GLANDULAR LESIONS PITFALLS IN MANAGEMENT. Dr Li Wai Hon HKSCCP The 15 th Anniversary Symposium 10 December 2016
|
|
|
- Elfreda Thomas
- 6 years ago
- Views:
Transcription
1 GLANDULAR LESIONS PITFALLS IN MANAGEMENT Dr Li Wai Hon HKSCCP The 15 th Anniversary Symposium 10 December 2016
2 Introduction Cervical glandular lesions are much less common than squamous lesion Incidence increasing, particularly in young women Invasive adenocarcinoma accounted for only 5% of cervical cancer cases in 1950s and 1960s Increased to 20-25% Up to 30% in young women < 35 yrs of age Adenocarcinoma-in-situ (AIS) Precursor of invasive adenocarcinoma Age range yrs, mean yrs AIS 15 yrs younger than adenocarcinoma Incidence ratio of AIS to CIN 3 reported as 1:26 to 1:237 Mixed disease 46%-72% AIS or invasive adenocarcinoma coexist with squamous lesion
3 Challenges in Management of Cervical Glandular Abnormalities Screening Cytology less sensitive in detecting glandular dysplasia Diagnosis Colposcopic features of AIS / adenocarcinoma subtle and non-specific Choice of diagnostic excisional procedures Cold knife conization vs Loop excision (LEEP) Achieve negative margins Management of AIS after diagnostic excisional procedure Hysterectomy vs Conservative treatment when future fertility is desired Surveillance protocol for patient opted for conservative management Endocervical versus endometrial origin of adenocarcinoma
4 Screening - Cytology 2014 Bethesda Nomenclature for Glandular Abnormalities Atypical Endocervical cells (NOS or specify in comments) Endometrial cells (NOS or specify in comments) Glandular cells (NOS or specify in comments) Atypical Endocervical cells, favor neoplastic Glandular cells, favor neoplastic Endocervical adenocarcinoma in situ Adenocarcinoma Endocervical Endometrial Extrauterine Not otherwise specified (NOS)
5 Screening - Cytology Cervical cytology is generally less sensitive in detecting glandular abnormalities compared to squamous lesions Differentiate high-grade squamous cells vs glandular cells Mimickers: endometrial cells, reactive endocervical cells, tubal metaplasia, cervical endometriosis Cytology results just prior to diagnosis of AIS: Glandular Only 38%-69% Squamous 26-31% Mixed squamous and glandular 15% Negative 4% Most glandular lesions are recognized in the course of the evaluation of women with abnormal squamous cytology 60% AIS buried under normal metaplastic or dysplastic squamous epithelium making the glandular component inaccessible to cytological sampling
6 Atypical Glandular Cells (AGC) < 0.5% of all cervical cytology ~50% coexist with squamous cytological abnormality (ASC / SIL) ~30% associated with premalignant or malignant disease Not specific to glandular cervical neoplasia
7 Possible Histological Diagnosis after AGC Histology Rates Comments Squamous Intraepithelial Lesions (SIL) Low-grade CIN 1 9% High-grade CIN % SCC 0.3-1% 20-28% Most are squamous (high-grade) rather than glandular Coexist with glandular lesions Adenocarcinoma-in-situ (AIS) 3-4% ~50% coexist with CIN Cervical Adenocarcinoma 1-2% Endometrial Hyperplasia 1% Endometrial Carcinoma 2-3% Ovarian Cancer % Others: fallopian tubes, metastatic (e.g. colon, breast) Benign 64-71% Reactive or reparative changes Cervical polyps Microglandular hyperplasia associated with OCPs Endocervical changes associated with IUD Tubal metaplasia Cervical endometriosis Arias-Stella reaction (pregnancy change) Geier CS, Wilson M, Creasman W. Clinical evaluation of atypical glandular cells of undetermined significance. Am J Obstet Gynecol 2001; 184:64. Schnatz PF, Guile M, O'Sullivan DM, Sorosky JI. Clinical significance of atypical glandular cells on cervical cytology. Obstet Gynecol 2006; 107:701.
8 Significance of AGC Risk of neoplasia is higher when reported as AGC favor neoplasia or Endocervical AIS Subcategories Risks AGC-NOS 9%-41% invasive cancer, AIS or CIN 2-3 AGC-favor neoplasia 27-96% invasive cancer, AIS or CIN 2-3 Endocervical AIS 48-68% AIS 38% invasive cervical adenocarcinoma Atypical endometrial cells More than 1/3 have significant uterine disease 80% endometrial origin in post-menopausal women 13-18% endometrial cancer 6-7% high grade lesions and squamous carcinoma Risk of malignancy with ACG increase with age <40 yrs 2% (mostly cervical) yrs 2.8% >50 years 15% (predominant endometrial carcinoma) Zhao C, Florea A, Onisko A, Austin RM. Histologic follow-up results in 662 patients with Pap test findings of atypical glandular cells: results from a large academic womens hospital laboratory employing sensitive screening methods. Gynecol Oncol 2009; 114:383.
9 Management of Abnormal Glandular Cytology (AGC or AIS) All subcategories of AGC and AIS (except atypical endometrial calls) Atypical endometrial cells Colposcopy Endocervical sampling (except pregnancy) Endometrial and Endocervical sampling Endometrial sampling (if >=35 yrs or at risk for endometrial cancer) (except pregnancy) Colposcopy (if no endometrial pathology) Triage by reflex HPV testing is not recommended Although cervical adenocarcinoma is HPV related, endometrial cancer is not, so reflex HPV testing does not identify a subgroup of women who need less invasive assessment Triage using repeat cervical cytology is unacceptable
10 Early Diagnosis of AIS A Challenge Unreliable cytology Unreliable colposcopy Colposcopic features of AIS more subtle than CIN and difficult to differentiate from metaplasia or other mimickers (require histology) Disease buried underneath normal or dysplastic squamous epithelium Small lesion size 48% only involve one quadrant of the cervix Skip (multifocal) lesions in 13%-17%
11 Colposcopic Features of Glandular Lesions - Pitfalls No single appearance characterizes glandular lesions (AIS or adenocarcinoma) non-specific Generally accepted colposcopic criteria for grading squamous lesions do not apply to glandular lesions Squamous lesions - Vascular pattern, inter-capillary distance, surface contour, colour tone, demarcations Glandular lesions - The degree of acetowhiteness reflects the degree of villous fusion (the more fusion, the whiter the lesion) and the histologic pseudostratification of columnar cells with their enlarged hyperchromatic nuclei Features of AIS overlap with squamous lesions, immature squamous metaplasia and other mimickers When glandular and squamous lesions co-exist (46-72%), the squamous component (80% high-grade) is more likely to be visible colposcopically
12 Three Common Colposcopic Appearance of Glandular Disease Papillary expression resembling an immature transformation zone Fused papillae in discrete AW patches, varying in size Look like fused villous processes of early, normal metaplasia Flat, variegated red and white area resembling an immature transformation zone (rather than uniform dense AW in high-grade squamous lesions) One or more isolated, elevated, individual, densely AW lesions overlying columnar epithelium

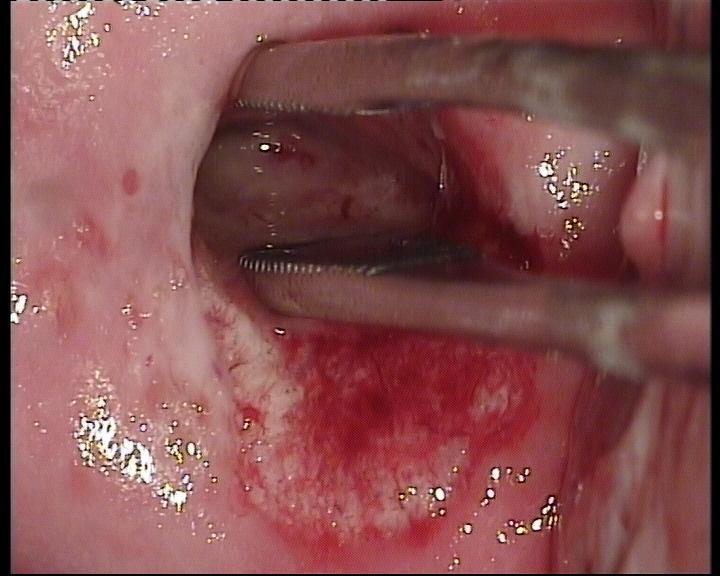
13 Papillary Expression Individual or fused villi / papillae in discrete AW patches, varying in size AIS AIS F28 Atypical endocervical cells NOS, ASCUS Atypical vessel Abnormal papillary coalescence Prominent atypical vessels, particularly associated with early invasion


14 Papillary Expression - Mimickers Glandular disease vs squamous metaplasia Fusion / coalescence of villi in both squamous metaplasia and AIS Surface distribution of normal metaplastic epithelium and AIS are similar Vessels of central villous core appear as dots when viewed end on Fusion of villi does not occur in CIN AIS Metaplasia


15 Papillary Expression Epithelial Budding Fused AW papillae Metaplasia AIS F40 AGC NOS Look like fused villous processes of early, normal metaplasia

16 Papillary Proliferations - Mimickers Adenocarcinoma Condyloma Acuminata (Wart) F68 Atypical endocervical cells NOS Fusion of villi Fine and finger-like papillae Fusion of villi Each papillae has central capillary loop of afferent and efferent blood vessel single or multiple dots in the tips Multiple warty lesions in genital tract



17 Papillary Proliferations - Mimickers Adenocarcinoma Condyloma Acuminata (Wart) F68 Atypical endocervical cells NOS F45 LSIL Fusion of villi Necrosis Fusion of villi F27 LSIL



18 Flat, Variegated Red and White area AIS / Adenocarcinoma F40 AGC AIS Fused papillae AIS CIN - Uniform Dense AW



19 One or More Isolated Densely AW Lesions Overlying Columnar Epithelium AIS Columnar epithelium AIS Variegated red and white Columnar epithelium F40 AGC F28 Atypical endocervical cells NOS, ASCUS Coalescence of papillae

20 Large Gland or Crypt Openings Associated with excessive mucus, together with other abnormal colposcopic features Variegated red and white Large gland or crypt openings
 squamous lesions do not skip, they are always contiguous")
21 Mixed Disease The presence of two or more squamous lesions separated by glandular-appearing epithelium is highly suggestive of a glandular lesion Squamous Glandular Squamous Primary (i.e. not post treatment) squamous lesions do not skip, they are always contiguous



22 Mixed Disease F45 Cytology AGC, favor neoplasia Mosaic pattern Biopsy CIN Endocervical sampling - AIS Endocervical adenocarcinoma CIN 3 Fused AW villi



23 Vascular Patterns Punctuation, mosaic pattern, corkscrew vessels although common in squamous lesions, do not appear in glandular disease Mosaic Punctation CIN 3 Corkscrew Central core vessels entrapped within dysplastic squamous epithelium


24 Vascular Patterns AIS Single or multiple dot formations as seen in the tips of the papillary projections AIS F28 Atypical endocervical cells NOS, ASCUS Formed by vessels that course through the villous projections and bend sharply in their tips


25 Atypical Vessels Squamous Cell Carcinoma Corkscrew-like vessels Waste-thread-like vessels (dropping a piece of thread on the floor) Tendril-like vessels (climbing plants that reach for and then spiral around surrounding structures)


")


26 Atypical Vessels Adenocarcinoma Adenocarcinoma F40 AGC Tendril-like vessels (climbing plants that reach for and then spiral around surrounding structures) Waste-thread-like vessels (dropping a piece of thread on the floor) *Character-like vessels *Root-like vessels (tapering or bulging)
27 However, features of AIS can be very subtle




28 F36 Cytology - Endocervical AIS F55 Cytology Endocervical AIS Cone Biopsy AIS, CIN 3 Cone - AIS



29 F47 Cytology HSIL Biopsy Adenocarcinoma
30 Role of Colposcopy Despite the limitations, colposcopy is still important for the following reasons: To exclude clinically overt invasive carcinoma To assess transformation zone (TZ), the extent of the lesion, including any co-existing squamous disease, and obtain biopsy to guide treatment Biopsy is required in all cases to confirm the diagnosis
31 Management after Colposcopy Subsequent management depends on: Initial cytology, colposcopy and biopsy results Biopsy Invasive Cancer Biopsy AIS Initial cytology AGC-favor neoplasia or Endocervical AIS Initial cytology AGC NOS Biopsy: No significant pathology Manage Accordingly Diagnostic Excisional Procedure * Follow Up Cytology / Cotest
32 Diagnostic Excisional Procedure Required in all women with AIS / suspected AIS before making any subsequent management decisions: To exclude adenocarcinoma Still ~1% risk of adenocarcinoma for negative margins Aim to achieve an interpretable negative margin Positive margin is associated with high risk of residual / persistent disease and recurrence, even adenocarcinoma Should be cylindrical and deep enough to account for the extent of the lesion, depth of crypt involvement and long enough to encompass the length of the disease Avoid thermal injury / distortion to the specimen especially the apex Further management decisions based on a thorough histological assessment, especially margin status
33 Importance of Margins Status Meta-analysis evaluating predictive value of conization margin status (n=1278, 33 studies) Cold knife cone (CKC), LEEP or laser conization Overall 34.4% margins positive Post-Conization Positive Margins Negative Margins Overall Patients underwent secondary excision (Re-Cone/Hysterectomy), n=607 Residual AIS 52.8% (180/341) 20.3% (54/266) 38.6% (234/607) Adenocarcinoma 5% (17/341) 1.5% (4/266) 3.5% (21/607) Patients treated conservatively, n=671 Recurrence AIS 19.4% (19/98) 2.6% (15/573) 5.1% (34/671) Subsequent Adenocarcinoma 6.1% (6/98) 0.3% (2/573) 1.2% (8/671) Overall, n=1278 Adenocarcinoma 5.2% (23/439) 0.7% (6/839) 2.3% (29/1278) Salani R et al. Adenocarcinoma in situ of the uterine cervix: a metaanalysis of 1278 patients evaluating the predictive value of conization margin status. Am J Obstet Gynecol 2009;200:182.e1-5
34 Extent of Excision - Individualized Tailored according to the colposcopic findings, age of the patient and childbearing requirements For young women, colposcopically visible SCJ More limited excision of the endocervix (i.e. 1cm above SCJ) may be reasonable in women aged less than 36 years Unlikely to have disease extending more than 10 mm from the SCJ For older women, or where the SCJ is not visible at colposcopy A cylindrical biopsy should be taken that includes all of the visible TZ and 20mm to 25mm of the endocervical canal Proximal linear extent of AIS may be as far as 25 mm from the SCJ Avoid thermal artefact to improve margins assessment NHS Cervical Screening Program. Colposcopy and Programme Management. Third Edition March 2016
35 Choice of Diagnostic Excisional Procedures Margin status and interpretation of margins are critical to future treatment planning especially in patients wishing to preserve fertility Cold Knife Cone (CKC) Obtained in one piece Larger depth and width LEEP Obtained in several pieces Thermal artifact at the edges obscuring assessment The mucus in glandular mucosa provides less resistance to electric current Laser Conization Size comparable to CKC but also results in thermal artefacts Specialized training and equipment
36 Cold Knife Cone (CKC) or LEEP? Most retrospective cohort studies have shown that CKC to be superior to LEEP in achieving negative margins in AIS CKC - 17%-25% positive margins LEEP % positive margins Meta-analysis by Salani et al 2009 Of the 14 studies reporting the type of excisional procedure used, 9 (64.3%) reported that CKC resulted in a higher rate of negative margins than LEEP and improved or equivalent rates over laser conization Kennedy AW et al. Further study of the management of cervical adenocarcinoma in situ. Gynecol Oncol 2002;86: Bull-Phelps SL et al. Fertility sparing surgery in 101 women with adenocarcinoma in situ of the cervix. Gynecol Oncol 2007;107: Latif NA et al. Management of Adenocarcinoma In Situ of the Uterine Cervix: A Comparison of Loop Electrosurgical Excision Procedure and Cold Knife Conization. Lower Gen Tract Dis 2015;19: Munro A et al. Comparison of cold knife cone biopsy and loop electrosurgical excision procedure in the management of cervical adenocarcinoma in situ: What is the gold standard? Gyn Onco 137 (2015)
37 Cold Knife Cone (CKC) or LEEP? Cold knife cone (CKC) was considered the gold standard Up to 50% AIS are diagnosed after loop excision Subsequent management controversial proceed to cold-knife cone regardless of margin However, conventional management by CKC has been challenged: Historically, AIS is thought to be a lesion of the endocervical canal with skip - lesions. However: Multifocal disease is found in only 13% 17% of cases The lesion is usually unicentric, contiguous with the SCJ, and extends up the canal for a variable distance Recent data suggest similar risk of positive margins and oncological outcome after CKC or LEEP Advantages of LEEP over CKC Avoidance of general anaesthesia Treatment in outpatient setting Lower morbidity Reduce obstetric complications (2nd trimester miscarriage and preterm delivery), especially for young patients wishing to preserve fertility
38 Cold Knife Cone (CKC) or LEEP? Most are retrospective studies Selection bias Prospective study is required to determine the oncological outcome and safety Study LEEP vs CKC Comments Latif et al 2015, n=115 Positive margins (20% vs 17%) Invasive cancer (3.3% vs 4.2%) Recurrence of AIS (6.7% vs 8.3%) Subsequent adenocarcinoma (0 vs 2.0%) Mean specimen volume (3.0 vs 4.3cm3) No significant difference Use of larger loop when AIS is known Munro et al 2015, n=338 Positive margins (31.8% vs 25.5%) ACIS persistence and/or recurrence Specimen depth No significant difference Hanegem et al 2012, aged <30, n= 112 Positive margins (27% vs 21%) Residual disease (21.4% vs 27.3%) Recurrent (0%) No significant difference Clinicians tends to treat smaller lesion with LEEP, larger lesions by CKC Latif NA et al. Management of Adenocarcinoma In Situ of the Uterine Cervix: A Comparison of Loop Electrosurgical Excision Procedure and Cold Knife Conization. Lower Gen Tract Dis 2015;19: Munro A et al. Comparison of cold knife cone biopsy and loop electrosurgical excision procedure in the management of cervical adenocarcinoma in situ: What is the gold standard? Gyn Onco 137 (2015) Hanegem et al. Fertility-sparing treatment in younger women with adenocarcinoma in situ of the cervix. Gyn Oncol 124 (2012) 72 77
39 Guidelines ASCCP Guidelines 2001 Cold-knife cone favored over loop excision 2012 Diagnostic excision using any modality, but care must be taken to: Keep specimen intact and margins interpretable Avoid fragmentation, including top-hat serial endocervical excisions May require larger loops British NHS Cervical Screening Program 2016 Excisional Procedure individualized age and colposcopic findings Australian Cervical Screening Program 2005 Cold-knife cone biopsy should be considered the gold standard HKCOG 2016 Cold-knife cone is recommended
40 Management of AIS after Diagnostic Excisional Procedure Total hysterectomy - treatment of choice for women who have completed childbearing Unable to predict the risk of residual disease or recurrence using the same conventional clinicopathological features for squamous lesions: Colposcopic changes associated with AIS can be minimal, so determining the limits of a lesion can be difficult AIS frequently extends into the endocervical canal, complicating determination of the desired depth of excision AIS can be multifocal and discontinuous, so negative margins on an excision specimen do not provide assurance Post Excisional Procedure Positive Margins Negative Margins Residual AIS 52.8% 20.3% Adenocarcinoma 5.2% 0.7% Difficulties of reliable cytological follow up Salani R et al. Adenocarcinoma in situ of the uterine cervix: a metaanalysis of 1278 patients evaluating the predictive value of conization margin status. Am J Obstet Gynecol 2009;200:182.e1-5
41 Conservative Fertility Sparing Management Mean age of AIS yrs Acceptable option - understands that up to 20% residual disease and small risk of cancer (0.7%) even if excision margins are negative Re-excision is indicated for positive margins Up to 60% residual disease ~6% invasive disease Conservative management for patients with positive excisional margins who decline re-excision should be undertaken with caution Require close follow-up even if margins negative Surveillance Negative HPV test after treatment identifies women at low risk for persistent or recurrent AIS Compliance to follow up
42 Follow Up - HPV DNA Testing The safety of conservative management of AIS depends on the accuracy of screening method utilized in predicting the residual disease High-risk HPV DNA was detected in 93% cervical adenocarcinoma (mostly HPV 16/18) HPV 16 most frequent (South East Asia HPV 18 predominant) HPV 18 more prevalent in adenocarcinoma (39%) than squamous cell carcinoma (18%) Combination of cytology and HPV test advantage over cytology alone for early detection of patients at increased risk of recurrence and progression Castellsagué et al. Worldwide Human Papillomavirus Etiology of Cervical Adenocarcinoma and Its Cofactors: Implications for Screening and Prevention. J Natl Cancer Inst Mar 1;98(5):
43 Follow Up - HPV DNA Testing Costa et al 2007, n=42, margins clear = 21, mean FU 40 months AIS underwent conservative treatment (CKC / LEEP / LASER Cone) FU using colposcopy, PAP smear, ECC +/- biopsy and HPV testing (HC II) repeated at 6-monthly interval HPV testing significantly predicted disease persistence / clearance at the 1 st FU visit with OR 12.6 ( ) Predictive power of PAP smear (OR ) did not reach statistical significance at any of the FU visits Combination of PAP smear and HPV testing: NPV of 100% seems to be very useful in prevent unnecessary hysterectomies PAP + HPV Test Sensitivity Specificity PPV NPV 1 st FU (at 6 month) 90% 50% 52.9% 88.9% 2 nd FU (at 12 month) 100% 52.6% 40% 100% S Costa et al. Human papillomavirus (HPV) test and PAP smear as predictors of outcome in conservatively treated adenocarcinoma in situ (AIS) of the uterine cervix. Gynecol Oncol 2007;106:
44 Management Algorithm for AIS after Diagnostic Excisional Procedure Completed childbearing Future fertility is desired Margins involved or ECC positive for CIN or AIS Margins Negative Hysterectomy is preferred Re-excision to achieve complete excision (preferred) Declined re-excision 6 / 12/ 18 months Cytology / Cotesting +/- Colposcopy ASCCP 2012 NHS Cervical Screening Program 2016 Long Term Follow Up / Hysterectomy






45 Don t forget to exclude pelvic pathology if no lesion identified AGC AGC-Endometrial Cells All Subcategories (except AGC endometrial cells) Endometrial Sampling Colposcopy + Biopsy + Endocervical Sampling Positive Negative Lesion Identified No Lesion Endometrial Sampling if not already performed Refer for Treatment (if a local excisional procedure is indicated and the original cytology is AGC favour neoplasia, a cold knife cone is recommended) No Lesion Ultrasound pelvis to exclude adnexal pathology AGC favour neoplasia Diagnostic Excisional Conization Abnormal cytology No lesion Endocervical AIS AGC NOS Repeat cytology 6 monthly 4 consecutive normal cytology Normal Screening
46 Pitfalls in the Diagnosis of Invasive Adenocarcinoma in Cervical Biopsy Non-cervical adenocarcinoma, especially endometrial cancer with cervical involvement Share similar histologic types Clinical presentation and imaging is important Histologic clues to the origin include: AIS / CIN - favours endocervical origin Endometrial hyperplasia - endometrial origin Immunohistochemistry
47 Endocervical vs Endometrial Adenocarcinoma with Cervical Involvement Immunohistochemistry Endocervical Adenocarcinoma Endometrial Adenocarcinoma with Cervical Involvement p ISH HPV + - CEA + - ER / PR - + Vimentin - + Pitfalls: ER & PR can vary in both p16 useful, however: p16 also strongly and diffusely positive in high grade serous, some undifferentiated and high grade endometrioid adenocarcinoma p53 diffusely positive in high-grade endometrial adenocarcinomas and metastatic high-grade tubal or ovarian adenocarcinomas involving the cervix, while primary cervical neoplasm should only show weak and heterogeneous staining ISH HPV can be negative in unusual endocervical adenocarcinoma e.g. clear cell, minimal deviation adenocarcinoma, serous, MMMT
48 Conclusion Cytology is less sensitive in detecting glandular dysplasia Colposcopic features of AIS / adenocarcinoma is subtle and non-specific Diagnostic excisional biopsy should be performed when AIS is found on punch biopsy or suspected cytologically to exclude adenocarcinoma Should achieve an interpretable negative margin High risk of residual disease and carcinoma if margins positive Hysterectomy is the treatment of choice for AIS who have completed childbearing Because of risk of residual disease and occult carcinoma even if excisional margins are clear Conservative management is an option when future fertility is desired Understood the possibility of persistent / recurrent disease and small chance of adenocarcinoma even if excisional margins are clear Good compliance to follow up Don t forget to exclude other pelvic malignancy if no lesion is found Differentiate between endocervical adenocarcinoma and endometrial adenocarcinoma with cervical involvement
49 Thank You
Colposcopy. Attila L Major, MD, PhD
 Colposcopy Attila L Major, MD, PhD Histology Colposcopy Cytology It has been estimated that annual Pap smear testing reduces a woman s chance of dying of cervical cancer from 4 in 1000 to about 5 in 10,000
Colposcopy Attila L Major, MD, PhD Histology Colposcopy Cytology It has been estimated that annual Pap smear testing reduces a woman s chance of dying of cervical cancer from 4 in 1000 to about 5 in 10,000
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines
 Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary
 Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary Glossary of Terms Colposcopy is the examination of the cervix, vagina and, in
Clinical Guidance: Recommended Best Practices for Delivery of Colposcopy Services in Ontario Best Practice Pathway Summary Glossary of Terms Colposcopy is the examination of the cervix, vagina and, in
Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two
 Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two Seshu P. Sarma, MD, FAAP Emory University Regional Training Center Atlanta, Georgia Produced by the Alabama Department of Public Health
Faculty Pap Smear Guidelines: Family Planning Update 2008 Part Two Seshu P. Sarma, MD, FAAP Emory University Regional Training Center Atlanta, Georgia Produced by the Alabama Department of Public Health
Becoming a colposcopist: Colposcope case studies
 Becoming a colposcopist: Colposcope case studies Seon-Kyung Lee, M.D. Department of Obstetrics and Gynecology College of Medicine, Kyung Hee University Value of Colposcopy Cytology is an effective screening
Becoming a colposcopist: Colposcope case studies Seon-Kyung Lee, M.D. Department of Obstetrics and Gynecology College of Medicine, Kyung Hee University Value of Colposcopy Cytology is an effective screening
Understanding Your Pap Test Results
 Understanding Your Pap Test Results Most laboratories in the United States use a standard set of terms called the Bethesda System to report pap test results. Normal: Pap samples that have no cell abnormalities
Understanding Your Pap Test Results Most laboratories in the United States use a standard set of terms called the Bethesda System to report pap test results. Normal: Pap samples that have no cell abnormalities
Making Sense of Cervical Cancer Screening
 Making Sense of Cervical Cancer Screening New Guidelines published November 2012 Tammie Koehler DO, FACOG The incidence of cervical cancer in the US has decreased more than 50% in the past 30 years because
Making Sense of Cervical Cancer Screening New Guidelines published November 2012 Tammie Koehler DO, FACOG The incidence of cervical cancer in the US has decreased more than 50% in the past 30 years because
Treatment of Cervical Intraepithelial Neoplasia. Case. How would you manage this woman?
 Treatment of Cervical Intraepithelial Neoplasia Karen Smith-McCune Professor, Department of Obstetrics, Gynecology and Reproductive Sciences I have no conflicts of interest Case How would you manage this
Treatment of Cervical Intraepithelial Neoplasia Karen Smith-McCune Professor, Department of Obstetrics, Gynecology and Reproductive Sciences I have no conflicts of interest Case How would you manage this
!"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$
*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$") !"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$ Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
!"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$ Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
The society for lower genital tract disorders since 1964.
 The society for lower genital tract disorders since 1964. Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
The society for lower genital tract disorders since 1964. Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
Management Algorithms for Abnormal Cervical Cytology and Colposcopy
 Management Algorithms for Abnormal Cervical Cytology and Colposcopy Table of Contents Standard Colposcopic Definitions... 1 Guidelines for the Assessment of Abnormal Cervical Cytology... 2 Ia: Persistent
Management Algorithms for Abnormal Cervical Cytology and Colposcopy Table of Contents Standard Colposcopic Definitions... 1 Guidelines for the Assessment of Abnormal Cervical Cytology... 2 Ia: Persistent
Cervical Dysplasia and HPV
 Cervical Dysplasia and HPV J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse HPV Double stranded DNA virus The HPV infect epithelial cells of the skin and mucous membranes Highest risk
Cervical Dysplasia and HPV J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse HPV Double stranded DNA virus The HPV infect epithelial cells of the skin and mucous membranes Highest risk
Workshop for O& G trainees and paramedics 17 Dec 2011 Cytological Interpretation
 Workshop for O& G trainees and paramedics 17 Dec 2011 Cytological Interpretation May Yu Director of Cytology Laboratory Service Department of Anatomical & Cellular Pathology Prince of Wales Hospital Cervical
Workshop for O& G trainees and paramedics 17 Dec 2011 Cytological Interpretation May Yu Director of Cytology Laboratory Service Department of Anatomical & Cellular Pathology Prince of Wales Hospital Cervical
Managament of Abnormal Cervical Cytology and Histology
 Managament of Abnormal Cervical Cytology and Histology Ali Ayhan, M.D Başkent University Faculty of Medicine Department of Gynecology and Obstetrics Division of Gynecologic Oncology Abnormal Cytologic
Managament of Abnormal Cervical Cytology and Histology Ali Ayhan, M.D Başkent University Faculty of Medicine Department of Gynecology and Obstetrics Division of Gynecologic Oncology Abnormal Cytologic
HPV and Cervical Cancer, Screening and Prevention. John Ragsdale, MD July 12, 2018 CME Lecture Series
 HPV and Cervical Cancer, Screening and Prevention John Ragsdale, MD July 12, 2018 CME Lecture Series We have come a long Way Prevalence HPV in Young Adults in U.S HPV genotypes 55-60% of All cancers 20%
HPV and Cervical Cancer, Screening and Prevention John Ragsdale, MD July 12, 2018 CME Lecture Series We have come a long Way Prevalence HPV in Young Adults in U.S HPV genotypes 55-60% of All cancers 20%
Updated ASCCP Consensus Guidelines For Managing Diagnosed Cervical Cancer Precursors Michael A. Gold, M.D.
 Updated ASCCP Consensus Guidelines For Managing Diagnosed Cervical Cancer Precursors Michael A. Gold, M.D. 27 May, 2014 London, England Faculty Disclosure X No, nothing to disclose Yes, please specify
Updated ASCCP Consensus Guidelines For Managing Diagnosed Cervical Cancer Precursors Michael A. Gold, M.D. 27 May, 2014 London, England Faculty Disclosure X No, nothing to disclose Yes, please specify
I have no financial interests to disclose.
 Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics I have no financial interests
Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics I have no financial interests
Management of Abnormal Cervical Cytology and Histology
 Management of Abnormal Cervical Cytology and Histology Assoc. Prof. Gökhan Tulunay Etlik Zübeyde Hanım Women s Diseases Teaching & Research Hospital Gynecologic Oncology Clinic Universally accepted guideline
Management of Abnormal Cervical Cytology and Histology Assoc. Prof. Gökhan Tulunay Etlik Zübeyde Hanım Women s Diseases Teaching & Research Hospital Gynecologic Oncology Clinic Universally accepted guideline
Cervical Screening Results Leading to Detection of Adenocarcinoma in Situ of the Uterine Cervix
 DOI:10.31557/APJCP.2019.20.2.377 Cervical Screening Results Leading to Detecting Cervical AIS RESEARCH ARTICLE Editorial Process: Submission:09/27/2018 Acceptance:01/18/2019 Cervical Screening Results
DOI:10.31557/APJCP.2019.20.2.377 Cervical Screening Results Leading to Detecting Cervical AIS RESEARCH ARTICLE Editorial Process: Submission:09/27/2018 Acceptance:01/18/2019 Cervical Screening Results
CERVICAL INTRAEPITHELIAL NEOPLASIA (CIN)
") CERVICAL INTRAEPITHELIAL NEOPLASIA (CIN) The cervix constitutes the lower third of the uterus. It is in two parts, the endocervix and the ectocervix. Ectocervix is covered with squamous epithelium. Endocervix
CERVICAL INTRAEPITHELIAL NEOPLASIA (CIN) The cervix constitutes the lower third of the uterus. It is in two parts, the endocervix and the ectocervix. Ectocervix is covered with squamous epithelium. Endocervix
I have no financial interests in any product I will discuss today.
 Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Conization. 1
 Cervical Conization www.zohrehyousefi.com 1 Cone Biopsy is a surgical procedure with removal of a cone shaped portion of the cervix The extent of involvement of epithelium on the ectocervix has been clearly
Cervical Conization www.zohrehyousefi.com 1 Cone Biopsy is a surgical procedure with removal of a cone shaped portion of the cervix The extent of involvement of epithelium on the ectocervix has been clearly
ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests
 ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests www.treatmentok.com Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Ann Arbor, Michigan Disclosures
ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests www.treatmentok.com Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Ann Arbor, Michigan Disclosures
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines. June 2013
 Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
Dysplasia: layer of the cervical CIN. Intraepithelial Neoplasia. p16 immunostaining. 1, Cervical. Higher-risk, requires CIN.
 CLINICAL PRACTICE GUIDELINE Guideline Number: DHMP_DHMC_PG1015 Guideline Subject: Routine Cervical Cancer Screening Effective Date: 9/2018 Revision Date: 9/2019 Pages: 2 of 2 Quality Management Committee
CLINICAL PRACTICE GUIDELINE Guideline Number: DHMP_DHMC_PG1015 Guideline Subject: Routine Cervical Cancer Screening Effective Date: 9/2018 Revision Date: 9/2019 Pages: 2 of 2 Quality Management Committee
EU guidelines for reporting gynaecological cytology
 EU guidelines for reporting gynaecological cytology Amanda Herbert Guy s & St Thomas Foundation NHS Trust 5th EFCS Annual Tutorial, Trondheim, Norway 28 th May 1 st June 2012 EU guidelines aim to harmonize
EU guidelines for reporting gynaecological cytology Amanda Herbert Guy s & St Thomas Foundation NHS Trust 5th EFCS Annual Tutorial, Trondheim, Norway 28 th May 1 st June 2012 EU guidelines aim to harmonize
BC Cancer Cervix Screening 2015 Program Results. February 2018
 BC Cancer Cervix Screening 2015 Program Results BC Cancer Cervix Screening 2015 Program Results 2 Table of Contents BC Cancer Cervix Screening 2015 Program Results... 1 Table of Contents... 2 Program Overview...
BC Cancer Cervix Screening 2015 Program Results BC Cancer Cervix Screening 2015 Program Results 2 Table of Contents BC Cancer Cervix Screening 2015 Program Results... 1 Table of Contents... 2 Program Overview...
Cervical Cancer Screening. David Quinlan December 2013
 Cervical Cancer Screening David Quinlan December 2013 Cervix Cervical Cancer Screening Modest variation provincially WHO and UK begin at 25 stop at 60 Finland begin at 30 stop at 60 Rationale for
Cervical Cancer Screening David Quinlan December 2013 Cervix Cervical Cancer Screening Modest variation provincially WHO and UK begin at 25 stop at 60 Finland begin at 30 stop at 60 Rationale for
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis
 In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma
 Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
Eradicating Mortality from Cervical Cancer
 Eradicating Mortality from Cervical Cancer Michelle Berlin, MD, MPH Vice Chair, Obstetrics & Gynecology Associate Director, Center for Women s Health June 2, 2009 Overview Prevention Human Papilloma Virus
Eradicating Mortality from Cervical Cancer Michelle Berlin, MD, MPH Vice Chair, Obstetrics & Gynecology Associate Director, Center for Women s Health June 2, 2009 Overview Prevention Human Papilloma Virus
Chapter 10: Pap Test Results
 Chapter 10: Pap Test Results On completion of this section, the learner will be able to: 1. Identify how Pap test results are interpreted and the reasons for normal and abnormal results. 2. Describe the
Chapter 10: Pap Test Results On completion of this section, the learner will be able to: 1. Identify how Pap test results are interpreted and the reasons for normal and abnormal results. 2. Describe the
Cervical Cancer Screening Update. Melissa Hartman, DO Women s Health
 Cervical Cancer Screening Update Melissa Hartman, DO Women s Health Previous Cervical Cancer Screening Organization Recommendation ACS (2011) ACP (2008) NCI (2003) Age 21 or 3 years after first intercourse
Cervical Cancer Screening Update Melissa Hartman, DO Women s Health Previous Cervical Cancer Screening Organization Recommendation ACS (2011) ACP (2008) NCI (2003) Age 21 or 3 years after first intercourse
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
Objectives. I have no financial interests in any product I will discuss today. Cervical Cancer Screening Guidelines: Updates and Controversies
 Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
Cervical Cancer Screening Guidelines: Updates and Controversies I have no financial interests in any product I will discuss today. Jody Steinauer, MD, MAS University of California, San Francisco Objectives
CPC on Cervical Pathology
 CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
Cytology/Biopsy/Leep Gynecologic Correlation: Practical Considerations and Approaches.
 Cytology/Biopsy/Leep Gynecologic Correlation: Practical Considerations and Approaches. Fadi W. Abdul-Karim MD MEd. Professor of Pathology. Vice chair for education. Robert Tomsich Pathology and Lab Med
Cytology/Biopsy/Leep Gynecologic Correlation: Practical Considerations and Approaches. Fadi W. Abdul-Karim MD MEd. Professor of Pathology. Vice chair for education. Robert Tomsich Pathology and Lab Med
PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT
 PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT QUESTION #1 WHICH OF THE FOLLOWING IS NOT A RISK FACTOR FOR CERVICAL CANCER? A. HIGH RISK HPV B. CIGARETTE SMOKING C.
PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT QUESTION #1 WHICH OF THE FOLLOWING IS NOT A RISK FACTOR FOR CERVICAL CANCER? A. HIGH RISK HPV B. CIGARETTE SMOKING C.
Case 3 - GYN. History: 66 year old, routine Pap test. Dr. Stelow
 Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
Case 3 - GYN History: 66 year old, routine Pap test Dr. Stelow Case 3 66 year year old woman Routine Pap Test Cytologic Features 3 dimensional clusters of cells with small to moderate amount of
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)
 - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H)") SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
SQUAMOUS CELLS: Atypical squamous cells (ASC) - of undetermined significance (ASC-US) - cannot exclude HSIL (ASC-H) ASC refers to cytologic changes suggestive of SIL, which are qualitativley or quantitatively
Case Based Problems. Recommended Guidelines. Workshop: Case Management of Abnormal Pap Smears and Colposcopies. Disclosure
 Disclosure Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Associate Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics This
Disclosure Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Associate Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics This
HKCOG GUIDELINES NUMBER 3 (revised November 2002) published by The Hong Kong College of Obstetricians and Gynaecologists
 published by The Hong Kong College of Obstetricians and Gynaecologists") HKCOG Guidelines Guidelines on the Management of An Abnormal Cervical Smear Number 3 revised November 2002 published by The Hong Kong College of Obstetricians and Gynaecologists A Foundation College of
HKCOG Guidelines Guidelines on the Management of An Abnormal Cervical Smear Number 3 revised November 2002 published by The Hong Kong College of Obstetricians and Gynaecologists A Foundation College of
GYN (Glandulars) Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital
 Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital") GYN (Glandulars) Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital and Bioreference Labs (Houston) Department of Pathology
GYN (Glandulars) Still Difficult After All These Years! Dina R Mody, MD Director of Cytology Laboratories and fellowship Program Methodist Hospital and Bioreference Labs (Houston) Department of Pathology
Glandular lesions in cervical cytology. Margareta Strojan Fležar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia
 Glandular lesions in cervical cytology Margareta Strojan Fležar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia 2nd PANNONIA CONGRESS OF PATHOLOGY, SIÓFOK, HUNGARY, 17-19 MAY
Glandular lesions in cervical cytology Margareta Strojan Fležar Institute of Pathology Faculty of Medicine University of Ljubljana Slovenia 2nd PANNONIA CONGRESS OF PATHOLOGY, SIÓFOK, HUNGARY, 17-19 MAY
POST-CONIZATION FOLLOW-UP OF PATIENTS WITH HIGH GRADE SQUAMOUS INTRAEPITHELIAL LESION TREATED BY LEEP PROCEDURE: A LITERATURE REVIEW
 POST-CONIZATION FOLLOW-UP OF PATIENTS WITH HIGH GRADE SQUAMOUS INTRAEPITHELIAL LESION TREATED BY LEEP PROCEDURE: A LITERATURE REVIEW Boureima Ali Nafissatou and Dong zhao * Department of Gynecology, Shanghai
POST-CONIZATION FOLLOW-UP OF PATIENTS WITH HIGH GRADE SQUAMOUS INTRAEPITHELIAL LESION TREATED BY LEEP PROCEDURE: A LITERATURE REVIEW Boureima Ali Nafissatou and Dong zhao * Department of Gynecology, Shanghai
1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal
 Diseases of cervix I. Inflammations 1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal squamous mucosa
Diseases of cervix I. Inflammations 1.Acute and Chronic Cervicitis - At the onset of menarche, the production of estrogens by the ovary stimulates maturation of the cervical and vaginal squamous mucosa
SOGC / SCC Clinical Practice Guideline
 SOGC / SCC Clinical Practice Guideline Colposcopic Management of Abnormal Cervical Cancer Screening and Histology These Clinical Practice Guidelines have been prepared and approved by the Executive and
SOGC / SCC Clinical Practice Guideline Colposcopic Management of Abnormal Cervical Cancer Screening and Histology These Clinical Practice Guidelines have been prepared and approved by the Executive and
Cervical Cancer 4/27/2016
 Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical College of Wisconsin May 6, 2016 Cervical Cancer In US about
Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical College of Wisconsin May 6, 2016 Cervical Cancer In US about
Cervical Cancer : Pap smear
 Taking a PAP SMEAR Cervical Cancer : Pap smear George N Papanicolaou introduced cervical cytology in clinical practice in 1940 In 1945, PAP smear was endorsed by American cancer society as an effective
Taking a PAP SMEAR Cervical Cancer : Pap smear George N Papanicolaou introduced cervical cytology in clinical practice in 1940 In 1945, PAP smear was endorsed by American cancer society as an effective
Cervical Testing and Results Management. An Evidenced-Based Approach April 22nd, Debora Bear, MSN, MPH
 Cervical Testing and Results Management An Evidenced-Based Approach April 22nd, 2010 Debora Bear, MSN, MPH Assistant Medical Director for Planned Parenthood of New Mexico, Inc. Burden of cervical cancer
Cervical Testing and Results Management An Evidenced-Based Approach April 22nd, 2010 Debora Bear, MSN, MPH Assistant Medical Director for Planned Parenthood of New Mexico, Inc. Burden of cervical cancer
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L14
 LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 09/5/95 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 09/5/95 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
chapter 4. The effect of oncogenic HPV on transformation zone epithelium
 chapter 4. The effect of oncogenic HPV on transformation zone epithelium CHAPTER 1 All squamous cervical cancer (and probably all cervical adenocarcinoma) is associated with oncogenic HPV, and the absence
chapter 4. The effect of oncogenic HPV on transformation zone epithelium CHAPTER 1 All squamous cervical cancer (and probably all cervical adenocarcinoma) is associated with oncogenic HPV, and the absence
Cryotherapy has No Place in Colposcopy Practice
 Cryotherapy has No Place in Colposcopy Practice No financial disclosures No conflicts of interest ? Precision? Personalized Medicine? Best Evidence Based Practice Prinicipals of Surgical Management CIN1
Cryotherapy has No Place in Colposcopy Practice No financial disclosures No conflicts of interest ? Precision? Personalized Medicine? Best Evidence Based Practice Prinicipals of Surgical Management CIN1
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology
 New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
New Diagnoses Need New Approaches: A Glimpse into the Near Future of Gynecologic Pathology United States and Canadian Academy of Pathology 102 nd Annual Meeting Baltimore, Maryland Christina S. Kong, M.D.
Clinical outcomes after conservative management of CIN1/2, CIN2, and CIN2/3 in women ages years
 Clinical outcomes after conservative management of CIN1/2, CIN2, and CIN2/3 in women ages 21-39 years Michelle I. Silver, PhD, ScM Cancer Prevention Fellow National Cancer Institute Division of Cancer
Clinical outcomes after conservative management of CIN1/2, CIN2, and CIN2/3 in women ages 21-39 years Michelle I. Silver, PhD, ScM Cancer Prevention Fellow National Cancer Institute Division of Cancer
Atypical Glandular Cells of Undetermined Significance Outcome Predictions Based on Human Papillomavirus Testing
 Anatomic Pathology / ATYPICAL GLANDULAR CELLS AND HUMAN PAPILLOMAVIRUS Atypical Glandular Cells of Undetermined Significance Outcome Predictions Based on Human Papillomavirus Testing Jeffrey F. Krane,
Anatomic Pathology / ATYPICAL GLANDULAR CELLS AND HUMAN PAPILLOMAVIRUS Atypical Glandular Cells of Undetermined Significance Outcome Predictions Based on Human Papillomavirus Testing Jeffrey F. Krane,
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
VIN/VAIN O C T O B E R 3 RD J M O R G A N
 VIN/VAIN O C T O B E R 3 RD 2 0 1 8 J M O R G A N Vaginal Intraepithelial Neoplasia VAIN I, II, III Incidence 0.1/100,000 women in US Mean age 50s (J Womens Health (Larchmt) 2009:18:1731) (J Obstet Gynaecol
VIN/VAIN O C T O B E R 3 RD 2 0 1 8 J M O R G A N Vaginal Intraepithelial Neoplasia VAIN I, II, III Incidence 0.1/100,000 women in US Mean age 50s (J Womens Health (Larchmt) 2009:18:1731) (J Obstet Gynaecol
This paper includes Author Insights, a video abstract available at
 DOI: 10.1111/1471-0528.14808 www.bjog.org Epidemiology Risk of persistent or recurrent cervical neoplasia in patients with pure adenocarcinoma-in-situ (AIS) or mixed AIS and high-grade cervical squamous
DOI: 10.1111/1471-0528.14808 www.bjog.org Epidemiology Risk of persistent or recurrent cervical neoplasia in patients with pure adenocarcinoma-in-situ (AIS) or mixed AIS and high-grade cervical squamous
Management that provides continuity of care for women
 Management that provides continuity of care for women If women are diagnosed with reproductive tract infection, prompt treatment should be instituted according to the WHO guidelines. Though it may be preferred
Management that provides continuity of care for women If women are diagnosed with reproductive tract infection, prompt treatment should be instituted according to the WHO guidelines. Though it may be preferred
Cervical Cancer Prevention in the 21 st Century Changing Paradigms
 Cervical Cancer Prevention in the 21 st Century Changing Paradigms Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M.
Cervical Cancer Prevention in the 21 st Century Changing Paradigms Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M.
To further assess abnormalities detected on cervical cytological sample. To guide colposcopically directed biopsy
 1 To further assess abnormalities detected on cervical cytological sample To guide colposcopically directed biopsy To exclude invasive disease To aid in outpatient management and treatment of precancerous
1 To further assess abnormalities detected on cervical cytological sample To guide colposcopically directed biopsy To exclude invasive disease To aid in outpatient management and treatment of precancerous
What Causes Cervical Cancer? Symptoms of Cervical Cancer
 Cervical Health Awareness Month is a chance to raise awareness about how women can protect themselves from HPV (human papillomavirus) and cervical cancer. HPV is a very common infection that spreads through
Cervical Health Awareness Month is a chance to raise awareness about how women can protect themselves from HPV (human papillomavirus) and cervical cancer. HPV is a very common infection that spreads through
Clinical Practice Guidelines June 2013
 Clinical Practice Guidelines June 2013 General Principles: The Papanicolaou (Pap) smear is widely credited with reducing mortality from cervical cancer, and remains the single best method for the early
Clinical Practice Guidelines June 2013 General Principles: The Papanicolaou (Pap) smear is widely credited with reducing mortality from cervical cancer, and remains the single best method for the early
SESSION J4. What's Next? Managing Abnormal PAPs in 2014
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION J4 What's Next? Managing Abnormal PAPs in 2014 Session Description: Linda Eckert, MD Review current guidelines
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION J4 What's Next? Managing Abnormal PAPs in 2014 Session Description: Linda Eckert, MD Review current guidelines
How invasive cervical cancer audit affects clinical practice
 How invasive cervical cancer audit affects clinical practice Referring to NHSCSP and EU guidelines and audits in Southampton and London Amanda Herbert Guy s & St Thomas Foundation NHS Trust How invasive
How invasive cervical cancer audit affects clinical practice Referring to NHSCSP and EU guidelines and audits in Southampton and London Amanda Herbert Guy s & St Thomas Foundation NHS Trust How invasive
Woo Dae Kang, Ho Sun Choi, Seok Mo Kim
 Is vaccination with quadrivalent HPV vaccine after Loop Electrosurgical Excision Procedure effective in preventing recurrence in patients with High-grade Cervical Intraepithelial Neoplasia (CIN2-3)? Chonnam
Is vaccination with quadrivalent HPV vaccine after Loop Electrosurgical Excision Procedure effective in preventing recurrence in patients with High-grade Cervical Intraepithelial Neoplasia (CIN2-3)? Chonnam
WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L14
 WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0 / 0 / 6 ANY MISSING OR INCOMPLETE TEST RESULTS
WOMEN S INTERAGENCY HIV STUDY LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0 / 0 / 6 ANY MISSING OR INCOMPLETE TEST RESULTS
Conflict of Interest Disclosure. Anita L. Nelson, MD. Principles Underlying Screening Recommendations. Learning Objectives
 Advanced Colposcopy Conflict of Interest Disclosure Anita L. Nelson, MD Anita L. Nelson, MD Professor OB-GYN David Geffen School of Medicine at UCLA CFHC s 2014 Women s Health Update Berkeley, CA May 20,
Advanced Colposcopy Conflict of Interest Disclosure Anita L. Nelson, MD Anita L. Nelson, MD Professor OB-GYN David Geffen School of Medicine at UCLA CFHC s 2014 Women s Health Update Berkeley, CA May 20,
EFC and European Standards for Colposcopic Evaluation
 EFC and European Standards for Colposcopic Evaluation Cagatay Taskiran, MD. Koc University School of Medicine, and VKF American Hospital Department of Obstetrics and Gynecology Division of Gynecologic
EFC and European Standards for Colposcopic Evaluation Cagatay Taskiran, MD. Koc University School of Medicine, and VKF American Hospital Department of Obstetrics and Gynecology Division of Gynecologic
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L14
 LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0/0/0 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
LABORATORY - PELVIC EXAM STUDIES COLPOSCOPY RESULTS FORM L4 ID LABEL HERE ---> - - - VISIT #: FORM COMPLETED BY: VERSION DATE: 0/0/0 ANY MISSING OR INCOMPLETE TEST RESULTS MUST BE EXPLAINED ON THIS FORM.
No Disclosures. Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results. Objectives 5/9/2016
 Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical Director, PPWI Medical College of Wisconsin May 6,
Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical Director, PPWI Medical College of Wisconsin May 6,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000
 Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
Hyperchromatic Crowded Groups: What is Your Diagnosis? Session 3000 Thomas A. Bonfiglio, M.D. Professor Emeritus, Pathology and Laboratory Medicine University of Rochester Disclosures In the past 12 months,
International Federation of Gynecology and Obstetrics
 International Federation of Gynecology and Obstetrics Treatment of Cervical Precancerous Lesions using Thermocoagulation(Cold Coagulation) and Cryotherapy General Principles All high grade CIN should be
International Federation of Gynecology and Obstetrics Treatment of Cervical Precancerous Lesions using Thermocoagulation(Cold Coagulation) and Cryotherapy General Principles All high grade CIN should be
Cervical Screening for Dysplasia and Cancer in Patients with HIV
 Cervical Screening for Dysplasia and Cancer in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute w w w.hivg uidelines.org Purpose of the Guideline Increase
Cervical Screening for Dysplasia and Cancer in Patients with HIV Adult Clinical Guideline from the New York State Department of Health AIDS Institute w w w.hivg uidelines.org Purpose of the Guideline Increase
Over-diagnoses in Cytopathology: Is histology the gold standard?
 Over-diagnoses in Cytopathology: Is histology the gold standard? Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M. Darragh,
Over-diagnoses in Cytopathology: Is histology the gold standard? Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M. Darragh,
Understand Your Results
 Understand Your Results The Pap test takes little time and may save your life. This simple screening test checks for cell changes in the cervix, the opening of the uterus. If your Pap results were abnormal,
Understand Your Results The Pap test takes little time and may save your life. This simple screening test checks for cell changes in the cervix, the opening of the uterus. If your Pap results were abnormal,
Cervical Precancer: Evaluation and Management
 TAJ June 2002; Volume 15 Number 1 ISSN 1019-8555 The Journal of Teachers Association RMC, Rajshahi Review fam Cervical Precancer: Evaluation and Management SM Khodeza Nahar Begum 1 Abstract Carcinoma of
TAJ June 2002; Volume 15 Number 1 ISSN 1019-8555 The Journal of Teachers Association RMC, Rajshahi Review fam Cervical Precancer: Evaluation and Management SM Khodeza Nahar Begum 1 Abstract Carcinoma of
Running head: EVIDENCE-BASED MEDICINE TWO-STEP DISCREPANCY
 Evidence-Based Medicine Two-Step Discrepancy 1 Running head: EVIDENCE-BASED MEDICINE TWO-STEP DISCREPANCY Evidence-Based Medicine Two-Step Discrepancy Julie Nelson Texas Woman s University Philosophy of
Evidence-Based Medicine Two-Step Discrepancy 1 Running head: EVIDENCE-BASED MEDICINE TWO-STEP DISCREPANCY Evidence-Based Medicine Two-Step Discrepancy Julie Nelson Texas Woman s University Philosophy of
Introduction to Colposcopy
 Introduction to Colposcopy Papanicolaou smear (Pap smear) screening test Colposcopy diagnostic test Introduction to Colposcopy Acetic acid and Lugol s iodine applied Cervix examined under magnification
Introduction to Colposcopy Papanicolaou smear (Pap smear) screening test Colposcopy diagnostic test Introduction to Colposcopy Acetic acid and Lugol s iodine applied Cervix examined under magnification
Human Papillomavirus (HPV) and Cervical Cancer Prevention
 and Cervical Cancer Prevention") Human Papillomavirus (HPV) and Cervical Cancer Prevention MOA Autumn Convention November 3, 2017 David J Boes, DO, FACOOG (Dist.) Associate Professor, MSU-COM 1 Disclosures None relative to this presentation
Human Papillomavirus (HPV) and Cervical Cancer Prevention MOA Autumn Convention November 3, 2017 David J Boes, DO, FACOOG (Dist.) Associate Professor, MSU-COM 1 Disclosures None relative to this presentation
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo. Case Discussions. 60 year old woman Routine gynecologic control LBC
 BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
BOSNIAN-TURKISH CYTOPATHOLOGY SCHOOL June 18-19, 2016 Sarajevo Case Discussions Prof Dr Sıtkı Tuzlalı Tuzlalı Pathology Laboratory 60 year old woman Routine gynecologic control LBC 1 2 Endometrial thickening
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
LLETZ (Large Loop Excision of the Transformation Zone) Fragmentation: Impact on Margin Assessment and Cervical Biopsy-LLETZ Correlation
 Fragmentation: Impact on Margin Assessment and Cervical Biopsy-LLETZ Correlation") LLETZ (Large Loop Excision of the Transformation Zone) Fragmentation: Impact on Margin Assessment and Cervical Biopsy-LLETZ Correlation Bridget Melley BSc. (Hons.) in Medical Science Galway-Mayo Institute
LLETZ (Large Loop Excision of the Transformation Zone) Fragmentation: Impact on Margin Assessment and Cervical Biopsy-LLETZ Correlation Bridget Melley BSc. (Hons.) in Medical Science Galway-Mayo Institute
I have no financial interests in any product I will discuss today.
 Cervical Cancer Prevention: 2012 and Beyond George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics University of California,
Cervical Cancer Prevention: 2012 and Beyond George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics University of California,
Cytology Report Format
 Squamous Precursor Lesions and Malignancies In Pap Test Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College
Squamous Precursor Lesions and Malignancies In Pap Test Dina R. Mody, MD, FCAP Director of Cytology The Methodist Hospital, Houston, TX Professor of Pathology and Laboratory Medicine Weill Medical College
Human Papillomavirus
 Human Papillomavirus Dawn Palaszewski, MD Assistant Professor of Obstetrics and Gynecology University of February 18, 2018 9:40 am Dawn Palaszewski, MD Assistant Professor Department of Obstetrics and
Human Papillomavirus Dawn Palaszewski, MD Assistant Professor of Obstetrics and Gynecology University of February 18, 2018 9:40 am Dawn Palaszewski, MD Assistant Professor Department of Obstetrics and
Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA
 Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA Cancer Care Ontario Cervical Cancer Screening Goals Increase patient participation in cervical screening Increase primary care
Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA Cancer Care Ontario Cervical Cancer Screening Goals Increase patient participation in cervical screening Increase primary care
Streamlining Protocols-From Strategy to Implementation. Doreen Ramogola-Masire Botswana UPenn Partnership June 2014
 Streamlining Protocols-From Strategy to Implementation Doreen Ramogola-Masire Botswana UPenn Partnership 18-20 June 2014 Botswana-UPenn Partnership Partnership between Government of Botswana, University
Streamlining Protocols-From Strategy to Implementation Doreen Ramogola-Masire Botswana UPenn Partnership 18-20 June 2014 Botswana-UPenn Partnership Partnership between Government of Botswana, University
Cytyc Corporation - Case Presentation Archive - July 2002
 ThinPrep Pap Test History: 34 Year Old Female LMP: Day 20 Specimen Type: Cervical/Vaginal Case provided by Mark Tulecke, M.D. and Gabrielle Trawinski CT (ASCP), Mount Auburn Hospital, Cambridge, Massachusetts.
ThinPrep Pap Test History: 34 Year Old Female LMP: Day 20 Specimen Type: Cervical/Vaginal Case provided by Mark Tulecke, M.D. and Gabrielle Trawinski CT (ASCP), Mount Auburn Hospital, Cambridge, Massachusetts.
AGC Subclasses and Risk of Invasive Cancers
 AGC Subclasses and Risk of Invasive Cancers Xuezhi (Daniel) Jiang, MD, PhD Associate Professor of Obstetrics & Gynecology The Reading Hospital of Tower Health Thomas Jefferson University Reading, PA Disclosures
AGC Subclasses and Risk of Invasive Cancers Xuezhi (Daniel) Jiang, MD, PhD Associate Professor of Obstetrics & Gynecology The Reading Hospital of Tower Health Thomas Jefferson University Reading, PA Disclosures
Study Number: Title: Rationale: Phase: Study Period Study Design: Centres: Indication Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
Your Colposcopy Visit
 Introduction Welcome to the colposcopy clinic. This booklet tells you about. The colposcopy examination.. Tests that are done in the colposcopy clinic.. What these tests look for Take a few minutes to
Introduction Welcome to the colposcopy clinic. This booklet tells you about. The colposcopy examination.. Tests that are done in the colposcopy clinic.. What these tests look for Take a few minutes to
Histopathology: Cervical HPV and neoplasia
 Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
Histopathology: Cervical HPV and neoplasia These presentations are to help you identify basic histopathological features. They do not contain the additional factual information that you need to learn about
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
Glandular Atypia In Cervical Smear: Cytohistologic And Clinical Correlation. K Elsapagh, S Swain, S Ghosh, H Dunsmore, K McMullen, J Steven, K Morton
 ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 5 Number 2 Glandular Atypia In Cervical Smear: Cytohistologic And Clinical Correlation K Elsapagh, S Swain, S Ghosh, H Dunsmore, K McMullen,
ISPUB.COM The Internet Journal of Gynecology and Obstetrics Volume 5 Number 2 Glandular Atypia In Cervical Smear: Cytohistologic And Clinical Correlation K Elsapagh, S Swain, S Ghosh, H Dunsmore, K McMullen,
Index. Cytoplasm, nonepithelial malignant tumor features 70
 Accurette device 23 Adenosarcoma, differential diagnosis 80, 81 Arias-Stella reaction 65 Atypical endocervical cells 8 Atypical endometrial cells 8 Atypical glandular cells (AGC) 8, 9 Atypical glandular
Accurette device 23 Adenosarcoma, differential diagnosis 80, 81 Arias-Stella reaction 65 Atypical endocervical cells 8 Atypical endometrial cells 8 Atypical glandular cells (AGC) 8, 9 Atypical glandular
An audit of liquid-based cervical cytology screening samples (ThinPrep and SurePath) reported as glandular neoplasia
 reported as glandular neoplasia") DOI:10.1111/j.1365-2303.2009.00695.x An audit of liquid-based cervical cytology screening samples (ThinPrep and SurePath) reported as glandular neoplasia S. A. Thiryayi, J. Marshall and D. N. Rana Manchester
DOI:10.1111/j.1365-2303.2009.00695.x An audit of liquid-based cervical cytology screening samples (ThinPrep and SurePath) reported as glandular neoplasia S. A. Thiryayi, J. Marshall and D. N. Rana Manchester
I have no financial interests in any product I will discuss today.
 Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
Cervical Cancer Screening Update and Implications for Annual Exams George F. Sawaya, MD Professor Department of Obstetrics, Gynecology and Reproductive Sciences Department of Epidemiology and Biostatistics
,,,,, PATHOLOGY QUIZ PATHOLOGY Q U I Z
 ,,,,, PATHOLOGY Q U I Z,,,,, PATHOLOGY QUIZ CASE HISTORY Alex Ferenczy, MD, Professor of Pathology and Obstetries and Gynaecology, The Sir Mortimer B. Davis ]ewish General HosPital, McGill University This
,,,,, PATHOLOGY Q U I Z,,,,, PATHOLOGY QUIZ CASE HISTORY Alex Ferenczy, MD, Professor of Pathology and Obstetries and Gynaecology, The Sir Mortimer B. Davis ]ewish General HosPital, McGill University This