RTC Dec Felicitas Koller and Eric Grogan
|
|
|
- Annabel Hudson
- 6 years ago
- Views:
Transcription

1 RTC Dec Felicitas Koller and Eric Grogan
2 Cancer Statistics, United States Number of patients Lung Breast New Cases Deaths Esophageal Colorectal Prostate Histology
3 Squamous Cell Worldwide >>> < Men vs. Women Age Disease Association Location Adenocarcinoma 3:1 (fifth decade) 15:1 (fifth decade) Rarely <30; mortality greatest in men Exposure to environmental factors; smoking, ETOH, pickled/smoked; deficiencies; tylosis, Plummer Vinson syndrome; end stage achalasia Squamous tissue in upper and middle third Rarely < 40, incidence increases with age Barrett s 40 fold increase Submucosal glands of esophagus; heterotopic islands of columnar epithelium; malignant degeneration of metaplastic columnar epithelium Survival 70% with polypoid; 15% advanced Nature Sensitive to chemotherapy Embedded in Barrett's esophagus, less sensitive to chemotherapy

4 Commences at C6 joins stomach at T11, usually cm long. 2.5 cm in diameter Structures: distance from incisors 13 cm cricopharyngeus 22 cm azygous vein 22 27cm carina 40 cm EG junction


5 The Layers at?? The esophagus lacks a serosa: mucosa, submucosa and muscularis propria Two interconnecting lymphatic plexuses arising from the submucosa and muscularis layers.


 The gastroesophageal fat pad")
6 GE junction at?? Endoscopically: The squamocolumnar epithelial junction (Zline) The transition from the smooth esophageal lining to the rugal folds of the stomach Externally: The collar of Helvetius (or loop of Willis) The gastroesophageal fat pad are consistent identifiers of the GEJ
7 Case Presentation 3/24/09 CC: 73 yo man with a 2 month history of progressive difficulty with swallowing. Solid foods pass the upper esophagus with some difficulty. Has no lodging, but has to drink more water No hx of esophagitis or stricture HTN, HLD, BPH, hx. of arrhythmia PSH: Anterior neck fusion WHAT ADDITIONAL HISTORY? Smoking, drinking, anemia, GERD or GERD sx, foul breath, regurgitation of food, hx of chemical or radiation exposure, medications DIFFERENTIAL DX? Obstructive lesions: tumors, inflammatory masses; Zenker's diverticulum, esophageal webs mediastinal masses,cervical spondylosis, radiation, chemical or medication induced; Schatzki's Ring, vascular compression, enlarged aorta or left atrium, aberrant vessels, lymphadenopathy, substernal thyroid Neuromuscular disorders: achalasia; DES, Hypertensive LES, nutcracker esophagus, scleroderma INITIAL TEST? Barium Swallow Why? both functional and anatomic.



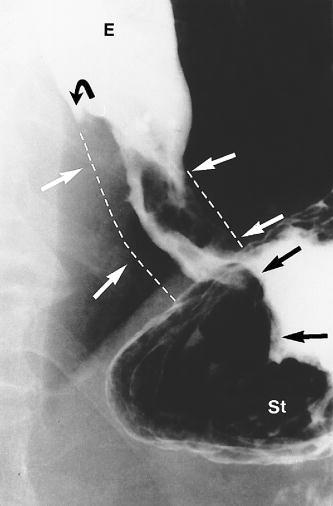
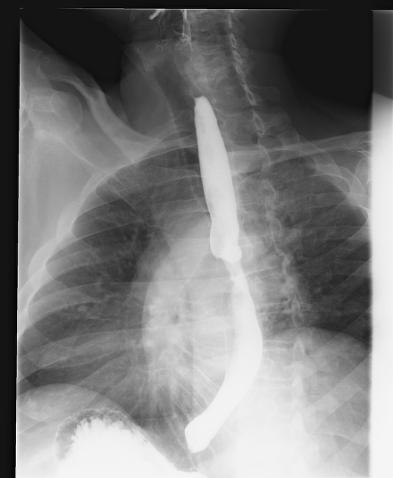
8 A B C D
9 1. A=nutcracker esophagus, B=cancer C=achalasia, D= cancer 2. A=Schatzki s ring, B=cancer, C=normal, D=Barrett s esophagus 3. A=reflux, B=compression from mediastinal mass, C= normal, D=achalasia 4. A=diffuse esophageal spasm, B=Zenker s diverticulum, c=normal, d=cancer


10
11 EGD with biopsy tissue 1. Location (w/ respect to incisors) 2. Nature of the lesion 3. Proximal and distal extent of the lesion 4. Relationship of the lesion to the cricop., GEJ, cardia 5. Distensibility of the stomach CT scan thorax length of the tumor, thickness of the esophagus and stomach, lymph node status and distant disease to the liver and lungs PET scan primary mass, regional lymph nodes and distant disease Esophageal ultrasound depth of the tumor, the length of the tumor, the degree of luminal compromise, the status of regional lymph nodes, and involvement of adjacent structures

12 EGD: 6 7 mm, 3cm long, 28 cm from the incisors. Patchy antral erythema, normal duodenum Pathology: invasive moderately differentiated squamous cell carcinoma, vascular invasion CT: focal mid esophageal wall thickening, no adenopathy PET: intense focal FDG activity in the mid thoracic esophagus immediately posterior to the left mainstem bronchus. 3 FDG avid nodules: r of midline at the same level, subcarinal and right paratracheal
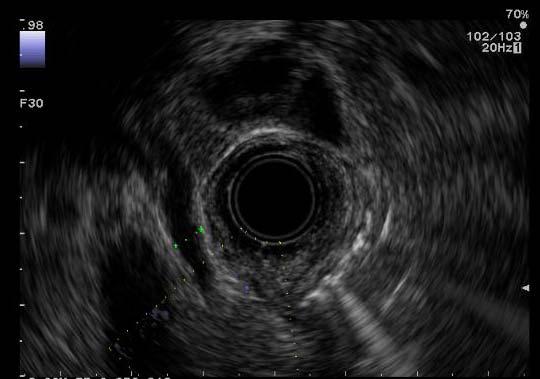
, represents the submucosa. 4 th hypoechoic (black), represents the muscularis propria. 5 th hyperechoic (white) is the periesophageal tissue.")
13 1 ST hyperechoic (white), represents the superficial mucosa (epithelium and lamina propria). 2 nd hypoechoic (black), represents the deep mucosa (muscularis mucosa). 3 rd hyperechoic (white), represents the submucosa. 4 th hypoechoic (black), represents the muscularis propria. 5 th hyperechoic (white) is the periesophageal tissue.


14 A, A T1 lesion is observed as a hypoechoic thickening of the mucosal layer adjacent to the normal appearing wall pattern; B, a T2 lesion is seen as a hypoechoic mass invading into but not through the muscularis propria

15
16 T2 N1 by EUS What s his stage What are his treatment options

17 Tumor Nodes Metastasis TX: Primary tumor cannot be assessed NX: Regional lymph nodes cannot be assessed MX: Distant metastasis cannot be assessed T0: No evidence of primary tumor N0: No regional lymph node metastasis M0: No distant metastasis Tis: Carcinoma in situ N1: Regional lymph node metastasis M1: Distant metastasis Tumors of the lower thoracic esophagus: M1a: Metastasis in celiac lymph nodes M1b: Other distant metastasis Tumors of the midthoracic esophagus: M1a: Not applicable M1b: Nonregional lymph nodes and/or other distant metastasis Tumors of the upper thoracic esophagus: M1a: Metastasis in cervical nodes M1b: Other distant metastasis T1: Tumor invades lamina propria or submucosa T2: Tumor invades muscularis propria T3: Tumor invades adventitia T4: Tumor invades adjacent structures

18 Stage 0 Stage 1 Stage 2 Stage 3 Stage 4 Tis, N0, M0 T1, N0, M0 Stage IIA T2, N0, M0 T3, N0, M0 T3, N1, M0 T4, any N, Any T, any N, M1 Stage IIB T1, N1, M0 T2, N1, M0 Stage IVA Any T, any N, M1a Stage IVB Any T, any N, M1b
19 1. Surgery alone 2. Surgery adjuvant chemo 3. Chemoradiation alone 4. Neoadjuvant chemoradiation and then surgery
20 Case Presentation 4/2009 6/2009 Patient receives neoadjuvant chemotherapy (cisplatin and capecitibine) as well as radiotherapy. Repeat PET imaging shows : 1.Decreased LN size with loss of FDG activity. 2.In the middle esophagus right below the carina, moderate FDG activity is seen associated with residual esophageal wall thickness. On previous scan, this was primary site of the cancer with intense FDG uptake and significant esophageal wall thickness. EGD: 1.UES was located at 19 cm from insertion, and the GE junction was located at 41 cm from insertion cm from insertion there was a partially circumferential superficial ulcer with scar tissue. There were proximal esophageal plaques consistent with candidal esophagitis. There was no Barrett's. Stomach: normal Duodenum: normal
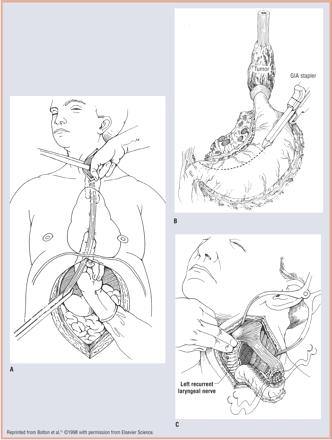
21 Transhiatal Transthoracic (Ivor Lewis) Three field (McKeown) Minimally invasive
22 Approach / Incisions Transhiatal Transthoracic Minimally invasive Conduit Stomach Colon Jejunum, supercharged Other Anastamosis Neck Chest Route Posterior mediastinum Retrosternal Subcutaneous
23 Case Presentation JI underwent operation 7/28/09: 1. Bronchoscopy. 2. Esophagogastroduodenoscopy. 3. Laparotomy with transthoracic esophagectomy. 4. Jejunostomy feeding tube. 5. Ligation of thoracic duct. 6. Pyloroplasty Pathology: 1) ESOPHAGUS AND STOMACH, DISTAL ESOPHAGECTOMY: LIMITED RESIDUAL SQUAMOUS CELL CARCINOMA, DISTAL ESOPHAGUS, IN SUBMUCOSA AND MUSCULARIS PROPRIA, 1.8 MM IN GREATEST EXTENT; PRESENT IN A BACKGROUND OF SEVERE MUCOSAL AND SUBMUCOSAL ULCERATION; ALL SURGICAL MARGINS WIDELY FREE OF CARCINOMA; TWO LYMPH NODES NEGATIVE FOR MALIGNANCY (0/2), (SEE COMMENT). 2) LYMPH NODES, LEVEL 7, EXCISION: 3 LYMPH NODES NEGATIVE FOR MALIGNANCY (0/3). COMMENT: These findings correspond to AJCC pathologic stage yiia (ypt2n0m n/a).

24 No difference in operative time, blood loss, morbidity or mortality Survival similar Anastomotic Leak rate Cervical 11% Thoracic 6% Putnam et al., Ann Thor Surg,, 1994
25
26
27 Identified endoscopically Resection, mediastinal debridement Diversion, delayed reconstruction 50% mortality

28 Smoking cessation Enteral nutrition in pts undergoing induction tx Epidural anesthesia Bronchopulmonary hygiene Early extubation No difference between TTE and THE
29 Incidence 1 3% (TTE=THE) Suspected with high continued CT output Pleural triglycerides, lymphocytes, chylomicrons Most will not close with conservative management
30 Non operative stratagies NPO, TPN ±octreotide MCT diet ± octreotide IR embolization of thoracic duct Operative ligation VATS vs. open
Quiz Adenocarcinoma of the distal stomach has been increasing in the last 20 years. a. True b. False
 Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Quiz 1 1. Which of the following are risk factors for esophagus cancer. a. Obesity b. Gastroesophageal reflux c. Smoking and Alcohol d. All of the above 2. Adenocarcinoma of the distal stomach has been
Case Scenario year-old white male presented to personal physician with dyspepsia with reflux.
 Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1 57-year-old white male presented to personal physician with dyspepsia with reflux. 7/12 EGD: In the gastroesophageal junction we found an exophytic tumor. The tumor occupies approximately
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
ESOPHAGEAL CANCER AND GERD. Prof Salman Guraya FRCS, Masters MedEd
 ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
ESOPHAGEAL CANCER AND GERD Prof Salman Guraya FRCS, Masters MedEd Learning objectives Esophagus anatomy and physiology Esophageal cancer Causes, presentations of esophageal cancer Diagnosis and management
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012
 Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Aliu Sanni MD SUNY Downstate Medical Center August 16, 2012 Case Presentation 60yr old AAF with PMH of CAD s/p PCI 1983, CVA, GERD, HTN presented with retrosternal chest pain on 06/12 Associated dysphagia
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications
 and Clinicoradiologic Implications") Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
Esophageal Cancer Staging Essentials: The New TNM Staging System (7th edition) and Clinicoradiologic Implications Poster No.: E-0060 Congress: ESTI 2012 Type: Scientific Exhibit Authors: K. Lee, T. J.
SETTING Fudan University Shanghai Cancer Center. RESPONSIBLE PARTY Haiquan Chen MD.
 OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
OFFICIAL TITLE A Phase Ⅲ Study of Left Side Thoracotomy Approach (SweetProcedure) Versus Right Side Thoracotomy Plus Midline Laparotomy Approach (Ivor-Lewis Procedure) Esophagectomy in Middle or Lower
 Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
Surgical Management of Esophageal Cancer Sophia L Fu, MD Long Island College Hospital SUNY Downstate Medical Center, Brooklyn, NY 03/27/2009 Questions The T and N status of esophageal carcinoma is most
 Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids
Lya Crichlow, MD Kings County Hospital Center September 3, 2009 Morbidity and Mortality Conference Case presentation 56 year old male who presented with 1 week history of dysphagia Unable to tolerate solids
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 Final Pathology:
 Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
Abstracting Upper GI Cancer Incidence and Treatment Data Quiz 1 Multiple Primary and Histologies Case 1 A 74 year old male with a history of GERD presents complaining of dysphagia. An esophagogastroduodenoscopy
01/26/2010 GENERAL SURGERY ABSITE ANATOMY ANATOMY. Yvonne M. Carter, MD Georgetown University Medical Center. Layers. mucosa. squamous epithelium
 GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
GENERAL SURGERY ABSITE REVIEW: ESOPHAGUS Yvonne M. Carter, MD Georgetown University Medical Center ANATOMY Layers mucosa muscle squamous epithelium columnar epithelium (distal 2cm) inner = circular outer
7/20/2017. Esophageal Cancer: A Less Common But Deadly Cancer. Objectives. Disclosure Statement NYNPA Conference October Saratoga New York
 Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
Esophageal Cancer: A Less Common But Deadly Cancer 2017 NYNPA Conference October 18-22 Saratoga New York Mary McGreal DNP, RN, ANP-C, CCRN, CMC, Adjunct Professor at Stony Brook University School of Nursing
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma
 Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Tumours of the Oesophagus & Gastro-Oesophageal Junction Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given
Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD
 Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
Esophagus Anatomy/Physiology Gastroesophageal reflux disease Principles of GERD treatment Treatment of reflux diseases GERD Manometry Question 50 years old female with chest pain and dysphagia. Manometry
Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006
 Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006 Esophageal Cancer - Est. 15,000 cases in 2006 - Est. 14,000 deaths - Overall 5-year survival: 15.6% - 33.6 % for local
Minimally Invasive Esophagectomy: OVERRATED!!! Sagar Damle UCHSC December 11, 2006 Esophageal Cancer - Est. 15,000 cases in 2006 - Est. 14,000 deaths - Overall 5-year survival: 15.6% - 33.6 % for local
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines. Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center
 Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
Management of Esophageal Cancer: Evidence Based Review of Current Guidelines Madhuri Rao, MD PGY-5 SUNY Downstate Medical Center Case Presentation 68 y/o male PMH: NIDDM, HTN, hyperlipidemia, CAD s/p stents,
The Learning Curve for Minimally Invasive Esophagectomy
 The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
The Learning Curve for Minimally Invasive Esophagectomy AATS Focus on Thoracic Surgery Mastering Surgical Innovation Las Vegas Nevada Oct. 27-28 2017 Scott J Swanson, M.D. Professor of Surgery Harvard
Determining the Optimal Surgical Approach to Esophageal Cancer
 Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Determining the Optimal Surgical Approach to Esophageal Cancer Amit Bhargava, MD Attending Thoracic Surgeon Department of Cardiovascular and Thoracic Surgery Open Esophagectomy versus Minimally Invasive
Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
THORACIC SURGERY: Dysphagia. Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone. Thoracic Surgery Toronto East General Hospital
 THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
THORACIC SURGERY: Dysphagia Dr. Robert Zeldin Dr. John Dickie Dr. Carmine Simone Thoracic Surgery Toronto East General Hospital Objectives Definitions Common causes Investigations Treatment options Anatomy
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP. Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D.
 A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
A Multidisciplinary Approach to Esophageal Dysphagia: Role of the SLP Darlene Graner, M.A., CCC-SLP, BRS-S Sharon Burton, M.D. What is the role of the SLP? Historically SLPs the preferred providers for
A Proposed Strategy for Treatment of Superficial Carcinoma. in the Thoracic Esophagus Based on an Analysis. of Lymph Node Metastasis
 Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
Kitakanto Med J 2002 ; 52 : 189-193 189 A Proposed Strategy for Treatment of Superficial Carcinoma in the Thoracic Esophagus Based on an Analysis of Lymph Node Metastasis Susumu Kawate,' Susumu Ohwada,'
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
9/18/2015. Disclosures. Objectives. Dysphagia Sherri Ekobena PA-C. I have no relevant financial interests to disclose I have no conflicts of interest
 Dysphagia Sherri Ekobena PA-C Disclosures I have no relevant financial interests to disclose I have no conflicts of interest Objectives Define what dysphagia is Define types of dysphagia Define studies
Dysphagia Sherri Ekobena PA-C Disclosures I have no relevant financial interests to disclose I have no conflicts of interest Objectives Define what dysphagia is Define types of dysphagia Define studies
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours?
 Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Surgical Problems in Proximal GI Cancer Management Cardia Tumours Question #1: What are cardia tumours? Question #2: How are cardia tumours managed? Michael F. Humer December 3, 2005 Vancouver, BC Case
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Determining Resectability and Appropriate Surgery for Esophageal Cancer
 Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
Determining Resectability and Appropriate Surgery for Esophageal Cancer Peter Baik, DO, FACOS Thoracic Surgery Cancer Treatment Centers of America 1 Esophageal and Esophagogastric Junction Cancers Siewert
AATS Focus on Thoracic Surgery: Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017?
 AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
AATS Focus on Thoracic Surgery: Mastering Surgical Innovation Las Vegas, NV October 28, 2017 Session VIII: Video Session Minimally Invasive Esophagectomy: Are We Still Getting Better in 2017? James D.
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.
 Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C.") Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
Endoscopic UltraSound (EUS) Endoscopic Mucosal Resection (EMR) Moishe Liberman Director C.E.T.O.C. Division of Thoracic Surgery Centre Hospitalier de l Université de Montréal Research Grants: Disclosures
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010
 LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
LSU HEALTH SCIENCES CENTER NSCLC Guidelines Feist-Weiller Cancer Center Molly Boyd, MD Glenn Mills, MD Syed Jafri, MD 1/1/2010 Initial Evaluation/Intervention: 1. Pathology Review 2. History and Physical
A218 : Esophagus cancer tissues. (formalin fixed)
") (formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
(formalin fixed) For research use only Specifications: No. of cases: 40 Tissue type: Esophagus cancer tissues No. of spots: 2 spots from each cancer case (80 spots) 4 non-neoplastic spots (4 spots) Total
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
ESOPHAGEAL CANCER. Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds
 ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
ESOPHAGEAL CANCER Dr. Paul Gardiner December 17, 2002 Discipline of Surgery Rounds ESOPHAGEAL CANCER I. EPIDEMIOLOGY INCIDENCE, DIAGNOSIS & STAGING II. TREATMENT OPTIONS Current role of induction therapies
An Update: Lung Cancer
 An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
An Update: Lung Cancer Andy Barlow Consultant in Respiratory Medicine Lead Clinician for Lung Cancer (West Herts Hospitals NHS Trust) Lead for EBUS-Harefield Hospital (RB&HFT) Summary Lung cancer epidemiology
Esophageal Cancer: A Multimodality Approach to Detection and Staging
 Esophageal Cancer: A Multimodality Approach to Detection and Staging, MBA Topic: Esophageal Cancer Imaging: A multimodality approach Conference: Society of Thoracic Imaging Location: Date/Time: March 14,
Esophageal Cancer: A Multimodality Approach to Detection and Staging, MBA Topic: Esophageal Cancer Imaging: A multimodality approach Conference: Society of Thoracic Imaging Location: Date/Time: March 14,
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Mediastinal Staging. Samer Kanaan, M.D.
 Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Mediastinal Staging Samer Kanaan, M.D. Overview Importance of accurate nodal staging Accuracy of radiographic staging Mediastinoscopy EUS EBUS Staging TNM Definitions T Stage Size of the Primary Tumor
Gastric Cancer in a Young Postpartum Female. Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012
 Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
Gastric Cancer in a Young Postpartum Female Kings County Hospital Center SUNY Downstate Case Conference May 24, 2012 Case HPI: 31 yo F, G5P3, 3 weeks s/p C-section, with gastric outlet obstruction. Pt
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Surgical strategies in esophageal cancer
 Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
Gastro-Conference Berlin 2005 October 1-2, 2005 Surgical strategies in esophageal cancer J. Rüdiger Siewert Department of Surgery, Klinikum rechts der Isar Technische Universität München Esophageal Cancer
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
WHO BENEFITS FROM ADJUVANT CHEMOTHERAPY RADIATION CHEMORADIATION? Dr. Paul Gardiner April 23, 2001 Discipline of Surgery Grand Rounds
 WHO BENEFITS FROM ADJUVANT CHEMOTHERAPY RADIATION CHEMORADIATION? Dr. Paul Gardiner April 23, 2001 Discipline of Surgery Grand Rounds LUNG Dr. Greenland ESOPHAGUS Dr. Gardiner ESOPHAGEAL CANCER 1200 new
WHO BENEFITS FROM ADJUVANT CHEMOTHERAPY RADIATION CHEMORADIATION? Dr. Paul Gardiner April 23, 2001 Discipline of Surgery Grand Rounds LUNG Dr. Greenland ESOPHAGUS Dr. Gardiner ESOPHAGEAL CANCER 1200 new
Patient. Male 76 year old C.C: abdominal pain
 Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer
 THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
THIS DOCUMENT IS North of Scotland Cancer Network Clinical Management Guideline for Non Small Cell Lung Cancer [Based on WOSCAN NSCLC CMG with further extensive consultation within NOSCAN] UNCONTROLLED
Oesophageal Cancer: The Image after Surgery
 Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Diagnosis and Preoperative Staging of Esophageal Cancer
 2 Diagnosis and Preoperative Staging of Esophageal Cancer ARNOLD J. MARKOWITZ, MD HANS GERDES, MD The clinical presentation of esophageal cancer in the United States and Europe has been changing, but unfortunately,
2 Diagnosis and Preoperative Staging of Esophageal Cancer ARNOLD J. MARKOWITZ, MD HANS GERDES, MD The clinical presentation of esophageal cancer in the United States and Europe has been changing, but unfortunately,
Oesophageal Cancer: The Image after Surgery
 Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Oesophageal Cancer: The Image after Surgery Poster No.: C-2253 Congress: ECR 2014 Type: Educational Exhibit Authors: A. Loureiro, N. V. V. B. Marques, M. Palmeiro, P. Pereira, 1 1 1 1 2 1 1 2 1 R. Gil,
Slide 1. Slide 2. Slide 3. Investigation and management of lung cancer Robert Rintoul. Epidemiology. Risk factors/aetiology
 Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Slide 1 Investigation and management of lung cancer Robert Rintoul Department of Thoracic Oncology Papworth Hospital Slide 2 Epidemiology Second most common cancer in the UK (after breast). 38 000 new
Minimally Invasive Esophagectomy
 American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
American Association of Thoracic Surgery (AATS) 95 th Annual Meeting Seattle, WA April 29, 2015 General Thoracic Masters of Surgery Video Session Minimally Invasive Esophagectomy James D. Luketich MD,
Esophagus Stomach 4/2/15
 Collecting Cancer Data: Esophagus & Stomach 2014-2015 NAACCR Webinar Series April 2, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Esophagus & Stomach 2014-2015 NAACCR Webinar Series April 2, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012
 Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012 Esophageal Leiomyoma Introduction Case presentation Operative video Discussion Esophageal Leiomyoma Benign tumors of the
Hong Kong Society of Upper Gastrointestinal Surgeons CLINICAL MEETING 29 NOV 2012 Esophageal Leiomyoma Introduction Case presentation Operative video Discussion Esophageal Leiomyoma Benign tumors of the
Faculty Disclosure. Objectives. State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) 24/11/2014
 24/11/2014") State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
State of the Art #3: Referrals for Gastroscopy (focus on common esophagus problems) Dr. Amy Morse November 2014 Faculty: Amy Morse Faculty Disclosure Relationships with commercial interests: Grants/Research
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Esophageal Cancer. Source: National Cancer Institute
 Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
Esophageal Cancer Esophageal cancer forms in the tissues that line the esophagus, or the long, hollow tube that connects the mouth and stomach. Food and drink pass through the esophagus to be digested.
GALLBLADDER CANCER. Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011
 GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
GALLBLADDER CANCER Lidie M. Lajoie MD Downstate Surgery M&M July 21, 2011 Agenda Case Presentation Epidemiology Pathogenesis & Pathology Staging Presentation & Diagnosis Stage-wise Management Outcomes/Prognosis
Esophageal cancer: Biology, natural history, staging and therapeutic options
 EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
EGEUS 2nd Meeting Esophageal cancer: Biology, natural history, staging and therapeutic options Michael Bau Mortensen MD, Ph.D. Associate Professor of Surgery Centre for Surgical Ultrasound, Upper GI Section,
UCLA General Surgery Residency Program Rotation Educational Policy Goals and Objectives
 UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
UPDATED: July 2009 ROTATION: THORACIC SURGERY UCLA General Surgery Residency Program ROTATION DIRECTOR: Mary Maish, M.D. CHIEF OF CARDIAC SURGERY: Robert Cameron, M.D. SITES: UCLA Medical Center - Westwood
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia
 National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
National Oesophago-Gastric Cancer Audit New Patient Registration sheet Patients with Oesophageal High Grade Glandular Dysplasia Patient Details Surname: NHS number: Forename: Postcode: Sex: Male Female
Robotic Surgery for Esophageal Cancer
 Robotic Surgery for Esophageal Cancer Kemp H. Kernstine, MD PhD Division of Thoracic Surgery City of Hope Medical Center and Beckman Research Institute May 1, 2010 Esophageal Cancer on the Rise JNCI 2005,
Robotic Surgery for Esophageal Cancer Kemp H. Kernstine, MD PhD Division of Thoracic Surgery City of Hope Medical Center and Beckman Research Institute May 1, 2010 Esophageal Cancer on the Rise JNCI 2005,
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition
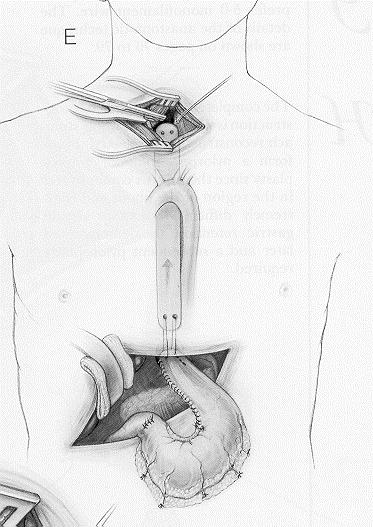
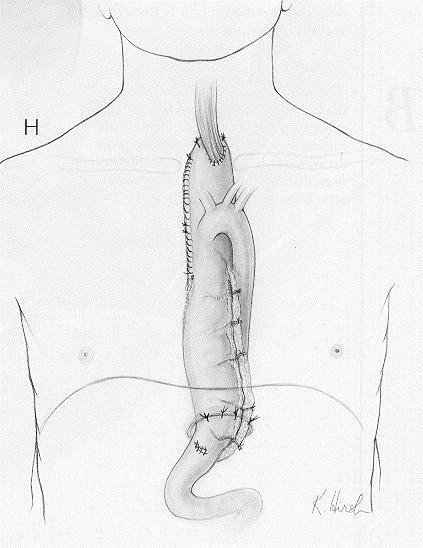
 22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
22 Limited en bloc Resection of the Gastroesophageal Junction with Isoperistaltic Jejunal Interposition J.R. Izbicki, W.T. Knoefel, D. C. Broering ] Indications Severe dysplasia in the distal esophagus
Esophageal Diverticulum. Ahmed Hozain, PGY III Kings County Hospital University Hospital of Brooklyn, Surgery Grand Rounds May 18 th, 2017
 Esophageal Diverticulum Ahmed Hozain, PGY III Kings County Hospital University Hospital of Brooklyn, Surgery Grand Rounds May 18 th, 2017 Case Presentation 53 YOF presented to KCHC with sx of dysphagia
Esophageal Diverticulum Ahmed Hozain, PGY III Kings County Hospital University Hospital of Brooklyn, Surgery Grand Rounds May 18 th, 2017 Case Presentation 53 YOF presented to KCHC with sx of dysphagia
Carcinoma of the Renal Pelvis and Ureter Histopathology
 Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1. January 06, 2012
 PATHOLOGY LAB #1. January 06, 2012") MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS GASTROINTESTINAL (GI) PATHOLOGY LAB #1 GOAL: January 06, 2012 Faculty Copy 1. Describe the basis morphologic and pathophysiologic changes which occur in
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
History. Prevalence at Endoscopy. Prevalence and Reflux Sx. Prevalence at Endoscopy. Barrett s Esophagus: Controversy and Management
 Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Barrett s Esophagus: Controversy and Management History Norman Barrett (1950) Chronic Peptic Ulcer of the Oesophagus and Oesophagitis Allison and Johnstone (1953) The Oesophagus Lined with Gastric Mucous
Esophagus and Esophagogastric Junction
 Esophagus and Esophagogastric Junction 16 Thomas William Rice, David Kelsen, Eugene H. Blackstone, Hemant Ishwaran, Deepa T. Patil, Adam J. Bass, Jeremy J. Erasmus, Hans Gerdes, and Wayne L. Hofstetter
Esophagus and Esophagogastric Junction 16 Thomas William Rice, David Kelsen, Eugene H. Blackstone, Hemant Ishwaran, Deepa T. Patil, Adam J. Bass, Jeremy J. Erasmus, Hans Gerdes, and Wayne L. Hofstetter
Medical Science DR JITENDRA TADGHARE DR BEENA VAIDYA DR MILAN SNEHKUNJ DR HARISINH PARMAR DR GAURAV BAVADIYA DR DEEP PARMAR.
 Retrospective Study of Surgical Management of Carcinoma Esophagus By Orringer s 2 Phase Transhiatal Versus Mc Evans 3 Phase Esophagectomy (Study of 25 Cases Each). Medical Science KEYWORDS : Carcinoma
Retrospective Study of Surgical Management of Carcinoma Esophagus By Orringer s 2 Phase Transhiatal Versus Mc Evans 3 Phase Esophagectomy (Study of 25 Cases Each). Medical Science KEYWORDS : Carcinoma
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Surgery for Gastric and Oesophageal Cancer
 Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
Surgery for Gastric and Oesophageal Cancer Trends in cancer mortality, England and Wales SMR base 1980 Oesophago-Gastric Cancer The National Problem 5 th commonest malignancy 4 th commonest cause of death
A 16 yr old boy with aggressive ca esophagus. DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health
 A 16 yr old boy with aggressive ca esophagus DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health Cancer of esophagus in a 16yr old Y.N 16 yr old boy unwell
A 16 yr old boy with aggressive ca esophagus DR Ayunga A.O Physician-Garisa PGH Associate Faculty Lecturer-UON Afya Bora Fellow in Global Health Cancer of esophagus in a 16yr old Y.N 16 yr old boy unwell
Esophageal Cancer. What is esophageal cancer?
 Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
Scan for mobile link. Esophageal Cancer Esophageal cancer occurs when cancer cells develop in the esophagus. The two main types are squamous cell carcinoma and adenocarcinoma. Esophageal cancer may not
Role of Surgery in Management of Non Small Cell Lung Cancer. Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City
 Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Role of Surgery in Management of Non Small Cell Lung Cancer Dr. Ahmed Bamousa Consultant thoracic surgery Prince Sultan Military Medical City Introduction Surgical approach Principle and type of surgery
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Charles Mulligan, MD, FACS, FCCP 26 March 2015
 Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Charles Mulligan, MD, FACS, FCCP 26 March 2015 Review lung cancer statistics Review the risk factors Discuss presentation and staging Discuss treatment options and outcomes Discuss the status of screening
Vesalius SCALpel : Esophagus (see also: esophageal folios) Anatomy/physiology
 Anatomy/physiology") Vesalius SCALpel : Esophagus (see also: esophageal folios) Anatomy/physiology upper 1/3 straited, lower 2/3 smooth muscle LN drainage: upper: paratracheal, supraclavicular lower: subcarinal, inferior pulmonary
Vesalius SCALpel : Esophagus (see also: esophageal folios) Anatomy/physiology upper 1/3 straited, lower 2/3 smooth muscle LN drainage: upper: paratracheal, supraclavicular lower: subcarinal, inferior pulmonary
42 yr old male with h/o Graves disease and prior I 131 treatment presents with hyperthyroidism and undetectable TSH. 2 hr uptake 20%, 24 hr uptake 50%
 Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Pinhole images of the neck are acquired in multiple projections, 24hrs after the oral administration of approximately 200 µci of I123. Usually, 24hr uptake value if also calculated (normal 24 hr uptake
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Bronchogenic Carcinoma
 A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
A 55-year-old construction worker has smoked 2 packs of ciggarettes daily for the past 25 years. He notes swelling in his upper extremity & face, along with dilated veins in this region. What is the most
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
Esophageal and GEJ Cancers. Case Presentations
 Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
[A RESEARCH COORDINATOR S GUIDE]
![[A RESEARCH COORDINATOR S GUIDE]](/thumbs/88/117127924.jpg "[A RESEARCH COORDINATOR S GUIDE]") 2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
The present staging system for esophageal carcinoma
 Esophageal Carcinoma: Depth of Tumor Invasion Is Predictive of Regional Lymph Node Status Thomas W. Rice, MD, Gregory Zuccaro, Jr, MD, David J. Adelstein, MD, Lisa A. Rybicki, MS, Eugene H. Blackstone,
Esophageal Carcinoma: Depth of Tumor Invasion Is Predictive of Regional Lymph Node Status Thomas W. Rice, MD, Gregory Zuccaro, Jr, MD, David J. Adelstein, MD, Lisa A. Rybicki, MS, Eugene H. Blackstone,
Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread
 Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
Esophagus Anatomy: From cricoid cartilage to diaphragm 25 Cms. 4 portions: Cervical 5 cms. Thoracic 25 cms. Abdominal 2 cms. Blood supply Lymphatic spread Upper 2/3 Cephalad Lower 1/3 Caudad Physiology:
Barrett s Esophagus. Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI
 Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Barrett s Esophagus Abdul Sami Khan, M.D. Gastroenterologist Aurora Healthcare Burlington, Elkhorn, Lake Geneva, WI A 58 year-old, obese white man has had heartburn for more than 20 years. He read a magazine
Case Scenario 1. The patient agreed to a CT guided biopsy of the left upper lobe mass. This was performed and confirmed non-small cell carcinoma.
 Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Case Scenario 1 An 89 year old male patient presented with a progressive cough for approximately six weeks for which he received approximately three rounds of antibiotic therapy without response. A chest
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education