Immunohistochemical principles The technical test approach. Pre-analytical parametres
|
|
|
- Deborah Parrish
- 6 years ago
- Views:
Transcription


1 Immunohistochemical principles The technical test approach Pre-analytical parametres Søren Nielsen Global Pathology Manager Agilent Technologies (Former Scheme Manager, NordiQC)
2 2


3 IHC project coordinator at Institute of Pathology, Aalborg, Denmark & Scheme manager NordiQC till > IHC slides annually BenchMark Ultra, Ventana Autostainer Link 48, Dako Omnis, Dako Bond III, Leica IHC cooperation partners Biocare Cell Marque Dako / Agilent Leica Thermo Fisher Ventana / Roche + Ad hoc projects/partners 3
4 Agenda: 1. Focus on the main IHC technical challenges 2. How to optimize IHC assays 3. How to set-up and use controls to calibrate, verify and validate IHC assays 4


5 No formula I without basics Tyres No IHC without high quality tissue 5
6 The Power of IHC e.g. Breast Pathology Hyperplasia or In-situ CK5, CK14, Heavy chain myosin, p63 In-situ or invasive CK5, CK14, Heavy chain myosin, p63 Lobular or ductal lesion E-cadherin, p120 Predictive - Prognostic ER, PR, HER2, Ki67 Intrinsic subtype PAM50 ER, PR, HER2, Ki67, CK5 6


7 Original nomenclature and grouping of IHC tests: Class I / Type I IHC tests: Interpreted in the context of histo- or cytomorphologic and clinical data. Results interpreted and used by pathologists. E.g. CD45, TTF1, SOX10, CDX2, p40 etc Class III /Type II IHC tests: Stand-alone tests being interpreted (largely) to provide predictive and prognostic information. Results interpreted by pathologists and used by clinicians to give tailored treatment. E.g. ER, HER2, ALK, PD-L1 etc. Am J Clin Pathol 2010;133:




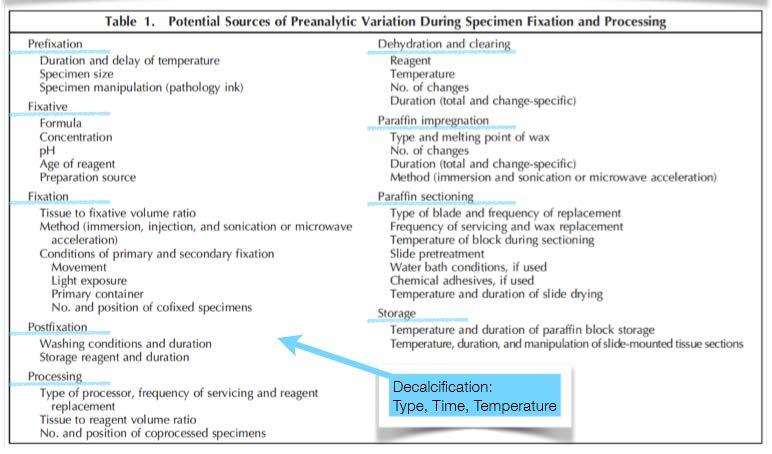
8 The biomarker protocol trap Caution: not for faint-hearted lab personel!!!!! Decalcification Preparation Tissue Type, Dimension, Laser resection, De-differentiation With 3 choices for 5 variables in each phase = > 4 million protocols. Controlment Quantification Reporting Fixation Time, Type, Volume Preanalytic Postanalytic Section Thickness Storage Drying Pre-treatment Manual Stainer Visualization Sensitivity, Specificity Primary antibody Clone, Dilution Buffer, Time, Temp Analytic Interpretation Localization Positive/Negative - cut-off level Development Sensitivity, Localization 8
9 The basal fundament for a technical optimal IHC performance: Appropriate tissue fixation and processing Appropriate and efficient epitope retrieval Appropriate choice & titre of antibody/clone Robust, specific & sensitive detection system Appropriate choice of control material 9
10 Appropriate tissue fixation and processing Problem 1: Delayed fixation Cold ischemic time Problem 2: Too short fixation in NBF Problem 3: Other fixatives than NBF Too long fixation in NBF is not a problem!!! Appropriate tissue fixation and processing Problem 1: Agressive decalcification Problem 2: Deviation from SOP e.g. section baking False negative or false positive 10
11 The vast majority of publications indicate inferior IHC/ISH performance in tissue subjected to delayed fixation. But To what degree? What is acceptable? What is best practice? 11

12 Time matters 12

 x")
13 4 C 20 C/RT H-score: intensity (0-3) x proportion (%) 13

14 Time and temp. matters 20 C/RT H-score: intensity (0-3) x proportion (%) 14


15 Cold ischemic time 1-2 hours: Phospho-HSP27 Phospho-AKT Phospho-ER Increased Reduced Stable Message; Consistency in tissue handling and transportation if possible Central for precision testing for precision medicine



16 Concl.: Cooling preserved specimens, whereas vacuum sealing added no effect (IHC and molecular assays) VS 4C - 1h VS 4C - 20h VS 4C - 1h VS 4C - 44h VS 4C - 92h VS RT - 92h VS RT - 44h VS RT - 92h
17 Pre-analytical variable Published guidelines Litterature based guidelines* ASCO/CAP - CLSI Fixation delay 1 hour < 12 hours (3-4 hours) Transportation temp. No data 4 C better than RT Vacuum sealing No data No data * Engel and. Moore (2011) Effects of Preanalytical Variables on the Detection of Proteins by Immunohistochemistry in Formalin-Fixed, Paraffin-Embedded Tissue. Archives of Pathology & Laboratory Medicine: May 2011, Vol. 135, No. 5, pp
18 Guidelines to; Tissue handling IHC / ISM methods Interpretation QA... 18
19 19
20 20
21 For more than 70 years NBF has shown to have a bizarre effect Formaldehyde is one of the fastest solutions regrading tissue penetration but one of the slowest regarding fixation Phase I Penetration Fast Phase II Binding Moderate Phase III Cross-linking Slow 21
22 Formaldehyde fixation How long will it take to fix? How fast does Formalin penetrate in tissue...??? 3 cm 22
23 Formaldehyde fixation How long will it take to fix? Penetration time at K = 3.6 (Baker s coeeficient) 1 hour = 3.6 mm 4 hours = 7.2 mm (1.8 mm/hr) 16 hours = 14.4 mm (0.9 mm/hr) 64 hours = 28.8 mm (0.45 mm/hr) 256 hours = 57.6 mm (0.225 mm/hr) ( d = K x t ) 1 h 16 h 3 cm (to double the depth takes 4x the time) 23



24 3 cm lymphnode not grossed 1 h 16 h 3 cm 24 CD10 56C6

25 Poor tissue handling 25



26 Poor tissue handling 26

27 NBF fix Alcohol fix 27
28 room temp. 37 C 4 x 4 x 4 mm liver tissue 100 % binding of formaldehyde after hours at 25 C 50 % binding of formaldehyde after 100 min. at 25 C Helander, KG. Kinetic studies of formaldehyde binding in tissue. Biotechnique and Histochemistry. 1994; 69,

29 <16-24 h Formaldehyde is a cross linking protein fixing agent, reacting clock-wise - the longer the more effective! Methylene glycol + free aldehyde = NBF 29 >16-24 h

30 To secure fixation and stabilization the fixation time is critical and not just the penetration time!!! h minimum for a 1 mm biopsy h minimum for a 4 mm specimen Penetration-time + Binding-time => Reaction/fixation-time 30

31 6-72h 8-72h 31


:86-92 The minimum formalin fixation")

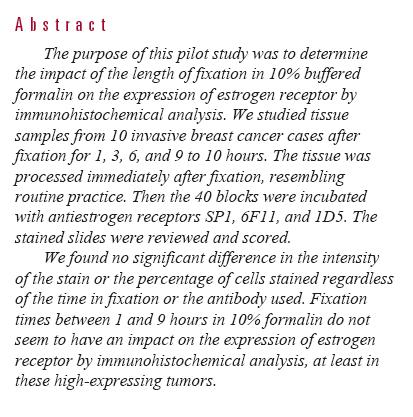
32 Minimum formalin fixation time for consistent estrogen receptor immunohistochemical staining of invasive breast carcinoma. Goldstein NS, Ferkowicz M, Odish E, Mani A, Hastah F Am J Clin Pathol Jul;120(1):86-92 The minimum formalin fixation time for reliable immunohistochemical ER results is 6 to 8 hours in our laboratory, regardless of the type or size of specimen 32 (core biopsy or resection). (mab clone 1D5)
33 33


34 Only tumours with a high ER expression to be validated in a larger study > 100 pts. 34

35 (Am J Surg Pathol 2014;38: ) CNB: 45 min. in NBF Res.: 8-72 h. in NBF CNB: mean average 91% pos. cells Res.: mean average 88% pos. cells. Caution: CNB: mean average 44% pos. cells Res.: mean average 58% pos. cells. Primarily only ER/PR high expressing tumour Each biomarker/antibody must be evaluated!!! 35
 Pathos 3h NBF, 6h prog.")
 Pathos 3h NBF, 6h prog.")
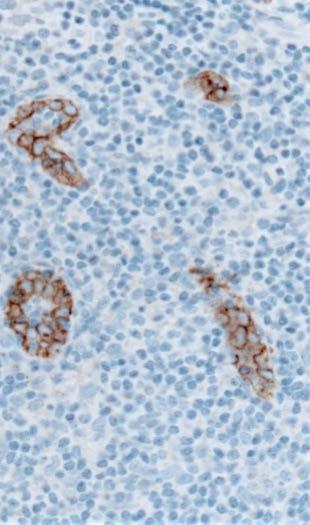
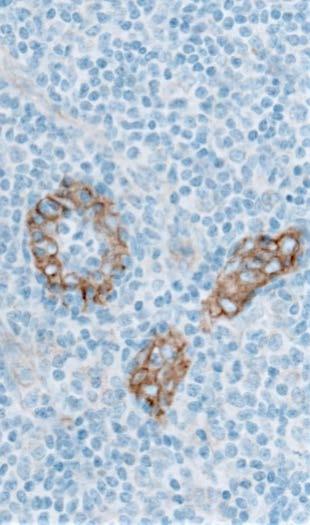
36 Colon: MSH2, mab clone G (same for MSH6, clone EP49) Pathos 3h NBF, 6h prog. Colon: MLH1, mab clone ES05 Pathos 24h NBF, 6h prog. (same for PMS2, clone EP51) Pathos 3h NBF, 6h prog. Pathos 24h NBF, 6h prog.

37 Colon: S100, polyclonal Pathos 3h NBF, 6h prog. Pathos 24h NBF, 6h prog. Pathos 48h NBF, 6h prog. Pathos 168h NBF, 6h prog. 37

38 Tonsil: S100, polyclonal S100 = Soluble in 100 % alcohol Pathos 3h NBF, 2h prog. Pathos 24h NBF, 2h prog. Pathos 48h NBF, 2h prog. Pathos 168h NBF, 2h prog. 38
39 13 hours versus 79 hours in 10% NBF (the week-end dilemma..) 101 breast carcinomas: 99 % Concordance between short fixation and long fixation for ER (SP1) 95 % Concordance between short fixation and long fixation for PR (1E2) 98 % Concordance between short fixation and long fixation for HER2 (A0485) 39
40 Internal IHC validation 4 h. NBF 24 h. NBF 48 h. NBF 168 h. NBF Tumour Tumour Tumour Tumour Tumour Tumour Tumour Tumour Tumour Breast carcinomas, HER-2 PATHWAY, rmab 4B5 (CC1 Mild, Ab inc. 20 min. 36 C, UltraView DAB)



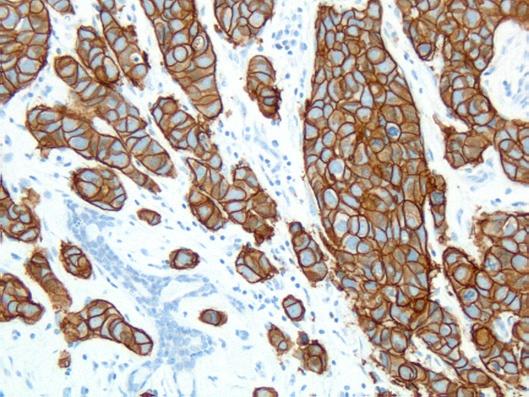
41 4 h 24 h 48 h 168 h Breast carcinoma 3+, HER-2 PATHWAY, rmab 4B5



42 4 h 24 h 48 h 168 h Breast carcinoma 1+, HER-2 PATHWAY, rmab 4B5
43 HER2 rmab 4B5 Internal IHC validation 4 h. NBF 24 h. NBF 48 h. NBF 168 h. NBF Tumour Tumour Tumour Tumour Tumour Tumour Tumour Tumour Tumour ER rmab SP1 Internal IHC validation 4 h. NBF 24 h. NBF 48 h. NBF 168 h. NBF Tumour Tumour Tumour Tumour Tumour Tumour Tumour Tumour Tumour Internal IHC validation 4 h. NBF 24 h. NBF 48 h. NBF 168 h. NBF Internal IHC validation 4 h. NBF 24 h. NBF 48 h. NBF 168 h. NBF Tumour Tumour PR rmab 1E2 Tumour Tumour Tumour Tumour Tumour ECAD mab NCH-36 Tumour Tumour Tumour Tumour Tumour Tumour Tumour Tumour Tumour Tumour Tumour Conclusion: IHC biomarkers not affected by NBF fixation time and patient material and control material can be fixed from 4-168h in 10% NBF. but
44 Internal SISH validation 4 h. NBF 24 h. NBF 48 h. NBF 168 h. NBF Tumour FN Tumour 2 Amp Tumour 3 (?) - FN FN Tumour FN FN Tumour Tumour 6 Amp Tumour FN Tumour 8 poly FN Tumour 9 poly FN HER-2 ISH: 8/36 cores could not be assessed..! Breast carcinomas, Dual SISH CCrb ext, P3. 8 m

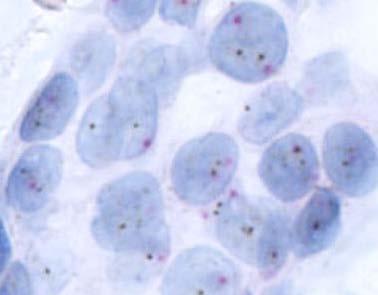
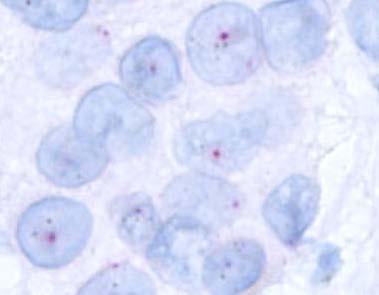
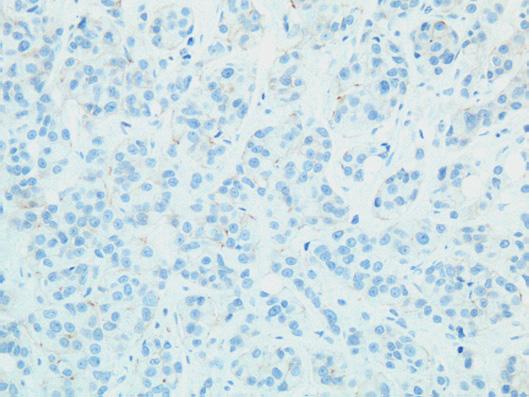
45 4 h 24 h 48 h 168 h Breast carcinoma, 1+ Dual SISH CCrb ext, P3. 8 m
46 Impact / Change of fixation time: 1. Use present standard times(s) as reference 2. Evaluate all biomarkers on material with the full diagnostic range of expression levels 3. Evaluate all different methods applied as diagnostic tools IHC / ISH / view-rna etc 46

47 Alternatives to Formalin 47

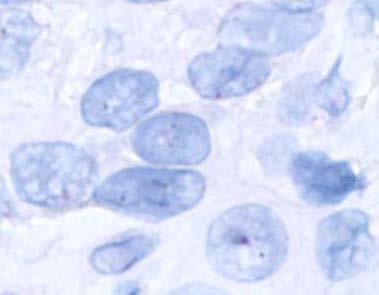
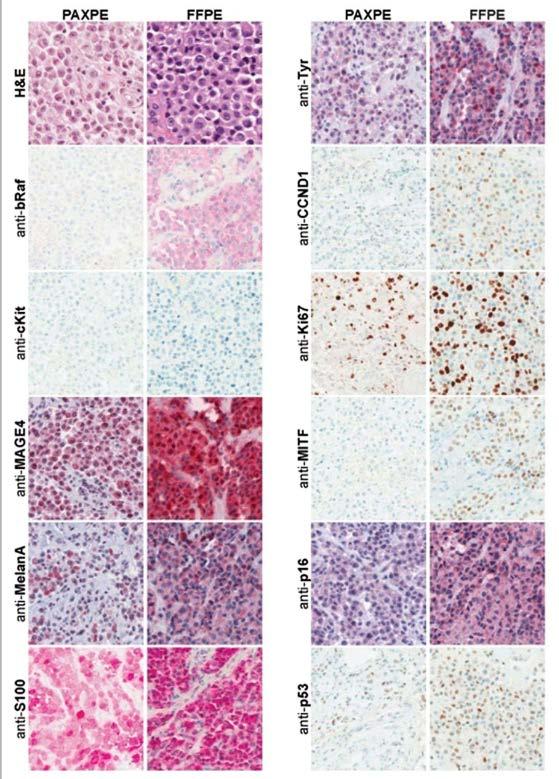
48 Fixative with focus on Morphology Molecular biology IHC 48


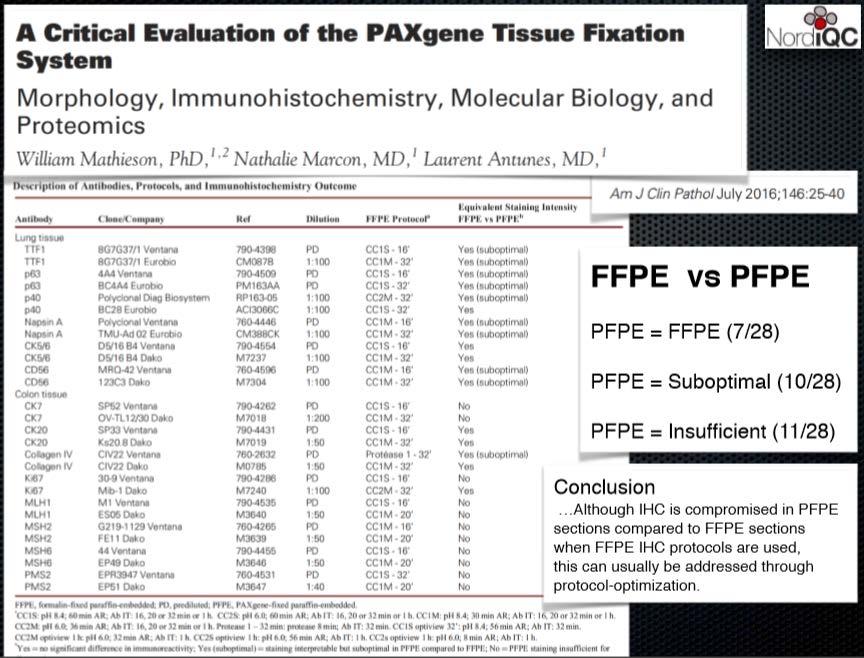
49 In conclusion, tissue fixed with the PAXgene Tissue System is morphologically comparable to formalin-fixed tissue but yields RNA which performs as well as RNA from fresh frozen tissue in RT PCR assays. For RNA from PFPE tissue, reverse transcription was not inhibited, and RNA purified from PFPE samples performed similarly to RNA isolated fromfresh frozen tissue regardless of amplicon length. 49
50 50
51 51
52 Pre-analytical variable Published guidelines Litterature based guidelines* ASCO/CAP - CLSI Fixative 10 % NBF** 10 % NBF Fixation time 8 72 hours Fixative tissue ratio 1:10 1:1 1:20 MW assisted fixation Pre-fixation 6 hours Pre-fixation 0 24 h. * Engel and. Moore (2011) Effects of Preanalytical Variables on the Detection of Proteins by Immunohistochemistry in Formalin-Fixed, Paraffin-Embedded Tissue. Archives of Pathology & Laboratory Medicine: May 2011, Vol. 135, No. 5, pp ** 10 % Neutral buffered formalin = 4 % Neutral buffered formaldehyde

53 Impact on IHC 53
: (4M formic acid + 0.")
54 Decalcification - Results: Courtesy Ole Nielsen 24 hrs 4% NBF fixation prior to decalcification. 193 different antibodies on TMA s Reference/No decalcification: +++ Buffet formic acid (BFA): (4M formic acid + 0.5M Na-formiat) 54

55 55Many Haemato-lymphoid markers affected

56 CD279 (PD-1), mab clone NAT105 No decalcification Formic acid 16 hours 10% EDTA 96 hours 56

57 CD105, mab clone SN6h No decalcification Formic acid 16 hours 10% EDTA 96 hours 57

58 CD105, mab clone 4G11 No decalcification Formic acid 16 hours 10% EDTA 96 hours 58
 IHC+ IHC++* IHC+++ DNA(+) DNA+/++ DNA++ * e.g.")
59 Strong acid: Mild acid: Calcium chelate: 10% HCL (Decal ) 10% Formic acid 5-10% EDTA Fast (1-2h) Intermediate (6-24h) Slow (24-96h) IHC+ IHC++* IHC+++ DNA(+) DNA+/++ DNA++ * e.g. CD79a, clone JCB117 reduced, Elastase, clone NP57 extracted 59


60 Prostate Ki67, rmab clone % NBF 24h 24h 10 % form. acid 10 % NBF + 10 % form. acid 24h 60
 2.")

61 1. AZF (or 10 % NBF) 2. 10% formic acid + 5% NBF
62 3-4 um sections mounted on Superfrost +, TOMO or Dako FLEX slides RTU systems based on 4 um sections Level adequate for morphology, signal-to-noise and interpretation 1 to 2 hours at 60 C Alternatively night over at 37 C followed by 1 hour at 60 C Having problems with attachment of sections Try change of slides (TOMO and Dako Flex superior) Verify formalin fixation time is adequate Too short time and long alcohol time hardens tissue Verify quality of reagents for tissue processing Verify section thickness Optimize HIER... 62



63 HER-2; FDA approved kit 1-2 μm 3-4 μm 6-7 μm





64 60 C 1h. Ref. score 60 C 16 h. 80 C 16 h. 95 C 1.5 h / /3 3+ 4/ / /5 2+ 4/34 60 C 1h. HER-2: C 16h. HER-2: 1+ 64


65 Paraffin Section Storage and Immunohistochemistry: Effects of Time, Temperature, Fixation, and Retrieval Protocol with Emphasis on p53 Protein and MIB1 Antigen Wester, Kenneth Ph.D.; Wahlund, Eva B.L.T.; Sundström, Christer M.D., Ph.D.; Ranefall, Petter Ph.D.; Bengtsson, Ewert Ph.D.; Russell, Pamela J. Ph.D.; Ow, Kim T. M. Sc.; Malmström, Per-Uno M.D., Ph.D.; Busch, Christer M.D., Ph.D. AIMM :Volume 8(1), March 2000, pp weeks at room-temp. Otherwise -20 / -80 C Baking just before use. Coating with paraffin is not confirmed to be beneficial
66 General settings for tissue processing for IHC Time to Fixation; 1 hour optimally at temp controlled conditions at 4C Use 10% Neutral Buffered Fomalin (same as 4% formaldehyde) Time in Fixation (10% NBF); 8-72 hours Gentle decalcification must be performed on appropriate fixed material 3-4 um sections applied on slides with high quality adhesiveness Store slides at maximum 1 week at room temp before IHC 66

67 Questions...??? 67
Breast cancer: Antibody selection, protocol optimzation controls and EQA
 Breast cancer: Antibody selection, protocol optimzation controls and EQA Workshop in Diagnostic Immunohistochemistry Oud St. Jan/ Old St. John Brugge (Bruges), Belgium June 13th 15nd 2018 Rasmus Røge,
Breast cancer: Antibody selection, protocol optimzation controls and EQA Workshop in Diagnostic Immunohistochemistry Oud St. Jan/ Old St. John Brugge (Bruges), Belgium June 13th 15nd 2018 Rasmus Røge,
SMH (Myosin, smooth muscle heavy chain)
") Material The slide to be stained for SMH comprised: Assessment Run 50 2017 SMH (Myosin, smooth muscle heavy chain) 1.Tonsil, 2. Esophagus, 3. Breast hyperplasia, 4. Breast ductal carcinoma in situ (DCIS),
Material The slide to be stained for SMH comprised: Assessment Run 50 2017 SMH (Myosin, smooth muscle heavy chain) 1.Tonsil, 2. Esophagus, 3. Breast hyperplasia, 4. Breast ductal carcinoma in situ (DCIS),
External Quality Assessment of Breast Marker Analysis. NordiQC data
 External Quality Assessment of Breast Marker Analysis NordiQC data Søren Nielsen Scheme Manager NordiQC Aalborg University Hospital, Denmark Aalborg 12.06 2015 Markers assessed in NordiQC Predictive markers
External Quality Assessment of Breast Marker Analysis NordiQC data Søren Nielsen Scheme Manager NordiQC Aalborg University Hospital, Denmark Aalborg 12.06 2015 Markers assessed in NordiQC Predictive markers
Assessment Run B HER2 IHC
 Assessment Run B24 2017 HER2 IHC Material The slide to be stained for HER2 comprised the following 5 materials: IHC: HER2 Score* (0, 1+, 2+, 3+) FISH: HER2 gene/chr 17 ratio** 1. Breast carcinoma, no.
Assessment Run B24 2017 HER2 IHC Material The slide to be stained for HER2 comprised the following 5 materials: IHC: HER2 Score* (0, 1+, 2+, 3+) FISH: HER2 gene/chr 17 ratio** 1. Breast carcinoma, no.
Optimization of antibodies, selection, protocols and controls Breast tumours
 Optimization of antibodies, selection, protocols and controls Breast tumours Søren Nielsen Project coordinator & Scheme Manager NordiQC Aalborg University Hospital, Denmark Breast panel: GCDFP-15 Mammaglobin
Optimization of antibodies, selection, protocols and controls Breast tumours Søren Nielsen Project coordinator & Scheme Manager NordiQC Aalborg University Hospital, Denmark Breast panel: GCDFP-15 Mammaglobin
Assessment Run B HER-2 IHC. HER-2/chr17 ratio**
 Assessment Run B2 20 HER-2 IHC Material The slide to be stained for HER-2 comprised the following 5 tissues: IHC HER-2 Score* (0, +, 2+,3+) FISH HER-2/chr7 ratio**. Breast ductal carcinoma 0..3 2. Breast
Assessment Run B2 20 HER-2 IHC Material The slide to be stained for HER-2 comprised the following 5 tissues: IHC HER-2 Score* (0, +, 2+,3+) FISH HER-2/chr7 ratio**. Breast ductal carcinoma 0..3 2. Breast
Assessment Run B HER2 IHC
 Assessment Run B26 208 HER2 IHC Material The slide to be stained for HER2 comprised the following 5 materials: IHC: HER2 Score* (0, +, 2+, 3+) FISH: HER2 gene/chr 7 ratio**. Breast carcinoma, no. 2+..3
Assessment Run B26 208 HER2 IHC Material The slide to be stained for HER2 comprised the following 5 materials: IHC: HER2 Score* (0, +, 2+, 3+) FISH: HER2 gene/chr 7 ratio**. Breast carcinoma, no. 2+..3
Estrogen receptor (ER)
") Material The slide to be stained for ER comprised: Assessment Run B26 2018 Estrogen receptor (ER) No. Tissue ER-positivity* ER-intensity* 1. Uterine cervix 80-90% Moderate to strong 2. Tonsil 1-5% Weak
Material The slide to be stained for ER comprised: Assessment Run B26 2018 Estrogen receptor (ER) No. Tissue ER-positivity* ER-intensity* 1. Uterine cervix 80-90% Moderate to strong 2. Tonsil 1-5% Weak
Assessment Run GATA3
 Assessment Run 44 2015 GATA3 Material The slide to be stained for GATA3 comprised: 1. Tonsil 2. Kidney, 3. Urothelial carcinoma, 4. Breast ductal carcinoma, 5. Colon adenocarcinoma All tissues were fixed
Assessment Run 44 2015 GATA3 Material The slide to be stained for GATA3 comprised: 1. Tonsil 2. Kidney, 3. Urothelial carcinoma, 4. Breast ductal carcinoma, 5. Colon adenocarcinoma All tissues were fixed
Estrogen receptor (ER)
") Assessment Run B7 204 Estrogen receptor (ER) Material The slide to be stained for ER comprised: No. Tissue ER-positivity* ER-intensity*. Uterine cervix 80-90% Moderate to strong 2. Breast carcinoma 0%
Assessment Run B7 204 Estrogen receptor (ER) Material The slide to be stained for ER comprised: No. Tissue ER-positivity* ER-intensity*. Uterine cervix 80-90% Moderate to strong 2. Breast carcinoma 0%
Carcinoembryonic antigen (CEA)
") Assessment Run 37 2013 Carcinoembryonic antigen (CEA) Material The slide to be stained for CEA comprised: 1. Appendix, 2. Liver, 3-4. Colon adenocarcinoma, 5. Urothelial carcinoma All tissues were fixed
Assessment Run 37 2013 Carcinoembryonic antigen (CEA) Material The slide to be stained for CEA comprised: 1. Appendix, 2. Liver, 3-4. Colon adenocarcinoma, 5. Urothelial carcinoma All tissues were fixed
NordiQC External Quality Assurance in Immunohistochemistry
 NordiQC External Quality Assurance in Immunohistochemistry Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark AALBORG (~ 200.000 inhabitants)
NordiQC External Quality Assurance in Immunohistochemistry Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark AALBORG (~ 200.000 inhabitants)
Assessment Run C1 2017
 Assessment Run C1 2017 PD-L1 The first assessment in this new NordiQC Companion module C1 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories to identify patients
Assessment Run C1 2017 PD-L1 The first assessment in this new NordiQC Companion module C1 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories to identify patients
Estrogen receptor (ER)
") Material The slide to be stained for ER comprised: Assessment B25 208 Estrogen receptor (ER) No. Tissue ER-positivity* ER-intensity*. Uterine cervix 80-90% Moderate to strong 2. Tonsil < 2-5% Weak to strong
Material The slide to be stained for ER comprised: Assessment B25 208 Estrogen receptor (ER) No. Tissue ER-positivity* ER-intensity*. Uterine cervix 80-90% Moderate to strong 2. Tonsil < 2-5% Weak to strong
Assessment Run C3 2018
 Assessment Run C3 2018 PD-L1 Amended version May 14 th 2018 The third assessment in NordiQC Companion module C3 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories
Assessment Run C3 2018 PD-L1 Amended version May 14 th 2018 The third assessment in NordiQC Companion module C3 focused on the accuracy of the PD-L1 IHC assays performed by the participating laboratories
Assessment Run
 Assessment Run 50 2017 S100 Material The slide to be stained for S100 comprised: 1. Appendix, 2. Tonsil, 3. Schwannoma, 4-5. Malignant melanoma, 6. Colon adenocarcinoma. All tissues were fixed in 10% neutral
Assessment Run 50 2017 S100 Material The slide to be stained for S100 comprised: 1. Appendix, 2. Tonsil, 3. Schwannoma, 4-5. Malignant melanoma, 6. Colon adenocarcinoma. All tissues were fixed in 10% neutral
Assessment Run NKX3.1 (NKX3.1)
") Assessment Run 49 2017 NKX3.1 (NKX3.1) Material The slide to be stained for NKX3.1 comprised: 1. Testis 2. Appendix 3-4. Prostate adenocarcinoma 5. Prostate hyperplasia All tissues were fixed in 10% neutral
Assessment Run 49 2017 NKX3.1 (NKX3.1) Material The slide to be stained for NKX3.1 comprised: 1. Testis 2. Appendix 3-4. Prostate adenocarcinoma 5. Prostate hyperplasia All tissues were fixed in 10% neutral
Thyroid transcription factor-1 (TTF1) Assessment run
 Assessment run") Thyroid transcription factor- (TTF) Assessment run 39 203 The slide to be stained for TTF comprised:. Thyroid gland, 2. Liver, 3. Normal lung, 4. Lung adenocarcinoma 5. Colon adenocarcinoma, 6 & 7. Lung
Thyroid transcription factor- (TTF) Assessment run 39 203 The slide to be stained for TTF comprised:. Thyroid gland, 2. Liver, 3. Normal lung, 4. Lung adenocarcinoma 5. Colon adenocarcinoma, 6 & 7. Lung
Lung Anaplastic Lymphoma Kinase (lu-alk)
") Assessment Run 5 207 Lung Anaplastic Lymphoma Kinase (lu-alk) Material The slide to be stained for lu-alk comprised:. Appendix, 2. Tonsil, 3. Merkel cell carcinoma, 4. Anaplastic large cell lymphoma with
Assessment Run 5 207 Lung Anaplastic Lymphoma Kinase (lu-alk) Material The slide to be stained for lu-alk comprised:. Appendix, 2. Tonsil, 3. Merkel cell carcinoma, 4. Anaplastic large cell lymphoma with
Quality Assurance in Immunohistochemistry: Experiences from NordiQC
 Nordic immunohistochemical Quality Control 2 Quality Assurance in Immunohistochemistry: Experiences from NordiQC Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg University Hospital Aalborg,
Nordic immunohistochemical Quality Control 2 Quality Assurance in Immunohistochemistry: Experiences from NordiQC Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg University Hospital Aalborg,
The impact of proficiency testing on lab immunoassays
 The impact of proficiency testing on lab immunoassays Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark Nordic Immunohistochemical Quality
The impact of proficiency testing on lab immunoassays Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark Nordic Immunohistochemical Quality
Immunohistochemistry. Potential and challenges To be or not to be
 Immunohistochemistry Potential and challenges To be or not to be Søren Nielsen Scheme Manager NordiQC Aalborg University Hospital, Denmark Vårmöte 19.05.2016 Karlstad Overview IHC project coordinator at
Immunohistochemistry Potential and challenges To be or not to be Søren Nielsen Scheme Manager NordiQC Aalborg University Hospital, Denmark Vårmöte 19.05.2016 Karlstad Overview IHC project coordinator at
Cytokeratin 19 (CK19)
") Assessment Run 34 202 Cytokeratin 9 (CK9) Material The slide to be stained for CK9 comprised:. Thyroid gland, 2. Appendix, 3. Esophagus, 4. Papillary thyroid carcinoma, 5 & 6. Pancreatic neuroendocrine
Assessment Run 34 202 Cytokeratin 9 (CK9) Material The slide to be stained for CK9 comprised:. Thyroid gland, 2. Appendix, 3. Esophagus, 4. Papillary thyroid carcinoma, 5 & 6. Pancreatic neuroendocrine
10 years of NordiQC Why are 30% of labs still getting it wrong?
 Mogens Vyberg & Søren Nielsen NordiQC Institute of Pathology Aalborg University Hospital Aalborg, Denmark May 29th 2015 10 years of NordiQC Why are 30% of labs still getting it wrong? Nothing to declare
Mogens Vyberg & Søren Nielsen NordiQC Institute of Pathology Aalborg University Hospital Aalborg, Denmark May 29th 2015 10 years of NordiQC Why are 30% of labs still getting it wrong? Nothing to declare
Assessment Run CK19
 Assessment Run 29 200 CK9 The slide to be stained for CK9 comprised:. Appendix, 2. Thyroid gland, 3. Pancreas, 4. Ductal breast carcinoma, 5. Esophagus, 6. Papillary thyroid carcinoma. All tissues were
Assessment Run 29 200 CK9 The slide to be stained for CK9 comprised:. Appendix, 2. Thyroid gland, 3. Pancreas, 4. Ductal breast carcinoma, 5. Esophagus, 6. Papillary thyroid carcinoma. All tissues were
Epithelial cell-cell adhesion molecule (Ep-CAM)
") Assessment Run 3 011 Epithelial cell-cell adhesion molecule (Ep-CAM) Material The slide to be stained for Ep-CAM comprised: 1. Appendix,. Kidney, 3. Adrenal gland, 4. Lung carcinoid, 5 & 6. Renal clear
Assessment Run 3 011 Epithelial cell-cell adhesion molecule (Ep-CAM) Material The slide to be stained for Ep-CAM comprised: 1. Appendix,. Kidney, 3. Adrenal gland, 4. Lung carcinoid, 5 & 6. Renal clear
HER2 ISH (BRISH or FISH)
") Assessment Run H14 2018 HER2 ISH (BRISH or FISH) Material Table 1. Content of the multi-block used for the NordiQC HER2 ISH assessment, run H14 HER2 IHC* IHC score Dual - SISH** FISH*** FISH*** HER2/chr17
Assessment Run H14 2018 HER2 ISH (BRISH or FISH) Material Table 1. Content of the multi-block used for the NordiQC HER2 ISH assessment, run H14 HER2 IHC* IHC score Dual - SISH** FISH*** FISH*** HER2/chr17
# Best Practices for IHC Detection and Interpretation of ER, PR, and HER2 Protein Overexpression in Breast Cancer
 #1034 - Best Practices for IHC Detection and Interpretation of ER, PR, and HER2 Protein Overexpression in Breast Cancer Richard W. Cartun, MS, PhD Andrew Ricci, Jr, MD Department of Pathology Hartford
#1034 - Best Practices for IHC Detection and Interpretation of ER, PR, and HER2 Protein Overexpression in Breast Cancer Richard W. Cartun, MS, PhD Andrew Ricci, Jr, MD Department of Pathology Hartford
Sal-like protein 4 (SALL4)
") Assessment Run 43 205 Sal-like protein 4 (SALL4) The slide to be stained for SALL4 comprised:. Appendix, 2. Testis, 3. Renal clear cell carcinoma, 4. Seminoma, 5. Intratubular germ cell neoplasia (IGCN),
Assessment Run 43 205 Sal-like protein 4 (SALL4) The slide to be stained for SALL4 comprised:. Appendix, 2. Testis, 3. Renal clear cell carcinoma, 4. Seminoma, 5. Intratubular germ cell neoplasia (IGCN),
IHC Stainer platforms. Overview, pros and cons
 IHC Stainer platforms Overview, pros and cons Bart De Wiest Quality manager IHC OLV Hospital, Aalst, Belgium Donald Van Hecke Lab & Quality manager AZ St-Lucas, Brugge, Belgium Goal of this lecture: to
IHC Stainer platforms Overview, pros and cons Bart De Wiest Quality manager IHC OLV Hospital, Aalst, Belgium Donald Van Hecke Lab & Quality manager AZ St-Lucas, Brugge, Belgium Goal of this lecture: to
Product Introduction. Product Codes: HCL029, HCL030 and HCL031. Issue
 Product Introduction Product Codes: HCL029, HCL030 and HCL031 Issue 1. 180510 Contents Introduction to Estrogen Receptor 2 ER immunohistochemistry 3 Quality control 5 Cell lines as controls 6 Estrogen
Product Introduction Product Codes: HCL029, HCL030 and HCL031 Issue 1. 180510 Contents Introduction to Estrogen Receptor 2 ER immunohistochemistry 3 Quality control 5 Cell lines as controls 6 Estrogen
NordiQC - update
 NordiQC - update 00-0 EQUALIS Uppsala 0 Tomas Seidal NordiQC participants NordiQC participants n:30 S DK N 6 F Ice Bel 54 NL 4 Ger 6 Aust USA 0 It 8 Argent 8.. 96% participation in S,DK & N ~ 60% in Finland
NordiQC - update 00-0 EQUALIS Uppsala 0 Tomas Seidal NordiQC participants NordiQC participants n:30 S DK N 6 F Ice Bel 54 NL 4 Ger 6 Aust USA 0 It 8 Argent 8.. 96% participation in S,DK & N ~ 60% in Finland
Nordic Immunohistochemical Quality Control
 Nordic Immunohistochemical Quality Control Immunohistochemistry in the classifiation of neoplasias of the alimentary tract & External Quality Assurance of Immunohistochemistry for GI cancer markers Mogens
Nordic Immunohistochemical Quality Control Immunohistochemistry in the classifiation of neoplasias of the alimentary tract & External Quality Assurance of Immunohistochemistry for GI cancer markers Mogens
PD-L1 Analyte Control DR
 Quality in Control PD-L1 Analyte Control DR PD-L1_PI_v2 Product Codes: HCL019, HCL020 and HCL021 Contents PD-L1 Analyte Control DR 2 What is PD-L1? 3 The Role of PD-L1 in Cancer 3 PD-L1 Assessment 4 PD-L1
Quality in Control PD-L1 Analyte Control DR PD-L1_PI_v2 Product Codes: HCL019, HCL020 and HCL021 Contents PD-L1 Analyte Control DR 2 What is PD-L1? 3 The Role of PD-L1 in Cancer 3 PD-L1 Assessment 4 PD-L1
Image analysis in IHC overview, considerations and applications
 Image analysis in IHC overview, considerations and applications Rasmus Røge, MD, Institute of Pathology, Aalborg University Hospital NordiQC workshop September 2016 Aalborg, Denmark Outline Theory Image
Image analysis in IHC overview, considerations and applications Rasmus Røge, MD, Institute of Pathology, Aalborg University Hospital NordiQC workshop September 2016 Aalborg, Denmark Outline Theory Image
Brief Formalin Fixation and Rapid Tissue Processing Do Not Affect the Sensitivity of ER Immunohistochemistry of Breast Core Biopsies
 Brief Formalin Fixation and Rapid Tissue Processing Do Not Affect the Sensitivity of ER Immunohistochemistry of Breast Core Biopsies Victoria Sujoy, MD, Mehrdad Nadji, MD, and Azorides R. Morales, MD From
Brief Formalin Fixation and Rapid Tissue Processing Do Not Affect the Sensitivity of ER Immunohistochemistry of Breast Core Biopsies Victoria Sujoy, MD, Mehrdad Nadji, MD, and Azorides R. Morales, MD From
Quality assurance and quality control in pathology in breast disease centers
 Quality assurance and quality control in pathology in breast disease centers Judith Sandbank M.D. Pathology Assaf-Harofeh Medical Center ISRAEL jsandbank@asaf.health.gov.il 1 st IBDC, 28 th January, 2011
Quality assurance and quality control in pathology in breast disease centers Judith Sandbank M.D. Pathology Assaf-Harofeh Medical Center ISRAEL jsandbank@asaf.health.gov.il 1 st IBDC, 28 th January, 2011
Breast cancer: IHC classification. Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
 Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
Breast cancer: IHC classification Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark http://upload.wikimedia.org/wikipedia/commons/1/1a/breast.svg
Quality Assurance and Quality Control in the Pathology Dept.
 Quality Assurance and Quality Control in the Pathology Dept. Judith Sandbank M.D. Pathology Assaf-Harofeh Medical Center ISRAEL jsandbank@asaf.health.gov.il 2 nd IBDC, 9 th February, 2012 Pathology as
Quality Assurance and Quality Control in the Pathology Dept. Judith Sandbank M.D. Pathology Assaf-Harofeh Medical Center ISRAEL jsandbank@asaf.health.gov.il 2 nd IBDC, 9 th February, 2012 Pathology as
HistoCyte Laboratories Ltd
 HistoCyte Laboratories Ltd Progesterone Receptor: The neglected breast receptor! Dr Ian Milton & Colin Tristram November 2018 UKNEQAS Autumn meeting Introduction Progesterone is an important prognostic
HistoCyte Laboratories Ltd Progesterone Receptor: The neglected breast receptor! Dr Ian Milton & Colin Tristram November 2018 UKNEQAS Autumn meeting Introduction Progesterone is an important prognostic
The unknown primary tumour: IHC classification part I, the primary panel - Antibody selection, protocol optimization, controls and EQA
 The unknown primary tumour: IHC classification part I, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark the primary panel - Antibody selection,
The unknown primary tumour: IHC classification part I, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark the primary panel - Antibody selection,
Dr. dr. Primariadewi R, SpPA(K)
") Curriculum Vitae Dr. dr. Primariadewi R, SpPA(K) Education : Medical Doctor from UKRIDA Doctoral Degree from Faculty of Medicine University of Indonesia Pathologist Specialist and Consultant from Faculty
Curriculum Vitae Dr. dr. Primariadewi R, SpPA(K) Education : Medical Doctor from UKRIDA Doctoral Degree from Faculty of Medicine University of Indonesia Pathologist Specialist and Consultant from Faculty
CC01 - Colon Cancer Tissue Microarray
 Reveal Biosciences offers Histochemical Staining, Immunohistochemistry (IHC), In Situ Hybridization (ISH), Whole Slide Imaging, and Quantitative Image Analysis on any TMA CC01 - Colon Cancer Tissue Microarray
Reveal Biosciences offers Histochemical Staining, Immunohistochemistry (IHC), In Situ Hybridization (ISH), Whole Slide Imaging, and Quantitative Image Analysis on any TMA CC01 - Colon Cancer Tissue Microarray
Reporting of Breast Cancer Do s and Don ts
 Reporting of Breast Cancer Do s and Don ts 7 th SGH Annual Breast Pathology Course Professor Michael Bilous Conjoint Professor Western Sydney University Consultant Pathologist, Australian Clinical Labs,
Reporting of Breast Cancer Do s and Don ts 7 th SGH Annual Breast Pathology Course Professor Michael Bilous Conjoint Professor Western Sydney University Consultant Pathologist, Australian Clinical Labs,
Product Introduction
 Product Introduction Product Codes: HCL026, HCL027 and HCL028 Contents Introduction to HER2 2 HER2 immunohistochemistry 3 Cell lines as controls 5 HER2 Analyte Control DR IHC 7 HER2 Analyte Control DR
Product Introduction Product Codes: HCL026, HCL027 and HCL028 Contents Introduction to HER2 2 HER2 immunohistochemistry 3 Cell lines as controls 5 HER2 Analyte Control DR IHC 7 HER2 Analyte Control DR
Single and Multiplex Immunohistochemistry
 Single and Multiplex Immunohistochemistry Steve Westra, BS Reagent Product Specialist Leica Biosystems IHC Theory Polyclonal vs Monoclonal Polyclonal reagents Detect a multitude of epitopes Batch to batch
Single and Multiplex Immunohistochemistry Steve Westra, BS Reagent Product Specialist Leica Biosystems IHC Theory Polyclonal vs Monoclonal Polyclonal reagents Detect a multitude of epitopes Batch to batch
Welcome! HER2 TESTING DIAGNOSTIC ACCURACY 4/11/2016
 HER2 TESTING DIAGNOSTIC ACCURACY Can t We Finally Get It Right? Allen M. Gown, M.D. Medical Director and Chief Pathologist PhenoPath Laboratories Seattle, Washington Clinical Professor of Pathology University
HER2 TESTING DIAGNOSTIC ACCURACY Can t We Finally Get It Right? Allen M. Gown, M.D. Medical Director and Chief Pathologist PhenoPath Laboratories Seattle, Washington Clinical Professor of Pathology University
Breast Cancer Diversity Various Disease Subtypes Clinical Diversity
 Breast Cancer Predictive Factor Testing: The Challenge and Importance of Standardizing Pre- Analytic Variables David G. Hicks MD Professor of Pathology & Laboratory Medicine Director of Surgical Pathology
Breast Cancer Predictive Factor Testing: The Challenge and Importance of Standardizing Pre- Analytic Variables David G. Hicks MD Professor of Pathology & Laboratory Medicine Director of Surgical Pathology
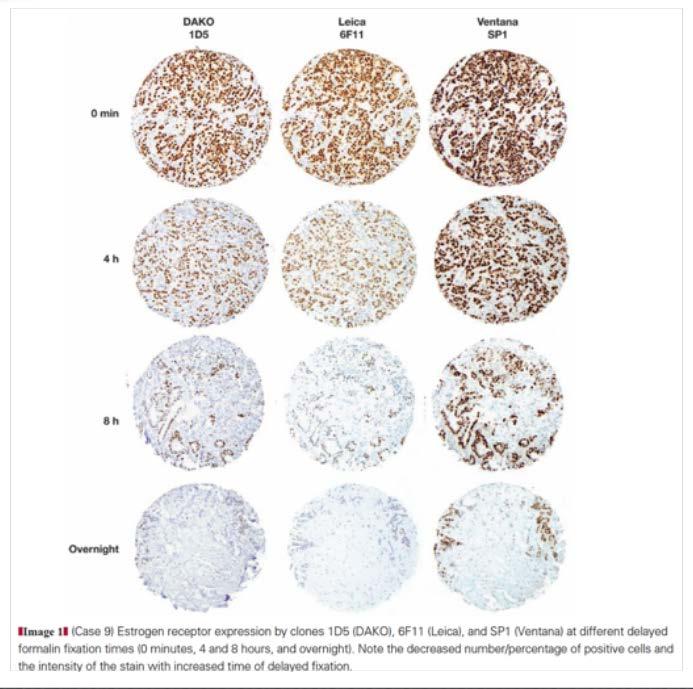
The Effect of Delay in Fixation, Different Fixatives, and Duration of Fixation in Estrogen and Progesterone Receptor Results in Breast Carcinoma
 Anatomic Pathology / Fixation Effects on ER and PR in Breast Cancer The Effect of Delay in Fixation, Different Fixatives, and Duration of Fixation in Estrogen and Progesterone Receptor Results in Breast
Anatomic Pathology / Fixation Effects on ER and PR in Breast Cancer The Effect of Delay in Fixation, Different Fixatives, and Duration of Fixation in Estrogen and Progesterone Receptor Results in Breast
LN04 - Lymphoma Tissue Microarray
 Reveal Biosciences offers Histochemical Staining, Immunohistochemistry (IHC), In Situ Hybridization (ISH), Whole Slide Imaging, and Quantitative Image Analysis on any TMA LN04 - Lymphoma Tissue Microarray
Reveal Biosciences offers Histochemical Staining, Immunohistochemistry (IHC), In Situ Hybridization (ISH), Whole Slide Imaging, and Quantitative Image Analysis on any TMA LN04 - Lymphoma Tissue Microarray
Quality in Control. ROS1 Analyte Control. Product Codes: HCL022, HCL023 and HCL024
 Quality in Control ROS1 Analyte Control Product Codes: HCL022, HCL023 and HCL024 Contents What is ROS1? 2 The Role of ROS1 in Cancer 3 ROS1 Assessment 3 ROS1 Analyte Control Product Details 4 ROS1 Analyte
Quality in Control ROS1 Analyte Control Product Codes: HCL022, HCL023 and HCL024 Contents What is ROS1? 2 The Role of ROS1 in Cancer 3 ROS1 Assessment 3 ROS1 Analyte Control Product Details 4 ROS1 Analyte
External Quality Assessment of melanocytic marker analyses NordiQC experience
 External Quality Assessment of melanocytic marker analyses NordiQC experience Jan Klos MD, Department of Pathology Stavanger University Hospital Norway 1 Content 18 Runs = 2112 submissions between 2001-2014
External Quality Assessment of melanocytic marker analyses NordiQC experience Jan Klos MD, Department of Pathology Stavanger University Hospital Norway 1 Content 18 Runs = 2112 submissions between 2001-2014
Assessment Run B HER-2
 Assessment Run B1 2006 HER-2 The slide to be stained for HER-2 comprised: 1. Cell line JIMT-1 (Amplified)* 2. Cell line MDA-453 (Amplified) 3. Cell line MCF-7 (Not amplified) 4. Cell line BT474 (Amplified)
Assessment Run B1 2006 HER-2 The slide to be stained for HER-2 comprised: 1. Cell line JIMT-1 (Amplified)* 2. Cell line MDA-453 (Amplified) 3. Cell line MCF-7 (Not amplified) 4. Cell line BT474 (Amplified)
Immunotherapy in NSCLC Pathologist role
 Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
System-wide Ownership Group: Allina Health Breast Program Committee. Hospital Division Quality Council: August 2018
 Oncology Clinical Service Line System-wide Consensus Guidelines: Evaluation and Management of Breast Lumpectomy and Mastectomy Specimens by Surgeons and Pathologists These guidelines apply to clinical
Oncology Clinical Service Line System-wide Consensus Guidelines: Evaluation and Management of Breast Lumpectomy and Mastectomy Specimens by Surgeons and Pathologists These guidelines apply to clinical
Assessment performed on Tuesday, July 29, 2014, at Lions Gate Hospital, North Vancouver
 Assessors report for ciqc Run 37: BRAF V600E (April 2014) Assessors: B Gilks, R Wolber, K Ung, P Tavassoli, J Garratt and J Won (recorder) Assessment performed on Tuesday, July 29, 2014, at Lions Gate
Assessors report for ciqc Run 37: BRAF V600E (April 2014) Assessors: B Gilks, R Wolber, K Ung, P Tavassoli, J Garratt and J Won (recorder) Assessment performed on Tuesday, July 29, 2014, at Lions Gate
The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, controls and EQA (part I)
") The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
The unkown primary tumour: IHC Classification, antibody selection, protocol optimization, Mogens Vyberg Professor of Clinical Pathology Director of NordiQC Aalborg University Hospital, Aalborg, Denmark
FAQs for UK Pathology Departments
 FAQs for UK Pathology Departments This is an educational piece written for Healthcare Professionals FAQs for UK Pathology Departments If you would like to discuss any of the listed FAQs further, or have
FAQs for UK Pathology Departments This is an educational piece written for Healthcare Professionals FAQs for UK Pathology Departments If you would like to discuss any of the listed FAQs further, or have
Breast cancer: Molecular STAGING classification and testing. Korourian A : AP,CP ; MD,PHD(Molecular medicine)
") Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
Breast cancer: Molecular STAGING classification and testing Korourian A : AP,CP ; MD,PHD(Molecular medicine) Breast Cancer Theory: Halsted Operative breast cancer is a local-regional disease The positive
07/06/2013. Commentary. The best way to achieve optimal treatment of today s patients is to ensure the availability of
 With main focus on the Estrogen Receptor Commentary The best way to achieve optimal treatment of today s patients is to ensure the availability of reliableand timelypathological th l i l assessment in
With main focus on the Estrogen Receptor Commentary The best way to achieve optimal treatment of today s patients is to ensure the availability of reliableand timelypathological th l i l assessment in
Assessment performed on Friday, September 18, 2015, at Vancouver General Hospital
 Assessors report for ciqc Run 49: ATRX (June 2015) Assessors: S Yip and J Won (recorder) Assessment performed on Friday, September 18, 2015, at Vancouver General Hospital Background The combined application
Assessors report for ciqc Run 49: ATRX (June 2015) Assessors: S Yip and J Won (recorder) Assessment performed on Friday, September 18, 2015, at Vancouver General Hospital Background The combined application
MT09 - Normal Human Tissue Microarray, FDA
 Reveal Biosciences offers Histochemical Staining, Immunohistochemistry (IHC), In Situ Hybridization (ISH), Whole Slide Imaging, and Quantitative Image Analysis on any TMA MT09 - Normal Human Tissue Microarray,
Reveal Biosciences offers Histochemical Staining, Immunohistochemistry (IHC), In Situ Hybridization (ISH), Whole Slide Imaging, and Quantitative Image Analysis on any TMA MT09 - Normal Human Tissue Microarray,
Immunohistochemistry on Fluid Specimens: Technical Considerations
 Immunohistochemistry on Fluid Specimens: Technical Considerations Blake Gilks Dept of Pathology University of British Columbia, Vancouver, BC, Canada Disclosures None Learning Objectives At the end of
Immunohistochemistry on Fluid Specimens: Technical Considerations Blake Gilks Dept of Pathology University of British Columbia, Vancouver, BC, Canada Disclosures None Learning Objectives At the end of
What kind of material should we use for ICC in our daily routine. Torill Sauer Department of Pathology, Akershus University Hospital
 What kind of material should we use for ICC in our daily routine Torill Sauer Department of Pathology, Akershus University Hospital Diversity of preparing cytological material Cell block Direct smears
What kind of material should we use for ICC in our daily routine Torill Sauer Department of Pathology, Akershus University Hospital Diversity of preparing cytological material Cell block Direct smears
Department of Pathology, Loyola University Medical Center, Maywood, IL 60153, USA 2
 Hindawi Publishing Corporation Pathology Research International Volume 2012, Article ID 947041, 7 pages doi:10.1155/2012/947041 Clinical Study The Effect of Cold Ischemia Time and/or Formalin Fixation
Hindawi Publishing Corporation Pathology Research International Volume 2012, Article ID 947041, 7 pages doi:10.1155/2012/947041 Clinical Study The Effect of Cold Ischemia Time and/or Formalin Fixation
Protocols for Zytomed Systems antibodies on fully automated IHC staining systems date of issue: September 20, 2012
 Protocols for Zytomed Systems antibodies on fully automated IHC staining systems date of issue: September 20, 2012 These protocols were provided by customers. Under no circumstances shall Zytomed Systems
Protocols for Zytomed Systems antibodies on fully automated IHC staining systems date of issue: September 20, 2012 These protocols were provided by customers. Under no circumstances shall Zytomed Systems
Next-Generation Immunohistochemistry: Multiplex tissue imaging with mass cytometry
 Nat Met, April 2014 Nat Med, April 2014 Next-Generation Immunohistochemistry: Multiplex tissue imaging with mass cytometry Journal Club Timo Böge Overview Introduction Conventional Immunohistochemistry
Nat Met, April 2014 Nat Med, April 2014 Next-Generation Immunohistochemistry: Multiplex tissue imaging with mass cytometry Journal Club Timo Böge Overview Introduction Conventional Immunohistochemistry
Immunohistochemical classification of breast tumours
 Immunohistochemical classification of breast tumours Workshop in Diagnostic Immunohistochemistry September 19 th - 21 th 2018 Anne-Vibeke Lænkholm Department of Surgical Pathology, Zealand University Hospital,
Immunohistochemical classification of breast tumours Workshop in Diagnostic Immunohistochemistry September 19 th - 21 th 2018 Anne-Vibeke Lænkholm Department of Surgical Pathology, Zealand University Hospital,
IDH1 R132H/ATRX Immunohistochemical validation
 IDH1 R132H/ATRX Immunohistochemical validation CIQC/DSM 2016 12 June 2016 0835-0905 Stephen Yip, M.D., Ph.D., FRCPC University of British Columbia Disclosure Statement I have nothing to disclose I will
IDH1 R132H/ATRX Immunohistochemical validation CIQC/DSM 2016 12 June 2016 0835-0905 Stephen Yip, M.D., Ph.D., FRCPC University of British Columbia Disclosure Statement I have nothing to disclose I will
Immunohistochemistry in Breast Pathology- Brief Overview of the Technique and Applications in Breast Pathology
 SMGr up Immunohistochemistry in Breast Pathology- Brief Overview of the Technique and Applications in Breast Pathology Bhanumathi K Rao 1 * 1 Department of Biochemistry, JSS Medical College, a constituent
SMGr up Immunohistochemistry in Breast Pathology- Brief Overview of the Technique and Applications in Breast Pathology Bhanumathi K Rao 1 * 1 Department of Biochemistry, JSS Medical College, a constituent
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer. Pathology. AGO e. V. in der DGGG e.v. sowie in der DKG e.v.
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Pathology Pathology Versions 2004 2017: Blohmer / Costa / Fehm / Friedrichs / Huober / Kreipe / Lück / Schneeweis / Sinn /
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Pathology Pathology Versions 2004 2017: Blohmer / Costa / Fehm / Friedrichs / Huober / Kreipe / Lück / Schneeweis / Sinn /
Proteomic Biomarker Discovery in Breast Cancer
 Proteomic Biomarker Discovery in Breast Cancer Rob Baxter Laboratory for Cellular and Diagnostic Proteomics Kolling Institute, University of Sydney, Royal North Shore Hospital robert.baxter@sydney.edu.au
Proteomic Biomarker Discovery in Breast Cancer Rob Baxter Laboratory for Cellular and Diagnostic Proteomics Kolling Institute, University of Sydney, Royal North Shore Hospital robert.baxter@sydney.edu.au
Milestones in Her 2 Testing
 Human Epidermal Growth Factor Receptor 2 (HER2) Testing - Validation, Application and Correlation Her2 is encoded by the C-erbB2 gene and is one of four oncoproteins belonging to the Human Epidermal Growth
Human Epidermal Growth Factor Receptor 2 (HER2) Testing - Validation, Application and Correlation Her2 is encoded by the C-erbB2 gene and is one of four oncoproteins belonging to the Human Epidermal Growth
DOUBLE STAINS. Toll-Free: Direct:
 DOUBLE STAINS CD61 + CD71 DAB Brown: CD61 Alk. Phos. Red: CD71 Bone Marrow DAB Brown: Megakaryocytes Alk. Phos. Red: Erythroid Precursors 400x CD61 (2f2) 0.1 ml concentrate............. 161M-14 0.5 ml
DOUBLE STAINS CD61 + CD71 DAB Brown: CD61 Alk. Phos. Red: CD71 Bone Marrow DAB Brown: Megakaryocytes Alk. Phos. Red: Erythroid Precursors 400x CD61 (2f2) 0.1 ml concentrate............. 161M-14 0.5 ml
ICSH guidelines for the standardization of bone marrow immunohistochemistry
 International Journal of Laboratory Hematology REVIEW The Official journal of the International Society for Laboratory Hematology INTERNATIONAL JOURNAL OF LABORATORY HEMATOLOGY ICSH guidelines for the
International Journal of Laboratory Hematology REVIEW The Official journal of the International Society for Laboratory Hematology INTERNATIONAL JOURNAL OF LABORATORY HEMATOLOGY ICSH guidelines for the
RNA preparation from extracted paraffin cores:
 Supplementary methods, Nielsen et al., A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor positive breast cancer.
Supplementary methods, Nielsen et al., A comparison of PAM50 intrinsic subtyping with immunohistochemistry and clinical prognostic factors in tamoxifen-treated estrogen receptor positive breast cancer.
Simultaneous de-waxing and standardisation of antigen retrieval in immunohistochemistry using commercially available equipment
 Reprinted by permission of UK NEQAS Immunocytochemistry and David S. Gray Kind thanks to David S. Gray for allowing ThermoFisher Scientific, Lab Vision Products, to distribute this article. Immunocytochemistry
Reprinted by permission of UK NEQAS Immunocytochemistry and David S. Gray Kind thanks to David S. Gray for allowing ThermoFisher Scientific, Lab Vision Products, to distribute this article. Immunocytochemistry
Patterns of E.cadherin and Estrogen receptor Expression in Histological Sections of Sudanese Patients with Breast Carcinoma
 Patterns of E.cadherin and Estrogen receptor Expression in Histological Sections of Sudanese Patients with Breast Carcinoma Hadia. Mohammed. Abdalla. Abdalrhman *, Elsadig.A.Adam, Ayda.D.A.Allatif 3,'Namareg.E.Afadul
Patterns of E.cadherin and Estrogen receptor Expression in Histological Sections of Sudanese Patients with Breast Carcinoma Hadia. Mohammed. Abdalla. Abdalrhman *, Elsadig.A.Adam, Ayda.D.A.Allatif 3,'Namareg.E.Afadul
Quality Indicators - Anatomic Pathology- HSC/STC Jul-Sep 2 nd Qtr. Apr-Jun 1 st Qtr
 Eastern Health Volume 86 Page 001 CIHRT Exhibit P-3595 Page 1 INDICATOR Financial Overtime Hours / FTE Workload Increase - FTE equivalent Workload Quality Indicators - Anatomic Pathology- HSC/STC TOTAL
Eastern Health Volume 86 Page 001 CIHRT Exhibit P-3595 Page 1 INDICATOR Financial Overtime Hours / FTE Workload Increase - FTE equivalent Workload Quality Indicators - Anatomic Pathology- HSC/STC TOTAL
Kristen E. Muller, DO, Jonathan D. Marotti, MD, Vincent A. Memoli, MD, Wendy A. Wells, MD, and Laura J. Tafe, MD
 AJCP / Original Article Impact of the 2013 ASCO/CAP HER2 Guideline Updates at an Academic Medical Center That Performs Primary HER2 FISH Testing Increase in Equivocal Results and Utility of Reflex Immunohistochemistry
AJCP / Original Article Impact of the 2013 ASCO/CAP HER2 Guideline Updates at an Academic Medical Center That Performs Primary HER2 FISH Testing Increase in Equivocal Results and Utility of Reflex Immunohistochemistry
The Panel Approach to Diagnostics. Lauren Hopson International Product Specialist Cell Marque Corporation
 The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
The Panel Approach to Diagnostics Lauren Hopson International Product Specialist Cell Marque Corporation Cell Marque Rocklin, California About Cell Marque: IVD primary antibody manufacturer Distributors
Applications of IHC. Determination of the primary site in metastatic tumors of unknown origin
 Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Applications of IHC Determination of the primary site in metastatic tumors of unknown origin Classification of tumors that appear 'undifferentiated' by standard light microscopy Precise classification
Classification of the unknown primary tumour: the primary IHC panel
 CIQC/CAP-ACP SEMINAR 2013: DIAGNOSTIC IHC AND MOLECULAR PATHOLOGY Classification of the unknown primary tumour: the primary IHC panel Aalborg University Hospital Denmark Tumours of unknown origin: Histology
CIQC/CAP-ACP SEMINAR 2013: DIAGNOSTIC IHC AND MOLECULAR PATHOLOGY Classification of the unknown primary tumour: the primary IHC panel Aalborg University Hospital Denmark Tumours of unknown origin: Histology
Quality Control/Quality Assurance in Diagnostic Immunohistochemistry
 CIHRT Exhibit P- Page Quality Control/Quality Assurance in Diagnostic Immunohistochemistry Emina Torlakovic, MD, PhD College of Medicine University of Saskatchewan Emina Emilia Torlakovic, MD, PhD Associate
CIHRT Exhibit P- Page Quality Control/Quality Assurance in Diagnostic Immunohistochemistry Emina Torlakovic, MD, PhD College of Medicine University of Saskatchewan Emina Emilia Torlakovic, MD, PhD Associate
Evolution of Pathology
 1 Traditional pathology Molecular pathology 2 Evolution of Pathology Gross Pathology Cellular Pathology Morphologic Pathology Molecular/Predictive Pathology Antonio Benivieni (1443-1502): First autopsy
1 Traditional pathology Molecular pathology 2 Evolution of Pathology Gross Pathology Cellular Pathology Morphologic Pathology Molecular/Predictive Pathology Antonio Benivieni (1443-1502): First autopsy
Immunohistochemical classification of the unknown primary tumour (UPT) Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark
 Part I. Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark") Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Immunohistochemical classification of the unknown primary tumour (UPT) Part I Prof. Mogens Vyberg NordiQC Institute of Pathology Aalborg, Denmark Tumours of unknown origin: Histology Brain tumour - biopsy
Breast cancer diagnostic solutions Deliver diagnostic confidence
 Breast cancer diagnostic solutions Deliver diagnostic confidence 2 Breast cancer diagnostic solutions Roche Tissue Diagnostics is committed to improving outcomes in breast cancer Breast cancer...the most
Breast cancer diagnostic solutions Deliver diagnostic confidence 2 Breast cancer diagnostic solutions Roche Tissue Diagnostics is committed to improving outcomes in breast cancer Breast cancer...the most
Workflow. Connecting the Pieces For Total Patient Care
 Workflow Connecting the Pieces For Total Patient Care Biocare provides a full line of IHC and molecular pathology products for cancer and infectious disease diagnosis. From a full range of equipment: including
Workflow Connecting the Pieces For Total Patient Care Biocare provides a full line of IHC and molecular pathology products for cancer and infectious disease diagnosis. From a full range of equipment: including
Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology
 Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology Ugur Ozerdem, M.D. 1 Abstract Background: There is a paradigm shift in breast biopsy philosophy. In
Utility of Adequate Core Biopsy Samples from Ultrasound Biopsies Needed for Today s Breast Pathology Ugur Ozerdem, M.D. 1 Abstract Background: There is a paradigm shift in breast biopsy philosophy. In
ONCO TEAM DIAGNOSTIC
 ONCO TEAM DIAGNOSTIC ONCO TEAM SPECIALISTS The team at ONCO TEAM has 23 specialists: o 11 general pathology seniors: - 8 PhD (1 PhD on lung tumors pathology) o 3 general pathology specialists; o 2 dermopathology
ONCO TEAM DIAGNOSTIC ONCO TEAM SPECIALISTS The team at ONCO TEAM has 23 specialists: o 11 general pathology seniors: - 8 PhD (1 PhD on lung tumors pathology) o 3 general pathology specialists; o 2 dermopathology
Immunohistochemical Expression of Hormone Receptors and The Histological Characteristics of Biochemically Hormone Receptor Negative Breast Cancers
 Breast Cancer Vol. 14 No. 1 January 2007 Original Article Immunohistochemical Expression of Hormone Receptors and The Histological Characteristics of Biochemically Hormone Receptor Negative Breast Cancers
Breast Cancer Vol. 14 No. 1 January 2007 Original Article Immunohistochemical Expression of Hormone Receptors and The Histological Characteristics of Biochemically Hormone Receptor Negative Breast Cancers
HER2 status assessment in breast cancer. Marc van de Vijver Academic Medical Centre (AMC), Amsterdam
, Amsterdam") HER2 status assessment in breast cancer Marc van de Vijver Academic Medical Centre (AMC), Amsterdam 13e Bossche Mamma Congres 17 th June 2015 Modern cancer therapies are based on sophisticated molecular
HER2 status assessment in breast cancer Marc van de Vijver Academic Medical Centre (AMC), Amsterdam 13e Bossche Mamma Congres 17 th June 2015 Modern cancer therapies are based on sophisticated molecular
Assessment of Breast Cancer with Borderline HER2 Status Using MIP Microarray
 Assessment of Breast Cancer with Borderline HER2 Status Using MIP Microarray Hui Chen, Aysegul A Sahin, Xinyan Lu, Lei Huo, Rajesh R Singh, Ronald Abraham, Shumaila Virani, Bal Mukund Mishra, Russell Broaddus,
Assessment of Breast Cancer with Borderline HER2 Status Using MIP Microarray Hui Chen, Aysegul A Sahin, Xinyan Lu, Lei Huo, Rajesh R Singh, Ronald Abraham, Shumaila Virani, Bal Mukund Mishra, Russell Broaddus,
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al -
 Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we
 9e avondsymposium: "Nieuwe ontwikkelingen in de behandeling van NSCLC" 9 november 2016, UMCG Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we Wim Timens Professor and Chair
9e avondsymposium: "Nieuwe ontwikkelingen in de behandeling van NSCLC" 9 november 2016, UMCG Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we Wim Timens Professor and Chair
The use of diagnostic FFPE material in cancer epidemiology research
 The use of diagnostic FFPE material in cancer epidemiology research Neil O Callaghan Genetic Epidemiology Laboratory Department of Pathology The University of Melbourne www.pedigree.org.au Overview Who
The use of diagnostic FFPE material in cancer epidemiology research Neil O Callaghan Genetic Epidemiology Laboratory Department of Pathology The University of Melbourne www.pedigree.org.au Overview Who
Optimal algorithm for HER2 testing
 Optimal algorithm for HER2 testing The revised definition of IHC 2+ (equivocal) is invasive breast cancer with Weak to moderate complete membrane staining observed in >10% of tumor cells. (see Figure 1
Optimal algorithm for HER2 testing The revised definition of IHC 2+ (equivocal) is invasive breast cancer with Weak to moderate complete membrane staining observed in >10% of tumor cells. (see Figure 1
Results you can trust
 PRODUCT I NF OR MAT ION pharmdx Results you can trust The first and only FDA-approved PD-L1 test to assess the magnitude of treatment effect on progression-free survival in melanoma patients from OPDIVO
PRODUCT I NF OR MAT ION pharmdx Results you can trust The first and only FDA-approved PD-L1 test to assess the magnitude of treatment effect on progression-free survival in melanoma patients from OPDIVO
Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano
 Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano Unit of Pathology Fondazione IRCCS Casa Sollievo della Sofferenza San Giovanni Rotondo, Foggia,Italy p.graziano@operapadrepio.it Disclosure
Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano Unit of Pathology Fondazione IRCCS Casa Sollievo della Sofferenza San Giovanni Rotondo, Foggia,Italy p.graziano@operapadrepio.it Disclosure