Current state of upfront treatment for newly diagnosed advanced ovarian cancer
|
|
|
- Kenneth Page
- 6 years ago
- Views:
Transcription
1 Current state of upfront treatment for newly diagnosed advanced ovarian cancer Ursula Matulonis, M.D. Associate Professor of Medicine, HMS Program Leader, Medical Gyn Oncology Dana-Farber Cancer Institute Boston, MA Phone:
2 Agenda Review trials for upfront management of newly diagnosed advanced ovarian cancer Review ongoing studies Review new therapies being tested
3 Ovarian cancer ,500 cases diagnosed per year in the United States and 16,500 deaths per year 1. Most patients are diagnosed in late stages; no screening test exists. Pathology: 4 different types (serous, endometrioid,, clear cell and mucinous) 1 Jemal A, Siegel R, Ward E, et al: Cancer statistics, CA: Cancer J Clin 59(4):225-49, 2009
4 Unique aspects of newly diagnosed advanced ovarian cancer Upfront surgical management is standard of care: allows access to tissue OC is very chemotherapy sensitive at diagnosis; >80% of cancers will respond to platinum- and taxane-based chemotherapy upfront at dx. Cancer becomes more treatment-refractory refractory following recurrence. Few but some CTC s. Outcomes for newly diagnosed ovarian cancer have reached a plateau with platinum/taxane taxane combinations.
5 Ovarian cancer staging Stage I: confined to ovary(ies) Stage II: local spread to pelvis Stage III: Stage IIIA: microscopic upper abdominal spread Stage IIIB: upper abd implants <2 cm Stage IIIC: 2cm implants and/or +nodal involvement Stage IV: spread outside the abdominal cavity. Definition of extent of debulking is what is residual post surgical debulking: optimal cytoreduction/debulking: 1cm residual suboptimal debulking: : > 1cm residual cancer

6 Advanced ovarian cancer
7 PFS and OS for newly diagnosed advanced ovarian cancer Study Median PFS Median OS Comments GOG 111 NEJM mos 38 mos Suboptimally and stage IV GOG 158 JCO mos 57.4 mos Optimally cytoreduced only GOG 172 NEJM mos 65 mos Optimally cytoreduced only. Longest survival observed in advanced ovarian cancer GOG 182 JCO mos 44 mos Both optimal and suboptimal. Study compared 5 arms of treatment Weekly pac vs q21 d Lancet mos (vs. 17 mos) Not reached Both optimal and suboptimal EORTC neoadjuvant IGCS 2008 Both 12 mos 29/30 mos Neoadjuvant vs. upfront debulking GOG 218: ASCO 2010
8 GOG111: Survival By Treatment Pac + cis (38 mos) Cy + cis (24 mos) Treatment Alive (N) Died (N) Median PFS Survival (mo) Relative Risk Cisplatin/ cyclophosphamide Cisplatin/paclitaxel McGuire WP, et al. N Engl J Med. 1996;334:1-6.
9 GOG0182-ICON5: Schema I Carboplatin AUC 6 (d1) Paclitaxel 175 mg/m2 (d1) x8 R A N D O M I Z E II III IV V Carboplatin AUC 5 (d1) Paclitaxel 175 mg/m 2 (d1) Gemcitabine 800 mg/m 2 (d1,8) Carboplatin AUC 5 (d1) Paclitaxel 175 mg/m 2 (d1) Doxil 30 mg/m 2 (d1, every other cycle) Carboplatin AUC 5 (d3) Topotecan 1.25 mg/m 2 (d1-3) Carboplatin AUC 6 (d8) Gemcitabine 1 g/m 2 (d1,8) x4 x4 x8 x8 Carboplatin AUC 6 (d1) Paclitaxel 175 mg/m 2 (d1) x4 JCO 2008
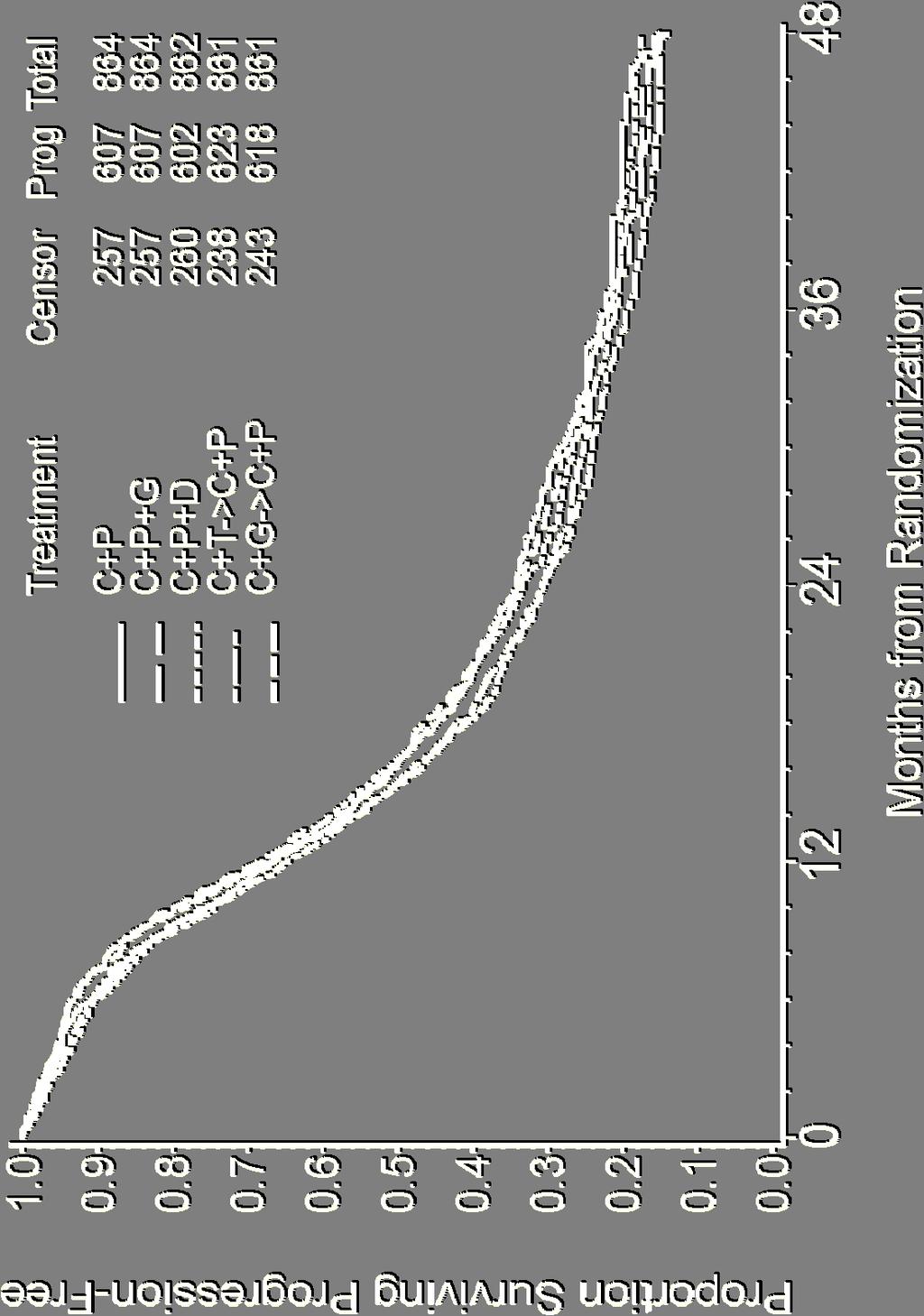
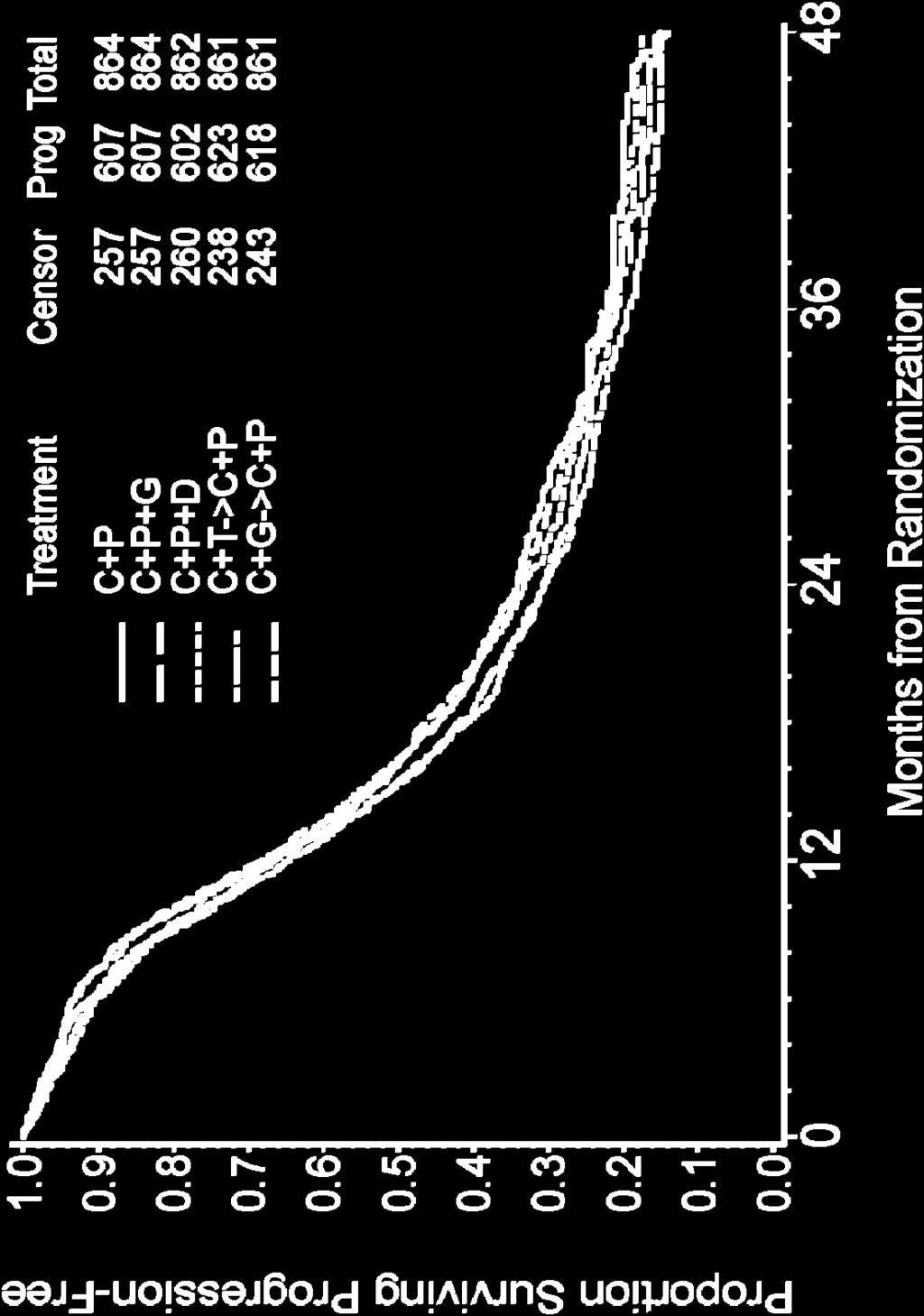
10 GOG0182-ICON5: Progression-Free Survival

11 GOG0182-ICON5: Overall Survival
12 Primary Therapy IP Median PFS, months Hazard ratio Median OS, months Hazard ratio GOG GOG GOG IV IP (P =.01) 0.80 (P =.05) IV IP (P =.02) 0.81 (P =.05) 0.75 (P =.03) PFS = Progression-free survival; OS = Overall survival; IV = Intravenous; IP = Intraperitoneal. 1. Alberts DS, et al. N Engl J Med. 1996;335: Markman M, et al. J Clin Oncol. 2001;19: Armstrong DK, et al. N Engl J Med. 2006;354:34-43.
13 GOG #172 Armstrong et.al. N Engl J Med 2006;354:34-43 BRCA Analysis DNA Banking Second look Laparotomy (if chosen) Ovarian cancer Optimal (<1cm) Stage III Stratify: Gross residual Planned 2 nd look R A N D O M I Z E Paclitaxel 135 mg/m 2 /24h Cisplatin 75 mg/m 2 q 21 days x 6 Paclitaxel 135 mg/m 2 /24h Cisplatin 100 mg/m 2 IP D2 Paclitaxel 60 mg/m 2 IP D8 q 21 days x 6
14 GOG #172: outcomes Regimen 1 Intravenous Regimen 2 Intraperitoneal Progression-free 18.3 mos 23.8 mos Overall Survival 49.5 mos 66.9 mos
15 Figure 1 By Treatment Group (GOG 172) 1.0 Proportion Progression-Free months for IV Rx Group PF Failed Total IV IP months for IP group (Δ = 6 months) Months on Study
16 GOG Protocol 172 By Treatment Group IP median overall survival = 66 months (Δ = 16 months) Proportion Surviving IV median overall survival = 49.5 months Rx Group Lost to Alive Dead Total Follow-up Rx IV Group 5 Alive Dead 78 Total IV IP Months on Study N Engl J Med. 2006;354: Relative risk of death = 0.75 (95% CI: 0.58, 0.97) P =.03
17 GOG Protocol 172 Toxicity G3/4 G3/4 G3/4 G3/4 G3/4 G3/4 G3/4 G3/4 G3/4 Leukopenia* Platelet GI* Renal* Neurologic Event* Fatigue* Infection* Metabolic* Pain* IV, % (N = 210) IP, % (N = 201) *P 0.05
18
19 Modulating Toxicity of IP Therapy New approaches to improve toxicity profile Timing of catheter placement Timing of chemotherapy relative to surgery relative to catheter placement Agents used Supportive care (anti-emetics, IV fluids, myeloid growth factor) Successful use of IP therapy requires: Training Skill Experience Dedication
20 GOG 252: Newest upfront IP study

21 IGCS Bangkok October 25 th 2008
22 Ovarian, tubal or peritonal cancer FIGO stage IIIc-IV (n = 718) Randomisation Primary Debulking Surgery Neoadjuvant chemotherapy 3 x Platinum based CT 3 x Platinum based CT Interval debulking (not obligatory) Interval debulking if no PD > 3 x Platinum based CT > 3 x Platinum based CT Primary Endpoint: Overall survival Secondary endpoints: Progression Free Survival, Quality of Life, Complications
23 Randomised EORTC-GCG/NCIC GCG/NCIC-CTG CTG trial on NACT + IDS versus PDS Statistical considerations 704 patients were required in order to show noninferiority with respect to survival between PDS and NACT, with a one-sided type I error of 0.05 and a power of 80%.
24 Randomised EORTC-GCG/NCIC GCG/NCIC-CTG CTG trial on NACT + IDS versus PDS Baseline Characteristics (ITT) PDS NACT -> > IDS FIGO Stage IIIc IV 77% 23% 77% 23% Serous 64% 58% Age 62 (25-86) 62 (33-81) CA125 > 30 KU/L 98% 99% Largest metastasis (mm) 80 (0-400) 80 (0-389)
25 Randomised EORTC-GCG/NCIC GCG/NCIC-CTG CTG trial on NACT + IDS versus PDS Surgical findings and results (PP1) PDS (n = 329) NACT -> > IDS (n = 339)* Metastases before > 2 cm 95% 68% Metastases before > 10 cm 62% 27% No residual after surgery 21% 53% 1 cm after surgery 46% 82% * % calculated on the 306 patients who underwent IDS.
26 Randomised EORTC-GCG/NCIC GCG/NCIC-CTG CTG trial on NACT + IDS versus PDS Surgical characteristics (PP1) Postoperative mortality (< 28 days) PDS (n = 329) NACT -> > IDS (n = 339)* 2.7% 0.6% Postoperative fever Gr % 2% Fistula (bowel/gu) 1.2% / 0.3% 0,3% / 0.6% Operative time (minutes) Red blood cell transfusion 51% 53% Hemorhage Grade 3/4 7% 1% Venous Gr 3/4 2.4% 0.3%
27 NACT + IDS versus PDS: ITT Progression-free survival Median PFS PDS: 12 months IDS: 12 months HR for IDS:0.99 (0.87, 1.13) 0 (years) O N Number of patients at risk : Treatment Upfront debu Neoadjuvant
28 NACT + IDS versus PDS: ITT Overall survival Median survial PDS: 29 months IDS: 30 months HR for IDS:0.98 (0.85, 1.14) (years) O N Number of patients at risk : Treatment Upfront debulking s Neoadjuvant chemo
29 NACT + IDS versus PDS: ITT Survival time: Figo stage EORTC Events / Patients Statistics Upfront debulkingneo-adj. Chemo (O-E) Var. HR & CI* (Upfront debulking : Neo-adj. Chemo) 1-HR % ± SD III 190 / / IV 68 / / Total 258/ / (72.3 %) (70.2 %) 2% ±9 increase Test for heterogeneity Chi-square=0.5, df=1: p> Upfront debulking Neo-adj. Chemo better better Treatment effect: p>0.1 *90% CI everywhere
30 NACT + IDS versus PDS: ITT Survival time: Age EORTC Events / Patients Upfront debulkingneo-adj. Chemo Statistics (O-E) Var. HR & CI* (Upfront debulking : Neo-adj. Chemo) 1-HR % ± SD <50 34 / / / / >70 53 / / Total 259/ / (71.7 %) (70.3 %) 3% ±9 increase Test for heterogeneity Chi-square=2.59, df=2: p> Upfront debulking Neo-adj. Chemo better better Treatment effect: p>0.1 *90% CI everywhere
31 Multivariate analysis for OS(PP1) P values Optimal debulking Histological type (9 categories) Largest tumor size at randomisation Figo Stage (IIIc vs IV) Country (14 categories) Age WHO PS Differentiation Grade Treatment arm NS NS NS
32 Conclusions 1. In Stage IIIc-IV IV OVCA, NACT followed IDS produces similar OS and PFS outcomes compared to standard primary debulking followed by chemotherapy in FIGO Stage IIIc-IV IV ovarian carcinoma. 2. There does not seem to be a subgroup based on 1. Stage IIIc or IV 2. Age 3. WHO performance 4. Histological type ovarian cancer 5. Countries with high or low optimal debulking rate for which PDS or NACT -> > IDS result in better survival. Because of the overall poorer PFS and OS compared to other studies, the use of neoadjuvant chemotherapy is not considered the standard of care in the United States, but is reserved for patients who are too ill to undergo initial surgery or those patients who have clearly non-debulkable cancer.
33 PFS and OS for newly diagnosed advanced ovarian cancer Study Median PFS Median OS Comments GOG 111 NEJM mos 38 mos Suboptimally and stage IV GOG 158 JCO mos 57.4 mos Optimally cytoreduced only GOG 172 NEJM mos 65 mos Optimally cytoreduced only. Longest survival observed in advanced ovarian cancer GOG 182 JCO mos 44 mos Both optimal and suboptimal. Study compared 5 arms of treatment Weekly pac vs q21 d Lancet mos (vs. 17 mos) Not reached Both optimal and suboptimal EORTC neoadjuvant IGCS 2008 Both 12 mos 29/30 mos Neoadjuvant vs. upfront debulking GOG 218: ASCO 2010
34 Dose dense paclitaxel versus q 3 week paclitaxel for newly diagnosed ovarian cancer 631 eligible patients were enrolled Eligibility: stage II to IV epithelial ovarian cancer Pts could have upfront or interval debulking surgery Primary endpoint was PFS Treatment 1 : Paclitaxel 180 mg/m2 + carboplatin AUC 6 day both day 1 or Paclitaxel 80 mg/m2 days 1, 8, 15 + carboplatin AUC 6 day 1 (dose dense group) 1 Creatinine clearance calculated by Jelliffe and treatment given for 6 cycles Katsumata et al, Lancet 2009
35 Progression-free survival PFS for: DD Pac: 28 months q3 week: 17.2 mos HR 0.75 (95% CI: ) p=0.015 Katsumata et al, Lancet 2009
36 Overall survival 3 year OS for: DD Pac 72% q3 week: 65% HR 0.75 (95% CI: ) p=0.03 Katsumata et al, Lancet 2009
37 Progression-free survival according to baseline characteristics Lancet, 2009

38 Grade 3/4 anemia was higher in the dose dense group From: Katsumata et al, Lancet 2009
39 GOG Frontline Trials GOG-218 Optimal or Suboptimal EOC, PPC, FT cancer Paclitaxel Carboplatin Placebo Paclitaxel Carboplatin Bevacizumab Paclitaxel Carboplatin Bevacizumab Placebo 15 months Placebo 15 months Bevacizumab 15 months Survival, PFS primary endpoints Biologic & QOL endpoints EOC = Epithelial ovarian cancer; PPC = Primary peritoneal cancer; FT = Fallopian tube; PFS = Progression-free survival; QOL = Quality of life.
40 GOG 218 results To be presented at ASCO 2010 Preliminary results were released via press release in March 2010 ( Patients receiving carboplatin/taxol/bevacizumab + bevacizumab maintenance did better than carbo/taxol alone. Patients receiving carboplatin/taxol/bevacizumab (no maintenance) did equally well as patients receiving carboplatin/taxol alone. At this point, our group is not using bevacizumab off study.
41 Newer biologics being added to upfront treatment PARP inhibitors Src inhibitors Other anti-angiogenics angiogenics besides bevacizumab Notch inhibitors
42 Protocol Pilot study screening for druggable mutations in both recurrent and newly diagnosed advanced ovarian cancer. Opened March 2010; 28 pts enrolled thus far. CLIA-approved PIK3CA, KRAS,, and BRAF testing at LMM (for clinical decision making). OncoMap platform used thereafter to test for 1100 mutations in 100 oncogenes (for research).
43 Standard of Care for pts with advanced epithelial ovarian cancer: 2010 Upfront debulking surgery by a gynecologic oncologist. If optimally cytoreduced (i.e. 1cm tumor remaining), options are: Placement of an IP port and IP/IV tx 1, IV carboplatin/paclitaxel,, or clinical trial. If suboptimally cytoreduced,, options are: IV carboplatin/paclitaxel (q3 week or weekly paclitaxel) 3 or clinical trial Neoadjuvant chemotherapy 2 has demonstrated equivalent results to upfront cytoreduction chemotherapy, but this appears more popular in Europe than the U.S. with lower OS and PFS overall compared to other studies. 1 Armstrong DK, et al, N Engl J Med 354(1):34-43, Vergote I et al. IGCS 2008 Meeting: Abstract #2008_1767. Available at: 3
44 Following completion of upfront chemotherapy CA125 monitoring every 3 months; although off study, controversy exists whether or not this is of benefit 1 Several drugs are being tested in the first maintenance setting. There is no standard of care for use of maintenance therapy 2 1 Rustin GJ et al, J Clin Oncol 27(18s):Abstr 1, Foster et al, Gyn Onc 115: , 2009
45 Conclusions Standard of care for newly diagnosed advanced ovarian, tubal or peritoneal cancer remains a platinum and taxane combination New options for patients include dose dense administration of paclitaxel Results of GOG 218 asking question of role of bevacizumab in newly diagnosed patients to be presented at ASCO 2010
Jemal A, Siegel R, Ward E, et al: Cancer statistics, CA: Cancer J Clin 59(4):225-49, 2009
:225-49, 2009") Ovarian cancer 2010-22,500 cases diagnosed per year in the United States and 16,500 deaths per year1. - Most patients are diagnosed in late stages; no screening test exists. - Pathology: 4 different types
Ovarian cancer 2010-22,500 cases diagnosed per year in the United States and 16,500 deaths per year1. - Most patients are diagnosed in late stages; no screening test exists. - Pathology: 4 different types
FoROMe Lausanne 6 février Anita Wolfer MD-PhD Cheffe de clinique Département d Oncologie, CHUV
 FoROMe Lausanne 6 février 2014 Anita Wolfer MD-PhD Cheffe de clinique Département d Oncologie, CHUV Epithelial Ovarian Cancer (EOC) Epidemiology Fifth most common cancer in women and forth most common
FoROMe Lausanne 6 février 2014 Anita Wolfer MD-PhD Cheffe de clinique Département d Oncologie, CHUV Epithelial Ovarian Cancer (EOC) Epidemiology Fifth most common cancer in women and forth most common
Randomized Phase III Trials of Intravenous vs. Intraperitoneal Therapy in Optimal Ovarian Cancer
 Randomized Phase III Trials of Intravenous vs. Intraperitoneal Therapy in Optimal Ovarian Cancer Deborah K. Armstrong, M.D. Associate Professor of Oncology, Gynecology and Obstetrics Development of Intraperitoneal
Randomized Phase III Trials of Intravenous vs. Intraperitoneal Therapy in Optimal Ovarian Cancer Deborah K. Armstrong, M.D. Associate Professor of Oncology, Gynecology and Obstetrics Development of Intraperitoneal
ACRIN Gynecologic Committee
 ACRIN Gynecologic Committee Fall Meeting 2010 ACRIN Abdominal Committee Biomarkers & Endpoints in Ovarian Cancer Trials Robert L. Coleman, MD Professor and Vice Chair, Clinical Research Department of Gynecologic
ACRIN Gynecologic Committee Fall Meeting 2010 ACRIN Abdominal Committee Biomarkers & Endpoints in Ovarian Cancer Trials Robert L. Coleman, MD Professor and Vice Chair, Clinical Research Department of Gynecologic
Winship Cancer Institute of Emory University Optimizing First Line Treatment of Advanced Ovarian Cancer
 Winship Cancer Institute of Emory University Optimizing First Line Treatment of Advanced Ovarian Cancer Ira R. Horowitz, MD, SM, FACOG, FACS John D. Thompson Professor and Chairman Department of Gynecology
Winship Cancer Institute of Emory University Optimizing First Line Treatment of Advanced Ovarian Cancer Ira R. Horowitz, MD, SM, FACOG, FACS John D. Thompson Professor and Chairman Department of Gynecology
Controversies in the Management of Advanced Ovarian Cancer
 안녕하세요 Controversies in the Management of Advanced Ovarian Cancer Mansoor R. Mirza Nordic Society of Gynaecological Oncology (NSGO) & Rigshospitalet Copenhagen University Hospital, Denmark Primary Debulking
안녕하세요 Controversies in the Management of Advanced Ovarian Cancer Mansoor R. Mirza Nordic Society of Gynaecological Oncology (NSGO) & Rigshospitalet Copenhagen University Hospital, Denmark Primary Debulking
Clinical Trials. Ovarian Cancer
 1.0 0.8 0.6 0.4 0.2 0.0 < 65 years old 65 years old Events Censored Total 128 56 184 73 35 108 0 12 24 36 48 60 72 84 27-10-2012 Ovarian Cancer Stuart M. Lichtman, MD Attending Physician 65+ Clinical Geriatric
1.0 0.8 0.6 0.4 0.2 0.0 < 65 years old 65 years old Events Censored Total 128 56 184 73 35 108 0 12 24 36 48 60 72 84 27-10-2012 Ovarian Cancer Stuart M. Lichtman, MD Attending Physician 65+ Clinical Geriatric
Intraperitoneal chemotherapy: where are we going? A. Gadducci Pisa
 Intraperitoneal chemotherapy: where are we going? A. Gadducci Pisa Intraperitoneal Chemotherapy (IP) in advanced ovarian cancer (EOC): Rationale The spread of disease is often limited to the peritoneal
Intraperitoneal chemotherapy: where are we going? A. Gadducci Pisa Intraperitoneal Chemotherapy (IP) in advanced ovarian cancer (EOC): Rationale The spread of disease is often limited to the peritoneal
PROGNOSTIC FACTORS AND FIRST LINE CHEMOTHERAPY IN AOC
 PROGNOSTIC FACTORS AND FIRST LINE CHEMOTHERAPY IN AOC Giorgia Mangili RUF ginecologia oncologica medica IRCCS San Raffaele Milano mangili.giorgia@hsr.it STANDARD CHEMOTHERAPY The standard chemotherapy
PROGNOSTIC FACTORS AND FIRST LINE CHEMOTHERAPY IN AOC Giorgia Mangili RUF ginecologia oncologica medica IRCCS San Raffaele Milano mangili.giorgia@hsr.it STANDARD CHEMOTHERAPY The standard chemotherapy
Co-Chairs Helen J MacKay and Diane Provencher On behalf of the OV21/PETROC Investigators CCTG, NCRI (UK), GEICO and SWOG
, GEICO and SWOG") OV21/PETROC: A Randomized Gynecologic Cancer Intergroup (GCIG) Phase II Study of Intraperitoneal (IP) vs. Intravenous (IV) Chemotherapy Following Neoadjuvant Chemotherapy and Optimal Debulking Surgery
OV21/PETROC: A Randomized Gynecologic Cancer Intergroup (GCIG) Phase II Study of Intraperitoneal (IP) vs. Intravenous (IV) Chemotherapy Following Neoadjuvant Chemotherapy and Optimal Debulking Surgery
The Ohio State University Approach to Advanced Ovarian Cancer Korean Society of Gynecologic Oncology
 The Ohio State University Approach to Advanced Ovarian Cancer Korean Society of Gynecologic Oncology April 26, 2013 Larry J. Copeland M.D. Thank You for Your Friendship! 1982 1996 2013 The Ohio State University
The Ohio State University Approach to Advanced Ovarian Cancer Korean Society of Gynecologic Oncology April 26, 2013 Larry J. Copeland M.D. Thank You for Your Friendship! 1982 1996 2013 The Ohio State University
GOG-172: Survival Outcomes
 CHEMOTHERAPY GOG-172: Survival Outcomes Progression-Free Survival Overall Survival Proportion Progression-Free 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 Rx Group IV IP PF Failed Total 50 160 210 63 142
CHEMOTHERAPY GOG-172: Survival Outcomes Progression-Free Survival Overall Survival Proportion Progression-Free 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0.0 Rx Group IV IP PF Failed Total 50 160 210 63 142
breast and OVARIAN cancer
 breast and OVARIAN cancer DR DAVID FENNELLY CONSULTANT MEDICAL ONCOLOGIST ST VINCENT S UNIVERSITY HOSPITAL DUBLIN HOW RELEVANT IS ONCOLOGY IN MEDICINE TODAY? Cancer is the second leading cause of death
breast and OVARIAN cancer DR DAVID FENNELLY CONSULTANT MEDICAL ONCOLOGIST ST VINCENT S UNIVERSITY HOSPITAL DUBLIN HOW RELEVANT IS ONCOLOGY IN MEDICINE TODAY? Cancer is the second leading cause of death
Table Selected Clinical Trials of Anti-Angiogenesis Therapy in Gynecologic Malignancies
 Table Selected Clinical Trials of Anti-Angiogenesis Therapy in Gynecologic Malignancies Uterus Study N Eligibility Regimen RR (No. of Responses) Median OS Grade 3/4 Toxicities Nimeiri et al[42] Total:
Table Selected Clinical Trials of Anti-Angiogenesis Therapy in Gynecologic Malignancies Uterus Study N Eligibility Regimen RR (No. of Responses) Median OS Grade 3/4 Toxicities Nimeiri et al[42] Total:
Side Effects. PFS (months) Study Regimen No. patients. OS (months)
 Study Regimen No. patients. OS (months)") Study Regimen No. patients PFS (months) OS (months) Side Effects Phase II PR ov ca 1 Phase II GOG PR+PS ov ca 1 Bev (15 mg/kg) q3wks Bev (15 mg/kg) q3wks 44 4.4 10.7 HTN, Proteinuria, GI perf (11%) stopped
Study Regimen No. patients PFS (months) OS (months) Side Effects Phase II PR ov ca 1 Phase II GOG PR+PS ov ca 1 Bev (15 mg/kg) q3wks Bev (15 mg/kg) q3wks 44 4.4 10.7 HTN, Proteinuria, GI perf (11%) stopped
10/24/14. Grand Rounds in Ovarian Cancer: Standards of Care and Novel Treatment Approaches. Disclosure. Learning Objectives
 10/24/14 Grand Rounds in Ovarian Cancer: Standards of Care and Novel Treatment Approaches Jessica Gahres, PA-C Memorial Sloan Kettering Cancer Center Don S. Dizon, MD Massachusetts General Hospital Cancer
10/24/14 Grand Rounds in Ovarian Cancer: Standards of Care and Novel Treatment Approaches Jessica Gahres, PA-C Memorial Sloan Kettering Cancer Center Don S. Dizon, MD Massachusetts General Hospital Cancer
Ovarian Cancer: Implications for the Pharmacist
 Ovarian Cancer: Implications for the Pharmacist Megan May, Pharm.D., BCOP Objectives Describe the etiology and pathophysiology of ovarian cancer Outline the efficacy and safety of treatment options for
Ovarian Cancer: Implications for the Pharmacist Megan May, Pharm.D., BCOP Objectives Describe the etiology and pathophysiology of ovarian cancer Outline the efficacy and safety of treatment options for
Residual Tumor Following Surgery: The Strongest Prognostic Factor or a Myth? Philipp Harter, MD Kliniken Essen Mitte Essen, Germany
 Residual Tumor Following Surgery: The Strongest Prognostic Factor or a Myth? Philipp Harter, MD Kliniken Essen Mitte Essen, Germany What Are Our Questions Q1: Prognostic factor residual disease? Q2: Differences
Residual Tumor Following Surgery: The Strongest Prognostic Factor or a Myth? Philipp Harter, MD Kliniken Essen Mitte Essen, Germany What Are Our Questions Q1: Prognostic factor residual disease? Q2: Differences
GOG212: Taxane Maintenance
 GOG212: Taxane Maintenance Epithelial Ovarian or Primary Peritoneal Cancer Optimal or Suboptimal Cytoreduction Clinical C with normal CA125, no symptoms, normal CT Primary Carboplatin and Paclitaxel (or
GOG212: Taxane Maintenance Epithelial Ovarian or Primary Peritoneal Cancer Optimal or Suboptimal Cytoreduction Clinical C with normal CA125, no symptoms, normal CT Primary Carboplatin and Paclitaxel (or
OVARIAN CANCER Updated July 2015 by: Dr. Jenny Ko (PGY 5 Medical Oncology Resident, University of Calgary)
") 1 OVARIAN CANCER Updated July 2015 by: Dr. Jenny Ko (PGY 5 Medical Oncology Resident, University of Calgary) Source: UpToDate 2015, ASCO/CCO/Alberta provincial guidelines, NCCN Reviewed by: Dr. Sarah Glaze
1 OVARIAN CANCER Updated July 2015 by: Dr. Jenny Ko (PGY 5 Medical Oncology Resident, University of Calgary) Source: UpToDate 2015, ASCO/CCO/Alberta provincial guidelines, NCCN Reviewed by: Dr. Sarah Glaze
Tarceva Trial EORTC 55041
 Tarceva Trial EORTC 55041 Primary Chemotherapy Tarceva consolidation 2 years Control Patients closed / 835 Leading Participating EORTC AGO-AUSTRIA, ANZGOG, GINECO, MRC/NCIC, MANGO Randomised trial on Erlotinib
Tarceva Trial EORTC 55041 Primary Chemotherapy Tarceva consolidation 2 years Control Patients closed / 835 Leading Participating EORTC AGO-AUSTRIA, ANZGOG, GINECO, MRC/NCIC, MANGO Randomised trial on Erlotinib
Ovarian Cancer. Disclosure. Ovarian Statistics Educational Objectives. The State of Ovarian Care in the US Why aren t we making more progress?
 Esteemed Physician Humanitarian Distinguished Citizen Disclosure Ovarian Cancer The State of Ovarian Care in the US Why aren t we making more progress? Dr. Goff has indicated that she has no relevant financial
Esteemed Physician Humanitarian Distinguished Citizen Disclosure Ovarian Cancer The State of Ovarian Care in the US Why aren t we making more progress? Dr. Goff has indicated that she has no relevant financial
Trial record 1 of 1 for:
 Find Studies About Studies Submit Studies Resources About Site Trial record 1 of 1 for: YO39523 Previous Study Return to List Next Study A Study of Atezolizumab Versus Placebo in Combination With Paclitaxel,
Find Studies About Studies Submit Studies Resources About Site Trial record 1 of 1 for: YO39523 Previous Study Return to List Next Study A Study of Atezolizumab Versus Placebo in Combination With Paclitaxel,
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Triple Negative Breast Cancer. Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008
 Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Review Heated Intraperitoneal Chemotherapy in the Management of Ovarian Cancer
 Review Heated Intraperitoneal Chemotherapy in the Management of Ovarian Cancer Andrea Jewell 1, Megan McMahon 1 and Dineo Khabele 1 1 Division of Gynecologic Oncology, Department of Obstetrics and Gynecology,
Review Heated Intraperitoneal Chemotherapy in the Management of Ovarian Cancer Andrea Jewell 1, Megan McMahon 1 and Dineo Khabele 1 1 Division of Gynecologic Oncology, Department of Obstetrics and Gynecology,
Carcinosarcoma Trial rial in s a in rare malign rare mali ancy
 Carcinosarcoma Trials in a rare malignancy BACKGROUND Rare and highly aggressive epithelial malignancies Biphasic tumors with epithelial and mesenchymal components Uterine carcinomas (UCS) uncommon with
Carcinosarcoma Trials in a rare malignancy BACKGROUND Rare and highly aggressive epithelial malignancies Biphasic tumors with epithelial and mesenchymal components Uterine carcinomas (UCS) uncommon with
Granulosa Cell Tumor Monitoring and Treatment. Outline: 1. Surgery 2. Adjuvant 3. Chemo 4. Hormonal 5. Investigational. Whole Genome Sequencing
 Potential Conflicts of Interest capped at a level befitting an academic role Lo B. Serving Two Masters 2010;362:669-671 Granulosa Cell Tumor Monitoring and Treatment Richard T. Penson, MD, MRCP Clinical
Potential Conflicts of Interest capped at a level befitting an academic role Lo B. Serving Two Masters 2010;362:669-671 Granulosa Cell Tumor Monitoring and Treatment Richard T. Penson, MD, MRCP Clinical
GCIG Rare Tumour Brainstorming Day
 GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
GCIG Rare Tumour Brainstorming Day Relatively (Not So) Rare Tumours Adenocarcinoma of Cervix Keiichi Fujiwara, Ros Glasspool Benedicte Votan, Jim Paul Aim of the Day To develop at least one clinical trial
CERVICAL/VULVAR CANCER CLINICAL TRIALS
 CERVICAL/VULVAR CANCER CLINICAL TRIALS ALL-COMERS Primary Treatment Locally Advanced Recurrent Cervical GTFB (07-0935) TISSUE BANK ALL GYN TISSUE ETCTN (Phase II) (17-0458) LAO-MD017/#10010 Phase II Study
CERVICAL/VULVAR CANCER CLINICAL TRIALS ALL-COMERS Primary Treatment Locally Advanced Recurrent Cervical GTFB (07-0935) TISSUE BANK ALL GYN TISSUE ETCTN (Phase II) (17-0458) LAO-MD017/#10010 Phase II Study
Survival impact of cytoreductive surgery ın advanced stage EOC
 Survival impact of cytoreductive surgery ın advanced stage EOC Ayhan Ali, MD Baskent University School of Medicine Department of Obstetrics and Gynecology, Division of Gynecologic Oncology 1 OVARIAN CANCER
Survival impact of cytoreductive surgery ın advanced stage EOC Ayhan Ali, MD Baskent University School of Medicine Department of Obstetrics and Gynecology, Division of Gynecologic Oncology 1 OVARIAN CANCER
Hitting the High Points Gynecologic Oncology Review
 Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
2/21/2016. Cancer Precision Medicine: A Primer. Ovarian Cancer Statistics and Standard of Care in 2015 OUTLINE. Background
 Cancer Precision Medicine: A Primer Rebecca C. Arend, MD Division of Gyn Oncology OUTLINE Background Where we are Where we have been Where we are going Targeted Therapy in Ovarian Cancer How to Individualized
Cancer Precision Medicine: A Primer Rebecca C. Arend, MD Division of Gyn Oncology OUTLINE Background Where we are Where we have been Where we are going Targeted Therapy in Ovarian Cancer How to Individualized
OVARIAN CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre)
") 1 OVARIAN CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Source: UpToDate 2017, ASCO/CCO/Alberta provincial guidelines, NCCN Reviewed by: Dr. Sarah Glaze (Gynecologic
1 OVARIAN CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Source: UpToDate 2017, ASCO/CCO/Alberta provincial guidelines, NCCN Reviewed by: Dr. Sarah Glaze (Gynecologic
AHFS Final. IV and intraperitoneal regimen for. Criteria Used in. Strength. Strength. Use: Based on. taxane (either IV. following
 AHFS Final Determination of Medical Acceptance: Off-label Use of Sequential IV Paclitaxel, Intraperitoneal Cisplatin, and Intraperitoneal Paclitaxel for Initial Adjuvan nt Treatment of Optimally Debulked
AHFS Final Determination of Medical Acceptance: Off-label Use of Sequential IV Paclitaxel, Intraperitoneal Cisplatin, and Intraperitoneal Paclitaxel for Initial Adjuvan nt Treatment of Optimally Debulked
Ovarian Cancer Survival. Ovarian Cancer Follow-up. Ovarian Cancer Treatment. Management of Recurrent Ovarian Carcinoma. 15,520 cancer deaths
 Management of Recurrent Ovarian Carcinoma Lee-may Chen, M.D. Department of Obstetrics, Gynecology, & Reproductive Sciences UCSF Comprehensive Cancer Center Ovarian Cancer Survival United States, 28: 1
Management of Recurrent Ovarian Carcinoma Lee-may Chen, M.D. Department of Obstetrics, Gynecology, & Reproductive Sciences UCSF Comprehensive Cancer Center Ovarian Cancer Survival United States, 28: 1
Breakfast with Professor Advances in ovarian cancer first-line treatment : The role of anti angiogenics
 Breakfast with Professor Advances in ovarian cancer first-line treatment : The role of anti angiogenics CLAUDIO CALAZAN Oncologia D Or Oncologistas Associados First-line treatment : The role of anti angiogenics
Breakfast with Professor Advances in ovarian cancer first-line treatment : The role of anti angiogenics CLAUDIO CALAZAN Oncologia D Or Oncologistas Associados First-line treatment : The role of anti angiogenics
Expert Call Innovation in Ovarian Cancer Hosted by John Sonnier, William Blair. December 13, 2016
 Expert Call Innovation in Ovarian Cancer Hosted by John Sonnier, William Blair December 13, 2016 1 Forward-Looking Statements This presentation includes forward-looking statements based on management's
Expert Call Innovation in Ovarian Cancer Hosted by John Sonnier, William Blair December 13, 2016 1 Forward-Looking Statements This presentation includes forward-looking statements based on management's
RANDOMISED PHASE III STUDY OF ERLOTINIB VERSUS OBSERVATION IN PATIENTS WITH NO EVIDENCE OF DISEASE PROGRESSION AFTER FIRST LINE, PLATINUM-BASED
 RANDOMISED PHASE III STUDY OF ERLOTINIB VERSUS OBSERVATION IN PATIENTS WITH NO EVIDENCE OF DISEASE PROGRESSION AFTER FIRST LINE, PLATINUM-BASED CHEMOTHERAPY FOR HIGH- RISK STAGE I AND STAGE II-IV OVARIAN
RANDOMISED PHASE III STUDY OF ERLOTINIB VERSUS OBSERVATION IN PATIENTS WITH NO EVIDENCE OF DISEASE PROGRESSION AFTER FIRST LINE, PLATINUM-BASED CHEMOTHERAPY FOR HIGH- RISK STAGE I AND STAGE II-IV OVARIAN
Ovarian Cancer: New insights into biology and treatment
 Ovarian Cancer: New insights into biology and treatment 2018 Master Class Course Ursula A. Matulonis, MD Director, Gynecologic Oncology Brock-Wilson Family Chair Dana-Farber Cancer Institute Professor
Ovarian Cancer: New insights into biology and treatment 2018 Master Class Course Ursula A. Matulonis, MD Director, Gynecologic Oncology Brock-Wilson Family Chair Dana-Farber Cancer Institute Professor
U T C H. No disclosure
 D U GOG T C H Randomized phase 3 trial comparing primary cytoreductive surgery with or without hyperthermic intraperitoneal chemotherapy for stage III epithelial ovarian cancer: OVHIPEC-2 Willemien van
D U GOG T C H Randomized phase 3 trial comparing primary cytoreductive surgery with or without hyperthermic intraperitoneal chemotherapy for stage III epithelial ovarian cancer: OVHIPEC-2 Willemien van
NCCN Guidelines for Ovarian Cancer V Meeting on 11/15/17
 OV-1 External request: Submission from Vermillion/ASPiRA Laboratories to consider: Inclusion of the following recommendation in the workup for suspected ovarian cancer: OVA1 and/or Multivariate Index Assay
OV-1 External request: Submission from Vermillion/ASPiRA Laboratories to consider: Inclusion of the following recommendation in the workup for suspected ovarian cancer: OVA1 and/or Multivariate Index Assay
OVARIAN CANCER CLINICAL TRIALS
 OVARIAN CANCER CLINICAL TRIALS FRONT-LINE THERAPIES STG III, IV PHASE 3 GOG 3015/Roche YO39523 (16-2745) Carbo/Taxol/Bev/Atezolizumab ECOG 0-2 Allows for primary cytoreductive surgery or interval debulking
OVARIAN CANCER CLINICAL TRIALS FRONT-LINE THERAPIES STG III, IV PHASE 3 GOG 3015/Roche YO39523 (16-2745) Carbo/Taxol/Bev/Atezolizumab ECOG 0-2 Allows for primary cytoreductive surgery or interval debulking
Angiogenesis in Ovarian Cancer
 Angiogenesis in Ovarian Cancer Dr Shibani Nicum Consultant Medical Oncologist and Lead for Gynae- Oncology Oxford University Hospitals Content 1. Epithelial Ovarian Cancer : epidemiology 2. Angiogenesis-normal
Angiogenesis in Ovarian Cancer Dr Shibani Nicum Consultant Medical Oncologist and Lead for Gynae- Oncology Oxford University Hospitals Content 1. Epithelial Ovarian Cancer : epidemiology 2. Angiogenesis-normal
From Research to Practice: What s New in Gynecologic Cancers?
 From Research to Practice: What s New in Gynecologic Cancers? David Warshal, M.D. Head, Division of Gynecologic Oncology MD Anderson Cooper Cancer Institute Associate Professor of Obstetrics and Gynecology
From Research to Practice: What s New in Gynecologic Cancers? David Warshal, M.D. Head, Division of Gynecologic Oncology MD Anderson Cooper Cancer Institute Associate Professor of Obstetrics and Gynecology
receive adjuvant chemotherapy
 Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
SOLO-1. Dott.ssa Elisabetta Sanna U.O.C. Ginecologia Oncologica- AOB Cagliari Direttore: Dott. Antonio Macciò
 SOLO-1 maintenance therapy in patients with newly diagnosed advanced ovarian cancer following platinum-based chemotherapy Dott.ssa Elisabetta Sanna U.O.C. Ginecologia Oncologica- AOB Cagliari Direttore:
SOLO-1 maintenance therapy in patients with newly diagnosed advanced ovarian cancer following platinum-based chemotherapy Dott.ssa Elisabetta Sanna U.O.C. Ginecologia Oncologica- AOB Cagliari Direttore:
Current Medical Oncology Approaches to Gynecologic Cancers. Mihaela Cristea, MD Associate Professor Medical Oncology
 Current Medical Oncology Approaches to Gynecologic Cancers Mihaela Cristea, MD Associate Professor Medical Oncology Nothing to disclose DISCLOSURE Ovarian Cancer Objectives: a. To discuss new FDA approved
Current Medical Oncology Approaches to Gynecologic Cancers Mihaela Cristea, MD Associate Professor Medical Oncology Nothing to disclose DISCLOSURE Ovarian Cancer Objectives: a. To discuss new FDA approved
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
New targets in endometrial and ovarian cancer
 New targets in endometrial and ovarian cancer SAMO Interdisciplinary Workshop on Gynecologic Tumors Luzern, January 16-17, 2016 C. Sessa IOSI Bellinzona Outline New targets in ovarian cancer - Cell cycle
New targets in endometrial and ovarian cancer SAMO Interdisciplinary Workshop on Gynecologic Tumors Luzern, January 16-17, 2016 C. Sessa IOSI Bellinzona Outline New targets in ovarian cancer - Cell cycle
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Eligibility Form. 1. Patient Profile. (This form must be completed before the first dose is dispensed.) Request prior approval for enrolment
 Request prior approval for enrolment") Bevacizumab in combination with Paclitaxel and Carboplatin - Frontline Treatment (Previously Untreated) Ovarian, Fallopian Tube, and Primary Peritoneal Cancer (This form must be completed before the first
Bevacizumab in combination with Paclitaxel and Carboplatin - Frontline Treatment (Previously Untreated) Ovarian, Fallopian Tube, and Primary Peritoneal Cancer (This form must be completed before the first
TRUST Trial on Radical Upfront Surgical Therapy
 AGO OP.7 / TRUST TRUST Trial on Radical Upfront Surgical Therapy A close international cooperation ENGOT ov33 Ongoing Trials status update AGO-OVAR OP.7 / TRUST ENGOT-ov33 Trial setting: Sponsor: Pt with
AGO OP.7 / TRUST TRUST Trial on Radical Upfront Surgical Therapy A close international cooperation ENGOT ov33 Ongoing Trials status update AGO-OVAR OP.7 / TRUST ENGOT-ov33 Trial setting: Sponsor: Pt with
Media Release. Third phase III study of Avastin-based regimen met primary endpoint in ovarian cancer. Basel, 08 February 2011
 Media Release Basel, 08 February 2011 Third phase III study of Avastin-based regimen met primary endpoint in ovarian cancer Avastin study in recurrent, platinum-sensitive ovarian cancer showed women lived
Media Release Basel, 08 February 2011 Third phase III study of Avastin-based regimen met primary endpoint in ovarian cancer Avastin study in recurrent, platinum-sensitive ovarian cancer showed women lived
Marcello Deraco M.D. Responsible Peritoneal Malignancies
 Perspectives in clinical research for the treatment of peritoneal carcinomatosisin from ovarian cancer Marcello Deraco M.D. Responsible Peritoneal Malignancies Advisable limits of cytoreduction Survey
Perspectives in clinical research for the treatment of peritoneal carcinomatosisin from ovarian cancer Marcello Deraco M.D. Responsible Peritoneal Malignancies Advisable limits of cytoreduction Survey
The role of neoadjuvant chemotherapy in patients with advanced (stage IIIC) epithelial ovarian cancer
 epithelial ovarian cancer") Radiology and Oncology Ljubljana Slovenia www.radioloncol.com research article 341 The role of neoadjuvant chemotherapy in patients with advanced (stage IIIC) epithelial ovarian cancer Erik Škof 1, Sebastjan
Radiology and Oncology Ljubljana Slovenia www.radioloncol.com research article 341 The role of neoadjuvant chemotherapy in patients with advanced (stage IIIC) epithelial ovarian cancer Erik Škof 1, Sebastjan
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC. Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy
 PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf
 MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
J Clin Oncol 26: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 26 NUMBER 1 JANUARY 1 2008 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Tumor Residual After Surgical Cytoreduction in Prediction of Clinical Outcome in Stage IV Epithelial Ovarian Cancer:
VOLUME 26 NUMBER 1 JANUARY 1 2008 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Tumor Residual After Surgical Cytoreduction in Prediction of Clinical Outcome in Stage IV Epithelial Ovarian Cancer:
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer
 Non-Small Cell Lung Cancer") Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Maintenance paradigm in non-squamous NSCLC
 Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
ESMO SUMMIT AFRICA. Latest evidence and current standard of care in advanced ovarian cancer. C.Sessa. Cape Town February 2018
 ESMO SUMMIT AFRICA Latest evidence and current standard of care in advanced ovarian cancer C.Sessa IOSI, Bellinzona, CH Cape Town 14-16 February 2018 CONFLICT OF INTEREST DISCLOSURE None Ovarian carcinoma
ESMO SUMMIT AFRICA Latest evidence and current standard of care in advanced ovarian cancer C.Sessa IOSI, Bellinzona, CH Cape Town 14-16 February 2018 CONFLICT OF INTEREST DISCLOSURE None Ovarian carcinoma
How to fight a silent killer: Lessons learned from Ovarian Cancer. Stephen A. Cannistra, M.D.
 How to fight a silent killer: Lessons learned from Ovarian Cancer Stephen A. Cannistra, M.D. How to fight a silent killer: Lessons learned from Ovarian Cancer Ovarian cancer is not common but is highly
How to fight a silent killer: Lessons learned from Ovarian Cancer Stephen A. Cannistra, M.D. How to fight a silent killer: Lessons learned from Ovarian Cancer Ovarian cancer is not common but is highly
Background. TAP, Paclitaxel + Doxorubicin + Cisplatin
 A randomized phase II study of paclitaxel/carboplatin/bevacizumab, paclitaxel/carboplatin/temsirolimus and ixabepilone/carboplatin/bevacizumab as initial therapy for measurable stage III or IVA; stage
A randomized phase II study of paclitaxel/carboplatin/bevacizumab, paclitaxel/carboplatin/temsirolimus and ixabepilone/carboplatin/bevacizumab as initial therapy for measurable stage III or IVA; stage
Original Research. Open Access
 To cite: Milani A, Kristeleit R, McCormack M, et al. Switching from standard to dose-dense chemotherapy in front-line treatment of advanced ovarian cancer: a retrospective study of feasibility and efficacy.
To cite: Milani A, Kristeleit R, McCormack M, et al. Switching from standard to dose-dense chemotherapy in front-line treatment of advanced ovarian cancer: a retrospective study of feasibility and efficacy.
New Treatments for Early Ovarian Cancer. Jonathan Ledermann UCL Cancer Institute University College London
 New Treatments for Early Ovarian Cancer Jonathan Ledermann UCL Cancer Institute University College London Lucerne Oct 213 Progression-free survival in first-line trials of platinum-based chemotherapy 1998
New Treatments for Early Ovarian Cancer Jonathan Ledermann UCL Cancer Institute University College London Lucerne Oct 213 Progression-free survival in first-line trials of platinum-based chemotherapy 1998
J Clin Oncol 25: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 25 NUMBER 24 AUGUST 20 2007 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Prognostic Factors for Stage III Epithelial Ovarian Cancer: A Gynecologic Oncology Group Study William E. Winter
VOLUME 25 NUMBER 24 AUGUST 20 2007 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Prognostic Factors for Stage III Epithelial Ovarian Cancer: A Gynecologic Oncology Group Study William E. Winter
symposium article Optimal primary therapy of ovarian cancer M. A. Bookman* introduction symposium article
 Annals of Oncology 27 (Supplement 1): i58 i62, 2016 doi:10.1093/annonc/mdw088 Optimal primary therapy of ovarian cancer M. A. Bookman* Arizona Oncology and US Oncology Research, Tucson, AZ, USA Background:
Annals of Oncology 27 (Supplement 1): i58 i62, 2016 doi:10.1093/annonc/mdw088 Optimal primary therapy of ovarian cancer M. A. Bookman* Arizona Oncology and US Oncology Research, Tucson, AZ, USA Background:
非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和
 資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
Two Cycles of Chemoradiation: 2 Cycles is Enough. Concurrent Chemotherapy / RT Regimens
 1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse?
 Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Epithelial Ovarian Cancer
 Epithelial Ovarian Cancer GYNE/ONC Practice Guideline Dr. Alex Hammond Dr. Ian Kerr Dr. Akira Sugimoto Dr. Stephen Welch Kay Faroni Christine Gawlik Kerri Thornton Approval Date: This guideline is a statement
Epithelial Ovarian Cancer GYNE/ONC Practice Guideline Dr. Alex Hammond Dr. Ian Kerr Dr. Akira Sugimoto Dr. Stephen Welch Kay Faroni Christine Gawlik Kerri Thornton Approval Date: This guideline is a statement
TREATMENT FOR RELAPSING PLATINUM SENSITIVE EPITHELIAL OVARIAN CANCER
 TREATMENT FOR RELAPSING PLATINUM SENSITIVE EPITHELIAL OVARIAN CANCER Sandro Pignata, MD, PhD Sabrina Chiara Cecere, MD Uro-Gynecological Department, Division of Medical Oncology, IRCCS National Cancer
TREATMENT FOR RELAPSING PLATINUM SENSITIVE EPITHELIAL OVARIAN CANCER Sandro Pignata, MD, PhD Sabrina Chiara Cecere, MD Uro-Gynecological Department, Division of Medical Oncology, IRCCS National Cancer
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
A Phase 2 Trial of Voreloxin (SNS-595) in Platinum - Resistant Epithelial Ovarian Cancer
 in Platinum - Resistant Epithelial Ovarian Cancer") A Phase Trial of Voreloxin (SNS-595) in Platinum - Resistant Epithelial varian Cancer William McGuire, M.D. Medical Director Harry and Jeanette Weinberg Cancer Institute November 6, 008 1 Voreloxin: First-In-Class
A Phase Trial of Voreloxin (SNS-595) in Platinum - Resistant Epithelial varian Cancer William McGuire, M.D. Medical Director Harry and Jeanette Weinberg Cancer Institute November 6, 008 1 Voreloxin: First-In-Class
Targeted Molecular Therapy Gynaecological Cancer Where are we now?
 Targeted Molecular Therapy Gynaecological Cancer Where are we now? 0 T O M D E G R E V E S U B - S P E C I A LT Y F E L L O W G Y N A E C O L O G I C A L O N C O L O G Y U N I V E R S I T Y O F P R E T
Targeted Molecular Therapy Gynaecological Cancer Where are we now? 0 T O M D E G R E V E S U B - S P E C I A LT Y F E L L O W G Y N A E C O L O G I C A L O N C O L O G Y U N I V E R S I T Y O F P R E T
North of Scotland Cancer Network Clinical Management Guideline for Cancer of the Ovary
 North of Scotland Cancer Network Cancer of the Ovary Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by NOSCAN Gynaecology Cancer
North of Scotland Cancer Network Cancer of the Ovary Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by NOSCAN Gynaecology Cancer
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER. Virginie Westeel Chest Disease Department University Hospital Besançon, France
 PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
Maintenance Therapy for Advanced NSCLC: Which Patients, Which Approach?
 Maintenance Therapy for Advanced NSCLC: Which Patients, Which Approach? Mark A. Socinski, MD Visiting Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology
Maintenance Therapy for Advanced NSCLC: Which Patients, Which Approach? Mark A. Socinski, MD Visiting Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology
Original Research. Background
 Original Research 849 in Carboplatin and Dose-Dense Paclitaxel Chemotherapy for Ovarian Malignancies: A Survey of NCCN Member Institutions Marina Stasenko, MD a ; R. Kevin Reynolds, MD a ; Carolyn Johnston,
Original Research 849 in Carboplatin and Dose-Dense Paclitaxel Chemotherapy for Ovarian Malignancies: A Survey of NCCN Member Institutions Marina Stasenko, MD a ; R. Kevin Reynolds, MD a ; Carolyn Johnston,
Avastin NAME OF THE MEDICINE DESCRIPTION PHARMACOLOGY. bevacizumab (rch)
") NAME OF THE MEDICINE Avastin bevacizumab (rch) CAS 216974-75-3 Bevacizumab is an immunoglobulin G (IgG) composed of two identical light chains, consisting of 214 amino acid residues and two 453 residue
NAME OF THE MEDICINE Avastin bevacizumab (rch) CAS 216974-75-3 Bevacizumab is an immunoglobulin G (IgG) composed of two identical light chains, consisting of 214 amino acid residues and two 453 residue
Biomarker for Response and Resistance in Ovarian Cancer
 2016 대한부인종양학회제 31 차춘계학술대회 New Trends in Translational Research Biomarker for Response and Resistance in Ovarian Cancer Shin-Wha Lee, M.D., Ph.D. Department of Obstetrics and Gynecology ASAN Medical Center
2016 대한부인종양학회제 31 차춘계학술대회 New Trends in Translational Research Biomarker for Response and Resistance in Ovarian Cancer Shin-Wha Lee, M.D., Ph.D. Department of Obstetrics and Gynecology ASAN Medical Center
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
The OReO Study. Study design & Protocol Study design Key Inclusion criteria Patient population Recruitment and retention tools
 The OReO Study A Phase IIIb, Randomised, Double-blind, Placebo-controlled, multi-centre Study of Olaparib Maintenance Re-treatment in Patients with Epithelial Ovarian Cancer Previously treated with a and
The OReO Study A Phase IIIb, Randomised, Double-blind, Placebo-controlled, multi-centre Study of Olaparib Maintenance Re-treatment in Patients with Epithelial Ovarian Cancer Previously treated with a and
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
A Gynecologic Cancer Intergroup Study of the NCIC Clinical Trials Group (NCIC CTG), the European Organization for Research and
, the European Organization for Research and") Randomized study of sequential cisplatintopotecan/carboplatin-paclitaxel versus carboplatin-paclitaxel: effects on quality of life A Gynecologic Cancer Intergroup Study of the NCIC Clinical Trials Group
Randomized study of sequential cisplatintopotecan/carboplatin-paclitaxel versus carboplatin-paclitaxel: effects on quality of life A Gynecologic Cancer Intergroup Study of the NCIC Clinical Trials Group
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Dr Sarah Mc Kenna, Consultant Medical Oncologist and Dr Joanne Millar, Consultant Medical Oncologist
 Title: Systemic Anti-Cancer Therapy (SACT) Guidelines for Ovarian Cancer Author(s) Ownership: Approval by: Operational Date: Dr Sarah Mc Kenna, Consultant Medical Oncologist and Dr Joanne Millar, Consultant
Title: Systemic Anti-Cancer Therapy (SACT) Guidelines for Ovarian Cancer Author(s) Ownership: Approval by: Operational Date: Dr Sarah Mc Kenna, Consultant Medical Oncologist and Dr Joanne Millar, Consultant
Medical Therapies in Ovarian Cancer The Arabic Perspectives. Mezghani Bassem -Tunisia
 Tunisian Health System: Social Welfare with a Public insurance for all citizens including Indigent persons. (± Additional private insurance) Choice: Public Hospital/Private Clinics (Indigents Public H)
Tunisian Health System: Social Welfare with a Public insurance for all citizens including Indigent persons. (± Additional private insurance) Choice: Public Hospital/Private Clinics (Indigents Public H)
1st line chemotherapy and contribution of targeted agents
 ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER 1st line chemotherapy and contribution of targeted agents Yi-Long Wu Guangdong Lung Cancer Institute Guangdong General Hospital Guangdong Academy
ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER 1st line chemotherapy and contribution of targeted agents Yi-Long Wu Guangdong Lung Cancer Institute Guangdong General Hospital Guangdong Academy
DATE: 22 May 2013 CONTEXT AND POLICY ISSUES
 TITLE: Intraperitoneal versus Intravenous Chemotherapy for the Treatment of Ovarian Cancer: A Review of the Comparative Clinical Evidence, Safety, Cost- Effectiveness, and Guidelines DATE: 22 May 2013
TITLE: Intraperitoneal versus Intravenous Chemotherapy for the Treatment of Ovarian Cancer: A Review of the Comparative Clinical Evidence, Safety, Cost- Effectiveness, and Guidelines DATE: 22 May 2013
Adjuvant Chemotherapy
 State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
Immune Therapy in Clear Cell Ovarian Cancer (ITICC) Hal Hirte Canadian Cancer Clinical Trials Group
 Hal Hirte Canadian Cancer Clinical Trials Group") Immune Therapy in Clear Cell Ovarian Cancer (ITICC) Hal Hirte Canadian Cancer Clinical Trials Group Results of Phase II Study of Durvalumab and Tremelimumab in recurrent clear cell ovarian cancer Trial
Immune Therapy in Clear Cell Ovarian Cancer (ITICC) Hal Hirte Canadian Cancer Clinical Trials Group Results of Phase II Study of Durvalumab and Tremelimumab in recurrent clear cell ovarian cancer Trial
Gynecologic Oncology
 Gynecologic Oncology 124 (2012) 10 14 Contents lists available at SciVerse ScienceDirect Gynecologic Oncology journal homepage: www.elsevier.com/locate/ygyno An analysis of patients with bulky advanced
Gynecologic Oncology 124 (2012) 10 14 Contents lists available at SciVerse ScienceDirect Gynecologic Oncology journal homepage: www.elsevier.com/locate/ygyno An analysis of patients with bulky advanced
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016