Colonic Polyp. Najmeh Aletaha. MD
|
|
|
- Nancy O’Brien’
- 6 years ago
- Views:
Transcription

1
2 Colonic Polyp Najmeh Aletaha. MD
3 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance
4 polyp of the colon refers to a protuberance into the lumen above the surrounding colonic mucosa. Colonic polyp Neoplastic Serrated polyps Adenomatous polyps Non-neoplastic Inflammatory polyps Hyperplastic polyps Hamartomatous polyps
5 INFLAMMATORY POLYPS Non-neoplastic intraluminal projections of mucosa and inflammatory cells Inflammatory polyps include: Inflammatory pseudopolyps pedunculated or sessile Risk of malignancy: No risk but may be associated with surrounding dysplasia in patients with IBD. Prolapse type inflammatory polyps Caused by peristalsis-induced trauma
6 HAMARTOMATOUS POLYPS Juvenile polyps: Hamartomatous lesions that consist of a lamina propria and dilated cystic glands More common in childhood, most common in the rectosigmoid, resulting in lower gastrointestinal bleeding or prolapse through the rectum, No increased colorectal cancer risk. Juvenile polyposis syndrome (JPS) Autosomal dominant condition, multiple hamartomatous polyps throughout the gastrointestinal tract, increased risk for colorectal and gastric cancer.
7 HAMARTOMATOUS POLYPS Peutz-Jeghers polyps: Hamartomatous lesion of glandular epithelium supported by smooth muscle cells Peutz-Jeghers syndrome (PJS), due to STK11 mutations, undergo malignant transformation, Patients with PJS are at increased risk of both gastrointestinal (gastric, small bowel, colon, pancreas) and nongastrointestinal cancers. Cronkhite-Canada syndrome: Rare, nonfamilial disorder associated with alopecia, cutaneous hyperpigmentation, gastrointestinal polyposis, onychodystrophy, diarrhea, weight loss, and abdominal pain. polyps are hamartomas and do not appear neoplastic pathologically. Respond to immunosuppressive therapy
8 SERRATED POLYPS: Heterogenous group of polyps with variable malignant potential. They include Hyperplastic polyps Traditional serrated adenomas Sessile serrated polyps
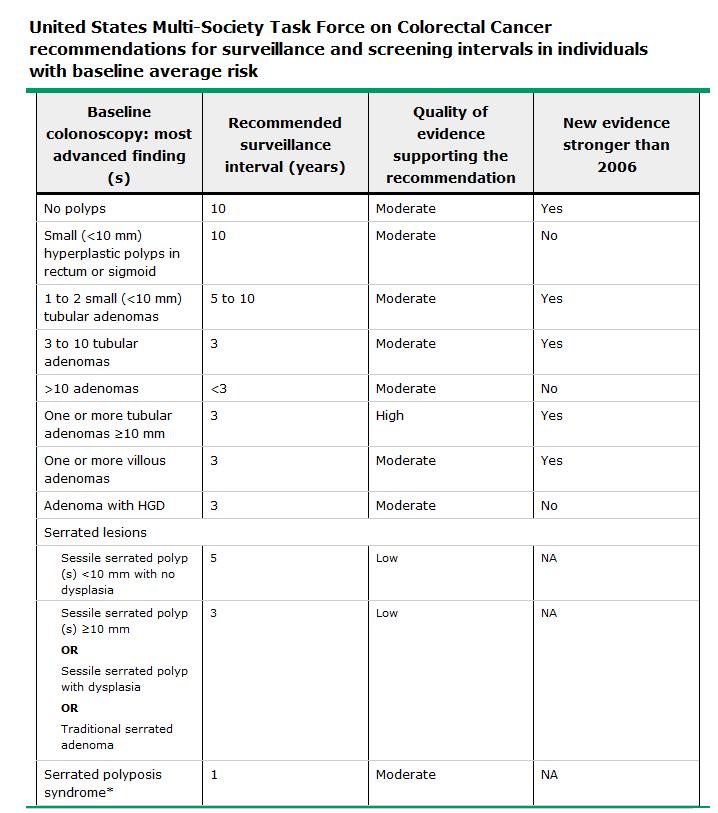
9 Hyperplastic polyps: most common non-neoplastic polyps in the colon, typically located in the rectosigmoid and are less than 5 mm in size. Small rectosigmoid hyperplastic polyps do not appear to increase the risk of colorectal cancer. Surveillance In patients with small (<10 mm) hyperplastic polyps confined to the rectum or sigmoid colon, surveillance colonoscopy is recommended in 10 years.
10 Sessile serrated polyps: SSPs or sessile serrated adenoma [SSA] are more prevalent in the proximal colon. These polyps have a smooth surface, are often flat or sessile, and may be covered with mucus. Histologically, may acquire morphologic evidence of dysplasia. Traditional serrated adenomas (TSAs): More prevalent in the rectosigmoid colon and may be pedunculated or sessile. TSA have diffuse but often mild cytologic dysplasia.
11 Risk of cancer Risk factors for a synchronous advanced adenoma in patients with SSPs include SSP/A size 10 mm, location in the proximal colon, and the presence of dysplasia. Management TSAs and SSA/Ps are managed clinically like adenomatous polyps and complete excision is recommended.
12 Surveillance Individuals with SSA/P <10 mm in size with no dysplasia are managed as low risk adenomas with a first surveillance colonoscopy in five years. Individuals with SSA/P 10 mm, a SSA/P with dysplasia, or TSA are managed as high-risk adenomas with a first surveillance colonoscopy in three years. Other expert consensus recommendations have suggested earlier colonoscopic follow-up (one- to three-year interval) in individuals with two or more SSA/P larger than 10 mm and in those with any SSA/P with cytologic dysplasia (expert opinion).
13 Serrated polyposis syndrome (SPS) or hyperplastic polyposis syndrome (HPS): Diagnosis Based on one or more of the following World Health Organization criteria: At least five serrated polyps proximal to the sigmoid colon, of which two or more are 10 mm. Any number of serrated polyps proximal to the sigmoid colon in an individual who has a first-degree relative with SPS. >20 serrated polyps of any size, distributed throughout the colon. Surveillance one to three years based on the number and size of polyps.
14 ADENOMATOUS POLYPS: Approximately two-thirds of all colonic polyps Risk factor Increasing age Increased BMI (Abdominal obesity may be a better predictor). Lack of physical activity Adenomatous polyps are more common in men, and large adenomas may be more common in African- Americans.


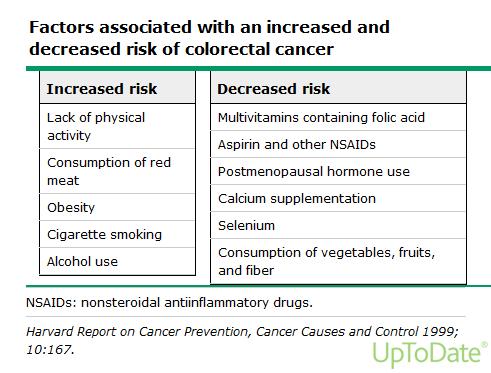
15 Risk factors Risk factors for Colorectal cancer
16
17 Dietary factors implicated in colorectal carcinogenesis Diet Dietary fiber vegetables folate (B Vitamin) Decreased risk fruits calcium

18 Diet Alcohol Refined carbohydrates Animal and saturated fat Consumption of red meat increased risk of colorectal cancer
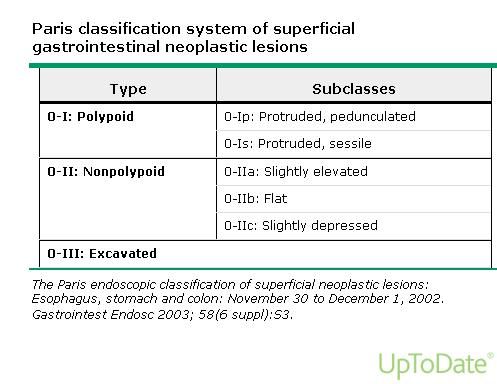
19 Endoscopic features and classification Based on their gross appearance, adenomas may be pedunculated, sessile, flat, depressed, or excavated.
20
21
22 Adenomatous Polyp Occur mainly in large bowel. Spordic and familial Vary from small pedunculated to large sessile Epithelium proliferation and dysplysia Histologic features 1. Tubular adenoma: tubular component of at least 75 percent. (more than 80 percent of colonic adenomas) 2. Villous adenoma: >75 percent villous features (5 to 15 percent of adenomas) 3. Tubulovillous adenoma: 25 to 75 percent villous features. (5 to 15 percent of colonic adenomas)
![Neoplastic Polyps 1] Tubular adenoma Represents 75% of all](/docs-images/79/79224291/images/23-4.jpg "neoplastic polyps.")
23 Neoplastic Polyps 1] Tubular adenoma Represents 75% of all neoplastic polyps. 75 % occur in the distal colon and rectum.
![Neoplastic Polyps 2] Villous Adenoma The least common, largest and](/docs-images/79/79224291/images/24-4.jpg "most ominous of epithelial polyps.")

24 Neoplastic Polyps 2] Villous Adenoma The least common, largest and most ominous of epithelial polyps. Age: 60 to 65 years, Present with rectal bleeding or anemia, large ones may secrete copious amounts of mucoid material rich in protein. 75% located in rectosigmoid area.
25 3] Tubulovillous adenoma Intermmediate in size, degree of dysplasia and malignant potential between tubular and villous adenomas.
26 ADENOMATOUS POLYPS: 5 percent or less of adenomas progress to cancer over 7 to 10 years. The risk of progression is higher for advanced adenomas (adenoma with high-grade dysplasia, >10 mm in size, or a villous component).
27 Management: Polypectomy Adenomas should be resected completely. Small adenomas may be completely removed using biopsy forceps larger adenomas require snare resection, with or without electrocautery or advanced endoscopic resection techniques (eg, EMR or ESD). Large sessile adenomas often require piecemeal resection. (& repeat colonoscopy to evaluate the site of excision within six months) In cases where endoscopic resection is not possible, surgical resection is required.
28 Management: Management of a polyp containing invasive carcinoma must be individualized. In early-stage (T1) colon cancers, polypectomy alone is usually adequate if the following risk factors for residual cancer and/or nodal metastases are absent: Poorly-differentiated histology. Lymphovascular invasion. Cancer at the resection margin. Invasion of the stalk of pedunculated polyp, by itself, is not an unfavorable prognostic finding, as long as the cancer does not extend to the margin of stalk resection. A 2 mm resection margin is regarded as adequate.
29 Invasion into the muscularis propria of the bowel wall (T2 lesion). Invasive carcinoma arising in a sessile (flat) polyp with unfavorable features (eg, lower third submucosal penetration, lymphovascular invasion, poorly differentiated). After complete resection of a polyp with cancer, we perform follow-up colonoscopy in three months to check for residual abnormal tissue at the polypectomy site if the polyp was sessile. The presence of any one of the risk factors for residual cancer and/or nodal metastases should prompt consideration of radical surgery.
30 Adenoma-carcinoma sequence Most colorectal cancers (CRCs) arise from adenomas, many of which are polyps that progress from small (<8 mm) to large ( 8 mm) polyps, and then to dysplasia and cancer. Neoplastic changes result from both inherited and acquired genetic defects.
31
32



33 Adenoma to Carcinoma Pathway Normal Adenoma Cancer APC loss K-ras mutation Chrom 18 loss p53 loss Normal Hyperproliferation pithelium Early Adenoma Intermediate Adenoma Late Adenoma Cancer
34 Familial Polyposis Syndrome Patients have genetic tendencies to develop neoplastic polyps. Familial polyposis coli (FPC) Genetic defect of Adenomatous polyposis coli (APC). APC gene located on the long arm of chromosome 5 (5q21). APC gene is a tumor suppressor gene Innumerable neoplastic polyps in the colon (500 to 2500) Polyps are also found elsewhere in alimentary tract Most polyps are tubular adenomas The risk of colorectal cancer is 100% by midlife. Gardener s syndrome Polyposis coli, multiple osteomas, epidermal cysts, and fibromatosis. Turcot syndrome Polyposis coli, glioma and fibromatosis

35 Familial polyposis coli (FPC)
 chromosomal instability that results in stepwise accumulation of mutations in a series of oncogenes and tumor suppressor genes.")
36 Adenocarcinoma of Large Intestine Carcinogenesis Two pathogenetically distinct pathways for the development of colon cancer, both seem to result from accumulation of multiple mutations: 1- The APC/B-catenin pathway ( 85 % ) chromosomal instability that results in stepwise accumulation of mutations in a series of oncogenes and tumor suppressor genes. adenoma-carcinoma sequence
37 Malignant Tumors of Large Intestine Adenocarcinoma Carcinogenesis 2- The DNA mismatch repair genes pathway: 10% to 15% of sporadic cases. There is accumulation of mutations (as in the APC/B-catenin schema) Five DNA mismatch repair genes (MSH2, MSH6, MLH1, PMS1, AND PMS2) Give rise to the hereditary non polyposis colon carcinoma (HNPCC) MLH1 gene is the one most commonly involved in sporadic colon carcinomas
38
39

40
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial Adenomatous Polyposis
 Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Pathology perspective of colonic polyposis syndromes
 Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
Pathology perspective of colonic polyposis syndromes When are too many polyps too many? David Schaeffer Head and Consultant Pathologist, Department of Pathology and Laboratory Medicine, Vancouver General
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Classification of polyposis syndromes two major groups. Adenomatous polyposis syndromes. Hamartomatous polyposis syndromes
 Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Pathology reports, related operative reports and consult letters must be provided with a request for assessment.
 Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Adenoma to Carcinoma Pathway
 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
Serrated Polyps and a Classification of Colorectal Cancer
 Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer
 General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
General Session 7: Controversies in Screening and Surveillance in Colorectal Cancer Complexities of Pathological Assessment: Serrated Polyps/Adenomas Carolyn Compton, MD, PhD Professor of Life Sciences,
Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN
 Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
Serrated Adenomas: What do they mean and what to do about them? Douglas K. Rex, MD Indiana University Hospital Indianapolis, IN Colorectal Cancer Molecular Basis Pathway Frequency Genes MSI Precursor Speed
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
FINAL HISTOLOGICAL DIAGNOSIS: Villo-adenomatous polyp with in-situ-carcinomatous foci (involving both adenomatous and villous component).
.") SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
SOLITARY VILLO ADENOMATOUS POLYP WITH CARCINOMATOUS CHANGES RECTUM: A Divvya B 1, M. Valluvan 2, Rehana Tippoo 3, P. Viswanathan 4, R. Baskaran 5 HOW TO CITE THIS ARTICLE: Divvya B, M. Valluvan, Rehana
Colonic polyps and colon cancer. Andrew Macpherson Director of Gastroentology University of Bern
 Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Colon Cancer Screening. Layth Al-Jashaami, MD GI Fellow, PGY 4
 Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Hereditary Gastric Cancer
 Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic. Scott Rieder Dr. Colquhoun
 Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3.
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Tumors of the Intestines. Malignant Lesion. Adenocarcinoma. sessile Serrated Adenomas
 Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
Tumors of the Intestines Non-Neoplastic Polyps Neoplastic Epithelial Polyps Other Tumors Hyperplastic, Hamartomatous, Juvenile, Peutz-Jeghers, Inflammatory abd Lymphoid Polyphs Benign Polyphs Malignant
removal of adenomatous polyps detects important effectively as follow-up colonoscopy after both constitute a low-risk Patients with 1 or 2
 Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Supplementary Table 1. Study Characteristics Author, yr Design Winawer et al., 6 1993 National Polyp Study Jorgensen et al., 9 1995 Funen Adenoma Follow-up Study USA Multi-center, RCT for timing of surveillance
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
6 semanas de embarazo. Tubulovillous adenoma with dysplasia icd 10. Inicio / Embarazo / 6 semanas de embarazo
 Inicio / Embarazo / 6 semanas de embarazo 6 semanas de embarazo Tubulovillous adenoma with dysplasia icd 10 Free, official coding info for 2018 ICD-10-CM D13.2 - includes detailed rules, notes, synonyms,
Inicio / Embarazo / 6 semanas de embarazo 6 semanas de embarazo Tubulovillous adenoma with dysplasia icd 10 Free, official coding info for 2018 ICD-10-CM D13.2 - includes detailed rules, notes, synonyms,
Development of Carcinoma Pathways
 The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014
 COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS. Family Health Clinical Genetics. Clinical Genetics department
 GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
B Base excision repair, in MUTYH-associated polyposis and colorectal cancer, BRAF testing, for hereditary colorectal cancer, 696
 Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions. South Island Cancer Nurses Network September 2013
 For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
Sessile Serrated Polyps
 Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
Årsmøtet i Den norske Patologforening 2014 Sessile Serrated Polyps Tor J. Eide Oslo Universitetssykehus The term serrated include a group of lesions with a sawtoothlike appearance of the crypts and the
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School
 Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Precursors of Colorectal Carcinoma Arzu Ensari, MD, PhD Department of Pathology Ankara University Medical School Hyperplastic polyp Adenomatous polyp Colorectal carcinoma IBD-associated (1-2%) Sporadic
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Familial Juvenile Polyposis Coli
 GASTROENTEROLOGY 982 ;82 :494-50 Familial Juvenile Polyposis Coli A Clinical and Pathologic Study of a Large Kindred HAROLD W. GROTSKY, ROBERT R. RICKERT, WILLARD D. SMITH, and JAMES F. NEWSOME The Departments
GASTROENTEROLOGY 982 ;82 :494-50 Familial Juvenile Polyposis Coli A Clinical and Pathologic Study of a Large Kindred HAROLD W. GROTSKY, ROBERT R. RICKERT, WILLARD D. SMITH, and JAMES F. NEWSOME The Departments
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes
 ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Syngal, MD, MPH, FACG, 1,2,3 Randall E. Brand, MD, FACG, 4 James M. Church, MD, FACG, 5,6,7
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Syngal, MD, MPH, FACG, 1,2,3 Randall E. Brand, MD, FACG, 4 James M. Church, MD, FACG, 5,6,7
Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum
 Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
Tsumura T, et al 1 Synchronous and Subsequent Lesions of Serrated Adenomas and Tubular Adenomas of the Colorectum T. Tsumura a T. Hiyama d S. Tanaka b M. Yoshihara d K. Arihiro c K. Chayama a Departments
2015 Winter School 대장종양성병변의진단과치료. Dong Kyung Chang. Sungkyunkwan University, School of Medicine Samsung Medical Center
 2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
Serrated Lesions in the Bowel Cancer Screening Programme
 Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Serrated Lesions in the Bowel Cancer Screening Programme Mark Arends Cambridge & Edinburgh Serrated Lesions of Large Bowel 1. Hyperplastic polyp 2. Serrated adenoma 3. Mixed polyp 4. Sessile serrated lesion
Summary. Cezary ŁozińskiABDF, Witold KyclerABCDEF. Rep Pract Oncol Radiother, 2007; 12(4):
:") Rep Pract Oncol Radiother, 2007; 12(4): 201-206 Original Paper Received: 2006.12.19 Accepted: 2007.04.02 Published: 2007.08.31 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
Rep Pract Oncol Radiother, 2007; 12(4): 201-206 Original Paper Received: 2006.12.19 Accepted: 2007.04.02 Published: 2007.08.31 Authors Contribution: A Study Design B Data Collection C Statistical Analysis
References. GI Biopsies. What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD
 What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
What Should Pathologists Assistants Know About Gastrointestinal Histopathology? James M Crawford, MD, PhD jcrawford1@nshs.edu Executive Director and Senior Vice President for Laboratory Services North
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Mr Chris Wakeman. General Surgeon University of Otago, Christchurch. 12:15-12:40 Management of Colorectal Cancer
 Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Hereditary Non Polyposis Colorectal Cancer(HNPCC) From clinic to genetics
 From clinic to genetics") From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
Colorectal Cancer - Working in Partnership. David Baty Genetics, Ninewells Hospital
 Colorectal Cancer - Working in Partnership David Baty Genetics, Ninewells Hospital Genetics and Pathology National initiatives Colorectal cancer Inherited CRC Sporadic CRC The Liquid Biopsy The future?
Colorectal Cancer - Working in Partnership David Baty Genetics, Ninewells Hospital Genetics and Pathology National initiatives Colorectal cancer Inherited CRC Sporadic CRC The Liquid Biopsy The future?
M. Azzam Kayasseh,Dubai,UAE
 Thanks A Lot Prof. Linda + Prof. Ernst #drkayasseh_crc_rsm #WEO_CRCSC #UEGW17 @dubaiendoscopyforum @drkayasseh.care.to.cure Twenty World Areas Age-Standardized CRC Incidence Rates by Sex GLOBOCAN 2008
Thanks A Lot Prof. Linda + Prof. Ernst #drkayasseh_crc_rsm #WEO_CRCSC #UEGW17 @dubaiendoscopyforum @drkayasseh.care.to.cure Twenty World Areas Age-Standardized CRC Incidence Rates by Sex GLOBOCAN 2008
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition
 SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
Colon Cancer Update Christie J. Hilton, DO
 POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
Genetics of Pancreatic Cancer. October 6, If you experience technical difficulty during the presentation:
 Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
CRC and Endoscopy. Objectives. Background
 CRC and Endoscopy Darren Ballard, MD Assistant Professor Gastroenterology/Hepatology Medical College of Wisconsin Objectives Review background demographics and pathways for colon cancer Review colorectal
CRC and Endoscopy Darren Ballard, MD Assistant Professor Gastroenterology/Hepatology Medical College of Wisconsin Objectives Review background demographics and pathways for colon cancer Review colorectal
Management of pt1 polyps. Maria Pellise
 Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Management of pt1 polyps Maria Pellise Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps 0.75 5.6% of large-bowel
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD
 Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University
 Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University") COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
Historical. Note: The parenthetical numbers in the Clinical Indications section refer to the source documents cited in the References Section below.
 Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Clinical UM Guideline
 Subject: Guideline #: Current Effective Date: 06/28/2016 Status: Revised Last Review Date: 05/05/2016 Description This document addresses colonoscopy, an endoscopic procedure which allows direct visual
Subject: Guideline #: Current Effective Date: 06/28/2016 Status: Revised Last Review Date: 05/05/2016 Description This document addresses colonoscopy, an endoscopic procedure which allows direct visual
Pathology in Slovenian CRC screening programme: Organisation and quality assurance. Snježana Frković Grazio and Matej Bračko
 Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
5/2/2018. Low Grade Dysplasia of GI Tract. High Grade Dysplasia of GI Tract. Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues
 Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Dysplasia in Gastrointestinal Tract: Practical Pearls and Issues Arief Suriawinata, M.D. Professor of Pathology and Laboratory Medicine Geisel School of Medicine at Dartmouth Department of Pathology and
Cancer Genomics 101. BCCCP 2015 Annual Meeting
 Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Colorectal carcinoma: Pathologic aspects
 Review Article Colorectal carcinoma: Pathologic aspects Matthew Fleming*, Sreelakshmi Ravula*, Sergei F. Tatishchev*, Hanlin L. Wang Department of Pathology and Laboratory Medicine, David Geffen School
Review Article Colorectal carcinoma: Pathologic aspects Matthew Fleming*, Sreelakshmi Ravula*, Sergei F. Tatishchev*, Hanlin L. Wang Department of Pathology and Laboratory Medicine, David Geffen School
Colorectal Cancer Syndromes. Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago
 Colorectal Cancer Syndromes Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago Outline Colon cancer General Genetics, Risk, Screening Specific Syndromes, when to suspect,
Colorectal Cancer Syndromes Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago Outline Colon cancer General Genetics, Risk, Screening Specific Syndromes, when to suspect,
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2019 Origination: 1/2004 Next Review: 1/2020 Policy Blue Cross and Blue Shield of Kansas
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2019 Origination: 1/2004 Next Review: 1/2020 Policy Blue Cross and Blue Shield of Kansas
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
3/30/2017. Disclosure of Relevant Financial Relationships. Case 5: Polypoid mass in ulcerative colitis. Case 5. TC Smyrk
 Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Case 5: Polypoid mass in ulcerative colitis TC Smyrk Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
AMSER Rad Path Case of the Month: December 2018
 AMSER Rad Path Case of the Month: December 2018 Rectosigmoid Carcinoma Catherine McNulty, MS IV, Tulane University School of Medicine Dr. Matthew Hartman, M.D. Medical Student Radiology Director Dr. Matthew
AMSER Rad Path Case of the Month: December 2018 Rectosigmoid Carcinoma Catherine McNulty, MS IV, Tulane University School of Medicine Dr. Matthew Hartman, M.D. Medical Student Radiology Director Dr. Matthew
By: Tania Cortas, MD Arizona Oncology 03/10/2015
 By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
Beyond the APC era Alternative pathways to CRC. Jeremy R Jass McGill University
 Beyond the APC era Alternative pathways to CRC Jeremy R Jass McGill University Outline Limitations of APC model KRAS and serrated polyps CRC and CpG island methylation Serrated pathway to CRC Fusion pathways
Beyond the APC era Alternative pathways to CRC Jeremy R Jass McGill University Outline Limitations of APC model KRAS and serrated polyps CRC and CpG island methylation Serrated pathway to CRC Fusion pathways
Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations
 Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Small Bowel Cases. Introduction. Introduction, Continued 12/7/2011. Lesions Found on endoscopic biopsies Just Like Signing Out
 Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
Small Bowel Cases Lesions Found on endoscopic biopsies Just Like Signing Out Introduction Small intestinal biopsies have a few special pitfalls, for example: Neuroendocrine tumors are readily mistaken
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Colorectal Cancer. Mark Chapman. MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist
 21 st March 2018 Consultant Coloproctologist") Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Colorectal Cancer Mark Chapman MA MS FRCS EBSQ(coloproct) 21 st March 2018 Consultant Coloproctologist Overview Epidemiology of colorectal cancer Adenoma carcinoma sequence Tumour diagnosis & staging Treatment
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed