This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository:
|
|
|
- Henry Gaines
- 5 years ago
- Views:
Transcription

1 This is an Open Access document downloaded from ORCA, Cardiff University's institutional repository: This is the author s version of a work that was submitted to / accepted for publication. Citation for final published version: Abraham, Jacinta and Staffurth, John Nicholas Hormonal therapy for cancer. Medicine 44 (1), pp /j.mpmed file Publishers page: < Please note: Changes made as a result of publishing processes such as copy-editing, formatting and page numbers may not be reflected in this version. For the definitive version of this publication, please refer to the published source. You are advised to consult the publisher s version if you wish to cite this paper. This version is being made available in accordance with publisher policies. See for usage policies. Copyright and moral rights for publications made available in ORCA are retained by the copyright holders.
2 Hormonal therapy for cancer Jacinta Abraham John Staffurth Jacinta Abraham BMedSci BMBS MRCP FRCR is a Consultant Clinical Oncologist and the Clinical Director at Velindre Cancer Centre, Cardiff, UK. She qualified from Nottingham Medical School in She specializes in breast cancer and has research interests in bisphosphonates, infertility in cancer and secondary breast cancer. Competing interests: none declared. John Staffurth MBBS MD MRCP FRCR is a Clinical Reader in Oncology at Cardiff University, and a Consultant Clinical Oncologist at Velindre Cancer Centre, Cardiff, UK. He qualified from Guy's Hospital, London University, UK in His research interests include prostate and bladder cancer, and radiotherapy. Competing interests: none declared. Abstract Hormone therapy is an effective and non-toxic therapy for oestrogen and progesterone receptor-positive breast cancer and prostate cancer. Serum levels of oestradiol and testosterone are controlled by the hypothalamic pituitary gonadal pathway. Oestradiol is produced in premenopausal women from the ovaries and in postmenopausal women by peripheral conversion of adrenal androgens by aromatase. In premenopausal women with breast cancer and men with prostate cancer, treatment is primarily achieved by castration. In postmenopausal women selective oestrogen receptor modulators (e.g. tamoxifen) or aromatase inhibitors are used. Hormone therapy can be used to reduce the size of the primary cancer prior to radical surgery or radiotherapy or to reduce the risk of recurrence. Hormone therapy is highly effective in patients with locally advanced or metastatic disease, with a high response rate. Most patients eventually relapse with castrate-refractory disease, for which increasing numbers of active agents are entering clinical practice. Keywords: Androgen deprivation therapy; anti-androgens; aromatase inhibitors; breast cancer; hormone therapy; prostate cancer; selective oestrogen receptor modulators Aetiology This paper will concentrate on the management of breast and prostate cancers in which the impact of hormone therapy is most clinically significant. Increased exposure to endogenous or exogenous oestrogens may be linked to the development of breast cancer (Table 1). However, there is no evidence that exposure to androgens is important in the development of prostate cancer. Historical evidence In 1896 Beatson demonstrated that surgical oophorectomy resulted in tumour regression in premenopausal women with metastatic breast cancer. Charles Huggins was awarded the Nobel Prize for medicine in 1966 following his discovery that surgical orchidectomy was a successful treatment for metastatic prostate cancer.
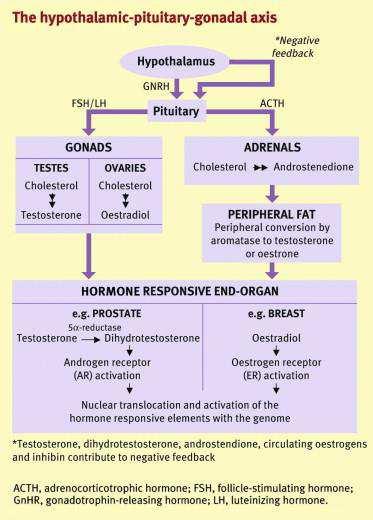
3 Hormone synthesis Oestrogen is synthesized from cholesterol in the parafollicular ovaries in premenopausal women via the hypothalamic pituitary gonadal axis (Figure 1), and in the adrenals in postmenopausal women. In premenopausal women, oestrogen production is cyclical: gonadotrophin-releasing hormone (GnRH) is released from the hypothalamus with a circadian rhythm under direct feedback by circulating hormones. GnRH reacts with anterior pituitary receptors, leading to the release of luteinizing and follicle-stimulating hormone; these stimulate the ovaries to produce oestradiol. In postmenopausal women, the main site of oestrogen synthesis is adipose tissue. Here, adrenal androgens (e.g. androstenedione) are converted from aromatase to oestrone. Oestrone is then converted to oestradiol by 17β-OH dehydrogenase. Postmenopausal synthesis varies depending on environmental and genetic factors (e.g. obesity). In men, the main circulating androgen is testosterone, 90% of which is produced by the testicular Leydig cells under control of the hypothalamic pituitary axis, as above. The remaining circulating androgens (e.g. dihydroxyandrostenedione) are produced in the adrenal cortex from cholesterol. Testosterone is metabolized by 5αreductase within the prostate to the more biologically active dihydrotestosterone, which acts as the ligand for the androgen receptor (AR). Hormone receptors In breast cancer, approximately 80% of postmenopausal women and 50% of premenopausal women have hormone receptor-positive disease. The degree of positivity is defined by the level of expression of both oestrogen (ER) and progesterone receptors, which are routinely measured immunohistochemically in newly diagnosed cases. Systemic treatment and, to some extent, prognosis is guided by hormone receptor status. In contrast, measurement of ARs is not currently routinely performed in prostate cancer it has no therapeutic or prognostic value because both hormone-dependent and castrate-refractory prostate cancers (CRPCs) possess functioning ARs. Recent work suggests that AR variants may underlie resistance to castration. 1 Hormone therapy in breast cancer Ovarian ablation In premenopausal women oestrogen suppression is achieved by chemical ablation, radiation to the ovaries or surgical oophorectomy. Chemical ablation is reversible and achieved by using a GnRH agonist (GnRHa or LHRHa) such as goserelin, usually as a monthly depot injection. Other hormonal agents in breast cancer An increasing number of hormonal treatment options are available to treat breast cancer. A description of the different licensed drugs is given in Table 2. The most commonly used treatments include tamoxifen and aromatase inhibitors (AIs). Tamoxifen: this is a selective oestrogen receptor modulator with complex actions on ERs, acting predominantly as an antagonist, with a weak agonist effects. In ER-positive early breast cancer, 5 years of tamoxifen after surgery reduces the annual recurrence rate by 41% and annual mortality rate by 34%. 2 There is evidence of a reduction in breast cancer recurrence and mortality by continuing tamoxifen in ER-positive disease for 10 years rather than stopping at 5 years. 3 Tamoxifen may be used in premenopausal and postmenopausal women. The main adverse effects are hot flushes, night sweats and vaginal discharge. There is an increased risk of thrombotic events. Vaginal bleeding should be promptly evaluated because of the increased risk of endometrial cancer. 4
4 Aromatase inhibitors: several Phase III clinical trials have established third-generation AIs as the new gold standard in the adjuvant hormonal treatment of receptor-positive early breast cancer. They are contraindicated in premenopausal women unless ovarian suppression has been induced. There are three main approaches with early breast cancer: up-front use for 5 years planned or unplanned switching, i.e. use of AIs for 2 3 years after 2 3 years of tamoxifen extended therapy, i.e. after 5 years use of tamoxifen. The main toxicities of AIs are hot flushes, arthralgia, reduced bone mineral density and increased risk of fractures. Women at risk of osteoporosis should be carefully monitored or treated with bisphosphonates where necessary. 5 A new approach is the use of AIs in combination with signal transduction or pathway inhibitors. Everolimus is an mtor inhibitor licensed for use in combination with exemestane in the metastatic setting. 6 Main indications for hormonal therapy in breast cancer As a neoadjuvant to reduce the size of the primary tumour, making it operable or reducing the extent of surgery, for example from mastectomy to wide local excision As an adjuvant after surgery to reduce the risk of recurrence and improve survival As a palliative treatment to shrink and control large inoperable cancers As a palliative treatment for metastatic disease to prolong and improve quality of life. Hormone therapy in prostate cancer Androgen deprivation therapy (ADT) Serum testosterone is reduced to castrate levels by surgical or chemical castration, using LHRHa or the newer LHRH antagonists. Castration can lead to hot flushes, sweats and reduced libido. Patients may notice reduced muscle mass, reduced strength and weight gain. There can be loss of bone mineral density and there are concerns of an increased risk of fatal cardiac events. Initial use of LHRHa results in a surge in serum testosterone, which may worsen symptoms: all patients should take oral antiandrogens for at least 3 weeks, starting 1 2 weeks prior to initial LHRHa injection. This is not needed with LHRH antagonists, which are preferred in emergency situations. Other hormonal agents in prostate cancer The hormonal agents commonly used in the management of CRPC are described in Table 3. Bicalutamide is a non-steroidal antiandrogen and competitive AR inhibitor that is often used as the initial agent for CRPC, with a response rate up to 66%. Singleagent bicalutamide (at a dose of 150 mg daily) can be used as an alternative to ADT in some clinical situations. There is a lower incidence of erectile dysfunction but equivalent efficacy has not been proven. Degarelix is an LHRH antagonist and does not cause a testosterone flare. It rapidly achieves castrate levels of testosterone and can be used in emergency situations such as new diagnoses presenting with cord compression. Abiraterone acetate and enzalutamide are newer agents causing much greater AR suppression, through different mechanisms; they have been shown to prolong survival both before and after docetaxel chemotherapy. 7 10
5 Corticosteroids are highly active in CRPC but have no proven survival advantage. Long-term use is associated with typical glucocorticoid adverse effects, such as proximal myopathy and reduced bone mineral density, and patients require regular review. Main indications for hormonal treatment in prostate cancer As a neoadjuvant prior to radiotherapy to improve local and biochemical (prostate-specific antigen) control in patients with locally advanced tumours As an adjuvant following radiotherapy to improve overall survival in high-risk disease Palliatively for metastatic or recurrent prostate cancer. Almost 100% of patients respond, with a median duration of response of 12 months. Hormone resistance Resistance develops in nearly all patients with metastatic breast and prostate cancer who initially respond to hormone therapy, resulting in disease progression. The molecular causes of resistance are complex, varied and not well understood. Mechanisms may include increased sensitivity of hormone receptors, pathway activation without exposure to hormones (constitutive activation) or up-regulated downstream survival pathways. As these become better characterized, new agents can be developed and trialled.
6 Table 1 Hormonal risks for breast cancer Risk factors Early menarche Late menopause Nulliparity Obesity Hormone replacement therapy Protective factors Breast-feeding Young age at full-term pregnancy
7 Table 2 Hormonal therapies in breast cancer Drug Type Dose/route Mode of action Tamoxifen Anti-oestrogen 20 mg daily p.o. Competes with oestradiol for ER binding Anastrozole Non-steroidal aromatase inhibitor 1 mg daily p.o. Competitive aromatase inhibition Letrozole Non-steroidal aromatase inhibitor 2.5 mg daily p.o. Competitive aromatase inhibition Exemestane Steroidal aromatase inhibitor 25 mg daily p.o. Irreversible aromatase inhibition Fulvestrant Oestrogen receptor antagonist 250 mg monthly i.m. Down-regulation of the ER protein Megestrol acetate Progestin mg daily p.o. Cellular action not fully understood Down-regulation of ovarian steroidogenesis ER, oestrogen receptor; i.m., intramuscular; p.o., oral.
8 Table 3 Hormonal therapies in prostate cancer Drug Type Dose/route Mode of action Goserelin LHRH agonist 3.6 mg every 28 days or 10.8 mg every 3 months s.c. Reduced pituitary production of LH and FSH Leuprorelin LHRH agonist 3.75 mg every 28 days or mg every 3 months Reduced pituitary production of LH and FSH s.c./i.m. Degarelix LHRH antagonist 240 mg then 80 mg every 28 days s.c. Reduced pituitary production of LH and FSH Bicalutamide 50 mg (combination dose) or 150 mg (single agent) daily Non-steroidal antiandrogen Competitive AR inhibition p.o. Prednisolone Corticosteroid 5 10 mg daily p.o. Adrenal suppression Dexamethasone Corticosteroid mg daily p.o. Adrenal suppression Abiraterone acetate Androgen synthesis 1000 mg daily p.o. with prednisolone 5 mg twice daily Reduced androgen production within inhibitor p.o. adrenal glands and prostate cancer cells Enzalutamide AR inhibitor 160 mg daily p.o. Competitive AR inhibition, block of AR translocation to the nucleus AR, androgen receptor; FSH, follicle-stimulating hormone; i.m., intramuscular; LH, luteinizing hormone; LHRH, luteinizing hormone-releasing hormone; p.o., oral; s.c., subcutaneous.
9 Figure 1
10 References 1 Antonarakis ES, Lu C, Wang H, et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N Engl J Med. 2014; 371: Early Breast Cancer Trialists Collaborative Group (EBCTC G). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet 2005; 365: Davies C, Pan H, Godwin, et al; Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) Collaborative Group. Long term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor positive breast cancer: ATLAS, a randomised trial. Lancet 2012; 381: Saadat M, Truong PT, Kader HA, et al. Outcomes in patients with primary breast cancer and a subsequent diagnosis of endometrial cancer: comparison of cohorts treated with and without tamoxifen. Cancer 2007; 110: Royal College of Physicians, the Bone and Tooth Society, the National Osteoporosis Society. Glucocorticoid-induced osteoporosis: guidelines for prevention and treatment. London: RCP, Baselga J, Campone M, Piccart M, et al. Everolimus in postmenopausal hormone-receptor-positive advanced breast cancer. N Engl J Med 2012, 366: Fizazi K, Scher HI, Molina A, et al.; COU-AA-301 Investigators. Abiraterone acetate for treatment of metastatic castration-resistant prostate cancer: final overall survival analysis of the COU-AA- 301 randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol 2012; 13: Ryan CJ, Smith MR, Fizazi K, et al.; COU-AA-302 Investigators. Abiraterone acetate plus prednisone versus placebo plus prednisone in chemotherapy-naive men with metastatic castrationresistant prostate cancer (COU-AA-302): final overall survival analysis of a randomised, double-blind, placebo-controlled phase 3 study. Lancet Oncol 2015; 16: Beer TM, Armstrong AJ, Rathkopf DE; PREVAIL Investigators. Enzalutamide in metastatic prostate cancer before chemotherapy. N Engl J Med 2014; 371: Scher HI, Fizazi K, Saad F, Taplin ME, et al.; AFFIRM Investigators. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med 2012; 367:
11 What s new The mechanisms behind resistance to hormonal therapies are being better characterized New drugs targeting these mechanisms have shown a survival advantage over previous best care and have entered routine practice Further agents overcoming resistance to these newer agents are now being studied In breast cancer, pathway inhibitors are used in combination with aromatase inhibitors to overcome resistance In prostate cancer these are abiraterone acetate and enzalutamide
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Use of Ovarian Suppression and Ablation in Breast Cancer Treatment
 Use of Ovarian Suppression and Ablation in Breast Cancer Treatment Dr Marina Parton Consultant Medical Oncologist Royal Marsden and Kingston Hospitals Overview Breast cancer phenotypes Use of ovarian manipulation
Use of Ovarian Suppression and Ablation in Breast Cancer Treatment Dr Marina Parton Consultant Medical Oncologist Royal Marsden and Kingston Hospitals Overview Breast cancer phenotypes Use of ovarian manipulation
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Lecture 10: Hormonal agents
 Lecture 10: Hormonal agents The survival and proliferation (growth) of some cancer cells is dependent on the action of steroid hormones. Early stage breast cancer and early stage prostate cancer are the
Lecture 10: Hormonal agents The survival and proliferation (growth) of some cancer cells is dependent on the action of steroid hormones. Early stage breast cancer and early stage prostate cancer are the
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
majority of the patients. And taking an aggregate of all trials, very possibly has a modest effect on improved survival.
 Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Extended Adjuvant Endocrine Therapy
 Extended Adjuvant Endocrine Therapy After all, 5 years Tamoxifen works.. For women with ER+ primary breast cancer, previous studies have shown that treatment with tamoxifen for 5 years has a carry-over
Extended Adjuvant Endocrine Therapy After all, 5 years Tamoxifen works.. For women with ER+ primary breast cancer, previous studies have shown that treatment with tamoxifen for 5 years has a carry-over
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Breast Cancer and Bone Loss. One in seven women will develop breast cancer during a lifetime
 Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Breast Cancer and Bone Loss One in seven women will develop breast cancer during a lifetime Causes of Bone Loss in Breast Cancer Patients Aromatase inhibitors Bil Oophorectomy Hypogonadism Steroids Chemotherapy
Metastatic prostate carcinoma. Lee Say Bob July 2017
 Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Anti-Androgen Therapies for Prostate Cancer: A Focused Review
 Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Anti-Androgen Therapies for Prostate Cancer: A Focused Review Nischala Ammannagari, MD, and Saby George, MD, FACP Abstract Among men in the United States, prostate cancer is the most common malignancy
Bad to the bones: treatments for breast and prostate cancer
 12 th Annual Osteoporosis: New Insights in Research, Diagnosis, and Clinical Care 23 rd July 2015 Bad to the bones: treatments for breast and prostate cancer Richard Eastell, MD FRCP (Lond, Edin, Ireland)
12 th Annual Osteoporosis: New Insights in Research, Diagnosis, and Clinical Care 23 rd July 2015 Bad to the bones: treatments for breast and prostate cancer Richard Eastell, MD FRCP (Lond, Edin, Ireland)
BREAST CANCER AND BONE HEALTH
 BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC)
") Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Secondary Hormonal therapies in mcrpc
 Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
A Layperson's Guide to Endocrine (Hormone) Therapy
 Therapy") A Layperson's Guide to Endocrine (Hormone) Therapy What we will cover What is the endocrine system Basic definition of endocrine therapy Classes of endocrine drugs How you can utilise endocrine therapy
A Layperson's Guide to Endocrine (Hormone) Therapy What we will cover What is the endocrine system Basic definition of endocrine therapy Classes of endocrine drugs How you can utilise endocrine therapy
Androgen Deprivation Therapy Its impact and the nursing role. Jane Thacker Uro-Oncology Nurse Specialist
 Androgen Deprivation Therapy Its impact and the nursing role Jane Thacker Uro-Oncology Nurse Specialist Overview of content To gain an understanding of ADT (androgendeprivation therapy) and why and how
Androgen Deprivation Therapy Its impact and the nursing role Jane Thacker Uro-Oncology Nurse Specialist Overview of content To gain an understanding of ADT (androgendeprivation therapy) and why and how
Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline
 Treatment Guideline") Mid Essex Locality Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline Contents FlowChart 2 Summary... 3 Key points... 3 Introduction... 3 Pharmacology... 3 Product information... 4 Place
Mid Essex Locality Degarelix Subcutaneous Injection (Firmagon ) Treatment Guideline Contents FlowChart 2 Summary... 3 Key points... 3 Introduction... 3 Pharmacology... 3 Product information... 4 Place
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Sequencing treatment for metastatic prostate cancer
 11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
11 Sequencing treatment for metastatic prostate cancer SOPHIE MERRICK, STYLIANI GERMANOU, ROGER KIRBY AND SIMON CHOWDHURY In the past 10 years there have been significant advances in the understanding
It is a malignancy originating from breast tissue
 59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
Clinical Policy: Goserelin Acetate (Zoladex) Reference Number: ERX.SPA.145 Effective Date:
 Reference Number: ERX.SPA.145 Effective Date:") Clinical Policy: (Zoladex) Reference Number: ERX.SPA.145 Effective Date: 10.01.16 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Zoladex) Reference Number: ERX.SPA.145 Effective Date: 10.01.16 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
LUNCH AND LEARN. April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology
 LUNCH AND LEARN April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology Medical Therapy for Prostate Cancer Androgen (testosterone) is required for the growth of both normal prostate and prostate cancers
LUNCH AND LEARN April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology Medical Therapy for Prostate Cancer Androgen (testosterone) is required for the growth of both normal prostate and prostate cancers
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Gonadotropin Releasing Hormone (GnRH) Analogs Drug Class Prior Authorization Protocol
 Analogs Drug Class Prior Authorization Protocol") Gonadotropin Releasing Hormone (GnRH) Analogs Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been
Gonadotropin Releasing Hormone (GnRH) Analogs Drug Class Prior Authorization Protocol Line of Business: Medicaid P&T Approval Date: February 21, 2018 Effective Date: April 1, 2018 This policy has been
 Mdi Medical Management of Breast Cancer Morbidity and Mortality Aug 13, 2009 Irina Kovatch, PGY3 Introduction Metastatic disease is the principal cause of death from breast cancer Metastatic events often
Mdi Medical Management of Breast Cancer Morbidity and Mortality Aug 13, 2009 Irina Kovatch, PGY3 Introduction Metastatic disease is the principal cause of death from breast cancer Metastatic events often
Western Locality Shared care information ~ Gonadorelin Analogues (Gnrh)
") Western Locality Shared care information ~ Gonadorelin Analogues (Gnrh) Specialist: Please complete the Shared Care letter sending a request to GP (see bottom of the page) April 2013 GP: Please indicate
Western Locality Shared care information ~ Gonadorelin Analogues (Gnrh) Specialist: Please complete the Shared Care letter sending a request to GP (see bottom of the page) April 2013 GP: Please indicate
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
ERLEADA (apalutamide) oral tablet
 oral tablet") ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ERLEADA (apalutamide) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
NCCN Guidelines for Prostate Cancer V Web teleconference 06/17/16 and 06/30/17
 Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Guideline Page and Request PROS-1 Submission from Myriad Genetic Laboratories, Inc. Request addition of recommendation for genetic risk assessment/testing to the Initial Clinical Assessment algorithm for
Integrated care: guidance on fracture prevention in cancer-associated bone disease; treatment options
 Paris, November 1st 2016 Integrated care: guidance on fracture prevention in cancer-associated bone disease; treatment options René Rizzoli MD International Osteoporosis Foundation and Division of Bone
Paris, November 1st 2016 Integrated care: guidance on fracture prevention in cancer-associated bone disease; treatment options René Rizzoli MD International Osteoporosis Foundation and Division of Bone
Clinical Policy: Goserelin Acetate (Zoladex) Reference Number: CP.PHAR.171 Effective Date: Last Review Date: Line of Business: Medicaid
 Reference Number: CP.PHAR.171 Effective Date: Last Review Date: Line of Business: Medicaid") Clinical Policy: (Zoladex) Reference Number: CP.PHAR.171 Effective Date: 10.01.16 Last Review Date: 11.17 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of
Clinical Policy: (Zoladex) Reference Number: CP.PHAR.171 Effective Date: 10.01.16 Last Review Date: 11.17 Line of Business: Medicaid Coding Implications Revision Log See Important Reminder at the end of
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes
 Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Drug Class Monograph
 Drug Class Monograph Class: Gonadotropin Releasing Hormone (GnRH) Analogs Drugs: Eligard (leuprolide acetate), Firmagon (degarelix), Lupaneta Pack (leuprolide acetate and norethindrone), Lupron Depot (leuprolide
Drug Class Monograph Class: Gonadotropin Releasing Hormone (GnRH) Analogs Drugs: Eligard (leuprolide acetate), Firmagon (degarelix), Lupaneta Pack (leuprolide acetate and norethindrone), Lupron Depot (leuprolide
Scottish Medicines Consortium
 Scottish Medicines Consortium anastrozole 1mg tablets (Arimidex ) No. (198/05) AstraZeneca UK Ltd New indication: for adjuvant treatment of postmenopausal women with hormone receptorpositive early invasive
Scottish Medicines Consortium anastrozole 1mg tablets (Arimidex ) No. (198/05) AstraZeneca UK Ltd New indication: for adjuvant treatment of postmenopausal women with hormone receptorpositive early invasive
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland
 What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
Chapter 8 Malignant Disease and Immunosuppression
 Chapter 8 page number 1 Chapter 8 Malignant Disease and Immunosuppression First line drugs Drugs recommended in both primary and secondary care Second line drugs Alternatives (often in specific conditions)
Chapter 8 page number 1 Chapter 8 Malignant Disease and Immunosuppression First line drugs Drugs recommended in both primary and secondary care Second line drugs Alternatives (often in specific conditions)
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
REFERENCE NUMBER: NH.PST.05 EFFECTIVE DATE: 10/10
 PAGE: 1 of 5 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
PAGE: 1 of 5 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Castrate resistant prostate cancer: the future of anti-androgens.
 Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Castrate resistant prostate cancer: the future of anti-androgens. Dmitri Pchejetski 1,2*, Heba Alshaker 3, Justin Stebbing 3,4* 1. Department of Medicine, Imperial College, London, UK 2. School of Medicine,
Hormonal therapies for the adjuvant treatment of early oestrogenreceptor-positive
 Hormonal therapies for the adjuvant treatment of early oestrogenreceptor-positive breast cancer Issued: November 2006 guidance.nice.org.uk/ta112 NICE 2006 Contents 1 Guidance... 3 2 Clinical need and practice...
Hormonal therapies for the adjuvant treatment of early oestrogenreceptor-positive breast cancer Issued: November 2006 guidance.nice.org.uk/ta112 NICE 2006 Contents 1 Guidance... 3 2 Clinical need and practice...
Medicines Management Group
 SHARED CARE PROTOCOL for FULVESTRANT (FASLODEX ) INJECTION Scope Fulvestrant may be considered for shared care arrangements for the treatment of metastatic breast cancer for disease relapse. Unique Identifier
SHARED CARE PROTOCOL for FULVESTRANT (FASLODEX ) INJECTION Scope Fulvestrant may be considered for shared care arrangements for the treatment of metastatic breast cancer for disease relapse. Unique Identifier
Final Appraisal Report. Ferring Pharmaceuticals Ltd. Advice No: 2109 December Recommendation of AWMSG
 Final Appraisal Report Degarelix (Firmagon ) for the treatment of advanced hormone-dependent prostate cancer Ferring Pharmaceuticals Ltd Advice No: 2109 December 2009 Recommendation of AWMSG Degarelix
Final Appraisal Report Degarelix (Firmagon ) for the treatment of advanced hormone-dependent prostate cancer Ferring Pharmaceuticals Ltd Advice No: 2109 December 2009 Recommendation of AWMSG Degarelix
Clinical Management Guideline for Planning and Treatment. The process to be followed when a course of chemotherapy is required to treat:
 Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Clinical Management Guideline for Planning and Treatment The process to be followed when a course of chemotherapy is required to treat: PROSTATE CANCER Patient information given at each stage following
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer
 Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Overview
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Overview Hormonal therapies for the adjuvant treatment of early oestrogen-receptor positive breast cancer The overview is written by members of the
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Overview Hormonal therapies for the adjuvant treatment of early oestrogen-receptor positive breast cancer The overview is written by members of the
Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer
 agonists in prostate cancer") B88 April 2015 2.1 Community Interest Company Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer This bulletin focuses on luteinising hormone-releasing hormone (LHRH) agonists. Currently
B88 April 2015 2.1 Community Interest Company Luteinising hormone-releasing hormone (LHRH) agonists in prostate cancer This bulletin focuses on luteinising hormone-releasing hormone (LHRH) agonists. Currently
Treatment of Advanced Prostate Cancer
 Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
A Prospective Observational Study to Evaluate the Efficacy and Safety Profiles of Leuprorelin 3 Month Depot for the Treatment of Pelvic Endometriosis
 SH SUEN & SCS CHAN A Prospective Observational Study to Evaluate the Efficacy and Safety Profiles of Leuprorelin 3 Month Depot for the Treatment of Pelvic Endometriosis Sik Hung SUEN MBChB, MRCOG Resident
SH SUEN & SCS CHAN A Prospective Observational Study to Evaluate the Efficacy and Safety Profiles of Leuprorelin 3 Month Depot for the Treatment of Pelvic Endometriosis Sik Hung SUEN MBChB, MRCOG Resident
Clinical Policy: Enzalutamide (Xtandi) Reference Number: CP.CPA.203 Effective Date: Last Review Date: 02.19
 Reference Number: CP.CPA.203 Effective Date: Last Review Date: 02.19") Clinical Policy: (Xtandi) Reference Number: CP.CPA.203 Effective Date: 11.16.16 Last Review Date: 02.19 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: (Xtandi) Reference Number: CP.CPA.203 Effective Date: 11.16.16 Last Review Date: 02.19 Line of Business: Commercial Revision Log See Important Reminder at the end of this policy for important
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
This includes bone loss, endometrial cancer, and vasomotor symptoms.
 Hello and welcome. My name is Chad Barnett. I m a Clinical Pharmacy Specialist in the Division of Pharmacy at the University of Texas, MD Anderson Cancer Center and I m very pleased today to be able to
Hello and welcome. My name is Chad Barnett. I m a Clinical Pharmacy Specialist in the Division of Pharmacy at the University of Texas, MD Anderson Cancer Center and I m very pleased today to be able to
January Abiraterone pre-docetaxel for patients with asymptomatic or minimally symptomatic metastatic castration resistant prostate cancer
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone pre-docetaxel for asymptomatic/minimally symptomatic metastatic castration resistant prostate cancer Abiraterone pre-docetaxel for patients with asymptomatic
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone pre-docetaxel for asymptomatic/minimally symptomatic metastatic castration resistant prostate cancer Abiraterone pre-docetaxel for patients with asymptomatic
SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer
![SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer](/thumbs/95/125806264.jpg "SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer") SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer Charles Moertel Lecture May 12, 2017 Gini Fleming Charles Moertel Founder of NCCTG Dedication to high quality clinical
SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer Charles Moertel Lecture May 12, 2017 Gini Fleming Charles Moertel Founder of NCCTG Dedication to high quality clinical
Hormone therapy in Breast Cancer patients with comorbidities
 Hormone therapy in Breast Cancer patients with comorbidities Diana Crivellari Centro di Riferimento Oncologico Aviano- ITALY Madrid November 9th, 2007 Main issues Comorbidities in elderly women Hormonal
Hormone therapy in Breast Cancer patients with comorbidities Diana Crivellari Centro di Riferimento Oncologico Aviano- ITALY Madrid November 9th, 2007 Main issues Comorbidities in elderly women Hormonal
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
ORILISSA (elagolix) oral tablet
 oral tablet") ORILISSA (elagolix) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
ORILISSA (elagolix) oral tablet Coverage for services, procedures, medical devices and drugs are dependent upon benefit eligibility as outlined in the member's specific benefit plan. This Pharmacy Coverage
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
38 years old, premenopausal, had L+snbx. Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI %
 38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
Citation for published version (APA): Buijs, C. (2008). Long-term side effects of adjuvant breast cancer treatment s.n.
: Buijs, C. (2008). Long-term side effects of adjuvant breast cancer treatment s.n.") University of Groningen Long-term side effects of adjuvant breast cancer treatment Buijs, Ciska IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite
University of Groningen Long-term side effects of adjuvant breast cancer treatment Buijs, Ciska IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite
BREAST CANCER BREAST CANCER
 BREAST CANCER George Raptis, M.D., M.B.A Division of Medical Oncology & Hematology College of Physicians & Surgeons Columbia University BREAST CANCER Epidemiology - Commonest cancer in women - About 235,000
BREAST CANCER George Raptis, M.D., M.B.A Division of Medical Oncology & Hematology College of Physicians & Surgeons Columbia University BREAST CANCER Epidemiology - Commonest cancer in women - About 235,000
Index. urologic.theclinics.com. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Note: Page numbers of article titles are in boldface type. A Acquired hypogonadism, prevalence of, 165 167 primary, 165 secondary, 167 Adipose tissue, as an organ, 240 241 Adrenal hyperplasia, congenital,
Adjuvant Systemic Therapy in Early Stage Breast Cancer
 Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER
 OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER STEPHEN E. JONES, M.D. US ONCOLOGY RESEARCH THE WOODLANDS, TX TOPICS PREMENOPAUSAL BREAST CANCER POSTMENOPAUSAL BREAST CANCER THE FUTURE TOPICS PREMENOPAUSAL
OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER STEPHEN E. JONES, M.D. US ONCOLOGY RESEARCH THE WOODLANDS, TX TOPICS PREMENOPAUSAL BREAST CANCER POSTMENOPAUSAL BREAST CANCER THE FUTURE TOPICS PREMENOPAUSAL
Abiraterone Acetate is an antiandrogen used in the treatment of Castration-Resistant Prostate Cancer(CRPC).
.") For the use only of an Oncologist or a Hospital or a Laboratory ABIRATERONE ACETATE TABLETS Zabiteron-250 COMPOSITION Abiraterone Acetate Tablets 250mg Each uncoated tablets contains: Abiraterone Acetate
For the use only of an Oncologist or a Hospital or a Laboratory ABIRATERONE ACETATE TABLETS Zabiteron-250 COMPOSITION Abiraterone Acetate Tablets 250mg Each uncoated tablets contains: Abiraterone Acetate
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Ibrance) Reference Number: CP.PHAR.125 Effective Date: 10.01.15 Last Review Date: 11.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Ibrance) Reference Number: CP.PHAR.125 Effective Date: 10.01.15 Last Review Date: 11.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents
 Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
The efficacy of second-line hormone therapy for recurrence during adjuvant hormone therapy for breast cancer
 517734TAM6210.1177/1758834013517734Therapeutic Advances in Medical OncologyR Mori and Y Nagao research-article2013 Therapeutic Advances in Medical Oncology Original Research The efficacy of second-line
517734TAM6210.1177/1758834013517734Therapeutic Advances in Medical OncologyR Mori and Y Nagao research-article2013 Therapeutic Advances in Medical Oncology Original Research The efficacy of second-line
Prostate cancer is now the most
 : a new hormonal treatment for prostate cancer Professor Malcolm Mason, School of Medicine, Cardiff University, Velindre Hospital, Whitchurch, Cardiff - hypothalamus According to NICE, prostate cancer
: a new hormonal treatment for prostate cancer Professor Malcolm Mason, School of Medicine, Cardiff University, Velindre Hospital, Whitchurch, Cardiff - hypothalamus According to NICE, prostate cancer
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
Aromatase inhibitors in breast cancer: Current and evolving roles
 CURRENT DRUG THERAPY JOHN HILL, MD Department of Hematology and Medical Oncology, The Cleveland Clinic HALLE MOORE, MD Associate Professor, Department of Hematology and Clinical Oncology, The Cleveland
CURRENT DRUG THERAPY JOHN HILL, MD Department of Hematology and Medical Oncology, The Cleveland Clinic HALLE MOORE, MD Associate Professor, Department of Hematology and Clinical Oncology, The Cleveland
Systemic Management of Breast Cancer
 Systemic Management of Breast Cancer Why Who When What How long Etc. Vernon Harvey Rotorua, June 2014 Systemic Management of Breast Cancer Metastatic Disease Adjuvant Therapy Aims of therapy Quality of
Systemic Management of Breast Cancer Why Who When What How long Etc. Vernon Harvey Rotorua, June 2014 Systemic Management of Breast Cancer Metastatic Disease Adjuvant Therapy Aims of therapy Quality of
SYSTEMIC THERAPY OPTIONS FOR BREAST CANCER IN 2014
 SYSTEMIC THERAPY OPTIONS FOR BREAST Oncology Day 2014 CANCER IN 2014 Dr. Katherine Enright, M.D., M.P.H., F.R.C.P.(C) Katherine.enright@Trilliumhealthpartners.ca OBJECTIVES 1. Outline an approach to the
SYSTEMIC THERAPY OPTIONS FOR BREAST Oncology Day 2014 CANCER IN 2014 Dr. Katherine Enright, M.D., M.P.H., F.R.C.P.(C) Katherine.enright@Trilliumhealthpartners.ca OBJECTIVES 1. Outline an approach to the
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Radium-223 chloride for the treatment of bone metastases in castrate resistant prostate cancer Draft scope Draft
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Radium-223 chloride for the treatment of bone metastases in castrate resistant prostate cancer Draft scope Draft
Reproductive physiology
 Reproductive physiology Sex hormones: Androgens Estrogens Gestagens Learning objectives 86 (also 90) Sex Genetic sex Gonadal sex Phenotypic sex XY - XX chromosomes testes - ovaries external features Tha
Reproductive physiology Sex hormones: Androgens Estrogens Gestagens Learning objectives 86 (also 90) Sex Genetic sex Gonadal sex Phenotypic sex XY - XX chromosomes testes - ovaries external features Tha
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Single Technology Appraisal (STA)
") Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
Thank you for agreeing to give us a statement on your organisation s view of the technology and the way it should be used in the NHS. Healthcare professionals can provide a unique perspective on the technology
HORMONAL THERAPY IN ADJUVANT CARE
 ADVANCES IN ENDOCRINE THERAPY FOR BREAST CANCER* Matthew J. Ellis, MD, PhD ABSTRACT Endocrine therapy is used frequently in breast cancer management, particularly in the setting of adjuvant care, but outstanding
ADVANCES IN ENDOCRINE THERAPY FOR BREAST CANCER* Matthew J. Ellis, MD, PhD ABSTRACT Endocrine therapy is used frequently in breast cancer management, particularly in the setting of adjuvant care, but outstanding
פ א ר מ ה P H A R x M A
 פ א ר מ ה P H A R x M A הביטאון לענייני תרופות ותראפיה ISRAEL DRUG BULLETIN Vol. 19, Bulletin No. 107 June-July 2012 Also in the Bulletin: Degarelix for Advanced Hormone-Dependent Prostate Cancer NEW TREATMENT
פ א ר מ ה P H A R x M A הביטאון לענייני תרופות ותראפיה ISRAEL DRUG BULLETIN Vol. 19, Bulletin No. 107 June-July 2012 Also in the Bulletin: Degarelix for Advanced Hormone-Dependent Prostate Cancer NEW TREATMENT
Multimedia Appendix 6 Educational Materials Table of Contents. Intervention Educational Materials Audio Script (version 1)
") Multimedia Appendix 6 Educational Materials Table of Contents Intervention Educational Materials... 1 Audio Script (version 1)... 1 Text (version 1)... 5 Slides (version 1)... 17 Audio Script (version
Multimedia Appendix 6 Educational Materials Table of Contents Intervention Educational Materials... 1 Audio Script (version 1)... 1 Text (version 1)... 5 Slides (version 1)... 17 Audio Script (version
Fulvestrant (Faslodex )
") In Partnership with Health Authorities & GPs continuing-care guidelines Fulvestrant (Faslodex ) in the Management of Postmenopausal Women with Advanced Breast Cancer Approved by: Date approved: October
In Partnership with Health Authorities & GPs continuing-care guidelines Fulvestrant (Faslodex ) in the Management of Postmenopausal Women with Advanced Breast Cancer Approved by: Date approved: October
Long Term Toxicity of Endocrine Therapy for premenopausal women with ER positive breast cancer
 Global Breast Cancer Conference 2017 21 st Apr, 2017@Chezu Island Long Term Toxicity of Endocrine Therapy for premenopausal women with ER positive breast cancer Shinji Ohno, M.D., Ph.D., F.A.C.S. Breast
Global Breast Cancer Conference 2017 21 st Apr, 2017@Chezu Island Long Term Toxicity of Endocrine Therapy for premenopausal women with ER positive breast cancer Shinji Ohno, M.D., Ph.D., F.A.C.S. Breast
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Seigo Nakamura,M.D.,Ph.D.
 Seigo Nakamura,M.D.,Ph.D. Professor of Surgery Director of Breast Center Showa University Hospital Chairman of the board of directors Japan Breast Cancer Society Inhibition of Estrogen-Dependent Growth
Seigo Nakamura,M.D.,Ph.D. Professor of Surgery Director of Breast Center Showa University Hospital Chairman of the board of directors Japan Breast Cancer Society Inhibition of Estrogen-Dependent Growth
Hormone therapy for prostate cancer
 The Clatterbridge Cancer Centre NHS Foundation Trust Hormone therapy for prostate cancer General information A guide for patients and carers Contents What is hormone therapy?... 1 How does hormone therapy
The Clatterbridge Cancer Centre NHS Foundation Trust Hormone therapy for prostate cancer General information A guide for patients and carers Contents What is hormone therapy?... 1 How does hormone therapy
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Objectives Critically review presentations on 1. Local therapy 2. Adjuvant chemotherapy for isolated local regional recurrence 3. The optimal duration
 Objectives Critically review presentations on 1. Local therapy 2. Adjuvant chemotherapy for isolated local regional recurrence 3. The optimal duration of endocrine therapy 4. Advances in HER2 directed
Objectives Critically review presentations on 1. Local therapy 2. Adjuvant chemotherapy for isolated local regional recurrence 3. The optimal duration of endocrine therapy 4. Advances in HER2 directed