Dr. Tareq Salah Ahmed,MD,ESMO. Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate
|
|
|
- Eunice Gibbs
- 6 years ago
- Views:
Transcription

1




2 Dr. Tareq Salah Ahmed,MD,ESMO Lecturer of clinical oncology, Assiut faculty of medicine ESMO accreditation certificate 1 st Assiut Urology department conference,marsa Alam 3 rd February 2015
3 Bladder cancer Epidemiology
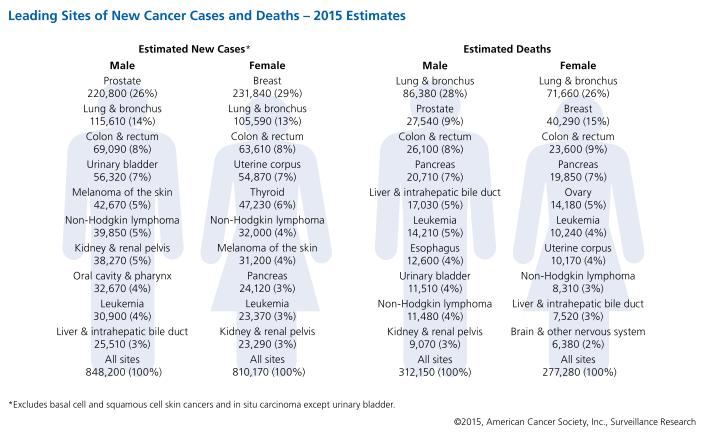


4 4th 8th
5


6 Incidence rates in Females Incidence rates in males
7
8
9 Gharbia Population based registry, report
10 Proportion (%) of the most common cancers in Males: Population-based data, Egypt Bladder Liver Non hodgkin Lung Leukemia Colorectum Prostate Skin (non melanoma) Brain & CNC Connective & soft tissue
11 Proportion (%) of the most common cancers in Females: Population-based data, Egypt Breast Non hodgkin Ovary Leukemia Colorectum Bladder Liver Brain & CNC Lung Connective & soft tissue
12 Proportion (%) of the most common cancers in both sexes Population-based data: Egypt Breast 17.6 NHL Bladder Liver Lung Leukemias Colorectum Brain & CNC Skin (non melanoma) Connective & soft tissue

13 The National Cancer Institute Cairo University
14 Most Common Sites in Males Bladder Liver Lymphoma Leukemia Lung Colorectal Soft tissue Skin Pancreas Larynx Percent of cases


15 SCC era TCC era

16

17

18 PERIOD REL FREQ AGE M:F BILHARZIAL OVA Squamous Cell Ca TRANSITIONAL CELL CA LATE STAGE III -IV RADICAL CYSTECTOCTOMY % % 58% 31% 86% 80% % % 27% 66% 40% 36%
19 Relative Frequency of Bladder Cancer, NCI * * 30 * Percent * * * * * * * * * * * * 10 * * Year
20 Prevalence Schistosomiasis Control in Egypt % * * Percent 30 * 20 * * * 25 * * * * 20 * * 10 * * 15 * 10 0 * * S.haematobium S.mansoni Year
21 TNM STAGING OF UROTHELIAL CARCINOMA OF URINARY BLADDER
22

23

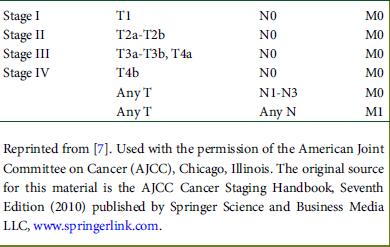
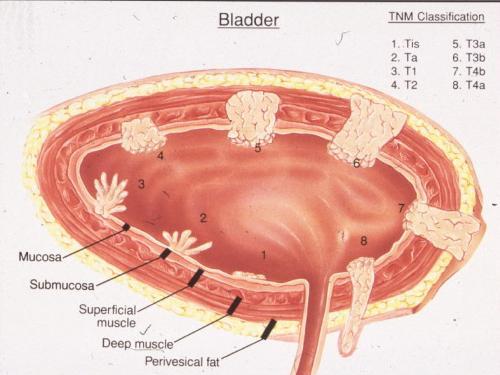
24 TNM Staging of urothelial carcinoma of bladder







25 BEFORE PLANNING THINK IN.. Patient Disease Treatment
26 Disease

27


28
29
30 overall survival rates : 30 % - 45 %
31



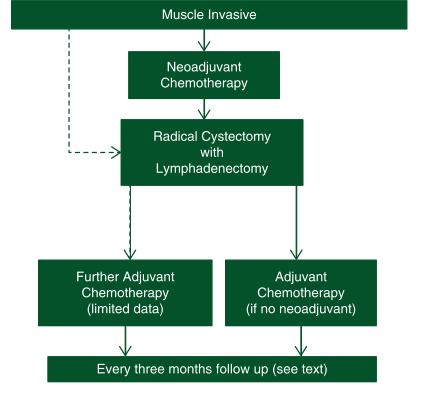
32 Muscle-invasive TCC bladder Cystectomy and reconstruction Bladder conservation Goals: Cure patient and optimize survival Prevention of pelvic failure and distant metastasis functional urinary reservoir and high QOL

, dose-fractionation")
33 Know your patients, the disease & your capabilities Patient related factors Symptoms, age, co-morbidity, erectile function, life expectancy, expectations Tumour related factors Stage, biopsy profile.. Treatment related factors XRT methods (XRT, BT, CFRT, IMRT), dose-fractionation Resource factors: expertise, infra-structure, equipment

34
35
36 What are the most important questions? 1- Overall survival. 2- Time to local recurrence. 3- Time to metastasis.( Distant failure).

37
38
39 Five-year survival after Radical Cystectomy Zaghloul. Cancer Gen Cytogen 2008; 80:
40 5-year survival of radical cystectomy CIS T1 T2 T3 T4
41 Five-year survival after Radical Cystectomy Zaghloul. Cancer Gen Cytogen 2008; 80:
42
43 5-year actuarial local recurrence rates in different radical cystectomy series Greven 92 Zaghloul 92 Visser 05 No % No % No % P0,is P P2a Hassan 06 No % P2b P P All NM
44 When is the Peak incidence of local recurrence to develop?
45 Local Recurrence is not rare in locally advanced Stages (Visser et al, 2005)
46
47
48 Distant Metastasis in different series Pollack et al,95 Zaghloul, 96 Madersbacher,03 No % No % No % Pa,1 NM P2a NM P2b NM P3 NM P4 NM N- NM NM N+ NM NM All
49 Distant Metastasis From Bladder Cancer The rate of distant metastasis in TCC ranged from from 12-35% (Miller, 1977 & Werf-Messing, 1982). In a retrospective study Zaghloul (1996) reported upon distant metastasis in 357 patients treated either with cystectomy, preoperative or postoperative radiotherapy (i.e. No chemotherapy received) the 5-year cumulative incidence of distant metastasis was 23±2%.
50 Results of Radical Cystectomy 5-year disease- free survival rates of radical cystectomy ranged from 25-48% depending upon the stage, grade & nodal status. Local recurrence represented 50-60% of the causes of failure after radical cystectomy in advanced stages. Most of the local recurrences were clinically detected within the first year after cystectomy. This suggests that it originate from a large residual tumour cell burden. Most of the local recurrences were inside the true pelvis that can be encompassed within the field of radiation.
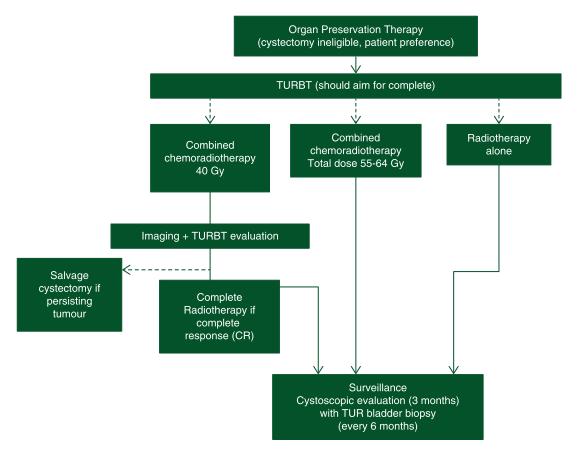
51 Bladder Preservation Protocols





52 Organ Preservation is not exclusive for UB carcinoma Anal carcinoma. Breast carcinoma. Esophageal carcinoma. Laryngeal carcinoma. Limb sarcomas. Prostate carcinoma.

53 WHY? Preserve Bladder function. Preserve sexual function. Maintain quality of life and body image. Avoid major surgery. Many patients are elderly. Co-morbidities that make patient inoperable.

54
55 Radical cystectomy (RC) is associated with considerable morbidity. Aside from the perioperative period, RC with urinary diversion poses great potential for long-term complications and morbidity. Bladder preservation therapies for muscle-invasive bladder cancer (MIBC) have been developed to address the needs of two cohorts : Patients with severe medical co-morbidities for whom a radical surgery is too high risk. Patients with limited disease who wish to avoid radical surgery. The goal of achieving complete response to treatment while maintaining bladder form and function has led to the development of multimodal approaches to this disease.
56 In medically operable patients ( fit for surgery), there is abundant evidence to support trimodal therapy as an acceptable treatment option for highly selected patients with MIBC with favourable pathological parameters. While outcomes are worse for medically inoperable patients ( unfit for surgery), bladder preservation approaches still offer curative potential.
57
. Complete TURBT.")

58 Small tumor size (<2 cm). Early tumor stage (T2,T3 disease). Complete TURBT. No ureteral obstruction (Hydronephrosis). No evidence of pelvic lymph node metastases. Absence of carcinoma in situ (Tis).

59 Radiotherapy Chemotherapy



60 University of Paris/Harvard University University of Erlangen
 +/- adjuvant chemo Non-CR Radical Cystectomy +/-")
61 Maximal TURBT Cover systemic disease XRT + Concomitant Chemotherapy Radiosenstization of tissues Cystoscopic response evaluation CR Consolidation Chemo-radiation (64Gy) +/- adjuvant chemo Non-CR Radical Cystectomy +/- adjuvant chemo





62 Max. TURBT 3 cycles of Gem+Cisplatin Follow up cystoscopy CR another 3 cycles + Rth Reaidual Disease Unfit Radiochemo fit Cysectomy



63 What is the importance of an aggressive TURBT for Cystectomy Avoidance? The TURBT must be done with the determination to resect all visible tumor. Nothing less will suffice NM Heney et al NATURE Rev Clin Oncol
64 Pathological exam of cystoscopic biopsy should comment on: Tumor growth pattern. Grade. Evidence of muscle invasion. Multifocality. Presence of associated carcinoma in situ.

65 What is the incidence comorbidities in patients with MIBC?

66
67 Co-morbidities and bladder cancer CO-MORBID ILLNESS None 1 2 OR MORE DM Hypertension Cardiovascular Pulmonary TOTAL % TYPE OF CO-MORBID ILLNESS MEAN AGE (n=2445) in south of Netherlands Goosens-Loan et al. Int J. Cancer: 135, ;

68 I ll save the patient.. From this serial killer!! Son, Patient will lose his bladder Sooner or later! Why not to try trimodality technique sir?
69 CYSTECTOMY 11% PARTIAL CYSTECTOMY 1% NO SUBSEQUENT SURGICAL PROCEDURE AT THE HOSPITAL 57% TURBT OR DESTRUCTION 31% TOTAL CYSTECTOMY PARTIAL CYSTECTOMY TURBT NO SUBSEQUENT SURGICAL PROCEDURE AT THE HOSPITAL Hayter et al IJROBP P
70 Cochrane Central Register of Controlled Trials and MEDLINE. Considered all controlled trials providing information about the efficacy and safety of trimodality therapy for selective organ preservation in urothelial cell carcinoma of the bladder as eligible.

71


72 .

73 What about side effects and toxicity?
74
75 Results Median follow-up was 5.4 years (range, 2.0 to 13.2 years). 7% experienced late grade 3 + pelvic toxicity: 5.7% GU and 1.9% GI. Notably there were no late grade 4 toxicities. No treatment-related deaths. None of the clinical variables studied predicted for late grade 3 + pelvic toxicity. Conclusion Rates of significant late pelvic toxicity for patients completing combined-modality therapy for invasive bladder cancer and retaining their native bladder are low.
76


77
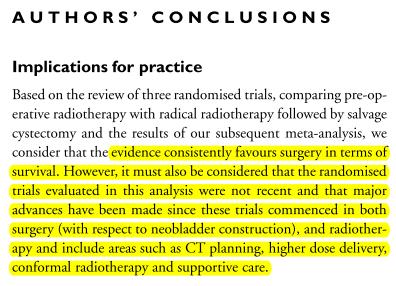
78
79

80
81
82
83
84
85
86

87
88 Bloom 1982 study, preoperative radiation treatment consisted of 4000 cgy in 4 weeks to the whole pelvis followed 4 weeks later by cystectomy (method not stated). The radical radiotherapy schedule was 4000 cgy in 4 weeks plus a 2000 cgy boost in 2 weeks to the bladder and perivesical tissue. Eighteen patients had salvage cystectomy for recurrent or residual tumour. Miller 1973 study the preoperative and radical radiotherapy schedules were 5000 cgy in 25 fractions over 5 weeks and 7000 cgy in 35 fractions over 7 weeks, respectively. Radical cystectomy consisted of radical cystoprostatectomy (anterior pelvic exenteration in women) and bilateral ureto-ileostomy with no node dissection. Two patients underwent salvage cystectomy following radical radiotherapy. Sell 1991 employed radiotherapy to the whole pelvis with rectal shielding using schedules of 4000 cgy in 20 fractions over 5 weeks (pre-operative) and a total dose of 6000 cgy (radical). Cystectomy was performed according to the method of Whitmore 1977, which included cystoprostatectomy plus pelvic lymph node dissection, and diversion as an ileal conduit. A nerve-sparing procedure was carried out in 9 patients from the radical cystectomy group and 2 from the radical radiotherapy group.
89


90 Rosinger et al 1992
91
92
93

94 RADIOLOGY PATHOLOGY UROLOGY ONCOLOGY

95
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer
 Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Some Seminal Studies. Chemotherapy Alone is Inadequate. Bladder Cancer Role of Radiation in Bladder Sparing. Primary Radiation for Bladder Cancer
 Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Cancer Role of Radiation in Bladder Sparing David C. Beyer M.D., FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Primary Radiation for Bladder Cancer No modern surgery / XRT randomized
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer
 Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Bladder Sparing Treatment of Muscle Invasive Bladder Cancer Pr Alexandre de la Taille CHU Mondor, Créteil INSERMU955Eq07 adelataille@hotmail.com High-Risk Invasive and Muscle-Invasive BCa Radical cystectomy
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline
 Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
Treatment of Non-Metastatic Muscle-Invasive Bladder Cancer: AUA/ASCO/ASTRO/SUO Guideline Jeffrey M. Holzbeierlein, MD, FACS John W Weigel Professor & Chair Director of Urologic Oncology University of Kansas
AUA Guidelines for Invasive Bladder Cancer: What s New?
 AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
AUA Guidelines for Invasive Bladder Cancer: What s New? Michael S. Cookson, MD, MMHC Professor and Chairman Department of Urology, University of Oklahoma History 1999: AUA guidelines Panel Non-muscle invasive
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Organ-sparing treatment of invasive transitional cell bladder carcinoma
 Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Radical Cystectomy in the Treatment of Bladder Cancer: Oncological Outcome and Survival Predictors
 ORIGINAL ARTICLE Radical Cystectomy in the Treatment of Bladder Cancer: Oncological Outcome and Survival Predictors Chen-Hsun Ho, 1,2 Chao-Yuan Huang, 1 Wei-Chou Lin, 3 Shih-Chieh Chueh, 1 Yeong-Shiau
ORIGINAL ARTICLE Radical Cystectomy in the Treatment of Bladder Cancer: Oncological Outcome and Survival Predictors Chen-Hsun Ho, 1,2 Chao-Yuan Huang, 1 Wei-Chou Lin, 3 Shih-Chieh Chueh, 1 Yeong-Shiau
Greater Baltimore Medical Center Sandra & Malcolm Berman Cancer Institute
 2008 ANNUAL REPORT Greater Baltimore Medical Center Sandra & Malcolm Berman Cancer Institute Cancer Registry Report The Cancer Data Management System/ Cancer Registry collects data on all types of cancer
2008 ANNUAL REPORT Greater Baltimore Medical Center Sandra & Malcolm Berman Cancer Institute Cancer Registry Report The Cancer Data Management System/ Cancer Registry collects data on all types of cancer
A patient with recurrent bladder cancer presents with the following history:
 MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
3.1 Investigations for Patients Presenting with Haematuria Table 1
 3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
3.1 Investigations for Patients Presenting with Haematuria Table 1 Patients at risk of bacterial endocarditis should be given antibiotic prophylaxis as per local guidelines. Patients with heart valve replacements
Point/Counterpoint: Quality of Life Considerations for Patients with Muscle Invasive Bladder Cancer Pro Trimodality Therapy
 Point/Counterpoint: Quality of Life Considerations for Patients with Muscle Invasive Bladder Cancer Pro Trimodality Therapy Kimberley S. Mak, MD, MPH Assistant Professor Boston Medical Center Boston University
Point/Counterpoint: Quality of Life Considerations for Patients with Muscle Invasive Bladder Cancer Pro Trimodality Therapy Kimberley S. Mak, MD, MPH Assistant Professor Boston Medical Center Boston University
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
Care of bladder cancer patients diagnosed in Northern Ireland 2010 & 2011 (Summary)
") Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary) Bannon, F., Ranaghan, L., & Gavin, A. (2014). Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary). N. Cancer Registry,
Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary) Bannon, F., Ranaghan, L., & Gavin, A. (2014). Care of bladder cancer patients diagnosed in 2010 & 2011 (Summary). N. Cancer Registry,
Cancer Cases Treated and Results
 Cancer Cases Treated and Results Below are some of the cases, from more than 30 cases we have treated so far with good results. When reading the PET/CT scans, the picture on the left is before treatment,
Cancer Cases Treated and Results Below are some of the cases, from more than 30 cases we have treated so far with good results. When reading the PET/CT scans, the picture on the left is before treatment,
Bone Metastases in Muscle-Invasive Bladder Cancer
 Journal of the Egyptian Nat. Cancer Inst., Vol. 18, No. 3, September: 03-08, 006 AZZA N. TAHER, M.D.* and MAGDY H. KOTB, M.D.** The Departments of Radiation Oncology* and Nuclear Medicine**, National Cancer
Journal of the Egyptian Nat. Cancer Inst., Vol. 18, No. 3, September: 03-08, 006 AZZA N. TAHER, M.D.* and MAGDY H. KOTB, M.D.** The Departments of Radiation Oncology* and Nuclear Medicine**, National Cancer
UROTHELIAL CELL CANCER
 UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
UROTHELIAL CELL CANCER Indications and regimens for neoadjuvant systemic treatment Astrid A. M. van der Veldt, MD, PhD, medical oncologist Department of Medical Oncology Erasmus Medical Center Cancer Institute
Clinical Value of C-reactive Protein and Erythrocyte Sedimentation Rate in Advanced Bladder Cancer
 Original Article Research in Oncology 2018; Vol. XX, No. X: X-X. DOI: 10.21608/resoncol.2018.4152.1060 Clinical Value of C-reactive Protein and Erythrocyte Sedimentation Rate in Advanced Bladder Cancer
Original Article Research in Oncology 2018; Vol. XX, No. X: X-X. DOI: 10.21608/resoncol.2018.4152.1060 Clinical Value of C-reactive Protein and Erythrocyte Sedimentation Rate in Advanced Bladder Cancer
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Clinical Commissioning Policy Proposition: Robotic Assisted Surgery for Bladder Cancer
 Clinical Commissioning Policy Proposition: Robotic Assisted Surgery for Bladder Cancer Reference: NHS England B14X08 Information Reader Box (IRB) to be inserted on inside front cover for documents of 6
Clinical Commissioning Policy Proposition: Robotic Assisted Surgery for Bladder Cancer Reference: NHS England B14X08 Information Reader Box (IRB) to be inserted on inside front cover for documents of 6
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Cochrane metaanalysis 5 year OS Intent to treat
 RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
RADICAL CYSTECTOMY IS THE ONLY EFFECTIVE TREATMENT FOR PATIENTS WITH OPERABLE MUSCLE INVASIVE BLADDER CANCER The Con position Scott Tyldesley Radiation Oncology, Vancouver Centre, BC Cancer Agency Cochrane
Highlighting Clinical Trials Muscle Invasive Bladder Cancer
 Highlighting Clinical Trials Muscle Invasive Bladder Cancer Part I: The Basics of MIBC Clinical Trials June 19, 2018 Presented by: Dr. Peter Black is a urologic oncologist at Vancouver General Hospital,
Highlighting Clinical Trials Muscle Invasive Bladder Cancer Part I: The Basics of MIBC Clinical Trials June 19, 2018 Presented by: Dr. Peter Black is a urologic oncologist at Vancouver General Hospital,
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Bladder Preservation Protocols in the Treatment of Muscle-Invasive Bladder Cancer
 Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
Bladder-preserving therapy is a safe and effective alternative to cystectomy for carefully selected patients with bladder cancer. Michael Mahany. Trumpeter Swans on Byer s Lake. Photograph. Denali National
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer Center Contemporary Experience
 International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER
 RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
RADIOTHERAPY IN THE MANAGEMENT OF CANCERS OF THE URINARY BLADDER INTRODUCTION Incidence: Mortality: 20/100000/year (Europe) 8-9/100000/year Worldwide fourth most common cancer in men Incidence: 31.1 mortality:
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY
 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Cancer is a group of more than 100 different diseases that are characterized by uncontrolled cellular growth,
Macmillan Publications
 S1 S2 S3 S3 S3 S4 S5 S6 S7 S8 S8 S9 S10 S11 S11 S12 S13 S14 S15 S17 S18 S19 Bladder Cancer: Non-Invasive, Invasive and Advanced Bone Cancer: Primary, Secondary Colon Cancer, Anal Cancer, Rectal Cancer
S1 S2 S3 S3 S3 S4 S5 S6 S7 S8 S8 S9 S10 S11 S11 S12 S13 S14 S15 S17 S18 S19 Bladder Cancer: Non-Invasive, Invasive and Advanced Bone Cancer: Primary, Secondary Colon Cancer, Anal Cancer, Rectal Cancer
Upper Egypt experience in bladder preservation using concurrent chemoradiotherapy
 Maklad et al. International Archives of Medicine 2013, 6:21 ORIGINAL RESEARCH Open Access Upper Egypt experience in bladder preservation using concurrent chemoradiotherapy Ahmed M Maklad 1*, Elsayed M
Maklad et al. International Archives of Medicine 2013, 6:21 ORIGINAL RESEARCH Open Access Upper Egypt experience in bladder preservation using concurrent chemoradiotherapy Ahmed M Maklad 1*, Elsayed M
September 10, Dear Dr. Clark,
 September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
Outcomes Report: Accountability Measures and Quality Improvements
 Outcomes Report: Accountability Measures and Quality Improvements The s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures. Because we are an accredited
Outcomes Report: Accountability Measures and Quality Improvements The s Cancer Committee ensures that patients with cancer are treated according to the nationally accepted measures. Because we are an accredited
ROBOTIC VS OPEN RADICAL CYSTECTOMY
 ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
Point-Counterpoint: Radiation & Bladder Cancer
 Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Radical Cystectomy Often Too Late? Yes, But...
 european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
Partial Cystectomy for Invasive Bladder Cancer
 European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
UPDATE ON RADIOTHERAPY
 1 Miriam Kleiter UPDATE ON RADIOTHERAPY Department for Companion Animals and Horses, Plattform Radiooncology and Nuclear Medicine, University of Veterinary Medicine Vienna Introduction Radiotherapy has
1 Miriam Kleiter UPDATE ON RADIOTHERAPY Department for Companion Animals and Horses, Plattform Radiooncology and Nuclear Medicine, University of Veterinary Medicine Vienna Introduction Radiotherapy has
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Cystectomies and bladder preservation: What you need to know
 Cystectomies and bladder preservation: What you need to know Robin Morash RN, BNSc, MHS Bladder Cancer Canada November 21, 2018 Presentation goals Review the options for treatment of muscle-invasive bladder
Cystectomies and bladder preservation: What you need to know Robin Morash RN, BNSc, MHS Bladder Cancer Canada November 21, 2018 Presentation goals Review the options for treatment of muscle-invasive bladder
Types of bladder cancer
 There are three main types of bladder cancer: Urothelial bladder cancer Squamous cell cancer Adenocarcinoma of the bladder There is more information about how we treat the different types of bladder cancer
There are three main types of bladder cancer: Urothelial bladder cancer Squamous cell cancer Adenocarcinoma of the bladder There is more information about how we treat the different types of bladder cancer
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Part II: Treatment. A Woman-to-Woman Talk with Dr. Armine Smith. Wednesday, March 8, Presented by
 Women & Bladder Cancer A Woman-to-Woman Talk with Dr. Armine Smith Wednesday, March 8, 2017 Part II: Treatment Presented by Dr. Smith is an Assistant Professor of Urology at Johns Hopkins University and
Women & Bladder Cancer A Woman-to-Woman Talk with Dr. Armine Smith Wednesday, March 8, 2017 Part II: Treatment Presented by Dr. Smith is an Assistant Professor of Urology at Johns Hopkins University and
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Koji Ichihara Hiroshi Kitamura Naoya Masumori Fumimasa Fukuta Taiji Tsukamoto
 Int J Clin Oncol (2013) 18:75 80 DOI 10.1007/s10147-011-0346-8 ORIGINAL ARTICLE Transurethral prostate biopsy before radical cystectomy remains clinically relevant for decision-making on urethrectomy in
Int J Clin Oncol (2013) 18:75 80 DOI 10.1007/s10147-011-0346-8 ORIGINAL ARTICLE Transurethral prostate biopsy before radical cystectomy remains clinically relevant for decision-making on urethrectomy in
Breast cancer Can I still keep my breast?
 Bladder Cancer Organ-Sparing Approaches SAMO Interdisciplinary Workshop on Urogenital Tumors September 15, 2012 Daniel R. Zwahlen, MD Radiation Oncology Breast cancer Can I still keep my breast? History
Bladder Cancer Organ-Sparing Approaches SAMO Interdisciplinary Workshop on Urogenital Tumors September 15, 2012 Daniel R. Zwahlen, MD Radiation Oncology Breast cancer Can I still keep my breast? History
Old and New Radiation for Bladder and Upper Tract Cancers. Bridget Koontz Radiation Oncology Duke Cancer Institute
 Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
BLADDER CANCER CONTENT CREATED BY. Learn more at
 BLADDER CANCER CONTENT CREATED BY Learn more at www.health.harvard.edu TALK TO YOUR DOCTOR Table of Contents WHAT IS BLADDER CANCER? 4 TYPES OF BLADDER CANCER 5 GRADING AND STAGING 8 TREATMENT OVERVIEW
BLADDER CANCER CONTENT CREATED BY Learn more at www.health.harvard.edu TALK TO YOUR DOCTOR Table of Contents WHAT IS BLADDER CANCER? 4 TYPES OF BLADDER CANCER 5 GRADING AND STAGING 8 TREATMENT OVERVIEW
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
GUIDELINES ON PROSTATE CANCER
 10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
10 G. Aus (chairman), C. Abbou, M. Bolla, A. Heidenreich, H-P. Schmid, H. van Poppel, J. Wolff, F. Zattoni Eur Urol 2001;40:97-101 Introduction Cancer of the prostate is now recognized as one of the principal
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
DEPARTMENT OF ONCOLOGY ELECTIVE
 DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
DEPARTMENT OF ONCOLOGY ELECTIVE 2015-2016 www.uwo.ca/oncology Oncology Elective Program Administrator: Ms. Kimberly Trudgeon Room A4-901C (Admin) LHSC London Regional Cancer Centre (Victoria Campus) Phone:
Pure non-bilharzial squamous cell carcinoma: An unusual form of carcinoma of the bladder
 Safini et al. 31 case Series report peer Reviewed open OPEN ACCESS Pure non-bilharzial squamous cell carcinoma: An unusual form of carcinoma of the bladder Fatima Safini, Hassan Jouhadi, Meriem Elbachiri,
Safini et al. 31 case Series report peer Reviewed open OPEN ACCESS Pure non-bilharzial squamous cell carcinoma: An unusual form of carcinoma of the bladder Fatima Safini, Hassan Jouhadi, Meriem Elbachiri,
Case Report Stereotactic Body Radiotherapy for Localized Ureter Transitional Cell Carcinoma: Three Case Reports
 Case Reports in Urology Volume 2015, Article ID 519897, 4 pages http://dx.doi.org/10.1155/2015/519897 Case Report Stereotactic Body Radiotherapy for Localized Ureter Transitional Cell Carcinoma: Three
Case Reports in Urology Volume 2015, Article ID 519897, 4 pages http://dx.doi.org/10.1155/2015/519897 Case Report Stereotactic Body Radiotherapy for Localized Ureter Transitional Cell Carcinoma: Three
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Radiation Oncology MOC Study Guide
 Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Radiation Oncology MOC Study Guide The following study guide is intended to give a general overview of the type of material that will be covered on the Radiation Oncology Maintenance of Certification (MOC)
Prostate Case Scenario 1
 Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
Prostate Case Scenario 1 H&P 5/12/16: A 57-year-old Hispanic male presents with frequency of micturition, urinary urgency, and hesitancy associated with a weak stream. Over the past several weeks, he has
An Update on Radiation Therapy for Prostate Cancer
 An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
Does the Use of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers Improve Survival in Bladder Cancer?
 Does the Use of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers Improve Survival in Bladder Cancer? Authors: Roderick Clark, 1 Kevin Wong, 2 Stacy Fan, 2 Joseph Chin, 1,3 Jonathan
Does the Use of Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers Improve Survival in Bladder Cancer? Authors: Roderick Clark, 1 Kevin Wong, 2 Stacy Fan, 2 Joseph Chin, 1,3 Jonathan
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists. Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University
 Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Optimal sequencing in treatment muscle invasive bladder cancer : oncologists Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Slide 2 Presented By Andrea Apolo at 2018 Genitourinary Cancers
Dr. Sause: Clinical, Research, and Administration. Vilija N. Avizonis, MD Radiation Oncologist; Intermountain Medical Center; Murray, Utah
 Dr. Sause: Clinical, Research, and Administration Vilija N. Avizonis, MD Radiation Oncologist; Intermountain Medical Center; Murray, Utah Objectives: Identify Dr. Sause's educational achievements Discuss
Dr. Sause: Clinical, Research, and Administration Vilija N. Avizonis, MD Radiation Oncologist; Intermountain Medical Center; Murray, Utah Objectives: Identify Dr. Sause's educational achievements Discuss
Bladder Cancer Canada November 21st, Bladder Cancer 2018: A brighter light at the end of the cystoscope
 Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Cancer Program Report 2014
 Cancer Program Report 2014 Queen of the Valley Hospital St Joseph Health Queen of the Valley Hospital - 2014 Site Table Site Total Class Sex Group Cases Analytic NonAn M F 0 I II ALL SITES 661 494 167
Cancer Program Report 2014 Queen of the Valley Hospital St Joseph Health Queen of the Valley Hospital - 2014 Site Table Site Total Class Sex Group Cases Analytic NonAn M F 0 I II ALL SITES 661 494 167
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology
 Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
BACKGROUND. Many patients with invasive urothelial cell cancer are poor candidates
 2181 Treatment Options for Muscle-invasive Urothelial Cancer for Patients Who Were Not Eligible for Cystectomy or Neoadjuvant Chemotherapy With Methotrexate, Vinblastine, Doxorubicin, and Cisplatin Report
2181 Treatment Options for Muscle-invasive Urothelial Cancer for Patients Who Were Not Eligible for Cystectomy or Neoadjuvant Chemotherapy With Methotrexate, Vinblastine, Doxorubicin, and Cisplatin Report
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Early radical cystectomy in NMIBC Marko Babjuk
 Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Oncology 101. Cancer Basics
 Oncology 101 Cancer Basics What Will You Learn? What is Cancer and How Does It Develop? Cancer Diagnosis and Staging Cancer Treatment What is Cancer? Cancer is a group of more than 100 different diseases
Oncology 101 Cancer Basics What Will You Learn? What is Cancer and How Does It Develop? Cancer Diagnosis and Staging Cancer Treatment What is Cancer? Cancer is a group of more than 100 different diseases
Chemo-radiotherapy in muscle invasive bladder cancer. Dr Paula Wells St Bartholomew s Hospital London
 Chemo-radiotherapy in muscle invasive bladder cancer Dr Paula Wells St Bartholomew s Hospital London Overview Evidence base for cystectomy vs bladder preservation Chemo-radiotherapy vs radiotherapy alone
Chemo-radiotherapy in muscle invasive bladder cancer Dr Paula Wells St Bartholomew s Hospital London Overview Evidence base for cystectomy vs bladder preservation Chemo-radiotherapy vs radiotherapy alone
Radiotherapy Physics and Equipment
 Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
Q&A. Overview. Collecting Cancer Data: Prostate. Collecting Cancer Data: Prostate 5/5/2011. NAACCR Webinar Series 1
 Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Bladder Cancer in Primary Care. Dr Penny Kehagioglou Consultant Clinical Oncologist
 Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
Bladder Cancer in Primary Care Dr Penny Kehagioglou Consultant Clinical Oncologist Objectives Patient presentation in primary care Investigating bladder cancer Management of bladder cancer Differential
5/26/16: CT scan of the abdomen showed a multinodular liver disease highly suspicious for metastasis and hydronephrosis of the right kidney.
 Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Case Scenario 1 History 5/23/16: A 52-year-old male, smoker was admitted to our hospital with a 3-month history of right pelvic pain, multiple episodes of gross hematuria, dysuria, and extreme
Bladder Preservation for muscle invasive disease. Nicholas
 Bladder Preservation for muscle invasive disease Nicholas James @Prof_Nick_James 1 Overview Evidence base for bladder preservation as alternative to surgery Chemoradiotherapy compared to radiotherapy alone
Bladder Preservation for muscle invasive disease Nicholas James @Prof_Nick_James 1 Overview Evidence base for bladder preservation as alternative to surgery Chemoradiotherapy compared to radiotherapy alone
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Multidisciplinary management of retroperitoneal sarcomas
 Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
Multidisciplinary management of retroperitoneal sarcomas Eric K. Nakakura, MD UCSF Department of Surgery UCSF Comprehensive Cancer Center San Francisco, CA 7 th Annual Clinical Cancer Update North Lake
The Predictors of Local Recurrence after Radical Cystectomy in Patients with Invasive Bladder Cancer
 The Predictors of Local Recurrence after Radical Cystectomy in Patients with Invasive Bladder Cancer Hiroki Ide, Eiji Kikuchi, Akira Miyajima, Ken Nakagawa, Takashi Ohigashi, Jun Nakashima and Mototsugu
The Predictors of Local Recurrence after Radical Cystectomy in Patients with Invasive Bladder Cancer Hiroki Ide, Eiji Kikuchi, Akira Miyajima, Ken Nakagawa, Takashi Ohigashi, Jun Nakashima and Mototsugu
Subject Index. Androgen antiandrogen therapy, see Hormone ablation therapy, prostate cancer synthesis and metabolism 49
 OOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index Androgen antiandrogen therapy, see Hormone ablation therapy, synthesis and metabolism 49 Bacillus Calmette-Guérin adjunct therapy with transurethral resection
OOOOOOOOOOOOOOOOOOOOOOOOOOOOOO Subject Index Androgen antiandrogen therapy, see Hormone ablation therapy, synthesis and metabolism 49 Bacillus Calmette-Guérin adjunct therapy with transurethral resection
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Index Note: Page numbers of article titles are in boldface type. A Abdominal drainage, after hepatic resection, 159 160 Ablation, radiofrequency, for hepatocellular carcinoma, 160 161 Adenocarcinoma, pancreatic.
Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy
 Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy Mitsui Memorial Hospital Department of Breast and Endocine surgery Daisuke Ota No financial support
Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy Mitsui Memorial Hospital Department of Breast and Endocine surgery Daisuke Ota No financial support
Chemotherapy and Bladder Cancer. Blayne Welk UBC Urology Grand Rounds June 4, 2008
 Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
Chemotherapy and Bladder Cancer Blayne Welk UBC Urology Grand Rounds June 4, 2008 Outline Review of Incidence and Impact of bladder cancer Neoadjuvant chemotherapy Adjuvant chemotherapy Bladder preservation
and Strength of Recommendations
 ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
ASTRO with ASCO Qualifying Statements in Bold Italics s patients with T1-2, N0 non-small cell lung cancer who are medically operable? 1A: Patients with stage I NSCLC should be evaluated by a thoracic surgeon,
Bilharzial Bladder Cancer in Egypt A Review of 420 Cases of Radical Cystectomy
 Jap. J. Clin. Oncol. 1979, 9 (1), 117-122 Bilharzial Bladder Cancer in Egypt A Review of 2 Cases of Radical Cystectomy A. EL-SAID, M.D., S. OMAR, M.D., S. IBRAHIM, M.D., H. TAWFIK, M.D., S. EISSA, M.D.,
Jap. J. Clin. Oncol. 1979, 9 (1), 117-122 Bilharzial Bladder Cancer in Egypt A Review of 2 Cases of Radical Cystectomy A. EL-SAID, M.D., S. OMAR, M.D., S. IBRAHIM, M.D., H. TAWFIK, M.D., S. EISSA, M.D.,
Understanding Systemic Chemotherapy Options in Bladder Cancer. Part III: Chemoradiotherapy
 Understanding Systemic Chemotherapy Options in Bladder Cancer Tuesday, July 25, 2017 Part III: Chemoradiotherapy Presented by Dr. Jean Hoffman-Censits is a genitourinary medical oncologist at the Sidney
Understanding Systemic Chemotherapy Options in Bladder Cancer Tuesday, July 25, 2017 Part III: Chemoradiotherapy Presented by Dr. Jean Hoffman-Censits is a genitourinary medical oncologist at the Sidney
Urinary Bladder Cancer
 Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast