Diagnosis and what happens after referral
|
|
|
- Corey Chandler
- 5 years ago
- Views:
Transcription

1 Diagnosis and what happens after referral Dr Kate Newbold Consultant in Clinical Oncology The Royal Marsden Women's cancers Breast cancer introduction 1
2 Treatment Modalities Early stage disease -larynx and naso/oro/hypopharynx: RT alone -oral cavity: surgery alone Advanced stage naso/oro/hypophrynx and larynx - organ preservation - radical chemoradiotherapy Advanced stage oral cavity/paranasal sinuses -primary surgery -adjuvant (chemo)radiotherapy
3 Early Stage disease Early Larynx -T1-2 N0 larynx -3.5 to 4 weeks of daily RT fractions Stage I-II naso/oro/hypopharynx - 6 weeks of daily RT alone - 30 fractions
4 Advanced Stage disease Stage III larynx -Induction chemotherapy and chemoradiotherapy Stage IV larynx -Laryngectomy Stage III-IV naso/oro/hypopharynx -Induction chemotherapy and chemoradiotherapy
5 5 The Royal Marsden Q: What is the 2 year survival rate for stage I-II head and neck cancer? 1. <20% 25% 25% 25% 25% % % 4. >70% <20% 20-50% 50-70% >70%
6 6 The Royal Marsden Q: What is the 2 year survival rate for stage III-IV head and neck cancer? 1. <20% 25% 25% 25% 25% % % 4. >70% <20% 20-50% 50-70% >70%
7 2 year survival rates (CRUK) Table 3.1: Stage and two-year crude survival, cancers of the oral cavity and pharynx, South and West of England, Oral cavity 2-year crude Pharynx 2-year crude No. of cases survival (CI) No. of cases survival (CI) % % All cases ( ) ( ) I Early disease ( ) ( ) II Locally advanced ( ) ( ) III Tumour in lymph nodes ( ) ( ) IV Metastatic ( ) ( ) Unknown ( ) ( )
8 Sequential induction chemotherapy followed by radical chemo-radiation in the treatment of locoregionally advanced head and neck cancer Bhide et al, BJC 2008 LC 72% at 2 years OS 63% at 2 years

9 2 year overall survival 86.7% 2 year PFS -Oral cavity 86% -Nasopharynx 94% -Oropharynx 84% -Pharyngolarynx 83% Radiotherapy and Oncology
10 Case study - Oropharynx 48 yr old accountant Presents with 2/12 history right sided otalgia Then noted right neck lump Married, non smoker, moderate alcohol, 2 children aged 10 and 12
11 11 The Royal Marsden Q: What would you do? 25% 25% 25% 25% A. Prescribe antibiotics B. Refer non-urgently for imaging C. Refer under 2ww D. Reassure A. B. C. D.
12 12 The Royal Marsden Q: If this patient was a smoker, would this have affected your decision? A. Yes B. No 50% 50% A. B.
13 Case study - Oropharynx The patient was prescribed antibiotics which showed no improvement, and was then referred. After investigation, it was discovered they had pct2 cn2b cm0 SCC p16+ right tonsil/base of tongue.
14 14 The Royal Marsden Q: What treatment option should be taken? A. Surgery 25% 25% 25% 25% B. Induction chemo followed by chemoradiation C. Chemoradiation D. Chemotherapy A. B. C. D.
15 Induction Chemotherapy Blanchard, P., et al., J Clin Oncol, (23): p Tax-PF was associated with significant reductions of progression, locoregional failure, and distant failure compared with PF, with HRs of 0.78 (95% CI, 0.69 to 0.87; P <.001), 0.79 (95% CI, 0.66 to 0.94; P =.007), and 0.63 (95% CI, 0.45 to 0.89; P =.009) respectively Currently for locally advanced disease T4 and/or N2B
16 Induction chemotherapy Evidence for chemotherapy in addition to radiotherapy in patients 70 years 2 x 21 day cycles of induction chemotherapy -Taxotere (75 mg/m2) day 1, Cisplatin (75 mg/m2) day1 and 5- Fluorouracil (750 mg/m2) days days inpatient -SEs: myelosuppression nausea and vomiting hair loss neuropathy tinnitus/hearing loss nephrotoxicity fertility Consider ambulatory in appropriate cases



17 Oropharynx 48 yr old professional Presents with 2/12 history right sided otalgia Then noted right neck lump Received antibx initially with no improvement Married, non smoker, moderate alcohol, ct2 cn2b cm0 SCC p16+ right tonsil/base of tongue
18 Delineation of Prognostic Groups
19 Chemoradiotherapy 6 weeks, 30 fractions OP treatment, mon fri Concomitant cisplatin chemo Day 1 and 29 of radiotherapy. Overnight stay
20 Preparation for chemoradiotherapy Women's cancers Breast cancer introduction 20
21 21 The Royal Marsden Q: Why do we perform dental assessment before radical radiotherapy? 25% 25% 25% 25% A. To make radiotherapy delivery easier B. To improve radiation dose homogeneity C. To reduce risk of osteoradionecrosis D. To reduce risk of infection A. B. C. D.
22 Preparation for Chemoradiotherapy (1) Dental assessment -RT causes xerostomia -RT reduces vasculaity of mandible Aim to prevent osteoradionecrosis Require OPG and review by oral surgeon/restorative dentist At least 14 days required between extractions and start RT
23 23 The Royal Marsden Q: Which should patients stop during treatment? A. Alcohol 25% 25% 25% 25% B. Smoking C. Dairy products D. Red meat A. B. C. D.
24 Preparation for Chemoradiotherapy (2) Nutrition -dietetic review -risk of re-feeding syndrome -degree of poor/malnutrition Alcohol -assess for risk of withdrawal Smoking -reduces rate of cure by 30% -increases treatment induced toxicty -offer cessation advice and help in conjunction with GP
25 Preparation for Chemoradiotherapy (3) Renal function -EDTA or Cockcroft calculation -GFR >60ml/min proceed with cisplatin -GFR <60ml/min consider carboplatin or cetuximab Hearing -if reduced hearing or pre-existing tinnitus -consider switching cisplatin to carboplatin or cetuximab
26 Preparation for Chemoradiotherapy (4) If cardiac pacemaker or implantable defibrillator - needs review by cardiac technologists -may need daily monitoring during treatment
27 Radiotherapy Planning Women's cancers Breast cancer introduction 27




28 Mould Room


29 Set-up on LINAC

30 Treatment planning

31 CT planning - 3D Reconstruction

32 CT Planning - dose calculation
33 Intensity-Modulated Radiotherapy (IMRT) Women's cancers Breast cancer introduction 33
34 What is Intensity Modulated Radiotherapy? Tumour Dose Conventional Radiotherapy Tissue Intensity Modulated Radiotherapy
35

36 Treatment planning

37 Linear Accelerator
38 Toxicity of radiotherapy normal tissue tolerance depends on total volume irradiated total dose fractionation schedule ie size of each fraction, number of fractions, duration of treatment previous surgery co-existing problems eg smoking, drinking, chronic disease
39 Toxicity of radiotherapy Early -2-3 weeks into treatment -reversible - settle within 4-6 weeks of completion of treatment -present to some degree in all patients -severity does not predict for late toxicity Late -6-9 months post RT -tends to be permanent, may be progressive -5-10% of patients will develop severe toxicity


40 Toxicity of radiotherapy early Skin erythema dry desquamation moist desquamation hair loss



41 Toxicity of Radiotherapy- early Mucous membranes loss of taste, dry mouth, dysphagia, mucositis
42 Loss of taste Damage to the circumvallate and fungiform papillae after 20Gy Bitter/sour affected more than sweet/salty Partial/complete recovery is usual but recovery can be slow
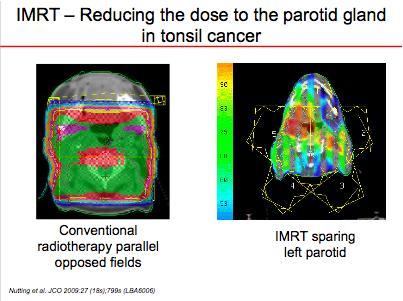
43 Xerostomia Major salivary glands produce 90% saliva Parotid gland often in irradiated volume The serous acini are more sensitive than the mucous acini, resulting in production of thick saliva Change in oral flora
44 Toxicity - late Skin -alopecia -oedema / fibrosis -Depigmentation Salivary glands -Xerostomia Dental Hearing -EAM -Middle ear -Cochlea Spinal cord -Lhermittes synd -Myelitis


45 Late Toxicity -Skin/Soft tissues

46 Osteoradionecrosis Occurs in the mandible Hypoxia and hypovascularity Related to Total dose Dose/# Brachytherapy Chemotherapy?
47 47 The Royal Marsden Q: Do breaks or gaps in radiotherapy: 25% 25% 25% 25% A. Reduce overall survival B. Reduce local control C. Reduce acute toxicity D. Reduce late toxicity A. B. C. D.
48 Importance of Overall Time of Treatment Decreased tumour control probability (TCP) when same dose is delivered over longer time Need to deliver higher dose to maintain TCP if treatment duration prolonged Explained by rapid repopulation in response to clonogenic cell depletion during RT
49 K. Kian Ang, 2001: Interval between Surgery and PORT
50 K. Kian Ang, 2001: Cumulative time of combined modality
51 Conclusion The Challenge -advanced disease -function preservation, cosmesis -proximity of critical structures -compliance -nutrition
52 MDT ENT Maxillo-Facial Plastics Restorative Dentists Clinical Oncologists Palliative Care Radiologists Histopathologists Cytopathologists Psychologist/psychiatrist SALT Dietitians Clinical Nurse Specialists Research Nurses Social Worker Physicists Radiographers Prosthetics Primary Care
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
Oral cavity cancer Post-operative treatment
 Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Oral cavity cancer Post-operative treatment Dr. Christos CHRISTOPOULOS Radiation Oncologist Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Important issues RT -techniques Patient selection
Principles of Management of Head & Neck Cancer. Jinka Sathya Associate professor of Oncology
 Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Principles of Management of Head & Neck Cancer Jinka Sathya Associate professor of Oncology Oral cavity Oro-pharynx Larynx Hypopharynx Nasophaynx Major sites of Mucosal H&N Cancers Head & Neck Cancer Oral
Head and neck cancer - patient information guide
 Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Head and neck cancer - patient information guide The development of reconstructive surgical techniques in the last 20 years has led to major advances in the treatment of patients with head and neck cancer.
Introduction to clinical Radiotherapy
 Introduction to clinical Radiotherapy Sarah Brothwood Radiotherapy Practice Educator Rosemere Cancer Centre Sarah.brothwood@lthtr.nhs.uk 01772 522694 Radiotherapy We have been able to see and document
Introduction to clinical Radiotherapy Sarah Brothwood Radiotherapy Practice Educator Rosemere Cancer Centre Sarah.brothwood@lthtr.nhs.uk 01772 522694 Radiotherapy We have been able to see and document
What is head and neck cancer? How is head and neck cancer diagnosed and evaluated? How is head and neck cancer treated?
 Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that start in the oral cavity, larynx, pharynx, salivary glands, nasal cavity or paranasal sinuses. They usually begin
Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that start in the oral cavity, larynx, pharynx, salivary glands, nasal cavity or paranasal sinuses. They usually begin
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy
 TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
TREATMENT TIME & TOBACCO: TWIN TERRORS Of H&N Therapy Anurag K. Singh, MD Professor of Medicine University at Buffalo School of Medicine Professor of Oncology Director of Radiation Research Roswell Park
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
Radiotherapy to the face or neck (shell)
") Radiotherapy to the face or neck (shell) The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer
Radiotherapy to the face or neck (shell) The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer
IMRT - Intensity Modulated Radiotherapy
 IMRT - Intensity Modulated Radiotherapy Advanced product in the RT technology Aims to deliver radiation more precisely to the tumor, while relatively limiting dose to the surrounding normal tissues 7 position
IMRT - Intensity Modulated Radiotherapy Advanced product in the RT technology Aims to deliver radiation more precisely to the tumor, while relatively limiting dose to the surrounding normal tissues 7 position
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Cisplatin100 plus Radiotherapy for locally Advanced Squamous Cell Carcinoma Head and Neck
 Cisplatin100 plus Radiotherapy for locally Advanced Squamous Cell Carcinoma Head and Neck Indication: 1) Concomitant chemo-radiotherapy for locally advanced squamous cell carcinoma head and neck 2) Post-operative
Cisplatin100 plus Radiotherapy for locally Advanced Squamous Cell Carcinoma Head and Neck Indication: 1) Concomitant chemo-radiotherapy for locally advanced squamous cell carcinoma head and neck 2) Post-operative
PRINCIPLES OF RADIATION ONCOLOGY
 PRINCIPLES OF RADIATION ONCOLOGY Ravi Pachigolla, MD Faculty Advisor: Anna Pou, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2000 HISTORY
PRINCIPLES OF RADIATION ONCOLOGY Ravi Pachigolla, MD Faculty Advisor: Anna Pou, MD The University of Texas Medical Branch Department of Otolaryngology Grand Rounds Presentation January 5, 2000 HISTORY
Radiotherapy Physics and Equipment
 Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
Radiological Sciences Department Radiotherapy Physics and Equipment RAD 481 Lecture s Title: Introduction Dr. Mohammed EMAM Ph.D., Paris-Sud 11 University Vision :IMC aspires to be a leader in applied
Neoplasie del laringe Diagnosi e trattamento
 Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Head and Neck Cancer. What is head and neck cancer?
 Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that usually originate in the squamous cells that line the mouth, nose and throat. Typical symptoms include a persistent
Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that usually originate in the squamous cells that line the mouth, nose and throat. Typical symptoms include a persistent
Head and Neck Reirradiation: Perils and Practice
 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Unknown primary cancer
 Unknown primary cancer The name Beyond Five refers to the long-term support that patients with head and neck cancer often need, which often extends beyond five years after diagnosis. CANCER OF UNKNOWN
Unknown primary cancer The name Beyond Five refers to the long-term support that patients with head and neck cancer often need, which often extends beyond five years after diagnosis. CANCER OF UNKNOWN
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck. Mei Tang, MD
 Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
SAMO MASTERCLASS HEAD & NECK CANCER. Nicolas Mach, PD Geneva University Hospital
 SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology
 Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
Goals and Objectives: Head and Neck Cancer Service Department of Radiation Oncology The head and neck cancer service provides training in the diagnosis, management, treatment, and follow-up care of head
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer
 to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer") The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
North of Scotland Cancer Network Clinical Management Guideline for Oropharyngeal Cancer
 Nth of Scotland Cancer Netwk Clinical Management Guideline f Oropharyngeal Cancer UNCONTROLLED WHEN PRINTED Based on NHST CMG with further extensive consultation within NOSCAN DOCUMENT CONTROL Original
Nth of Scotland Cancer Netwk Clinical Management Guideline f Oropharyngeal Cancer UNCONTROLLED WHEN PRINTED Based on NHST CMG with further extensive consultation within NOSCAN DOCUMENT CONTROL Original
Head and Neck Cancer Treatment
 Scan for mobile link. Head and Neck Cancer Treatment Head and neck cancer overview The way a particular head and neck cancer behaves depends on the site in which it arises (the primary site). For example,
Scan for mobile link. Head and Neck Cancer Treatment Head and neck cancer overview The way a particular head and neck cancer behaves depends on the site in which it arises (the primary site). For example,
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Cisplatin Vinorelbine (Oral) therapy +/- radiotherapy
 therapy +/- radiotherapy") 1 REGIMEN TITLE: Cisplatin Vinorelbine (Oral) therapy +/- radiotherapy Page 1 of 5 Indication: First line in Radical/ Induction, Adjuvant and Advanced & Palliative treatment of Non-small cell lung cancer
1 REGIMEN TITLE: Cisplatin Vinorelbine (Oral) therapy +/- radiotherapy Page 1 of 5 Indication: First line in Radical/ Induction, Adjuvant and Advanced & Palliative treatment of Non-small cell lung cancer
Nasopharyngeal Cancer:Role of Chemotherapy
 Nasopharyngeal Cancer:Role of Chemotherapy PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 16/9/2017 2 nd Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Nasopharyngeal Cancer:Role of Chemotherapy PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 16/9/2017 2 nd Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
First, how does radiation work?
 Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Hello, I am Prajnan Das, Faculty Member in the Department of Radiation Oncology at The University of Texas MD Anderson Cancer Center. We are going to talk today about some of the basic principles regarding
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Head and Neck Cancer Service
 Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. Head and Neck Cancer Service Dr Hoda Al Booz Consultant in Clinical Oncology Bristol Cancer Institute Dr Hoda Al Booz. MMedSci, MD, FFRRCSI, FRCR. documents/
Clinical Discussion. Dr Pankaj Chaturvedi. Professor and Surgeon Tata Memorial Hospital
 Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Clinical Discussion Dr Pankaj Chaturvedi Professor and Surgeon Tata Memorial Hospital chaturvedi.pankaj@gmail.com 47/M/smoker Hopkins : Transglottic lesion No cartilage infiltration but sclerosis Left
Radiation Treatment for Breast. Cancer. Melissa James Radiation Oncologist August 2015
 Radiation Treatment for Breast Cancer Melissa James Radiation Oncologist August 2015 OUTLINE External Beam Radiation treatment. (What is Radiation, doctor?) Role of radiation. (Why am I getting radiation,
Radiation Treatment for Breast Cancer Melissa James Radiation Oncologist August 2015 OUTLINE External Beam Radiation treatment. (What is Radiation, doctor?) Role of radiation. (Why am I getting radiation,
Neodjuvant chemotherapy
 Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Dietetic support following treatment for Head and Neck cancer
 Dietetic support following treatment for Head and Neck cancer Laura Askins Specialist Dietitian The Royal Marsden Discussion points: Reported concerns Issues in achieving an adequate nutritional status
Dietetic support following treatment for Head and Neck cancer Laura Askins Specialist Dietitian The Royal Marsden Discussion points: Reported concerns Issues in achieving an adequate nutritional status
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no
 67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
67 F, 40 PY Smoker, Past heavy alcohol consumer, h/o COPD, Congestive heart failure. Presentation: Lump left upper neck x 1 year, non-tender, no overlying skin changes, gradually increasing in size. Recent
Nasopharynx Cancer. 1 Feb Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar)
 Dr Peter Luk (Pathology Registrar)") Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Nasopharyngeal Cancer/Multimodality Treatment
 Nasopharyngeal Cancer/Multimodality Treatment PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 22/10/2016 1 st Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Nasopharyngeal Cancer/Multimodality Treatment PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 22/10/2016 1 st Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
State of the art for radiotherapy of SCCHN
 State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
Radiotherapy to one side of the mouth and neck
 Clinical Oncology Radiotherapy to one side of the mouth and neck Consent information for patients Radiotherapy may be given on its own or with chemotherapy (separate information will be given about chemotherapy).
Clinical Oncology Radiotherapy to one side of the mouth and neck Consent information for patients Radiotherapy may be given on its own or with chemotherapy (separate information will be given about chemotherapy).
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS
 MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
Audit on Hospitalisation during (Chemo)Radiotherapy for Head and Neck Cancers
Radiotherapy for Head and Neck Cancers") Audit on Hospitalisation during (Chemo)Radiotherapy for Head and Neck Cancers NESCN Head & Neck NSSG David Wilkinson ST7 Clinical Oncology 4 th March 2015 Background CRT & RT can cure inoperable H&N cancer
Audit on Hospitalisation during (Chemo)Radiotherapy for Head and Neck Cancers NESCN Head & Neck NSSG David Wilkinson ST7 Clinical Oncology 4 th March 2015 Background CRT & RT can cure inoperable H&N cancer
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej. The role of brachytherapy in recurrent. oral cavity
 Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
Rola brachyterapii w leczeniu wznów nowotworów języka i dna jamy ustnej The role of brachytherapy in recurrent tumours of the tongue and fundus of the oral cavity Janusz Skowronek, MD, PhD, Ass. Prof.
Standard care plan for Carboplatin and Etoposide Chemotherapy References
 CHEMOTHERAPY CARE PLAN Document Title: Document Type: Subject: Approved by: Currency: Carboplatin/Etoposide Chemotherapy Clinical Guideline Standard Care Plan 2 Years Review date: Author(s): Standard care
CHEMOTHERAPY CARE PLAN Document Title: Document Type: Subject: Approved by: Currency: Carboplatin/Etoposide Chemotherapy Clinical Guideline Standard Care Plan 2 Years Review date: Author(s): Standard care
I am writing in response to your request for information made under the Freedom of Information Act 2000 in relation to head and neck cancer.
 Ref: FOI/CAD/ID 3000 20 November 2015 Please reply to: FOI Administrator Trust Management Service Centre Maidstone Hospital Hermitage Lane Maidstone Kent ME16 9QQ Email: mtw-tr.foiadmin@nhs.net Freedom
Ref: FOI/CAD/ID 3000 20 November 2015 Please reply to: FOI Administrator Trust Management Service Centre Maidstone Hospital Hermitage Lane Maidstone Kent ME16 9QQ Email: mtw-tr.foiadmin@nhs.net Freedom
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Radiotherapy for lymphoma
 Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
Radiotherapy for lymphoma The name of your consultant is: The radiographer who explained the treatment to you is: You can contact us on: What is radiotherapy? Radiotherapy treats cancer by using high energy
Head and Neck Cancer surgeon level data - first report. Queen Victoria Hospital NHS Foundation Trust
 Head and Neck Cancer surgeon level data - first report Queen Victoria Hospital NHS Foundation Trust 1 of 8 Foreword This report for the first time presents data for individual surgeons relating to head
Head and Neck Cancer surgeon level data - first report Queen Victoria Hospital NHS Foundation Trust 1 of 8 Foreword This report for the first time presents data for individual surgeons relating to head
Lung Pathway Group Cisplatin & PO Vinorelbine in Non- Small Cell Lung Cancer (NSCLC)
") Lung Pathway Group Cisplatin & PO Vinorelbine in Non- Small Cell Lung Cancer (NSCLC) Indication: First line in radical/induction treatment in locally advanced NSCLC First line palliative treatment in advanced/metastatic
Lung Pathway Group Cisplatin & PO Vinorelbine in Non- Small Cell Lung Cancer (NSCLC) Indication: First line in radical/induction treatment in locally advanced NSCLC First line palliative treatment in advanced/metastatic
Salivary gland cancer
 Salivary gland cancer The name Beyond Five refers to the long-term support that patients with head and neck cancer often need, which often extends beyond five years after diagnosis. CONTENTS What are the
Salivary gland cancer The name Beyond Five refers to the long-term support that patients with head and neck cancer often need, which often extends beyond five years after diagnosis. CONTENTS What are the
Radiotherapy that includes the mouth and care of your teeth
 The Clatterbridge Cancer Centre NHS Foundation Trust Radiotherapy that includes the mouth and care of your teeth Radiotherapy A guide for patients and carers Contents Dental care before radiotherapy...
The Clatterbridge Cancer Centre NHS Foundation Trust Radiotherapy that includes the mouth and care of your teeth Radiotherapy A guide for patients and carers Contents Dental care before radiotherapy...
Head and Neck cancer
 Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Having radiotherapy to the head and neck
 Sussex Cancer Care Having radiotherapy to the head and neck Brighton and Sussex University Hospitals NHS Trust Disclaimer The information in this leaflet is for guidance purposes only and is in no way
Sussex Cancer Care Having radiotherapy to the head and neck Brighton and Sussex University Hospitals NHS Trust Disclaimer The information in this leaflet is for guidance purposes only and is in no way
Response Evaluation Of Accelerated Fractionation With Concomitant Boost Chemoradiation In Locally Advanced Squamous Cell Head And Neck Cancer
 IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 2 Ver. IV (Feb. 2016), PP 27-32 www.iosrjournals.org Response Evaluation Of Accelerated Fractionation
IOSR Journal of Dental and Medical Sciences (IOSR-JDMS) e-issn: 2279-0853, p-issn: 2279-0861.Volume 15, Issue 2 Ver. IV (Feb. 2016), PP 27-32 www.iosrjournals.org Response Evaluation Of Accelerated Fractionation
Radiation Therapy. This reference summary reviews what to expect during and after radiation therapy.
 Radiation Therapy Introduction Radiation therapy is a very common treatment for a variety of cancers. Radiation therapy, also called radiotherapy, is a cancer treatment that uses high doses of radiation
Radiation Therapy Introduction Radiation therapy is a very common treatment for a variety of cancers. Radiation therapy, also called radiotherapy, is a cancer treatment that uses high doses of radiation
Merck Merck response to NICE ACD: Cetuximab in the treatment of LA SCCHN: 26 th February 2007
 response to NICE ACD: Cetuximab in the treatment of LA SCCHN: 26 th February 2007 NICE Single Technology Appraisal of cetuximab for the treatment of locally advanced squamous cell carcinoma of the head
response to NICE ACD: Cetuximab in the treatment of LA SCCHN: 26 th February 2007 NICE Single Technology Appraisal of cetuximab for the treatment of locally advanced squamous cell carcinoma of the head
Laryngeal Conservation
 Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Laryngeal Conservation Sarah Rodriguez, MD Faculty Advisor: Shawn Newlands, MD, PhD The University of Texas Medical Branch Department of Otolaryngolgy Grand Rounds Presentation February 2005 Introduction
Head and NeckCancer: multi-modal therapeuticintegration
 Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Update on Sarcomas of the Head and Neck. Kevin Harrington
 Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
Update on Sarcomas of the Head and Neck Kevin Harrington Overview Classification and incidence of sarcomas Clinical presentation Challenges to treatment Management approaches Prognostic factors Radiation-induced
Head and Neck QPI Group Audit Report Head and Neck Quality Performance Indicators Consultant Clinical Oncologist, NHS Grampian
 Head and Neck QPI Group Audit Report Head and Neck Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: February 2018 Dr Rafael Moleron Consultant Clinical Oncologist, NHS
Head and Neck QPI Group Audit Report Head and Neck Quality Performance Indicators Patients diagnosed April 2016 March 2017 Published: February 2018 Dr Rafael Moleron Consultant Clinical Oncologist, NHS
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia)
") PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia) Dr. Miriam Joy C. Calaguas Dept. of Radiation Oncology St. Luke s Medical Center
PILOT STUDY OF CONCURRENT CHEMO-RADIOTHERAPY FOR ADVANCED NASOPHARYNGEAL CARCINOMA (Forum for Nuclear Cooperation in Asia) Dr. Miriam Joy C. Calaguas Dept. of Radiation Oncology St. Luke s Medical Center
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
ORAL CANCER CONTENTS Beyond Five 1
 Oral cancer The name Beyond Five refers to the long-term support that patients with head and neck cancer often need, which often extends beyond five years after diagnosis. ORAL CANCER CONTENTS Oral Cancer...
Oral cancer The name Beyond Five refers to the long-term support that patients with head and neck cancer often need, which often extends beyond five years after diagnosis. ORAL CANCER CONTENTS Oral Cancer...
Carboplatin and Fluorouracil
 Carboplatin and Fluorouracil Indication Palliative chemotherapy for recurrent or metastatic head and neck squamous cell cancer for patients where cisplatin and / or cetuximab are not appropriate. Performance
Carboplatin and Fluorouracil Indication Palliative chemotherapy for recurrent or metastatic head and neck squamous cell cancer for patients where cisplatin and / or cetuximab are not appropriate. Performance
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations
 Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Squamous Cell Carcinoma of the Oral Cavity: Radio therapeutic Considerations Troy G. Scroggins Jr. MD Chairman, Department of Radiation Oncology Ochsner Health Systems 1 Association of Postoperative Radiotherapy
Scottish Audit of Head and Neck Cancers. A Prospective Audit
 Scottish Audit of Head and Neck Cancers Steering Group Scottish Audit of Head and Neck Cancers A Prospective Audit Report 1999 2002 Edited by David Loeb and Tracey Rapson Statistical Analysis by Tracey
Scottish Audit of Head and Neck Cancers Steering Group Scottish Audit of Head and Neck Cancers A Prospective Audit Report 1999 2002 Edited by David Loeb and Tracey Rapson Statistical Analysis by Tracey
Anne Marie Brown Macmillan Head & Neck CNS
 Advances in the Treatment of Head & Neck cancer Anne Marie Brown Macmillan Head & Neck CNS Aims To provide a brief revision of Head & Neck anatomy and background statistics To demonstrate the processes
Advances in the Treatment of Head & Neck cancer Anne Marie Brown Macmillan Head & Neck CNS Aims To provide a brief revision of Head & Neck anatomy and background statistics To demonstrate the processes
Radiotherapy to the Head and Neck
 Radiotherapy to the Head and Neck Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
Radiotherapy to the Head and Neck Delivering the best in care UHB is a no smoking Trust To see all of our current patient information leaflets please visit www.uhb.nhs.uk/patient-information-leaflets.htm
5/20/ ) Haffty GB: Concurrent chemoradiation in the treatment of head and neck cancer. Hematol. Oncol. Clin: North Am.
 Haffty GB: Concurrent chemoradiation in the treatment of head and neck cancer. Hematol. Oncol. Clin: North Am.") Prague, 24-25 25 April 29 ALTERNATING CHEMORADIATION: FOR WHOM? M. Merlano MD Holy Cross Gen. Hospital Cuneo - Italy ALTERNATING CHEMORADIATION: FOR WHOM? Definition of alternating chemoradiation Targets
Prague, 24-25 25 April 29 ALTERNATING CHEMORADIATION: FOR WHOM? M. Merlano MD Holy Cross Gen. Hospital Cuneo - Italy ALTERNATING CHEMORADIATION: FOR WHOM? Definition of alternating chemoradiation Targets
Lung Pathway Group Carboplatin & PO Vinorelbine in Non-Small Cell Lung Cancer (NSCLC)
") Lung Pathway Group Carboplatin & PO Vinorelbine in Non-Small Cell Lung Cancer (NSCLC) Indication: First line in radical/induction treatment in locally advanced NSCLC First line palliative treatment in
Lung Pathway Group Carboplatin & PO Vinorelbine in Non-Small Cell Lung Cancer (NSCLC) Indication: First line in radical/induction treatment in locally advanced NSCLC First line palliative treatment in
Alberta Head and Neck Cancer Priority Setting Project
 Alberta Head and Neck Cancer Priority Setting Project About You 1. Which group best describes you? (Check all that apply). * A person diagnosed with cancer of the head and neck A family member or caregiver
Alberta Head and Neck Cancer Priority Setting Project About You 1. Which group best describes you? (Check all that apply). * A person diagnosed with cancer of the head and neck A family member or caregiver
Testicular Germ Cell Cancer Explained
 The Beatson West of Scotland Cancer Centre Pan Glasgow Urology / Oncology Patient Information Testicular Germ Cell Cancer Explained The Beatson West of Scotland Cancer Centre 1053 Great Western Road, Glasgow
The Beatson West of Scotland Cancer Centre Pan Glasgow Urology / Oncology Patient Information Testicular Germ Cell Cancer Explained The Beatson West of Scotland Cancer Centre 1053 Great Western Road, Glasgow
Oral complications: an overview DR ANDREW DAVIES FRCP CONSULTANT IN PALLIATIVE MEDICINE ROYAL SURREY COUNTY HOSPITAL, GUILDFORD, UK
 Oral complications: an overview DR ANDREW DAVIES FRCP CONSULTANT IN PALLIATIVE MEDICINE ROYAL SURREY COUNTY HOSPITAL, GUILDFORD, UK Introduction Introduction Outline: Epidemiology Aetiology Clinical features
Oral complications: an overview DR ANDREW DAVIES FRCP CONSULTANT IN PALLIATIVE MEDICINE ROYAL SURREY COUNTY HOSPITAL, GUILDFORD, UK Introduction Introduction Outline: Epidemiology Aetiology Clinical features
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
BCCA Protocol Summary for Treatment of Advanced Squamous Cell Carcinoma of the Head and Neck Cancer Using Fluorouracil and Platinum
 BCCA Protocol Summary for Treatment of Advanced Squamous Cell Carcinoma of the Head and Neck Cancer Using Fluorouracil and Platinum Protocol Code: Tumour Group: Contact Physician: HNAVFUP Head and Neck
BCCA Protocol Summary for Treatment of Advanced Squamous Cell Carcinoma of the Head and Neck Cancer Using Fluorouracil and Platinum Protocol Code: Tumour Group: Contact Physician: HNAVFUP Head and Neck
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
Side effects of radiotherapy.
 Side effects of radiotherapy. Paweł Potocki, MD Jagiellonian University Medical College Kraków University Hospital Departament of Clinical Oncology ppotocki@su.krakow.pl Basics Techniques: Radiation type:
Side effects of radiotherapy. Paweł Potocki, MD Jagiellonian University Medical College Kraków University Hospital Departament of Clinical Oncology ppotocki@su.krakow.pl Basics Techniques: Radiation type:
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
CISPLATIN Chemo-radiation regimen Gynaecological Cancer
 Systemic Anti Cancer Treatment Protocol CISPLATIN Chemo-radiation regimen Gynaecological Cancer PROCTOCOL REF: MPHAGYNCIX (Version No: 1.0) Approved for use in: Locally advanced cervical cancer (adjuvant/curative)
Systemic Anti Cancer Treatment Protocol CISPLATIN Chemo-radiation regimen Gynaecological Cancer PROCTOCOL REF: MPHAGYNCIX (Version No: 1.0) Approved for use in: Locally advanced cervical cancer (adjuvant/curative)
Citation Key for more information see:
 Citation Key for more information see: http://open.umich.edu/wiki/citationpolicy Use + Share + Adapt { Content the copyright holder, author, or law permits you to use, share and adapt. } Public Domain
Citation Key for more information see: http://open.umich.edu/wiki/citationpolicy Use + Share + Adapt { Content the copyright holder, author, or law permits you to use, share and adapt. } Public Domain
STUDY FINDINGS PRESENTED ON TAXOTERE REGIMENS IN HEAD AND NECK, LUNG AND BREAST CANCER
 Contact: Anne Bancillon + 33 (0)6 70 93 75 28 STUDY FINDINGS PRESENTED ON TAXOTERE REGIMENS IN HEAD AND NECK, LUNG AND BREAST CANCER Key results of 42 nd annual meeting of the American Society of Clinical
Contact: Anne Bancillon + 33 (0)6 70 93 75 28 STUDY FINDINGS PRESENTED ON TAXOTERE REGIMENS IN HEAD AND NECK, LUNG AND BREAST CANCER Key results of 42 nd annual meeting of the American Society of Clinical
ENDPOINTS IN ONCOLOGY- HOW LONG WILL A CANCER PATIENT SURVIVE? DR GUNJAN BAIJAL CONSULTANT RADIATION ONCOLOGY MANIPAL GOA
 ENDPOINTS IN ONCOLOGY- HOW LONG WILL A CANCER PATIENT SURVIVE? DR GUNJAN BAIJAL CONSULTANT RADIATION ONCOLOGY MANIPAL GOA Why so much of cancer today? Times have changed HISTORICAL PERSPECTIVE CANCER as
ENDPOINTS IN ONCOLOGY- HOW LONG WILL A CANCER PATIENT SURVIVE? DR GUNJAN BAIJAL CONSULTANT RADIATION ONCOLOGY MANIPAL GOA Why so much of cancer today? Times have changed HISTORICAL PERSPECTIVE CANCER as
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
Appendix 4 Urology Care Pathways
 Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
Appendix 4 Urology Care Pathways Cancer Care Pathways outline the steps and stages in the patient journey from referral through to diagnostics, staging, treatment, follow up, rehabilitation and if applicable
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Cancer of the upper aerodigestive tract: assessment and management in people aged 16 and over
 Cancer of the upper aerodigestive tract: assessment and management in people aged and over NICE guideline Draft for consultation, March 0 This guideline covers This guideline covers assessing and managing
Cancer of the upper aerodigestive tract: assessment and management in people aged and over NICE guideline Draft for consultation, March 0 This guideline covers This guideline covers assessing and managing
HDR Brachytherapy for Skin Cancers. Joseph Lee, M.D., Ph.D. Radiation Oncology Associates Fairfax Hospital
 HDR Brachytherapy for Skin Cancers Joseph Lee, M.D., Ph.D. Radiation Oncology Associates Fairfax Hospital No conflicts of interest Outline Case examples from Fairfax Hospital Understand radiation s mechanism
HDR Brachytherapy for Skin Cancers Joseph Lee, M.D., Ph.D. Radiation Oncology Associates Fairfax Hospital No conflicts of interest Outline Case examples from Fairfax Hospital Understand radiation s mechanism
Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE. Prof. Hisham Mehanna.
 Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE Prof. Hisham Mehanna Chief investigator: Hisham Mehanna Arm 1: Mehmet Sen Arm2: John Chester/Martin
Comparing Alternative treatment Regimens for intermediate and high risk oropharyngeal cancer CompARE Prof. Hisham Mehanna Chief investigator: Hisham Mehanna Arm 1: Mehmet Sen Arm2: John Chester/Martin