Bladder Cancer. Clinical Case Conference
|
|
|
- Theodore Gregory
- 6 years ago
- Views:
Transcription
1 Bladder Cancer Clinical Case Conference
2 Clinical Case 89 yo M with gross hematuria Labs: Chem: BUN/Cr increased 22/1.27 CBC: H/H 13/36, WBCs wnl UA: >50 RBCs, otherwise wnl UCx: No growth Cystoscopy at OSH showed bladder tumor
3 Work-up 3/27/12: CT urogram 2.6x1.4 cm soft tissue mass with irregular borders at the right ureterovesical junction; moderate hydroureter and hydronephrosis (R>L); no distant mets 3/27/12: CT chest negative for mets 4/2/12: Cystoscopy with biopsy by Dr. Parsons high-grade invasive urothelial carcinoma 4/26/12: TURBT large tumor involving the bladder trigone with bilateral ureteral orifice involvement. Pathology showed high grade TCC (papillary urothelial carcinoma) with invasion of muscularis propria 4/26/12: bilateral ureteral stents placed
4 Clinical Case PAST MEDICAL HISTORY: Hypertension Cholecystitis TB, treated 35 years ago PAST SURGICAL HISTORY: Open cholecystectomy, 1998 MEDICATIONS: Tamsulosin Nifedipine Atenolol
5 Clinical Case SOCIAL HISTORY: Immigrated to U.S. from Korea in 1976 and worked in shipyards and later, as a janitor. He is married and has two adult children. Patient has never smoked. Occ beer. FAMILY HISTORY: No known cancer.


6 Clinical Case CT urogram

7 Epidemiology US: Median age at dx 70yo 75% are male Whites 2x more than blacks or hispanics
8 Epidemiology Risk factors Tobacco smoking (esp cigarette) Aromatic amines (dyes, paints, solvents, leather dust, inks, rubber, and textiles) Prior radiation therapy Prior chemotherapy (Cytoxan) Chronic trauma (long-term indwelling catheters) Schistosoma haematobium infection (bilharzia) in Africa, particularly in Egypt
9 Economics Bladder cancer is underfunded funding if resources shared equitably (Lung cancer funding is so bad it is off the chart. )
10 Muscle Invasive
11 Lymph node involvement Overall ~20% pt1 5% pt2-t3a 30% pt3b 64% pt4 50% Muscle Invasive Skinner DG, et al. High dose, short course preoperative radiation therapy and immediate single stage radical cystectomy with pelvic node dissection in the management of bladder cancer. J Urol 1982.

12 N staging N1-N2 = Regional lymph nodes = true pelvis perivesical hypogastric, obturator, external iliac, presacral M1 = above aortic bifurcation N3 = Common iliac nodes
")
13 Staging AJCC 2010 (7 th )
")
14 Staging AJCC 2010 (7 th )
15 Clinical Presentation Painless hematuria (75%) UTI Irritative/obstructive voiding symptoms
16 Workup 1) H&P, CBC, UA, Ucx +/- urine cytology UA: RBCs, no casts Urine cytology: 34% sensitive, 98% specific 2) Cystoscopy w/ biopsy 3) Upper urinary tract imaging CT urography > U/S & IV pyelography MRI if patient can t receive contrast
17 Workup 4) CT/MRI abd/pelvis before TURBT 5) Metastatic workup (muscle invasive): Chest imaging Bone scan if sxs or elevated alk-phos PET: FDG not used because conc in urine 11 C choline data is poor, difficult to use 11 C acetate, 11 C methionine under investigation

18 Histology Urothelial carcinoma Transitional cell (TCC) >90% in US/Europe Non-urothelial carcinoma SCC 5% Adenocarcinoma 1-2%
19 Natural History Non-muscle invasive (NMIBC) 75-80% of patients Most die of other causes 10-20% progress to muscle invasive Muscle invasive Leads to metastasis and death 50% survival at 5yrs regardless of tx Metastatic <10% of patients (often previously treated localized disease) Lung, bone, liver most common Median survival mon

20 Non-muscle invasive: Risk stratify
21 Non-muscle invasive: Management Risk stratify (EORTC risk calculator) TURBT + single dose of mitomycin C and/or additional intravesical chemotherapy. Intravesical Mitomycin C x1 w/in 1 hr High risk or CIS: Intravesical BCG weekly then maintenance Surveillance Flex cystoscopy and urine cytology Frequency based on risk
22 Non-muscle invasive: XRT? Multi-center randomized trial in UK 210 patients with pt1g3 NXM0 transitional cell Group 1 unifocal disease and no Tis Arm 1: TURBT + observation Arm 2: TURBT + 60Gy/30 fractions (3- or 4-field) to bladder only. Group 2 multifocal disease and/or Tis Arm 1: TURBT + BCG or MMC Arm 2: TURBT + 60Gy/30 fractions (3- or 4-field) to bladder only. Harland SJ, et al. J Urol 2007.
23 Progression-free survival 5-year PFS: 52% in control vs. 41% with adjuvant RT (NS) Recurrence-free survival 5-year RFS: 29% in control vs. 31% with adjuvant RT (NS) Non-muscle invasive: No XRT Harland SJ, et al. J Urol 2007.

24 Levels of evidence in NCCN Guidelines Category I recommendations are the least numerous in NCCN guidelines.
25 ct3 ct4a NEXT SLIDE
26 XRT vs. Surgery: SPARE trial UK SPARE Trial Randomized feasibility trial T2/T3 transitional cell carcinoma Opened 2007 CLOSED 2009 due to poor accrual (After 30 mon, only 45 patients)

27 XRT vs. Surgery 10-year retrospective review, nonrandomized 458 patients undergoing RT or cystectomy in Yorkshire, UK Radiotherapy: cystectomy = 3:1 Overall 10-year survival: 22% RT vs 24% cystectomy (NS) Munro NP, et al. IJROBP 2010.
28 Selection Criteria Surgery/Cystectomy In the US, surgery is viewed as standard of care though no evidence it is superior to RT. Surgery often preferred: Multifocal Presence of Tis (esp extensive) Hydroureter/hydronephrosis Subtotal resection Radiation/Bladder Preservation Optimal candidate: Unifocal <5 cm No hydronephrosis/hydroureter Good bladder function Visibly complete TURBT Radiation also preferable for: Older, obese, diabetic (anesthesia risk) Unable to function s/p cystectomy (elderly)
29 Radical Cystectomy Ileal conduit Bladder, pelvic lymph nodes, perivesical fat, urethra Women: anterior wall of vagina, ovaries and uterus Men: prostate and SV are also taken Like a long ureter to a stoma Ileal conduit urinary diversion
30 Cystectomy Orthotopic Neobladder By 2002, 50-90% of patients were getting neobladder Must act like a detrusor muscle Ileal >colon because it is distensible less reflux, urgency, incontinence Mucosa adapts absorption protection/coating Disadvantages: Nocturnal incontinence Can take weeks to months to mature Urethral recurrence? Relative contra-indications: Renal disease from long-standing obstruction Liver disease, IBD Prior chemo-rt Elderly
31 ct3 ct4a NEXT SLIDE
32 Neoadjuvant Chemotherapy Neoadjuvant CMV chemo for muscle-invasive bladder cancer: long-term results of BA trial Randomized phase III trial: 976 patients (20 countries, led by UK) T2-T4a Arm 1: CMV + (XRT or Cystectomy) Arm 2: No chemotherapy + (XRT or Cystectomy) 16% reduction in risk of death with chemo Median survival months with chemo JCO 2011.
33 Neoadjuvant Chemotherapy Meta-analyses (incl 2 large RCTs) show 5% OS benefit at 5 yrs with cisplatincontaining regimens for patients with muscle-invasive bladder cancer BUT neoadjuvant chemo still not standard of care.
34 ct3 ct4a NEXT SLIDE
35 Cystectomy vs. RT salvage cystectomy Retrospective 552 patients ( ) Christie Hospital in Manchester, UK 2/3 retained their bladder # of Patients Median Age OS at 5yrs Radical cystectomy yo 45.5% RT --> salvage cystectomy yo 42% Conclusion: primary RT with salvage cystectomy does not compromise survival Addla SK, et. al. J Urol 2009.
36 ChemoRT: NCIC randomized trial National Cancer Institute of Canada Clinical Trials Group Prospective randomized trial ( ) 99 patients with T2-T4b Randomized to: RT alone (40 Gy in 20 fx) or IV cisplatin (3 cycles) with concurrent RT Interim cystoscopy Definitive therapy: RT (addtnl 20 Gy in 10 fx) or cystectomy Coppin CM, et al. JCO 1996.
37 ChemoRT: NCIC randomized trial Results: Pelvic failure (5-yr): Chemo-RT (40%) vs. RT (59%) (SS) No difference in 3-yr OS Pelvic Disease- Free Survival Overall Survival NS But then 1992 study in JCO MVAC >>cisplatin for metastatic bladder
 and cisplatin. Follow up cystoscopy (4 weeks) and complete urologic evaluation: Complete response: consolidation cisplatin-rt (25.")
38 Bladder Preservation RTOG 8802 Neoadjuvant combined modality program with selective organ preservation for invasive bladder cancer: Results of RTOG 8802 Phase II trial 91 patients MCV x 2 cycles + concurrent RT (39.6 Gy/22) and cisplatin. Follow up cystoscopy (4 weeks) and complete urologic evaluation: Complete response: consolidation cisplatin-rt (25.2/14) Persistent tumor: Cystectomy pcr 80% 60% of these kept bladder Similar survival between chemoxrt and surgery Tester W, et al. JCO 1996.
39 Bladder Preservation RTOG patients T2-4aNx s/p maximal TURBT Phase III, randomized neoadjuvant MCV 2c concurrent cisplatin 2c + WP 1.8/39.6 Gy vs. same but no MCV Both restaged 4 weeks later with cystoscopy, biopsy, EUA, cytology. If CR, then 1.8/25.2 Gy boost (total dose 64.8 Gy) + cisplatin 1c. Stopped early due to MCV toxicity (14% died). Results: no significant change in CR, OS, or DMFS. Shipley et al. JCO 1998.
40 James ND, et al. NEJM ChemoRT Multicenter, phase III, randomized 360 patients with MIBC (T2-T4a, N0) RT +/- synchronous 5FU + MMC 55Gy/20 or 64Gy/32 NS
41 QOL after Bladder Preservation Long-term survivors from RTOG protocols Zietman AL, et al. J Urol 2003.
42 QOL after Bladder Preservation Urodynamics and clinical evaluation: 24 of 32 (75%) had normally functioning bladders Symptoms causing distress in the past week:
43 if possible
44 Palliative RT for Bladder Cancer Multicenter, randomized, prospective trial 500 patients recruited, 3 mon data available on Gy in 10 fractions vs. 21 Gy in 3 fractions Results: Bladder sxs improvement 71% vs. 64% (NS) No difference in toxicity Duchesne GM, IJROBP 2000.
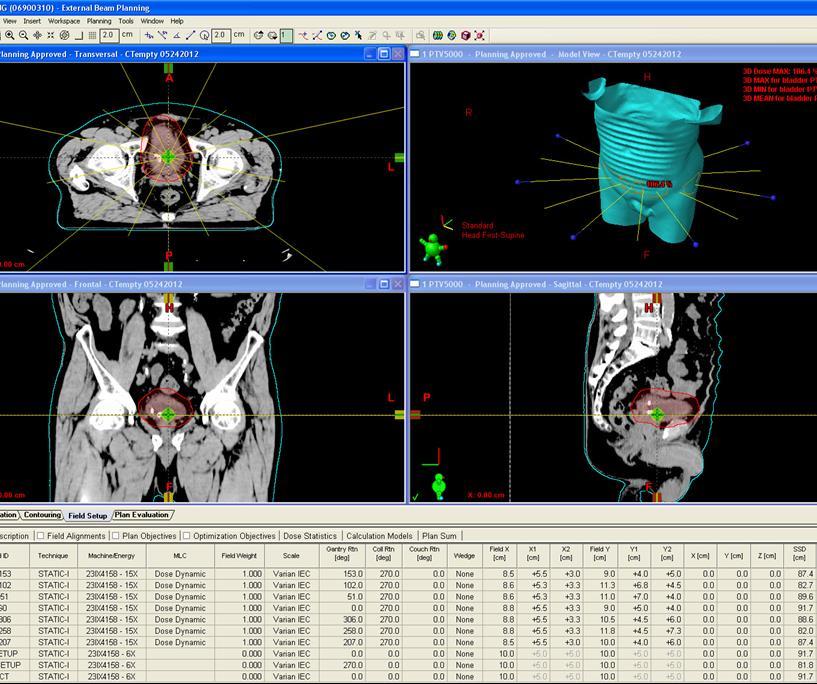
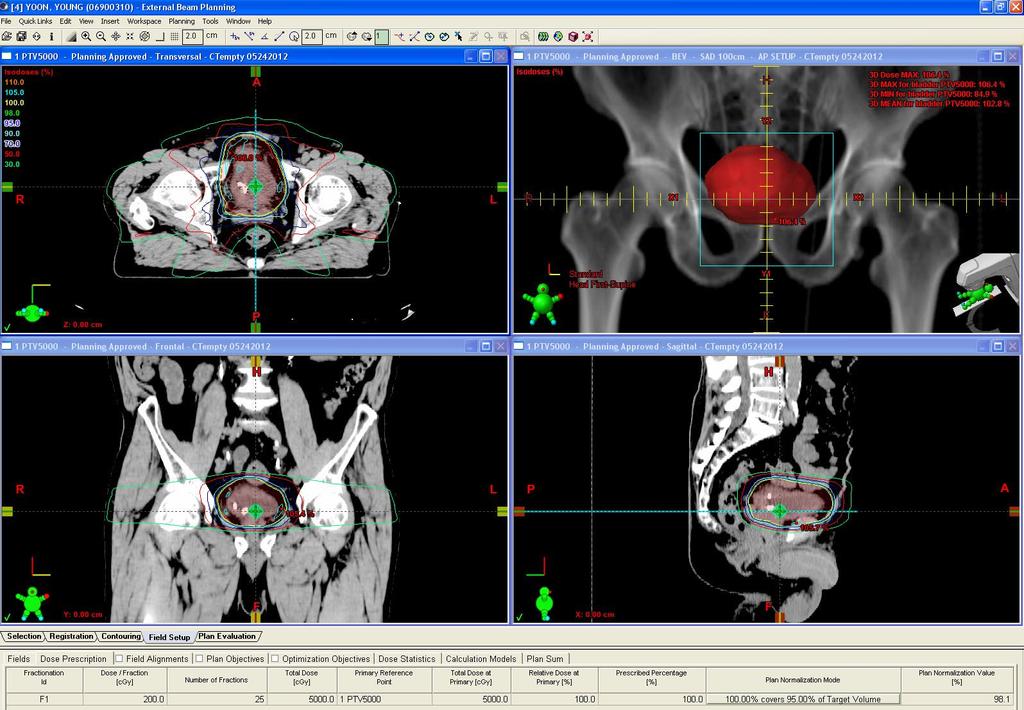
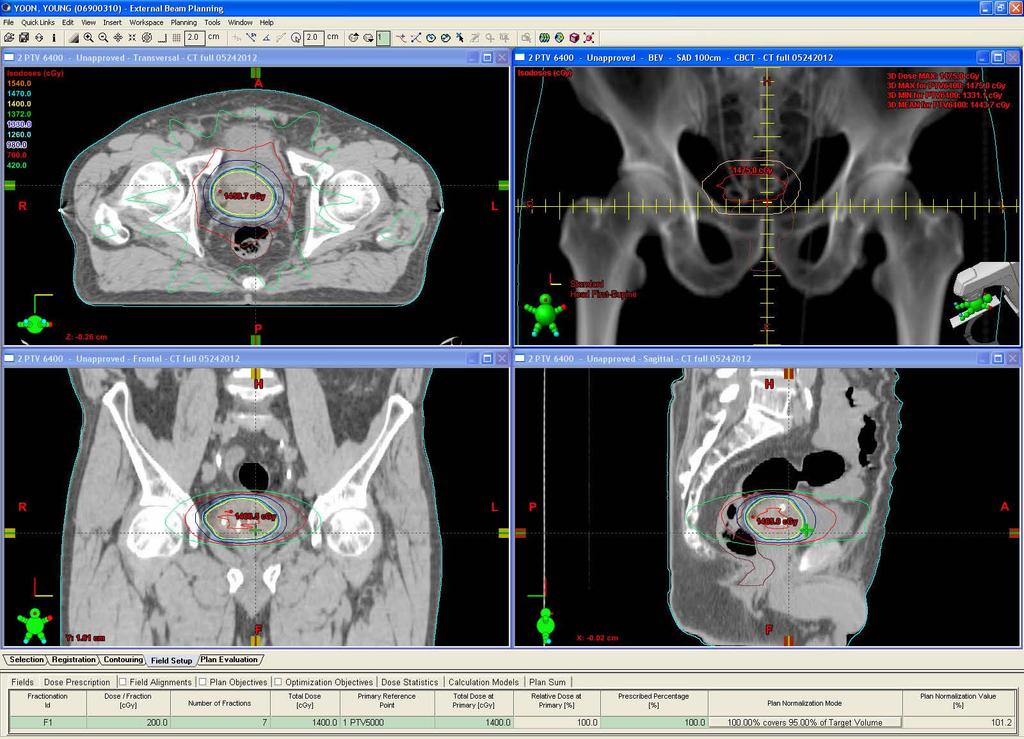
45 Radiation Technique Sim and treat with an empty bladder BOOST: Sim and treat full bladder Empty rectum Dose constraints: Bladder 65Gy to whole bladder but up to 80Gy if 1/3 of bladder spared (QUANTEC V65<50%) Rectum V50<50% Femoral Heads V50<5%
46 Clinical Case RT Plan 50Gy/25 to whole bladder Tumor boost to 64 Gy (200cGyx7) Partial bladder Daily CBCT for IGRT No nodal coverage
47
48
49

50 Clinical Case Outcome 11/26/12 He is fully functional and in good spirits! Patient s Medical Oncologist
51 Questions? Thank you!
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer
 Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Cochrane metaanalysis 5 year OS Intent to treat
 RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016
 BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
Chemotherapy and Bladder Cancer. Blayne Welk UBC Urology Grand Rounds June 4, 2008
 Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer
 Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
Case 1. Receives induction BCG weekly x 6 without significant toxicity Next step should be:
 Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Case 1 89 year old male with initial occurrence of gross hematuria Office flexible cystoscopy shows two papillary tumors with some surface necrosis Complete TURBT into muscle Florescence cysto shows two
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Urinary Bladder Cancer
 Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Dr. Tareq Salah Ahmed,MD,ESMO. Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate
 Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015 Bladder cancer
Old and New Radiation for Bladder and Upper Tract Cancers. Bridget Koontz Radiation Oncology Duke Cancer Institute
 Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
A patient with recurrent bladder cancer presents with the following history:
 MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Point-Counterpoint: Radiation & Bladder Cancer
 Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Bladder Cancer in Primary Care. Dr Penny Kehagioglou Consultant Clinical Oncologist
 Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
September 10, Dear Dr. Clark,
 September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER
 RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
AUA Guidelines for Invasive Bladder Cancer: What s New?
 AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
Panel: A Case-based Approach to the Management of Bladder Cancer
 Panel: A Case-based Approach to the Management of Bladder Cancer ~ Moderator: Robert Donohue, MD Panel: David C. Beyer, MD E. David Crawford, MD Donald L. Lamm, MD Paul D. Maroni, MD TCC Cases Robert E.
Panel: A Case-based Approach to the Management of Bladder Cancer ~ Moderator: Robert Donohue, MD Panel: David C. Beyer, MD E. David Crawford, MD Donald L. Lamm, MD Paul D. Maroni, MD TCC Cases Robert E.
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
UROTHELIAL CELL CANCER
 UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Chemo-radiotherapy in muscle invasive bladder cancer. Dr Paula Wells St Bartholomew s Hospital London
 Chemo-radiotherapy in muscle invasive bladder cancer Dr Paula Wells St Bartholomew s Hospital London Overview Evidence base for cystectomy vs bladder preservation Chemo-radiotherapy vs radiotherapy alone
Chemo-radiotherapy in muscle invasive bladder cancer Dr Paula Wells St Bartholomew s Hospital London Overview Evidence base for cystectomy vs bladder preservation Chemo-radiotherapy vs radiotherapy alone
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
NMIBC. Piotr Jarzemski. Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland
 NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
Bladder Preservation for muscle invasive disease. Nicholas
 Bladder Preservation for muscle invasive disease Nicholas James @Prof_Nick_James 1 Overview Evidence base for bladder preservation as alternative to surgery Chemoradiotherapy compared to radiotherapy alone
Bladder Preservation for muscle invasive disease Nicholas James @Prof_Nick_James 1 Overview Evidence base for bladder preservation as alternative to surgery Chemoradiotherapy compared to radiotherapy alone
Bladder Cancer Canada November 21st, Bladder Cancer 2018: A brighter light at the end of the cystoscope
 Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Organ-sparing treatment of invasive transitional cell bladder carcinoma
 Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience. Paul Gellhaus Assistant Clinical Professor
 Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience Paul Gellhaus Assistant Clinical Professor Iowa??? none Disclosures Caveats Dr. Michael O Donnell
Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience Paul Gellhaus Assistant Clinical Professor Iowa??? none Disclosures Caveats Dr. Michael O Donnell
Breast cancer Can I still keep my breast?
 Bladder Cancer Organ-Sparing Approaches SAMO Interdisciplinary Workshop on Urogenital Tumors September 15, 2012 Daniel R. Zwahlen, MD Radiation Oncology Breast cancer Can I still keep my breast? History
Bladder Cancer Organ-Sparing Approaches SAMO Interdisciplinary Workshop on Urogenital Tumors September 15, 2012 Daniel R. Zwahlen, MD Radiation Oncology Breast cancer Can I still keep my breast? History
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
The pathology of bladder cancer
 1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Hey Doc, there s blood in my urine Evaluation of hematuria. Christian S. Kuhr, MD FACS May 4, 2018
 Hey Doc, there s blood in my urine Evaluation of hematuria Christian S. Kuhr, MD FACS May 4, 2018 Objectives Understand the algorithm for hematuria evaluation Know the differential diagnosis for hematuria
Hey Doc, there s blood in my urine Evaluation of hematuria Christian S. Kuhr, MD FACS May 4, 2018 Objectives Understand the algorithm for hematuria evaluation Know the differential diagnosis for hematuria
Neoplasms of the Prostate and Bladder
 Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
Neoplasms of the Prostate and Bladder 2015-2016 FCDS Educational Webcast Series Steven Peace, BS, CTR September 19, 2015 2015 Focus o Anatomy o SSS 2000 o MPH Rules o AJCC TNM 1 CDC & Florida DOH Attribution
Early radical cystectomy in NMIBC Marko Babjuk
 Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Point/Counterpoint: Quality of Life Considerations for Patients with Muscle Invasive Bladder Cancer Pro Trimodality Therapy
 Point/Counterpoint: Quality of Life Considerations for Patients with Muscle Invasive Bladder Cancer Pro Trimodality Therapy Kimberley S. Mak, MD, MPH Assistant Professor Boston Medical Center Boston University
Point/Counterpoint: Quality of Life Considerations for Patients with Muscle Invasive Bladder Cancer Pro Trimodality Therapy Kimberley S. Mak, MD, MPH Assistant Professor Boston Medical Center Boston University
Partial Cystectomy for Invasive Bladder Cancer
 European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline
 Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
Urological Tumours 1 Kidney tumours 2 Bladder tumours
 Urological Tumours 1 Kidney tumours 2 Bladder tumours Tim Bracey SpR Histopathology Derriford Hospital Kidney tumours What are we going to talk about?! Anatomy of urinary tract! Types of kidney tumours!
Urological Tumours 1 Kidney tumours 2 Bladder tumours Tim Bracey SpR Histopathology Derriford Hospital Kidney tumours What are we going to talk about?! Anatomy of urinary tract! Types of kidney tumours!
PREVENTION & SCREENING
 A) PUBLIC HEALTH EPIDEMIOLOGY Incidence: 16 per 100,000 (males 26 per 100,000, females 7 per 100,000). Accounts for 6.1% of all new male cancer cases and 2.1% of all new female cancer cases in Canada.
A) PUBLIC HEALTH EPIDEMIOLOGY Incidence: 16 per 100,000 (males 26 per 100,000, females 7 per 100,000). Accounts for 6.1% of all new male cancer cases and 2.1% of all new female cancer cases in Canada.
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
Non Muscle Invasive Bladder Cancer. Primary and Recurrent TCC 4/10/2010. Two major consequences: Strategies: High-Risk NMI TCC
 Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015
 Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Information for Patients. Bladder Cancer. English
 Information for Patients Bladder Cancer English Table of contents What is the function of the bladder?... 3 What is bladder cancer?... 3 What causes bladder cancer?... 3 Stages of the disease... 3 Risk
Information for Patients Bladder Cancer English Table of contents What is the function of the bladder?... 3 What is bladder cancer?... 3 What causes bladder cancer?... 3 Stages of the disease... 3 Risk
EAU MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 EAU MUSLE-INVASIVE AND METASTATI LADDER ANER (Limited text update March 2016) J.A. Witjes (hair), E. ompérat, N.. owan, M. De Santis, G. Gakis, N. James, T. Lebret, A.G. van der Heijden, M.J. Ribal Guidelines
EAU MUSLE-INVASIVE AND METASTATI LADDER ANER (Limited text update March 2016) J.A. Witjes (hair), E. ompérat, N.. owan, M. De Santis, G. Gakis, N. James, T. Lebret, A.G. van der Heijden, M.J. Ribal Guidelines
Part II: Treatment. A Woman-to-Woman Talk with Dr. Armine Smith. Wednesday, March 8, Presented by
 Women & Bladder Cancer A Woman-to-Woman Talk with Dr. Armine Smith Wednesday, March 8, 2017 Part II: Treatment Presented by Dr. Smith is an Assistant Professor of Urology at Johns Hopkins University and
Women & Bladder Cancer A Woman-to-Woman Talk with Dr. Armine Smith Wednesday, March 8, 2017 Part II: Treatment Presented by Dr. Smith is an Assistant Professor of Urology at Johns Hopkins University and
Bladder Preservation Protocols in the Treatment of Muscle-Invasive Bladder Cancer
 Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
Invasive Bladder Transitional Cell Carcinoma OBJECTIVES
 Invasive Bladder Transitional Cell Carcinoma UBC Urology Grand Rounds 7 September 2005 John Morrell R5 OBJECTIVES Review role of lymphadenectomy Review role of chemotherapy Review results of bimodal bladder
Invasive Bladder Transitional Cell Carcinoma UBC Urology Grand Rounds 7 September 2005 John Morrell R5 OBJECTIVES Review role of lymphadenectomy Review role of chemotherapy Review results of bimodal bladder
Bladder Cancer: Overview, diagnosis and treatment with a focus on outpatient clinical issues
 Bladder Cancer: Overview, diagnosis and treatment with a focus on outpatient clinical issues William F. Santis, M.D. Concord Hospital Center for Urologic Care September 28, 2013 Goals: Overview of bladder
Bladder Cancer: Overview, diagnosis and treatment with a focus on outpatient clinical issues William F. Santis, M.D. Concord Hospital Center for Urologic Care September 28, 2013 Goals: Overview of bladder
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Cystectomies and bladder preservation: What you need to know
 Cystectomies and bladder preservation: What you need to know Robin Morash RN, BNSc, MHS Bladder Cancer Canada November 21, 2018 Presentation goals Review the options for treatment of muscle-invasive bladder
Cystectomies and bladder preservation: What you need to know Robin Morash RN, BNSc, MHS Bladder Cancer Canada November 21, 2018 Presentation goals Review the options for treatment of muscle-invasive bladder
Chemotherapy Treatment Algorithms for Urology Cancer
 Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Guidelines for the Management of Bladder Cancer
 Guidelines for the Management of Bladder Cancer Date Approved by Network Governance July 2012 Date for Review July 2015 Changes Between Version 3 and 4 Sections 5.2 and 8 updated Page 1 of 9 1. Scope of
Guidelines for the Management of Bladder Cancer Date Approved by Network Governance July 2012 Date for Review July 2015 Changes Between Version 3 and 4 Sections 5.2 and 8 updated Page 1 of 9 1. Scope of
Veterans and Bladder Cancer webinar. Part I: Medical Overview
 Veterans and Bladder Cancer webinar Tuesday March 1, 2016 Part I: Medical Overview Presented by Dr. Jennifer Taylor is an assistant professor of urology at the University of Pittsburgh School of Medicine.
Veterans and Bladder Cancer webinar Tuesday March 1, 2016 Part I: Medical Overview Presented by Dr. Jennifer Taylor is an assistant professor of urology at the University of Pittsburgh School of Medicine.
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Bladder Case # 1. Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia.
 DISCHARGE SUMMARY Bladder Case # 1 Date: 04/22/2010 Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia. Hospital Course: Mr.
DISCHARGE SUMMARY Bladder Case # 1 Date: 04/22/2010 Principal Diagnosis: Bladder Tumor, Suspect Transitional Cell Carcinoma. Secondary Diagnoses: 1. Hypertension. 2. Hyperlipidemia. Hospital Course: Mr.
MEDitorial March Bladder Cancer
 MEDitorial March 2010 Bladder Cancer Last month, my article addressed the issue of blood in the urine ( hematuria ). A concerning cause of hematuria is bladder cancer, a variably malignant tumor starting
MEDitorial March 2010 Bladder Cancer Last month, my article addressed the issue of blood in the urine ( hematuria ). A concerning cause of hematuria is bladder cancer, a variably malignant tumor starting
Controversies in the management of Non-muscle invasive bladder cancer
 Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
RECENT DEVELOPMENTS in Muscle Invasive Bladder Cancer
 RECENT DEVELOPMENTS in Muscle Invasive Bladder Cancer IX CIS and EURASIA ONCOLOGY and RADOLOGY CONGRESS, ONCOUROLOGY SESSION 16 June 2016 Richard E Greenberg, MD, FACS Chief Urologic Oncology, Fox Chase
RECENT DEVELOPMENTS in Muscle Invasive Bladder Cancer IX CIS and EURASIA ONCOLOGY and RADOLOGY CONGRESS, ONCOUROLOGY SESSION 16 June 2016 Richard E Greenberg, MD, FACS Chief Urologic Oncology, Fox Chase
Management options for high-risk, BCG-refractory NMIBC. Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center
 Management options for high-risk, BCG-refractory NMIBC Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center Bladder Cancer in U.S. 4 th most common cancer in men 9 th
Management options for high-risk, BCG-refractory NMIBC Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center Bladder Cancer in U.S. 4 th most common cancer in men 9 th
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Pathology Driving Decisions
 Pathology Driving Decisions Part I: Understanding Your Diagnosis and Your Treatment Options May 7, 2018 Presented by: Dr. Matthew Mossanen completed his college and medical school training at UCLA. He
Pathology Driving Decisions Part I: Understanding Your Diagnosis and Your Treatment Options May 7, 2018 Presented by: Dr. Matthew Mossanen completed his college and medical school training at UCLA. He
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy
 San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
San Antonio Breast Cancer Symposium 2010 Highlights Radiotherapy Kathleen C. Horst, M.D. Assistant Professor Department of Radiation Oncology Stanford University The Optimal SEquencing of Adjuvant Chemotherapy
Glossary of Terms Primary Urethral Cancer
 Patient Information English Glossary of Terms Primary Urethral Cancer Advanced cancer A tumour that grows into deeper layers of tissue, adjacent organs, or surrounding muscles. Anaesthesia (general, spinal,
Patient Information English Glossary of Terms Primary Urethral Cancer Advanced cancer A tumour that grows into deeper layers of tissue, adjacent organs, or surrounding muscles. Anaesthesia (general, spinal,
The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
 30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
Upper Tract Tcc. Mohan Arianayagam FRACS (Urology)
") Upper Tract Tcc Mohan Arianayagam FRACS (Urology) Epidemiology Peak incidence 75 to 79 years 2x more common in men 7% of all renal tumours 5% of all urothelial tumours Synchronous bilateral is rare ~ 1.6%
Upper Tract Tcc Mohan Arianayagam FRACS (Urology) Epidemiology Peak incidence 75 to 79 years 2x more common in men 7% of all renal tumours 5% of all urothelial tumours Synchronous bilateral is rare ~ 1.6%
Bladder Cancer Basics For the Newly Diagnosed
 Bladder Cancer Basics For the Newly Diagnosed Bladder Cancer Advocacy Network The information in this patient guide is not intended to take the place of medical care or the advice of your doctor. Please
Bladder Cancer Basics For the Newly Diagnosed Bladder Cancer Advocacy Network The information in this patient guide is not intended to take the place of medical care or the advice of your doctor. Please
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER
 UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Bladder cancer - suspected
 Background information Information resources for patients and carers Updates to this care map Bladder cancer - clinical presentation History Examination Consider differential diagnoses Clinical indications
Background information Information resources for patients and carers Updates to this care map Bladder cancer - clinical presentation History Examination Consider differential diagnoses Clinical indications
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Q&A. Collecting Cancer Data: Bladder. Collecting Cancer Data: Bladder 3/3/2011. NAACCR Webinar Series 1. Agenda
 Collecting Cancer Data: Bladder March 3, 2011 NAACCR 2010-2011 Webinar Series Agenda Coding Moment Bladder Overview Multiple Primary Histology Rules Collaborative Stage Data Collection System Diagnostic,
Collecting Cancer Data: Bladder March 3, 2011 NAACCR 2010-2011 Webinar Series Agenda Coding Moment Bladder Overview Multiple Primary Histology Rules Collaborative Stage Data Collection System Diagnostic,
EAU GUIDELINES ON NON-MUSCLE INVASIVE (TaT1, CIS) BLADDER CANCER
 BLADDER CANCER") EU GUIDELINES ON NON-MUSLE INVSIVE (TaT1, IS) LDDER NER (Limited text update March 2017) M. abjuk (hair), M. urger (Vice-hair), E. ompérat, P. Gontero,.H. Mostafid, J. Palou,.W.G. van Rhijn, M. Rouprêt,
EU GUIDELINES ON NON-MUSLE INVSIVE (TaT1, IS) LDDER NER (Limited text update March 2017) M. abjuk (hair), M. urger (Vice-hair), E. ompérat, P. Gontero,.H. Mostafid, J. Palou,.W.G. van Rhijn, M. Rouprêt,
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Bladder replacement in men and women: when and when not? Outline. Continent Diversion History
 1 Bladder replacement in men and women: when and when not? Eila C. Skinner, MD Professor of Clinical Urology Keck USC School of Medicine Outline 1) Selection criteria for orthotopic diversion: Tumor-related
1 Bladder replacement in men and women: when and when not? Eila C. Skinner, MD Professor of Clinical Urology Keck USC School of Medicine Outline 1) Selection criteria for orthotopic diversion: Tumor-related
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Care of bladder cancer patients diagnosed in Northern Ireland 2010 & 2011 (Summary)
") Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary) Bannon, F., Ranaghan, L., & Gavin, A. (2014). Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary). N. Cancer Registry,
Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary) Bannon, F., Ranaghan, L., & Gavin, A. (2014). Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary). N. Cancer Registry,
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer
 Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Should the primary be treated in patients with metastatic disease? Upper Tract Urothelial Cancer Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology
Open clinical uro-oncology trials in Canada
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES