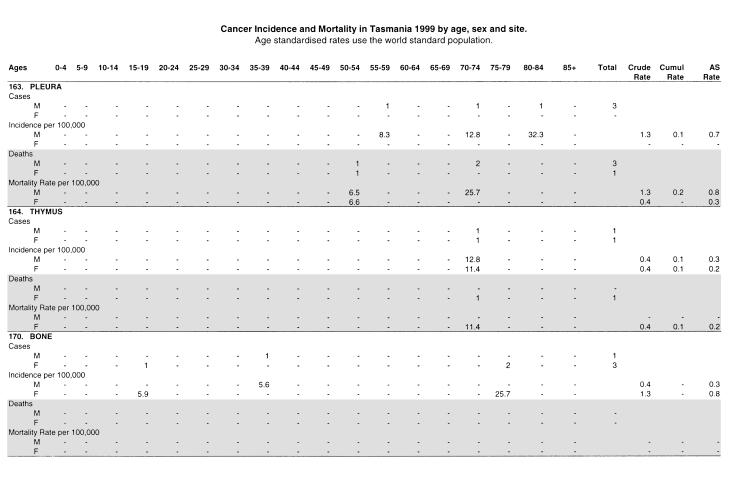
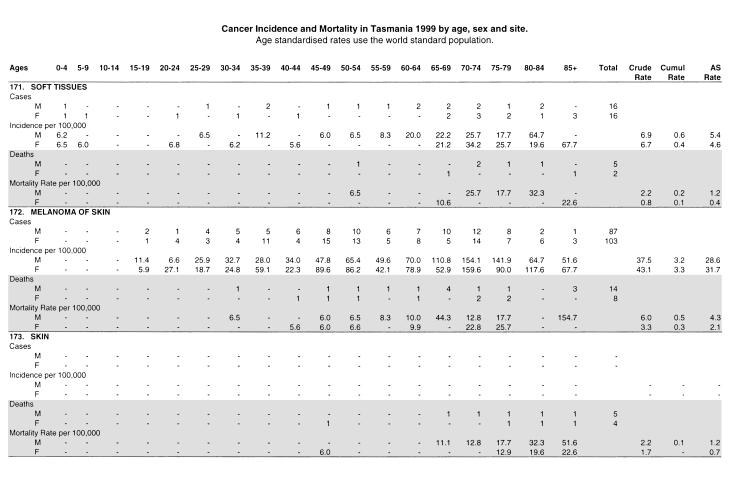
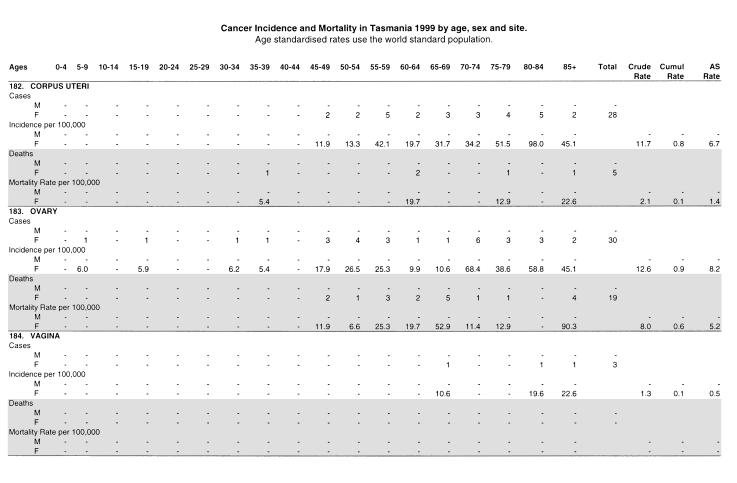
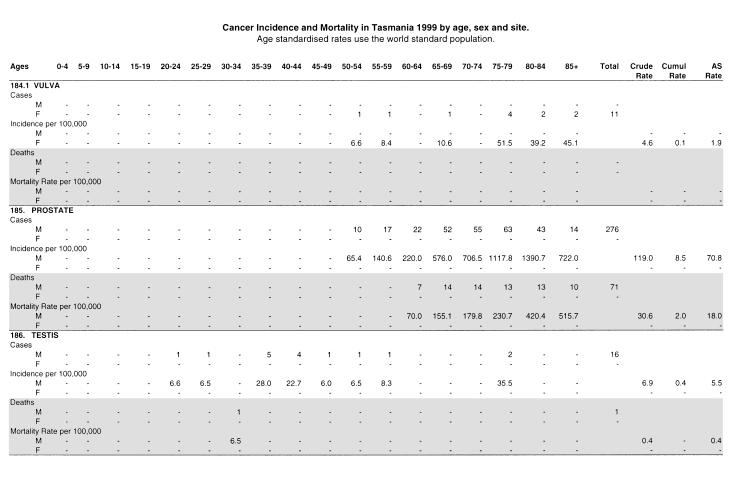
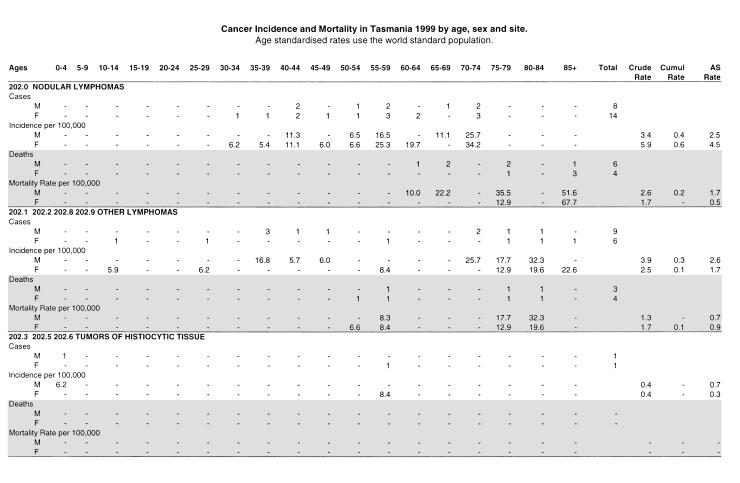
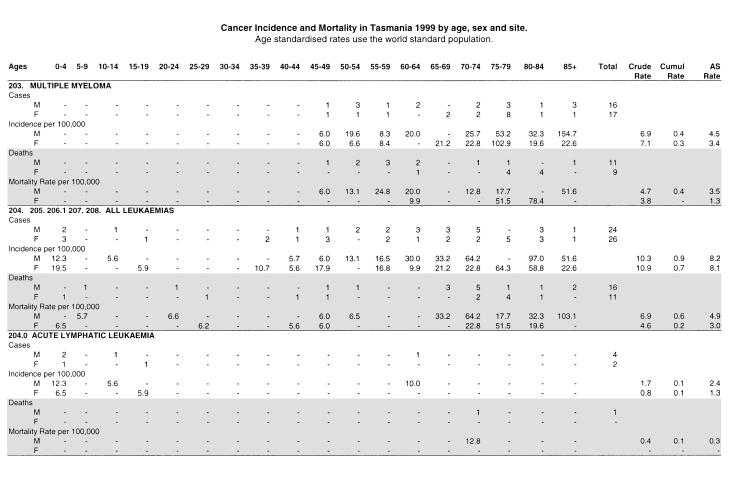
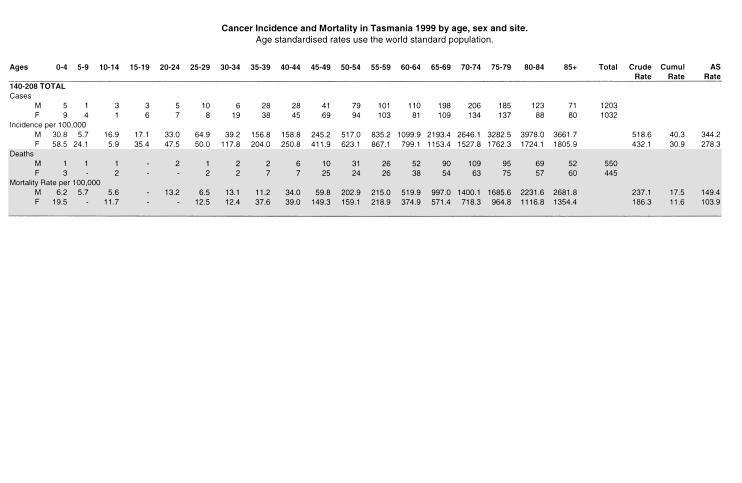
15 CANCER INCIDENCE AND MORTALITY TABLE 1999 Numbers of new cases and deaths Age-specific incidence and mortality rates per 100,000 Crude incidence and mortality rates per 100,000 (Crude Rate) Cumulative incidence and mortality rates (Cumul Rate) Age standardised incidence and mortality rates using the world standard population (AS Rate) 13
16 14
17 15
18 16
19 17
20 18
21 19
22 20
23 21
24 22
25 23
26 24
27 25
28 26
29 27
30 28
31 29
32 30
33 31
34 32
35 33
36 34
37 APPENDICES Appendix A: Appendix B: Appendix C: Appendix D: Appendix E: Appendix F: Cancer codes and specific coding practices Statistical methods and calculations Population data Indices of data quality Use of cancer registry data Cancer registry staff, volunteers and committee members Appendix G: Incidence summary and mortality summary,
38 Appendix A: CANCER CODES (ICD-9) AND SPECIFIC CODING PRACTICES Buccal Cavity and Pharynx: Lip 141. Tongue 142. Salivary Gland 143. Gum 144. Floor of Mouth 145. Other and Unspecified Parts of the Mouth 146. Oropharynx 147. Nasopharynx 148. Hypopharynx 149. Other and Ill-defined Sites within the Lip, Oral Cavity and Pharynx Genito-Urinary Organs: Cervix Uteri (invasive) 181. Placenta 182. Body of Uterus 183. Ovary and other Uterine Adnexa 184. Other and Unspecified Female Genital Organs 185. Prostate 186. Testis 187. Penis and Other Male Genital Organs 188. Bladder 189. Kidney and Other and Unspecified Urinary Organs Digestive Organs and Peritoneum: Oesophagus 151. Stomach 152. Small Intestine 153. Colon 154. Rectum, Rectosigmoid Junction and Anal Canal 155. Liver and Intrahepatic Bile Ducts specified as Primary 156. Gall Bladder and Extrahepatic Bile Ducts 157. Pancreas 158. Peritoneum and Retroperitoneal Tissue 159. Unspecified Digestive Organs Respiratory System: Nasal Cavities, Middle Ear and Accessory Sinuses 161. Larynx 162. Trachea, Bronchus and Lung 163. Pleura 164. Thymus, Heart and Mediastinum Bone, Connective Tissue, Skin and Breast: Other and Unspecified Sites: Eye 191. Brain 192. Cranial Nerves, Spinal Cord, Meninges and Other Unspecified Parts 193. Thyroid Gland 194. Other Endocrine Glands 195. Other and Ill-defined Sites 199. Unspecified Site Lymphatic and Hematopoietic Tissue: Diffuse Non-Hodgkin s Lymphoma 201. Hodgkin s Disease 202. Other Lymphomas 203. Multiple Myeloma and Immunoproliferative Neoplasms 204. Lymphoid Leukaemia 205. Myeloid Leukaemia 206. Monocytic Leukaemia 207. Erythroleukaemias and Other Specified Leukaemias 208. Unspecified Cell Leukaemias 170. Bone and Articular Cartilage 171. Connective and Other Soft Tissue 172. Skin Malignant Melanoma 173. Skin other than Melanoma 174. Female Breast 175. Male Breast 36
39 Comments on the use of ICD-9 code in this report 140. Lip: applies to squamous cell carcinomas arising from the mucosa, muco-epidermal junction or vermillion border Small intestine: includes sarcomas and carcinomas but lymphomas are coded to 200 or Liver: only those tumours proved by histological examination or special tests are included; others regarded as metastatic Peritoneum and Retroperitoneal tissue: on the advice of an authority on soft tissue tumours, primaries are being coded to Bronchus and Lung: includes only tumours considered to be primary Bone: includes only primary bone tumours Cutaneous Melanoma: invasive lesions only included Non-Melanoma Skin: only mortality rates are shown in this report Cervix Uteri: includes microinvasive lesions but not in-situ cancers Bladder: includes invasive tumours only Secondary Sites: all coded under 199 if primary site unknown Lymphosarcoma and Reticulosarcoma: only diffuse non-hodgkin s lymphomas are included under this code number Leukaemias: certain changes have been made to 2060, 2070 and 2072 to incorporate them in the Acute Myeloid (AML) 2050 FAB Classification (M1-M7). Please note that none of the 3 digit ICD-9 codes have been changed ( ). However, it must be pointed out that some of the 4-digit codes of ICD-9 have been expanded or condensed to concur with changes in pathology classifications and where numbers warrant this practice. As the International Agency for Research in Cancer (IARC) scientific publication Cancer in Five Continents is based on 3-digit codes, this modification does not affect international comparisons. 37
40 Appendix B: STATISTICAL METHODS AND CALCULATIONS The 1999 report contains numbers of new cases and deaths, and age specific, crude, cumulative, and age standardised incidence and mortality rates of Tasmanian residents diagnosed with cancer. They are based on registrations completed by 7 June Incidence Cancer incidence is defined as the number of new cases of cancer in a population during a specific period. The incidence data in this report relate to the number of primary cancers first diagnosed between January 1999 and December 1999 in persons who were residents of Tasmania at the time of diagnosis. Mortality The mortality data in this report relate to deaths from cancer, of people who were first diagnosed as having cancer while they were residents of Tasmania. In many instances, Tasmanian cancer patients who die elsewhere are notified to the Tasmanian cancer registry by other State or Territory cancer registries. Details of patients diagnosed interstate who die in Tasmania are forwarded to the relevant cancer registry. Deaths from other causes are also recorded so that survival rates can be calculated. Crude rates (CR) Age specific rates Age specific rates are calculated by dividing the number of cases occurring in each specified age group by the corresponding population in the same age group and are expressed as an annual rate per 100,000 population. Age standardised rates (ASR) Rates are adjusted for age to facilitate comparisons between populations that have different age structures, eg between youthful and aging communities. In this publication we use direct standardisation in which age specific rates are used to calculate the number of cases that would have occurred if the population had the same age distribution as the World Standard Population. This effectively removes the influence of age structure on the summary rate, which is described as the age standardised rate. The method may be used for both incidence and mortality calculations. Cumulative rates The cumulative rate is a directly standardised rate calculated by summing the age specific rate for each year of life prior to age 75. Cumulative risk to age 75 can be calculated from the cumulative rate. The crude incidence (rate) is calculated as the number of new cases of cancer divided by the population at risk in a specified time period. The crude mortality rate substitutes deaths for new cases in this calculation. Both are conventionally expressed as annual rates per 100,000 population. They are referred to as crude rates because there is no adjustment for age. The estimated Tasmanian population by age and sex for 1999 was supplied by the Australian Bureau of Statistics (ABS), Cat No
41 Appendix C: POPULATION DATA Table 2: Estimated Resident Population of Tasmania by Age Group as at 30 June Age Group Males Females Persons ,209 15,373 31, ,560 16,591 34, ,700 17,091 34, ,566 16,951 34, ,163 14,750 29, ,420 16,005 31, ,294 16,123 31, ,862 18,625 36, ,628 17,940 35, ,720 16,750 33, ,281 15,085 30, ,093 11,878 23, ,001 10,136 20, ,027 9,450 18, ,785 8,771 16, ,636 7,774 13, ,092 5,104 8, ,939 4,430 6,369 All ages 231, , ,803 Table 3: Age Distribution of World Standard Population 2 Age Group World , , , , , , , , , , , , , , , , All ages 100,000 The standard world population 3 approximates the proportional age distribution of the whole world. It is used widely for direct standardisation to enable comparisons between populations of differing age structure. 1 Demography: Tasmania Australian Bureau of Statistics 2000, p15. 2 Parkin D M, Whelan S, Ferlay J, Raymond L and Young J. Cancer Incidence in Five Continents Vol VII. IARC Scientific Publication No 143. Lyon: International Agency for Research on Cancer, 1997 (p 67). 3 Doll R, Payne P, Waterhouse J (eds). Cancer Incidence in Five Continents. A Technical Report. Berlin: Springer-Verlag (for UICC),
42 Appendix D: INDICES OF DATA QUALITY Indices of data quality Three indices of data quality are commonly used by Australian Cancer Registries: the mortality to incidence ratio (M/I%), histological verification percentage (HV%) and death certificate only (DCO). The Tasmanian Cancer Registry has calculated two of these indices (M/I% and HV%) and also determined morphological verification (MV%) and primary site unknown (PSU). The number of DCO cases 1 has not been formally calculated, as the Registry does not register cases on the basis of death certificate only. Each death certificate notification is actively followed up until the time and place of diagnosis are ascertained and the diagnosis verified. If the diagnostic details cannot be confirmed, the case is not registered. In 1999, approximately ten (0.5%) DCOs were unable to be verified and therefore were not registered. One way of assessing the completeness of cancer ascertainment is the M/I%. This measure is calculated by dividing the number of deaths attributed to a specific cancer in a defined population by the number of new cases of the same cancer registered during the same period in the same population. For cancers with a poor prognosis, the ratio will be close to 100%. If it exceeds 100% this may indicate that the cancer is being under-registered, but a more likely explanation for this result with uncommon cancers is that it is a result of random fluctuations in the annual number of new cases and deaths. HV% is an indicator of the quality of the data because it is the percentage of cases with histological verification. Histological verification of diagnosis shows that it has been possible to investigate a patient with such thoroughness that a portion of the suspected neoplasm has been removed for microscopic examination. 2 For 1999, 87% of all female and 85% of all male registered cases had a diagnosis on the basis of tissue examination. HV% included only the cancers that were diagnosed following tissue or needle biopsy and did not include diagnoses made on the basis of cytology examination of smears or aspirates (including haematological examinations). If we include all diagnoses based on exfoliative cytology and haematological examinations (for leukaemia) as well as diagnoses based on histological examination of a tissue specimen, then the percentage of all cancers with morphological verification 3 (MV%) in 1999 was 93%. The list below shows the number and percentage of cancer cases diagnosed by the various examination techniques in Some cases were diagnosed by more than one technique, and hence the total number of examinations exceeds the number of cases registered. Examination Technique Number Percent Histology 1, Radiology Cytology Imaging 1 0 Haematology 40 2 Clinical Other 21 1 The Registry calculated the percentage of all cancers that were classified as primary site unknown (PSU), because it is one of the quality indicators used for international comparisons. 4 PSU includes other and illdefined sites within the digestive organs and peritoneum, other and ill-defined sites within the respiratory system and intrathoracic organs and primary site unknown. In 1999, the percentage of all cases classified as PSU was 3.8% for males and 5.1% for females. 1 Those cases for which no other information than a death certificate mentioning cancer can be obtained. 2 Parkin D.M, Chen V.W, Ferlay J, Galceran J, Storm H.H and Whelan S. Comparability and Quality Control in Cancer Registration. IARC Technical Report No 19. Lyon: International Agency for Research on Cancer, 1994 (p 43). 3 Parkin D.M, Whelan S, Ferlay J, Raymond L and Young J. Cancer Incidence in Five Continents Vol VII. IARC Scientific Publication No 143. Lyon: International Agency for Research on Cancer, 1997 (p 50). 4 Parkin D.M, Chen V.W, Ferlay J, Galceran J, Storm H.H and Whelan S. Comparability and Quality Control in Cancer Registration. IARC Technical Report No 19. Lyon: International Agency for Research on Cancer, 1994 (p 51). 40
43 Table 4: Indices of Data Quality ICD-9 Site Incidence Mortality M/I% HV% MV% Males 140 Lip Head & Neck Oesophagus Stomach Colon Rectal Liver Gall Bladder Pancreas Lung Melanoma of Skin Prostate Testis Bladder Kidney Brain Thyroid Unspecified Site All Lymphomas Multiple Myeloma All Leukaemias All Cancers 1, Females 140 Lip Head & Neck Oesophagus Stomach Colon Rectal Liver Gall Bladder Pancreas Lung Melanoma of Skin Breast Cervix Uterus Ovary Vagina Bladder Kidney Brain Thyroid Unspecified Site All Lymphomas Multiple Myeloma All Leukaemias All Cancers 1, Note non-melanocytic skin cancers are not included in this table. 41
44 Appendix E: USE OF CANCER REGISTRY DATA Confidentiality of information Confidentiality of data is a requirement of the Public Health Act The Registry cannot release data identifying an individual unless authorised by the Director of Public Health. The relevant sections of this Act are described below. Disclosure of information relating to a notifiable disease Section 61: A person, unless authorised to do so under section 147, must not disclose any information in relation to: (a) Any notification relating to a notifiable disease; or (b) Any investigation or inquiry into a notifiable disease; or (c) The identity of any person to whom any notification, investigation or inquiry relates. Disclosure of information Section 147: A person must not disclose any information obtained for the purpose of this Act relating to a person except in accordance with any relevant guidelines and: (a) With the written consent of the person or parent or guardian of a child or person to whom the information relates; or (b) To a registered medical practitioner who is directly involved in the treatment of that person; or (c) To a person apparently in charge of any institution or facility which is involved in the diagnosis or treatment of that person; or (d) To a person authorised by the Director; or (e) For the purpose of notifying a notifiable disease; or (f) For the purpose of an epidemiological study or research authorised by the Director; or (g) For the purpose of legal proceedings arising out of this Act; or (h) For a purpose authorised or required by this Act or another Act; or (i) For the purposes of study or research approved by the Director. Requests for non-identifying data Non-identifying cancer data are available upon request. Data are usually released as incidence or mortality rates, or number of cases or deaths, for specific cancers, cancer morphologies, time periods or age groups. Data that can be compiled using existing reporting systems have a turnaround of approximately 48 hours. Data needing input from the biostatistician require more notice. Such data are provided to epidemiological and clinical researchers, the Department of Health and Human Services, students and the public. In addition to data requests, the Registry receives personal enquiries regarding cancer. When appropriate, these enquiries are referred to other agencies or health professionals. Requests for identifying data The release of named data is strictly controlled. Named data may be released only after approval of a formal application submitted to the Data Release Committee of the Tasmanian Cancer Registry and with subsequent approval by the Director of Public Health. Applications for research purposes need the approval of the researchers institutional ethics committee. Applicants are required to send a covering letter with the study protocol and copies of approvals from the ethics committees to the Director of the Tasmanian Cancer Registry. Published data Annual reports from the Registry provide data on cancer numbers and incidence and mortality. Additional information is provided on selected cancer sites. It should be recognised that active follow-up is necessary to complete registrations for 20% of cases each year, which results in a two-year interval from year of diagnosis to date of publication of incidence data. Considerable time is spent on matching, classifying and validating cancer cases notified to the Registry. In addition the Tasmanian Cancer Registry supplies data to the National Cancer Statistics Clearing House (NCSCH) and to the International Association of Cancer Registries (IACR). 42
45 Appendix F: CANCER REGISTRY STAFF, VOLUNTEERS AND COMMITTEE MEMBERS Cancer Registry Staff and Volunteers, 2001 Professor T Dwyer Medical Director (to April 2001) Dr A Venn Acting Director (September 2000 February 2001) Director (from April 2001) Mrs S Pavlides Database Manager (November 2000 February 2001) Registrar (from March 2001) Mrs V Webb Mrs K Jackman Mrs S Browne Mrs P Whelan Mrs J Clifford Mrs A Button Dr L Blizzard Miss J Fryer Mrs D Shugg Mrs P Vallance Administrative Officer Administrative Officer Clerical Assistant Volunteer Volunteer Volunteer Biostatistician, Menzies Centre Biostatistician, Menzies Centre Honorary Research Associate Librarian Members of the Advisory Committee, 2001 Dr A Venn Mrs S Pavlides Dr M Jacobs Ms V Gardner Professor P Stanton Dr R Young Mrs M Ramsden Menzies Centre for Population Health Research Tasmanian Cancer Registry Department of Health and Human Services Department of Health and Human Services School of Medicine, Department of Surgery School of Medicine, Department of Clinical Sciences Cancer Council of Tasmania Members of the Data Release Committee, 2001 Dr R Kimber Dr M Baikie Dr S Gauden Dr R Kelsall Royal Hobart Hospital Royal Hobart Hospital (retired) WP Holman Clinic Forensic Pathology 43
46 Appendix G: INCIDENCE SUMMARY, 1999 Table 5: Incidence Summary, 1999 ICD-9 SITE MALES FEMALES TOTAL *N CR ASR N CR ASR N 140 Lip Tongue Salivary Gland Gum Floor of Mouth Other Mouth Oropharynx Nasopharynx Hypopharynx Other Pharynx Oesophagus Stomach Small Intestine Colon Rectum Liver Gall Bladder Pancreas Nasal Cavities Larynx Lung Pleura Thymus Bone Soft Tissues Melanoma of Skin Skin Incidence of non-melanocytic skin cancer is not recorded Breast Cervix Uteri Placenta Corpus Uteri Ovary Vagina Vulva Prostate Testis Penis Bladder Kidney Eye Brain Other CNS Thyroid Other Endocrine Unspecified Site All Lymphomas Histiocytic Tissue Multiple Myeloma All Leukaemias Total New Cases * N = Number CR = Crude Rate ASR = Age Standardised Rate 44
47 MORTALITY SUMMARY, 1999 Table 6: Mortality Summary, 1999 ICD-9 SITE MALES FEMALES TOTAL *N CR ASR N CR ASR N 140 Lip Tongue Salivary Gland Gum Floor of Mouth Other Mouth Oropharynx Nasopharynx Hypopharynx Other Pharynx Oesophagus Stomach Small Intestine Colon Rectum Liver Gall Bladder Pancreas Nasal Cavities Larynx Lung Pleura Thymus Bone Soft Tissues Melanoma of Skin Skin Breast Cervix Uteri Placenta Corpus Uteri Ovary Vagina Vulva Prostate Testis Penis Bladder Kidney Eye Brain Other CNS Thyroid Other Endocrine Unspecified Site All Lymphomas Histiocytic Tissue Multiple Myeloma All Leukaemias Total Deaths * N = Number CR = Crude Rate ASR = Age Standardised Rate 45
48
CANCER IN TASMANIA INCIDENCE AND MORTALITY 1996
 CANCER IN TASMANIA INCIDENCE AND MORTALITY 1996 CANCER IN TASMANIA INCIDENCE AND MORTALITY 1996 Menzies Centre For Population Health Research Editors: Dace Shugg, Terence Dwyer and Leigh Blizzard Publication
CANCER IN TASMANIA INCIDENCE AND MORTALITY 1996 CANCER IN TASMANIA INCIDENCE AND MORTALITY 1996 Menzies Centre For Population Health Research Editors: Dace Shugg, Terence Dwyer and Leigh Blizzard Publication
Cancer in Estonia 2014
 Cancer in Estonia 2014 Estonian Cancer Registry (ECR) is a population-based registry that collects data on all cancer cases in Estonia. More information about ECR is available at the webpage of National
Cancer in Estonia 2014 Estonian Cancer Registry (ECR) is a population-based registry that collects data on all cancer cases in Estonia. More information about ECR is available at the webpage of National
CANCER IN TASMANIA INCIDENCE AND MORTALITY 1995
 CANCER IN TASMANIA INCIDENCE AND MORTALITY 1995 ACKNOWLEDGEMENTS The Department of Community and Health Services in Tasmania is acknowledged for financial support to the Registry. The work of collecting
CANCER IN TASMANIA INCIDENCE AND MORTALITY 1995 ACKNOWLEDGEMENTS The Department of Community and Health Services in Tasmania is acknowledged for financial support to the Registry. The work of collecting
Cancer Association of South Africa (CANSA)
") Cancer Association of South Africa (CANSA) Fact Sheet on ICD-10 Coding of Neoplasms Introduction The International Statistical Classification of Diseases and Related Health Problems, 10 th Revision (ICD-10)
Cancer Association of South Africa (CANSA) Fact Sheet on ICD-10 Coding of Neoplasms Introduction The International Statistical Classification of Diseases and Related Health Problems, 10 th Revision (ICD-10)
Cancer survival in Hong Kong SAR, China,
 Chapter 5 Cancer survival in Hong Kong SAR, China, 1996 2001 Law SC and Mang OW Abstract The Hong Kong cancer registry was established in 1963, and cancer registration is done by passive and active methods.
Chapter 5 Cancer survival in Hong Kong SAR, China, 1996 2001 Law SC and Mang OW Abstract The Hong Kong cancer registry was established in 1963, and cancer registration is done by passive and active methods.
Cancer survival in Shanghai, China,
 Cancer survival in Shanghai, China, 1992 1995 Xiang YB, Jin F and Gao YT Abstract The Shanghai cancer registry, established in 1963, is the oldest one in mainland China; cancer registration is entirely
Cancer survival in Shanghai, China, 1992 1995 Xiang YB, Jin F and Gao YT Abstract The Shanghai cancer registry, established in 1963, is the oldest one in mainland China; cancer registration is entirely
Cancer survival in Seoul, Republic of Korea,
 Cancer survival in Seoul, Republic of Korea, 1993 1997 Ahn YO and Shin MH Abstract The Seoul cancer registry was established in 1991. Cancer is a notifiable disease, and registration of cases is done by
Cancer survival in Seoul, Republic of Korea, 1993 1997 Ahn YO and Shin MH Abstract The Seoul cancer registry was established in 1991. Cancer is a notifiable disease, and registration of cases is done by
ANNUAL CANCER REGISTRY REPORT-2005
 ANNUAL CANCER REGISTRY REPORT-25 CANCER STATISTICS Distribution of neoplasms Of a total of 3,115 new neoplasms diagnosed or treated at the Hospital from January 25 to December, 25, 1,473 were seen in males
ANNUAL CANCER REGISTRY REPORT-25 CANCER STATISTICS Distribution of neoplasms Of a total of 3,115 new neoplasms diagnosed or treated at the Hospital from January 25 to December, 25, 1,473 were seen in males
Cancer survival in Busan, Republic of Korea,
 Cancer survival in Busan, Republic of Korea, 1996 2001 Shin HR, Lee DH, Lee SY, Lee JT, Park HK, Rha SH, Whang IK, Jung KW, Won YJ and Kong HJ Abstract The Busan cancer registry was established in 1996;
Cancer survival in Busan, Republic of Korea, 1996 2001 Shin HR, Lee DH, Lee SY, Lee JT, Park HK, Rha SH, Whang IK, Jung KW, Won YJ and Kong HJ Abstract The Busan cancer registry was established in 1996;
Cancer in the Northern Territory :
 Cancer in the Northern Territory 1991 21: Incidence, mortality and survival Xiaohua Zhang John Condon Karen Dempsey Lindy Garling Acknowledgements The authors are grateful to the many people, who have
Cancer in the Northern Territory 1991 21: Incidence, mortality and survival Xiaohua Zhang John Condon Karen Dempsey Lindy Garling Acknowledgements The authors are grateful to the many people, who have
WLH Tumor Frequencies between cohort enrollment and 31-Dec Below the Women Lifestyle and Health tumor frequencies are tabulated according to:
 DESCRIPTION Below the Women Lifestyle and Health tumor frequencies are tabulated according to: Benign =171 (Cervix uteri) treated as not recorded =191 (non-melanoma skin cancer) treated as not recorded
DESCRIPTION Below the Women Lifestyle and Health tumor frequencies are tabulated according to: Benign =171 (Cervix uteri) treated as not recorded =191 (non-melanoma skin cancer) treated as not recorded
APPENDIX ONE: ICD CODES
 APPENDIX ONE: ICD CODES ICD-10-AM ICD-9-CM Malignant neoplasms C00 C97 140 208, 238.6, 273.3 Lip, oral cavity and pharynx C00 C14 140 149 Digestive organs C15 C26 150 157, 159 Oesophagus 4 C15 150 excluding
APPENDIX ONE: ICD CODES ICD-10-AM ICD-9-CM Malignant neoplasms C00 C97 140 208, 238.6, 273.3 Lip, oral cavity and pharynx C00 C14 140 149 Digestive organs C15 C26 150 157, 159 Oesophagus 4 C15 150 excluding
Cancer in Central and South America BOLIVIA
 Cancer in Central and South America BOLIVIA This country profile for the Cancer in Central and South America project provides, for each participating cancer registry tables and graphics showing numbers
Cancer in Central and South America BOLIVIA This country profile for the Cancer in Central and South America project provides, for each participating cancer registry tables and graphics showing numbers
WLH Tumor Frequencies between cohort enrollment and 31-Dec Below the Women Lifestyle and Health tumor frequencies are tabulated according to:
 WLH Tumor Frequencies between cohort enrollment and 31-Dec 2012 DESCRIPTION Below the Women Lifestyle and Health tumor frequencies are tabulated according to: Benign =171 (Cervix uteri) treated as not
WLH Tumor Frequencies between cohort enrollment and 31-Dec 2012 DESCRIPTION Below the Women Lifestyle and Health tumor frequencies are tabulated according to: Benign =171 (Cervix uteri) treated as not
Annual Report. Cape Cod Hospital and Falmouth Hospital Regional Cancer Network Expert physicians. Quality hospitals. Superior care.
 Annual Report Cape Cod Hospital and Falmouth Hospital Regional Cancer Network 2013 Expert physicians. Quality hospitals. Superior care. Cape Cod Hospital s Davenport- Mugar Hematology/Oncology Center and
Annual Report Cape Cod Hospital and Falmouth Hospital Regional Cancer Network 2013 Expert physicians. Quality hospitals. Superior care. Cape Cod Hospital s Davenport- Mugar Hematology/Oncology Center and
Cancer survival and prevalence in Tasmania
 Cancer survival and prevalence in Tasmania 1978-2008 Cancer survival and prevalence in Tasmania 1978-2008 Tasmanian Cancer Registry University of Tasmania Menzies Research Institute Tasmania 17 Liverpool
Cancer survival and prevalence in Tasmania 1978-2008 Cancer survival and prevalence in Tasmania 1978-2008 Tasmanian Cancer Registry University of Tasmania Menzies Research Institute Tasmania 17 Liverpool
2011 to 2015 New Cancer Incidence Truman Medical Center - Hospital Hill
 Number of New Cancers Truman Medical Center Hospital Hill Cancer Registry 2015 Statistical Summary Incidence In 2015, Truman Medical Center diagnosed and/or treated 406 new cancer cases. Four patients
Number of New Cancers Truman Medical Center Hospital Hill Cancer Registry 2015 Statistical Summary Incidence In 2015, Truman Medical Center diagnosed and/or treated 406 new cancer cases. Four patients
Truman Medical Center-Hospital Hill Cancer Registry 2014 Statistical Summary Incidence
 Truman Medical Center-Hospital Hill Cancer Registry 2014 Statistical Summary Incidence In 2014, there were 452 new cancer cases diagnosed and or treated at Truman Medical Center- Hospital Hill and an additional
Truman Medical Center-Hospital Hill Cancer Registry 2014 Statistical Summary Incidence In 2014, there were 452 new cancer cases diagnosed and or treated at Truman Medical Center- Hospital Hill and an additional
Overview of 2010 Hong Kong Cancer Statistics
 Overview of 2010 Hong Kong Cancer Statistics Cancer Registration in Hong Kong The Hong Kong Cancer Registry has since the 1960s been providing population-based cancer data for epidemiological research
Overview of 2010 Hong Kong Cancer Statistics Cancer Registration in Hong Kong The Hong Kong Cancer Registry has since the 1960s been providing population-based cancer data for epidemiological research
CHAPTER 10 CANCER REPORT. Jeremy Chapman. and. Angela Webster
 CHAPTER 10 CANCER REPORT Jeremy Chapman and Angela Webster CANCER REPORT ANZDATA Registry 2004 Report This report summarises the cancer (excluding nonmelanocytic skin cancer) experience of patients treated
CHAPTER 10 CANCER REPORT Jeremy Chapman and Angela Webster CANCER REPORT ANZDATA Registry 2004 Report This report summarises the cancer (excluding nonmelanocytic skin cancer) experience of patients treated
S2 File. Clinical Classifications Software (CCS). The CCS is a
. The CCS is a") S2 File. Clinical Classifications Software (CCS). The CCS is a diagnosis categorization scheme based on the ICD-9-CM that aggregates all diagnosis codes into 262 mutually exclusive, clinically homogeneous
S2 File. Clinical Classifications Software (CCS). The CCS is a diagnosis categorization scheme based on the ICD-9-CM that aggregates all diagnosis codes into 262 mutually exclusive, clinically homogeneous
Florida Cancer Data System STAT File Documentation Version 2019
 Florida Cancer Data System STAT File Documentation Version 2019 Field Description NAACCR Item Recoded Patient ID Number 20 Addr at DX - State 80 X County at DX 90 Addr at DX Country 102 X Marital Status
Florida Cancer Data System STAT File Documentation Version 2019 Field Description NAACCR Item Recoded Patient ID Number 20 Addr at DX - State 80 X County at DX 90 Addr at DX Country 102 X Marital Status
Information Services Division NHS National Services Scotland
 Cancer in Scotland October 2012 First published in June 2004, revised with each National Statistics publication Next due for revision April 2013 Information Services Division NHS National Services Scotland
Cancer in Scotland October 2012 First published in June 2004, revised with each National Statistics publication Next due for revision April 2013 Information Services Division NHS National Services Scotland
Cancer in Utah: An Overview of Cancer Incidence and Mortality from
 Cancer in Utah: An Overview of Cancer Incidence and Mortality from 1973-2010 A publication of the Utah Cancer Registry January 2014 Prepared by: C. Janna Harrell, MS Senior Research Analyst Kimberly A.
Cancer in Utah: An Overview of Cancer Incidence and Mortality from 1973-2010 A publication of the Utah Cancer Registry January 2014 Prepared by: C. Janna Harrell, MS Senior Research Analyst Kimberly A.
ALL CANCER (EXCLUDING NMSC)
") ALL CANCER (EXCLUDING NMSC) AVERAGE NUMBER OF CASES PER YEAR (2012-2016) AVERAGE NUMBER OF DEATHS PER YEAR (2012-2016) Male Female Both sexes Male Female Both sexes 4,607 4,632 9,240 1 2,238 2,036 4,274
ALL CANCER (EXCLUDING NMSC) AVERAGE NUMBER OF CASES PER YEAR (2012-2016) AVERAGE NUMBER OF DEATHS PER YEAR (2012-2016) Male Female Both sexes Male Female Both sexes 4,607 4,632 9,240 1 2,238 2,036 4,274
Chapter II: Overview
 : Overview Chapter II: Overview This chapter provides an overview of the status of cancer in Minnesota, using cases reported to the Minnesota Cancer Surveillance System (MCSS) and deaths reported to the
: Overview Chapter II: Overview This chapter provides an overview of the status of cancer in Minnesota, using cases reported to the Minnesota Cancer Surveillance System (MCSS) and deaths reported to the
Cancer in Ireland : Annual Report of the National Cancer Registry
 Cancer in Ireland 1994-213: Annual Report of the National Cancer Registry 215 Page 3 ABBREVIATIONS 95% CI 95% confidence interval APC Annual percentage change ASR Age-standardised rate (European standard
Cancer in Ireland 1994-213: Annual Report of the National Cancer Registry 215 Page 3 ABBREVIATIONS 95% CI 95% confidence interval APC Annual percentage change ASR Age-standardised rate (European standard
Information Services Division NHS National Services Scotland
 Cancer in Scotland April 2013 First published in June 2004, revised with each National Statistics publication Next due for revision October 2013 Information Services Division NHS National Services Scotland
Cancer in Scotland April 2013 First published in June 2004, revised with each National Statistics publication Next due for revision October 2013 Information Services Division NHS National Services Scotland
ALL CANCER (EXCLUDING NMSC)
") ALL CANCER (EXCLUDING NMSC) AVERAGE NUMBER OF CASES PER YEAR (2011-2015) AVERAGE NUMBER OF DEATHS PER YEAR (2011-2015) Male Female Both sexes Male Female Both sexes 4,557 4,516 9,073 1 2,196 1,984 4,180
ALL CANCER (EXCLUDING NMSC) AVERAGE NUMBER OF CASES PER YEAR (2011-2015) AVERAGE NUMBER OF DEATHS PER YEAR (2011-2015) Male Female Both sexes Male Female Both sexes 4,557 4,516 9,073 1 2,196 1,984 4,180
Cancer survival in Chennai (Madras), India,
, India,") Cancer survival in Chennai (Madras), India, 199 1999 Swaminathan R, Rama R, Nalini S and Shanta V Abstract The Madras metropolitan tumour registry was established in 1981, and registration of incident
Cancer survival in Chennai (Madras), India, 199 1999 Swaminathan R, Rama R, Nalini S and Shanta V Abstract The Madras metropolitan tumour registry was established in 1981, and registration of incident
Overview of 2009 Hong Kong Cancer Statistics
 Overview of 2009 Hong Kong Cancer Statistics Cancer Registration in Hong Kong The Hong Kong Cancer Registry has since 1963 been providing population-based cancer data for epidemiological research and healthcare
Overview of 2009 Hong Kong Cancer Statistics Cancer Registration in Hong Kong The Hong Kong Cancer Registry has since 1963 been providing population-based cancer data for epidemiological research and healthcare
National Cancer Patient Experience Survey 2016 Technical Documentation July 2017
 National Cancer Patient Experience Survey 2016 Technical Documentation July 2017 1 Contents 1. Introduction 2. Scoring 3. Significance Tests (for national data) 4. Case-mix Adjustment (for local data)
National Cancer Patient Experience Survey 2016 Technical Documentation July 2017 1 Contents 1. Introduction 2. Scoring 3. Significance Tests (for national data) 4. Case-mix Adjustment (for local data)
2016 Cancer Registry Annual Report
 2016 Cancer Registry Annual Report Cancer Committee Chairman s Report The Cancer Committee at Cancer Treatment Centers of America (CTCA) at Eastern Regional Medical Center (Eastern), established in 2006,
2016 Cancer Registry Annual Report Cancer Committee Chairman s Report The Cancer Committee at Cancer Treatment Centers of America (CTCA) at Eastern Regional Medical Center (Eastern), established in 2006,
Trends in Cancer Survival in NSW 1980 to 1996
 Trends in Cancer Survival in NSW 19 to 1996 Xue Q Yu Dianne O Connell Bruce Armstrong Robert Gibberd Cancer Epidemiology Research Unit Cancer Research and Registers Division The Cancer Council NSW August
Trends in Cancer Survival in NSW 19 to 1996 Xue Q Yu Dianne O Connell Bruce Armstrong Robert Gibberd Cancer Epidemiology Research Unit Cancer Research and Registers Division The Cancer Council NSW August
A Time- and Resource-Efficient Method for Annually Auditing All Reporting Hospitals in Your State: the Inpatient & Outpatient Hospital Discharge Files
 A Time- and Resource-Efficient Method for Annually Auditing All Reporting Hospitals in Your State: the Inpatient & Outpatient Hospital Discharge Files By Dr. Martin A. Whiteside Director, Office of Cancer
A Time- and Resource-Efficient Method for Annually Auditing All Reporting Hospitals in Your State: the Inpatient & Outpatient Hospital Discharge Files By Dr. Martin A. Whiteside Director, Office of Cancer
Overview of 2013 Hong Kong Cancer Statistics
 Overview of 2013 Hong Kong Cancer Statistics Cancer Registration in Hong Kong The Hong Kong Cancer Registry (HKCaR) is a population-based cancer registry, collecting the basic demographic data, information
Overview of 2013 Hong Kong Cancer Statistics Cancer Registration in Hong Kong The Hong Kong Cancer Registry (HKCaR) is a population-based cancer registry, collecting the basic demographic data, information
155.2 Malignant neoplasm of liver not specified as primary or secondary. C22.9 Malignant neoplasm of liver, not specified as primary or secondary
 ICD-9 TO ICD-10 Reference ICD-9 150.9 Malignant neoplasm of esophagus unspecified site C15.9 Malignant neoplasm of esophagus, unspecified 151.9 Malignant neoplasm of stomach unspecified site C16.9 Malignant
ICD-9 TO ICD-10 Reference ICD-9 150.9 Malignant neoplasm of esophagus unspecified site C15.9 Malignant neoplasm of esophagus, unspecified 151.9 Malignant neoplasm of stomach unspecified site C16.9 Malignant
Information Services Division NHS National Services Scotland
 Cancer in Scotland April 2017 First published in June 2004, revised with each National Statistics publication Next due for revision October 2017 Information Services Division NHS National Services Scotland
Cancer in Scotland April 2017 First published in June 2004, revised with each National Statistics publication Next due for revision October 2017 Information Services Division NHS National Services Scotland
Republican Research and Practical Center for Radiation Medicine and Human Ecology. Ilya Veyalkin Head of Laboratory of Epidemiology Gomel, Belarus
 Republican Research and Practical Center for Radiation Medicine and Human Ecology Ilya Veyalkin Head of Laboratory of Epidemiology Gomel, Belarus The contaminated area in the Republic of Belarus consisted
Republican Research and Practical Center for Radiation Medicine and Human Ecology Ilya Veyalkin Head of Laboratory of Epidemiology Gomel, Belarus The contaminated area in the Republic of Belarus consisted
Cancer in Norway Cancer incidence, mortality, survival and prevalence in Norway
 Cancer in Norway 7 Cancer incidence, mortality, survival and prevalence in Norway Special issue: Long-term cancer survival: patterns and trends in Norway 96-7 Cancer in Norway 7 Editor-in-chief: Freddie
Cancer in Norway 7 Cancer incidence, mortality, survival and prevalence in Norway Special issue: Long-term cancer survival: patterns and trends in Norway 96-7 Cancer in Norway 7 Editor-in-chief: Freddie
Cancer in Norway Cancer incidence, mortality, survival and prevalence in Norway
 Cancer in Norway 2007 Cancer incidence, mortality, survival and prevalence in Norway Special issue: Long-term cancer survival: patterns and trends in Norway 1965-2007 Cancer in Norway 2007 Editor-in-chief:
Cancer in Norway 2007 Cancer incidence, mortality, survival and prevalence in Norway Special issue: Long-term cancer survival: patterns and trends in Norway 1965-2007 Cancer in Norway 2007 Editor-in-chief:
Overview of Hong Kong Cancer Statistics of 2015
 Overview of Hong Kong Cancer Statistics of 2015 This report summarizes the key cancer statistics of Hong Kong for the year of 2015, which is now available on the website of Hong Kong Cancer Registry. Cancer
Overview of Hong Kong Cancer Statistics of 2015 This report summarizes the key cancer statistics of Hong Kong for the year of 2015, which is now available on the website of Hong Kong Cancer Registry. Cancer
Hazelinks - Cancer incidence analysis (First data extraction)
") Hazelinks - Cancer incidence analysis (First data extraction) Authors Prof Malcolm Sim Ms Christina Dimitriadis Dr Caroline Gao Mr Anthony Del Monaco 1 1 Contents Abbreviations... 3 Executive Summary...
Hazelinks - Cancer incidence analysis (First data extraction) Authors Prof Malcolm Sim Ms Christina Dimitriadis Dr Caroline Gao Mr Anthony Del Monaco 1 1 Contents Abbreviations... 3 Executive Summary...
Research Article Cancer Incidence in Egypt: Results of the National Population-Based Cancer Registry Program
 Hindawi Publishing Corporation Journal of Cancer Epidemiology Volume 2014, Article ID 437971, 18 pages http://dx.doi.org/10.1155/2014/437971 Research Article Cancer Incidence in Egypt: Results of the National
Hindawi Publishing Corporation Journal of Cancer Epidemiology Volume 2014, Article ID 437971, 18 pages http://dx.doi.org/10.1155/2014/437971 Research Article Cancer Incidence in Egypt: Results of the National
*
 Introduction Cancer is complex, can have many possible causes, and is increasingly common. For the U.S. population, 1 in 2 males and 1 in 3 females is at risk of developing cancer in their lifetime. The
Introduction Cancer is complex, can have many possible causes, and is increasingly common. For the U.S. population, 1 in 2 males and 1 in 3 females is at risk of developing cancer in their lifetime. The
Chapter 1 MAGNITUDE AND LEADING SITES OF CANCER
 Chapter 1 MAGNITUDE AND LEADING SITES OF CANCER Table 1.1 gives the total number of cancers diagnosed at five different hospital based cancer registries (HBCRs), over the period of two years from 1st January
Chapter 1 MAGNITUDE AND LEADING SITES OF CANCER Table 1.1 gives the total number of cancers diagnosed at five different hospital based cancer registries (HBCRs), over the period of two years from 1st January
2012 Cancer Report 2011 Registry Data
 2012 Cancer Report 2011 Registry Data Contents Goals and Objectives 1 2012 Cancer Committee Members 2 Total Cancer Cases 1981-2011 3 Cancer Registry Frequency Report 1981-2011 4-5 Cancer Registry Frequency
2012 Cancer Report 2011 Registry Data Contents Goals and Objectives 1 2012 Cancer Committee Members 2 Total Cancer Cases 1981-2011 3 Cancer Registry Frequency Report 1981-2011 4-5 Cancer Registry Frequency
Cancer survival in Bhopal, India,
 Chapter 13 Cancer survival in Bhopal, India, 1991 1995 Dikshit R, Kanhere S and Surange S Abstract The Bhopal population-based cancer registry was established in 1986 under the national cancer registry
Chapter 13 Cancer survival in Bhopal, India, 1991 1995 Dikshit R, Kanhere S and Surange S Abstract The Bhopal population-based cancer registry was established in 1986 under the national cancer registry
Cancer survival in Harare, Zimbabwe,
 Chapter 31 Cancer survival in Harare, Zimbabwe, 1993 1997 Chokunonga E, Borok MZ, Chirenje ZM, Nyabakau AM and Parkin DM Abstract The Zimbabwe national cancer registry was established in 1985 as a population-based
Chapter 31 Cancer survival in Harare, Zimbabwe, 1993 1997 Chokunonga E, Borok MZ, Chirenje ZM, Nyabakau AM and Parkin DM Abstract The Zimbabwe national cancer registry was established in 1985 as a population-based
American Cancer Society Estimated Cancer Deaths by Sex and Age (years), 2013
, 2013") American Cancer Society Estimated Cancer Deaths by Sex and Age (years), 2013 All ages Younger than 45 45 and Older Younger than 65 65 and Older All sites, men 306,920 9,370 297,550 95,980 210,940 All sites,
American Cancer Society Estimated Cancer Deaths by Sex and Age (years), 2013 All ages Younger than 45 45 and Older Younger than 65 65 and Older All sites, men 306,920 9,370 297,550 95,980 210,940 All sites,
Cancer in Colorado Incidence, Mortality, and Survival
 Cancer in Colorado 1998-2003 Incidence, Mortality, and Survival Jack L. Finch, M.S. Statistical Analyst III Kieu O. Vu, M.S.P.H. Statistical Analyst II 2007 Colorado Central Cancer Registry Randi K. Rycroft,
Cancer in Colorado 1998-2003 Incidence, Mortality, and Survival Jack L. Finch, M.S. Statistical Analyst III Kieu O. Vu, M.S.P.H. Statistical Analyst II 2007 Colorado Central Cancer Registry Randi K. Rycroft,
Cancer in Ireland with estimates for
 Cancer in Ireland 1994-2015 with estimates for 2015-2017: Annual Report of the National Cancer Registry 2017 Page ABBREVIATIONS 95% CI 95% confidence interval APC Annual percentage change ASR Age-standardised
Cancer in Ireland 1994-2015 with estimates for 2015-2017: Annual Report of the National Cancer Registry 2017 Page ABBREVIATIONS 95% CI 95% confidence interval APC Annual percentage change ASR Age-standardised
Annual report on status of cancer in China, 2010
 Original Article Annual report on status of cancer in China, 2010 Wanqing Chen, Rongshou Zheng, Siwei Zhang, Ping Zhao, Hongmei Zeng, Xiaonong Zou, Jie He National Office for Cancer Prevention and Control,
Original Article Annual report on status of cancer in China, 2010 Wanqing Chen, Rongshou Zheng, Siwei Zhang, Ping Zhao, Hongmei Zeng, Xiaonong Zou, Jie He National Office for Cancer Prevention and Control,
LANDMARK MEDICAL CENTER CANCER PROGRAM YEAR IN REVIEW 2013
 LANDMARK MEDICAL CENTER CANCER PROGRAM YEAR IN REVIEW 2013 Landmark Medical Center offers a comprehensive cancer care services to our patients. LMC Cancer program is committed to ensure that patients receive
LANDMARK MEDICAL CENTER CANCER PROGRAM YEAR IN REVIEW 2013 Landmark Medical Center offers a comprehensive cancer care services to our patients. LMC Cancer program is committed to ensure that patients receive
Cancer in Ireland : Annual Report of the National Cancer Registry
 Cancer in Ireland 1-: Annual Report of the National Cancer Registry ABBREVIATIONS % CI % confidence interval APC Annual percentage change ASR Age-standardised rate (European standard population) CNS Central
Cancer in Ireland 1-: Annual Report of the National Cancer Registry ABBREVIATIONS % CI % confidence interval APC Annual percentage change ASR Age-standardised rate (European standard population) CNS Central
incidence rate x 100,000/year
 Tier R=rare C=common Cancer Entity European crude and age adjusted incidence by cancer, years of diagnosis 2000 and 2007 Analisys based on 83 population-based cancer registries * applying the European
Tier R=rare C=common Cancer Entity European crude and age adjusted incidence by cancer, years of diagnosis 2000 and 2007 Analisys based on 83 population-based cancer registries * applying the European
Cancer survival in Khon Kaen, Thailand,
 Cancer survival in Khon Kaen, Thailand, 1993 1997 Suwanrungruang K, Vatanasapt P, Kamsa-Ard S, Sriamporn S and Wiangnon S Abstract The Khon Kaen cancer registry was established in 1984 as a hospital-based
Cancer survival in Khon Kaen, Thailand, 1993 1997 Suwanrungruang K, Vatanasapt P, Kamsa-Ard S, Sriamporn S and Wiangnon S Abstract The Khon Kaen cancer registry was established in 1984 as a hospital-based
Cancer Incidence and Mortality: District Cancer Registry, Trivandrum, South India
 DOI:10.22034/APJCP.2017.18.6.1485 RESEARCH ARTICLE Cancer Incidence and Mortality: District Cancer Registry, Trivandrum, South India Aleyamma Mathew 1 *, Preethi Sara George 1, Kalavathy MC 1, Padmakumari
DOI:10.22034/APJCP.2017.18.6.1485 RESEARCH ARTICLE Cancer Incidence and Mortality: District Cancer Registry, Trivandrum, South India Aleyamma Mathew 1 *, Preethi Sara George 1, Kalavathy MC 1, Padmakumari
APPENDIX A: CANCER REGISTRATION IN TASMANIA
 APPENDIX A: CANCER REGISTRATION IN TASMANIA ABOUT THE TASMANIAN CANCER REGISTRY The Tasmanian Cancer Registry was established in 1977 as a population-based registry covering the whole of Tasmania. The
APPENDIX A: CANCER REGISTRATION IN TASMANIA ABOUT THE TASMANIAN CANCER REGISTRY The Tasmanian Cancer Registry was established in 1977 as a population-based registry covering the whole of Tasmania. The
Nationwide Cancer Incidence in Korea, 1999~2001; First Result Using the National Cancer Incidence Database
 Cancer Res Treat. 2005;37(6):325-331 Nationwide Cancer Incidence in Korea, 1999~2001; First Result Using the National Cancer Incidence Database Hai-Rim Shin, M.D. 1, Young-Joo Won, M.P.H. 1, Kyu-Won Jung,
Cancer Res Treat. 2005;37(6):325-331 Nationwide Cancer Incidence in Korea, 1999~2001; First Result Using the National Cancer Incidence Database Hai-Rim Shin, M.D. 1, Young-Joo Won, M.P.H. 1, Kyu-Won Jung,
Macmillan-NICR Partnership: GP Federation Cancer Profiles (with Prevalence )
") Macmillan-NICR Partnership: GP Federation Cancer Profiles 2011-2015 (with Prevalence 1993-2015) 1 C a n c e r S t a t i s t i c s b y G P F e d e r a t i o n a r e a : 2 0 1 1-2015 Table of Contents Introduction...
Macmillan-NICR Partnership: GP Federation Cancer Profiles 2011-2015 (with Prevalence 1993-2015) 1 C a n c e r S t a t i s t i c s b y G P F e d e r a t i o n a r e a : 2 0 1 1-2015 Table of Contents Introduction...
2. Occupancy rate of beds in the hospital: Occupancy rate of at least 60%
 Appendix A Training Centre Accreditation Checklist A. Accreditation of the HOSPITAL 1. Total number of beds in the hospital : Minimum 500 beds 2. Occupancy rate of beds in the hospital: Occupancy rate
Appendix A Training Centre Accreditation Checklist A. Accreditation of the HOSPITAL 1. Total number of beds in the hospital : Minimum 500 beds 2. Occupancy rate of beds in the hospital: Occupancy rate
Neoplasms/Lymphoma/Leukemia
 Neoplasms/Lymphoma/Leukemia Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and
Neoplasms/Lymphoma/Leukemia Session Guidelines This is a 15 minute webinar session for CNC physicians and staff CNC holds webinars monthly to address topics related to risk adjustment documentation and
CANCER IN IRELAND with estimates for : ANNUAL REPORT OF THE NATIONAL CANCER REGISTRY
 CANCER IN IRELAND 1994-2016 with estimates for 2016-2018: ANNUAL REPORT OF THE NATIONAL CANCER REGISTRY 2018 ABBREVIATIONS 95% CI 95% confidence interval APC Annual percentage change ASR Age-standardised
CANCER IN IRELAND 1994-2016 with estimates for 2016-2018: ANNUAL REPORT OF THE NATIONAL CANCER REGISTRY 2018 ABBREVIATIONS 95% CI 95% confidence interval APC Annual percentage change ASR Age-standardised
Suggested citation Thursfield V, Farrugia H. Cancer in Victoria: Statistics & Trends Cancer Council Victoria, Melbourne 2016
 CANCER IN VICTORIA STATISTICS & TRENDS 2015 Cancer Council Victoria 2016 November 2016, Cancer Council Victoria, Melbourne Editors: Vicky Thursfield and Helen Farrugia Suggested citation Thursfield V,
CANCER IN VICTORIA STATISTICS & TRENDS 2015 Cancer Council Victoria 2016 November 2016, Cancer Council Victoria, Melbourne Editors: Vicky Thursfield and Helen Farrugia Suggested citation Thursfield V,
Globally Optimal Statistical Classification Models, I: Binary Class Variable, One Ordered Attribute
 Globally Optimal Statistical Classification Models, I: Binary Class Variable, One Ordered Attribute Paul R. Yarnold, Ph.D. and Robert C. Soltysik, M.S. Optimal Data Analysis, LLC Imagine a random sample
Globally Optimal Statistical Classification Models, I: Binary Class Variable, One Ordered Attribute Paul R. Yarnold, Ph.D. and Robert C. Soltysik, M.S. Optimal Data Analysis, LLC Imagine a random sample
CANCER FACTS & FIGURES For African Americans
 CANCER FACTS & FIGURES For African Americans Pennsylvania, 2006 Pennsylvania Cancer Registry Bureau of Health Statistics and Research Contents Data Hightlights...1 Pennsylvania and U.S. Comparison...5
CANCER FACTS & FIGURES For African Americans Pennsylvania, 2006 Pennsylvania Cancer Registry Bureau of Health Statistics and Research Contents Data Hightlights...1 Pennsylvania and U.S. Comparison...5
All Discovered Death Outcome Detail (Form 124/120)
") This file includes all reported deaths regardless of consent. ID WHI Common ID Col#1 DEATHALL All Discovered Death Col#2 Any report of death, regardless of consent status. 0 No 106,931 66.1 1 Yes 54,877
This file includes all reported deaths regardless of consent. ID WHI Common ID Col#1 DEATHALL All Discovered Death Col#2 Any report of death, regardless of consent status. 0 No 106,931 66.1 1 Yes 54,877
CANCER IN AUSTRALIA. Australasian Association of Cancer Registries
 CANCER IN AUSTRALIA 2014 Australasian Association of Cancer Registries CANCER IN AUSTRALIA 2014 Cancer series number 91 Australian Institute of Health and Welfare, Canberra Cat. no. CAN 89 The Australian
CANCER IN AUSTRALIA 2014 Australasian Association of Cancer Registries CANCER IN AUSTRALIA 2014 Cancer series number 91 Australian Institute of Health and Welfare, Canberra Cat. no. CAN 89 The Australian
Cancer in Norway Cancer incidence, mortality, survival and prevalence in Norway
 Cancer in Norway 217 Cancer incidence, mortality, survival and prevalence in Norway Cancer in Norway 217 Cancer in Norway 217 Editor-in-chief: Inger Kristin Larsen Editorial team: IK Larsen, B Møller,
Cancer in Norway 217 Cancer incidence, mortality, survival and prevalence in Norway Cancer in Norway 217 Cancer in Norway 217 Editor-in-chief: Inger Kristin Larsen Editorial team: IK Larsen, B Møller,
Trends in Cancer Survival in Scotland
 Scottish Cancer Intelligence Unit Trends in Cancer Survival in Scotland - Trends in survival are presented for the half million adult cancer patients diagnosed in Scotland between and. The Results show,
Scottish Cancer Intelligence Unit Trends in Cancer Survival in Scotland - Trends in survival are presented for the half million adult cancer patients diagnosed in Scotland between and. The Results show,
Introduction to ICD-O-3 coding rules
 Introduction to ICD-O-3 coding rules Weena Laddachayaporn, MD National Cancer Institute, Bangkok, Thailand ICD-O-3 The International Classification of Diseases for Oncology Is a coding system for primary
Introduction to ICD-O-3 coding rules Weena Laddachayaporn, MD National Cancer Institute, Bangkok, Thailand ICD-O-3 The International Classification of Diseases for Oncology Is a coding system for primary
Estimated Minnesota Cancer Prevalence, January 1, MCSS Epidemiology Report 04:2. April 2004
 MCSS Epidemiology Report 04:2 Suggested citation Perkins C, Bushhouse S.. Minnesota Cancer Surveillance System. Minneapolis, MN, http://www.health.state.mn.us/divs/hpcd/ cdee/mcss),. 1 Background Cancer
MCSS Epidemiology Report 04:2 Suggested citation Perkins C, Bushhouse S.. Minnesota Cancer Surveillance System. Minneapolis, MN, http://www.health.state.mn.us/divs/hpcd/ cdee/mcss),. 1 Background Cancer
 This is the published version Stevenson, Chris, Harding, John, van der Hoek, Robert, Christensen, Edith, Leeds, Kate, Southgate, Kathy and Nobbs, Amanda 2001, Cancer in Australia 1998, Australian Institute
This is the published version Stevenson, Chris, Harding, John, van der Hoek, Robert, Christensen, Edith, Leeds, Kate, Southgate, Kathy and Nobbs, Amanda 2001, Cancer in Australia 1998, Australian Institute
John R. Marsh Cancer Center
 John R. Marsh Cancer Center Lung Program Overview: 2014-2015 Initiatives Lung CT Screening Dr. Gregory Zimmerman In cooperation with The Lung Cancer Steering Committee, Diagnostic Imaging Services at the
John R. Marsh Cancer Center Lung Program Overview: 2014-2015 Initiatives Lung CT Screening Dr. Gregory Zimmerman In cooperation with The Lung Cancer Steering Committee, Diagnostic Imaging Services at the
Nationwide Cancer Incidence in Korea,
 Cancer Res Treat. 2009;41(3):122-131 DOI 10.4143/crt.2009.41.3.122 Special Article Nationwide Cancer Incidence in Korea, 2003 2005 Young-Joo Won, Ph.D. 1 Joohon Sung, M.D. 1,2 Kyu-Won Jung, M.S. 1 Hyun-Joo
Cancer Res Treat. 2009;41(3):122-131 DOI 10.4143/crt.2009.41.3.122 Special Article Nationwide Cancer Incidence in Korea, 2003 2005 Young-Joo Won, Ph.D. 1 Joohon Sung, M.D. 1,2 Kyu-Won Jung, M.S. 1 Hyun-Joo
AMERICAN JOINT COMMITTEE ON CANCER AJCC CANCER STAGING
 AMERICAN JOINT COMMITTEE ON CANCER AJCC CANCER STAGING ATLAS EDITORS FREDERICK L. GREENE, m.d. Chair, Department of General Surgery Carolinas Medical Center Charlotte, North Carolina CAROLYN C. COMPTON,
AMERICAN JOINT COMMITTEE ON CANCER AJCC CANCER STAGING ATLAS EDITORS FREDERICK L. GREENE, m.d. Chair, Department of General Surgery Carolinas Medical Center Charlotte, North Carolina CAROLYN C. COMPTON,
Prediction of Cancer Incidence and Mortality in Korea, 2013
 pissn 1598-2998, eissn 256 Cancer Res Treat. 213;45(1):15-21 Special Article http://dx.doi.org/1.4143/crt.213.45.1.15 Open Access Prediction of Cancer Incidence and Mortality in Korea, 213 Kyu-Won Jung,
pissn 1598-2998, eissn 256 Cancer Res Treat. 213;45(1):15-21 Special Article http://dx.doi.org/1.4143/crt.213.45.1.15 Open Access Prediction of Cancer Incidence and Mortality in Korea, 213 Kyu-Won Jung,
HOSPITAL-BASED CANCER REGISTRY ANNUAL REPORT 2011
 HOSPITAL-BASED CANCER REGISTRY ANNUAL REPORT 2011 SONGKLANAGARIND HOSPITAL FACULTY OF MEDICINE PRINCE OF SONGKLA UNIVERSITY HATYAI SONGKHLA THAILAND EDITOR PARADEE PRECHAWITTAYAKUL, B.Sc. June, 2013 Songklanagarind
HOSPITAL-BASED CANCER REGISTRY ANNUAL REPORT 2011 SONGKLANAGARIND HOSPITAL FACULTY OF MEDICINE PRINCE OF SONGKLA UNIVERSITY HATYAI SONGKHLA THAILAND EDITOR PARADEE PRECHAWITTAYAKUL, B.Sc. June, 2013 Songklanagarind
Cancer Incidence in New Jersey Implementation of the Year 2000 Population Standard
 Cancer Incidence in New Jersey 1995-1999 Implementation of the Year 2000 Population Standard Prepared by: Stasia S. Burger, MS, CTR Judith B. Klotz, MS, DrPH Rachel Weinstein, MS, PhD Toshi Abe, MSW, CTR
Cancer Incidence in New Jersey 1995-1999 Implementation of the Year 2000 Population Standard Prepared by: Stasia S. Burger, MS, CTR Judith B. Klotz, MS, DrPH Rachel Weinstein, MS, PhD Toshi Abe, MSW, CTR
Cancer in New Brunswick
 Cancer in New Brunswick 2002-2006 Message from the New Brunswick Cancer Network (NBCN) Co-CEOs The New Brunswick Cancer Network is pleased to provide the Provincial Cancer Report 2002-2006. This is the
Cancer in New Brunswick 2002-2006 Message from the New Brunswick Cancer Network (NBCN) Co-CEOs The New Brunswick Cancer Network is pleased to provide the Provincial Cancer Report 2002-2006. This is the
Prediction of Cancer Incidence and Mortality in Korea, 2018
 pissn 1598-2998, eissn 256 Cancer Res Treat. 218;5(2):317-323 Special Article https://doi.org/1.4143/crt.218.142 Open Access Prediction of Cancer Incidence and Mortality in Korea, 218 Kyu-Won Jung, MS
pissn 1598-2998, eissn 256 Cancer Res Treat. 218;5(2):317-323 Special Article https://doi.org/1.4143/crt.218.142 Open Access Prediction of Cancer Incidence and Mortality in Korea, 218 Kyu-Won Jung, MS
Trends in Irish cancer incidence with predictions to 2020
 Trends in Irish cancer incidence 1994-22 with predictions to 22 Trends in Irish cancer incidence 1994-22 with projections to 22 National Cancer Registry June 26 1 Acknowledgements. I would like to thank
Trends in Irish cancer incidence 1994-22 with predictions to 22 Trends in Irish cancer incidence 1994-22 with projections to 22 National Cancer Registry June 26 1 Acknowledgements. I would like to thank
Cancer Treatment Centers of America ATLANTA CANCER REGISTRY. Annual Report
 Cancer Treatment Centers of America ATLANTA CANCER REGISTRY Annual Report CANCER COMMITTEE Chairman s Report On behalf of the Cancer Committee a multidisciplinary team of boardcertified physicians and
Cancer Treatment Centers of America ATLANTA CANCER REGISTRY Annual Report CANCER COMMITTEE Chairman s Report On behalf of the Cancer Committee a multidisciplinary team of boardcertified physicians and
Appendix A: Definitions for Cancer Incidence Data
 Appendices Cancer in Minnesota, 1988-2002 231 Appendix A: Definitions for Cancer Incidence Data MCSS collects information on all microscopically confirmed malignant and in situ tumors diagnosed in Minnesota
Appendices Cancer in Minnesota, 1988-2002 231 Appendix A: Definitions for Cancer Incidence Data MCSS collects information on all microscopically confirmed malignant and in situ tumors diagnosed in Minnesota
Cancer Incidences in Rural Delhi
 Cancer Incidences in Rural Delhi - 2004-2005 RESEARCH COMMUNICATION Cancer Incidences in Rural Delhi - 2004-05 N Manoharan*, B B Tyagi, Vinod Raina Abstract There are no data available on cancer incidence
Cancer Incidences in Rural Delhi - 2004-2005 RESEARCH COMMUNICATION Cancer Incidences in Rural Delhi - 2004-05 N Manoharan*, B B Tyagi, Vinod Raina Abstract There are no data available on cancer incidence
CODING PRIMARY SITE. Nadya Dimitrova
 CODING PRIMARY SITE Nadya Dimitrova OUTLINE What is coding and why do we need it? ICD-10 and ICD-O ICD-O-3 Topography coding rules ICD-O-3 online WHAT IS CODING AND WHY DO WE NEED IT? Coding: to assign
CODING PRIMARY SITE Nadya Dimitrova OUTLINE What is coding and why do we need it? ICD-10 and ICD-O ICD-O-3 Topography coding rules ICD-O-3 online WHAT IS CODING AND WHY DO WE NEED IT? Coding: to assign
MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site
 POLICY: PG0364 ORIGINAL EFFECTIVE: 04/22/16 LAST REVIEW: 07/26/18 MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site GUIDELINES This policy does not certify benefits or authorization
POLICY: PG0364 ORIGINAL EFFECTIVE: 04/22/16 LAST REVIEW: 07/26/18 MEDICAL POLICY Gene Expression Profiling for Cancers of Unknown Primary Site GUIDELINES This policy does not certify benefits or authorization
HUNT CANCER INSTITUTE CANCER SERVICES REPORT 2014
 HUNT CANCER INSTITUTE CANCER SERVICES REPORT 2014 COMMISSION ON CANCER STANDARD 1.12 Hunt Cancer Institute Mission Statement To be first in the South Bay/Peninsula communities in the provision of quality
HUNT CANCER INSTITUTE CANCER SERVICES REPORT 2014 COMMISSION ON CANCER STANDARD 1.12 Hunt Cancer Institute Mission Statement To be first in the South Bay/Peninsula communities in the provision of quality
DATA REQUEST RESPONSE- XRT AND BRACHYTHERAPY
 Date: 10 th April 2018 DATA REQUEST RESPONSE- XRT AND BRACHYTHERAPY Request: 1. Utilization Data of Overseas Beam Therapy and Brachytherapy 2. Diagnoses Data of Overseas Claims for Beam Therapy and Brachytherapy
Date: 10 th April 2018 DATA REQUEST RESPONSE- XRT AND BRACHYTHERAPY Request: 1. Utilization Data of Overseas Beam Therapy and Brachytherapy 2. Diagnoses Data of Overseas Claims for Beam Therapy and Brachytherapy
Comprehensive cancer cover
 Retirement Investments Insurance Health Comprehensive cancer cover Life Insurance+ with critical illness and Critical Illness+ Cancer is one of the biggest fears for the British public This is why our
Retirement Investments Insurance Health Comprehensive cancer cover Life Insurance+ with critical illness and Critical Illness+ Cancer is one of the biggest fears for the British public This is why our
Journal of the Statistical and Social Inquiry Society of Ireland Volume XXXIX. D.W. Donnelly & A.T. Gavin
 Journal of the Statistical and Social Inquiry Society of Ireland Volume XXXIX TRENDS AND PATTERNS IN CANCER MORTALITY IN NORTHERN IRELAND D.W. Donnelly & A.T. Gavin NI Cancer Registry, Queen s University
Journal of the Statistical and Social Inquiry Society of Ireland Volume XXXIX TRENDS AND PATTERNS IN CANCER MORTALITY IN NORTHERN IRELAND D.W. Donnelly & A.T. Gavin NI Cancer Registry, Queen s University
Cancer Program Report 2014
 Cancer Program Report 2014 Queen of the Valley Hospital St Joseph Health Queen of the Valley Hospital - 2014 Site Table Site Total Class Sex Group Cases Analytic NonAn M F 0 I II ALL SITES 661 494 167
Cancer Program Report 2014 Queen of the Valley Hospital St Joseph Health Queen of the Valley Hospital - 2014 Site Table Site Total Class Sex Group Cases Analytic NonAn M F 0 I II ALL SITES 661 494 167
Outcomes Report: Accountability Measures and Quality Improvements
 Outcomes Report: Accountability Measures and Quality Improvements The FH Memorial Medical Center s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures.
Outcomes Report: Accountability Measures and Quality Improvements The FH Memorial Medical Center s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures.
CANCER IN NSW ABORIGINAL PEOPLES. Incidence, mortality and survival September 2012
 CANCER IN NSW ABORIGINAL PEOPLES Incidence, mortality and survival September 2012 CANCER IN NSW ABORIGINAL PEOPLES Contents Tables 1 Figures 2 Message from the Chief Cancer Officer 4 Executive summary
CANCER IN NSW ABORIGINAL PEOPLES Incidence, mortality and survival September 2012 CANCER IN NSW ABORIGINAL PEOPLES Contents Tables 1 Figures 2 Message from the Chief Cancer Officer 4 Executive summary
What is the problem, and how big is it?
 Rare cancers What is the problem, and how big is it? Rare (orphan) diseases NIH Office for Rare Diseases Prevalence less than 5/10 000 in the community In the US
Rare cancers What is the problem, and how big is it? Rare (orphan) diseases NIH Office for Rare Diseases Prevalence less than 5/10 000 in the community In the US
Epidemiology in Texas 2006 Annual Report. Cancer
 Epidemiology in Texas 2006 Annual Report Cancer Epidemiology in Texas 2006 Annual Report Page 94 Cancer Incidence and Mortality in Texas, 2000-2004 The Texas Department of State Health Services Texas Cancer
Epidemiology in Texas 2006 Annual Report Cancer Epidemiology in Texas 2006 Annual Report Page 94 Cancer Incidence and Mortality in Texas, 2000-2004 The Texas Department of State Health Services Texas Cancer
Cancer Survival in Wales, Goroesi Cancr yng Nghymru,
 Cancer Survival in Wales, 1989-1998 Goroesi Cancr yng Nghymru, 1989-1998 Welsh Cancer Intelligence & Surveillance Unit Uned Arolygiaeth a Gwybodaeth Cancr Cymru DIRECTOR S INTRODUCTION I am pleased to
Cancer Survival in Wales, 1989-1998 Goroesi Cancr yng Nghymru, 1989-1998 Welsh Cancer Intelligence & Surveillance Unit Uned Arolygiaeth a Gwybodaeth Cancr Cymru DIRECTOR S INTRODUCTION I am pleased to
CHAPTER 10 CANCER REPORT. Germaine Wong Kirsten Howard Jonathan Craig Stephen McDonald Jeremy Chapman
 CHAPTER 10 CANCER REPORT Germaine Wong Kirsten Howard Jonathan Craig Stephen McDonald Jeremy Chapman CANCER REPORT ANZDATA Registry 2006 Report INTRODUCTION RISK OF CANCERS IN KIDNEY DISEASES Notification
CHAPTER 10 CANCER REPORT Germaine Wong Kirsten Howard Jonathan Craig Stephen McDonald Jeremy Chapman CANCER REPORT ANZDATA Registry 2006 Report INTRODUCTION RISK OF CANCERS IN KIDNEY DISEASES Notification