HPV vaccination Effects on cervical screening and the Compass Trial
|
|
|
- Tabitha Riley
- 6 years ago
- Views:
Transcription
1 vaccination Effects on cervical screening and the Compass Trial A/ Prof Marion Saville Executive Director VCS Inc. I am co-pi of the Compass Trial which has received support from Roche Molecular Systems and Ventana Inc., USA.
2 IN THIS TALK Update the impact of the vaccine type specific prevalence of screen detected abnormalities so far Describe the Compass trial Update on the pilot Adjustments for the main trial Lessons learned so far
3
4
5

6 National notified coverage Australia As held at Sept Excludes consumers who have opted off.
 A/Prof S Tabrizi Dr Julia Brotherton et al. www.thelancet.com/infection Published online August 6, 2014 http://dx.doi.org/10.")
7 Adjusted prevalence ratio for vaccine targeted types Fully vaccinated women 0.07 ( ) Unvaccinated women 0.65 ( ) A/Prof S Tabrizi Dr Julia Brotherton et al. Published online August 6,
8 Time (years) bandwidth =.5 17 years & younger AIS/CIN2+ histopathology: Victoria by age Apparent decline in youngest age groups Under 18 yo HGA incidence declined from 0.85% in 2006 to 0.22% in 2009 IRR 1.14 decline in incidence was 14% greater after commencement of vaccination years HGA incidence (%) years bandwidth =.5 Time (years) bandwidth =.5 Time (years) years HGA incidence (%) years and older J Brotherton et al. The Lancet 2011; 377: bandwidth =.5 Time (years) bandwidth =.5 Time (years)
 x 100.")
9 vaccine effectiveness for cervical histological outcome, by age in 2007, for completed vaccine course Footnotes: All high grade histology defined as CIN2, CIN3, AIS, and mixed CIN3/AIS. Vaccine effectiveness defined as (1- adjusted hazard rate) x 100. Age in 2007 years.
10 The Compass Trial A sentinel experience of the renewed NCSP A joint initiative of VCS and UNSW
11 Cumulative Detection Rate (per 10 5 ) Testing versus Cytology for the Prevention of Cervical Cancer Women with negative test at entry Cytology screening screening Time Since Negative Test at Entry (Years)
12 Why another primary RCT? Evaluate primary in partially vaccinated population using updated testing technology More focus on optimal management of positive women Specific evaluation of safety, effectiveness and costs in Australian context Pragmatic trial/demonstration of concept
13 Longitudinal outcomes: positive women 16 +ve at baseline Higher risk Else 18 +ve Intermediate risk Else other +ve Oncogenic -ve Low risk Cumulative CIN3+ in 20,514 women (median age 34 years) Khan MJ, Castle PE, et al. The elevated 10-year risk of cervical precancer and cancer in women with human papillomavirus () type 16 or 18 and the possible utility of type-specific testing in clinical practice. JNCI 2005
14 Why another primary RCT? Evaluate primary in partially vaccinated population using updated testing technology More focus on optimal management of positive women Specific evaluation of safety, effectiveness and costs in Australian context Pragmatic trial/demonstration of concept
15 The Compass Pilot 6-yearly screening (partial genotyping) Two arms with different follow-up for women who test positive for intermediate risk 3-yearly LBC (ThinPrep) screening
16 Pilot study 5,000 women at 1:2:2 randomisation allocation 2 primary screening technologies involved Roche COBAS QIAGEN partial genotyping
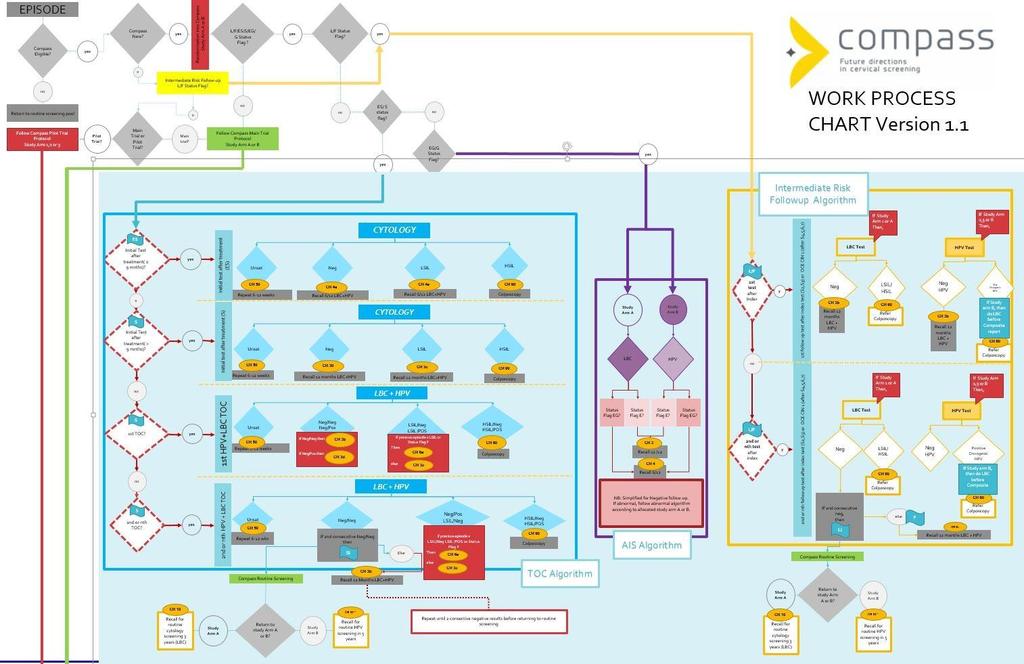
17 Woman attends for cervical screening Practitioner collects LBC sample Lab Randomise 3 yearly cytology 6 yearly test 6 Yearly test Intermediate risk Intermediate risk Intermediate risk test p16/ki67 Staining LBC
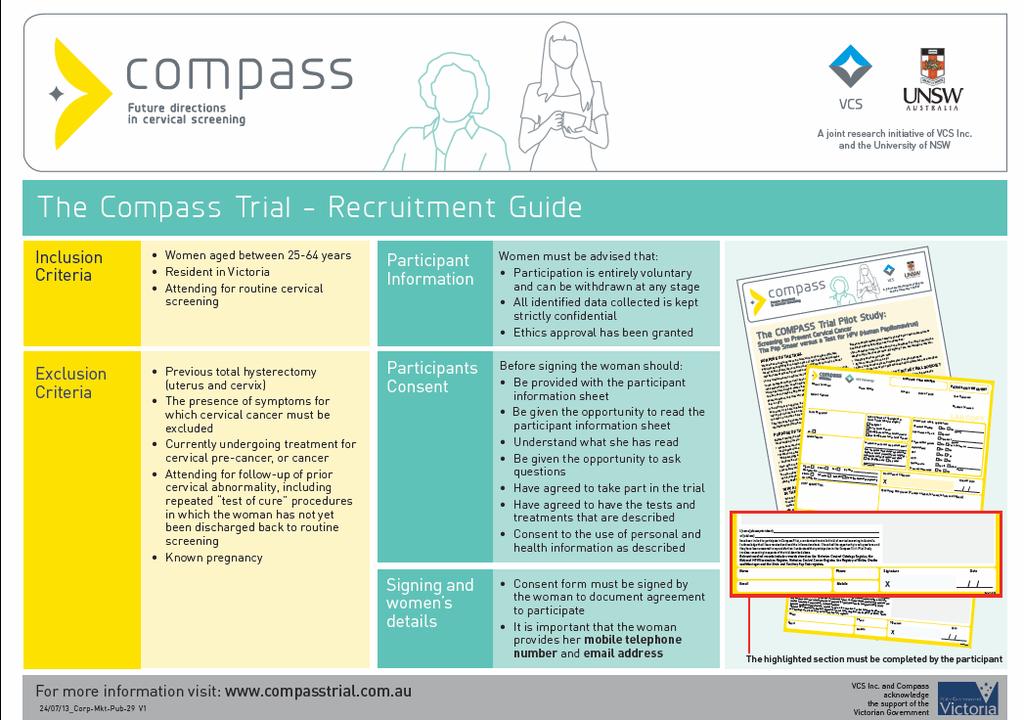
18 Population Women aged years Resident in Victoria Attending for routine cervical screening
19 Aims of the Pilot: To quantify participant and GP acceptance of randomization process and use of longer routine screening intervals Measuring the recruitment rate Assess laboratory feasibility for 2 technologies Time and motion study Unsatisfactory rate Quantify baseline test performance Positivity rates Diagnostic yield for histologically-confirmed CIN3 In vaccinated cohorts separately from unvaccinated cohorts
20
21 Randomisation Randomization occurs in the laboratory on receipt of first sample For the duration of the study the woman remains in the allocated study arm
22 What does the laboratory report contain? An overall cervical screening risk assessment Low risk, negative test Intermediate risk, infection (not 16/18 +/- 45) Higher risk, infection (16/18 +/- 45) A statement of test(s) performed and the results A recommendation for follow-up taking account of Screening history, clinical notes and laboratory findings
23

24
25
26
27
28 Follow-up of women in Compass Management of follow-up via VCCR Collecting and storing addresses and mobile telephone numbers Active recall for rescreening three months prior to the due date for the next test
29 Safety monitoring 5% of women in the arm will be recalled at 3 years for LBC If the CIN 3+ rate is higher than anticipated then the IDSMC may elect to recall all women in these arms and potentially stop the trial early In the renewed programme a similar model of safety monitoring could be utilised although the % of women required for early testing would be much lower
30 PROGRESS OF THE PILOT Consented participants: 5184 Eligible participants: 4970 No. clinics referring samples: No. clinicians referring samples
31 Lessons learned so far Acceptance by women and GPs of the longer interval seems to have been high The partial genotyping tests can be introduced into the lab using standard approaches to the introduction of new tests including appropriate training for laboratory staff 16, 18 +/- 45 rates are very low in both the older (unvaccinated) cohorts and the younger (vaccinated) cohorts A model safety-monitoring framework has been established
32 Compass main trial A sentinel experience of the Renewed NCSP Aiming to recruit 108,000 women before Renewal is implemented To confirm with empirical evidence the modelled performance of primary screening with an test and partial genotyping in a substantially vaccinated population To compare the performance of dual stain (p16/ki-67) with LBC in the triage of women with intermediate risk


33 p16/ki-67 Dual Stained Cytology
34 Adjustments to protocol Adjust screening interval for arms to 5 years, and in the LBC arm to 2.5 years Undertake LBC in samples from women who have tested positive for 16/ 18 +/- 45 To inform the interpretation and next steps after colposcopy
35 Study Arm A Image Read LBC Randomisation 1:2 (LBC:) Unsatisfactory cytology Negative cytology p/d LSIL p/d HSIL 1 Repeat LBC in 6-12 weeks Routine screening in 2.5 years-lbc Oncogenic DNA testing Colposcopy 2 Unsatisfactory Negative oncogenic Concealed Dual Stain (5%) Concealed Dual Stain Other oncogenic positive 16/18 ± 45 positive Concealed Dual Stain Repeat in 6-12 weeks Repeat cytology in 12 months (LBC) 3 Repeat test in 12 months 3 Colposcopy 2 12 months Negative cytology p/d LSIL p/d HSIL+ Concealed Dual Stain (5%) Negative 5 Positive oncogenic Concealed Dual Stain Repeat cytology in 12 months (LBC) 3 Colposcopy 2 Repeat test in 12 months 3 Colposcopy 2 12 months Negative cytology p/d LSIL p/d HSIL+ Concealed Dual Stain (5%) Negative Positive oncogenic Concealed Dual Stain Routine screening in 2.5 years (LBC) Colposcopy 2 Routine screening in 2.5 years (LBC) Colposcopy 2 Footnotes: Study arm A 1) Includes any glandular abnormality, possible HG endocervical glandular lesions and atypical glandular cells of uncertain significance. 2) If results at colposcopy are negative/cin 1/, women require two negative follow-up tests at 12 months and 24 months, using index test, before returning to routine screening (return to original study arm). If CIN 2+/AIS: treatment and follow-up according to NHMRC guidelines. Colposcopy unsatisfactory: managed by the individual specialist, informed by NHMRC 2005 guidelines (see detailed management flow charts). 3) Unless the National Cervical Screening renewal states otherwise. 4) AIS annual cytology for the life of the trial Version 1.2_DRAFT_2September2014
36 Study Arm B Oncogenic DNA Testing Randomisation 1:2 (LBC:) Unsatisfactory Negative Other hr Positive 16/18 ± 45 Positive Repeat test in 6-12 weeks Routine screening in 5 years 5% return in 2.5 years for LBC Safety Monitoring Image read LBC Colposcopy 2 Image read LBC Unsat cytology Negative cytology p/d LSIL p/d HSIL 1 Repeat LBC test in 6-12 weeks Repeat test in 12 months Repeat test in 12 months Colposcopy 2 12 months Negative Positive oncogenic Image read LBC 12 months Repeat test in 12 months Colposcopy 2 Negative Positive oncogenic Routine screening in 5 years Colposcopy 2 Footnotes: Study arm B 1) Includes any glandular abnormality, possible HG endocervical glandular lesions and atypical cells of uncertain significance. 2) If results at colposcopy are negative/cin1/, women require two negative follow-up tests at 12 months and 24 months, using index test, before returning to routine screening (return to original study arm). If CIN 2+/AIS: treatment and follow-up according to 2005 NHMRC guidelines (see detailed management flow charts). Colposcopy unsatisfactory: managed by the individual specialist, informed by NHMRC 2005 guidelines (see detailed management flow charts). 3) AIS will have test of cure until returned to routinely 5 yrly screening. Management will be similar to proposed NCSP management guidelines Version 1.2_DRAFT_2September2014
37 Study Arm B Oncogenic DNA Testing Randomisation 1:2 (LBC:) Unsatisfactory Concealed Dual Stain (5%) Negative Concealed Dual Stain Other hr Positive Concealed Dual Stain 16/18 ± 45 Positive Repeat test in 6-12 weeks Routine screening in 5 years 5% return in 2.5 years for LBC Safety Monitoring Randomisation 1:1 Image read LBC Colposcopy 2 Dual Stained Image read LBC Unsat DS Negative DS Positive DS Unsat cytology Negative cytology p/d LSIL p/d HSIL 1 Repeat DS test in 6-12 weeks Repeat test in 12 months Image read LBC Colposcopy 2 12 months Repeat LBC test in 6-12 weeks Repeat test in 12 months Repeat test in 12 months Colposcopy 2 Concealed Dual Stain (5%) Negative Positive oncogenic Concealed Dual Stain Concealed Dual Stain (5%) Negative Positive oncogenic Concealed Dual Stain Image read LBC Image read LBC Repeat test in 12 months Colposcopy 2 12 months Repeat test in 12 months Colposcopy 2 Concealed Dual Stain (5%) Negative Positive oncogenic Concealed Dual Stain Concealed Dual Stain (5%) Negative Positive oncogenic Concealed Dual Stain Routine screening in 5 years Colposcopy 2 Routine screening in 5 years Colposcopy 2 Footnotes: Study arm B 1) Includes any glandular abnormality, possible HG endocervical glandular lesions and atypical cells of uncertain significance. 2) If results at colposcopy are negative/cin1/, women require two negative follow-up tests at 12 months and 24 months, using index test, before returning to routine screening (return to original study arm). If CIN 2+/AIS: treatment and follow-up according to 2005 NHMRC guidelines (see detailed management flow charts). Colposcopy unsatisfactory: managed by the individual specialist, informed by NHMRC 2005 guidelines (see detailed management flow charts). 3) AIS will have test of cure until returned to routinely 5 yrly screening. Management will be similar to proposed NCSP management guidelines Version 1.2_DRAFT_2September2014
38 Adjustments to protocol Include all women who are presenting for screening or in follow up Women in follow up after previous LSIL would be managed as if they had a previous intermediate risk cervical screening result Women being followed after treatment for HSIL would undergo test of cure with LBC instead of conventional Pap
39
40 Adjustments to protocol Extend the upper age for recruitment to 69 years Reflecting an Exit test at 70 to 74 years as proposed for the renewed NCSP
41 The main trial challenges To have funding and ethics approval in place To complete recruitment before the Renewal is implemented
42 Lessons learned so far Need to keep the complexity within the labs and register(s) Need to continue to generate screening reports that clearly convey overall risk for cervical cancer precursors and that contain a single clinical recommendation Need to develop a language for the NCSP centred on risk The renewed programme will need a transition plan for women in follow for previous screen detected abnormalities
43 Conclusion This is a very exciting time to be involved in cervical screening We have the opportunity to have a renewed NCSP that is even more effective than our very successful current program, is less expensive and asks less of women and GPs Following the conclusion of phase 1 of Renewal we know where we are going. We still have to work out how we are going to get there, phase 2 of Renewal It is going to be enormously challenging to change the practice of the thousands of GPs around Australia and to communicate these changes to women given the high level of community understanding of Pap smears every two years message. We need to continue to learn from each other throughout this process.
 Dr. Jeffery Tan (RWH) Dr. Sally Lord (CTC) Key Responsibilities Protocol development, review and revision. Associate Investigators Dr. Stella Heley Dr.")
 Dr Michael Caruana Others to be determined Key Responsibilities Give advice on protocol and operational aspects of trial Quality Assurance Panel Histopathology Chair: A/Prof.")
 Key Responsibilities Regularly review safety data in a blinded manner Recommend study termination if pre specified stopping criteria are met Make safety or monitoring recommendations")
 Prof Jonathan Carter A/Prof Rachel Skinner Prof Suzanne Garland Prof Andrew Grulich Prof Annabelle Farnsworth Dr Deborah Bateson Dr Eduardo Franco Ms Bridget Whelan Key")
44 Co-Principal Investigators A/Prof Karen Canfell A/Prof Marion Saville Chief Investigators Dr. Phil Castle Prof Ruth Salom A/Prof. Dorota Gertig (VCS) Dr. Julia Brotherton (VCS) Dr. David Wrede (RWH) Dr. Jeffery Tan (RWH) Dr. Sally Lord (CTC) Key Responsibilities Protocol development, review and revision. Associate Investigators Dr. Stella Heley Dr. Lara Roeske Ms Gillian Phillips Dr. Jane Collins Ms Sandy Anderson Miss Jessica Darlington-Brown Dr. Andrew Martin (CTC) Dr Michael Caruana Others to be determined Key Responsibilities Give advice on protocol and operational aspects of trial Quality Assurance Panel Histopathology Chair: A/Prof. Annabelle Farnsworth Key Responsibilities Review histopathology slides in a blinded manner Data Safety Monitoring Board (Chair: Prof. Michael Quinn) Key Responsibilities Regularly review safety data in a blinded manner Recommend study termination if pre specified stopping criteria are met Make safety or monitoring recommendations as appropriate Scientific Advisory Committee (Chair: Prof. Bruce Armstrong) Prof Jonathan Carter A/Prof Rachel Skinner Prof Suzanne Garland Prof Andrew Grulich Prof Annabelle Farnsworth Dr Deborah Bateson Dr Eduardo Franco Ms Bridget Whelan Key Responsibilities Advise on study protocol development Annual progress meetings (more frequent if required) Review pilot and main trial analysis NHMRC Clinical Trials centre Key Responsibilities Provision of randomisation mechanism Contribute to statistical aspects of protocol design Key Responsibilities Laboratory Management GP Recruitment Participant recruitment Implement linkage to VCCR & NVPR Key Responsibilities Lead protocol design Data management Lead data analysis and write-up
45

46

47
The Compass trial: Informing changes to the National Cervical Screening Program
 The Compass trial: Informing changes to the National Cervical Screening Program Marion Saville I am Co-Principal Investigator on the Compass trial which has received equipment and funding contribution
The Compass trial: Informing changes to the National Cervical Screening Program Marion Saville I am Co-Principal Investigator on the Compass trial which has received equipment and funding contribution
Cervical screening and the Nurse: current and future directions. Dr Lara Roeske
 Cervical screening and the Nurse: current and future directions Dr Lara Roeske A specialist gynecological pathology laboratory Cervical cytology 300,000 per annum, predominantly conventional Cervical histopathology
Cervical screening and the Nurse: current and future directions Dr Lara Roeske A specialist gynecological pathology laboratory Cervical cytology 300,000 per annum, predominantly conventional Cervical histopathology
Innovations in screening for cervical cancer: The Australian Example
 Innovations in screening for cervical cancer: The Australian Example Karen Canfell 1. Director, Cancer Research Division, Cancer Council NSW. 3. Adjunct Professor, School of Public Health, University of
Innovations in screening for cervical cancer: The Australian Example Karen Canfell 1. Director, Cancer Research Division, Cancer Council NSW. 3. Adjunct Professor, School of Public Health, University of
The new Cervical Screening Test for Australian women: Louise Farrell
 The new Cervical Screening Test for Australian women: Louise Farrell Outline and explain the changes to the National Cervical Screening Program due to commence in Dec 2017 LEARNING OBJECTIVES FOR TODAY
The new Cervical Screening Test for Australian women: Louise Farrell Outline and explain the changes to the National Cervical Screening Program due to commence in Dec 2017 LEARNING OBJECTIVES FOR TODAY
The future of breast cancer screening in Australia: Insights from the transformation of the National Cervical Screening Program
 The future of breast cancer screening in Australia: Insights from the transformation of the National Cervical Screening Program BreastScreen Australia Conference, April 2018 Karen Canfell Director, Cancer
The future of breast cancer screening in Australia: Insights from the transformation of the National Cervical Screening Program BreastScreen Australia Conference, April 2018 Karen Canfell Director, Cancer
HPV TESTING AND THE RENEWAL PROGRAMME. Deborah Neesham Gynaecological Oncologist RWH
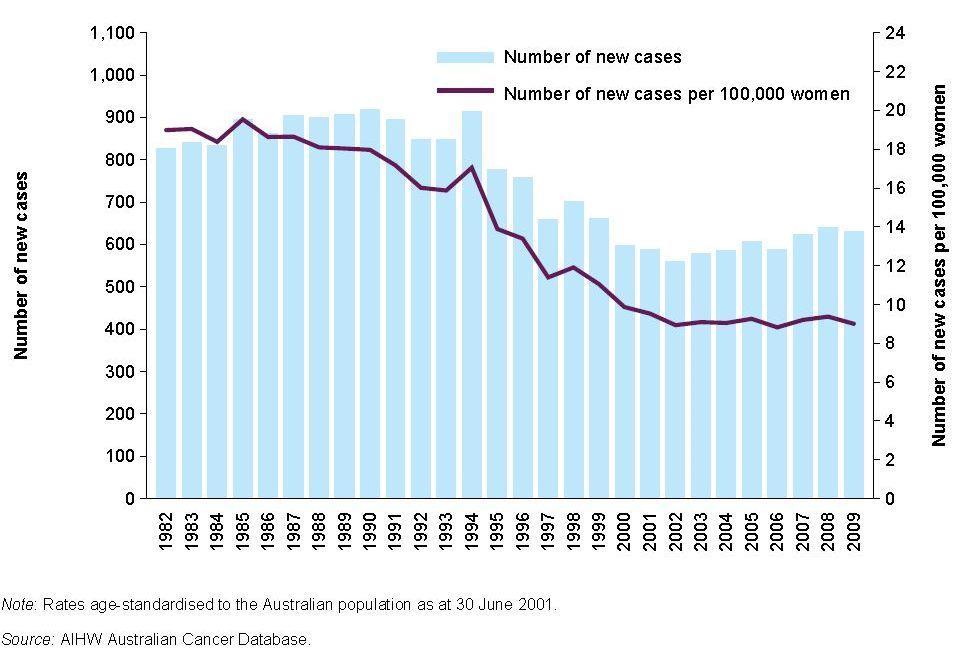
 HPV TESTING AND THE RENEWAL PROGRAMME Deborah Neesham Gynaecological Oncologist RWH Statistics AIHW 2012 801 women were diagnosed with cervical cancer in 2011 and there were 226 deaths from cervical cancer
HPV TESTING AND THE RENEWAL PROGRAMME Deborah Neesham Gynaecological Oncologist RWH Statistics AIHW 2012 801 women were diagnosed with cervical cancer in 2011 and there were 226 deaths from cervical cancer
o 2-yearly (Pap test) o 18 to 69 years 1 o Registry reminder
 o 18 to 69 years 1 o Registry reminder") Invasive cervical cancer cases per 100,000 Main changes from Dec 2017 The Renewed National Cervical Screening Program The Big Picture Brisbane 22 nd April 2017 Ian Hammond National Cervical Screening Program:
Invasive cervical cancer cases per 100,000 Main changes from Dec 2017 The Renewed National Cervical Screening Program The Big Picture Brisbane 22 nd April 2017 Ian Hammond National Cervical Screening Program:
The National Cervical Screening Program: On the Cusp of Change
 The National Cervical Screening Program: On the Cusp of Change A/Prof Marion Saville I am Co-Principal Investigator on the Compass trial which has received equipment and funding contribution from Roche
The National Cervical Screening Program: On the Cusp of Change A/Prof Marion Saville I am Co-Principal Investigator on the Compass trial which has received equipment and funding contribution from Roche
The Introduction of Primary HPV Screening in Australia
 The Introduction of Primary HPV Screening in Australia Dr Louise Farrell Member: Steering Committee Renewal Implementation Project National Cervical Screening Program, Department of Health Australia Head
The Introduction of Primary HPV Screening in Australia Dr Louise Farrell Member: Steering Committee Renewal Implementation Project National Cervical Screening Program, Department of Health Australia Head
The Renewed National Cervical Screening Program
 The Renewed National Cervical Screening Program Implementing the Changes IAN HAMMOND, ALISON LANG & TRACEY BESSELL What are the changes 5 yearly HPV test, partial genotyping Reflex liquid based cytology
The Renewed National Cervical Screening Program Implementing the Changes IAN HAMMOND, ALISON LANG & TRACEY BESSELL What are the changes 5 yearly HPV test, partial genotyping Reflex liquid based cytology
Preventing cervical cancer Australia. The Renewed National Cervical Screening Program 2019 Common Questions and Cases
 The Renewed National Cervical Screening Program 2019 Common Questions and Cases Preventing cervical cancer Australia - National HPV vaccination program - The National cervical screening program Annabelle
The Renewed National Cervical Screening Program 2019 Common Questions and Cases Preventing cervical cancer Australia - National HPV vaccination program - The National cervical screening program Annabelle
Screening for the Precursors of Cervical Cancer in the Era of HPV Vaccination. Dr Stella Heley Senior Liaison Physician Victorian Cytology Service
 Screening for the Precursors of Cervical Cancer in the Era of HPV Vaccination Dr Stella Heley Senior Liaison Physician Victorian Cytology Service Victorian Cytology Service Dr Stella Heley Dr Siobhan Bourke
Screening for the Precursors of Cervical Cancer in the Era of HPV Vaccination Dr Stella Heley Senior Liaison Physician Victorian Cytology Service Victorian Cytology Service Dr Stella Heley Dr Siobhan Bourke
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors.
 Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Smith M, Lew JB, Simms K, Canfell K. Impact of HPV sample self-collection
Appendix This appendix was part of the submitted manuscript and has been peer reviewed. It is posted as supplied by the authors. Appendix to: Smith M, Lew JB, Simms K, Canfell K. Impact of HPV sample self-collection
Women s and Children s Health Network
 Women s and Children s Health Network South Australian Cervix Screening Registry Statistical Report 2013 Editorial Committee Victorian Cytology Service (VCS): Professor Dorota Gertig, SACSR Medical Director
Women s and Children s Health Network South Australian Cervix Screening Registry Statistical Report 2013 Editorial Committee Victorian Cytology Service (VCS): Professor Dorota Gertig, SACSR Medical Director
Declining endocervical rates: does it matter? Dorota Gertig Medical Director, VCCR
 Declining endocervical rates: does it matter? Dorota Gertig Medical Director, VCCR Background Outline Current recommendations Australian and international Review key studies Data from AIHW and VCCR Analysis
Declining endocervical rates: does it matter? Dorota Gertig Medical Director, VCCR Background Outline Current recommendations Australian and international Review key studies Data from AIHW and VCCR Analysis
Impact for Indigenous Women: The VIP-I study and the National HPV Vaccine Program
 Impact for Indigenous Women: The VIP-I study and the National HPV Vaccine Program Dina Saulo 1, Skye McGregor 1, Sepehr Tabrizi 3, Suzanne Garland 3, Julia Brotherton 4,3, Bette Liu 1,2 Rachel Skinner
Impact for Indigenous Women: The VIP-I study and the National HPV Vaccine Program Dina Saulo 1, Skye McGregor 1, Sepehr Tabrizi 3, Suzanne Garland 3, Julia Brotherton 4,3, Bette Liu 1,2 Rachel Skinner
The Future of Cervical Screening. Jenny Ross
 The Future of Cervical Screening Jenny Ross Introduction Cervical cancer and the Pap smear History of cervical screening in Australia New knowledge about HPV and cervical cancer HPV Vaccination Program
The Future of Cervical Screening Jenny Ross Introduction Cervical cancer and the Pap smear History of cervical screening in Australia New knowledge about HPV and cervical cancer HPV Vaccination Program
NATIONAL CERVICAL SCREENING PROGRAMME
 NATIONAL CERVICAL SCREENING PROGRAMME ADVISORY GROUP MINUTES TUESDAY 25 NOVEMBER 2014 Venue: Start time: Advisory Group Members Attendees Apologies: Ministry of Health Attendees: University of New South
NATIONAL CERVICAL SCREENING PROGRAMME ADVISORY GROUP MINUTES TUESDAY 25 NOVEMBER 2014 Venue: Start time: Advisory Group Members Attendees Apologies: Ministry of Health Attendees: University of New South
National Cervical Screening Program MBS Item Descriptors
 National Cervical Screening Program MBS Item Descriptors Item Item descriptor 73070 A test, including partial genotyping, for oncogenic human papillomavirus that may be associated with cervical pre-cancer
National Cervical Screening Program MBS Item Descriptors Item Item descriptor 73070 A test, including partial genotyping, for oncogenic human papillomavirus that may be associated with cervical pre-cancer
The Renewed National Cervical Screening Program:
 The Renewed National Cervical Screening Program: Key information for Health Professionals Contents: Overview: National Cervical Screening Program... 2 Background: HPV and cervical cancer... 3 HPV testing
The Renewed National Cervical Screening Program: Key information for Health Professionals Contents: Overview: National Cervical Screening Program... 2 Background: HPV and cervical cancer... 3 HPV testing
XXV. HPV disease: Prevention and. management in the 21st century. SCIENTIFIC MEETING SYDNEY 2017
 XXV SCIENTIFIC MEETING SYDNEY 2017 Prevention and HPV disease: management in the 21st century Sofitel Sydney Australia 16th - 19th March 2017 www.asccp.com.au HPV disease: Prevention and management in
XXV SCIENTIFIC MEETING SYDNEY 2017 Prevention and HPV disease: management in the 21st century Sofitel Sydney Australia 16th - 19th March 2017 www.asccp.com.au HPV disease: Prevention and management in
Northern Ireland Cervical Screening Programme
 Northern Ireland Cervical Screening Programme ANNUAL REPORT & STATISTICAL BULLETIN 2010-2011 1 Report produced by : Quality Assurance Reference Centre, PHA Date of Publication: September 2012 2 Contents
Northern Ireland Cervical Screening Programme ANNUAL REPORT & STATISTICAL BULLETIN 2010-2011 1 Report produced by : Quality Assurance Reference Centre, PHA Date of Publication: September 2012 2 Contents
Natural History of HPV Infections 15/06/2015. Squamous cell carcinoma Adenocarcinoma
 14,670 5796 United States/ Canada 17,165 8124 Central America 48,328 21,402 South America 59,929 29,814 Europe 78,896 61,670 Africa 157,759 86,708 Southcentral Asia 61,132 31,314 Eastern Asia 42,538 22,594
14,670 5796 United States/ Canada 17,165 8124 Central America 48,328 21,402 South America 59,929 29,814 Europe 78,896 61,670 Africa 157,759 86,708 Southcentral Asia 61,132 31,314 Eastern Asia 42,538 22,594
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines
 Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Appropriate Use of Cytology and HPV Testing in the New Cervical Cancer Screening Guidelines Tim Kremer, MD Ralph Anderson, MD 1 Objectives Describe the natural history of HPV particularly as it relates
Cervical cancer screening in Norway
 Cervical cancer screening in Norway «The future of cancer screening in Estonia: health benefits and best practices» 17 November 2016, Tartu Stefan Lönnberg Cancer Registry of Norway Screening governance
Cervical cancer screening in Norway «The future of cancer screening in Estonia: health benefits and best practices» 17 November 2016, Tartu Stefan Lönnberg Cancer Registry of Norway Screening governance
Cervical Cancer Screening. David Quinlan December 2013
 Cervical Cancer Screening David Quinlan December 2013 Cervix Cervical Cancer Screening Modest variation provincially WHO and UK begin at 25 stop at 60 Finland begin at 30 stop at 60 Rationale for
Cervical Cancer Screening David Quinlan December 2013 Cervix Cervical Cancer Screening Modest variation provincially WHO and UK begin at 25 stop at 60 Finland begin at 30 stop at 60 Rationale for
ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests
 ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests www.treatmentok.com Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Ann Arbor, Michigan Disclosures
ASCCP 2013 Guidelines for Managing Abnormal Cervical Cancer Screening Tests www.treatmentok.com Barbara S. Apgar, MD, MS Professor of Family Medicine University of Michigan Ann Arbor, Michigan Disclosures
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma
 Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
Lessons From Cases of Screened Women Who Developed Cervical Carcinoma R. Marshall Austin MD,PhD Magee-Womens Hospital of University of Pittsburgh Medical Center raustin@magee.edu Why Focus Study On Cases
COLPOSCOPY QUALITY IMPROVEMENT PROGRAM (C QuIP) VICTORIAN CERVICAL CYTOLOGY REGISTRY PILOT STUDY. Dorota Gertig, Marion Saville
 VICTORIAN CERVICAL CYTOLOGY REGISTRY PILOT STUDY. Dorota Gertig, Marion Saville") COLPOSCOPY QUALITY IMPROVEMENT PROGRAM (C QuIP) VICTORIAN CERVICAL CYTOLOGY REGISTRY PILOT STUDY Dorota Gertig, Marion Saville on behalf of the C QuIP Steering Committee June 2013 1 CONTENTS 1. Executive
COLPOSCOPY QUALITY IMPROVEMENT PROGRAM (C QuIP) VICTORIAN CERVICAL CYTOLOGY REGISTRY PILOT STUDY Dorota Gertig, Marion Saville on behalf of the C QuIP Steering Committee June 2013 1 CONTENTS 1. Executive
Aboriginal and Torres Strait Islander women and cervical cancer prevention. Menzies School of Health
 Aboriginal and Torres Strait Islander women and cervical cancer prevention Menzies School of Health Research @lisa_j_whop Cervical cancer incidence, worldwide GLOBOCAN 2012 Indigenous Australian women
Aboriginal and Torres Strait Islander women and cervical cancer prevention Menzies School of Health Research @lisa_j_whop Cervical cancer incidence, worldwide GLOBOCAN 2012 Indigenous Australian women
NATIONAL CERVICAL CANCER SCREENING PROGRAMME Monitor 2017
 a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a NATIONAL CERVICAL CANCER SCREENING PROGRAMME Monitor
a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a a NATIONAL CERVICAL CANCER SCREENING PROGRAMME Monitor
BUILDING TRUST, MANAGING RISK: VACCINE CONFIDENCE AND HUMAN PAPILLOMAVIRUS VACCINATION
 BUILDING TRUST, MANAGING RISK: VACCINE CONFIDENCE AND HUMAN PAPILLOMAVIRUS VACCINATION Associate Professor Kristine Macartney Deputy Director, National Centre for Immunisation Research & Surveillance www.ncirs.usyd.edu.au
BUILDING TRUST, MANAGING RISK: VACCINE CONFIDENCE AND HUMAN PAPILLOMAVIRUS VACCINATION Associate Professor Kristine Macartney Deputy Director, National Centre for Immunisation Research & Surveillance www.ncirs.usyd.edu.au
Cuid d Fheidhmeannacht na Seirbhíse Sláinte. Part of the Health Service Executive. CS/PR/PM-20 Rev 2 ISBN Programme Report 2014/2015
 Programme Report 2014/2015 Contents Summary points 2 Introduction to the statistics 2014/2015 3 Part 1 Cervical screening activity 3 Programme coverage 4 Laboratory turnaround time 7 Notification of results
Programme Report 2014/2015 Contents Summary points 2 Introduction to the statistics 2014/2015 3 Part 1 Cervical screening activity 3 Programme coverage 4 Laboratory turnaround time 7 Notification of results
Evidence-based treatment of a positive HPV DNA test. Th. Agorastos Prof. of Obstetrics & Gynaecology Aristotle University Thessaloniki/GR
 Evidence-based treatment of a positive HPV DNA test Th. Agorastos Prof. of Obstetrics & Gynaecology Aristotle University Thessaloniki/GR HPV DNA testing Indications 1. Triage after cytology with ASCUS/LSIL
Evidence-based treatment of a positive HPV DNA test Th. Agorastos Prof. of Obstetrics & Gynaecology Aristotle University Thessaloniki/GR HPV DNA testing Indications 1. Triage after cytology with ASCUS/LSIL
Proposed new national cervical screening program. Dr Elizabeth Jackson Obstetrician Gynaecologist Cairns
 Proposed new national cervical screening program Dr Elizabeth Jackson Obstetrician Gynaecologist Cairns www.drelizabethjackson.com Cervical cancer in Australia 12th most common cancer affecting Australian
Proposed new national cervical screening program Dr Elizabeth Jackson Obstetrician Gynaecologist Cairns www.drelizabethjackson.com Cervical cancer in Australia 12th most common cancer affecting Australian
Pushing the Boundaries of the Lab Diagnosis in Asia
 Pushing the Boundaries of the Lab Diagnosis in Asia Diana Lim MBBS, FRCPA, FRCPath (UK) Senior Consultant National University Health System and National University of Singapore Department of Pathology
Pushing the Boundaries of the Lab Diagnosis in Asia Diana Lim MBBS, FRCPA, FRCPath (UK) Senior Consultant National University Health System and National University of Singapore Department of Pathology
The new European (and Italian) guidelines for cervical screening will recommend PAP from 25 to 34 HPV (+ triage) from 35 to 64
 guidelines for cervical screening will recommend PAP from 25 to 34 HPV (+ triage) from 35 to 64") The new European (and Italian) guidelines for cervical screening will recommend PAP from 25 to 34 HPV (+ triage) from 35 to 64 risk of overdiagnosis and over treatment Failures in reproductive functioning:
The new European (and Italian) guidelines for cervical screening will recommend PAP from 25 to 34 HPV (+ triage) from 35 to 64 risk of overdiagnosis and over treatment Failures in reproductive functioning:
Primary High Risk HPV Testing with Cytology Triage
 Primary High Risk HPV Testing with Cytology Triage NHS Cervical Screening Programme Public Health England leads the NHS Screening Programmes Human papillomavirus (HPV) High risk (HR) HPV is associated
Primary High Risk HPV Testing with Cytology Triage NHS Cervical Screening Programme Public Health England leads the NHS Screening Programmes Human papillomavirus (HPV) High risk (HR) HPV is associated
The Control of Cervical Cancer in New Zealand: Achievements and Prospects
 The Control of Cervical Cancer in New Zealand: Achievements and Prospects August 5 th 2016, Potter s Park Event centre, Auckland Purpose of the Symposium The purpose of the one day forum, organised by
The Control of Cervical Cancer in New Zealand: Achievements and Prospects August 5 th 2016, Potter s Park Event centre, Auckland Purpose of the Symposium The purpose of the one day forum, organised by
Human papillomavirus and vaccination for cervical cancer
 Human papillomavirus and vaccination for cervical cancer Dorothy Machalek Department of Microbiology and Infectious Diseases Royal Women s Hospital, Melbourne, Australia VIRUSES AND CANCER Responsible
Human papillomavirus and vaccination for cervical cancer Dorothy Machalek Department of Microbiology and Infectious Diseases Royal Women s Hospital, Melbourne, Australia VIRUSES AND CANCER Responsible
Changes to cervical screening. Information for patients
 Changes to cervical screening Information for patients On December 1, 2017, cervical cancer screening in Australia changed from two-yearly Pap testing to five-yearly HPV testing. Why has cervical screening
Changes to cervical screening Information for patients On December 1, 2017, cervical cancer screening in Australia changed from two-yearly Pap testing to five-yearly HPV testing. Why has cervical screening
European Union survey on organization and quality control of cervical cancer screening and HPV vaccination programs
 European Union survey on organization and quality control of cervical cancer screening and HPV vaccination programs Introduction to the Survey The purpose of this project is to collect information regarding
European Union survey on organization and quality control of cervical cancer screening and HPV vaccination programs Introduction to the Survey The purpose of this project is to collect information regarding
Making Sense of Cervical Cancer Screening
 Making Sense of Cervical Cancer Screening New Guidelines published November 2012 Tammie Koehler DO, FACOG The incidence of cervical cancer in the US has decreased more than 50% in the past 30 years because
Making Sense of Cervical Cancer Screening New Guidelines published November 2012 Tammie Koehler DO, FACOG The incidence of cervical cancer in the US has decreased more than 50% in the past 30 years because
Future Directions for HPV and Cervical Screening. Jane Grant Metro Auckland Cervical Screening Forum June 2017
 Future Directions for HPV and Cervical Screening Jane Grant Metro Auckland Cervical Screening Forum June 2017 HPV Primary Screening HPV Self Sampling Research Source: Cervical Cancer : Symptoms, Stages
Future Directions for HPV and Cervical Screening Jane Grant Metro Auckland Cervical Screening Forum June 2017 HPV Primary Screening HPV Self Sampling Research Source: Cervical Cancer : Symptoms, Stages
SESSION J4. What's Next? Managing Abnormal PAPs in 2014
 37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION J4 What's Next? Managing Abnormal PAPs in 2014 Session Description: Linda Eckert, MD Review current guidelines
37th Annual Advanced Practice in Primary and Acute Care Conference: October 9-11, 2014 2:45 SESSION J4 What's Next? Managing Abnormal PAPs in 2014 Session Description: Linda Eckert, MD Review current guidelines
EFCS Symposium. Is cervical cancer screening based on HPV testing with cytology triage as safe as perceived?
 EFCS Symposium Is cervical cancer screening based on HPV testing with cytology triage as safe as perceived? Amanda Herbert Guy s & St Thomas NHS Foundation Trust Is cervical cancer screening based on HPV
EFCS Symposium Is cervical cancer screening based on HPV testing with cytology triage as safe as perceived? Amanda Herbert Guy s & St Thomas NHS Foundation Trust Is cervical cancer screening based on HPV
HPV Primary Screening Update. Prof. Vu Ba Quyet Director of NO&G hospital
 HPV Primary Screening Update Prof. Vu Ba Quyet Director of NO&G hospital 1 Who can we not worry about? 2 Key questions Who should be screened? Starting age? Ending age? How often? How to manage results?
HPV Primary Screening Update Prof. Vu Ba Quyet Director of NO&G hospital 1 Who can we not worry about? 2 Key questions Who should be screened? Starting age? Ending age? How often? How to manage results?
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines. June 2013
 Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
Cervical Cancer Screening for the Primary Care Physician for Average Risk Individuals Clinical Practice Guidelines General Principles: Since its introduction in 1943, Papanicolaou (Pap) smear is widely
P16 et Ki67 Biomarkers: new tool for risk management and low grade intraepithelial lesions (LGSIL): be ready for the future.
: be ready for the future.") P16 et Ki67 Biomarkers: new tool for risk management and low grade intraepithelial lesions (LGSIL): be ready for the future. Mark H Stoler, MD University of Virginia Health System, Charlottesville, VA,
P16 et Ki67 Biomarkers: new tool for risk management and low grade intraepithelial lesions (LGSIL): be ready for the future. Mark H Stoler, MD University of Virginia Health System, Charlottesville, VA,
CINtec PLUS and the Pap smear: a co-testing alternative
 CINtec PLUS and the Pap smear: a co-testing alternative Rosemary Tambouret MD p16/ki67 (CINtec PLUS) and the Pap smear Rosemary Tambouret MD CINtec PLUS dual stain: p16 and Ki67 p16 is anti-proliferative
CINtec PLUS and the Pap smear: a co-testing alternative Rosemary Tambouret MD p16/ki67 (CINtec PLUS) and the Pap smear Rosemary Tambouret MD CINtec PLUS dual stain: p16 and Ki67 p16 is anti-proliferative
6 th EFC Satellite meeting, Saturday 1 st December 2018
 6 th EFC Satellite meeting, Saturday 1 st December 2018 Introduction Pekka Nieminen President-elect of the European Federation for Colposcopy, Department of Obstetrics and Gynaecology, Helsinki University
6 th EFC Satellite meeting, Saturday 1 st December 2018 Introduction Pekka Nieminen President-elect of the European Federation for Colposcopy, Department of Obstetrics and Gynaecology, Helsinki University
Guidelines for cervical cancer screening in South Africa
 Southern African Journal of Gynaecological Oncology 2017; 9(1):8-12 Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Southern African Journal of Gynaecological Oncology 2017; 9(1):8-12 Open Access article distributed under the terms of the Creative Commons License [CC BY-NC-ND 4.0] http://creativecommons.org/licenses/by-nc-nd/4.0
Cervical Cancer Prevention in the 21 st Century Changing Paradigms
 Cervical Cancer Prevention in the 21 st Century Changing Paradigms Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M.
Cervical Cancer Prevention in the 21 st Century Changing Paradigms Teresa M. Darragh, MD UCSF Departments of Pathology and Obstetrics, Gynecology & Reproductive Sciences Faculty Disclosures: Teresa M.
UICC HPV and CERVICAL CANCER CURRICULUM. UICC HPV and Cervical Cancer Curriculum Chapter 5. Application of HPV vaccines Prof. Suzanne Garland MD
 UICC HPV and CERVICAL CANCER CURRICULUM 01 Chapter 5. Application of HPV vaccines Director of Microbiological Research Director of Clinical Microbiology and Infectious Diseases The Royal Women's Hospital
UICC HPV and CERVICAL CANCER CURRICULUM 01 Chapter 5. Application of HPV vaccines Director of Microbiological Research Director of Clinical Microbiology and Infectious Diseases The Royal Women's Hospital
Human Papillomaviruses: Biology and Laboratory Testing
 For our patients and our population Human Papillomaviruses: Biology and Laboratory Testing Geoffrey Higgins Microbiology and Infectious Diseases For our patients and our population HPV Associated Cancers
For our patients and our population Human Papillomaviruses: Biology and Laboratory Testing Geoffrey Higgins Microbiology and Infectious Diseases For our patients and our population HPV Associated Cancers
Cervical cancer prevention: Advances in primary screening and triage system
 Cervical cancer prevention: Advances in primary screening and triage system Dr Farid Hadi Regional Medical and Scientific Affairs Roche Diagnostics Asia-Pacific, Singapore Cervical cancer is highly preventable
Cervical cancer prevention: Advances in primary screening and triage system Dr Farid Hadi Regional Medical and Scientific Affairs Roche Diagnostics Asia-Pacific, Singapore Cervical cancer is highly preventable
Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA
 Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA Cancer Care Ontario Cervical Cancer Screening Goals Increase patient participation in cervical screening Increase primary care
Screening for Cervical Cancer: Demystifying the Guidelines DR. NEERJA SHARMA Cancer Care Ontario Cervical Cancer Screening Goals Increase patient participation in cervical screening Increase primary care
Details of HPV-based Cervical Cancer Screening in Turkey
 Details of HPV-based Cervical Cancer Screening in Turkey Murat Gultekin, MD, Assoc. Prof., Gyn Oncol Divison Cervical Cancer in Turkey Incidence: 4-5 /100.000 (Years 2004-2015) Annual New Cases: 1.800
Details of HPV-based Cervical Cancer Screening in Turkey Murat Gultekin, MD, Assoc. Prof., Gyn Oncol Divison Cervical Cancer in Turkey Incidence: 4-5 /100.000 (Years 2004-2015) Annual New Cases: 1.800
Beyond Pap Morphological Triage: p16/ki67 Dual Staining
 Moving away from Beyond Pap Morphological Triage: p16/ki67 Dual Staining Nicolas Wentzensen MD, PhD, MS Deputy Chief, Clinical Genetics Branch; Head, Clinical Epidemiology Unit National Cancer Institute
Moving away from Beyond Pap Morphological Triage: p16/ki67 Dual Staining Nicolas Wentzensen MD, PhD, MS Deputy Chief, Clinical Genetics Branch; Head, Clinical Epidemiology Unit National Cancer Institute
Submission from the Auckland Regional Public Health Service on the Proposed New Guidelines for the Management of Women with Abnormal Cervical Smears
 Regional Public Health Service Cornwall Complex Floor 2, Building 15 Greenlane Clinical Centre Private Bag 92 605 Symonds Street New Zealand Telephone: 09-623 4600 Facsimile: 09-623 4633 6 December 2006
Regional Public Health Service Cornwall Complex Floor 2, Building 15 Greenlane Clinical Centre Private Bag 92 605 Symonds Street New Zealand Telephone: 09-623 4600 Facsimile: 09-623 4633 6 December 2006
HPV Genotyping: A New Dimension in Cervical Cancer Screening Tests
 HPV Genotyping: A New Dimension in Cervical Cancer Screening Tests Lee P. Shulman MD The Anna Ross Lapham Professor in Obstetrics and Gynecology and Chief, Division of Clinical Genetics Feinberg School
HPV Genotyping: A New Dimension in Cervical Cancer Screening Tests Lee P. Shulman MD The Anna Ross Lapham Professor in Obstetrics and Gynecology and Chief, Division of Clinical Genetics Feinberg School
Case Based Problems. Recommended Guidelines. Workshop: Case Management of Abnormal Pap Smears and Colposcopies. Disclosure
 Disclosure Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Associate Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics This
Disclosure Workshop: Case Management of Abnormal Pap Smears and Colposcopies Rebecca Jackson, MD Associate Professor Obstetrics, Gynecology & Reproductive Sciences and Epidemiology & Biostatistics This
Study Number: Title: Rationale: Phase: Study Period Study Design: Centres: Indication Treatment: Objectives: Primary Outcome/Efficacy Variable:
 The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
The study listed may include approved and non-approved uses, formulations or treatment regimens. The results reported in any single study may not reflect the overall results obtained on studies of a product.
How invasive cervical cancer audit affects clinical practice
 How invasive cervical cancer audit affects clinical practice Referring to NHSCSP and EU guidelines and audits in Southampton and London Amanda Herbert Guy s & St Thomas Foundation NHS Trust How invasive
How invasive cervical cancer audit affects clinical practice Referring to NHSCSP and EU guidelines and audits in Southampton and London Amanda Herbert Guy s & St Thomas Foundation NHS Trust How invasive
Early effect of the HPV vaccination programme on cervical abnormalities in Victoria, Australia: an ecological study
 Early effect of the HPV vaccination programme on cervical abnormalities in Victoria, Australia: an ecological study Julia M L Brotherton, Masha Fridman, Cathryn L May, Genevieve Chappell, A Marion Saville,
Early effect of the HPV vaccination programme on cervical abnormalities in Victoria, Australia: an ecological study Julia M L Brotherton, Masha Fridman, Cathryn L May, Genevieve Chappell, A Marion Saville,
Cervical Cancer 4/27/2016
 Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical College of Wisconsin May 6, 2016 Cervical Cancer In US about
Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical College of Wisconsin May 6, 2016 Cervical Cancer In US about
Management Algorithms for Abnormal Cervical Cytology and Colposcopy
 Management Algorithms for Abnormal Cervical Cytology and Colposcopy Table of Contents Standard Colposcopic Definitions... 1 Guidelines for the Assessment of Abnormal Cervical Cytology... 2 Ia: Persistent
Management Algorithms for Abnormal Cervical Cytology and Colposcopy Table of Contents Standard Colposcopic Definitions... 1 Guidelines for the Assessment of Abnormal Cervical Cytology... 2 Ia: Persistent
Clinical Policy Title: Fluorescence in situ hybridization for cervical cancer screening
 Clinical Policy Title: Fluorescence in situ hybridization for cervical cancer screening Clinical Policy Number: 01.01.02 Effective Date: April 1, 2015 Initial Review Date: January 21, 2015 Most Recent
Clinical Policy Title: Fluorescence in situ hybridization for cervical cancer screening Clinical Policy Number: 01.01.02 Effective Date: April 1, 2015 Initial Review Date: January 21, 2015 Most Recent
Clinical outcomes after conservative management of CIN1/2, CIN2, and CIN2/3 in women ages years
 Clinical outcomes after conservative management of CIN1/2, CIN2, and CIN2/3 in women ages 21-39 years Michelle I. Silver, PhD, ScM Cancer Prevention Fellow National Cancer Institute Division of Cancer
Clinical outcomes after conservative management of CIN1/2, CIN2, and CIN2/3 in women ages 21-39 years Michelle I. Silver, PhD, ScM Cancer Prevention Fellow National Cancer Institute Division of Cancer
Cervical Cancer Screening Guidelines Update
 Frontier AIDS Education and Training Center Cervical Cancer Screening Guidelines Update Hillary Liss, MD Harborview Medical Center, Madison and Adult Medicine Clinics Frontier AETC, Medical Program Director
Frontier AIDS Education and Training Center Cervical Cancer Screening Guidelines Update Hillary Liss, MD Harborview Medical Center, Madison and Adult Medicine Clinics Frontier AETC, Medical Program Director
Goals. In the News. Primary HPV Screening 3/9/2015. Your PAP and HPV Update Primary HPV Testing- Screening Intervals- HPV Vaccine Updates-
 Your PAP and HPV Update 2015 Connie Mao, MD University of Washington Goals Primary HPV Testing- Is it time to stop doing pap smears? Screening Intervals- Should patients have a choice? HPV Vaccine Updates-
Your PAP and HPV Update 2015 Connie Mao, MD University of Washington Goals Primary HPV Testing- Is it time to stop doing pap smears? Screening Intervals- Should patients have a choice? HPV Vaccine Updates-
Recent Changes in Cervical Cancer Screening in Canada
 Recent Changes in Cervical Cancer Screening in Canada Meg McLachlin, MD, FRCPC Program Head, Pathology Senior Medical Director, Diagnostic Services Recent Changes in Cervical Cancer Screening in Canada
Recent Changes in Cervical Cancer Screening in Canada Meg McLachlin, MD, FRCPC Program Head, Pathology Senior Medical Director, Diagnostic Services Recent Changes in Cervical Cancer Screening in Canada
Department of Health Standard for the Cervical Cancer Screening Program. Approval Date: 08 May 2018 Effective Date: 13 May 2018
 Document Title: Department of Health Standard for the Cervical Cancer Screening Program Document Ref. Number: DOH/CCSC/SD/1.0 Version: 1.0 Approval Date: 08 May 2018 Effective Date: 13 May 2018 Last Reviewed:
Document Title: Department of Health Standard for the Cervical Cancer Screening Program Document Ref. Number: DOH/CCSC/SD/1.0 Version: 1.0 Approval Date: 08 May 2018 Effective Date: 13 May 2018 Last Reviewed:
Molecular Triage: Partial and Extended Genotyping and More!
 Molecular Triage: Partial and Extended Genotyping and More! Thomas C. Wright, Jr. MD Professor Emeritus Columbia University, New York Pathologist, Enzo Clinical Laboratories, Farmingdale, NY Disclosures
Molecular Triage: Partial and Extended Genotyping and More! Thomas C. Wright, Jr. MD Professor Emeritus Columbia University, New York Pathologist, Enzo Clinical Laboratories, Farmingdale, NY Disclosures
The society for lower genital tract disorders since 1964.
 The society for lower genital tract disorders since 1964. Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
The society for lower genital tract disorders since 1964. Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
!"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$
*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$") !"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$ Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
!"#$%&'(#)*$+&,$-&.#,$/#0()1-$ ),1')$2(%&,2#,%$%(0'#$34567$ Updated Consensus Guidelines for Managing Abnormal Cervical Cancer Screening Tests and Cancer Precursors American Society for and Cervical Pathology
Colposcopy Standards Working Group 2: Risk-based colposcopy
 Colposcopy Standards Working Group 2: Risk-based colposcopy Chairs: Nicolas Wentzensen and L. Stewart Massad Members: Mark Schiffman, Michelle Khan, Rebecca Perkins, Katie Smith, Julia Gage, Michael Gold,
Colposcopy Standards Working Group 2: Risk-based colposcopy Chairs: Nicolas Wentzensen and L. Stewart Massad Members: Mark Schiffman, Michelle Khan, Rebecca Perkins, Katie Smith, Julia Gage, Michael Gold,
No Disclosures. Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results. Objectives 5/9/2016
 Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical Director, PPWI Medical College of Wisconsin May 6,
Updated Guidelines for Cervical Cancer Screening and Prevention Management of Abnormal Results Kathy A. King, MD Assistant Professor of OB/GYN Medical Director, PPWI Medical College of Wisconsin May 6,
The role of human papillomavirus testing in the management of women with low-grade abnormalities: multicentre randomised controlled trial
 DOI: 10.1111/j.1471-0528.2010.02519.x www.bjog.org Epidemiology The role of human papillomavirus testing in the management of women with low-grade abnormalities: multicentre randomised controlled trial
DOI: 10.1111/j.1471-0528.2010.02519.x www.bjog.org Epidemiology The role of human papillomavirus testing in the management of women with low-grade abnormalities: multicentre randomised controlled trial
The devil is in the details
 The cobas KNOW THE RISK For cervical cancer prevention The devil is in the details Leading with the cobas as your primary screening method uncovers disease missed by cytology, and can protect women from
The cobas KNOW THE RISK For cervical cancer prevention The devil is in the details Leading with the cobas as your primary screening method uncovers disease missed by cytology, and can protect women from
Programme Report Irish Cervical Screening Programme. October 2000 to August 2008
 Programme Report Irish Cervical Screening Programme October 2000 to August 2008 Members of the Board of the National Cancer Screening Service Dr Sheelah Ryan, Chairperson Dr Gráinne Flannelly Dr Marie
Programme Report Irish Cervical Screening Programme October 2000 to August 2008 Members of the Board of the National Cancer Screening Service Dr Sheelah Ryan, Chairperson Dr Gráinne Flannelly Dr Marie
HPV: cytology and molecular testing
 HPV: cytology and molecular testing Human Papillomavirus and how we test for it at Medlab Central Palmerston North for Cervical Cancer prevention and management. Developed by Reem Mustafa Cytology and
HPV: cytology and molecular testing Human Papillomavirus and how we test for it at Medlab Central Palmerston North for Cervical Cancer prevention and management. Developed by Reem Mustafa Cytology and
Preventing Cervical Cancer 2018 WHAT THIS WILL MEAN FOR PRIMARY CARE
 Preventing Cervical Cancer 2018 WHAT THIS WILL MEAN FOR PRIMARY CARE DR GARY FENTIMAN, CLINICAL LEADER COLPOSCOPY, N C S P TAKE-HOME LESSONS Vaccination is Primary Prevention for Cervical Cancer Women
Preventing Cervical Cancer 2018 WHAT THIS WILL MEAN FOR PRIMARY CARE DR GARY FENTIMAN, CLINICAL LEADER COLPOSCOPY, N C S P TAKE-HOME LESSONS Vaccination is Primary Prevention for Cervical Cancer Women
Manitoba Cervical Cancer Screening Program. Operations & Statistical Report and 2006
 anitoba Cervical Cancer Screening Program Operations & Statistical Report 2005 and 2006 1 MCCSP 2005-2006 Report ANITOBA CERVICAL CANCER SCREENING PROGRAM 2005 and 2006 Operations & Statistical Report
anitoba Cervical Cancer Screening Program Operations & Statistical Report 2005 and 2006 1 MCCSP 2005-2006 Report ANITOBA CERVICAL CANCER SCREENING PROGRAM 2005 and 2006 Operations & Statistical Report
/SH14236_AC CSIRO 2015 Sexual Health 2015, 12(4),
,") 10.1071/SH14236_AC CSIRO 2015 Sexual Health 2015, 12(4), 279 286 Women s views on human papillomavirus self-sampling: focus groups to assess acceptability, invitation letters and a test kit in the Australian
10.1071/SH14236_AC CSIRO 2015 Sexual Health 2015, 12(4), 279 286 Women s views on human papillomavirus self-sampling: focus groups to assess acceptability, invitation letters and a test kit in the Australian
What is HPV and why is it so important?
 Understanding HPV For many years, Pap smears have been the most effective way to tell if a woman is at risk of developing cervical cancer. The Pap smear may also identify a common viral infection called
Understanding HPV For many years, Pap smears have been the most effective way to tell if a woman is at risk of developing cervical cancer. The Pap smear may also identify a common viral infection called
Scottish Cervical Screening Programme. Colposcopy and Programme Management
 Scottish Cervical Screening Programme Colposcopy and Programme Management Addendum to NHSCSP Publication No 20 Second Edition Exceptions Applicable in NHS Scotland April 2013 (Final Version 2.8 to incorporate
Scottish Cervical Screening Programme Colposcopy and Programme Management Addendum to NHSCSP Publication No 20 Second Edition Exceptions Applicable in NHS Scotland April 2013 (Final Version 2.8 to incorporate
UK National Screening Committee HPV as primary screen for cervical cancer - an evidence review. Consultation comments pro-forma.
 UK National Screening Committee HPV as primary screen for cervical cancer - an evidence review Consultation comments pro-forma Name: Sarah May Email address: sarahmay@ibms.org Organisation (if appropriate):
UK National Screening Committee HPV as primary screen for cervical cancer - an evidence review Consultation comments pro-forma Name: Sarah May Email address: sarahmay@ibms.org Organisation (if appropriate):
Colposcopy. Attila L Major, MD, PhD
 Colposcopy Attila L Major, MD, PhD Histology Colposcopy Cytology It has been estimated that annual Pap smear testing reduces a woman s chance of dying of cervical cancer from 4 in 1000 to about 5 in 10,000
Colposcopy Attila L Major, MD, PhD Histology Colposcopy Cytology It has been estimated that annual Pap smear testing reduces a woman s chance of dying of cervical cancer from 4 in 1000 to about 5 in 10,000
Eradicating Mortality from Cervical Cancer
 Eradicating Mortality from Cervical Cancer Michelle Berlin, MD, MPH Vice Chair, Obstetrics & Gynecology Associate Director, Center for Women s Health June 2, 2009 Overview Prevention Human Papilloma Virus
Eradicating Mortality from Cervical Cancer Michelle Berlin, MD, MPH Vice Chair, Obstetrics & Gynecology Associate Director, Center for Women s Health June 2, 2009 Overview Prevention Human Papilloma Virus
Modernization of your cytology laboratory and Co-Testing Approach for Cervical Screening
 Modernization of your cytology laboratory and Co-Testing Approach for Cervical Screening 2 nd ESPC & 27 th IAP-AD annual meeting Dubai - UAE Mousa Al-Abbadi, MD, FIAC, FCAP, CPHQ, CPE Professor of Pathology
Modernization of your cytology laboratory and Co-Testing Approach for Cervical Screening 2 nd ESPC & 27 th IAP-AD annual meeting Dubai - UAE Mousa Al-Abbadi, MD, FIAC, FCAP, CPHQ, CPE Professor of Pathology
SE Coast Cervical Screening QARC Interim Guidance for laboratories on cervical sample acceptance
 SE Coast Cervical ing QARC Interim Guidance for laboratories on cervical sample acceptance List of accepted reasons/categories for sample rejection and inadequate cytology reports in SE Coast Version 6,
SE Coast Cervical ing QARC Interim Guidance for laboratories on cervical sample acceptance List of accepted reasons/categories for sample rejection and inadequate cytology reports in SE Coast Version 6,
An Update from The Study of the Prevention of Anal Cancer
 An Update from The Study of the Prevention of Anal Cancer Associate Professor Dave Templeton RPA Sexual Health, Sydney Local Health District Kirby Institute, UNSW Australia 39 th New Zealand Sexual Health
An Update from The Study of the Prevention of Anal Cancer Associate Professor Dave Templeton RPA Sexual Health, Sydney Local Health District Kirby Institute, UNSW Australia 39 th New Zealand Sexual Health
Cost and cost-effectiveness of breast cancer screening Harry J. de Koning, MD PhD
 Cost and cost-effectiveness of breast cancer screening Harry J. de Koning, MD PhD Professor of Public Health & Screening Evaluation Chair national evaluation breast cancer screening NL PI EU-TOPIA (towards
Cost and cost-effectiveness of breast cancer screening Harry J. de Koning, MD PhD Professor of Public Health & Screening Evaluation Chair national evaluation breast cancer screening NL PI EU-TOPIA (towards
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Garland SM, Hernandez-Avila M, Wheeler CM, et al. Quadrivalent
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Garland SM, Hernandez-Avila M, Wheeler CM, et al. Quadrivalent
The introduction of HPV testing to cervical screening in Scotland
 The introduction of HPV testing to cervical screening in Scotland Frequently asked questions for professionals Key messages From early 2020, cervical cytology (looking at cells under a microscope) will
The introduction of HPV testing to cervical screening in Scotland Frequently asked questions for professionals Key messages From early 2020, cervical cytology (looking at cells under a microscope) will
A RANDOMIZED CONTROLLED TRIAL OF HUMAN PAPILLOMA VIRUS (HPV) TESTING FOR CERVICAL CANCER SCREENING (HPV FOCAL Study)
 TESTING FOR CERVICAL CANCER SCREENING (HPV FOCAL Study)") A RANDOMIZED CONTROLLED TRIAL OF HUMAN PAPILLOMA VIRUS (HPV) TESTING FOR CERVICAL CANCER SCREENING () Principal Investigators Dr. Andrew Coldman BC Cancer Agency Population Oncology 8 th Floor 686 West
A RANDOMIZED CONTROLLED TRIAL OF HUMAN PAPILLOMA VIRUS (HPV) TESTING FOR CERVICAL CANCER SCREENING () Principal Investigators Dr. Andrew Coldman BC Cancer Agency Population Oncology 8 th Floor 686 West
Dysplasia: layer of the cervical CIN. Intraepithelial Neoplasia. p16 immunostaining. 1, Cervical. Higher-risk, requires CIN.
 CLINICAL PRACTICE GUIDELINE Guideline Number: DHMP_DHMC_PG1015 Guideline Subject: Routine Cervical Cancer Screening Effective Date: 9/2018 Revision Date: 9/2019 Pages: 2 of 2 Quality Management Committee
CLINICAL PRACTICE GUIDELINE Guideline Number: DHMP_DHMC_PG1015 Guideline Subject: Routine Cervical Cancer Screening Effective Date: 9/2018 Revision Date: 9/2019 Pages: 2 of 2 Quality Management Committee
The effects of immunisation on infection and Disease
 The effects of immunisation on infection and Disease Jepser Bonde and Kate Cuschieri Presented at ECC Liverpool October 2016 Jesper.Hansen.Bonde@regionh.dk Kate.Cuschieri@luht.scot.nhs.uk Scotland's Cervical
The effects of immunisation on infection and Disease Jepser Bonde and Kate Cuschieri Presented at ECC Liverpool October 2016 Jesper.Hansen.Bonde@regionh.dk Kate.Cuschieri@luht.scot.nhs.uk Scotland's Cervical