2018 ASTRO Refresher Course: Prostate Cancer. Timur Mitin, MD PhD Oregon Health and Science University
|
|
|
- Cori Strickland
- 6 years ago
- Views:
Transcription
1 2018 ASTRO Refresher Course: Prostate Cancer Timur Mitin, MD PhD Oregon Health and Science University
2 Disclosures UpToDate Chapter author, royalties Oregon Health and Science University Practicing Radiation Oncologist, salary

3 Learning Objectives Review the most recent literature Learn how to incorporate clinical evidence into clinical practice
4
5 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters
6 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters


7 Prostate Cancer Screening Trials Andriole et al.,, JNCI 2012; Schroder et al., Lancet 2014; Hugosson et al., Lancet 2010
8 Comparing to screening mammography Based on randomized clinical trials, for women ages 40-49, NNI was estimated at 1904 (USPSTF, Intern Med 2009, 151: ) Based on Cancer Intervention and Surveillance Modeling Network analysis: for women ages NNS was estimated at 746, for women between NNS was 351, for women ages NNS was 233, for women ages NNS was 377 (Hendrick and Helvie, AJR, 2012, 198: )
9 PSA Screening Guidelines USPSTF (May 2012): recommends against PSA screening AUA (April 2013) <40 yo: No screening recommended 40-54yo: No screening recommended unless higher risk (ex: family hx, AA) yo: Risk/Benefit discussion with patient and screening if patient is in agreement shared decision making based on a man s values and preferences 70+ yo: No screening recommended, some men in excellent health may benefit

10 PSA Screening Guidelines
11 Conclusion Conflicting evidence from randomized trials Conflicting national guidelines If one considers offering PSA screening, it should start with a thorough discussion of risks and benefits

12 ProtecT: The Trial of the Century Turner, Br J Ca 2014
13 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters
14 ProtecT: Patients Criteria yo PSA 3-20, median 4.6 ct1-t2n0m0, 76% T1c Initial workup DRE PSA TRUS biopsy MRI optional Bone scan if PSA >10 or G>7 Randomized by practice Stratified by Age Gleason PSA Lane, Lancet Oncol 2014
 Lane, Lancet Oncol 2014")
15 ProtecT: Treatments Active monitoring PSA q3 mo x 1y, q6 mo thereafter Rise of 50% in 12 mo: consider biopsy RT 3D CRT 74 Gy/37 fx 3-6 mo neoadjuvant and concurrent ADT Prostatectomy 82% open, 6% lap, 6% robot 66% nerve-sparing PLND if PSA 10, Gleason 7 29% with ECE (upstaged to T3) Lane, Lancet Oncol 2014
 99.0% (Surgery) 99.")
16 ProtecT: Outcomes Prostate-cancer-specific survival at 10 years: 98.8% (AM) 99.0% (Surgery) 99.6% (EBRT+ADT) Hamdy, N Engl J Med 2016

17 ProtecT: GS 6 vs 7
18 Other lessons from ProtecT: Conversion to treatment 291/545 (53%) of AM underwent surgery or RT by 10y AM often deferral, not avoidance, of treatment 19% tx within 9 mo Primary treatment failure RP: 4.6% (18) (PSA 0.2 at 3mo) RT: 14% (55) (PSA 2+nadir)
19 Active surveillance: take-home message Does not jeopardize overall and prostate cancer-specific survival A shared-decision with patient: Metastastic disease developed in 6.3 vs 3.0 per 1000 person-yr on AM vs RT No difference in survival Differences in quality of life Different approach in US: Toronto experience (Klotz et al., JCO 2010): Confirmatory biopsy at 6-12 months, then q 3-4 years until age 80 Johns Hopkins experience (Tosoian et al., JCO 2011): Annual biopsies NCCN guidelines (Version ): A repeat prostate biopsy should be considered as often as annually to assess for disease progression, because PSA kinetics may not be as reliable as monitoring parameters to determine progression of disease. Biopsy is no longer indicated when life expectancy is < 10 years.
20 Active surveillance: take-home message
21 ProtecT: QOL Donovan, N Engl J Med 2016

22 Kiri Sandler (UCLA): Survey of expert GU radiation oncologists I often recommend AS to patients with PCa 95.20% % 50.00% 0.00% 16.70% Gleason 3+3 Gleason 3+4 McClelland et al., Clinical Genitourinary Cancer, in press

23 Low/Intermediate PCa: Brachytherapy BJU, 2012
24 Low/Intermediate PCa: Brachytherapy

25 Kiri Sandler (UCLA): Survey of expert GU radiation oncologists For a patient with Gleason 6 PCa who desires treatment, with no baseline urinary symptoms and a 40 cc gland, my first choice recommendation is: 50.00% 16.70% 50.00% 33.30% 0.00% EBRT Brachy Either McClelland et al., in submission
26 Conclusion Active surveillance is the default treatment modality for patients with low risk prostate cancer Potential for increased risk of metastatic disease progression should be discussed with patients Active surveillance may also be considered for patients with intermediate risk prostate cancer Brachytherapy may offer the most durable biochemical control for patients with low/intermediate risk disease
27 Updated Recommendations: For patients with low-risk prostate cancer who require or choose active treatment, LDR alone, EBRT alone, or RP should be offered to eligible patients For low-intermediate risk prostate cancer (Gleason 7, PSA < 10 or Gleason 6, PSA 10-20), LDR brachy alone may be offered as monotherapy I-125 and Pd-103 are each reasonable isotope options for patients receiving LDR brachytherapy No recommendation can be made for or against Cs-131 or HDR monotherapy
28 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters
29 EBRT: Conventional vs Hypofractionated RTOG 0415 CHHiP (UK, Ireland, Switzerland, New Zealand) HYPRO (Dutch) PROFIT (Canada, Australia and France)
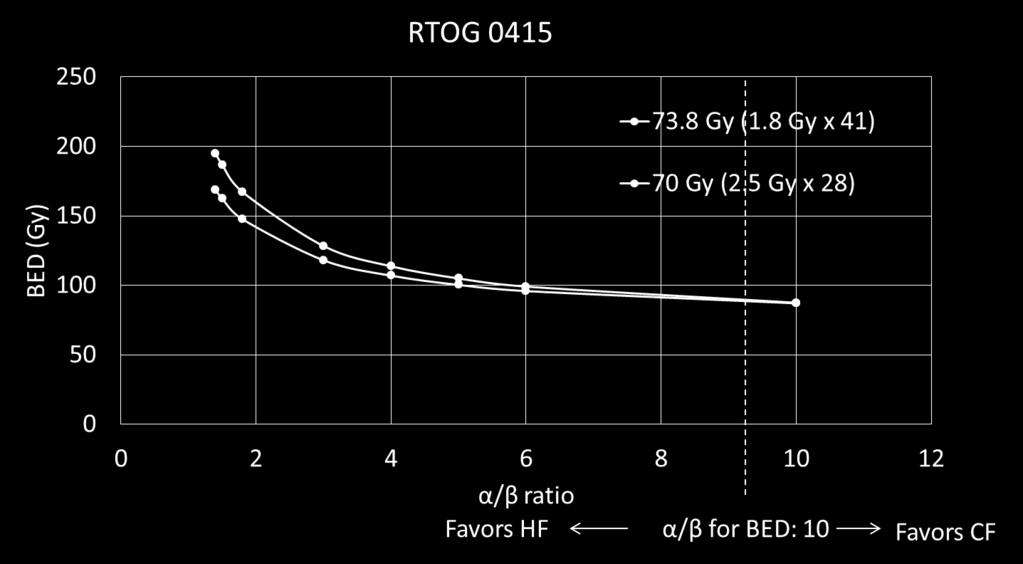
30 Hypofractionation: RTOG 0415

 All qd 21% 3D, 79% IMRT Fiducials required No")
31 RTOG men, median age 67 years All low-risk: T1b-T2c, Gleason 2-6, PSA <10 No ADT RT Randomization: 73.8/41 (1.8) vs 70/28 (2.5) All qd 21% 3D, 79% IMRT Fiducials required No SVs or LN
32 RTOG 0415: efficacy 5 yr DFS CF: 85.3% HF: 86.3% HR 0.85 ( ) p(ni)<0.001 Interpretation HF is non-inferior to CF with respect to 5 yr DFS 5 yr biochemical recurrence CF: 8.1% HF: 6.3% HR 0.77 ( ) p(ni)< yr OS CF: 93.2% HF: 92.5% HR 0.95 ( ) p(ni)=0.008
 p=0.005 GU Gr 2: 1.31 (1.07-1.61) p=0.009")
33 RTOG: toxicity Early (90d) no difference Late GI Gr 2: 1.59 ( ) p=0.005 GU Gr 2: 1.31 ( ) p=0.009


34 RTOG 0415: Toxicity With permission by Dr. Bruner
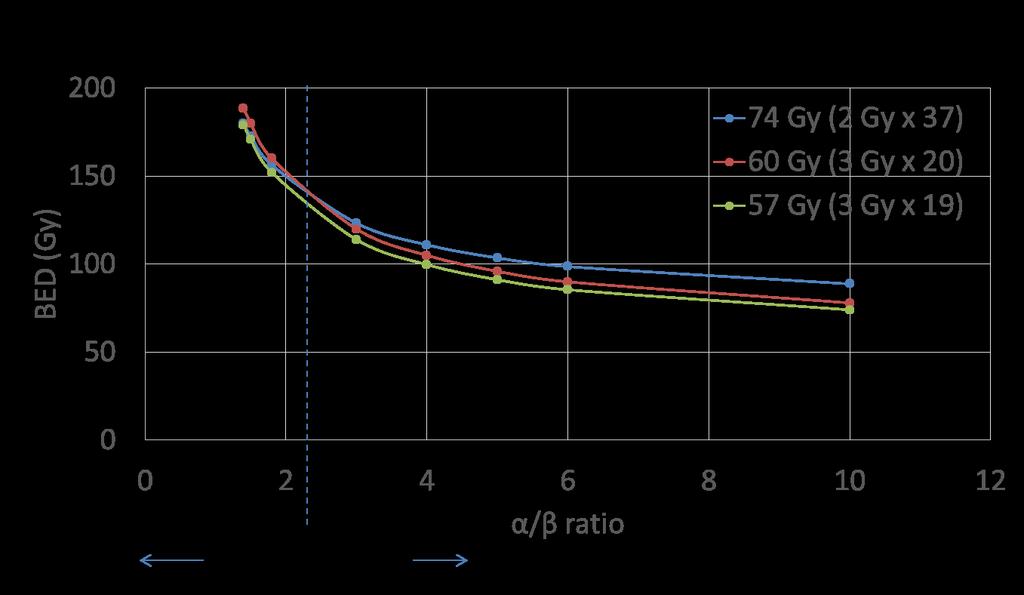
35 Hypofractionation: CHHiP

 RT Randomization: 74/37")

36 Hypofractionation: CHHiP 3216 men, 71 centers UK, Ireland, Switzerland, New Zealand Median 69 yo T1b-T3aN0, PSA <30 (mean 11) 13% low / 73% int / 12% high 96% ADT (median 24 wks) RT Randomization: 74/37 (2), 60/20 (3), 57/19 (3) No SVs or LN All IMRT; 30% IGRT Estimate PCa α/β 2.4 for 60/20 and 1.4 for 57/19 Dearnaley, Lancet Oncol 2016
37 CHHiP: efficacy 5 yr brfs/crfs 74 Gy: 88.3% ( %) 60 Gy: 90.6% ( %) vs 74: HR 0.84 ( ), p= Gy: 85.9% ( %) vs 74: HR 1.20 ( ), p=0.11 Interpretation (NI HR 1.208) 60 Gy is non-inferior to Gy not non-inferior to 74 Not designed to compare 60 Gy vs 57 Gy OS: no differences
38 CHHiP: acute toxicity GI grade 2: 38% vs 25%(SS) GU grade 2: 49% vs 46% (NS) By week 18, there was no difference Earlier peak of acute toxicity weeks 4-5 compared to weeks 7-8
39 CHHiP: late toxicity at 5 yrs GI GI grade 2: 12% GU grade 2: 10% Cumulative grade 3 toxicity < 4% GU
40 CHHiP: nuances 9% death within 5 years of starting ADT-RT: 16% Pca-related 35% related to 2 nd malignancy 44% non-cancer causes 5% unknown Pre-specified subgroup analysis: age and biochemical control Improved biochemical control between 60/20 and 57/19 last fraction matters! 3 Gy fractions rarely used in UK until , now 20% of patients are treated with 60/20
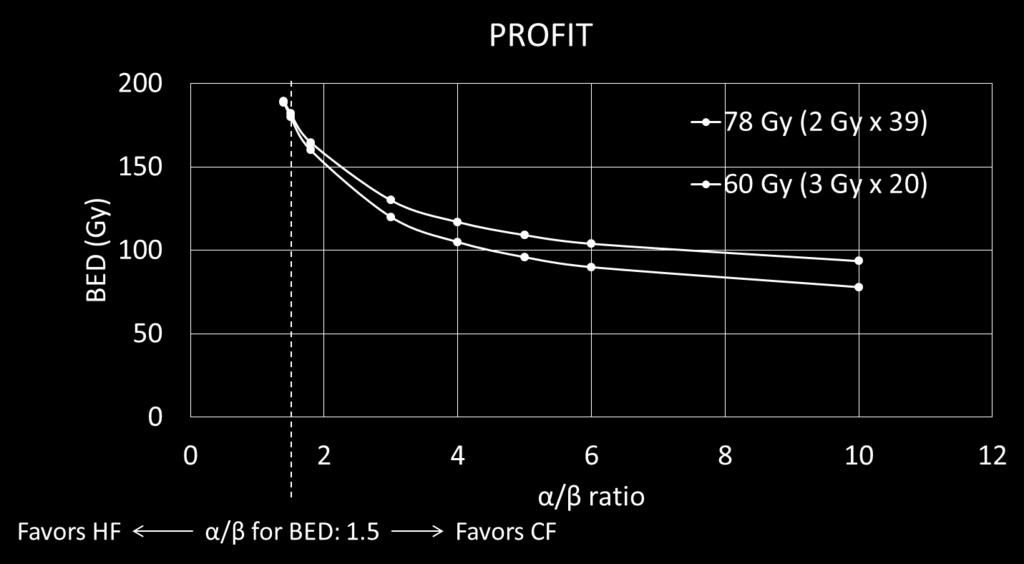
41 Hypofractionation: PROFIT
42 PROFIT: Trial and Efficacy 1206 men, 27 sites Canada, Australia, France Intermediate risk T1-T2, Gleason 6, PSA T2b-c, Gleason 6, PSA <20 T1-2, Gleason 7, PSA <20 ADT: not permitted with RT RT Randomization: 78/39 (2) vs 60/20 (3) Prostate +/- base of SV IGRT required Central plan review Results: Catton et al., JCO 35, 2017


43 PROFIT: Toxicity P=0.003 P=0.006 Catton et al., JCO 35, 2017
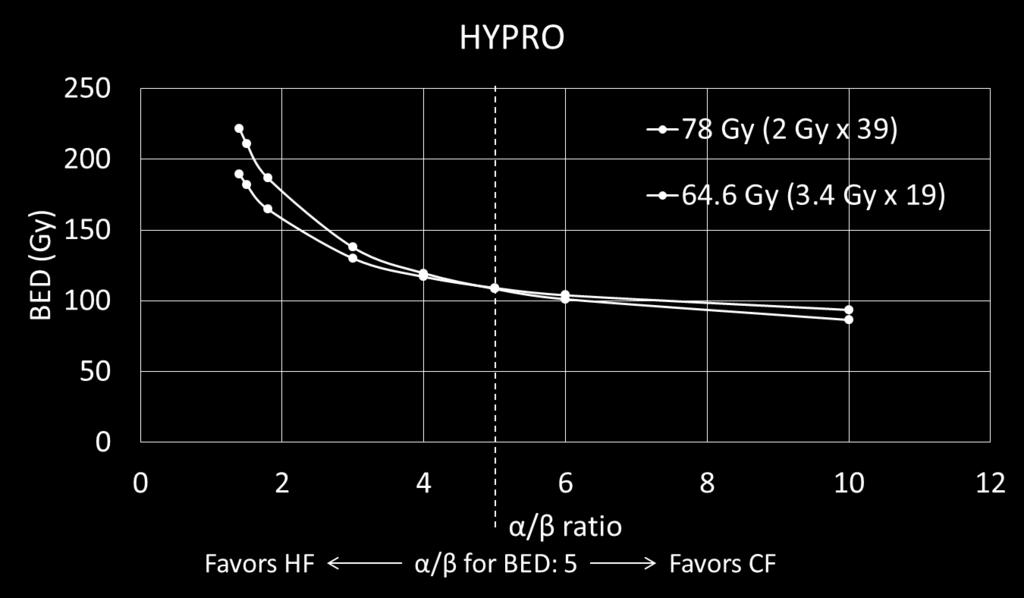
44 Hypofractionation: HYPRO
 qd vs 64.6/19 (3.")
45 HYPRO: Trial 820 men, median age 70 years 7 centers in Netherlands T1b-T4N0, PSA <60 0% low/26% int/74% high ADT 66%, median 32 mo RT Randomization: 78/39 (2.0) qd vs 64.6/19 (3.4) tiw Prostate; SV dose based on risk; no LN 95% IMRT, 94% fiducials
46 HYPRO: efficacy 5 yr RFS 64.6 Gy: 80.5% ( %) 78 Gy: 77.1% ( %) HR 0.86 ( ), p=0.36 Interpretation HF not superior Lower than CHHiP (88-90%), consistent with higher-risk disease OS no differences

47 HYPRO: toxicity
48 Meta-analysis Biochemical Control Acute GI Toxicity Late GI Toxicity Acute GU Toxicity Late GU Toxicity Datta, et al. IJROBP 2017

49 Kiri Sandler (UCLA): Survey of expert GU radiation oncologists Default EBRT fractionation for Gleason 3+4 PCa 54.80% 40.50% 60.00% 40.00% 20.00% 0.00% Conventional Moderate hypo SBRT 4.80% McClelland et al., in submission
50
51 Conclusion 4 randomized trials show no difference in treatment efficacy between conventional and hypofractionated RT to prostate at 5 years Three trials (60/20 or 70/28) showed no increased late toxicity at 5 years No treatment of pelvic lymph nodes Only one of three trials allowed treatment of SV base HYPRO had persistently higher treatment-related toxicity in hypofractionated arm with 3.4 Gy per fraction three times per week SVs were treated based on risk of involvement Longer follow-up needed Many institutions consider moderate hypofractionation (60/20 or 70/28) as a new standard for EBRT to prostate gland
52 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters
53 High Risk Prostate Cancer: Is EBRT enough? Spratt et al., The ABS Task Group Report, Brachytherapy 2016
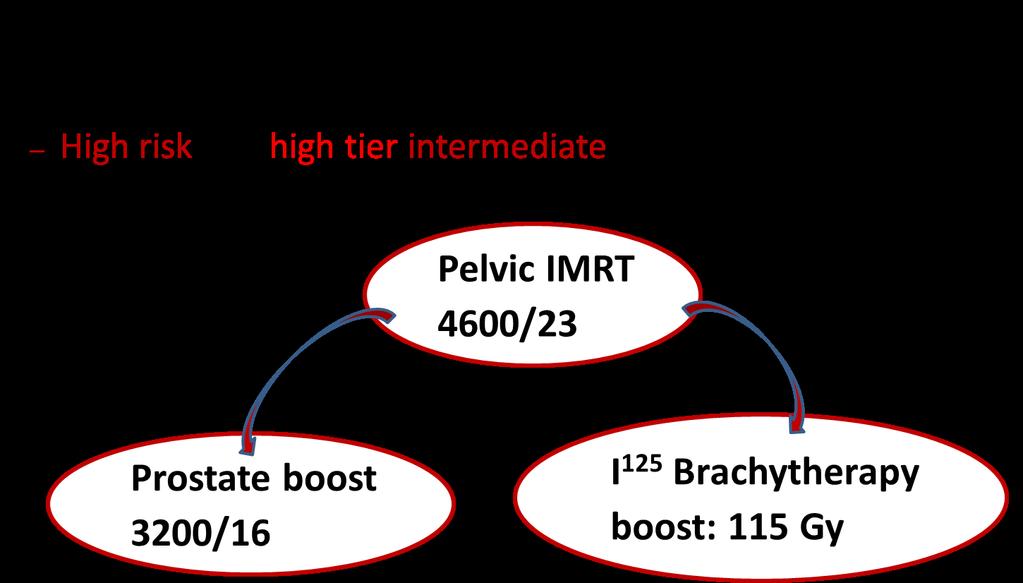
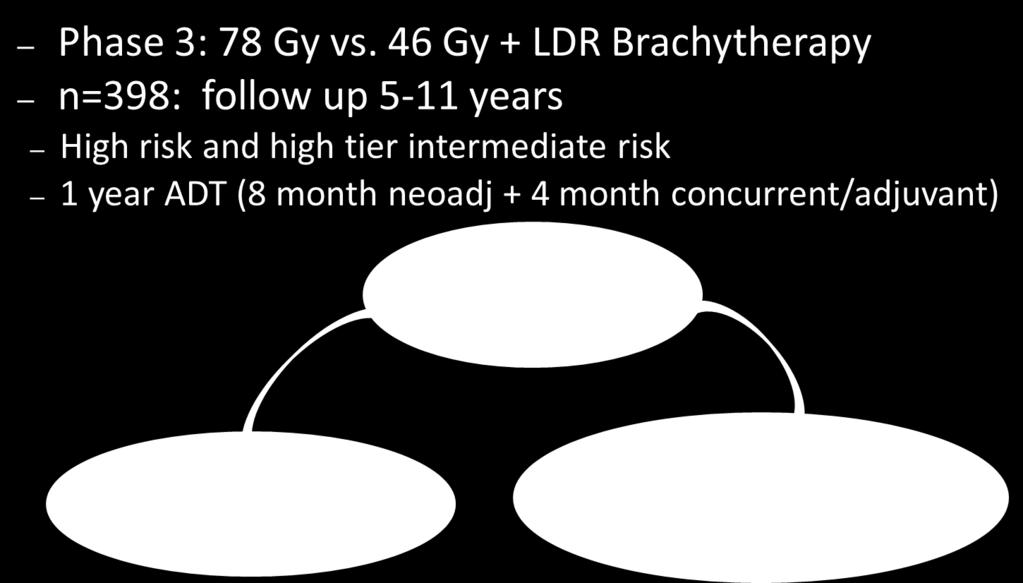
54 ASCENDE-RT Courtesy of Dr. Crook
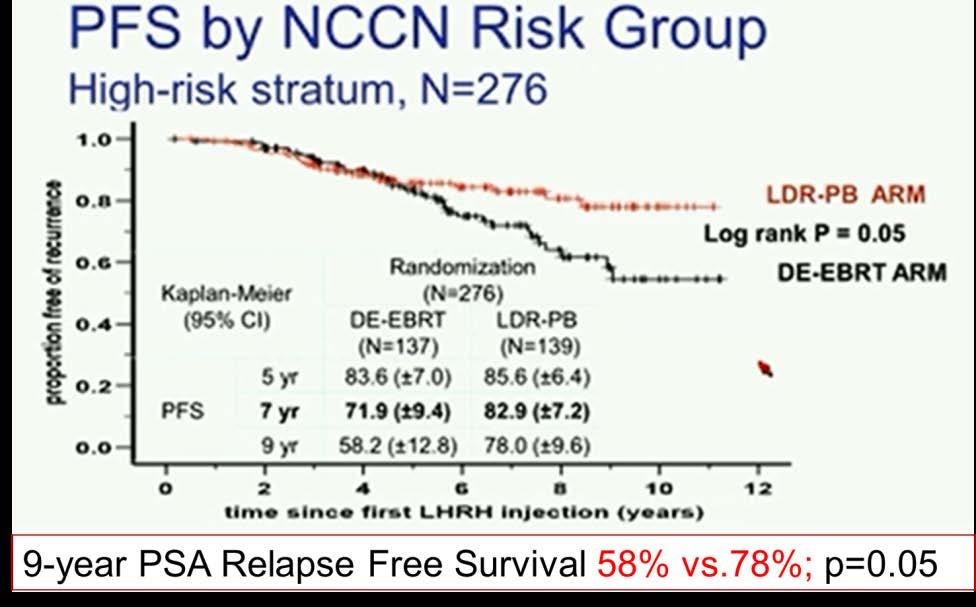
55 ASCENDE-RT: Results Morris et al., IJROBP 2017, slides courtesy of Dr. Crook

56 ASCENDE-RT Results:
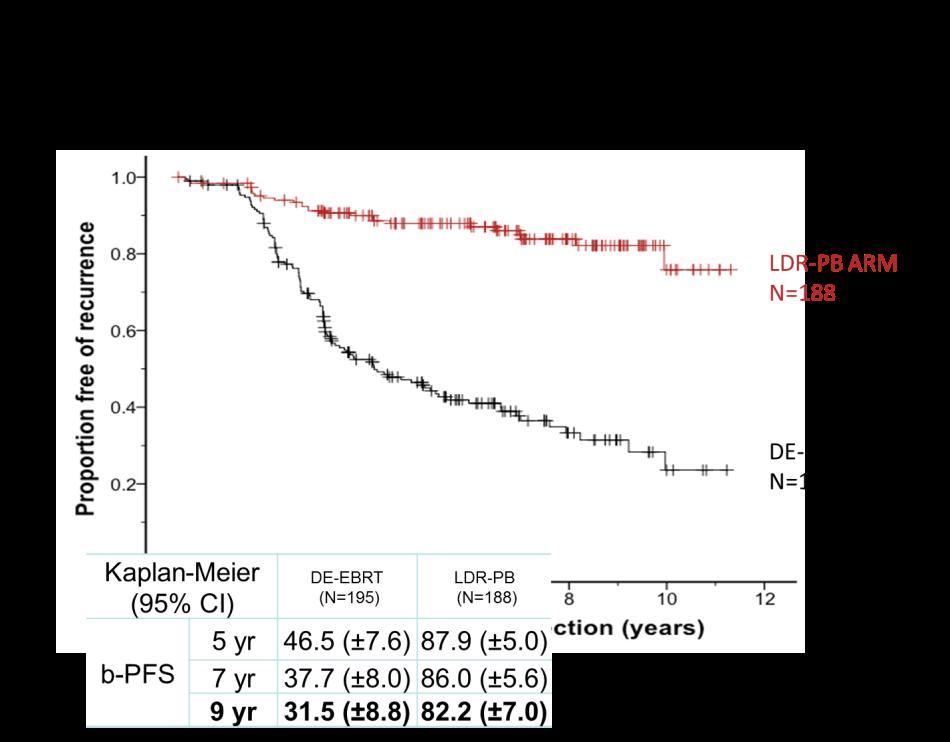
57 ASCENDE-RT Results:
58 ASCENDE-RT Toxicity: 398 pts accrued Implants by 16 radiation oncologists Prior to incorporation of MRI in QA Cumulative grade 3 GU toxicity: 19% vs. 5 years (p<0.001) 6 years persistent grade 3 GU toxicity is 6.3% Cumulative grade 3 GI toxicity: 9% vs. 4% (NS) Rodda et al., IJROBP 2017
59 ASCENDE-RT Toxicity: Rodda et al., IJROBP 2017


60 Kiri Sandler (UCLA): Survey of expert GU radiation oncologists First choice treatment for patients with high risk PCa, no baseline urinary symptoms and 40 cc gland % 50.00% 0.00% 54.80% 45.20% EBRT with ADT EBRT with ADT + Brachy boost McClelland et al., Clinical Genitourinary Cancer, in press
61 High Risk Prostate Cancer: Brachy Boost Orio et al., Brachytehrapy 2016
62 Conclusion For high risk prostate cancer brachytherapy boost improves biochemical control based on 3 randomized clinical trials There is an increased cumulative grade 3 GU toxicity Brachytherapy requires technical skills and expertise, that is declining in the United States

63 Updated Recommendations: For patients with intermediate-risk prostate cancer choosing EBRT with or without ADT, brachy boost (LDR or HDR) should be offered to eligible patients. For patients with high-risk prostate cancer receiving EBRT and ADT, brachy boost (LDR or HDR) should be offered to eligible patients
64 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters
65 ADT with EBRT Low Risk: EBRT alone* Intermediate Risk: EBRT +/- 4-6 months of ADT High Risk: EBRT + 24 months of ADT *If discussing comparable outcomes between surgery and EBRT in ProtecT trial, may have to incorporate 3-6 months of ADT.
66 ADT with EBRT Low Risk: EBRT alone* Intermediate Risk: EBRT +/- 4-6 months of ADT High Risk: EBRT + 24 months of ADT *If discussing comparable outcomes between surgery and EBRT in ProtecT trial, may have to incorporate 3-6 months of ADT.

67 ADT in intermediate risk PCa Zumsteg and Zelefsky, Lancet Oncology 2012


68 ADT in intermediate risk PCa Castle et al., IJROBP 2012


69 ADT in intermediate risk PCa PSA relapse-free survival ahr Zumsteg et al., IJROBP 2012

70 ADT in intermediate risk PCa Zumsteg and Zelefky, JCO 2012
71 ADT in intermediate risk PCa Dong et al., Can J Urol 2017
72 ADT in intermediate risk PCa GETUG 14 Abstract (Dubray et al) at ASCO 2016: 80 Gy +/- 4 months of ADT Median followup of 84 months (range, 3-132) Biochemical relapse-free survival: 76% vs 84% at 5 years (p=0.02)
73 ADT in intermediate risk PCa RTOG 9910: 70.2 Gy 4 vs 9 months of ADT 85% with intermediate risk No difference in outcomes Pisansky et al., JCO 2014
74 ADT in intermediate PCa NCDB analysis: Favorable intermediate RT 75.6 Gy+ or with brachy boost : 18,598 patients Use of ADT decreased from 44% in 2004 to 40% in 2007 ADT not associated with improved survival Falchook et al., Cancer 2016
75 ADT with EBRT Low Risk: EBRT alone* Intermediate Risk: EBRT +/- 4-6 months of ADT High Risk: EBRT + 24 months of ADT *If discussing comparable outcomes between surgery and EBRT in ProtecT trial, may have to incorporate 3-6 months of ADT.
76 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters

77 Post-prostatectomy EBRT: adjuvant or salvage? Pooled analysis with propensity score matching: 10 academic US centers 1566 consecutive patients Median followup after RT: 5 years
78 Post-prostatectomy EBRT: adjuvant or salvage? 1. Persistently elevated PSA after surgery = ESRT 2. Sensitivity analysis revealed that decreased risk of BF associated with ART lost SS when more than 56% in the ART cohort were assumed to have been cured by surgery alone Hwang et al., JAMA Onc Published online 1/25/2018
79 Post-prostatectomy EBRT: adjuvant or salvage? SWOG 8794 (Thompson et al., J Urol 2009) No restriction on PSA level at enrollment Relationship between pre-rt PSA level and risk of metastases development: 0.2 ng/ml vs 0.2 to 1.0 ng/ml Local recurrence: 22% in observation vs 8% in adjuvant RT EORTC (Bolla et al., Lancet 2012) Undetectable PSA defined as 0.4 ng/ml Salvage pelvic RT administered to 54% of patients on observation arm with biochemical progression ARO 96/02 (Wiegel et al., JCO 2009) Only PSA < 0.1 ng/ml Salvage RT strongly recommended in observation arm as soon as PSA became detectable, no information provided on the rate of salvage RT
80 Post-prostatectomy EBRT: adjuvant or salvage? Herrera and Berthold, Frontiers in Oncology 2016
81 Margin Status for Adjuvant RT ARO 96/02 (Wiegel, European Urology 2014) EORTC (Van der Kwast, JCO 2007)
82 Salvage RT: outcomes Herrera and Berthold, Frontiers in Oncology 2016

83 Stephenson et al., JCO 2007
84 The role of ADT with Salvage RT GETUG-AFU (Carrie et al., Lancet 2016) 66 Gy in 33 fractions +/- 6 months of ADT (goserelin) PFS at 5 years: 80% vs 62% (HR 0.5, p< ) No difference in overall survival RTOG 9601 (Shipley et al., NEJM 2017): 64.8 Gy in 36 fractions +/- 2 years of ADT (bicalutamide, 150 mg daily) OS at 12 years: 76.3% vs 71.3% (HR 0.77, p=0.04) No benefit for ADT in PSA < 0.7 ng/ml on post-hoc subgroup analysis
85 Salvage RT Dose SAKK 09/10 randomized trial 64 in 2 vs 70 in 2 No difference in acute toxicity: Grade 2 GU 13% vs 16.6% Grade 3 GU 0.6% vs 1.7% Grade 2 GI 16% vs 15.4% Grade 3 GI 0.6 % vs 2.3% Ghadjar et al., JCO 2015
86 Radicals
87 Kiri Sandler (UCLA) : Survey of expert GU radiation oncologists As a general rule, for patients with high risk features after radical prostatectomy, I recommend: % 50.00% 0.00% Adjuvant RT 54.80% 45.20% Early salvage RT McClelland et al., in submission
88 Conclusion All patients with high risk features after RP (+margin, pt3, persistently elevated PSA) should be seen by radiation oncologists for consultation to discuss the merits of adjuvant RT vs careful monitoring with early salvage RT in case of biochemical recurrence: 30% of patients with high risk features will not experience biochemical progression if observed OS was improved only when adjuvant RT was compared to no further RT even in case of disease progression Early salvage RT has excellent outcomes The role of ADT with EARLY salvage RT is unclear, although could be justified by RTOG 9601
89 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters
90 Pelvis: RTOG 9413 Lawton et al., IJROBP 2007
91 Pelvis: RTOG 9413 Roach et al., IJROBP 2006
92 Laparoscopic Sentinel Lymph Node Dissection in patients selected for EBRT based on cn0 99Tc-nanocolloid injected into peripheral zone each quadrant of prostate gland transrectally w/ US guidance Positive SLNs found in 42% of patients with clinically N0 PCa referred for EBRT Gleason Sum Overall (N=224) pn0 (N=133) pn1 (N=91) Grivas et al., IJROBP 2017
93 Patterns of Recurrence after EBRT to Prostate Zumsteg et al., Journal of Urology, 2015

94 Kiri Sandler (UCLA), unpublished: Survey of expert GU radiation oncologists For localized high risk PCa, I treat pelvic lymph nodes: % 31.00% 69.00% 50.00% 0.00% Rarely Often
95 LN-positive PCa 703 consecutive patients treated with RP, PLND and adjuvant treatments between 1988 and 2003 at two large academic institutions All underwent CT and bone scan prior to surgery 171 received ADT and RT 532 received ADT alone Matched analysis for effect of RT on CSS and OS (1 RT:4 no RT) Mean follow up 8.4 years HR 2.5, p=0.004 HR 2.3, p<0.001 Briganti et al., European Urology 2011

96 LN-positive PCa Lin et al., JNCI 2015
97 LN-positive PCa Mitin et al., Oncology 2013
98 LN-positive PCa
99 Conclusion The role of prophylactic RT to pelvic lymph nodes is controversial RTOG 9413: no difference in primary outcome between WP and RO Future studies with advanced imaging (PSMA or C-11 PET) and/or SLNB may select appropriate patients for prophylactic RT to pelvic lymph nodes Patients with pn+ PCa have an excellent prognosis Strong association with adjuvant RT administration
100 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters




101 Bone metastases: Radium-223 Short-range high-energy alphaemitting particle Targets osteoblastic bone metastases by acting as a calcium mimetic Perez et al. Principles and Practice of Radiation Oncology, 5th ed. 2007

102 Bone metastases: Radium-223 Lewis et al., Oncology 2015
103 Bone metastases: Radium-223 Bone pain Diarrhea Nausea Vomiting Constipation Anemia (2%) Neutropenia Timing Baseline Subsequent Thrombocytopenia (2%) Lab Values ANC 1.5 x 10^9/L Platelets 100 x 10^9/L Hgb 10 g/dl ANC 1 x 10^9/L Platelets 50 x 10^9/L
104 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters

105 Prognostic Biomarkers


106 Prognostic Biomarkers Eur Urol Focus, 2017 (epub)
107 Prognostic Biomarkers NCCN Guidelines Version Developed with extensive industry support, guidance and involvement Marketed under the less rigorous FDA regulatory pathway for biomakers Full assessment of their clinical utility requires prospective randomized clinical trials, which are unlikely to be done A bad tumor marker is as bad as a bad drug. (Dr. Hayes) The NCCN panel believes that men with clinically localized disease may consider the use of tumor-based molecular assays at this time.
108 PET Imaging

109 PET imaging Evans et al., PRO 2018
110 Outline Screening for Prostate cancer Low/intermediate risk Prostate cancer Active surveillance vs treatment Surgery vs EBRT Brachytherapy vs EBRT Hypofractionated EBRT High risk Prostate cancer Incorporation of brachytherapy boost ADT with EBRT Post-prostatectomy RT Adjuvant vs salvage Lymph-node positive Prostate cancer Role of pelvic RT Bone metastases from Prostate cancer Radium-223 systemic therapy Prognostic biomarkers/pet imaging Contours and DVH parameters


111 Anthony Zietman Anthony D Amico William Shipley Jason Efstathiou Paul Nguyen Charles R. Thomas Howard Sandler Arthur Hung Tom Beer Christopher Ryan

112 Questions:
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
External Beam Radiation Therapy for Low/Intermediate Risk Prostate Cancer
 External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
External Beam Therapy for Low/Intermediate Risk Prostate Cancer Jeff Michalski, M.D. The Carlos A. Perez Distinguished Professor of Department of and Siteman Cancer Center Learning Objectives Understand
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
External Beam Radiotherapy for Prostate Cancer
 External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
External Beam Radiotherapy for Prostate Cancer Chomporn Sitathanee, Radiation Oncology Unit Ramathibodi Hospital, Mahidol University Roles of RT in prostate cancer Definitive RT; intact prostate Post radical
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
An Update on Radiation Therapy for Prostate Cancer
 An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
An Update on Radiation Therapy for Prostate Cancer David C. Beyer, MD, FACR, FACRO, FASTRO Arizona Oncology Services Phoenix, Arizona Objectives Review significant new data Identify leading trends in PCa
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
3/22/2014. Goals of this Presentation: in 15 min & 5 min Q & A. Radiotherapy for. Localized Prostate Cancer: What is New in 2014?
 3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
3/22/ Goals of this Presentation: in 15 min & 5 min Q & A 1. Potency Preservation. a. Dosimetric considerations Radiotherapy for b. Drugs 2. Update on duration of short term ADT Mack III, MD Professor
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924
 EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
EORTC radiation Oncology Group Intergroup collaboration with RTOG EORTC 1331-ROG; RTOG 0924 Title of the Study Medical Condition Androgen deprivation therapy and high dose radiotherapy with or without
2/14/09. Why Discuss this topic? Managing Local Recurrences after Radiation Failure. PROSTATE CANCER Second Treatment
 Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
Why Discuss this topic? Mack Roach III, MD Professor and Chair Radiation Oncology UCSF Managing Local Recurrences after Radiation Failure 1. ~15 to 75% of CaP pts recur after definitive RT. 2. Heterogeneous
SRO Tutorial: Prostate Cancer Clinics
 SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
SRO Tutorial: Prostate Cancer Clinics May 7th, 2010 Daniel M. Aebersold Klinik und Poliklinik für Radio-Onkologie Universität Bern, Inselspital Is cure necessary in those in whom it may be possible, and
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER
 PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
PROSTATE CANCER, Radiotherapy ADVANCES in RADIOTHERAPY for PROSTATE CANCER Alberto Bossi Radiotherapy and Oncology Gustave Roussy, Villejuif, France PROSTATE CANCER, Radiotherapy IGRT RT + ADT: short vs
PORT after RP. Adjuvant. Salvage
 PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
When radical prostatectomy is not enough: The evolving role of postoperative
 When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer
 Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer Daisaku Hirano, MD Department of Urology Higashi- matsuyama Municipal Hospital, Higashi- matsuyama- city, Saitama- prefecture,
Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer Daisaku Hirano, MD Department of Urology Higashi- matsuyama Municipal Hospital, Higashi- matsuyama- city, Saitama- prefecture,
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy. Dr. Matt Andrews Supervisor: Dr. David Bowes
 The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps?
 Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Managing Prostate Cancer After Initital Treatment Fails: Are There Good Next Steps? Michael J Zelefsky, M.D. Professor of Radiation Oncology Chief Brachytherapy Service Department of Radiation Oncology
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017
 Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017 Relevant Disclosures Advisory role, ownership interest, previous unrestricted grant
Prostate Cancer Genomics When To Treat and With What? Ashley E. Ross, M.D., Ph.D. Texas Urology Specialists August 2017 Relevant Disclosures Advisory role, ownership interest, previous unrestricted grant
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate cancer: Update from the BCCA
 Prostate cancer: Update from the BCCA Tom Pickles Clinical Professor, UBC Topics 1. Incidence & Utilization rates 2. New developments with External Beam RT IGRT, VMAT and other enhancements Optimizing
Prostate cancer: Update from the BCCA Tom Pickles Clinical Professor, UBC Topics 1. Incidence & Utilization rates 2. New developments with External Beam RT IGRT, VMAT and other enhancements Optimizing
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD
 Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
Hypofractionation for Prostate Cancer: the Present Luca Incrocci, MD PhD Professor of Genito-Urinary Radiotherapy Erasmus MC Cancer Institute Rotterdam, The Netherlands Themadag Prostaatcarcinoom 15 maart
CyberKnife SBRT for Prostate Cancer
 CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
CyberKnife SBRT for Prostate Cancer Robert Meier, MD Swedish Radiosurgery Center Swedish Cancer Institute Seattle, WA 2017 ESTRO Meeting, Vienna Austria 5-year safety, efficacy & quality of life outcomes
Salvage HDR Brachytherapy. Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK
 Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Salvage HDR Brachytherapy Amit Bahl Consultant Clinical Oncologist The Bristol Cancer Institute, UK Disclosures Still No financial disclosures! Limited personal experience of HDR Brachy as salvage option
Future Directions in Prostate Cancer: The Case for Protons. John J. Coen, MD Helen & Harry Gray Cancer Center
 Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Radiation Therapy for Prostate Cancer. Resident Dept of Urology General Surgery Grand Round November 24, 2008
 Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Embracing Technology & Timing of Salvage Hormones
 Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
PSA nadir post LDR Brachytherapy and early Salvage Therapy. Dr Duncan McLaren UK & Ireland Users Group Meeting 2016
 PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
PSA nadir post LDR Brachytherapy and early Salvage Therapy Dr Duncan McLaren UK & Ireland Users Group Meeting 2016 Differences in PSA relapse rates based on definition used PSA ng/ml Recurrence ASTRO Recurrence
Timing of Androgen Deprivation: The Modern Debate Must be conducted in the following Contexts: 1. Clinical States Model
 Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
The Rise, Fall, and Rise Again of Proton Therapy or Never count out a well-financed therapy
 The Rise, Fall, and Rise Again of Proton Therapy or Never count out a well-financed therapy Anthony Zietman MD Shipley Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School
The Rise, Fall, and Rise Again of Proton Therapy or Never count out a well-financed therapy Anthony Zietman MD Shipley Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy?
 Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Would SBRT Hypofractionated Approach Be as Good? Then Why Bother With Brachytherapy? Yasuo Yoshioka, MD Department of Radiation Oncology Osaka University Graduate School of Medicine Osaka, Japan Disclosure
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Prostate Cancer: from Beginning to End
 Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
10th anniversary of 1st validated CaPspecific
 Quality of Life after Treatment of Localised Prostate Cancer Dr Jeremy Grummet Clinical Uro-Oncology Fellow May 28, 2008 1 Why? This is important May be viewed as soft science Until we know which treatment
Quality of Life after Treatment of Localised Prostate Cancer Dr Jeremy Grummet Clinical Uro-Oncology Fellow May 28, 2008 1 Why? This is important May be viewed as soft science Until we know which treatment
Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK
 Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Lead Group Log Radiotherapy & Cervical Cancer Dr Mary McCormack Consultant Clinical Oncologist University College Hospital, London,UK Cervical Cancer treatment Treatment planning should be made on a multidisciplinary
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE
 CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
CYBERKNIFE SBRT FOR THE TREATMENT OF PROSTATE CANCER: 5 VS. 44 FRACTIONS THE PHILADELPHIA CYBERKNIFE CENTER EXPERIENCE Olusola Obayomi-Davies M.D. Philadelphia CyberKnife Center September 26 th, 2017 Disclosure
D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy combined HDR + EBRT 574 HDR monotherapy Total Patients
 Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Salvage Prostate Brachytherapy D. Jeffrey Demanes M.D. FACRO, FACR, FASTRO Director UCLA Brachytherapy 1996-2013 1515 combined HDR + EBRT 574 HDR monotherapy 36 Salvage 2125 Total Patients No Disclosure
Radioligand imaging & treatment of prostate cancer
 Radioligand imaging & treatment of prostate cancer Christiaan Schiepers, MD, PhD University of California Los Angeles CANM-CAMRT JOINT ANNUAL CONFERENCE MARCH 22-24, 2018 VANCOUVER, B.C. I do not have
Radioligand imaging & treatment of prostate cancer Christiaan Schiepers, MD, PhD University of California Los Angeles CANM-CAMRT JOINT ANNUAL CONFERENCE MARCH 22-24, 2018 VANCOUVER, B.C. I do not have
Prostate Cancer in comparison to Radiotherapy alone:
 Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
 Measure #104 (NQF 0390): Prostate Cancer: Adjuvant Hormonal Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL
Measure #104 (NQF 0390): Prostate Cancer: Adjuvant Hormonal Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL
Controversies in Prostate Cancer Screening
 Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Controversies in Prostate Cancer Screening William J Catalona, MD Northwestern University Chicago Disclosure: Beckman Coulter, a manufacturer of PSA assays, provides research support PSA Screening Recommendations
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
Prostate Cancer. 3DCRT vs IMRT : Hasan Murshed
 Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Prostate Cancer 3DCRT vs IMRT : the second debate Hasan Murshed Take home message IMRT allows dose escalation. Preliminary data shows IMRT technique improves cancer control while keeping acceptable morbidity
Radical Prostatectomy:
 Overtreatment and undertreatment Radical Prostatectomy: An Emerging Standard of Care for High Risk Prostate Cancer Matthew R. Cooperberg, MD,MPH UCSF Radiation Oncology Update San Francisco, CA April 2,
Overtreatment and undertreatment Radical Prostatectomy: An Emerging Standard of Care for High Risk Prostate Cancer Matthew R. Cooperberg, MD,MPH UCSF Radiation Oncology Update San Francisco, CA April 2,
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015
 Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
Pre-test. Prostate Cancer The Good News: Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest
 Pre-test Matthew R. Cooperberg, MD, MPH UCSF 40 th Annual Advances in Internal Medicine Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest 1. I do not offer routine PSA screening, and
Pre-test Matthew R. Cooperberg, MD, MPH UCSF 40 th Annual Advances in Internal Medicine Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest 1. I do not offer routine PSA screening, and
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
IMRT RTOG Definitive IMRT for Low Risk Prostate Cancer. All about dose and dose matters, probably Although hormones may matter
 Definitive for Low Risk Prostate Cancer Howard Sandler, MD, MS Bloom Family Chair in Cancer Therapeutics Cedar-Sinai Medical Center All about dose and dose matters, probably Although hormones may matter
Definitive for Low Risk Prostate Cancer Howard Sandler, MD, MS Bloom Family Chair in Cancer Therapeutics Cedar-Sinai Medical Center All about dose and dose matters, probably Although hormones may matter
Where are we with PSA screening?
 Where are we with PSA screening? Faculty/Presenter Disclosure Rela%onships with commercial interests: None Disclosure of Commercial Support This program has received no financial support. This program
Where are we with PSA screening? Faculty/Presenter Disclosure Rela%onships with commercial interests: None Disclosure of Commercial Support This program has received no financial support. This program
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE. ELENA CASTRO Spanish National Cancer Research Centre
 VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Navigating the Stream: Prostate Cancer and Early Detection. Ifeanyi Ani, M.D. TPMG Urology Newport News
 Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
How can we Personalize RT as part of Breast-Conserving Therapy?
 How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
How can we Personalize RT as part of Breast-Conserving Therapy? Jay R. Harris Dana-Farber Cancer Institute (DFCI) Brigham and Women s Hospital (BWH) Harvard Medical School Disclosures I have no COI disclosures
Prostate Cancer Incidence
 Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Neoplasie prostatiche Radioterapia: le nuove strategie
 Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
Neoplasie prostatiche Radioterapia: le nuove strategie Dr. PL Losardo U.O.C di Radioterapia Azienda Ospedaliero-Universitaria di Parma Parma, 19.5.2015 VS Very Low risk Low risk Intermediate risk High
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer
 Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer 100 80 60 Cancer Death Rates for Men, US 1930-2002 Rate Per 100,000 Lung William K. Oh, M.D. 40 Stomach Colon & rectum Prostate
Rationale for Multimodality Therapy for High Risk Localized Prostate Cancer 100 80 60 Cancer Death Rates for Men, US 1930-2002 Rate Per 100,000 Lung William K. Oh, M.D. 40 Stomach Colon & rectum Prostate
New Technologies for the Radiotherapy of Prostate Cancer
 Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Prostate Cancer Meyer JL (ed): IMRT, IGRT, SBRT Advances in the Treatment Planning and Delivery of Radiotherapy. Front Radiat Ther Oncol. Basel, Karger, 27, vol. 4, pp 315 337 New Technologies for the
Brachytherapy for Prostate Cancer
 Brachytherapy for Prostate Cancer Who should be thinking about this and why... Juanita Crook Professor Radiation Oncology University of Toronto Princess Margaret Hospital Many options watchful waiting?
Brachytherapy for Prostate Cancer Who should be thinking about this and why... Juanita Crook Professor Radiation Oncology University of Toronto Princess Margaret Hospital Many options watchful waiting?
Tanaka et al. BMC Cancer (2017) 17:573 DOI /s
 17:573 DOI /s") Tanaka et al. BMC Cancer (2017) 17:573 DOI 10.1186/s12885-017-3565-1 RESEARCH ARTICLE Comparison of PSA value at last follow-up of patients who underwent low-dose rate brachytherapy and intensity-modulated
Tanaka et al. BMC Cancer (2017) 17:573 DOI 10.1186/s12885-017-3565-1 RESEARCH ARTICLE Comparison of PSA value at last follow-up of patients who underwent low-dose rate brachytherapy and intensity-modulated
IN RADIOTERAPIA BEST PAPERS. Direttore Unità Operativa Complessa Radioterapia Oncologica
 IN RADIOTERAPIA BEST PAPERS 2014 FILIPPO ALONGI Direttore Unità Operativa Complessa Radioterapia Oncologica PROSTATE RT: WHERE WE ARE GOING? RT has evolved from radium(1911) to high Technology and high
IN RADIOTERAPIA BEST PAPERS 2014 FILIPPO ALONGI Direttore Unità Operativa Complessa Radioterapia Oncologica PROSTATE RT: WHERE WE ARE GOING? RT has evolved from radium(1911) to high Technology and high
GRANDANGOLO: CA PROSTATA
 GRANDANGOLO: CA PROSTATA AIRO 2014, Padova Alessio G. Morganti RT dose-effect Creak A et al. Br J Cancer 2013! randomized study:! 126 patients! med. FUP: 13.7 years! T1b-T3b! neoadjuv. ADT + 3D-RT! 64
GRANDANGOLO: CA PROSTATA AIRO 2014, Padova Alessio G. Morganti RT dose-effect Creak A et al. Br J Cancer 2013! randomized study:! 126 patients! med. FUP: 13.7 years! T1b-T3b! neoadjuv. ADT + 3D-RT! 64
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
Oligometastasis. Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie?
 Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
PROSTATE CANCER BRACHYTHERAPY. Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College
 PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
PROSTATE CANCER BRACHYTHERAPY Kazi S. Manir MD,DNB,PDCR RMO cum Clinical Tutor Department of Radiotherapy R. G. Kar Medical College Risk categorization Very Low Risk Low Risk Intermediate Risk High Risk
HDR vs. LDR Is One Better Than The Other?
 HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
HDR vs. LDR Is One Better Than The Other? Daniel Fernandez, MD, PhD 11/3/2017 New Frontiers in Urologic Oncology Learning Objectives Indications for prostate brachytherapy Identify pros/cons of HDR vs
ARRO-Case Postoperative Radiotherapy in Prostate Cancer
 ARRO-Case Postoperative Radiotherapy in Prostate Cancer Kara Downs Romano, Daniel Trifiletti, Timothy Showalter Radiation Oncology University of Virginia Charlottesville, VA Case: HPI 64 year old man with
ARRO-Case Postoperative Radiotherapy in Prostate Cancer Kara Downs Romano, Daniel Trifiletti, Timothy Showalter Radiation Oncology University of Virginia Charlottesville, VA Case: HPI 64 year old man with
Focal Therapy is a Fool s Paradise : The whole prostate must be treated!
 Focal Therapy is a Fool s Paradise : The whole prostate must be treated! Ofer Yossepowitch, MD Head, Department of Urology Tel Aviv Sourasky Medical Center Preaching against focal therapy in a focal therapy
Focal Therapy is a Fool s Paradise : The whole prostate must be treated! Ofer Yossepowitch, MD Head, Department of Urology Tel Aviv Sourasky Medical Center Preaching against focal therapy in a focal therapy
The benefit of a preplanning procedure - view from oncologist. Dorota Kazberuk November, 2014 Otwock
 The benefit of a preplanning procedure - view from oncologist Dorota Kazberuk 21-22 November, 2014 Otwock Brachytherapy is supreme tool in prostate cancer management with a wide range of options in every
The benefit of a preplanning procedure - view from oncologist Dorota Kazberuk 21-22 November, 2014 Otwock Brachytherapy is supreme tool in prostate cancer management with a wide range of options in every
The Spa Hotel, Tunbridge Wells Friday 23 rd March Platinum sponsor
 The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
High-Risk Prostate Cancer: Local Therapy Matters
 prostate cancer High-Risk Prostate Cancer: Local Therapy Matters Adam L. Liss, MD, and Daniel A. Hamstra, MD, PhD The second in a series of two articles on radiation and prostate cancer. See the May issue
prostate cancer High-Risk Prostate Cancer: Local Therapy Matters Adam L. Liss, MD, and Daniel A. Hamstra, MD, PhD The second in a series of two articles on radiation and prostate cancer. See the May issue
Sommerakademie Munich, June
 Active surveillance: Shrinking the grey zone Sommerakademie Munich, June 30 2016 Active surveillance Overview of 20 year history Laurence Klotz, MD, CM Professor of Surgery Sunnybrook Heatlh Sciences Centre
Active surveillance: Shrinking the grey zone Sommerakademie Munich, June 30 2016 Active surveillance Overview of 20 year history Laurence Klotz, MD, CM Professor of Surgery Sunnybrook Heatlh Sciences Centre
Prostate Cancer Local or distant recurrence?
 Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
How to deal with patients who fail intracavitary treatment
 How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
How to deal with patients who fail intracavitary treatment A. Heidenreich Department of Urology Non-surgical therapy of PCA IMRT SEEDS IGRT HDR-BRACHY HIFU CRYO LDR - Brachytherapy Author Follow-up bned
Intensity Modulated Radiotherapy (IMRT) of the Prostate
 of the Prostate") Medical Policy Manual Medicine, Policy No. 137 Intensity Modulated Radiotherapy (IMRT) of the Prostate Next Review: August 2018 Last Review: November 2017 Effective: December 1, 2017 IMPORTANT REMINDER
Medical Policy Manual Medicine, Policy No. 137 Intensity Modulated Radiotherapy (IMRT) of the Prostate Next Review: August 2018 Last Review: November 2017 Effective: December 1, 2017 IMPORTANT REMINDER
American Urological Association (AUA) Guideline
 Guideline") 1 (AUA) Guideline Approved by the AUA Board of Directors April 2013 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2013 by the American
1 (AUA) Guideline Approved by the AUA Board of Directors April 2013 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2013 by the American
Systematic Review of Brachytherapy & Proton Beam Therapy for Low-Risk Prostate Cancer: Preliminary Findings
 Systematic Review of Brachytherapy & Proton Beam Therapy for Low-Risk Prostate Cancer: Preliminary Findings May 28, 2008 Dan Ollendorf, MPH, ARM Chief Review Officer Systematic Review Objectives To compare
Systematic Review of Brachytherapy & Proton Beam Therapy for Low-Risk Prostate Cancer: Preliminary Findings May 28, 2008 Dan Ollendorf, MPH, ARM Chief Review Officer Systematic Review Objectives To compare
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Erectile Dysfunction (ED) after Radiotherapy (RT) for Prostate Cancer. William M. Mendenhall, MD
 after Radiotherapy (RT) for Prostate Cancer. William M. Mendenhall, MD") Erectile Dysfunction (ED) after Radiotherapy (RT) for Prostate Cancer William M. Mendenhall, MD Meta-Analysis of Probability of Maintaining Erectile Function after Treatment of Localized Cancer Treatment
Erectile Dysfunction (ED) after Radiotherapy (RT) for Prostate Cancer William M. Mendenhall, MD Meta-Analysis of Probability of Maintaining Erectile Function after Treatment of Localized Cancer Treatment
2015 myresearch Science Internship Program: Applied Medicine. Civic Education Office of Government and Community Relations
 2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes