Rare GI Malignancies
|
|
|
- MargaretMargaret Cross
- 5 years ago
- Views:
Transcription
1 Rare GI Malignancies Jordan Karlitz, MD Associate Professor of Medicine, Division of Gastroenterology Director, Hereditary GI Cancer and Genetics Program Tulane University School of Medicine
2 Outline Gastrointestinal Stromal Tumors (GISTs) Mucosal Associated Lymphoid Tissue Tumors (MALT). Neuroendocrine Tumors (NETs) and Pancreatic Neuroendocrine Tumors (PNETs)
3 Outline Clinical Presentation Diagnosis Treatment Prognosis/Survival tumors relatively rare so epidemiology not as robust as more common tumors.
4 GIST Gastrointestinal Stromal Tumors 2 categories of stromal/mesenchymal tumors (tumors arising from stromal/mesenchymal components of GI tract) 1) GIST any portion GI tract but usually stomach >> proximal small bowel. 2) Others lipoma, leiomyoma (benign smooth muscle tumor), schwannomas etc. Mesenchymal=diffuse network of cells forming the embryonic mesoderm and giving rise to connective tissue, muscle, blood and blood vessels and lymphatic system.

5 GISTs and other mesenchymal tumors are submucosal
6 GIST continued 6,000 new cases per year in USA likely underestimate as we may be missing smaller lesions. GISTs initially thought to arise from smooth muscle and were confused with leiomyomas. With advances in molecular biology, GISTs became better defined. Main distinguishing characteristic is the almost universal expression of CD117 antigen (leiomyomas and other submucosal lesions do not express this).
7 CD117 part of the KIT transmembrane receptor tyrosine kinase, which is a product of the c KIT protooncogene. Mutation leads to activation (gain of function) of tyrosine kinase protein (sporadic>hereditary). Those GISTs that are not CD117 positive have mutations in other proteins that play a similar role in oncogenic stimulation. Gleevac (Imatinib) is a tyrosine kinase inhibitor and targets GISTs but not other submucosal lesions (i.e. leiomyomas).
8 GISTs are thought to arise from stem cells within the gut wall whose future differentiation would be towards the interstitial cells of Cajal (ICC). ICC have both smooth muscle and neuronal differentiation and serve as the GI pacemaker cells, regulating peristalsis.
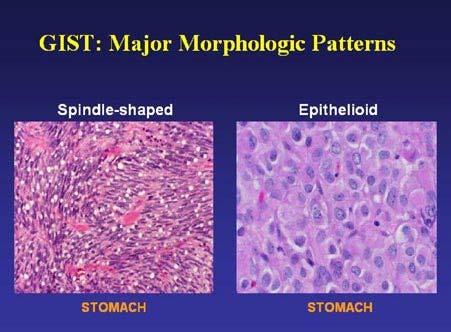
9 Histology Spindle cell (elongated nuclei) 70% Epitheliod (oval/round nuclei) 20% Mixed 10% Molecular studies (i.e. CD117) are more important.
10
11 Behavior Depends on size, mitotic rate and location (SI more aggressive than stomach). Not defined simply as benign or malignant, but more of a spectrum of aggressive behavior (metastases, risk of recurrence post resection) based on above. Even small GISTs (i.e. 1 cm) can behave in a malignant fashion. Clinical manifestations range from no symptoms to bleeding, abdominal mass, abdominal pain.
12 Risk of aggression size Mitotic count Very low risk < 2cm <5 per 50 HPF Low risk 2-5 cm <5 per 50 HPF Intermediate High risk <5 cm 5-10 cm >5 cm >10 cm Any size 6-10 per 50HPF <5 per 50 HPF >5 per 50 HPF Any mitotic rate >10 per 50 HPF
13 Diagnosis Various imaging tests including CT and PET scan. EGD/EUS EUS can help to distinguish GISTs from other submucosal lesions. GISTs arise from the muscularis propria.

14 epithelium Lamina propria Muscularis mucosa submucosa Muscularis propria Mucosa=epithelium + lamina propria
15 GI tract wall layers Mucosa (carcinoid) Muscularis mucosa/lamina propria (carcinoid) Submucosa (lipoma, cysts, varices, carcinoid) Muscularis propria (GIST) Carinoids, GISTS Hypoechoic (dark) Lipoma Hyperechoic (bright) Muscle dark

16 Lipoma in submucosahyperechoic lesion In hyperechoic layer Muscularis propria hypoechoic layer

17 Hypoechoic lesion from muscularis propria=gist
18 Management All gastric GISTS >2 cm surgical removal. (****some say resect all sizes, even < 1 cm) < 2 cm controversial as growth rate and metastatic potential is unclear. < 2 cm? Follow endoscopically,? remove endoscopically,? Remove surgically. Endoscopic removal also controversial due to risk of + margin and tumor spillage.
19 Larger GISTs can be quite aggressive and even after surgery with negative margins the recurrence rate can be high (55% at 5 years for larger lesions).
20 Gleevac/Imatinib Tyrosine kinase inhibitors. Decreases post operative recurrence as adjuvant therapy. Neoadjuvant therapy to shrink GISTs prior to surgery also used in some cases. Used in metatstatic disease with success but can get Gleevac resistance eventually. Following the introduction of imatinib, the median survival of advanced GIST was 60 months.
21 MALT Lymphoma Mucosa Associated Lymphoid Tissue=MALT= lymphoid tissue of the gut MALT tissue is organized in a similar fashion to lymphoid tissue elsewhere in the body. Lymphoma in MALT tissue usually arises from B cells in the marginal zone. The term MALT lymphoma is often used interchangeably with marginal zone B cell lymphoma.
22 Diffuse large B cell lymphomas of the stomach may evolve from MALT lymphomas, however others have no relation to the marginal zone of MALT tissue.

23 Normal Lymphoid Tissue Structure Marginal zone Follicle center Marginal zone magnified
24 Gastric tissue does not normally contain MALT but may acquire it in response to H. Pylori infection. MALT tissue that is induced by H. Pylori transforms to a lymphoma in a small percentage of patients. MALT lymphomas are usually low grade and can regress after H. Pylori treatment. Occasionally they can be quite aggressive and won t respond to antibiotics.
25 Epidemiology MALT lymphoma accounts for 40% of all gastric lymphomas (45 50% are Large B cell lymphoma). Incidence in H. Pylori infected patients is 1:30,000 to 1:80,000. Median age 60 Male=female H. pylori present in biopsy of 90% of MALT lymphoma cases and serology is + in 98%
26 Pathogenesis/pathology H. pylori induces gastritis and development of MALT tissue. H. Pylori specific T cells promote growth and recruitment of abnormal B cell clones that can grow autonomously, even after H. Pylori is eradicated in some cases. 41% in antrum Multifocal in 33% Ulcers 47% Erythema 30%
27 See lymphoid lesions that invade and destroy gastric glands and crypts. Lymphocytes tend to have cytologic atypia. Express pan B cell antigens including CD19,20,79.
28 MALT Lymphoma

29 lymphoma

30 Magnified view
31 Diagnosis/Staging EGD with biopsy and H. Pylori testing. Other tests include CT, bone marrow biopsy, LDH=staging. EUS to assess extent of stomach wall involvement. 90% are stage 1= gastric wall (can range from mucosa alone or extend all the way to serosa). Stage 2=LNs Stage 3=Adjacent organs Stage 4=Disseminated
32 Stage 1: survival is 80 95% at 5 years. Stage 1: Prognosis worsens in stage 1 if disease extends deeper to serosa.
33 Treatment H. Pylori treatment is mainstay in early stage disease with 50 80% remission. XRT/Chemo/Surgery is reserved for more advanced disease or for early stage disease that doesn t regress with antibiotics or if H. pylori negative or certain chromosomal translocations.
34 Neuroendocrine Tumors (NETs) and Pancreatic Neuroendocrine Tumors (PNETs) NET/PNET arise from neuroendocrine cells. Neuroendocrine cell cells that receive neuronal input and in turn, release hormones to the blood. Can be functional (hormone based syndromesi.e. carcinoid syndrome) or non functional. NET= carcinoid (most common NET/PNET). PNET= gastrinoma, insulinoma, somatostatinoma, VIPoma, glucogonoma.
35 NETs/PNETs can be part of hereditary syndromes Multiple endocrine neoplasia syndrome (MEN) pancreas, pituitary, parathyroid. I.e. Gastrinoma. Neurofibromatosis somatostatinomas Tuberous Sclerosis PNETs Von Hippel Lindau PNETs
36 NETs/PNETS diagnosis Seen on EGD and colonoscopy (carcinoids). Picked up on body imaging incidentally (PNETs) or for symptoms. Neuroendocrine markers Chromogranin A (tumor diagnosis NETs/PNETs and response to treatment). Carcinoid syndrome serum serotonin, urine 5 HIAA (5 hydroxyindoleacetic Acid).
37 NETs/PNETs diagnosis continued PNETs gastrin, insulin etc. (see later) NET/PNET specific imaging=octreoscan NETs and PNETS often have somatostatin receptors (hormone that decreases release of many GI hormones). Octreoscan Octreotide (similar to somatostatin) is radiolabelled, injected into vein and binds NETs/PNETs.

38 Small Carcinoid Octreoscan
39 Rectal Carcinoid
40 Carcinoids (NET) Incidence about 5/100,000 per year, but increasing over time. 45% in small bowel 31% in colorectal (10% colon, 21% rectum). 16% appendix 7% in stomach Non functional (no symptoms due to hormones) > functional (carcinoid syndrome diarrhea, flushing, wheezing). Location important factor for prognosis.
41 Gastric Carcinoids not all the same 75% type 1 associated with pernicious anemia (atrophic gastritis). high PH with secondary increased gastrin. Metastases rare. Generally EMR if small. Indolent behavior. Current status of gastrointestinal carcinoids. Gastroenterology May;128(6):
42 Gastric Carcinoids not all the same 5 10% type 2 associated with gastrinoma with increased gastrin and low PH. Metastases rare. Generally EMR if small. Indolent behavior.
43 Gastric Carcinoids not all the same 15 25% type 3 normal gastrin and PH. More aggressive. Often require surgery. 65% metastases at time of surgery. Overall 5 year survival type 3 < 35%.
44 Mid gut carcinoids Ileum > jejenum 25% have more than one SB lesion. Frequently associated with carcinoid syndrome if liver metastases (functional tumor). Metastases common, especially if > 1 cm in size (70% metastases if > 1 cm). Median survival with metastases is 103 months. Treatment resection of SB and mesentery.
45 Appendiceal Carcinoids Most common tumor of appendix. Not as frequently associated with metastases c/w small bowel. Appendectomy if < 2 cm, right hemicolectomy if > 2 cm. 5 year survival overall of 98%.
46 Colonic Carcinoids Frequently seen in rectum during colonoscopy If rectal and < 1 cm and confined to mucosa/submucosa, metastases infrequent. EMR (Endoscopic mucosal resection). Rectal 1 2 cm, metastases in 6%. Possible EMR. Rectal > 2 cm, metastases 24%. Surgery. Rest of colon frequently surgery. Overall 5 year survival 62% for colon, 87% for rectum.
47 Gastrinoma/Zollinger Ellison Syndrome cases per 1 million people per year. Tumor releasing gastrin despite already low gastric PH (inappropriate gastrin release). Tumor in pancreas or duodenum. High gastric output with gastric and small bowel ulcerations and diarrhea. 25% associated with multiple endocrine neoplasia syndrome. < 1/1000 duodenal ulcers associated with ZES (consider if no NSAIDS, no H. pylori).
48 Gastrinoma Diagnosis High gastrin level in setting of low gastric (acidic) PH. Secretin stimulation test secretin stimulates gastric G cells to secrete gastrin (see very high levels of gastrin). Octreoscan EUS Rule out MEN syndrome
49 Gastrinoma treatment/prognosis High dose PPI Surgery Patients with liver metastases have a 10 year survival of 30 percent compared with a 15 year survival of 83 percent in those without liver metastases.
50 Insulinoma Most common PNET 4 cases per 1 million people per year Always in pancreas Secrete insulin inappropriately with resultant hypoglycemia with typical associated symptoms. Associated with MEN 1
51 Insulinoma Diagnosis and treatment Octreoscan often negative compared to other PNETS because few somatostatin receptors. EUS helpful Treat with surgery NIH cases series some patients with insulinoma, even if metastatic, can live up to 25 years.
52 Other PNETS, very rare Glucogonoma 1 in 1 10 million people per year Increased glucagon associated with hyperglycemia and migratory necrolytic erythema (rash). Somatostatin analogues (octreotide) inhibit hormone release and are used for treatment (mainly for symptoms). Surgery Most metastatic at time of diagnosis however these patients can live 4 5 years or longer after diagnosis per case series reports.
53 Migratory necrolytic erythema
54 Somatostatinoma 1 in 40 million people per year. Can occur outside pancreas. High somatostatin levels impede release of multiple hormones with resultant malabsorption, weight loss. Associated with MEN 1 and neurofibromatosis I (von Recklinghausen disease). Somatostatin analogues (octreotide) inhibit VIP release and are used for treatment (symptom control). Surgery 70 92% present with metastatic disease with 15%, 5 year survival in stage 4 disease.
55 VIPoma 1 in 10 million people per year. Increased vasoactive intestinal polypeptide. Large volume, watery diarrhea. Hypokalemia MEN type 1 in 5%. Somatostatin analogues (octreotide) inhibit VIP release and are used for treatment (symptom control). Surgery Median survival is 96 months
56 Conclusions GIST, MALT lymphoma, carcinoids relatively rare but picked up more frequently with increased endoscopy, imaging. PNETs rare. Epidemiologic data regarding incidence and prognosis not as robust as more common conditions. Size (i.e. GISTs), location (i.e. carcinoids), histology (i.e. GISTs) play important role in aggressivity. Association with hereditary syndromes rule these out.
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Subepithelial Lesions of the Gut: When Should I Worry?
 Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
Subepithelial Lesions of the Gut: When Should I Worry? President, ASGE Chairman, GI & Hepatology Scottsdale, AZ Faigel.douglas@mayo.edu Case 55 yo male with reflux EGD for Barrett s Screening SET, mucosal
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Diagnosing and monitoring NET
 Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Commonly Encountered Neuro-Endocrine Tumors of the Gut
 Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
Commonly Encountered Neuro-Endocrine Tumors of the Gut Moderators: Giuseppe Aliperti, MD Steven Edmundowicz, MD Panelists Douglas O. Faigel, MD Professor of Medicine Department of Gastroenterology Oregon
Unexpected Findings at Endoscopy
 The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
The Endoscopic Incidentaloma: What to Tell Your Patient t with Unexpected Endoscopic Findings: Gastric Intestinal Metaplasia, Silent Ileitis, Carcinoid David Greenwald, MD Montefiore Medical Center Albert
Gastrointestinal pathology 2018 lecture 4. Dr Heyam Awad FRCPath
 Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
Gastrointestinal pathology 2018 lecture 4 Dr Heyam Awad FRCPath Topics to be covered Peptic ulcer disease Hiatal hernia Gastric neoplasms Peptic ulcer disease (PUD)= chronic gastric ulcer Causes H pylori
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
Unusual Pancreatic Neoplasms RTC 2/11/2011
 Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Unusual Pancreatic Neoplasms RTC 2/11/2011 Objectives Intraductal Papillary Mucinous Neoplasm (IPMN) Mucinous Cystic Neoplasm (MCN) Islet Cell Tumors Insulinoma Glucagonoma VIPoma Somatostatinoma Gastrinoma
Carcinoid Tumors: The Beginning and End. Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011
 Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Imaging of Gastrointestinal Stromal Tumors (GIST) Amir Reza Radmard, MD Assistant Professor Shariati hospital Tehran University of Medical Sciences
 Amir Reza Radmard, MD Assistant Professor Shariati hospital Tehran University of Medical Sciences") Imaging of Gastrointestinal Stromal Tumors (GIST) Amir Reza Radmard, MD Assistant Professor Shariati hospital Tehran University of Medical Sciences Describe the typical imaging findings of GIST at initial
Imaging of Gastrointestinal Stromal Tumors (GIST) Amir Reza Radmard, MD Assistant Professor Shariati hospital Tehran University of Medical Sciences Describe the typical imaging findings of GIST at initial
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide)
") GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
NEUROENDOCRINE CARCINOID TUMORS PANCREATIC NEUROENDOCRINE TUMORS
 University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
Type 2 gastric neuroendocrine tumor: report of one case
 Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Case Report Type 2 gastric neuroendocrine tumor: report of one case Yuanliang Li, Xin Su, Huangying Tan Department of Integrative Oncology, China-Japan Friendship Hospital, Beijing 100029, China Correspondence
Principles of diagnosis, work-up and therapy The Gastroenterologist s role
 Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
RADIOFREQUENCY ABLATION
 RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
RADIOFREQUENCY ABLATION ELIZABETH DAVID M D FRCPC VASCULAR A ND INTERVENTIONAL RADIOLOGIST SUNNYBROOK HEALTH SCIENCES CENTRE GIST GASTROINTESTINAL STROMAL TUMORS Stromal or mesenchymal neoplasms affecting
Sandostatin LAR. Sandostatin LAR (octreotide acetate) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.09 Subject: Sandostatin LAR Page: 1 of 5 Last Review Date: March 16, 2018 Sandostatin LAR Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.09 Subject: Sandostatin LAR Page: 1 of 5 Last Review Date: March 16, 2018 Sandostatin LAR Description
AN ARGUMENT FOR SURGERY FOR GASTRINOMA. Lauren Wilson R1 General Surgery
 AN ARGUMENT FOR SURGERY FOR GASTRINOMA Lauren Wilson R1 General Surgery WHAT IS A GASTRINOMA? Gastrin secreting cells derived from multipotential stem cells of endodermal origin or enteroendocrine cells
AN ARGUMENT FOR SURGERY FOR GASTRINOMA Lauren Wilson R1 General Surgery WHAT IS A GASTRINOMA? Gastrin secreting cells derived from multipotential stem cells of endodermal origin or enteroendocrine cells
Regression of Advanced Gastric MALT Lymphoma after the Eradication of Helicobacter pylori
 Gut and Liver, Vol. 6, No. 2, April 2012, pp. 270-274 CASE REPORT Regression of Advanced Gastric MALT Lymphoma after the Eradication of Helicobacter pylori Soo-Kyung Park, Hwoon-Yong Jung, Do Hoon Kim,
Gut and Liver, Vol. 6, No. 2, April 2012, pp. 270-274 CASE REPORT Regression of Advanced Gastric MALT Lymphoma after the Eradication of Helicobacter pylori Soo-Kyung Park, Hwoon-Yong Jung, Do Hoon Kim,
Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract
 Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract Eric J. May 1, Shannon P. Sheedy 1, Joel G. Fletcher 1, Mark J. Truty 2, Thomas C. Smyrk 3, Jeff L. Fidler 1 1. Radiology,
Cross-sectional Imaging of Neuroendocrine Tumors of the Gastrointestinal Tract Eric J. May 1, Shannon P. Sheedy 1, Joel G. Fletcher 1, Mark J. Truty 2, Thomas C. Smyrk 3, Jeff L. Fidler 1 1. Radiology,
Neuroendocrine Tumors: Just the Basics. George Fisher, MD PhD
 Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Endocrine Tumors of the Gastrointestinal System. F. V. Nowak Ohio University March 22, 2005
 Endocrine Tumors of the Gastrointestinal System F. V. Nowak Ohio University March 22, 2005 Gastroenteropancreatic Endocrine System Clear cells of endodermal origin found in the pancreas, stomach, small
Endocrine Tumors of the Gastrointestinal System F. V. Nowak Ohio University March 22, 2005 Gastroenteropancreatic Endocrine System Clear cells of endodermal origin found in the pancreas, stomach, small
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust
 GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Gastrinoma: Medical Management. Haley Gallup
 Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Endoscopic approach to subepithelial lesions
 513538TAG7310.1177/1756283X13513538Therapeutic Advances in GastroenterologyL Menon and JM Buscaglia research-article2013 Therapeutic Advances in Gastroenterology Review Endoscopic approach to subepithelial
513538TAG7310.1177/1756283X13513538Therapeutic Advances in GastroenterologyL Menon and JM Buscaglia research-article2013 Therapeutic Advances in Gastroenterology Review Endoscopic approach to subepithelial
SCOPE TODAYS SESSION. Case 1: Case 2. Basic Theory Stuff: Heavy Stuff. Basic Questions. Basic Questions
 MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
Collecting Cancer Data: GIST/NET 1/9/14
 Collecting Cancer Data: Gastrointestinal Stromal Tumor (GIST) Gastrointestinal Neuroendocrine Tumors (NET) 2013 2014 NAACCR Webinar Series January 9, 2014 Q&A Please submit all questions concerning webinar
Collecting Cancer Data: Gastrointestinal Stromal Tumor (GIST) Gastrointestinal Neuroendocrine Tumors (NET) 2013 2014 NAACCR Webinar Series January 9, 2014 Q&A Please submit all questions concerning webinar
Pathology testing and Neuroendocrine tumours (NETs)
") Pathology testing and Neuroendocrine tumours (NETs) NETs are probably far more common than we think. Most grow so slowly and produce such widely varied and non-specific symptoms, or no symptoms at all,
Pathology testing and Neuroendocrine tumours (NETs) NETs are probably far more common than we think. Most grow so slowly and produce such widely varied and non-specific symptoms, or no symptoms at all,
Peptic ulcer disease. Nomin-Erdene. D SOM-531
 Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Peptic ulcer disease Nomin-Erdene. D SOM-531 Learning objectives Stomach gross anatomy PUD Epidemiology Pathogenesis Clinical manifestation Diagnosing Treatment Complicated ulcer disease Surgical procedures
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Stomach. R.B. Kolachalam, MD
 Stomach R.B. Kolachalam, MD Relevent Anatomy 1.four regions: Cardia, Fundus, Body, and the Pylorus 2. fixed in two locations- at the GEJ and the duodenum Gastric Anatomy body of the stomach: site of mechanical
Stomach R.B. Kolachalam, MD Relevent Anatomy 1.four regions: Cardia, Fundus, Body, and the Pylorus 2. fixed in two locations- at the GEJ and the duodenum Gastric Anatomy body of the stomach: site of mechanical
Brief History. Identification : Past History : HTN without regular treatment.
 Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Brief History Identification : Name : 陳 x - Admission : 94/10/06 Gender : male Age : 75 y/o Chief Complaint : Urinary difficulty for months. Past History : HTN without regular treatment. Brief History
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid
 Neuroendocrine Tumors and Lung Carcinoid") Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Gastrointestinal Tract Cancer
 Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastrointestinal Tract Cancer Tumors of the Stomach Gastric adenocarcinoma Incidence and Epidemiology Incidence mortality rates USA High incidence: Japan, China, Chile, Ireland risk lower socioeconomic
Gastroenterology Tutorial
 Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Gastroenterology Tutorial Gastritis Poorly defined term that refers to inflammation of the stomach. Infection with H. pylori is the most common cause of gastritis. Most patients remain asymptomatic Some
Digestive system L 2. Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section
 Digestive system L 2 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the general structure of digestive tract: a-mucosa. b-submucosa. c-muscularis externa d-adventitia
Digestive system L 2 Lecturer Dr. Firdous M. Jaafar Department of Anatomy/Histology section objectives 1-Describe the general structure of digestive tract: a-mucosa. b-submucosa. c-muscularis externa d-adventitia
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms
 Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
CT Scan Abdomen Management
 Weird and Wonderful Tumours in the GI Tract GIST Carcinoid Lymphoma Facilitator: Rona Cheifetz Panel Members: Carol Swallow, Surgical Oncology Jamie Appleby, General Surgery Meg Knowling, Medical Oncology
Weird and Wonderful Tumours in the GI Tract GIST Carcinoid Lymphoma Facilitator: Rona Cheifetz Panel Members: Carol Swallow, Surgical Oncology Jamie Appleby, General Surgery Meg Knowling, Medical Oncology
An Overview of NETS. Richard R.P. Warner M.D
 An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Objectives. Terminology 03/11/2013. Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors. Pathology Update 2013
 Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Pitfalls in the diagnosis of Gastroenteropancreatic Neuroendocrine Tumors Pathology Update 2013 Ozgur Mete, MD Consultant in Endocrine Pathology, Department of Pathology, University Health Network Assistant
Endocrinology and VHL: The adrenal and the pancreas
 Overview Endocrinology and VHL: The adrenal and the pancreas LAUREN FISHBEIN MD, PHD UNIVERSITY OF COLORADO SCHOOL OF MEDICINE DIVISION OF ENDOCRINOLOGY, METABOLISM AND DIABETES DIVISION OF BIOMEDICAL
Overview Endocrinology and VHL: The adrenal and the pancreas LAUREN FISHBEIN MD, PHD UNIVERSITY OF COLORADO SCHOOL OF MEDICINE DIVISION OF ENDOCRINOLOGY, METABOLISM AND DIABETES DIVISION OF BIOMEDICAL
Index. Surg Oncol Clin N Am 15 (2006) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Treatment algorithm Neuroendocrine tumours. Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece
 Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Physiological processes in the GI tract:
 Gastrointestinal physiology for medical students General principal of gastrointestinal function Motility, nervous control and blood circulation Physiological processes in the GI tract: Motility Secretion
Gastrointestinal physiology for medical students General principal of gastrointestinal function Motility, nervous control and blood circulation Physiological processes in the GI tract: Motility Secretion
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Gastrointestinal Carcinoid Tumor Early Detection, Diagnosis, and Staging
 Gastrointestinal Carcinoid Tumor Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
Gastrointestinal Carcinoid Tumor Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Images In Gastroenterology
 Images In Gastroenterology Thong-Ngam D, et al. THAI J GASTROENTEROL 2005 Vol. 6 No. 2 May - Aug. 2005 105 Imaging of Gastrointestinal Stromal Tumors Pornpim Fuangtharnthip, M.D. Narumol Hargroove, M.D.
Images In Gastroenterology Thong-Ngam D, et al. THAI J GASTROENTEROL 2005 Vol. 6 No. 2 May - Aug. 2005 105 Imaging of Gastrointestinal Stromal Tumors Pornpim Fuangtharnthip, M.D. Narumol Hargroove, M.D.
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ.
 Professor of Surgery, Taibah Univ.") By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
By Prof. Mohamed Khaled Zaky, MB,BCh; MSc; MD; FRCSI (Gen. Surg.) Professor of Surgery, Taibah Univ. Objectives Types Incidence Risk factors (& prevention) Pathology: Gross, microscopic, spread, staging,
B Breast cancer, managing risk of lobular, in hereditary diffuse gastric cancer, 51
 Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Index Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, gastric. See also Gastric cancer. D2 nodal dissection for 57 70 Adjuvant therapy, for gastric cancer, impact of D2 dissection
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC
 Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
Update on the pathological classification of gastritis. Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada
 Update on the pathological classification of gastritis Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada CLASSIFICATION GASTRITIS GASTROPATHY 1. Acute 2. Chronic 3. Uncommon
Update on the pathological classification of gastritis Hala El-Zimaity, M.D. M.S. Epidemiology McMaster University Hamilton, Ontario Canada CLASSIFICATION GASTRITIS GASTROPATHY 1. Acute 2. Chronic 3. Uncommon
Patient. Male 76 year old C.C: abdominal pain
 Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Patient Male 76 year old C.C: abdominal pain Bowel stool retention Suspected pulmonary TB at right upper lung Infiltration in right lower lung Pleural thickening at the Right chest Localized dilated small
Diagnosis abnormal morphology and /or abnormal biochemistry
 Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
Diagnosis abnormal morphology and /or abnormal biochemistry MEN 1 GEP Tumours Pancreatico-Nodal (-Duodenal) Affects 35-80% of MEN1 patients Functioning or non functioning Hyperplasia microadenoma macrotumours
Neuroendocrine Tumors
 Neuroendocrine Tumors FCDS Annual Conference Boca Raton Marriott at Boca Center July 28, 2016 Steven Peace, BS, CTR Anatomy and Physiology of the (Neuro)Endocrine System WHO Classification, Tumor Grade
Neuroendocrine Tumors FCDS Annual Conference Boca Raton Marriott at Boca Center July 28, 2016 Steven Peace, BS, CTR Anatomy and Physiology of the (Neuro)Endocrine System WHO Classification, Tumor Grade
Gastrointestinal Anatomy and Physiology. Bio 219 Napa Valley College Dr. Adam Ross
 Gastrointestinal Anatomy and Physiology Bio 219 Napa Valley College Dr. Adam Ross Functions of digestive system Digestion Breakdown of food (chemically) using enzymes, acid, and water Absorption Nutrients,
Gastrointestinal Anatomy and Physiology Bio 219 Napa Valley College Dr. Adam Ross Functions of digestive system Digestion Breakdown of food (chemically) using enzymes, acid, and water Absorption Nutrients,
Overview of digestion
 Key concepts in Digestion. Overview of digestion introduction to the GI system Prof. Barry Campbell Cellular & Molecular Physiology e-mail: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl DIGESTION
Key concepts in Digestion. Overview of digestion introduction to the GI system Prof. Barry Campbell Cellular & Molecular Physiology e-mail: bjcampbl@liv.ac.uk http://pcwww.liv.ac.uk/~bjcampbl DIGESTION
Polypoid lesions of the gastrointestinal tract
 Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015 Polypoid lesions
Polypoid lesions of the gastrointestinal tract Professor Neil A Shepherd Gloucester & Cheltenham, UK 27 th IAP-AD Congress 2 nd Emirates Surgical Pathology Conference Dubai, 26 November 2015 Polypoid lesions
DIGESTIVE TRACT ESOPHAGUS
 DIGESTIVE TRACT From the lower esophagus to the lower rectum four fundamental layers comprise the wall of the digestive tube: mucosa, submucosa, muscularis propria (externa), and adventitia or serosa (see
DIGESTIVE TRACT From the lower esophagus to the lower rectum four fundamental layers comprise the wall of the digestive tube: mucosa, submucosa, muscularis propria (externa), and adventitia or serosa (see
[A RESEARCH COORDINATOR S GUIDE]
![[A RESEARCH COORDINATOR S GUIDE]](/thumbs/88/117127924.jpg "[A RESEARCH COORDINATOR S GUIDE]") 2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
2013 COLORECTAL SURGERY GROUP Dr. Carl J. Brown Dr. Ahmer A. Karimuddin Dr. P. Terry Phang Dr. Manoj J. Raval Authored by Jennifer Lee A cartoon about colonoscopies. 1 [A RESEARCH COORDINATOR S GUIDE]
NET / GIST / MEN. 2014/2015 FCDS Educational Webcast Series. October 16, Steven Peace, CTR
 NET / GIST / MEN 2014/2015 FCDS Educational Webcast Series October 16, 2014 Steven Peace, CTR Anatomy and Physiology of the (Neuro)Endocrine System WHO Classification, Tumor Grade, Hereditary Syndromes
NET / GIST / MEN 2014/2015 FCDS Educational Webcast Series October 16, 2014 Steven Peace, CTR Anatomy and Physiology of the (Neuro)Endocrine System WHO Classification, Tumor Grade, Hereditary Syndromes
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Zollinger-Ellison Syndrome
 Zollinger-Ellison Syndrome National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is Zollinger-Ellison syndrome (ZES)? ZES
Zollinger-Ellison Syndrome National Digestive Diseases Information Clearinghouse U.S. Department of Health and Human Services NATIONAL INSTITUTES OF HEALTH What is Zollinger-Ellison syndrome (ZES)? ZES
Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
 Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
Hindawi Publishing Corporation Journal of Oncology Volume 2008, Article ID 212067, 5 pages doi:10.1155/2008/212067 Clinical Study Small Bowel Tumors: Clinical Presentation, Prognosis, and Outcomein33PatientsinaTertiaryCareCenter
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Tumor markers. Chromogranin A. Analyte Information
 Tumor markers Chromogranin A Analyte Information -1-2018-04-22 Chromogranin A Introduction Chromogranin A (CgA) is a 439-amino acid protein with a molecular weight of 48 to 60 kda, depending on glycosylation
Tumor markers Chromogranin A Analyte Information -1-2018-04-22 Chromogranin A Introduction Chromogranin A (CgA) is a 439-amino acid protein with a molecular weight of 48 to 60 kda, depending on glycosylation
BC CRC Update Unusual Colorectal Tumors
 BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
BC CRC Update Unusual Colorectal Tumors Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary I
Radiology Pathology Conference
 Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Radiology Pathology Conference Nadia F. Yusaf, M.D. PGY-3 1/29/2010 Presentation material is for education purposes only. All rights reserved. 2010 URMC Radiology Page 1 of 90 Case 1 60 year- old man presents
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Community Case. Saeed Awan R5
 Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Clinicopathologic Spectrum of Gastrointestinal Stromal Tumours; Six Years Experience at King Hussein Medical Center
 Clinicopathologic Spectrum of Gastrointestinal Stromal Tumours; Six Years Experience at King Hussein Medical Center Sahem T. Alqusous MD*, Osama J. Rabadi MD, MRCS*, Ala D. Al Omari MD*, Nabeeha N.Abbasi
Clinicopathologic Spectrum of Gastrointestinal Stromal Tumours; Six Years Experience at King Hussein Medical Center Sahem T. Alqusous MD*, Osama J. Rabadi MD, MRCS*, Ala D. Al Omari MD*, Nabeeha N.Abbasi
Imaging of Neuroendocrine Metastases
 Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Gastrointestinal Malignancies. Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline
 Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
Gastrointestinal Malignancies Dr Rodney ITAKI Pathology Division, SMHS, UPNG Anatomical Pathology Discipline Esophagus normal anatomy Hollow tube 23-25cm long in adults Extends from pharynx to level of
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear
: CT, MRI, EUS, Nuclear") Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
Imaging Pancreatic Neuroendocrine Tumors (PNETs): CT, MRI, EUS, Nuclear Eric Tamm, M.D. Department of Diagnostic Radiology Division of Diagnostic Imaging MD Anderson Cancer Center Houston, TX Disclosure
27
 26 27 28 29 30 31 32 33 34 35 Diagnosis:? Diagnosis: Juvenile Polyposis with BMPR1A Mutation 36 Juvenile Polyposis Syndrome Rare Autosomal Dominant Disorder with Multiple Juvenile Polyps in GI Tract Juvenile
26 27 28 29 30 31 32 33 34 35 Diagnosis:? Diagnosis: Juvenile Polyposis with BMPR1A Mutation 36 Juvenile Polyposis Syndrome Rare Autosomal Dominant Disorder with Multiple Juvenile Polyps in GI Tract Juvenile
Alimentary Canal (I)
") Alimentary Canal (I) Esophagus and Stomach (Objectives) By the end of this lecture, the student should be able to discuss the microscopic structure in correlation with the function of the following organs:
Alimentary Canal (I) Esophagus and Stomach (Objectives) By the end of this lecture, the student should be able to discuss the microscopic structure in correlation with the function of the following organs:
How good is EUS in the diagnosis of submucosal mass lesion
 How good is EUS in the diagnosis of submucosal mass lesion Dr. Yuk Tong LEE MBChB, MD(CUHK), FRCP (Edin), FRCP(Lond), FHKCP, FHKAM Specialist in Gastroenterology and Hepatology Submucosal tumour, SMT Subepithelial
How good is EUS in the diagnosis of submucosal mass lesion Dr. Yuk Tong LEE MBChB, MD(CUHK), FRCP (Edin), FRCP(Lond), FHKCP, FHKAM Specialist in Gastroenterology and Hepatology Submucosal tumour, SMT Subepithelial
Original Report. Carcinoid Tumors of the Stomach: A Clinical and Radiographic Study
 Aaron J. Binstock 1 C. Daniel Johnson 1 David H. Stephens 1 Ricardo V. Lloyd 2 Joel G. Fletcher 1 Received July 25, 2000; accepted after revision September 29, 2000. 1 Department of Radiology, Mayo Clinic,
Aaron J. Binstock 1 C. Daniel Johnson 1 David H. Stephens 1 Ricardo V. Lloyd 2 Joel G. Fletcher 1 Received July 25, 2000; accepted after revision September 29, 2000. 1 Department of Radiology, Mayo Clinic,
Neuroendocrine tumors of GI and Pancreatobiliary tracts. N. Volkan Adsay, MD
 Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
Neuroendocrine tumors of GI and Pancreatobiliary tracts N. Volkan Adsay, MD New (2017) WHO WHO 2017 (endocrine book; for pancreas) WHO 2017 (endocrine book; for pancreas) PD-NE ca WD-NE Tumor Intended
A VIPER IN THE COURTYARD L A I L A ABUZA I D, M D
 A VIPER IN THE COURTYARD L A I L A ABUZA I D, M D E N D O C R I N O L O G Y FELLOW NO DISCOLSURES OBJECTIVES: Recognize signs and symptoms of hyperthyroidism Develop a differential diagnosis for a patient
A VIPER IN THE COURTYARD L A I L A ABUZA I D, M D E N D O C R I N O L O G Y FELLOW NO DISCOLSURES OBJECTIVES: Recognize signs and symptoms of hyperthyroidism Develop a differential diagnosis for a patient
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
An Unexpected Cause of Hypoglycemia
 An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
An Unexpected Cause of Hypoglycemia Stacey A. Milan, MD FACS Surgical Oncology Nothing to disclose Disclosures Objectives Identify indications for workup of hypoglycemia Define work up for hypoglycemic
Polyps in general: is a descriptive term of forming a mass that is exophytic & polypoid.
 ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
ميحرلا نمحرلا هللا مسب Gastric Tumors: Benign tumours & tumor-like conditions: -Mucosal: Gastric polyps (they are uncommon) -Mesenchymal tumours: Leiomyoma & Lipoma (can occur anywhere in the body) Malignant:
Multi-cystic gist of stomach: an unusual presentation as obstructive jaundice.
 Multi-cystic gist of stomach: an unusual presentation as obstructive jaundice. Dr. Kirankumar P. Jadhav *, Prof. Dr. Sanjiv S. Thakur**Prof. Dr. Ajay S. Chandanwalle*** Dr. Schin M. Kharat****, Dr. Chhaya
Multi-cystic gist of stomach: an unusual presentation as obstructive jaundice. Dr. Kirankumar P. Jadhav *, Prof. Dr. Sanjiv S. Thakur**Prof. Dr. Ajay S. Chandanwalle*** Dr. Schin M. Kharat****, Dr. Chhaya
HISTOLOGY. GIT Block 432 Histology Team. Lecture 1: Alimentary Canal (1) (Esophagus & Stomach) Done by: Ethar Alqarni Reviewed by: Ibrahim Alfuraih
 (Esophagus & Stomach) Done by: Ethar Alqarni Reviewed by: Ibrahim Alfuraih") HISTOLOGY Lecture 1: Alimentary Canal (1) (Esophagus & Stomach) Done by: Ethar Alqarni Reviewed by: Ibrahim Alfuraih Color Guide: Black: Slides. Red: Important. Green: Doctor s notes. Blue: Explanation.
HISTOLOGY Lecture 1: Alimentary Canal (1) (Esophagus & Stomach) Done by: Ethar Alqarni Reviewed by: Ibrahim Alfuraih Color Guide: Black: Slides. Red: Important. Green: Doctor s notes. Blue: Explanation.
Histopathology: gastritis and peptic ulceration
 Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Histopathology: gastritis and peptic ulceration These presentations are to help you identify, and to test yourself on identifying, basic histopathological features. They do not contain the additional factual
Pancreatic Cancer Early Detection, Diagnosis, and Staging
 Pancreatic Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can
Pancreatic Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can
Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization
 Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization JP King PGY2 May 22, 2015 Neuroendocrine Tumor (NET) WHO Classification Location
Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization JP King PGY2 May 22, 2015 Neuroendocrine Tumor (NET) WHO Classification Location
EXOCRINE: 93% Acinar Cells Duct Cells. ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others
 EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
Anatomy of the biliary tract
 Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Harvard-MIT Division of Health Sciences and Technology HST.121: Gastroenterology, Fall 2005 Instructors: Dr. Jonathan Glickman Anatomy of the biliary tract Figure removed due to copyright reasons. Biliary
Learning. A part of your guide to Neuroendocrine Tumours (NETs)
") Learning A part of your guide to Neuroendocrine Tumours (NETs) Your support guide This book will help you better understand NETs. It is however a reference only; you should always go to your doctor or
Learning A part of your guide to Neuroendocrine Tumours (NETs) Your support guide This book will help you better understand NETs. It is however a reference only; you should always go to your doctor or