INVASIVE BREAST CANCER CURRENT ISSUES IN RADIATION
|
|
|
- Angel Arnold
- 6 years ago
- Views:
Transcription
1 INVASIVE BREAST CANCER CURRENT ISSUES IN RADIATION Bruce G. Haffty, MD Professor and Chairman Dept Radiation Oncology UMDNJ-RWJMS Cancer Institute of New Jersey
2 Mastectomy vs BCS +RT BCS Without Radiation Elderly patients Controversies and Special Circumstances Collagen Vascular Disease Risk Factors for IBTR: Margins,Age, Interactions BRCA1/2 and Breast Conserving Therapy Histological Subtypes, LCIS, Triple Negative Technical and Management Issues Sequencing Chemo-RT and Tamoxifen Fractionation Options Boost Regional Nodal RT IMRT Prone Breast
3 Randomized Trials: Mastectomy vs Breast Conserving Therapy Equivalent long term survival and DFS is evident from numerous randomized trials from the U.S.And Europe NSABP, NCI, Milan, Danish, Dutch, UK, others Outcome is similar for both node positive and node negative patients for tumor sizes up to 4-5 cm. Follow-up over 20 years in US, Milan trials
4 No. of patients Comparing CS+RT With Mastectomy For Early-Stage Breast Cancer (Prospective Randomized Trials) Institut Gustave -Roussy ( ) Milan ( ) NSABP B-06 ( ) NCI ( ) EORTC ( ) Danish ( ) Follow-up (yr) Overall survival CS+RT (%) Mastecto my (%) Local recurrence CS+RT (%) Mastecto my (%)
5 Local-Regional Relapse: MASTvs BCS Jatoi, Am J Clin Oncol, 2005

6 Is there a group where RT might not be needed?


7 Breast Conserving Surgery?with or without radiation Multiple randomized trials 3-fold reduction in local (inbreast)relapse Small but significant differences in disease free survival?small difference in survival
8 BCS with/without RT-Local Control Randomized Trials Author n Follow-up RT No RT Fisher B Years 12.4% 40.9% Liljegren Years 2.3% 18.4% Veronesi Years 5.8% 23.5% Clark Years 5.5% 25.7% Fisher B years 2.8% 16.5% Winzer years 3.2% 27.8%
9 BCS with/without RT Local Control Meta-analysis Vinh-Hung, JNCI 96:2004
10 BCS With/Without RT Survival Meta-Analysis Vinh-Hung, JNCI 96:2004)
11 EBCTCG-Meta-analysis-BCS+/- RT (EBCTCG, Lancet 366:17,2005) Local Relapse Node Negative Survival Node Negative Local Relapse Node Positive Survival Node Positive
12 EBCTCG-Meta-analysis
13 EBCTCG-Meta-analysis (EBCTCG, Lancet 366:17,2005) women in 78 Randomized Trials- RT vs No RT Comparisons involving <10% difference in LR had little impact on mortality Comparisons involving >10% difference in LR had substantial impact-5% absolute difference in mortality Over 15 years-avoidance of one breast cancer death for every 4 local relapse CHILE 2007
14 BCS without RT- Is it acceptable in Selected Cases?-Prospective data (Lim et al: Int J Rad Onc. 65:2006) Prospective Trial Patients with favorable histology 1 cm margins, No EIC, No LVI Pre-selected stopping boundry crossed 23% Local Relapse (19 patients) Conclude that even in this favorable subset, RT is indicated
15 Lumpectomy without RT in Older Patients Canadian study Local relapse 7.7% vs 0.6%, p =.001 Axillary relapse 2.5% vs 0.5%, p =.049 No difference in distant metastasis or survival Fyles AW, NEJM, 351:10, CALGB study Local relapse 4% vs 1% No difference in mastectomy rates, mets, survival Cosmesis poorer with RT Hughes K, NEJM, 351:10, 2004
16 CALGB/RTOG Update Hughes, Proc. San Antonio Meeting, 2006 Now with median F/U = 7.9 years LRR-3(1%) TamRT vs 23(7%) Tam, p<.001 Subsequent mastectomy 3 vs 9, p =.07 Breast Cancer Mortality 2% vs 2%, p =.92 All Cause Mortality 26% vs 27%, p =.84 CHILE 2007
17 BCS vs BCS+RT in Elderly Smith et al. JNCI: 98:2006 8,724 patients From the SEER- MEDICARE Database CALGB 9343 eligible Complete SEER-Medicare records Compared those who received CS alone to those who received CS+RT CHILE 2007

18 SEER-Medicare/ T1/N0/ Events by RT
19 Number NeededTreat( # pts w/rt to prevent 1 LR) Age with low comorbidity NNT Similar NNT (21) of antihypertensive medication (X-10 years) to prevent 1 coronary event Similar NNT for biphosphonates X 3 years to prevent 1 bone fracture Age 85 and older w/comorbidity NNT-125 CHILE 2007
20 Special circumstances: Contraindications to BCS+RT? BRCA1/BRCA2 carriers-no Collagen Vascular Disease-No Focally Involved margin-no Special Histology (Lobular, Medullary, rare subtypes)-no Advanced Disease-No-Neo-adjuvant Multiple Lesions-Selected cases OK? Prior Radiation-Selected cases OK?
21 Collagen Vascular Disease and Breast RT Initial anecdotal reports of poor cosmesis and complications were of concern Several case-control analysis, however failed to confirm these concerns with some minor exceptions Sceroderma subset of CVD patients, however, appear to have more problems
22 Study CVD Findings De Naeyer et al. Fleck et al. Robertson et al. Total No. No. with breast cancer Design 3 1 Case report 9 4 Case report 2 2 Case report Necrosis and progressive fibrosis Necrosis, brachial plexopathy, and severe moist desquamation Severe breast fibrosis, erythema, and pain Chen et al Case control Morris et al Retrospec tive Ross et al. 61? Case control Phan et al. 38? Case control Rakfal et al. 6 4 Case report Late complication rates higher only in scleroderma Increased radiation late effects appear in nonrheumatoid arthritis cases No differences in acute/chronic complications No difference was observed in the incidence of acute or late complications between the two groups. No severe acute or late radiation complications
23 Effect of Margins On Local Relapse Study # Pts Jobsen et al. Smitt et al. Vicini et al. Freedman et al. Neuschatz et al. Obedian and Haffty Peterson et al. F/U (Yrs) LR- Neg LR Close LR Pos % 12.2% % 16% 9% % 18-24% 30% % 14% 12% % 9% 17% % 2% 17% % 17% 11%
24 Margin Status Age and IBTR Jobsen, Int. J. Rad Onc. 57:2003
25 Local relapse in Conservatively Managed Breast Cancer-Margins, Systemic Therapy and Age Complex interactions of clinical, pathological and likely molecular variables Margins are a significant contributing factor Use of systemic therapy likely modifies the effect of margins (?Delays effect vs decreases effect) Evidence suggests that margins may be more critical in younger women
26 Margins and the conservative management of breast cancer Although wide margins are desirable, focally involved margins are not an absolute contraindication to breast conserving therapy Uncertainties in the available data necessitate the use of sound clinical judgment and common sense Review the pathology Talk to the surgeon
27 Young Age and IBTR Study Patient Age Younger Older P- # Cutoff IBTR IBTR Value Tenon % 10%.001 Curie % 15%.0001 JCRT % 10%.002 PENN % 12%.001 Beaumont % 7%.004 Yale % 12%.001
28 Young Age and Local relapse (BCT) These and other studies clearly demonstrate a strong correlation between young age and IBTR. Young age was also a significant predictor of IBTR in the EORTC boost vs no boost trial. The use of a boost was most beneficial in the younger patients.
29 BCT and BRCA1/2 Selected Studies Study #Pts. +DEL F/U IBTR Sporadic IBTR Genetic Rotterdam year 16% 30% MSKCC/ Montreal year 7% 13% MSKCC year 6.9% 22% Yale year 21% 46% Collaborative Group yrs 17% 24% Reduced by BSO

30 BCT and BRCA1/2 Ipsilateral Breast Events
31 Local (in breast) relapses in BRCA1/2 The majority of in-breast relapses in BRCA1/2 patients are new second tumors (not true relapses This observation is based on changes in histology and location of the second in breast event Examples: Medullary tumor recurring after 21 years in a different location from an infiltrating ductal primary DCIS occurring after 8 years from an infiltrating tubular primary
32 Ipsilateral and contralateral events in BRCA1 and BRCA2 Carriers None of our BRCA carriers were on adjuvant tamoxifen None of our BRCA carriers had prophylactic oophorectomy Both of these interventions have been shown in recent studies to lower the rate of second breast cancers
33 Reduction in 2nd primary breast tumors from Tamoxifen Data from Narod demonstrated a significant reduction in second breast tumors in BRCA carriers with Tamoxifen Odds ration of 0.38 for BRCA1 Odds ratio of 0.63 for BRCA2
34 Reductions in Breast Cancer Risk from Prophylactic Oophorectomy in BRCA Carriers Kauff :significant reduction in 2nd primary breast tumors by prophylactic oophorectomy 3 of 98 in prophylactic group compared to 8 of 72 in surveillance group Rebbeck demonstrated similar reductions in breast cancer risk with prophylactic oophorectomy Risk of breast cancer developing in prophylactic group was 21% compared to 42% in control group (hazard ratio of 0.47)
35 Risk of IBTR in BRCA Carriers-Effect of Prophylactic BSO and Tamoxifen Pierce et al. JCO, 24: BRCA1/2 (GC) compared to 445 sporadic controls (SC) Overall no significant difference in 15 year risk of IBTR (GC-24% vs SC-17%) GC who did not undergo BSO compared to SC: IBTR HR was 1.9, p =.03 GC who did undergo BSO risk of IBTR was similar to SC Tamoxifen was associated with a nonsignificant reduction in IBTR CHILE 2007
36 BRCA1/2 in CS+RT Late local relapses result in high local relapse rates if left unchecked Hormonal manipulation and/or oophorectomy appear to decrease this risk If CS+RT is chosen, prophylactic oophorectomy and hormonal therapy seems prudent No evidence of compromised normal tissue reactions with radiation CHILE 2007
37 Histological Subtypes: Lobular Invasive Lobular Similar overall prognosis as IDC Usually ER+ More commonly mammographically occult Despite presumed multifocality Not a contraindication to BCS Similar relapse rates as IDC, but some conflicting reports (Hussein, The Breast, 12:2002. Peiro, Br Can Res Trt, 59:2000.)
38 Lobular: Outcomes with BCS+RT MD Anderson Experience (Vo et al. Am J Surg,192:2006) 84 ILC compared to 1126 IDC No Difference in any endpoint Local Failure 3.5% ILC vs 8.3% IDC Overall failure 20% ILC vs 21% IDC Survival 81% ILC vs 85% IDC Contralateral events 11.9% ILC vs 11.3% IDC
39 Component of LCIS Local Relapse Rates Study # # IBTR IBTR P Ctrl LCIS Ctrl LCIS Yale % 7% Ns Harvard % 13% ns Michigan % 0% ns Beaumont % 14%.04 FoxChase % 15%.001
40 LCIS Alone Histological Subtypes LCIS Can be observed or treated with mastectomy Not treated with RT-However 25 Women with LCIS tx with BCS+RT Only 1 IBTR 17.6% Contralateral Breast Authors propose CS+RT as an alternative Cutuli, Eu J Can 41:2005
41 Histologic Subtypes Triple Negative-ER,PR,Her2/neu (Basal Type Cancers) Aggressive cancers-not responsive to hormonal agents or herceptin Mounting evidence that these tumors may be better treated with alternative chemotherapy agents (cis-platin, mitomycin, PARP inhibitors Common histology of patients with BRCA1 mutations Theoretically should be radiation sensitive CHILE 2007
42 Distant metastasis and local control Triple neg (n=117) vs Others (n=375) Haffty et al. J Clin Oncol, 24: CHILE 2007
43 Integrating systemic therapy and radiation in breast cancer In conservatively managed patients systemic therapy alone (without radiation) does not significantly improve local control NSABP-06 Lumpectomy Arm Results Local relapse 40% with Lumpectomy (Without RT) and CTX However, systemic therapy used in combination with RT following BCS, clearly impacts on local control
44 Systemic Tx-Effect on Local Control Selected Series of BCS+RT Study #pt F/U SysTx With Local Relapse SysTx Without SysTx NSABP CTX 2.6% 13%.001 P NSABP Tam 3.4% 10.3%.001 Buchholz CTX TAM Haffty CTX Van der Leest 758 (<40 yrs) TAM 4.4% 14.8%.004 6% 12% CTX 10% 22% <.001
45 Effect of CTX on Local Control Van der Leest, Cancer 109: 2007 CHILE 2007
46 Integrating systemic therapy and radiation in breast cancer These studies clearly indicate an impact of systemic therapy on local control in the conservative management of breast cancer However, how best to integrate systemic therapy and radiation remains controversial
47 Fig 2. Associations between delay in postoperative radiotherapy (RT) and local recurrence rates (LRRs) in studies of the sequencing of adjuvant RT and chemotherapy for breast cancer Huang, J. et al. J Clin Oncol; 21: Copyrigh t A m erican Society o f Clinical O ncolog y
48 Sequencing chemo-radiation in CS+RT These studies are in conflict with more recent evidence that shows no compromise in local control with chemo given first The randomized trial from Harvard sheds further light on this controversy, but questions remain regarding close or positive margins and the duration of chemotherapy
49 Sequencing chemo-rt in BCS 244 patients randomized to 12 weeks of CTX (CAMFP) before or after RT No overall differences in local control, distant metastasis or survival Interaction with margin status Negative marg-6% CTX first vs 13% RT first Close marg-32% CTX first vs 4% RT first Positive marg-23% CTX first vs 20% RT first Bellon et al, JCO 23:2005
50 Sequencing CTX-RT in CS+RT Data extracted from randomized trial of AC vs AC+T RT significantly delayed in AC+T arm by at least 84 days (4-21 day cycles of Taxol) No differences noted in toxicity No differences in local control Sartor, JCO 23:2005
51 Fig 2. Breast-conserving therapy with radiotherapy Sartor, C. I. et al. J Clin Oncol; 23: Copyrigh t A m erican Society o f Clinical O ncolog y
52 Sequencing CTX-RT In my view, the available evidence suggests no compromise in local control with reasonable delays in RT, provided CTX is given in an efficient, timely manner Questions remain regarding patients with close or positive margins Although concurrent chemo-rt has fallen out of favor, it might be considered for higher risk patients, preferably on prospective trials Challenge: Combining modern current agents with radiation and maintaining acceptable toxicity
53 Sequencing TAM and RT Theoretical compromise in local control if tamoxifen is given concurrently with radiation Cells put in resting state-less radiosensitive in laboratory settings Concurrent chemo and tamoxifen less effective than given sequentially No prospective or (until recently) retrospective data Trend has been to delay tamoxifen until after radiation has been administered
54 Sequencing Tamoxifen and RT J Clin Oncol: January 2005 Study # # IBTR IBTR Cosm/ Con Seq Con Seq Comp Yale % 7.5% NA Upenn % 4.8% No Diff SWOG % 14% No Diff
55 Sequencing TAM and RT Although retrospective, these 3 studies independently observed no difference in local control as a function of Tamoxifen Sequencing with RT A randomized trial, to investigate local control, cosmesis and complications has been suggested Worthy of investigation, but priority is in question
56 Post-Mastectomy RT Indicated Locally advanced regardless of nodal status (Even if CR or major response to Neoadjuvant chemo) Four or more nodes on dissection Possibly Indicated T1/T2 with 1-3 Nodes Strongly consider for +LVI, young age, close/positive margins, ECE, >20% nodes involved T3N0 Positive invasive margins Probably not Indicated T1/T2 Node Negative (or sentinel node with micrometastasis)
57 Co-Factors That Increase the LRR Risk for Patients with 1-3 +LN 10-yr LRR > 15% (1-3 +LN) LVSI younger age tumors >4 cm ECE over 2mm 3 +LN >20% +LN close margins Reference IBCSG NSABP MDACC MDACC NSABP MDACC MDACC CHILE 2007
58 Co-Factors That Increase the LRR Risk for Patients with 1-3 +LN 10-yr LRR > 15% (1-3 +LN) LVSI younger age tumors >4 cm ECE over 2mm 3 +LN >20% +LN close margins Reference IBCSG NSABP MDACC MDACC NSABP MDACC MDACC CHILE 2007

59 Fig 2. Unsupervised two-dimensional cluster analysis of 258 genes in 62 patients revealed two distinct groups of tumors; their locoregional recurrence rates were 41.4% (12 of 29) compared with 18.2% (six of 33) Cheng, S. H. et al. J Clin Oncol; 24: Copyrigh t A m erican Society o f Clinical O ncolog y
60 Genetic Profiling-PMRT Cheng SH et al. JCO 24:4594, 2006 Genomic profiling/258 and 34 gene profile 94 patients post-mastectomy (No RT) 67 without LRR 27 with LRR Predictive index <0.8 or > 0.8 Local-regional control 91% vs 40%
61 Genomic Predictors of LRR Category/ Genomic Score Node neg >0.8 < N >0.8 <0.8 >=4 + N >0.8 <0.8 Cheng SH et al. JCO 24:4594, 2006 # Patients/ # LRR 3 Year LRC Probability 24/1 96% 3/2 33% 34/1 100% 19/12 47% 4/1 75% 10/10 0%
62 Fig 3. Kaplan-Meier survival estimates for locoregional control in validation data set by (A) 258-gene and (B) 34-gene prediction tree models Cheng, S. H. et al. J Clin Oncol; 24: Copyrigh t A m erican Society o f Clinical O ncolog y
63 Technical Issues in RT Management Early Stage Breast Cancer Fractionation Schemes Boost Strategies Management of the Regional Lymphatics IMRT Prone Breast RT Partial Breast RT
64 Randomized Fractionation Trials Study Scheme # Patients Local Relapse Whelan 50 Gy/ % OCOG 42.5 Gy/ % Owen 50 Gy/ % ICR/UK 43 Gy/ % 39 Gy/ % Baillet 45 Gy/ Paris, Fr. 23 Gy/ UK START B 40 Gy/ Gy/25 UK FAST 30 Gy/ Gy/5 50 Gy/25
65 Fractionation in BCS+RT Although Gy/Day to Gy remains standard, randomized evidence supports other approaches Accelerated whole breast RT has been widely adopted in Canada and Europe Option for women with difficulty traveling or schedule conflicts Longer follow-up and additional data are awaited.
66 Randomized Boost Trials Study Scheme # Pts LR F/U (yrs) EORTC Bartelink UPDATE JCO 50 Gy/ Gy/ Lyon,Fr 50 Gy/ Romestaing + 10Gy/ Nice, Fr 50 Gy/ Teissier +10 Gy/ Budapest Polgar 50 Gy/ /
67 EORTC-Boost vs No Boost Bartelink, NEJM 345:19:2001
68 EORTC-Boost Trial Age Dependent Benefit of Boost Update 2007 Benefit to Boost in All Age groups <= % vs 13.5% % vs 8.7% % vs 4.9% >= % vs 3.8% Bartelink JCO: 25: 2007 CHILE 2007
69 Use of a Boost in CS+RT Benefit has been clearly demonstrated in randomized trials, but the absolute benefit is small in some patients I routinely boost the vast majority of patients, but acknowledge a relatively small benefit (but small risk) in older women with clear margins I also routinely boost DCIS


70 Standard Tangents w/heart Block Consider in Left-Sided, Tx w/adria/herceptin other cardiotoxic regimens CHILE 2007
71 Regional Nodal Irradiation in BCS+RT No clear consensus Potential Benefits Improved regional control Improved DFS or OS, extrapolating from post-mastectomy studies Potential Risks Added toxicity Added complexity and costs
72 Regional Nodal RT in BCS EORTC Ongoing Trials Node positive or any medial/central Randomized to Breast Only vs Breast +Upper IM, Medial Supraclav NCIC MA.20 Node positive and high risk node negative Randomized to Breast only vs Breast plus supraclav, high axilla and upper IM
73 Regional Nodal RT-My Practice Node negative by dissection (>6 Nodes), or Sentinel Node Negative Breast only Node positive by dissection Breast + SC +/- IM Node positive by Sentinel Node Breast + SC if dissected Breast + SC + Axilla if no dissection +/- IM Selected cases consider high tangents Node unknown-no dissection Breast + SC + Axilla +/- IM Selected cases consider high tangents
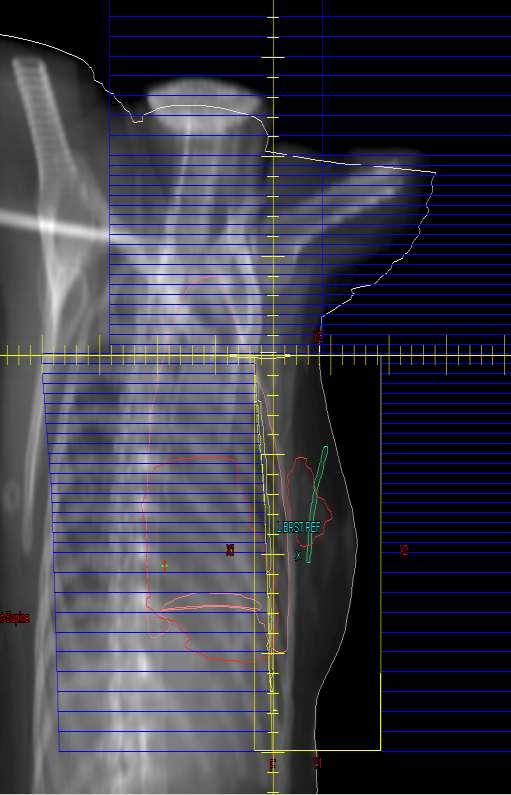
74 Mono-isocentric 3 Field Breast Technique

75 CHILE 2007

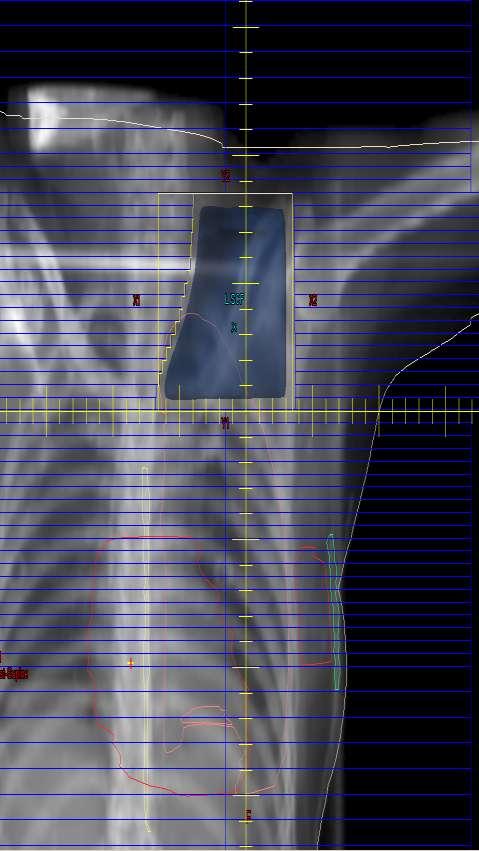
76 High Tangents Schlembach, Int J Rad Onc: 51:2001 Cranial Edge 2cm below humeral head Deep edge 2cm lung from chestwall interface Covers 80% of Level I/II Nodes
77 Axillary Treatment with CS High tangents may provide more adequate coverage For those without dissection at high risk my own bias is to use a third field treating the SC and Axilla, with CT planning to document coverage Numerous studies demonstrate adequate axillary control rates with XRT without Surgery
78 Axillary Dissection vs Radiation Louis-Sylvestre J Clin Oncol 22: 2004 Randomized Trial-658 Clinically Node Negative Randomized to AXD vs AXRT No Difference in DFS or OS Axillary Control at 15 years favored AXD (1% vs 3%, p =.04) CHILE 2007
79 Regional Nodal Irradiation Sentinel Node Postive-MDACC 196 Patients SLN+ NO Dissection 60% Received RT No Axillary Relapses Hwang et al. Cancer 110:2007 Authors suggest that RT to may be alternative to completion AXD CHILE 2007
80 Axillary radiation in lieu of surgery for SN Positive Patients Sentinel Node Positive-Current standard is to proceed with nodal dissection Available data suggests axillary radiation may be adequate in this setting Retrospective data is evolving Studies to address this are under way- EORTC-AMAROS Trial AMAROS TRIAL Sentinel Node Positive Patients Randomized to AXD vs AXRT
81 Internal Mammary Treatment Remains Controversial Study IM Survival Survival P Note Tx W/IM WO/IM Meier Surg Randomized Lacour Surg 56% 53%.40 Randomized Fowble RT 80% 81%.87 Retrospective All BCS +RT Obedian RT 72% 84%.63 Retrospective All BCS +RT Stemmer RT 78% 64%.08 RT not given NO IM group: Technical Problems
82 IMRT for Early Breast Role of IMRT in early breast cancer and the associated technology is rapidly evolving Numerous techniques have been reported Can be performed in standard time slots Improved dose homogeneity is evident Potential advantage in large breasts and other selected patients Clinical outcomes data, cost/benefit, optimal technique and patient selection await further studies

83 Dose Homogeneity with IMRT Uncompensated IMRT Vicini, Int J Rad Onc, 54: 5, 2002

84 Dose Homogeneity Open vs Wedge vs Electronic Compensator OPEN FIELD WEDGED E-COMP HOT SPOT HOT SPOT CHILE 2007
85 IMRT for Breast Is it beneficial in all settings? What is the Cost vs Benefit? What is considered IMRT? Is inverse planning required? Are standard tangents with electronic compensation/field within field IMRT? Is there a minimum number of fields required? What are the issues regarding gating/breath holding techniques? What is the threshold/criteria for an IMRT charge ($$$) code?
86 IMRT-ASTRO Plenary Session Randomized Trial: IMRT vs Standard Wedges-358 Patients IMRT improved homogeneity (p <.0001) Decrease in Moist Desquamation w/ IMRT (31% vs 48%, p=.0019) Pignot et al. ASTRO, 2006 CHILE 2007
87 Prone Breast RT Clinical Data and Techniques are evolving Check out Current ASTRO Presentations May be advantageous for large pendulous breasts receiving whole breast RT Role in Partial Breast External Beam promising (Formenti et al, Int J Rad Onc, 60: ,2004)

88 Prone Breast RT

89 Prone Breast RT Goodman, Int J Rad Onc: 60: 2004
90 Prone Breast RT-MSKCC 245 Pts, Median F/U = 4.9 years Local Relapse 6.1% Stegman IJROBP, 68: 2007 Treatment breaks-2% Grade III dermatitis 2% Grade III fibrosis 2.4% Preferred treatment for breast only at MSKCC CHILE 2007
91 Early Breast Questions for the future APBI Fractionation Subsets for withholding RT Role of regional nodal irradiation Axillary RT vs AXD Concurrent chemoradiation Risk factors and contraindications Randomized Trials UK Start/Others CALGB/Canadian/ ECOG DCIS Others EORTC/NCIC and other studies EORTC-AMAROS Novel prospective trials Pathologic profiling genetic/molecular
92 Thank You Congreso de la Sociedad Chilena de Mastologia Bruce G. Haffty, MD CHILE 2007
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
Evolution of Regional Nodal Management of Breast Cancer
 Evolution of Regional Nodal Management of Breast Cancer Bruce G. Haffty, MD Director (Interim) Rutgers Cancer Institute of New Jersey Professor and Chair Department of Radiation Oncology Rutgers, The State
Evolution of Regional Nodal Management of Breast Cancer Bruce G. Haffty, MD Director (Interim) Rutgers Cancer Institute of New Jersey Professor and Chair Department of Radiation Oncology Rutgers, The State
Neoadjuvant Treatment of. of Radiotherapy
 Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
How can we Personalize RT as part of Breast-Conserving Therapy?
 How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
PMRT for N1 breast cancer :CONS. Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center
 PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice. Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin
 1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Whole Breast Irradiation: Class vs. Hypofractionation
 Whole Breast Irradiation: Class vs. Hypofractionation Kyung Hwan Shin, MD, PhD. Dept. of Radiation Oncology, Seoul National University Hospital 2018. 4. 6. GBCC Treatment Trends of Early Breast Cancer
Whole Breast Irradiation: Class vs. Hypofractionation Kyung Hwan Shin, MD, PhD. Dept. of Radiation Oncology, Seoul National University Hospital 2018. 4. 6. GBCC Treatment Trends of Early Breast Cancer
2017 Topics. Biology of Breast Cancer. Omission of RT in older women with low-risk features
 2017 Topics Biology of Breast Cancer Early-stage HER2+ breast cancer-can we avoid RT? Prediction tools for locoregional recurrence Omission of RT in older women with low-risk features Local-Regional Recurrence
2017 Topics Biology of Breast Cancer Early-stage HER2+ breast cancer-can we avoid RT? Prediction tools for locoregional recurrence Omission of RT in older women with low-risk features Local-Regional Recurrence
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
RADIOTHERAPY IN BREAST CANCER :
 RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
RADIOTHERAPY IN BREAST CANCER : PAST, PRESENT, FUTURE Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Cancer Institute Narayana Superspecialty Hospital Breast cancer is the classic paradigm
Current Status of Accelerated Partial Breast Irradiation. Julia White MD Professor, Radiation Oncology
 Current Status of Accelerated Partial Breast Irradiation Julia White MD Professor, Radiation Oncology I have no disclosures relative to the presented material Agenda ABPI Timeline APBI by Method Clinical
Current Status of Accelerated Partial Breast Irradiation Julia White MD Professor, Radiation Oncology I have no disclosures relative to the presented material Agenda ABPI Timeline APBI by Method Clinical
03/14/2019. Postmastectomy radiotherapy; the meta-analyses, and the paradigm change to altered fractionation Mark Trombetta M.D.
 radiotherapy; the meta-analyses, and the paradigm change to altered fractionation Mark Trombetta M.D. Division of Radiation Oncology Allegheny Health Network Cancer Institute Professor of Radiation Oncology
radiotherapy; the meta-analyses, and the paradigm change to altered fractionation Mark Trombetta M.D. Division of Radiation Oncology Allegheny Health Network Cancer Institute Professor of Radiation Oncology
Disclosure. Objectives 03/19/2019. Current Issues in Management of DCIS Radiation Oncology Considerations
 Current Issues in Management of DCIS Radiation Oncology Considerations Fariba Asrari, M.D. Director. Johns Hopkins Breast Center at Green Spring Station Department of Radiation Oncology & Molecular Sciences
Current Issues in Management of DCIS Radiation Oncology Considerations Fariba Asrari, M.D. Director. Johns Hopkins Breast Center at Green Spring Station Department of Radiation Oncology & Molecular Sciences
Principles of breast radiation therapy
 ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC)
") Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Case Conference: Post-Mastectomy Radiotherapy
 Case Conference: Post-Mastectomy Radiotherapy Outline - Case Intro Guidelines Studies - Case Conclusion Summary Outline Case Intro to PMRT Guidelines Studies Case conclusion Summary Outline - Case Intro
Case Conference: Post-Mastectomy Radiotherapy Outline - Case Intro Guidelines Studies - Case Conclusion Summary Outline Case Intro to PMRT Guidelines Studies Case conclusion Summary Outline - Case Intro
Early Stage Breast Cancer
 Local-Regional Management of Early Stage Breast Cancer Meena S. Moran, MD Associate Professor, Yale University School of Medicine Disclosure I have no conflicts of interest to disclose. Learning Objectives
Local-Regional Management of Early Stage Breast Cancer Meena S. Moran, MD Associate Professor, Yale University School of Medicine Disclosure I have no conflicts of interest to disclose. Learning Objectives
Consensus Guideline on Accelerated Partial Breast Irradiation
 Consensus Guideline on Accelerated Partial Breast Irradiation Purpose: To outline the use of accelerated partial breast irradiation (APBI) for the treatment of breast cancer. Associated ASBS Guidelines
Consensus Guideline on Accelerated Partial Breast Irradiation Purpose: To outline the use of accelerated partial breast irradiation (APBI) for the treatment of breast cancer. Associated ASBS Guidelines
Evaluating the Z011 study and how local-regional therapy for early breast cancer may change
 Evaluating the Z011 study and how local-regional therapy for early breast cancer may change Karen Hoffman, M.D., M.H.Sc., M.P.H. Dept of Radiation Oncology The University of Texas MD Anderson Cancer Center
Evaluating the Z011 study and how local-regional therapy for early breast cancer may change Karen Hoffman, M.D., M.H.Sc., M.P.H. Dept of Radiation Oncology The University of Texas MD Anderson Cancer Center
Hypofractionated Radiotherapy for breast cancer: Updated evidence
 2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
2 rd Bangladesh Breast Cancer Conference, Dhaka, December 2017 Hypofractionated Radiotherapy for breast cancer: Updated evidence Tabassum Wadasadawala Associate Professor of Radiation Oncology Tata Memorial
Prophylactic Mastectomy State of the Art
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 6 th Brazilian Breast Cancer Conference Sao Paulo, Brazil 9 March 2012 Prophylactic Mastectomy State of the Art Monica Morrow
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 6 th Brazilian Breast Cancer Conference Sao Paulo, Brazil 9 March 2012 Prophylactic Mastectomy State of the Art Monica Morrow
Breast Cancer: Management of the Axilla in Greg McKinnon MD FRCSC SON Vancouver Oct 2016
 Breast Cancer: Management of the Axilla in 2016 Greg McKinnon MD FRCSC SON Vancouver Oct 2016 No Disclosures Principle #1 There is no point talking about surgical therapy in isolation. From a patient
Breast Cancer: Management of the Axilla in 2016 Greg McKinnon MD FRCSC SON Vancouver Oct 2016 No Disclosures Principle #1 There is no point talking about surgical therapy in isolation. From a patient
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Objectives Intraoperative Radiation Therapy for Early Stage Breast Cancer
 Objectives Intraoperative Radiation Therapy for Early Stage Breast Cancer Cristina Lopez-Peñalver, MD, FACS October 11, 2014 Disclosures I have no relevant commercial relationships to disclose. Discuss
Objectives Intraoperative Radiation Therapy for Early Stage Breast Cancer Cristina Lopez-Peñalver, MD, FACS October 11, 2014 Disclosures I have no relevant commercial relationships to disclose. Discuss
Bruno CUTULI Policlinico Courlancy REIMS. WORKSHOP SULL IRRADIAZIONE MAMMARIA IPOFRAZIONATA Il carcinoma duttale in situ
 Bruno CUTULI Policlinico Courlancy REIMS WORKSHOP SULL IRRADIAZIONE MAMMARIA IPOFRAZIONATA Il carcinoma duttale in situ XXI CONGRESSO AIRO GENOVA 22.11.2011 INTRODUCTION Due to wide diffusion of mammography,
Bruno CUTULI Policlinico Courlancy REIMS WORKSHOP SULL IRRADIAZIONE MAMMARIA IPOFRAZIONATA Il carcinoma duttale in situ XXI CONGRESSO AIRO GENOVA 22.11.2011 INTRODUCTION Due to wide diffusion of mammography,
Intraoperative. Radiotherapy
 Intraoperative Radiotherapy ROBERTO ORECCHIA UNIVERSITY of MILAN & EUROPEAN INSTITUTE of ONCOLOGY & CNAO FOUNDATION Breast Cancer Brescia, 30th September 2011 IORT, very selective technique to intensify
Intraoperative Radiotherapy ROBERTO ORECCHIA UNIVERSITY of MILAN & EUROPEAN INSTITUTE of ONCOLOGY & CNAO FOUNDATION Breast Cancer Brescia, 30th September 2011 IORT, very selective technique to intensify
Breast Cancer Radiotherapy: Clinical challenges in 2011 from a European Perspective. Dr DA WHEATLEY CONSULTANT ONCOLOGIST ROYAL CORNWALL HOSPITAL
 Breast Cancer Radiotherapy: Clinical challenges in 2011 from a European Perspective Dr DA WHEATLEY CONSULTANT ONCOLOGIST ROYAL CORNWALL HOSPITAL Radiotherapy in Early Breast Cancer Why do we do it? Who
Breast Cancer Radiotherapy: Clinical challenges in 2011 from a European Perspective Dr DA WHEATLEY CONSULTANT ONCOLOGIST ROYAL CORNWALL HOSPITAL Radiotherapy in Early Breast Cancer Why do we do it? Who
ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER
 ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER KHANH NGUYEN, MD, MA DEPARTMENT OF RADIATION ONCOLOGY BAYHEALTH CANCER CENTER BREAST CANCER STATISTICS Most common
ACCELERATED BREAST IRRADIATION EVOLVING PARADIGM FOR TREATMENT OF EARLY STAGE BREAST CANCER KHANH NGUYEN, MD, MA DEPARTMENT OF RADIATION ONCOLOGY BAYHEALTH CANCER CENTER BREAST CANCER STATISTICS Most common
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
Speaker s Bureau. Travel expenses. Advisory Boards. Stock. Genentech Invuity Medtronic Pacira. Faxitron. Dune TransMed7 Genomic Health.
 Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
Management of DCIS Shawna C. Willey, MD, FACS Professor of Surgery, Georgetown University Director, Medstar Regional Breast Health Program Chief, Department of Surgery Medstar Georgetown University Hospital
State of the Art in 2000 State of the Art today Gazing forward
 2010 Buschke Lecture: The Relationship between Local Recurrence and Survival in Breast Cancer Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School
2010 Buschke Lecture: The Relationship between Local Recurrence and Survival in Breast Cancer Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School
Multidisciplinary management of breast cancer
 Multidisciplinary management of breast cancer C. Polgár 1,2 1 National Institute of Oncology 2 Semmelweis University Department of Oncology Incidence of breast cancer in Hungary 2014 Female population
Multidisciplinary management of breast cancer C. Polgár 1,2 1 National Institute of Oncology 2 Semmelweis University Department of Oncology Incidence of breast cancer in Hungary 2014 Female population
ASTRO Refresher Course 2016 Breast Cancer
 ASTRO Refresher Course 2016 Breast Cancer Jennifer R. Bellon, M.D. Dana-Farber Cancer Institute Associate Professor of Radiation Oncology Harvard Medical School I have no relevant conflicts of interest
ASTRO Refresher Course 2016 Breast Cancer Jennifer R. Bellon, M.D. Dana-Farber Cancer Institute Associate Professor of Radiation Oncology Harvard Medical School I have no relevant conflicts of interest
Partial Breast Irradiation for Breast Conserving Therapy
 To Radiate or Not? Is APBI the Right Compromise Solution? Partial Breast Irradiation for Breast Conserving Therapy Julia White MD Professor, Radiation Oncology Agenda Role of radiotherapy in breast conservation
To Radiate or Not? Is APBI the Right Compromise Solution? Partial Breast Irradiation for Breast Conserving Therapy Julia White MD Professor, Radiation Oncology Agenda Role of radiotherapy in breast conservation
What are Adequate Margins of Resection for Breast-Conserving Therapy?
 What are Adequate Margins of Resection for Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School What are Adequate Margins
What are Adequate Margins of Resection for Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School What are Adequate Margins
doi: /j.ijrobp
 doi:10.1016/j.ijrobp.2009.12.047 Int. J. Radiation Oncology Biol. Phys., Vol. 79, No. 4, pp. 977 984, 2011 Copyright Ó 2011 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ see front matter
doi:10.1016/j.ijrobp.2009.12.047 Int. J. Radiation Oncology Biol. Phys., Vol. 79, No. 4, pp. 977 984, 2011 Copyright Ó 2011 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/$ see front matter
Breast cancer. (early and advanced) Radiotherapy
 Radiotherapy") Breast cancer (early and advanced) Radiotherapy Need for RT. ESTRO-HERO estimation Tumor site RT courses 2012 Increase in number 2025 Increase in rate (%) Breast 396,891 40,524 10.2 Lung 315,197 56,558
Breast cancer (early and advanced) Radiotherapy Need for RT. ESTRO-HERO estimation Tumor site RT courses 2012 Increase in number 2025 Increase in rate (%) Breast 396,891 40,524 10.2 Lung 315,197 56,558
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective
 Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective Tokyo-West Tokushukai Hospital Department of Breast Oncology Tokyo-West Tokushukai Hospital, Tokyo, Japan Kaz Sato, MD,
Recent Updates in Surgical Management of Breast Cancer Asian Patient's Perspective Tokyo-West Tokushukai Hospital Department of Breast Oncology Tokyo-West Tokushukai Hospital, Tokyo, Japan Kaz Sato, MD,
Radiation Treatment for Breast. Cancer. Melissa James Radiation Oncologist August 2015
 Radiation Treatment for Breast Cancer Melissa James Radiation Oncologist August 2015 OUTLINE External Beam Radiation treatment. (What is Radiation, doctor?) Role of radiation. (Why am I getting radiation,
Radiation Treatment for Breast Cancer Melissa James Radiation Oncologist August 2015 OUTLINE External Beam Radiation treatment. (What is Radiation, doctor?) Role of radiation. (Why am I getting radiation,
Recurrence, new primary and bilateral breast cancer. José Palacios Calvo Servicio de Anatomía Patológica
 Recurrence, new primary and bilateral breast cancer José Palacios Calvo Servicio de Anatomía Patológica Ipsilateral Breast Tumor Relapse (IBTR) IBTR can occur in approximately 5 20% of women after breast-conserving
Recurrence, new primary and bilateral breast cancer José Palacios Calvo Servicio de Anatomía Patológica Ipsilateral Breast Tumor Relapse (IBTR) IBTR can occur in approximately 5 20% of women after breast-conserving
The Management of Breast Cancer 2015 ASTRO Spring Refresher
 The Management of Breast Cancer 2015 ASTRO Spring Refresher Gary M. Freedman, M.D. Associate Professor Disclosure I have no conflicts of interest to disclose. 2 Learning Objectives Apply knowledge of randomized
The Management of Breast Cancer 2015 ASTRO Spring Refresher Gary M. Freedman, M.D. Associate Professor Disclosure I have no conflicts of interest to disclose. 2 Learning Objectives Apply knowledge of randomized
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy
 Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Post-Lumpectomy Radiation Techniques and Toxicities
 Post-Lumpectomy Radiation Techniques and Toxicities Laura Willson, MD Abbott Northwestern Hospital Dept. of Radiation Oncology February 2, 2019 Learning Objectives How radiation therapy works Standard
Post-Lumpectomy Radiation Techniques and Toxicities Laura Willson, MD Abbott Northwestern Hospital Dept. of Radiation Oncology February 2, 2019 Learning Objectives How radiation therapy works Standard
Breast Conservation Therapy
 May 18, 2018 Breast Conservation Therapy One Treatment No Longer Fits All Presenter: Paul B. Fowler, MD Radiation Oncology, MGSH/MUMH 1 Objectives: 1. Define stages of breast cancer that are candidates
May 18, 2018 Breast Conservation Therapy One Treatment No Longer Fits All Presenter: Paul B. Fowler, MD Radiation Oncology, MGSH/MUMH 1 Objectives: 1. Define stages of breast cancer that are candidates
Breast cancer: Clinical evidence. of new treatments. Aero academy Conference Innovation and Safety. Patients Come First
 Breast cancer: Clinical evidence of new treatments Aero academy Conference Innovation and Safety Patients Come First January 26 & 27, 2018 Lisbon, Portugal Disclosure & Disclaimer An honorarium is provided
Breast cancer: Clinical evidence of new treatments Aero academy Conference Innovation and Safety Patients Come First January 26 & 27, 2018 Lisbon, Portugal Disclosure & Disclaimer An honorarium is provided
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006
 Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Radiation Therapy for the Oncologist in Breast Cancer
 REVIEW ARTICLE Chonnam National University Medical School Sung-Ja Ahn, M.D. Adjuvant Tamoxifen with or without in Patients 70 Years of Age with Stage I ER-Positive Breast Cancer: Efficacy Outcomes (10
REVIEW ARTICLE Chonnam National University Medical School Sung-Ja Ahn, M.D. Adjuvant Tamoxifen with or without in Patients 70 Years of Age with Stage I ER-Positive Breast Cancer: Efficacy Outcomes (10
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Conservative Surgery and Radiation Stage I and II Breast Cancer
 Conservative Surgery and Radiation Stage I and II Breast Cancer Variant 1: Premenopausal 41-year-old woman, 1.1-cm GII IDC, upper outer quadrant (UOQ), ER/PR ( ), HER2 ( ), primary excised with lumpectomy,
Conservative Surgery and Radiation Stage I and II Breast Cancer Variant 1: Premenopausal 41-year-old woman, 1.1-cm GII IDC, upper outer quadrant (UOQ), ER/PR ( ), HER2 ( ), primary excised with lumpectomy,
SSO-ASTRO Consensus Guidance Margins for Breast-Conserving Surgery with Whole Breast Irradiation in Stage I and II Invasive Breast Cancer
 SSO-ASTRO Consensus Guidance Margins for Breast-Conserving Surgery with Whole Breast Irradiation in Stage I and II Invasive Breast Cancer Dr. Yvonne Tsang St. Paul s Hospital Introductions Breast-conserving
SSO-ASTRO Consensus Guidance Margins for Breast-Conserving Surgery with Whole Breast Irradiation in Stage I and II Invasive Breast Cancer Dr. Yvonne Tsang St. Paul s Hospital Introductions Breast-conserving
Accelerated Radiation Treatment for Early Stage Breast Cancer. update and perspective
 Accelerated Radiation Treatment for Early Stage Breast Cancer update and perspective School of Breast Oncology Atlanta, 11/2013 Douglas W. Arthur, M.D. Professor Traditional Whole Breast Irradiation WBI
Accelerated Radiation Treatment for Early Stage Breast Cancer update and perspective School of Breast Oncology Atlanta, 11/2013 Douglas W. Arthur, M.D. Professor Traditional Whole Breast Irradiation WBI
Recent Update in Surgery for the Management of Breast Cancer
 Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Genomic Profiling of Tumors and Loco-Regional Recurrence
 1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Genomic Profiling of Tumors and Loco-Regional Recurrence Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Advances in Breast Cancer
 Advances in Breast Cancer Developed in collaboration Learning Objectives Upon completion, participants should be able to: Apply genomic medicine to treatment decisions for patients with HR+/HER2- early
Advances in Breast Cancer Developed in collaboration Learning Objectives Upon completion, participants should be able to: Apply genomic medicine to treatment decisions for patients with HR+/HER2- early
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Is Breast Radiation Therapy Necessary in the Elderly? Cancer and Leukemia Group B Radiation Therapy Oncology Group Eastern Cooperative Oncology Group
 Is Breast Radiation Therapy Necessary in the Elderly? Cancer and Leukemia Group B Radiation Therapy Oncology Group Eastern Cooperative Oncology Group CALGB 9343 Submitted 1990 Opened July 15, 1994 Closed
Is Breast Radiation Therapy Necessary in the Elderly? Cancer and Leukemia Group B Radiation Therapy Oncology Group Eastern Cooperative Oncology Group CALGB 9343 Submitted 1990 Opened July 15, 1994 Closed
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Cancer. Savita Dandapani
 New Modalities for Breast Cancer Savita Dandapani Disclosures Accuray Talk at ASTRO 10/2015. Xoft provided slides for the partial breast radiation equipment. Early Stage: Deep Inspiratory Breath Hold (DIBH)
New Modalities for Breast Cancer Savita Dandapani Disclosures Accuray Talk at ASTRO 10/2015. Xoft provided slides for the partial breast radiation equipment. Early Stage: Deep Inspiratory Breath Hold (DIBH)
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease?
 Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease? Mylin A. Torres, MD Director, Glenn Family Breast Center Louis and Rand Glenn Family Chair in Breast
Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease? Mylin A. Torres, MD Director, Glenn Family Breast Center Louis and Rand Glenn Family Chair in Breast
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Spotlights on the surgery role at San Antonio
 Spotlights on the surgery role at San Antonio Riccardo Masetti, MD Professor of Surgery Director, Multidisciplinary Breast Center Catholic University Rome, Italy Roma, 21 maggio 2017 Prof. Masetti has
Spotlights on the surgery role at San Antonio Riccardo Masetti, MD Professor of Surgery Director, Multidisciplinary Breast Center Catholic University Rome, Italy Roma, 21 maggio 2017 Prof. Masetti has
UK Interdisciplinary Breast Cancer Symposium. Should lobular phenotype be considered when deciding treatment? Michael J Kerin
 UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
Ca in situ e ormonoterapia. Discussant : LORENZA MARINO
 Ca in situ e ormonoterapia Discussant : LORENZA MARINO Ca in situ e ormonoterapia Quali fattori di rischio? Radioterapia? Ormonoterapia? BCS Recurrence rates (FUP 13-20y) Cuzick, Lancet Oncol.2011; 12(1):
Ca in situ e ormonoterapia Discussant : LORENZA MARINO Ca in situ e ormonoterapia Quali fattori di rischio? Radioterapia? Ormonoterapia? BCS Recurrence rates (FUP 13-20y) Cuzick, Lancet Oncol.2011; 12(1):
2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights
 2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights Mylin A. Torres, M.D. Director, Glenn Family Breast Center Associate Professor Department of Radiation Oncology Winship Cancer Institute
2017 San Antonio Breast Cancer Symposium: Local Therapy Highlights Mylin A. Torres, M.D. Director, Glenn Family Breast Center Associate Professor Department of Radiation Oncology Winship Cancer Institute
Breast Cancer Basics. Clinical Oncology for Public Health Professionals. Ben Ho Park, MD, PhD
 This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this
ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA
 ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA THE NATURAL HISTORY OF HORMONE RECEPTOR- POSITIVE BREAST CANCER IS VERY LONG Recurrence hazard rate 0.3 0.2 0.1 0 ER+ (n=2,257)
ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA THE NATURAL HISTORY OF HORMONE RECEPTOR- POSITIVE BREAST CANCER IS VERY LONG Recurrence hazard rate 0.3 0.2 0.1 0 ER+ (n=2,257)
Surgical treatment of BRCA mutated patients. Viviana Galimberti MD European Institute of Oncology Milan, Italy
 Surgical treatment of BRCA mutated patients Viviana Galimberti MD European Institute of Oncology Milan, Italy No pharmaceutical company funding was used I declare I have no conflicts of interest as regards
Surgical treatment of BRCA mutated patients Viviana Galimberti MD European Institute of Oncology Milan, Italy No pharmaceutical company funding was used I declare I have no conflicts of interest as regards
Guidelines for the treatment of Breast cancer with radiotherapy v.1.0 September 2017
 Guidelines for the treatment of Breast cancer with radiotherapy v.1.0 September 2017 Author: Dr Virginia Wolstenholme, Consultant Clinical Oncologist, Barts Health Date agreed: September 2017 Date to be
Guidelines for the treatment of Breast cancer with radiotherapy v.1.0 September 2017 Author: Dr Virginia Wolstenholme, Consultant Clinical Oncologist, Barts Health Date agreed: September 2017 Date to be
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
ALND. Dr. MJ Vrancken
 ALND Dr. MJ Vrancken ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice opera8on; dorsal approach 2 ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice
ALND Dr. MJ Vrancken ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice opera8on; dorsal approach 2 ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice
IORT What We ve Learned So Far
 IORT What We ve Learned So Far The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation
IORT What We ve Learned So Far The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation
M D..,., M. M P.. P H., H, F. F A.. A C..S..
 Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Slide 1. Slide 2. Slide 3 History of Nurse Navigator
 Slide 1 The Nurse Navigators role in Early Stage Breast Cancer, and Development of Tailored Treatment Plan Laura Ochoa, RN, ANP-BC, Ph.D. Slide 2 Barnes Jewish Hospital at Washington University Slide 3
Slide 1 The Nurse Navigators role in Early Stage Breast Cancer, and Development of Tailored Treatment Plan Laura Ochoa, RN, ANP-BC, Ph.D. Slide 2 Barnes Jewish Hospital at Washington University Slide 3
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Protocol of Radiotherapy for Breast Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
107 年 12 月修訂 Protocol of Radiotherapy for Breast Cancer Indication of radiotherapy Indications for Post-Mastectomy Radiotherapy (1) Axillary lymph node 4 positive (2) Axillary lymph node 1-3 positive:
ESMO Breast Cancer Preceptorship Singapore November Special Issues in Treatment of Young Women with Breast Cancer
 ESMO Breast Cancer Preceptorship Singapore November 2017 Special Issues in Treatment of Young Women with Breast Cancer Prudence Francis MD Peter MacCallum Cancer Centre Melbourne, Australia Conflict of
ESMO Breast Cancer Preceptorship Singapore November 2017 Special Issues in Treatment of Young Women with Breast Cancer Prudence Francis MD Peter MacCallum Cancer Centre Melbourne, Australia Conflict of
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
What is an Adequate Lumpectomy Margin in 2018?
 What is an Adequate Lumpectomy Margin in 2018? Stuart J. Schnitt, M.D. Brigham and Women s Hospital, Dana-Farber Cancer Institute, and Harvard Medical School Boston, MA None Disclosures Topics Current
What is an Adequate Lumpectomy Margin in 2018? Stuart J. Schnitt, M.D. Brigham and Women s Hospital, Dana-Farber Cancer Institute, and Harvard Medical School Boston, MA None Disclosures Topics Current
Breast Cancer: Current Approaches to Diagnosis and Treatment
 Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer. Cheol Min Kang 2018/04/05
 Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions
 1 1 NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health
1 1 NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health
Breast cancer (screening) in older individuals: the oncologist s viewpoint for the geriatrician
 in older individuals: the oncologist s viewpoint for the geriatrician") Breast cancer (screening) in older individuals: the oncologist s viewpoint for the geriatrician Hans Wildiers Medical oncologist, Leuven, Belgium Past chairman of the EORTC elderly task force President-elect
Breast cancer (screening) in older individuals: the oncologist s viewpoint for the geriatrician Hans Wildiers Medical oncologist, Leuven, Belgium Past chairman of the EORTC elderly task force President-elect
Acute and late adverse effects of breast cancer radiation: Two hypo-fractionation protocols
 ORIGINAL ARTICLES Acute and late adverse effects of breast cancer radiation: Two hypo-fractionation protocols Mohamed Abdelhamed Aboziada 1, Samir Shehata 2 1 Department of Radiation Oncology, South Egypt
ORIGINAL ARTICLES Acute and late adverse effects of breast cancer radiation: Two hypo-fractionation protocols Mohamed Abdelhamed Aboziada 1, Samir Shehata 2 1 Department of Radiation Oncology, South Egypt
Combined chemotherapy and Radiotherapy for Patients with Breast Cancer and Extensive Nodal Involvement.
 Combined chemotherapy and Radiotherapy for Patients with Breast Cancer and Extensive Nodal Involvement. Ung O, Langlands A, Barraclough B, Boyages J. J Clin Oncology 13(2) : 435-443, Feb 1995 STUDY DESIGN
Combined chemotherapy and Radiotherapy for Patients with Breast Cancer and Extensive Nodal Involvement. Ung O, Langlands A, Barraclough B, Boyages J. J Clin Oncology 13(2) : 435-443, Feb 1995 STUDY DESIGN