Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
|
|
|
- Austin Turner
- 6 years ago
- Views:
Transcription
1 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care
2 No Disclosures
3 Learning Objectives Review the classification scheme for GE junction cancers Review workup and evaluation Review Minimally Invasive Esophagectomy
4 Epidemiology Esophageal Cancer is 6 th leading cause of death worldwide Incidence has been rising in Western countries ~17,000 cases anticipated 2015 in US Adenocarcinoma 70% Obesity, GERD, Barretts Squamous Cell Carcinoma 30% Tobacco, Alcohol
5 Squam Esophageal Adeno Adeno Melanoma Prostate Breast/lung/ colon Distal 1/3 Pohl & Welch, JNCI 2005
6 Cancer at the GE Junction Siewart Classification I located in the distal 5 cm of esophagus, but does not cross GE junction II centered around the GE junction III greater than 5 cm distal to the GE junction Treated as Gastric Cancer Marriette, Lancet Onc 2011
7 Patient Examples of GE Junction Cancer Esophageal Cancer I/II Gastric Cancer III
 Assessment of T-stage; Nodal involvement FNA of suspicious node CT /")
8 Evaluation of the Esophageal Mass High quality endoscopy Defines the anatomic esophagogastric junction Describes the anatomic location Endoscopic ultrasound (EUS) Assessment of T-stage; Nodal involvement FNA of suspicious node CT / PET

9 Staging of Esophageal Cancer T Stage T1a : lamina propria, muscularis mucosa T1b : submucosa T2 : muscularis propria T3 : adventitia T4 : adjacent structures N Stage N1 : 1-2 nodes N2 : 3-6 nodes N3 : > 7 nodes J Thoracic Surg 2017
10 Accuracy of EUS for T Stage / Nodes Operator dependent Very good at early vs late (ie T1 vs T3/4) More difficult discerning between earlier lesions (ie T1a vs T1b vs T2) Review of 107 patients with early stage (Tis, T1) compared to final pathology Understaging: 30% of T1a 49% of T1b Overstaging: 29% of T1a 51% of T1b J Thor and Cardiovas Surg 2014

11 Risk of Nodal Disease Based on T stage Lymph node involvement greatest predictor of prognosis T stage is best predictor of lymph node involvement Squam us T1 T1a T1b T2 T3 T4 20% 0-3% 5-40% 40 % Adeno 10% 0-2% 0-40% 50 % 60 % 80 % 80 % 90 % Clin Endosc 2014
12 Staging Laparoscopy Used selectively in patient with Type II/III tumors Yield is variable (5%-30%) Extraluminal assessment of tumor location Evaluate future conduit Placement of feeding jejunostomy
13 Early Stage (T1, N0) Endoscopic Therapies for Tis or T1a EMR / ESD followed by ablation Esophagectomy Locally Advanced (T2 or N+) Neoadjuvant therapy Metastatic Definitive Chemotherapy
14 Endoscopic Therapies Endoscopic Mucosal Resection Endoscopic Submucosal Dissection Ablation of Surrounding Barrett s
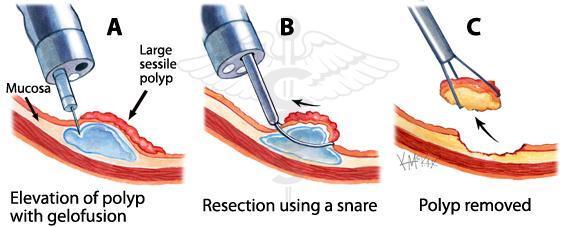
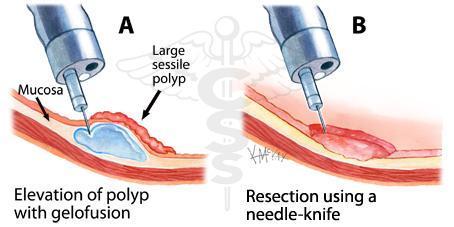
15 Colorectalsurgeonsydney.com
16 Locally Advanced Disease T2 tumors N+ disease Neoadjuvant Chemotherapy & Radiation Paclitaxel and Carboplatin weekly x 5 weeks 50.4 Gy over 28 fractions
17 CROSS Trial Randomized patients to preop chemoxrt + surgery vs. surgery alone Carboplatin & Paclitaxel 41.4 Gy radiation over 23 fractions R0 resection rate (92% vs 69%) 29% complete pathologic response 23% adenocarcinoma 49% squamous Van Hagen, NEJM 2012
18 CROSS Trial
19 CROSS Patterns of Recurrence CRT had lower local recurrence rate Anastomosis: 2.8% vs 8.7% Mediastinum: 7.0% vs 20.5% CRT had lower distant recurrence rate Carcinomatosis: 4.2% vs 13.7% Hematogenous: 28.6% vs 35.4% No difference in Nodal recurrence Celiac, Periaortic, Supraclavicular Oppedijk et al. JCO :385
20 MAGIC Trial Evaluated Perioperative Chemotherapy vs Surgery Alone Gastric Cancer including the lower 1/3 of esophagus 25% were GE Jxn (11%) or Esophageal (14%) Epirubicin/Cisplatin/Fluoruracil 3 cycles preop / 3 cycles post op 86% of patients completed preop chemo 55% started post op chemo 41% of patients assigned to the chemotherapy group completed all 6 cycles
21 Cunningham et al, NEJM 2006
22 FLOT FLOT Fluorouracil / leucovorin Oxaliplatin Docetaxel Phase 3 FLOT 4 - abstract FLOT vs ECF/ ECX Improved OS (50 v 35 mo) Improved PFS (30 v 18 mo) Improved R0 Smaller tumors FLOT vs Cross Propensity matched study No survival benefit CRT had better tumor response, fewer nodes ESOPEC Randomizing pts to FLOT vs CROSS Opened 2016 Expected NCT ESMO 2017 Abs LBA27 Eur J Surg Onc 2017 BMC Cancer 2016


23 Surgical Approaches to Esophagectomy Transhiatal Abdominal incision Neck incision Anastomosis in the Neck Ivor Lewis Abdominal incision Right chest incision Anastomosis in the Chest Minimally Invasive Esophagectomy

24 Marriette, Lancet Onc 2011
25 Comparison of Open Approaches Transhiatal % Ivor Lewis % P-Value Pneumonia NS Sepsis/Shock NS Return to OR Morbidity NS Serious Morbidity NS Mortality Papenfuss et al, J Surg Onc 2014
26 Minimally Invasive Esophagectomy Improvement in Morbidity Extent of Lymphadenectomy Multiple approaches described
27 >1000 MIE 48% Neck Anastomosis 52% Chest Anastomosis Neck Chest P value RLN 8% 1% <0.001 Leak 5% 4% 0.4 Mortality 2.5% 0.9% 0.08 Luketich, Ann Surg 2012
28 MIE vs Traditional Esophagectomy RCT of 115 patients to MIE (prone) vs Right Thoractomy, Laparotomy, Cervical incision > 90% had modern neoadjuvant chemoradiation: carboplatin, paclitaxel, XRT Significant difference in early postoperative pulmonary complications favoring MIE 34% vs 12% in hospital No difference in LN, RO, Mortality Bierre, Lancet 2012

: Extensive MLND J Gastrointest Surg")
29 - Single-institution retrospective study of 129 patients undergoing curative-intent esophagectomy for pt1 ESCC - Group 1 (n=42): standard MLND - Group 2 (n=87): Extensive MLND J Gastrointest Surg (2017)

30 The Aurora Approach THE TEEM Trans Hiatal Esophagectomy Transcervical Endoscopic Esophageal Mobilization **Da Vinci Xi Robot-Assisted
31 THE TEEM Approach - Aurora one of few centers around the world to use this technique - Combines the oncologic advantage of transthoracic approach with the morbidity advantage of the transhiatal approach
32 Video / Graphic
33 THE TEEM Operative Data Complications Year Author Country N Abdomen OR time No of LNs Pulmonary Leak RLN Palsy LOS 30d Mort 1993 Bumm Germany 30 Open 4 (13.3%) 6 (20%) 2 (6.6%) 2 (6.6%) 2004 Tangoku Japan (24.4%) 4 (9.8%) 15 (36.6%) 2010 Wu China 40 Open 32 (80%), Lap 8 (20%) (2.5%) 3 (7.5%) 2 (5%) Parker US (Mayo Florida) 8 Laparoscopic (25%) 2 (25%) Feng China 27 Open (26%) 5 (18%) 5 (18%) (3.7%) 2014 Wang China (5.7%) 5 (7.1%) 2 (2.9%) Okumura et al Japan 63 Open (6.3%) 14 (22.2%) 6 (11.5%) 1 (1.6%) 2016 Nomura Japan 20 Open Mori Japan 22 DaVinci S for mediastinum (18%) 1 (4.5%) Fujiwara Japan (6.7%) 9 (15%) 20 (33.3%) Aurora Health Care US Aurora N= min Time Afib Leak VC Pneum Bleed 30 d mort 37% 6% 15% 7% 7% 0 Bierre, Lancet 2012
34 Thank You
35 Management of Complete response for SCC Complete pathologic response is higher in SCC than Adeno Progression free survival is better in patients treated with surgery Overall survival is not improved Cancer specific survival was improved in surgery groups? High mortality rate in surgery arm (10%)
36 Roswell Park Experience 81 patients from Endoscopic resection of T1a patients Ablation of associated Barrett s 7 patients had T1b disease (all negative margins) 3.25 years of follow up 84% eradication of HGD One patient developed invasive carcinoma Treated endoscopically 100% cancer specific survival Nurkin, Surg End 2013
37 Human epidermal growth factor (HER2) Associated with cell proliferation Amplified in 10-25% of GE Jxn cancers Trastuzumab Monoclonal antibody to HER2
38 Trastuzumab for Gastric Cancer Study (ToGA) Compared Chemotherapy +/- trastuzumab Capecitabine/fluorouracil plus cisplatin Locally advanced or Metastatic Gastric/EGJ cancers Approximately 20% were EGJ Improvements in OS, PFS ToGA, Lancet 2010
39 ToGA, Lancet 2010
40 RTOG 1010 Evaluate the addition of Trastuzumab to Neoadjuvant therapy for GE Jxn cancer Carboplatin, Paclitaxel, XRT +/- trastuzumab Anticipated 480 Enrollees Local PI: Dr. Robert Behrens
Determining the Optimal Surgical Approach to Esophageal Cancer
 Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Minimally Invasive Esophagectomy
 Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Minimally Invasive Esophagectomy M A R K B E R R Y, M D A S S O C I AT E P R O F E S S O R D E PA R T M E N T OF C A R D I O T H O R A C I C S U R G E R Y S TA N F O R D U N I V E R S I T Y S E P T E M
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Resectable locally advanced oesophagogastric cancer
 Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006
 Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006 Esophageal Cancer - Est. 15,000 cases in 2006 - Est. 14,000 deaths - Overall 5-year survival: 15.6% - 33.6 % for local
Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006 Esophageal Cancer - Est. 15,000 cases in 2006 - Est. 14,000 deaths - Overall 5-year survival: 15.6% - 33.6 % for local
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand?
 MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
MINIMALLY INVASIVE ESOPHAGECTOMY FOR CANCER: where do we stand? Ph Nafteux, MD Copenhagen, Nov 3rd 2011 Department of Thoracic Surgery, University Hospitals Leuven, Belgium W. Coosemans, H. Decaluwé, Ph.
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT
 Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
The Learning Curve for Minimally Invasive Esophagectomy
 The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
1. Epidemiology of Esophageal Cancer 2. Operative Strategies 3. Minimally Invasive Esophagectomy 4. Video
 Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Minimally Invasive Esophagectomy Guilherme M Campos, MD, FACS Assistant Professor of Surgery Director G.I. Motility Center Director Bariatric Surgery Program University of California San Francisco ESOPHAGEAL
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
7/20/2017. Esophageal Cancer: A Less Common But Deadly Cancer. Objectives. Disclosure Statement NYNPA Conference October Saratoga New York
 Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Esophageal and GEJ Adenocarcinoma: Chemo + RT is the Preferred Treatment
 Esophageal and GEJ Adenocarcinoma: Chemo + RT is the Preferred Treatment David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan-Kettering Cancer Center Preop Therapy in Esophageal and
Esophageal and GEJ Adenocarcinoma: Chemo + RT is the Preferred Treatment David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan-Kettering Cancer Center Preop Therapy in Esophageal and
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Surgical strategies in esophageal cancer
 Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
AATS Focus on Thoracic Surgery: Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017?
 AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
Robotic Surgery for Esophageal Cancer
 Robotic Surgery for Esophageal Cancer Kemp H. Kernstine, MD PhD Division of Thoracic Surgery City of Hope Medical Center and Beckman Research Institute May 1, 2010 Esophageal Cancer on the Rise JNCI 2005,
Robotic Surgery for Esophageal Cancer Kemp H. Kernstine, MD PhD Division of Thoracic Surgery City of Hope Medical Center and Beckman Research Institute May 1, 2010 Esophageal Cancer on the Rise JNCI 2005,
 Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Determining Resectability and Appropriate Surgery for Esophageal Cancer
 Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Minimally Invasive Esophagectomy
 American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
A Proposed Strategy for Treatment of Superficial Carcinoma. in the Thoracic Esophagus Based on an Analysis. of Lymph Node Metastasis
 Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
ESOPHAGEAL CANCER. Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds
 ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
intent treatment be in the elderly?
 Gastric cancer: How strong can curative intent treatment be in the elderly? Caio Max S. Rocha Lima, M.D. Professor of Medicine University of Miami & Sylvester Cancer Center Gastric cancer: epidemiology
Gastric cancer: How strong can curative intent treatment be in the elderly? Caio Max S. Rocha Lima, M.D. Professor of Medicine University of Miami & Sylvester Cancer Center Gastric cancer: epidemiology
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Updated Apr 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre)
") Local Esophageal Cancer Summary Updated Apr 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Reviewed by Dr. Yoo-Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer Centre, University
Local Esophageal Cancer Summary Updated Apr 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Reviewed by Dr. Yoo-Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer Centre, University
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD
 Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Michael A. Choti, MD, FACS Department of Surgery Johns Hopkins Medicine, Baltimore, MD Surgical Therapy of Gastric Cancer CLINICAL QUESTIONS 1. How much of the stomach should be removed? 2. How many lymph
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy
 Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Upper Gastrointestinal. Friday, March 2, :00 p.m. 2:45 p.m.
 Upper Gastrointestinal Friday, March 2, 2018 2:00 p.m. 2:45 p.m. Social Q&A Use your phone, tablet, or laptop to Submit questions to speakers and moderators Answer interactive questions / audience response
Upper Gastrointestinal Friday, March 2, 2018 2:00 p.m. 2:45 p.m. Social Q&A Use your phone, tablet, or laptop to Submit questions to speakers and moderators Answer interactive questions / audience response
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran
 Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran Institute of Clinical Cancer Research Krankenhaus Nordwest UCT - University Cancer Center
Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran Institute of Clinical Cancer Research Krankenhaus Nordwest UCT - University Cancer Center
Esophageal and GEJ Cancers. Case Presentations
 Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.
 Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.") Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
How to stage early BE cancer - EUS or endoscopic removal?
 How to stage early BE cancer - EUS or endoscopic removal? Presented by Bas Weusten Institution St. Antonius Hospital, Nieuwegein Academic Medical Center, Amsterdam case 56 y old female patient Lung transplant
How to stage early BE cancer - EUS or endoscopic removal? Presented by Bas Weusten Institution St. Antonius Hospital, Nieuwegein Academic Medical Center, Amsterdam case 56 y old female patient Lung transplant
B Breast cancer, managing risk of lobular, in hereditary diffuse gastric cancer, 51
 Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
(Neo-) adjuvant Treatment of Gastric Cancer. - The European View
 adjuvant Treatment of Gastric Cancer. - The European View") (Neo-) adjuvant Treatment of Gastric Cancer - The European View Florian Lordick, MD Professor of Oncology Director of the University Cancer Center Leipzig (UCCL) University of Leipzig, Germany My Conflict
(Neo-) adjuvant Treatment of Gastric Cancer - The European View Florian Lordick, MD Professor of Oncology Director of the University Cancer Center Leipzig (UCCL) University of Leipzig, Germany My Conflict
Towards a more personalized approach in the treatment of esophageal cancer focusing on predictive factors in response to chemoradiation Wang, Da
 University of Groningen Towards a more personalized approach in the treatment of esophageal cancer focusing on predictive factors in response to chemoradiation Wang, Da IMPORTANT NOTE: You are advised
University of Groningen Towards a more personalized approach in the treatment of esophageal cancer focusing on predictive factors in response to chemoradiation Wang, Da IMPORTANT NOTE: You are advised
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
 Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids
Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Di Lu 1#, Xiguang Liu 1#, Mei Li 1#, Siyang Feng 1#, Xiaoying Dong 1, Xuezhou Yu 2, Hua Wu 1, Gang Xiong 1, Ruijun Cai 1, Guoxin Li 3, Kaican Cai 1
 Case Report Three-port mediastino-laparoscopic esophagectomy (TPMLE) for an 81-year-old female with early-staged esophageal cancer: a case report of combining single-port mediastinoscopic esophagectomy
Case Report Three-port mediastino-laparoscopic esophagectomy (TPMLE) for an 81-year-old female with early-staged esophageal cancer: a case report of combining single-port mediastinoscopic esophagectomy
Barrett s Esophagus: Old Dog, New Tricks
 Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
Barrett s Esophagus: Old Dog, New Tricks Stuart Jon Spechler, M.D. Chief, Division of Gastroenterology, VA North Texas Healthcare System; Co-Director, Esophageal Diseases Center, Professor of Medicine,
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Esophageal Cancer: A Multimodality Approach to Detection and Staging
 Esophageal Cancer: A Multimodality Approach to Detection and Staging, MBA Topic: Esophageal Cancer Imaging: A multimodality approach Conference: Society of Thoracic Imaging Location: Date/Time: March 14,
Esophageal Cancer: A Multimodality Approach to Detection and Staging, MBA Topic: Esophageal Cancer Imaging: A multimodality approach Conference: Society of Thoracic Imaging Location: Date/Time: March 14,
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Part II. A randomized trial
 77 Part II A randomized trial 78 79 Chapter 5 Preliminary experience of minimally invasive esophagectomy for cancer. Maas KW Biere SSAY Gisbertz SS van der Peet DL M.A. Cuesta Submitted 80 Chapter 5 ABSTRACT
77 Part II A randomized trial 78 79 Chapter 5 Preliminary experience of minimally invasive esophagectomy for cancer. Maas KW Biere SSAY Gisbertz SS van der Peet DL M.A. Cuesta Submitted 80 Chapter 5 ABSTRACT
Printed by Hadi Ranjkeshzadeh on 11/12/2010 4:40:23 PM. For personal use only. Not approved for distribution. Copyright 2010 National Comprehensive
 Discussion Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform consensus. Category 2A: The recommendation
Discussion Categories of Evidence and Consensus Category 1: The recommendation is based on high-level evidence (e.g. randomized controlled trials) and there is uniform consensus. Category 2A: The recommendation
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy
 Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Priv. Doz. Dr. Dr. med. T.O. Götze Institute of Clinical Cancer Research Director: Prof. Dr. S.-E. Al- Batran University Cancer
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Priv. Doz. Dr. Dr. med. T.O. Götze Institute of Clinical Cancer Research Director: Prof. Dr. S.-E. Al- Batran University Cancer
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Determining the optimal number of lymph nodes harvested during esophagectomy
 Original Article Determining the optimal number of lymph nodes harvested during esophagectomy Khaldoun Almhanna, Jill Weber, Ravi Shridhar, Sarah Hoffe, Jonathan Strosberg, Kenneth Meredith Department
Original Article Determining the optimal number of lymph nodes harvested during esophagectomy Khaldoun Almhanna, Jill Weber, Ravi Shridhar, Sarah Hoffe, Jonathan Strosberg, Kenneth Meredith Department
VATS after induction therapy: Effective and Beneficial Tips on Strategy
 VATS after induction therapy: Effective and Beneficial Tips on Strategy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J. Swanson, M.D. Professor of
VATS after induction therapy: Effective and Beneficial Tips on Strategy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J. Swanson, M.D. Professor of
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
سرطان المعدة. Gastric Cancer حمود حامد
 سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
RTC Dec Felicitas Koller and Eric Grogan
 RTC Dec 11 2009 Felicitas Koller and Eric Grogan Cancer Statistics, United States Number of patients 200000 150000 100000 50000 0 Lung Breast New Cases Deaths Esophageal Colorectal Prostate http://www.cancer.org/statistics
RTC Dec 11 2009 Felicitas Koller and Eric Grogan Cancer Statistics, United States Number of patients 200000 150000 100000 50000 0 Lung Breast New Cases Deaths Esophageal Colorectal Prostate http://www.cancer.org/statistics
Surgery for Gastric and Oesophageal Cancer
 Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
NICE guideline Published: 24 January 2018 nice.org.uk/guidance/ng83
 Oesophago-gastric cancer: assessment and management in adults NICE guideline Published: 24 January 18 nice.org.uk/guidance/ng83 NICE 18. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Oesophago-gastric cancer: assessment and management in adults NICE guideline Published: 24 January 18 nice.org.uk/guidance/ng83 NICE 18. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness
 Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness Sunil Malhotra, M.D. Department of Surgery University of Colorado Resident Debate April 30, 2007 Esophageal Cancer
Transhiatal Esophagectomy: Lower Mortality, Diminished Morbidity, Equal Effectiveness Sunil Malhotra, M.D. Department of Surgery University of Colorado Resident Debate April 30, 2007 Esophageal Cancer
A video demonstration of the Li s anastomosis the key part of the non-tube no fasting fast track program for resectable esophageal carcinoma
 Surgical Technique A video demonstration of the the key part of the non-tube no fasting fast track program for resectable esophageal carcinoma Yan Zheng*, Yin Li*, Zongfei Wang, Haibo Sun, Ruixiang Zhang
Surgical Technique A video demonstration of the the key part of the non-tube no fasting fast track program for resectable esophageal carcinoma Yan Zheng*, Yin Li*, Zongfei Wang, Haibo Sun, Ruixiang Zhang
Lymph node metastasis is one of the most important prognostic
 ORIGINAL ARTICLE Comparison of Survival and Recurrence Pattern Between Two-Field and Three-Field Lymph Node Dissections for Upper Thoracic Esophageal Squamous Cell Carcinoma Young Mog Shim, MD, Hong Kwan
ORIGINAL ARTICLE Comparison of Survival and Recurrence Pattern Between Two-Field and Three-Field Lymph Node Dissections for Upper Thoracic Esophageal Squamous Cell Carcinoma Young Mog Shim, MD, Hong Kwan
Management of Barrett s: From Imaging to Resection
 Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
Management of Barrett s: From Imaging to Resection Michael Wallace, MD, MPH, FACG Professor of Medicine Mayo Clinic Florida Goals of Endoscopic Evaluation in Barrett s Detect Barrett s and dysplasia Reduce/eliminate
The CROSS road in neoadjuvant therapy for esophageal cancer: long-term results of CROSS trial
 Editorial The CROSS road in neoadjuvant therapy for esophageal cancer: long-term results of CROSS trial Ian Wong, Simon Law Division of Esophageal and Upper Gastrointestinal Surgery, Department of Surgery,
Editorial The CROSS road in neoadjuvant therapy for esophageal cancer: long-term results of CROSS trial Ian Wong, Simon Law Division of Esophageal and Upper Gastrointestinal Surgery, Department of Surgery,
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
FTS Oesophagectomy: minimal research to date 3,4
 Fast Track Programme in patients undergoing Oesophagectomy: A Single Centre 5 year experience Sullivan J, McHugh S, Myers E, Broe P Department of Upper Gastrointestinal Surgery Beaumont Hospital Dublin,
Fast Track Programme in patients undergoing Oesophagectomy: A Single Centre 5 year experience Sullivan J, McHugh S, Myers E, Broe P Department of Upper Gastrointestinal Surgery Beaumont Hospital Dublin,
Overall survival analysis of neoadjuvant chemoradiotherapy and esophagectomy for esophageal cancer
 Original Article Overall survival analysis of neoadjuvant chemoradiotherapy and esophagectomy for esophageal cancer Faisal A. Siddiqui 1, Katelyn M. Atkins 2, Brian S. Diggs 3, Charles R. Thomas Jr 1,
Original Article Overall survival analysis of neoadjuvant chemoradiotherapy and esophagectomy for esophageal cancer Faisal A. Siddiqui 1, Katelyn M. Atkins 2, Brian S. Diggs 3, Charles R. Thomas Jr 1,
General introduction and outline of thesis
 General introduction and outline of thesis General introduction and outline of thesis 11 GENERAL INTRODUCTION AND OUTLINE OF THESIS The incidence of esophageal cancer is increasing in the western world.
General introduction and outline of thesis General introduction and outline of thesis 11 GENERAL INTRODUCTION AND OUTLINE OF THESIS The incidence of esophageal cancer is increasing in the western world.
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Gastric Cancer: Surgery and Regional Therapy. Epidemiology. Risk factors
 Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
Gastric Cancer: Surgery and Regional Therapy Timothy J. Kennedy, MD Montefiore Medical Center Assistant Professor of Surgery Upper Gastrointestinal and Pancreas Surgery December 15, 2012 1 Epidemiology
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT
 ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy
 Anna Dorothea Wagner, PD & MER Department of Oncology University of Lausanne Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Structure 1. Background and overview 2. Adjuvant chemotherapy:
Anna Dorothea Wagner, PD & MER Department of Oncology University of Lausanne Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Structure 1. Background and overview 2. Adjuvant chemotherapy:
Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ
 Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology
Lek. Agnieszka Słowik Oddział Kliniczny Onkologii Collegium Medicum UJ 1. Introduction 2. Epidemiology 3. Gastric cancer and pancreatic cancer a. Risk factors b. Symptoms c. Location d. Diagnosis e. Histopathology
The Royal Marsden. Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon
 The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
The Royal Marsden Surgery for Gastric and GE Junction Cancer: primary palliative when and where? William Allum Consultant Surgeon Any surgeon can cure Surgeon - dependent No surgeon can cure EMR D2 GASTRECTOMY
RFA and Cyrotherapy for Esophageal Disease
 RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
RFA and Cyrotherapy for Esophageal Disease Daniel L. Miller MD Chief, General Thoracic Surgery WellStar Healthcare System/ Mayo Clinic Care Network Clinical Professor of Surgery Medical College of Georgia/
WHO BENEFITS FROM ADJUVANT CHEMOTHERAPY RADIATION CHEMORADIATION? Dr. Paul Gardiner April 23, 2001 Discipline of Surgery Grand Rounds
 WHO BENEFITS FROM ADJUVANT CHEMOTHERAPY RADIATION CHEMORADIATION? Dr. Paul Gardiner April 23, 2001 Discipline of Surgery Grand Rounds LUNG Dr. Greenland ESOPHAGUS Dr. Gardiner ESOPHAGEAL CANCER 1200 new
WHO BENEFITS FROM ADJUVANT CHEMOTHERAPY RADIATION CHEMORADIATION? Dr. Paul Gardiner April 23, 2001 Discipline of Surgery Grand Rounds LUNG Dr. Greenland ESOPHAGUS Dr. Gardiner ESOPHAGEAL CANCER 1200 new
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Dr. Andres Wiernik. Lung Cancer
 Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
Dr. Andres Wiernik Lung Cancer Lung Cancer Facts - Demographics World Incidence: 1 8 million / year World Mortality: 1 6 million / year 5-year survival rates vary from 4 17% depending on stage and regional
Getting to the Bottom of Treatment: An Update in the Management of Esophagogastric Cancers
 Getting to the Bottom of Treatment: An Update in the Management of Esophagogastric Cancers Disclosures None Cindy L. O Bryant, PharmD, BCOP, FCCP, FHOPA Professor, University of Colorado Skaggs School
Getting to the Bottom of Treatment: An Update in the Management of Esophagogastric Cancers Disclosures None Cindy L. O Bryant, PharmD, BCOP, FCCP, FHOPA Professor, University of Colorado Skaggs School
Esophageal and Esophagogastric Junction Cancers
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Esophageal and Esophagogastric Junction Cancers Version 3.2015 NCCN.org NCCN Guidelines for Patients available at www.nccn.org/patients
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Esophageal and Esophagogastric Junction Cancers Version 3.2015 NCCN.org NCCN Guidelines for Patients available at www.nccn.org/patients
Stenting for Esophageal Cancer Technical Issues and Outcomes
 Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Stenting for Esophageal Cancer Technical Issues and Outcomes Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Disclosures Research and Educational
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
The incidence of esophageal carcinoma has increased
 The Best Operation for Esophageal Cancer? Arjun Pennathur, MD, Jie Zhang, MD, Haiquan Chen, MD, and James D. Luketich, MD Heart, Lung, and Esophageal Surgery Institute, University of Pittsburgh Medical
The Best Operation for Esophageal Cancer? Arjun Pennathur, MD, Jie Zhang, MD, Haiquan Chen, MD, and James D. Luketich, MD Heart, Lung, and Esophageal Surgery Institute, University of Pittsburgh Medical
Lymph node invasion might have more prognostic impact than R status in advanced esophageal adenocarcinoma
 The American Journal of Surgery (2013) 205, 711-717 Clinical Surgery Lymph node invasion might have more prognostic impact than R status in advanced esophageal adenocarcinoma Magali Cabau, M.D. a, Guillaume
The American Journal of Surgery (2013) 205, 711-717 Clinical Surgery Lymph node invasion might have more prognostic impact than R status in advanced esophageal adenocarcinoma Magali Cabau, M.D. a, Guillaume
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
Upper Gastrointestinal Cancers in the Elderly. Choo Su Pin Senior Consultant Medical Oncology National Cancer Centre Singapore
 Upper Gastrointestinal Cancers in the Elderly Choo Su Pin Senior Consultant Medical Oncology National Cancer Centre Singapore Gastric Cancer --High Global Burden Global Cancer Deaths % of all cancer (2008)
Upper Gastrointestinal Cancers in the Elderly Choo Su Pin Senior Consultant Medical Oncology National Cancer Centre Singapore Gastric Cancer --High Global Burden Global Cancer Deaths % of all cancer (2008)