Rectal Cancer: Classic Hits
|
|
|
- Stewart Camron Gray
- 6 years ago
- Views:
Transcription
1 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1
2 Objectives Review the Classic hits from the literature on the treatment of rectal cancer..over my lifetime and some other stuff too. Colon and Rectal Cancer Estimated ,000 new cases 49,000 deaths 40,000 Rectal Cancers 15,000 Deaths 2

3 Colon vs Rectal Cancer Different lymphatic drainage Anatomic differences Is the biology different?? Rectal Anatomy 3

4 Lymphatic Drainage Rectal lymphatics drain upward toward the IMA Case Presentation 52 year old man comes to the office with a biopsy proven adenocarcinoma 10 cm from the anus 4


5 1970 s 1970 s 5
6 Rectal Cancer 1970 s Surgery only real option Very little or no pre-operative evaluation Most likely get an APR Outcomes, even when curative were poor Survival in 40% Local recurrence very high 1970 s Radical resection Conventional approach Blunt dissection Emphasis on distal margin 5-10 cm distal margin APR most common procedure 6
7 Zollinger Atlas of Surgery s Localized disease Surgery could be curative Local recurrence up to 50% Stage I: 5-10% Stage II: 25-30% Stage III: upto 50% 7

8 Local Control A real problem Some people die of local disease without systemic disease Aggressive local control should improve quality of life and may even impact survival Why is local control a problem for rectal cancer 8

9 Why is local control a problem for rectal cancer Pelvis A Deep Hole 9

10 Why is local control a problem for rectal cancer Unlike colon cancer, local recurrence is a huge problem for rectal cancer!!!!! 10

11 1970 s Other Approaches Radiation Began a host of single institutional reports that radiation therapy may be beneficial 11

12 Gastrointestinal Tumor Study Group - GITSG Gastrointestinal Tumor Study Group - GITSG Question: Can we control cancer recurrence with: Chemotherapy Radiation Combined chemo and radiation 12

13 GITSG-1985 Postoperative Adjuvant Therapy Accrural Goal 530 patients Randomized 227 Control Chemotherapy Radiation Combined chemoradiation 13
14 Disease Free Combined 70% Control 45% Survival Combined 56% Control 36% P=.07 14
15 GITSG Accrual stopped early because it was clear that patients with postoperative chemoradiation had improved outcomes GITSG Conclusions Postoperative adjuvant therapy decreases time to recurrence. Combined chemoradiation produced the best result Significantly improved local regional control with combined Less local recurrences, XRT Less distant recurrences, chemo Toxicity, while not minimal, was acceptable 15
16 National Surgical Adjuvant Breast and Bowel Project (NSABP) patients Accrural Curative resection Dukes B,C Randomized to postoperative: Surgery alone Chemotherapy Radiation therapy NSABP Results Postoperative adjuvant therapy LR DM Suvival Control CT XRT
17 NSABP Results Postoperative adjuvant therapy LR DM Suvival Control CT XRT NSABP Results Postoperative adjuvant therapy Radiation effective for local control. No impact on survival Chemotherapy effective for survival. No impact on local control 17

18 North Central Cancer Treatment Group NCCTG 209 patients accrued, Randomized to postoperative Radiation Chemotherapy and radiation 18
19 NCCTG Results Postoperative adjuvant therapy LR DM Suvival CT/XRT XRT NCCTG Results Postoperative adjuvant therapy Combined postoperative chemoradiation therapy improved LOCAL CONTROL SURVIVAL 19
20 NIH Consensus Statement 1990 Local regional control for rectal cancer is critical Stage II and Stage III patients at risk NIH Consensus Statement 1990 Stage I No adjuvant therapy Low local recurrence Excellent survival Stage II/III Combined postoperative chemo- and radiationtherapy Improved survival (marginal) Improved local control (significant) 50% reduction, but still high 20

21 Late 1980 s Early 1990 s Era of postoperative chemoradiation therapy for Stage II/III rectal cancer Improved local control and survival!!! Late 1980 s Early 1990 s 21

22 Late 1980 s Early 1990 s Next Question Can we do it better?? Pre-operative Therapy vs Postoperative therapy 22
23 Postoperative Pros Full pathological staging, avoids overtreatment No delay in surgical treatment?? Less complications Cons Complications lead to no treatment No down staging, no increase in sphincter preservation Radiating your anastomosis, small bowel Preoperative Pros Downstaging, shrinkage of tumors Sterilize margins, improve outcomes with bulky tumors Improved effects with better oxygenated tissus Removing irradiated tissue?? Better compliance Cons Overtreatment, poor selection Delay surgical therapy Wound healing, anastomotic leaks, surgical complications 23

24 Stockholm I 1995 Multicenter, patients randomized Surgery alone Short course pre-operative radiation 25 Gy over 5 days Surgery within a week 24

25 Stockholm I Stockholm I 25
26 Stockholm I Much improved local control 16% vs 30% Increased complications Mostly wound related Increased perioperative mortality 8% vs 2% Mostly cardiovascular in patients >75 years Stockholm II Adjusted radiation fields Age < patients randomized Surgery Short course, high dose radiation followed by surgery 26
27 Stockholm II Pelvic recurrence Surgery - 25% Pre-op radiation 12% Survival, in patients with curative surgery Pre-op 46% Surgery 39% Stockholm II Pelvic recurrence Surgery - 25% Pre-op radiation 12% Survival, in patients with curative surgery Pre-op 46% Surgery 39% 27

28 Swedish Rectal Cancer Trial 1997 Improved Survival with Preoperative Radiotherapy in Resectable Rectal Cancer New England Journal
29 Local Recurrence Swedish Rectal Cancer Trial Probability of Local Recurrence All Patients Surgery alone Radiotherapy plus surgery Dukes Stage A Probability of Local Recurrence Dukes Stage B Years Years Figure 1. Rates of Local Recurrence among All Patients Undergoing Resection, According to Dukes Stage and Treatment Assignment. The bars indicate 95 percent confidence limits Dukes Stage C Local Recurrence Swedish Rectal Cancer Trial Probability of Local Recurrence Probability of Local Recurrence Dukes Stage B Dukes Stage C Local recurrence 11% vs 27% favoring 0.6 radiation over 0.6 control All Patients Surgery alone Radiotherapy plus surgery Years Years Figure 1. Rates of Local Recurrence among All Patients Undergoing Resection, According to Dukes Stage and Treatment Assignment. The bars indicate 95 percent confidence limits Dukes Stage A 29
30 Survival Swedish Rectal Cancer Trial Probability of Survival All Patients Surgery alone Radiotherapy plus surgery Dukes Stage A Probability of Survival Dukes Stage B Years Dukes Stage C Years Figure 2. Overall Survival among All Eligible Patients Undergoing Surgery, According to Dukes Stage and Treatment Assignment. The bars indicate 95 percent confidence limits. Survival Swedish Rectal Cancer Trial Probability of Survival All Patients Dukes Stage A Surgery alone 0.2 Radiotherapy plus surgery Overall survival 58% vs 48%, Favoring radiation over control Probability of Survival 1.0 Dukes Stage B Dukes Stage C Years Years Figure 2. Overall Survival among All Eligible Patients Undergoing Surgery, According to Dukes Stage and Treatment Assignment. The bars indicate 95 percent confidence limits. 30
31 Mid 1990 s Pre-operative therapy becoming more common Still controversial Rectal Cancer What are the surgeons doing?? 31
 32")
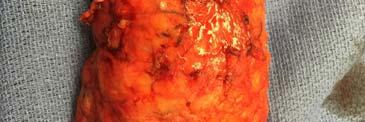
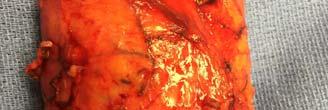
32 Total Mesorectal Excision (TME) Total Mesorectal Excision 32
33 Total Mesorectal Excision Found tumor deposits in mesorectum up to 4 cm distal to the tumor Some drainage is downward in a retrograde fashion?? Cause of suture line recurrence and local recurrence Advocated complete mesorectal excision for rectal cancers Conventional Surgery Blunt Dissection Left mesorectum behind with lymph node metastases. NOT RECURRENCE..PERSISTENCE BAD SURGERY!!! 33


34 Zollinger Atlas of Surgery Total Mesorectal Excision En bloc resection of rectum with surrounding lymphatic tissue Precise sharp dissection, keeping intact the fascia propia Complete dissection to pelvic floor, below the mesorectum Low pelvic anastomosis 34

35 Rectum is like a roll of Bounty 35

36 Rectum Mesoectum 36
37 Conventional Line of Dissection TME Line of Dissection Mesoectum 37


38 Total Mesorectal Excision Total Mesorectal Excision 38






39 39




40 TME Pelvis after specimen removed 40


41 Complete vs Incomplete TME Parfitt J R, Driman D K J Clin Pathol 2007;60: Bread loafing - TME Parfitt J R, Driman D K J Clin Pathol 2007;60:
42 Total Mesorectal Excision Reported on 50 cases with TME 2 year follow up with no recurrences Total Mesorectal Excision Increased sphincter salvage Higher leak rates Surgical technique is critical to management of rectal cancer 42
43 TME Local Recurrence Selected Series Total Mesorectal Excision Surgical technique matters!!! With good surgery, is radiation necessary?? Are results reproducible?? Yes Can it be taught/learned?? 43
44 Can it be taught? Stockholm TME Project workshops over 3-4 days each Live video Surgical training with Heald Specimen analysis Pathology training, circumferential radial margin 44
45 Stockholm TME Project Surgeons from Stockholm I and II trials Stockholm TME Project Results 45
46 Local Recurrence Stockholm I and II, TME Project I II TME XRT 9% 6% 1.5% No XRT 21% 21% 9% Stockholm TME Project Much greater sphincter salvage 50% less local recurrence TME results and radiation effects seemed additive!!! 46
47 TME vs Radiation Dutch Trial TME vs Radiation Dutch Trial Multicenter, patients randomized to: 1. Short course XRT then TME 2. TME alone 47
48 Dutch Trial Local Recurrence Local Recurrence XRT/Surgery 2.4% Surgery 8.2% Rate of Local Recurrence (%) Surgery alones (n= 875) RadiotherapyS plus surgery (n= 873) Years NO. AT RISK RadiotherapyS plus surgerys Surgery alone 873S S S S S S S S S S 37 Figure 2. Rates of Local Recurrence in the Population of 1748 Eligible Patients Who Underwent Macroscopically Complete Local Resection, According to Treatment Group. Dutch Experience Even with TME, preoperative radiation has beneficial effect on local control At 2 years no effect on survival 80% survival in both groups is excellent Greater sphincter salvage with TME 48
49 Circumferential Margin Key to cure Local recurrence of rectal adenocarcinoma due to inadequate surgical resection: Histological study of lateral tumor spread and surgical excision P. Quirke, Leeds UK Lancet, Circumferential Margin Key to cure Local recurrence of rectal adenocarcinoma due to inadequate surgical resection: Histological study of lateral tumor spread and surgical excision P. Quirke, Leeds UK Lancet,
50 Circumferential Margins 52 patients Bread loafing to examine circumferential margins 14/52 (27%) had a positive circumferential margin 12/14 developed local recurrence Margins Distal margins, while important, are rarely the problem Rectal cancer infrequently infiltrates intramurally, 2 cm seems adequate Lymphatic spread can be up to 4 cm, partial mesorectal excision need 4-5 cm margin NEGATIVE CIRCUMFERENTIAL MARGIN 50


51 Early 2000 s Early 2000 s 51
52 Circumferential Margins Norway, 2002 Circumferential Margin Population based in Norway, TME with known circumferential margin, no radiation 7% overall local recurrence 52
53 Circumferential Margin Margin > 1mm (negative) Local recurrence 5% Distant metastases 12% Margin 1 mm (positive) Local recurrence 22% Distant metastases 40% Circumferential Margin 53
54 Positive Circumferential Margin If good TME is done Bad biology If poor TME is done Bad surgeon How do we tell?? Pathologists assess gross specimen and grade the TME quality Improves quality, ensures standardization, provides feedback 54
55 Putting it all together Preoperative versus Postoperative Chemoradiotherapy for Rectal Cancer German Rectal Cancer Study Group New England Journal of Medicine, 2004 German Rectal Cancer Trial patients pre-op chemoradiation 402 patients post-op Long course, 50.4 Gy over 5 weeks TME done 55
56 German Rectal Cancer Trial Results No difference in 5 year survival Pre 76% Post 74% Both excellent and significant improvement from 1970 s Improved local recurrence for preoperative therapy Pre 6% Post 13% German Rectal Cancer Trial Results Significant downstaging Improved sphincter salvage Short course therapy, No downstaging Better compliance Pre 90% received full therapy Post only about 50% received full therapy Less toxicity OVERTREATMENT 18% in post group Stage I Need better pre-operative staging 56
57 Case Presentation 52 year old man comes to the office with a biopsy proven adenocarcinoma 10 cm from the anus Management 2016 Multidisciplinary approach Pre-operative Staging Rectal ultrasound, MRI, CT scan 57
58 Clinical Stage I Immediate surgery with a total mesorectal excision Negative circumferential margin 2 cm distal margin If partial mesorectal excision (upper rectal cancer) then 4-5 cm margin with no coning in on mesentery No other therapy Selective use of local resection Clinical Stage II/III Neoadjuvant chemoradiation Radical surgery with a total mesorectal excision Negative circumferential margin 2 cm distal margin If partial mesorectal excision (upper rectal cancer) then 4-5 cm margin with no coning in on mesentery Postoperative chemotherapy 58
 Curative")

59 Expectations Improved local control (<10%) Curative treatment is curative 80% Greater sphincter salvage

60 2013 Multi-Institutional Co-operative trials are the key to understanding cancer and evolving treatment algorithms 60
61 Questions as we move forward?? Are we OVER treating?? Are all T3 cancers the same??? Are all node positive cancers the same?? Can we identify high risk groups?? Can we eliminate (selectively) Radiation?? Surgery?? Chemotherapy?? We Keep Adding it on. 61

62 A Complete Clinical Response Now what? Diseases of the Colon and Rectum,
63 Inclusion Criteria Palpable tumors, no more than 7 cm from anal verge ct2-t4, cn0-n1, cm0 High resolution MRI or 3-D Endorectal ultrasound Chest/Abd/Pelvic CT scan Treatment 54 Gy 45 Gy via 3-field approach 9-Gy boost to the primary tumor and perirectal tissue (54 Gy total). 3 cycles bolus 5-FU (450 mg/m2), 50 mg of leucovorin for 3 consecutive days every 3 weeks After radiation, patients received 3 additional cycles of chemotherapy every 3 weeks. 63
64 Conclusions Extended Chemoradiation with 54 Gy Initial complete response 68%!! 17% failure in first 12 month 10% failure long term Salvage surgery likely 51% handled non-operatively!! 3 Year Survival 53 months follow up Overall 94% Disease Free 75% 64
65 MSKCC Non Operative Study Distal Rectal Cancer MRI Staging Randomization Arm 1 Induction (INCT) FOLFOX/CapeOx (15 16 weeks) Arm 2 Consolidation (CNCT) Chemoradiation (5.5 weeks) Interval Evaluation DRE, Endoscopy, MRI (optional) Interval Evaluation DRE, Endoscopy, MRI (optional) Chemoradiation (5.5 weeks) FOLFOX/CapeOx (15 16 weeks) Restaging DRE, Endoscopy, MRI Surgery No Clinical Response Non Operative Management Complete or Near Complete Clinical Response 65
66 To test: PROSPECT Trial Objective Standard radiation, chemotherapy, & TME Against Chemotherapy & surgery with selective use of radiation PROSPECT Study Schema Response >=20% TME FOLFOX x 6 Selective Arm Response<20% FOLFOX x 6 Restage 5FU/Cap- CMT TME FOLFOX x 2 RANDOMIZE: 1:1 Standard Arm 5FU/Cap- CMT TME FOLFOX x 8 66
67 PROSPECT Trial 411 sites approved Most have not enrolled any patients We have enrolled 8 Only 10 have more than us INOVA has enrolled 2. No one else in Virginia Wake, Duke, NC Combined 2 Combined we are second behind MSK in enrollment Future Classic Hits Non-operative care will be appropriate for select individuals More chemotherapy upfront, including systemic chemotherapy More selective use of radiotherapy 67

68 Thank you High Resolution MRI MERCURY BMJ Oct 14;333(7572):
69 High Resolution MRI MERCURY 408 consecutive patients with rectal cancer 11 hospitals, 4 countries High Resolution MRI Predicting negative CRM In patients with primary surgery or short course XRT Accuracy 91% PPV 71% NPV 94% 69
70 Accuracy DRE 70% MRI 92% Predicting Negative Margin DRE vs MRI T Parameter MRI Distance into muscularis propria T3a: < 1mm T3b: 1-5 mm T3c: 5-15 mm T3d: > 15 mm 70

71 Good Prognosis MRI Criteria Upper and Mid Rectal Cancer T1, T2 T3a,b Regardless of N component No tumor within 1 mm of MRF Lower Rectal No invasion of intersphinteric plane 71
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
A Review of Rectal Cancer. Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center
 A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Rectal Cancer Update 2008 The Last 5 cm. Consensus Building
 Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
11/09/2014. Update Management of Rectal Cancer. Outline. I have no disclosures
 Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
Update Management of Rectal Cancer June 7, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures Outline Pre-operative staging Who needs neoadjuvant
RECTAL CARCINOMA: A DISTANCE APPROACH. Stephanie Nougaret
 RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
RECTAL CARCINOMA: A DISTANCE APPROACH Stephanie Nougaret stephanienougaret@free.fr Despite the major improvements that have been made due to total mesorectal excision (TME) management of rectal cancer
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Role of MRI for Staging Rectal Cancer
 Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Role of MRI for Staging Rectal Cancer High-resolution MRI has supplanted endoscopic ultrasound for staging rectal cancer. High-resolution MR images closely match histology and can show details such as
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference
 Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal cancer management: a team sport The role of radiology and the multidisciplinary conference W. Donald Buie MD MSc FRCSC Professor of Surgery and Oncology Department of Surgery University of Calgary
Rectal Cancer Cookbook Update. A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux
 Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Neoadjuvant Therapy for Rectal Cancer is Overrated. Joon H. Lee, Research Resident University of Colorado 8/31/2009
 Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Pathohistological Assessment of the Circular Margin of Resection During Total Mesorectal Excision, Conducted on The Malignant Formations of the Rectum
 International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Cover Page The handle http://hdl.handle.net/887/22038 holds various files of this Leiden University dissertation. Author: Swellengrebel, H.A.M. Title: Challenges in the multimodality treatment of rectal
Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer
 SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
SAGES Society of American Gastrointestinal and Endoscopic Surgeons http://www.sages.org Guidelines for Laparoscopic Resection of Curable Colon and Rectal Cancer Author : SAGES Webmaster PREAMBLE The following
Current Issues and Controversies in the Management of Rectal Cancer
 Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
RECTAL CANCER: Adjuvant Therapy. Maury Rosenstein, MD Montefiore Medical Center December 2012
 RECTAL CANCER: Adjuvant Therapy Maury Rosenstein, MD Montefiore Medical Center December 2012 Overview Indications for adjuvant therapy Preoperative Postoperative New Advances Epidemiology Approximately
RECTAL CANCER: Adjuvant Therapy Maury Rosenstein, MD Montefiore Medical Center December 2012 Overview Indications for adjuvant therapy Preoperative Postoperative New Advances Epidemiology Approximately
Rectal Cancer Location: the Surgical Perspective
 Rectal Cancer Location: the Surgical Perspective September 5, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures 1 Outline Surgical Anatomy review
Rectal Cancer Location: the Surgical Perspective September 5, 2014 W. Donald Buie MD,MSc, FRCSC Associate Professor of Surgery University of Calgary I have no disclosures 1 Outline Surgical Anatomy review
CREATE Trial Proposal: Survey of current practice and potential trial participation
 CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
CREATE Trial Proposal: Survey of current practice and potential trial participation Approximately a quarter of newly diagnosed rectal cancer patients have features on pre-treatment pelvic MRI indicating
CRC Surgery Educational Slide Deck. Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto
 CRC Surgery Educational Slide Deck Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto Staging Our group has made a major contribution re N-issues We
CRC Surgery Educational Slide Deck Dr. Andy Smith Sunnybrook Surgical Oncology Research Group Department of Surgery University of Toronto Staging Our group has made a major contribution re N-issues We
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer
 Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer") Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
Chemoradiation (CRT) Safety Analysis of ACOSOG Z6041: A Phase II Trial of Neoadjuvant CRT followed by Local Excision in ut2 Rectal Cancer Emily Chan, Qian Shi, Julio Garcia-Aguilar, Peter Cataldo, Jorge
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Rectal Cancer : Curative treatment without surgery
 Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Rectal Cancer. GI Practice Guideline
 Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
UCL. Rectum Adenocarcinoma. Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans
 Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES. Devon Paula Richardson
 NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 State of the art: Radio- /chemotherapy for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 State of the art: Radio- /chemotherapy for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
Guideline for the Management of Vulval Cancer
 Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Differential lymph node retrieval in rectal cancer: associated factors and effect on survival
 Original Article Differential lymph node retrieval in rectal cancer: associated factors and effect on survival Cedrek McFadden 1, Brian McKinley 1, Brian Greenwell 2, Kaylee Knuckolls 1, Patrick Culumovic
Original Article Differential lymph node retrieval in rectal cancer: associated factors and effect on survival Cedrek McFadden 1, Brian McKinley 1, Brian Greenwell 2, Kaylee Knuckolls 1, Patrick Culumovic
Operative Technique: Karen Horvath, MD, FACS. SCOAP Retreat June 17, 2011
 Operative Technique: Total Mesorectal Excision Karen Horvath, MD, FACS University it of Washington, Seattle SCOAP Retreat June 17, 2011 No Disclosures Purpose What is Total Mesorectal Excision (TME)? How
Operative Technique: Total Mesorectal Excision Karen Horvath, MD, FACS University it of Washington, Seattle SCOAP Retreat June 17, 2011 No Disclosures Purpose What is Total Mesorectal Excision (TME)? How
State of the art: Standard(s) of radio/chemotherapy for rectal cancer
 of radio/chemotherapy for rectal cancer") State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Terminology: anal canal cancer. Terminology: Anal margin cancer. Treatment Epidermoid
 Terminology: anal canal cancer Epidermoid Below dentate line squamous CC At and above dentate line «basaloid», «cloacogenic», or «transi6onal» = non kera6nizing types of squamous cell carcinoma same =t
Terminology: anal canal cancer Epidermoid Below dentate line squamous CC At and above dentate line «basaloid», «cloacogenic», or «transi6onal» = non kera6nizing types of squamous cell carcinoma same =t
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER
 ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
BREAST CANCER SURGERY. Dr. John H. Donohue
 Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy
 TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy Nam Kyu Kim M.D., Ph.D., FACS, FRCS, FASCRS Professor Department of Surgery Yonsei University College of Medicine Seoul,
TME and autonomic nerve preservation techniques: based on Video and Cadaveric anatomy Nam Kyu Kim M.D., Ph.D., FACS, FRCS, FASCRS Professor Department of Surgery Yonsei University College of Medicine Seoul,
CT PET SCANNING for GIT Malignancies A clinician s perspective
 CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
CT PET SCANNING for GIT Malignancies A clinician s perspective Damon Bizos Head, Surgical Gastroenterology Charlotte Maxeke Johannesburg Academic Hospital Case presentation 54 year old with recent onset
PROCARE FINAL FEEDBACK
 1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Neoadjuvant treatment Evolution and Current Status
 Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
Staging of rectal cancer on MRI: What the surgeons want to know.
 Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
Staging of rectal cancer on MRI: What the surgeons want to know. Poster No.: C-1108 Congress: ECR 2014 Type: Educational Exhibit Authors: G. Ayub, R. Chittal, A. Lowe, A. S. Punekar ; Leeds/, 1 2 1 2 2
PROCARE FINAL FEEDBACK Definitions
 1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
Local Excision of Rectal Cancer Techniques and Outcomes
 Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
Local Excision of Rectal Cancer Techniques and Outcomes Manoj J. Raval, MD, MSc, FRCSC Clinical Assistant Professor, UBC Rectal Cancer Update 2008 October 25, 2008 Overview Techniques & Description Patient
PREOPERATIVE RADIOTHERAPY IN RECTAL CANCER
 Lower Gastrointestinal Research Group Department of Molecular Medicine and Surgery Karolinska Institutet, Stockholm, Sweden PREOPERATIVE RADIOTHERAPY IN RECTAL CANCER ASPECTS OF DIFFERENT REGIMENS David
Lower Gastrointestinal Research Group Department of Molecular Medicine and Surgery Karolinska Institutet, Stockholm, Sweden PREOPERATIVE RADIOTHERAPY IN RECTAL CANCER ASPECTS OF DIFFERENT REGIMENS David
Case Scenario 1. The patient has now completed his neoadjuvant chemoradiation and has been cleared for surgery.
 Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Case Scenario 1 July 10, 2010 A 67-year-old male with squamous cell carcinoma of the mid thoracic esophagus presents for surgical resection. The patient has completed preoperative chemoradiation. This
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Meta analysis in Rectal Cancer
 Meta analysis in Rectal Cancer Dr. Monica Irukulla Professor and Head Department of Radiation Oncology Nizam s Institute of Medical Sciences hyderabad Areas of meta analysis in rectal cancers Epidemiology
Meta analysis in Rectal Cancer Dr. Monica Irukulla Professor and Head Department of Radiation Oncology Nizam s Institute of Medical Sciences hyderabad Areas of meta analysis in rectal cancers Epidemiology
Rectal Cancer. Rectal Cancer: The CCF perspective 16/11/2017. Meagan Costedio, MD, FACS, FASCRS. 38,220 new cases estimated in
 Rectal Cancer: The CCF perspective Meagan Costedio, MD, FACS, FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division of Colorectal Surgery Rectal
Rectal Cancer: The CCF perspective Meagan Costedio, MD, FACS, FASCRS Medical Director Colorectal Surgery University Hospitals Ahuja Medical Center Associate Professor - Division of Colorectal Surgery Rectal
RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY
 AFTER LONG COURSE CHEMORADIOTHERAPY") COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
COLORECTAL CLINICAL SUBGROUP RECTAL CANCER APPARENT COMPLETE RESPONSE (acr) AFTER LONG COURSE CHEMORADIOTHERAPY Finalised by: Dr Simon Gollins Mr Andrew Renehan Dr Mark Saunders Mr Nigel Scott Dr Shabbir
Disclosures. Colorectal Cancer Update GAFP November Risk Assessment. Colon and Rectal Cancer The Challenge. Issues in Colon and Rectal Cancer
 Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
MRI of Rectal Cancer
 MRI of Rectal Cancer Arnd-Oliver Schäfer Mathias Langer MRI of Rectal Cancer Clinical Atlas Prof. Dr. Arnd-Oliver Schäfer Department of Diagnostic Radiology Freiburg University Hospital Hugstetter Straße
MRI of Rectal Cancer Arnd-Oliver Schäfer Mathias Langer MRI of Rectal Cancer Clinical Atlas Prof. Dr. Arnd-Oliver Schäfer Department of Diagnostic Radiology Freiburg University Hospital Hugstetter Straße
American College of Surgeons Clinical Research Program Surgical Investigators Webinar. November 17, Moderator: Y. Nancy You, M.D.
 American College of Surgeons Clinical Research Program Kelly K. Hunt, M.D. Program Director American College of Surgeons Clinical Research Program Surgical Investigators Webinar November 17, 2017 Moderator:
American College of Surgeons Clinical Research Program Kelly K. Hunt, M.D. Program Director American College of Surgeons Clinical Research Program Surgical Investigators Webinar November 17, 2017 Moderator:
Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study
 Original Article Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study Elmer E. van Eeghen 1, Frank den Boer 2, Sandra D. Bakker 1,
Original Article Outcome of rectal cancer after radiotherapy with a long or short waiting period before surgery, a descriptive clinical study Elmer E. van Eeghen 1, Frank den Boer 2, Sandra D. Bakker 1,
Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological Response
 Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Innovations in Rectal Cancer Surgery
 Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Disclosures. Personalized Approaches to Gastrointestinal Cancers. Objectives. What is personalized cancer care. Go through some genomic studies
 Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Personalized Approaches to Gastrointestinal Cancers Emily Groves, MD Colorectal Surgery Assistant Professor, Division of Surgical Oncology Disclosures None Objectives What is personalized medicine and
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Staging of cancer patients is an important tool for the selection
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:997 1003 Improvement of Staging by Combining Tumor and Treatment Parameters: The Value for Prognostication in Rectal Cancer MARLEEN J. E. M. GOSENS,* J.
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:997 1003 Improvement of Staging by Combining Tumor and Treatment Parameters: The Value for Prognostication in Rectal Cancer MARLEEN J. E. M. GOSENS,* J.
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Controversies in management of squamous esophageal cancer
 2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
2015.06.12 12.47.48 Page 4(1) IS-1 Controversies in management of squamous esophageal cancer C S Pramesh Thoracic Surgery, Department of Surgical Oncology, Tata Memorial Centre, India In Asia, squamous
Preoperative or Postoperative Therapy for the Management of Patients with Stage II or III Rectal Cancer
 Evidence-Based Series 2-4 Version 2 A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Preoperative or Postoperative Therapy for the Management of Patients with
Evidence-Based Series 2-4 Version 2 A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Preoperative or Postoperative Therapy for the Management of Patients with
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Aspects on local recurrence of rectal
 FROM THE DepaRTMEnt of Clinical science intervention and TECHnology, division of surgery and department of oncology-pathology Karolinska Institutet, Stockholm, Sweden Aspects on local recurrence of rectal
FROM THE DepaRTMEnt of Clinical science intervention and TECHnology, division of surgery and department of oncology-pathology Karolinska Institutet, Stockholm, Sweden Aspects on local recurrence of rectal
Background: Patients and methods: Results: Conclusions:
 Chapter 7 7 Results of European pooled analysis of IORT containing multimodality treatment for locally advanced rectal cancer: adjuvant chemotherapy prevents local recurrence rather than distant metastase
Chapter 7 7 Results of European pooled analysis of IORT containing multimodality treatment for locally advanced rectal cancer: adjuvant chemotherapy prevents local recurrence rather than distant metastase
Optimization of Surgical and Pathological Quality Performance in Radical Surgery for Colon and Rectal Cancer: Margins and Lymph Nodes
 Evidence-Based Series 17-4 Version 2 A Quality Initiative of the Program in Evidence-based Care (PEBC), Cancer Care Ontario (CCO) Optimization of Surgical and Pathological Quality Performance in Radical
Evidence-Based Series 17-4 Version 2 A Quality Initiative of the Program in Evidence-based Care (PEBC), Cancer Care Ontario (CCO) Optimization of Surgical and Pathological Quality Performance in Radical
Management of early rectal cancer: Any role for adjuvant chemotherapy
 Management of early rectal cancer: Any role for adjuvant chemotherapy Andrés Cervantes Professor of Medicine CURRENTS CONCEPTS IN RECTAL CANCER DIAGNOSIS AND THERAPY TME surgery Optimal staging by MRI
Management of early rectal cancer: Any role for adjuvant chemotherapy Andrés Cervantes Professor of Medicine CURRENTS CONCEPTS IN RECTAL CANCER DIAGNOSIS AND THERAPY TME surgery Optimal staging by MRI
Colorectal Surgery. Patient Care. Goals and Objectives
 Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
Colorectal Surgery Patient Care 1) Interpret the results of clinical evaluations (history, physical examination) performed on patients with a) Hemorrhoids b) Perianal abscess/fistula c) Anal fissure d)
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of preoperative high dose rate brachytherapy for rectal cancer Rectal cancer is a
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of preoperative high dose rate brachytherapy for rectal cancer Rectal cancer is a
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Histologic response after neoadjuvant chemoradiotherapy in locally advanced rectal adenocarcinoma: experience from Sudan.
 Histologic response after neoadjuvant chemoradiotherapy in locally advanced rectal adenocarcinoma: experience from Sudan. Ahmed Abd Elrahman Abdalla 1, Awad Ali M. Alawad 2, Hussein Abdalla M. Ali 3 1.
Histologic response after neoadjuvant chemoradiotherapy in locally advanced rectal adenocarcinoma: experience from Sudan. Ahmed Abd Elrahman Abdalla 1, Awad Ali M. Alawad 2, Hussein Abdalla M. Ali 3 1.