Screening for Prostate Cancer with the Prostate Specific Antigen (PSA) Test: Recommendations 2014
|
|
|
- Alban Summers
- 5 years ago
- Views:
Transcription

1 Screening for Prostate Cancer with the Prostate Specific Antigen (PSA) Test: Recommendations 2014 Canadian Task Force on Preventive Health Care October 2014 Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude canadien sur les soins de santé préventifs
2 CTFPHC Prostate Cancer Screening Working Group Members Task Force Members Neil Bell (Chair) James Dickinson Michel Joffres Harminder Singh Elizabeth Shaw Marcello Tonelli Public Health Agency: Sarah Connor Gorber* Amanda Shane* Lesley Dunfield* Evidence Review and Synthesis Centre: Donna Fitzpatrick-Lewis* Ali Usman* *non-voting member 2
3 Background Prostate cancer is the most commonly diagnosed non-skin cancer among Canadian men. Long term survival with prostate cancer is now >90% in Canada. 1 in 7 men will be detected as having prostate cancer (at current levels of screening). The PSA test was introduced in Canada in 1986, but its use for screening did not become widespread until
4 Global Rates of Prostate Cancer Mortality 25 fold variation in prostate cancer mortality worldwide. Early reduction in prostate cancer mortality is probably due to improvements in treatment with surgery, radiation and hormone therapy. For example, in the UK: Low rates of screening but reduction in mortality rates for prostate cancer are still seen. Melissa Center, Ahmedin Jemal, Joanne Loret-Tieulent, Elizabeth Ward, Jacques Ferlay, Otis Brawley, Freddie Bray. International variation in prostate cancer incidence and mortality rates. Eur Urol 2012;61:
5 Objectives of the 2014 Guideline To update the 1994 guideline by the CTFPHC on screening for prostate cancer. To review the latest evidence on the benefits and harms of screening for prostate cancer with PSA. To provide recommendations on screening for prostate cancer using PSA with or without digital rectal examination (DRE) for men in the general population. 5
6 Screening for Prostate Cancer with PSA METHODS 6
7 Methods of the CTFPHC Independent panel of: clinicians and methodologists expertise in prevention, primary care, literature synthesis, and critical appraisal application of evidence to practice and policy Prostate Cancer Screening Working Group 6 Task Force members establish research questions and analytical framework 7
8 Methods of the CTFPHC (continued) Evidence Review and Synthesis Centre (ERSC) Undertakes a systematic review of the literature based on the analytical framework Prepares a systematic review of the evidence with GRADE tables Participates in working group and task force meetings Obtain expert opinions (i.e. urologist) 8
9 CTFPHC Review Process Internal review process involving guideline working group, Task Force, scientific officers and ERSC staff External review process involving key stakeholders Generalist and disease specific stakeholders Federal and P/T stakeholders CMAJ undertakes an independent peer review journal process to review guidelines 9
10 External Reviewers for Prostate Cancer Disease Specific Stakeholders Canadian Urological Association (4 reviewers) Prostate Cancer Canada (2 reviewers) Canadian Cancer Society (1 reviewer) Generalist Organizations College of Family Physicians of Canada (1 reviewer) Federal and P/T Stakeholders Public Health Agency of Canada (2 reviewers) Health Canada (1 reviewer) Canadian Institutes of Health Research (1 reviewer) Council of Chief Medical Officers of Health (1 reviewer) Anonymous reviewers from CMAJ (5) 10
11 Analytical Framework 1 Population at risk of prostate cancer Screening 2 No prostate cancer Early detection of prostate cancer 3 Treatment Surgery Radiation therapy Hormonal therapy Cryotherapy Ultrasonography Watchful waiting Active surveillance Reduced prostate cancer- specific and all- cause mortality Harms of screening 4 Harms of treatment 11
12 Key Research Questions KQ1a. What is the direct evidence that screening for prostate cancer with prostate-specific antigen (PSA), as a single-threshold test or as a function of multiple tests over time, decreases morbidity and/or prostate cancer-specific and all-cause mortality? KQ1b. Is there evidence to support differential screening based on individual risk factors for prostate cancer such as age, black race/ ethnicity, family history of prostate cancer or previously assessed increased PSA values either absolute values or increased PSA measures over time? KQ2. What are the harms of PSA-based screening for prostate cancer? 12
13 Key Research Questions (continued) KQ3. What are the benefits of treatment of early-stage or screendetected prostate cancer? KQ4. Is there evidence that tailoring the method of following up abnormal screening results to patient characteristics lead to clinically important differences in the harms and benefits of screening with PSA? KQ5. What are the harms of treatment of early-stage or screendetected prostate cancer? 13
14 Contextual Questions Stage one: Assist in making a decision about the direction of the recommendation: 1. What are the patient values and preferences for PSA screening for prostate cancer? Stage 2: If evidence is sufficient to recommend screening: 1. What process and outcome performance measures or indicators have been identified in the literature to measure and monitor the impact of PSA screening for prostate cancer? 14
?")
15 Contextual Questions (continued) Stage 2: If evidence is sufficient to recommend screening: 2. What is the optimal screening interval for PSA screening for prostate cancer and should this interval vary based on risk level (e.g., age, prior PSA levels, or other measures such as Gleason score)? 3. What are the most effective (accurate and reliable) risk assessment tools to identify: a) risk of prostate cancer and b) risk of poor outcomes after PSA testing and biopsy? 4. What is the cost-effectiveness of PSA screening for asymptomatic adults for prostate cancer? Costs to the system and to patients will be included if found. 15
16 Eligible Study Types Population: This recommendation applies to men in the general population. This includes men with lower urinary tract symptoms (nocturia, urgency, frequency and poor stream) or with benign prostatic hyperplasia (BPH). Effectiveness of screening on preselected outcomes: Systematic reviews, randomized controlled trials Harms of screening: Studies of any design Contextual questions: Studies of any design 16
17 How is Evidence Graded? The GRADE System: Grading of Recommendations, Assessment, Development & Evaluation What are we grading? 1. Quality of Evidence confidence or certainty in estimate of effects high, moderate, low, very low 2. Strength of Recommendation strong and weak 17
18 1. How is the Quality of Evidence Determined? The quality of the evidence is graded as: High confidence that the true effect lies close to the estimate of effect Moderate confidence that the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different Low confidence that the true effect is close to the estimate of the effect. The true effect may be substantially different from the estimate of the effect Very Low Any estimate of effect is very uncertain 18
19 1. How is the Quality of Evidence Determined? (continued) RCT Studies - start as high quality evidence Observational Studies start as low quality evidence Both can be downgraded or upgraded based on various study characteristics 19
20 2. How is the Strength of Recommendations Determined? The strength of the recommendations (strong or weak) are based on four factors: Quality of supporting evidence Certainty about the balance between desirable and undesirable effects Certainty / variability in values and preferences of individuals Certainty about whether the intervention represents a wise use of resources 20
21 Interpretations of the Recommendations Implications Strong Recommendation Weak Recommendations For patients Most individuals would want the recommended course of action; only a small proportion would not. For clinicians Most individuals should receive the intervention. For policy makers The recommendation can be adapted as policy in most situations. The majority of individuals in this situation would want the suggested course of action but many would not. Recognize that different choices will be appropriate for individual patients; Clinicians must help patients make management decisions consistent with values and preferences. Policy making will require substantial debate and involvement of various stakeholders. 21
22 Screening for Prostate Cancer with PSA RECOMMENDATIONS 22
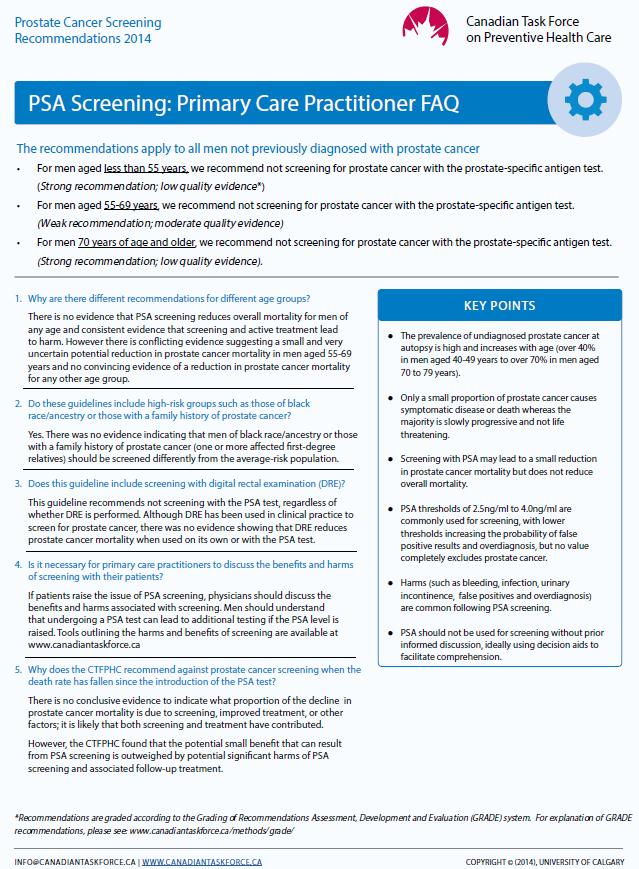
23 Summary of the Recommendations Clinicians and Policy Makers For men aged less than 55 years of age, we recommend not screening for prostate cancer with the prostate-specific antigen test. (Strong recommendation; low quality evidence) Basis of the recommendation The CTFPHC based this recommendation on the low incidence of prostate cancer and prostate cancer mortality, and the lack of evidence for benefit of screening in this age group, as well as the evidence of harms. The strong recommendation implies that the CTFPHC is confident the harms of screening and subsequent testing/ treatment outweigh the benefits. 23
24 Summary of the Recommendations Clinicians and Policy Makers For men aged years, we recommend not screening for prostate cancer with the prostate specific antigen test. (Weak recommendation; moderate quality evidence) Basis of the recommendation The CTFPHC placed a relatively low value on a small and uncertain potential reduction in the risk of prostate cancer mortality and a relatively higher value on the risk of harms associated with diagnosis and treatment due to false positive results and overdiagnosis. The weak recommendation against screening implies that the harms of screening and subsequent testing/treatment probably outweigh benefits, but uncertainty exists. 24
25 Summary of the Recommendations Clinicians and Policy Makers For men aged 70 years and older, we recommend not screening for prostate cancer with the prostate-specific antigen test. (Strong recommendation; low quality evidence) Basis of the recommendation The CTFPHC based this recommendation on the lower life expectancy and the lack of evidence for benefits of screening in this age group, as well as the evidence of harms. The strong recommendation implies that the CTFPHC is confident the harms of screening and subsequent testing/ treatment outweigh the benefits. 25
26 Summary of the Recommendations Clinicians and Policy Makers These recommendations apply to all men who have not been previously diagnosed with prostate cancer. This includes men with lower urinary tract symptoms (nocturia, urgency, frequency and poor stream) or with benign prostatic hyperplasia (BPH). These recommendations do not apply to the use of the PSA test for surveillance after diagnosis or treatment for prostate cancer. 26
27 27 * European Randomized Study of Screening for Prostate Cancer Findings: Benefits of Screening with PSA Moderate Quality of Evidence The evidence review identified 6 RCTs of varying quality: Of these 6 trials, 3 had a low risk of bias (RoB). 1 low RoB trial (Goteborg) was a report from a site within a larger multicentre trial (ERSPC*). In formulating the recommendation, all sites from the ERSPC were considered together. This resulted in 2 low RoB trials that formed the basis of the recommendation: 1 found a positive effect of screening on prostate cancer-specific mortality, while 1 found no effect. A small absolute reduction in mortality from prostate cancer was found in one trial. There was no reduction in all cause mortality.
28 Findings: Benefits of Screening with PSA Study (country) PLCO U.S. population ERSPC (Finland, Sweden, Italy, Netherlands, Belgium, Switzerland and Spain) Study Characteristics RCT 76,693 men age 55-74, annual PSA screening for six years and DRE annually for four years 14 year follow-up RCT 162,243 men Age (core group 55-69) PSA every 4 years 13 year follow-up PSA Threshold Contaminati on (rate of screening in control group) 4 ng/ml 52% Most sites 3.0 ng/ml 20% Prostate cancer mortality Relative Risk (95% C.I.) 1.09 ( ) Core gp: 0.79 ( ) All ages: 0.83 ( ) All-Cause Mortality Relative Risk (95% C.I.) Absolute Effect (per 1000 men screened) GRADE Quality of Evidence * 0.96 ( ) No effect moderate Core gp: 1.00 ( ) All ages: 1.00 ( ) 1.28 fewer deaths per 1,000 men screened moderate *Grading of Recommendations, Assessment, Development and Evaluation (GRADE) rates the continuum of quality of evidence in four categories of high, moderate, low or very low see evidence review for complete assessment of study quality Prostate, Lung, Colorectal and Ovarian Screening Study European Randomized Study for Screening for Prostate Cancer (published online August 7, 2014) 28
29 29 * European Randomized Study of Screening for Prostate Cancer Findings: Harms of Screening with PSA The main harms of screening identified were: Harms of biopsy Harms of overdiagnosis False positives
30 Findings: Harms of Biopsy Harm Study type Study characteristics Proportions (proportion % with 95% CI) Harms of < 30 days Haematuria* Biopsy Mean=30.86% (20.18% to 41.51%) of men who had a biopsy GRADE Quality of Evidence * Very low Infection* Mean=0.94% (0.01% to 1.86%) of men who had a biopsy Not requiring hospitalization Hospitalization=2.07% (1.59% to 2.54%) of men who had a biopsy Death = 0.17% (0.09% to 0.25%) Very low Very Low *Grading of Recommendations, Assessment, Development and Evaluation (GRADE) rates the continuum of quality of evidence in four categories of high, moderate, low or very low see evidence review for complete assessment of study quality* 30
31 Findings: Additional Harms of Screening Harm Study type Study characteristics Overdiagnosi ERSPC s modelling data, various sources Proportions GRADE Quality (proportion % with 95% CI) of Evidence * 40-56% of cases diagnosed Very low Definition: Overdiagnosis occurs when cancer is detected correctly, but would not cause symptoms or death during the patient s lifetime. All data can be found in Dunfield L, Usman A, Fitzpatrick-Lewis D, Shane A, eds. Screening for prostate cancer with prostate specific antigen (PSA) and treatment of early-stage or screen-detected prostate cancer: A systematic review of the clinical benefits and harms. Ottawa: Canadian Task Force;
32 Findings: Additional Harms of Screening Harm Study type Study characteristics Proportions (proportion % with 95% CI) GRADE Quality of Evidence * False Positives ERSPC observation al PSA>3ng/ml cut-point biopsy referral 17.8% of men screened at least once had one or more false positive (all centres) Very low Not all men who screened above threshold had a biopsy Some men who screen positive on the first round could be diagnosed with prostate cancer on a subsequent round Some men will have multiple biopsies Kilpelainen TP, Tammela TL, Roobol M, et al. False-positive screening results in the European Randomized Study of Screening for Prostate Cancer. Eur J Cancer 2011;47:
33 Treatments of Prostate Cancer The primary treatments reviewed: Radical Prostatectomy Radiation Therapy Androgen Deprivation Therapy (ADT) Combination Therapy 33
34 Findings: Benefits of Treatment Some treatments were found to reduce the risk of prostate cancer-specific mortality, although the quality of evidence was variable. Prostatectomy was the only treatment with high QoE Hormone therapy alone was found to produce an increased risk of prostate cancer-specific mortality. Very limited and low QoE to support a reduction in the risk of allcause mortality for the following treatments: Prostatectomy Radiation Therapy Combination Therapy (Radiation and Hormone Therapy) 34
35 Findings: Benefits of Treatment Treatment Findings Study Type Prostate cancer-specific mortality (RR) Prostatectomy The risk of prostate cancerspecific RCT 0.68 (o.52 to 0.89) mortality was reduced. Inconclusive results on all-cause 50 fewer per 1000 (from 17 mortality: some trials reported no fewer to 75 fewer) effect, while cohort studies showed an effect. Radiation Therapy Hormone Therapy The risk of both prostate cancerspecific and all-cause mortality were reduced. There was an increased risk of prostate-specific mortality. No effect on all-cause mortality. Cohort 0.42 (0.33 to 0.53) 33 fewer per 1000 (from 27 fewer to 38 fewer) Cohort 0.74 (0.57 to 0.96) 18 fewer per 1000 (from 3 fewer to 31 fewer) Cohort 1.62 (1.16 to 2.26) 43 more per 1000 (from 11 more to 88 more) All-cause morality (RR) GRADE Quality of Evidence * 0.92 (o.83 to 1.02) -High QoE for prostate-specific 46 fewer per 1000 mortality (from 97 fewer to 11 -Moderate QoE for more) all-cause mortality 0.38 (0.32 to 0.47) 221 fewer per 1000 (from 189 fewer to 242 fewer) 0.69 (0.62 to 0.77) 137 fewer per 1000 (from 101 fewer to 168 fewer) 1.13 (1 to 1.27) 69 more per 1000 (from 0 to 144 more) - Low QoE for both prostatespecific and allcause mortality -Low QoE for prostate-specific and all-cause mortality -Low QoE for prostate-specific and all-cause mortality Combination Radiation and Hormone Therapy The combined hormonal and radiation therapies decrease both prostate-specific and all-cause mortality. Observational 0.52 (0.29 to 0.93) 56 fewer per 1000 (from 9 fewer to 83 fewer) 0.44 (0.32 to 0.59) 289 fewer per 1000 (from 211 fewer to 347 fewer) - Low QoE for prostate-specific and all-cause mortality 35
36 Findings: Harms of Treatment Radical prostatectomy, radiation therapy and ADT are the most common treatments for prostate cancer and are associated with potential harms that include: Urinary incontinence Erectile dysfunction Bowel dysfunction 36
37 Findings: Harms of Treatment Harms of Treatment Study Type Relative Risk (RR) GRADE Quality of Evidence * Urinary Incontinence RCT 3.22 (2.27 to 4.56) 178 more per 1000 (from 102 more to 286 more) 8.31 (1.1 to 62.63) 149 more per 1000 (from 2 more to 1000 more) Cohort 3.68 (2.37 to 5.72) 167 more per 1000 (from 85 more to 293 more) 1.35 (0.9 to 2.02) 22 more per 1000 (from 6 fewer to 63 more) Observational 1.32 (0.75 to 2.3)19 more per 1000 (from 15 fewer to 76 more) Erectile Dysfunction RCT 1.39 (0.77 to 2.53) 221 more per 1000 (from 130 fewer to 867 more) Cohort 1.56 (1.33 to 1.83) 234 more per 1000 (from 138 more to 347 more) 1.30 (1.17 to 1.43) 127 more per 1000 (from 72 more to 182 more) Observational 2.35 (1.53 to 3.59) 442 more per 1000 (from 174 more to 849 more) Bowel Dysfunction RCT 0.42 (0.04 to 4.14) 54 fewer per 1000 (from 90 fewer to 293 more) Cohort 0.69 (0.43 to 1.11)15 fewer per 1000 (from 27 fewer to 5 more) High QoE Moderate QoE Moderate QoE Very low QOE Very low QoE Low QoE Low QoE Low QoE Moderate QoE Low QoE Very low QoE Observational 1.65 (0.84 to 3.25) 31 more per 1000 (from 8 fewer to 106 more) 2.44 (0.24 to 24.4) 40 more per 1000 (from 21 fewer to 653 more) Very low QoE Very low QoE 37
38 Prostatectomy and Post-Surgical Harms ANY <30 days Observational studies: VERY LOW QoE 2246/ %; CI 95% ( )* 247/ %; CI 95% ( )* 395/ %; CI 95% ( )* 60/ %; CI 95% ( )* Mortality <30days Observational studies: VERY LOW QoE 53/11, %; CI 95% ( )* 1/ %; CI 95% ( )* *Grading of Recommendations, Assessment, Development and Evaluation (GRADE) rates the continuum of quality of evidence in four categories of high, moderate, low or very low see evidence review for complete assessment of study quality* 38
39 Additional Findings Evidence on patient preferences and values: Men with perceived self-vulnerability to the disease and physician recommendation are associated with patient request for screening. High quality evidence is lacking about the best way to facilitate informed decision making about screening. Practitioners should distinguish between benefits and harms of screening, subsequent investigation and treatment. Discussions should include overview of diagnostic and therapeutic options in the event PSA test results are abnormal. 39
40 Additional Findings Evidence on resource implications: The CTFPHC did not consider the costs of screening or treatment of prostate cancer when formulating these recommendations. 40
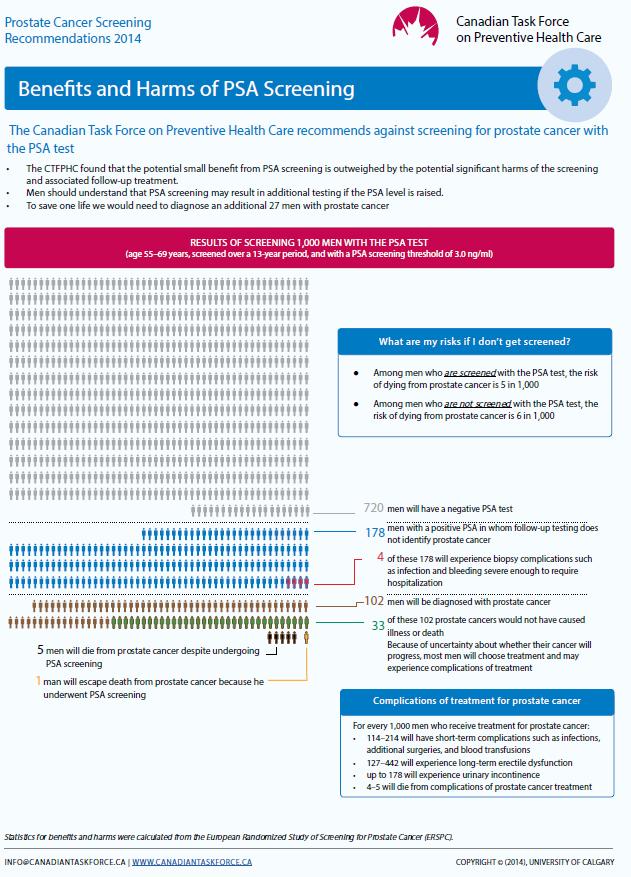
41 Balancing the Benefits and Harms of Screening There is conflicting evidence of a small and very uncertain potential reduction in prostate cancer mortality in men years (1 death avoided per 1,000 invited for screening). If you screen 5 of 1000 men die of prostate cancer If you don t screen 6 of 1000 men die of prostate cancer For one death avoided from prostate cancer 27 or 28 additional men will be diagnosed with prostate cancer There is no convincing evidence of a reduction in prostate cancer mortality for any other age group. 41
42 Balancing the Benefits and Harms of Screening (continued) There is consistent evidence that screening and active treatment lead to harm. Therefore, the potential small benefit from screening is outweighed by the potential significant harms and the CTFPHC recommends not screening for prostate cancer with the PSA test. 42
43 Considerations for the Implementation of Weak Recommendations The implication of the weak recommendation for men aged years is that clinicians who believe a patient places a high value on the small potential benefit of screening and may not be concerned about harms, may wish to discuss the benefits/harms of screening with men in this age group. A weak recommendation implies that most people would want the recommended course of action, but some would not. 43
44 Considerations for the Implementation of Strong Recommendations The implication of the strong recommendation for men <55 and 70 years and older is that clinicians should not routinely discuss screening with men in these age groups, unless the topic is raised by the patient. A strong recommendation implies that most men will be best served by the recommended course of action. 44
45 Considerations for High Risk Populations High risk populations include men of black ethnicity or men with a family history of prostate cancer. Men of black ethnicity were included in the USA studies, however, the results are not broken down by risk level or risk factor. Instead, the studies provide results for the male population as a whole. Therefore, there is currently no trial data to suggest that men at high risk should be screened differently from men in the general population. Clinicians may wish to discuss the benefits and harms of screening in men at high risk, with explicit consideration of their values and preferences. 45
46 Comparison to Previous CTFPHC and International Guidelines The 2014 CTFPHC recommendation is consistent with recommendations issued by other industrialized countries, including: The USPSTF (2012) The Cancer Council Australia (2010) The National Health Service UK (2013) However, there are other guidelines available providing conflicting recommendations. 46
47 Screening for Prostate Cancer with PSA CONCLUSIONS 47
48 Conclusions Among men aged years, the harms of screening probably outweigh the benefits, but uncertainty exists. Therefore, the CTFPHC made a weak recommendation to not screen for prostate cancer with the PSA test in this age group. The implication of the weak recommendation is that clinicians should discuss the benefits and harms of screening so they can make an informed decision in line with their values and preferences. 48
49 Conclusions (continued) Among men younger than 55 years and 70 years and older, there is a lack of evidence for benefit of screening and clear evidence of harms. There is certainty that the harms of screening outweigh the benefits. Therefore, the CTFPHC made a strong recommendation to not screen for prostate cancer with the PSA test in these age groups. The implication of the strong recommendations is that clinicians should not routinely discuss screening with men unless the topic is raised. 49
50 Evidence Review Reference For more information on the details of this guideline please see: Canadian Task Force for Preventive Health Care website: Dunfield L, Usman A, Fitzpatrick-Lewis D, Shane A, eds. Screening for prostate cancer with prostate specific antigen (PSA) and treatment of early-stage or screen-detected prostate cancer: A systematic review of the clinical benefits and harms. Ottawa: Canadian Task Force;
51 Screening for Prostate Cancer with PSA KT TOOLS 51
52 52

53 53
54 54
55 Questions & Answers Thank you 55
Recommendations on Screening for Colorectal Cancer 2016
 Recommendations on Screening for Colorectal Cancer 2016 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude
Recommendations on Screening for Colorectal Cancer 2016 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude
Recommendations on Screening for Lung Cancer 2016
 Recommendations on Screening for Lung Cancer 2016 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude canadien
Recommendations on Screening for Lung Cancer 2016 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude canadien
Acknowledgments: Maureen Rice, Rachel Warren, Judy Brown, Meghan Kenny, Sharon Peck-Reid, Sarah Connor Gorber
 Screening for prostate cancer with prostate specific antigen and treatment of early-stage or screen-detected prostate cancer: a systematic review of the clinical benefits and harms May 2014 Lesley Dunfield
Screening for prostate cancer with prostate specific antigen and treatment of early-stage or screen-detected prostate cancer: a systematic review of the clinical benefits and harms May 2014 Lesley Dunfield
Recommendations on Screening for High Blood Pressure in Canadian Adults 2012
 Recommendations on Screening for High Blood Pressure in Canadian Adults 2012 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health
Recommendations on Screening for High Blood Pressure in Canadian Adults 2012 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health
RECOMMENDATIONS FOR GROWTH MONITORING, PREVENTION AND MANAGEMENT OF OVERWEIGHT AND OBESITY IN CHILDREN AND YOUTH IN PRIMARY HEALTH CARE 2015
 Slide 2 Use of deck RECOMMENDATIONS FOR GROWTH MONITORING, PREVENTION AND MANAGEMENT OF OVERWEIGHT AND OBESITY IN CHILDREN AND YOUTH IN PRIMARY HEALTH CARE 2015 These slides are made available publicly
Slide 2 Use of deck RECOMMENDATIONS FOR GROWTH MONITORING, PREVENTION AND MANAGEMENT OF OVERWEIGHT AND OBESITY IN CHILDREN AND YOUTH IN PRIMARY HEALTH CARE 2015 These slides are made available publicly
Recommendations on Screening for Cognitive Impairment in Older Adults 2015
 Recommendations on Screening for Cognitive Impairment in Older Adults 2015 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health
Recommendations on Screening for Cognitive Impairment in Older Adults 2015 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health
CTFPHC Working Group Members:
 Cognitive Impairment - Guideline Presentation Speaker deck OVERVIEW We will review the following: 1. Background on Cognitive Impairment 2. Methods of the CTFPHC 3. Recommendations and Key Findings 4. Implementation
Cognitive Impairment - Guideline Presentation Speaker deck OVERVIEW We will review the following: 1. Background on Cognitive Impairment 2. Methods of the CTFPHC 3. Recommendations and Key Findings 4. Implementation
Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement
 Clinical Review & Education JAMA US Preventive Services Task Force RECOMMENDATION STATEMENT Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement US Preventive Services
Clinical Review & Education JAMA US Preventive Services Task Force RECOMMENDATION STATEMENT Screening for Prostate Cancer US Preventive Services Task Force Recommendation Statement US Preventive Services
Recommendations on Behavioural Interventions for Prevention and Treatment of Cigarette Smoking in School-aged Children and Youth 2017
 Recommendations on Behavioural Interventions for Prevention and Treatment of Cigarette Smoking in School-aged Children and Youth 2017 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention
Recommendations on Behavioural Interventions for Prevention and Treatment of Cigarette Smoking in School-aged Children and Youth 2017 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention
Prostate-Specific Antigen Based Screening for Prostate Cancer Evidence Report and Systematic Review for the US Preventive Services Task Force
 Clinical Review & Education JAMA US Preventive Services Task Force EVIDENCE REPORT Prostate-Specific Antigen Based Screening for Prostate Cancer Evidence Report and Systematic Review for the US Preventive
Clinical Review & Education JAMA US Preventive Services Task Force EVIDENCE REPORT Prostate-Specific Antigen Based Screening for Prostate Cancer Evidence Report and Systematic Review for the US Preventive
Dr. Michel Joffres Dr. Gabriela Lewin Dr. Patricia Parkin Dr. Kevin Pottie (telecon) Dr. Elizabeth Shaw Dr. Harminder Singh
 Dr. Elizabeth Shaw Dr. Harminder Singh") Last Edited by Diane Perazzo 28/05/13 CANADIAN TASK FORCE ON PREVENTIVE HEALTH CARE February 11 12, 2013 Meeting PUBLIC RECORD OF MEETING (REVISED: MAY 28, 2013) Present: CTFPHC Members Chair: Dr. Marcello
Last Edited by Diane Perazzo 28/05/13 CANADIAN TASK FORCE ON PREVENTIVE HEALTH CARE February 11 12, 2013 Meeting PUBLIC RECORD OF MEETING (REVISED: MAY 28, 2013) Present: CTFPHC Members Chair: Dr. Marcello
PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC
 PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC Disclosures Faculty / Speaker s name: Darrel Drachenberg Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
PSA To screen or not to screen? Darrel Drachenberg, MD, FRCSC Disclosures Faculty / Speaker s name: Darrel Drachenberg Relationships with commercial interests: Grants/Research Support: None Speakers Bureau/Honoraria:
The U.S. Preventive Services Task Force (USPSTF) makes
 makes") Annals of Internal Medicine Clinical Guideline Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement Virginia A. Moyer, MD, MPH, on behalf of the U.S. Preventive Services
Annals of Internal Medicine Clinical Guideline Screening for Prostate Cancer: U.S. Preventive Services Task Force Recommendation Statement Virginia A. Moyer, MD, MPH, on behalf of the U.S. Preventive Services
Questions and Answers about Prostate Cancer Screening with the Prostate-Specific Antigen Test
 Questions and Answers about Prostate Cancer Screening with the Prostate-Specific Antigen Test About Cancer Care Ontario s recommendations for prostate-specific antigen (PSA) screening 1. What does Cancer
Questions and Answers about Prostate Cancer Screening with the Prostate-Specific Antigen Test About Cancer Care Ontario s recommendations for prostate-specific antigen (PSA) screening 1. What does Cancer
Amanda Shane. Dawn Opgenorth. Ali Usman (telecom) Dr. Parminder Raina Dr. Sharon Straus
 Dr. Parminder Raina Dr. Sharon Straus") CANADIAN CTFPHC ON PREVENTIVE HEALTH CARE Meeting of June 24-25, 2013 PUBLIC RECORD OF MEETING (REVISED: SEPTEMBER 30, 2013) Present: CTFPHC Members Chair: Dr. Marcello Tonelli Vice- Chair: Dr. Richard
CANADIAN CTFPHC ON PREVENTIVE HEALTH CARE Meeting of June 24-25, 2013 PUBLIC RECORD OF MEETING (REVISED: SEPTEMBER 30, 2013) Present: CTFPHC Members Chair: Dr. Marcello Tonelli Vice- Chair: Dr. Richard
First do no harm? The importance of communicating overdiagnosis in guideline recommendations:
 First do no harm? The importance of communicating overdiagnosis in guideline recommendations: Approach of the Canadian Task Force on Preventive Health Care Wilson BJ, Bell NR, Grad R, Groulx S, Moore A,
First do no harm? The importance of communicating overdiagnosis in guideline recommendations: Approach of the Canadian Task Force on Preventive Health Care Wilson BJ, Bell NR, Grad R, Groulx S, Moore A,
U.S. Preventive Services Task Force: Draft Prostate Cancer Screening Recommendation (April 2017)
") 1 U.S. Preventive Services Task Force: Draft Prostate Cancer Screening Recommendation (April 2017) Alex Krist MD MPH Professor and Director of Research Department of Family Medicine and Population Health
1 U.S. Preventive Services Task Force: Draft Prostate Cancer Screening Recommendation (April 2017) Alex Krist MD MPH Professor and Director of Research Department of Family Medicine and Population Health
PSA testing in New Zealand general practice
 PSA testing in New Zealand general practice Ross Lawrenson, Charis Brown, Fraser Hodgson. On behalf of the Midland Prostate Cancer Study Group Academic Steering Goup: Zuzana Obertova, Helen Conaglen, John
PSA testing in New Zealand general practice Ross Lawrenson, Charis Brown, Fraser Hodgson. On behalf of the Midland Prostate Cancer Study Group Academic Steering Goup: Zuzana Obertova, Helen Conaglen, John
CTFPHC Working Group Members:
 Developmental Delay- Guideline Presentation Speaker deck OVERVIEW We will review the following: 1. Introduction to CTFPHC 2. Background on Developmental Delay 3. Methods for Guideline Development 4. Recommendations
Developmental Delay- Guideline Presentation Speaker deck OVERVIEW We will review the following: 1. Introduction to CTFPHC 2. Background on Developmental Delay 3. Methods for Guideline Development 4. Recommendations
Cigna Medical Coverage Policy
 Cigna Medical Coverage Policy Subject Prostate-Specific Antigen (PSA) Screening for Prostate Cancer Table of Contents Coverage Policy... 1 General Background... 1 Coding/Billing Information... 12 References...
Cigna Medical Coverage Policy Subject Prostate-Specific Antigen (PSA) Screening for Prostate Cancer Table of Contents Coverage Policy... 1 General Background... 1 Coding/Billing Information... 12 References...
USA Preventive Services Task Force PSA Screening Recommendations- May 2018
 GPGU - NOTÍCIAS USA Preventive Services Task Force PSA Screening Recommendations- May 2018 Rationale Importance Prostate cancer is one of the most common types of cancer that affects men. In the United
GPGU - NOTÍCIAS USA Preventive Services Task Force PSA Screening Recommendations- May 2018 Rationale Importance Prostate cancer is one of the most common types of cancer that affects men. In the United
PSA Screening and Prostate Cancer. Rishi Modh, MD
 PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
Otis W. Brawley, MD, MACP, FASCO, FACE
 Otis W. Brawley, MD, MACP, FASCO, FACE Chief Medical and Scientific Officer American Cancer Society Professor of Hematology, Medical Oncology, Medicine and Epidemiology Emory University Atlanta, Georgia
Otis W. Brawley, MD, MACP, FASCO, FACE Chief Medical and Scientific Officer American Cancer Society Professor of Hematology, Medical Oncology, Medicine and Epidemiology Emory University Atlanta, Georgia
Prostate Cancer Screening Clinical Practice Guideline. Approved by the National Guideline Directors November, 2015
 Prostate Cancer Screening Clinical Practice Guideline This guideline is informational only. It is not intended or designed as a substitute for the reasonable exercise of independent clinical judgment by
Prostate Cancer Screening Clinical Practice Guideline This guideline is informational only. It is not intended or designed as a substitute for the reasonable exercise of independent clinical judgment by
Prostate Cancer Screening. Eric Shreve, MD Bend Urology Associates
 Prostate Cancer Screening Eric Shreve, MD Bend Urology Associates University of Cincinnati Medical Center University of Iowa Hospitals and Clinics PSA Human kallikrein 3 Semenogelin is substrate Concentration
Prostate Cancer Screening Eric Shreve, MD Bend Urology Associates University of Cincinnati Medical Center University of Iowa Hospitals and Clinics PSA Human kallikrein 3 Semenogelin is substrate Concentration
Screening for Colorectal Cancer
 Screening for Colorectal Cancer April 1, 2014 Revised August 2014 McMaster Evidence Review and Synthesis Centre Team: Donna Fitzpatrick-Lewis, Ali Usman, Rachel Warren, Meghan Kenny, Maureen Rice, Andy
Screening for Colorectal Cancer April 1, 2014 Revised August 2014 McMaster Evidence Review and Synthesis Centre Team: Donna Fitzpatrick-Lewis, Ali Usman, Rachel Warren, Meghan Kenny, Maureen Rice, Andy
Prostate Cancer Screening: Risks and Benefits across the Ages
 Prostate Cancer Screening: Risks and Benefits across the Ages 7 th Annual Symposium on Men s Health Continuing Progress: New Gains, New Challenges June 10, 2009 Michael J. Barry, MD General Medicine Unit
Prostate Cancer Screening: Risks and Benefits across the Ages 7 th Annual Symposium on Men s Health Continuing Progress: New Gains, New Challenges June 10, 2009 Michael J. Barry, MD General Medicine Unit
Canadian Task Force on Preventive Health Care
 Screening for Cervical Cancer: Recommendations 2013 Canadian Task Force on Preventive Health Care Presentation for free use to disseminate Guidelines. Feb 2013 Putting Prevention into Practice Canadian
Screening for Cervical Cancer: Recommendations 2013 Canadian Task Force on Preventive Health Care Presentation for free use to disseminate Guidelines. Feb 2013 Putting Prevention into Practice Canadian
Prostate Cancer. Biomedical Engineering for Global Health. Lecture Fourteen. Early Detection. Prostate Cancer: Statistics
 Biomedical Engineering for Global Health Lecture Fourteen Prostate Cancer Early Detection Prostate Cancer: Statistics Prostate gland contributes enzymes, nutrients and other secretions to semen. United
Biomedical Engineering for Global Health Lecture Fourteen Prostate Cancer Early Detection Prostate Cancer: Statistics Prostate gland contributes enzymes, nutrients and other secretions to semen. United
PROSTATE CANCER Amit Gupta MD MPH
 PROSTATE CANCER Amit Gupta MD MPH Depts. of Urology and Epidemiology Amit-Gupta-1@uiowa.edu dramitgupta@gmail.com Tel: 319-384-5251 OUTLINE PSA screening controversy How to use PSA more effectively Treatment
PROSTATE CANCER Amit Gupta MD MPH Depts. of Urology and Epidemiology Amit-Gupta-1@uiowa.edu dramitgupta@gmail.com Tel: 319-384-5251 OUTLINE PSA screening controversy How to use PSA more effectively Treatment
Prostate-Specific Antigen (PSA) Screening for Prostate Cancer
 Screening for Prostate Cancer") Medical Coverage Policy Effective Date... 4/15/2018 Next Review Date... 4/15/2019 Coverage Policy Number... 0215 Prostate-Specific Antigen (PSA) Screening for Prostate Cancer Table of Contents Related
Medical Coverage Policy Effective Date... 4/15/2018 Next Review Date... 4/15/2019 Coverage Policy Number... 0215 Prostate-Specific Antigen (PSA) Screening for Prostate Cancer Table of Contents Related
Where are we with PSA screening?
 Where are we with PSA screening? Faculty/Presenter Disclosure Rela%onships with commercial interests: None Disclosure of Commercial Support This program has received no financial support. This program
Where are we with PSA screening? Faculty/Presenter Disclosure Rela%onships with commercial interests: None Disclosure of Commercial Support This program has received no financial support. This program
Urological Society of Australia and New Zealand PSA Testing Policy 2009
 Executive summary Urological Society of Australia and New Zealand PSA Testing Policy 2009 1. Prostate cancer is a major health problem and is the second leading cause of male cancer deaths in Australia
Executive summary Urological Society of Australia and New Zealand PSA Testing Policy 2009 1. Prostate cancer is a major health problem and is the second leading cause of male cancer deaths in Australia
Elevated PSA. Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017
 Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Elevated PSA Dr.Nesaretnam Barr Kumarakulasinghe Associate Consultant Medical Oncology National University Cancer Institute, Singapore 9 th July 2017 Issues we will cover today.. The measurement of PSA,
Examining the Efficacy of Screening with Prostate- Specific Antigen Testing in Reducing Prostate Cancer Mortality
 St. Catherine University SOPHIA Master of Arts/Science in Nursing Scholarly Projects Nursing 5-2012 Examining the Efficacy of Screening with Prostate- Specific Antigen Testing in Reducing Prostate Cancer
St. Catherine University SOPHIA Master of Arts/Science in Nursing Scholarly Projects Nursing 5-2012 Examining the Efficacy of Screening with Prostate- Specific Antigen Testing in Reducing Prostate Cancer
Contemporary Approaches to Screening for Prostate Cancer
 Contemporary Approaches to Screening for Prostate Cancer Gerald L. Andriole, MD Robert K. Royce Distinguished Professor Chief of Urologic Surgery Siteman Cancer Center Washington University School of Medicine
Contemporary Approaches to Screening for Prostate Cancer Gerald L. Andriole, MD Robert K. Royce Distinguished Professor Chief of Urologic Surgery Siteman Cancer Center Washington University School of Medicine
Section Editors Robert H Fletcher, MD, MSc Michael P O'Leary, MD, MPH
 1 de 32 04-05-2013 19:24 Official reprint from UpToDate www.uptodate.com 2013 UpToDate Author Richard M Hoffman, MD, MPH Disclosures Section Editors Robert H Fletcher, MD, MSc Michael P O'Leary, MD, MPH
1 de 32 04-05-2013 19:24 Official reprint from UpToDate www.uptodate.com 2013 UpToDate Author Richard M Hoffman, MD, MPH Disclosures Section Editors Robert H Fletcher, MD, MSc Michael P O'Leary, MD, MPH
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015
 Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Prostate cancer is the most commonly diagnosed
 CMAJ Early release, published at www.cmaj.ca on October 27, 2014. Subject to revision. Guidelines Recommendations on screening for prostate cancer with the prostate-specific antigen test Canadian Task
CMAJ Early release, published at www.cmaj.ca on October 27, 2014. Subject to revision. Guidelines Recommendations on screening for prostate cancer with the prostate-specific antigen test Canadian Task
HEPATITIS C WORKING GROUP
 Recommendations on Hepatitis C Screening for Adults (2017): Guideline Presentation Speaker deck (Slide 3) HEPATITIS C WORKING GROUP The Hepatitis C Working Group included members from the Canadian Task
Recommendations on Hepatitis C Screening for Adults (2017): Guideline Presentation Speaker deck (Slide 3) HEPATITIS C WORKING GROUP The Hepatitis C Working Group included members from the Canadian Task
Prostate-Specific Antigen (PSA) Test
 Test") Prostate-Specific Antigen (PSA) Test What is the PSA test? Prostate-specific antigen, or PSA, is a protein produced by normal, as well as malignant, cells of the prostate gland. The PSA test measures the
Prostate-Specific Antigen (PSA) Test What is the PSA test? Prostate-specific antigen, or PSA, is a protein produced by normal, as well as malignant, cells of the prostate gland. The PSA test measures the
HIGH MORTALITY AND POOR SURVIVAL OF MEN WITH PROSTATE CANCER IN RURAL AND REMOTE AUSTRALIA
 HIGH MORTALITY AND POOR SURVIVAL OF MEN WITH PROSTATE CANCER IN RURAL AND REMOTE AUSTRALIA The prostate is a small gland the size of a walnut which produces fluid to protect and lubricate the sperm It
HIGH MORTALITY AND POOR SURVIVAL OF MEN WITH PROSTATE CANCER IN RURAL AND REMOTE AUSTRALIA The prostate is a small gland the size of a walnut which produces fluid to protect and lubricate the sperm It
Prostate Cancer Incidence
 Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Screening for Prostate Cancer
 Screening for Prostate Cancer Review against programme appraisal criteria for the UK National Screening Committee (UK NSC) Version 1: This document summarises the work of ScHARR 1 2 and places it against
Screening for Prostate Cancer Review against programme appraisal criteria for the UK National Screening Committee (UK NSC) Version 1: This document summarises the work of ScHARR 1 2 and places it against
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
Screening and Diagnosis Prostate Cancer
 Screening and Diagnosis Prostate Cancer Daniel Heng MD MPH FRCPC Chair, Genitourinary Tumor Group Tom Baker Cancer Center University of Calgary, Canada @DrDanielHeng Outline Screening Evidence Recommendations
Screening and Diagnosis Prostate Cancer Daniel Heng MD MPH FRCPC Chair, Genitourinary Tumor Group Tom Baker Cancer Center University of Calgary, Canada @DrDanielHeng Outline Screening Evidence Recommendations
PSA & Prostate Cancer Screening
 PSA & Prostate Cancer Screening DR JONATHAN REES MD MRCS MRCGP When a thing ceases to be a subject of controversy, it ceases to be a subject of interest Do you think we should have a national screening
PSA & Prostate Cancer Screening DR JONATHAN REES MD MRCS MRCGP When a thing ceases to be a subject of controversy, it ceases to be a subject of interest Do you think we should have a national screening
Prostate-Specific Antigen Based Screening for Prostate Cancer: A Systematic Evidence Review for the U.S. Preventive Services Task Force
 Evidence Synthesis Number 154 Prostate-Specific Antigen Based Screening for Prostate Cancer: A Systematic Evidence Review for the U.S. Preventive Services Task Force Prepared for: Agency for Healthcare
Evidence Synthesis Number 154 Prostate-Specific Antigen Based Screening for Prostate Cancer: A Systematic Evidence Review for the U.S. Preventive Services Task Force Prepared for: Agency for Healthcare
Overview. What is Cancer? Prostate Cancer 3/2/2014. Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014
 Prostate Cancer Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014 Overview Start with the basics: Definition of cancer Most common cancers in men Prostate, lung, and colon cancers Cancer
Prostate Cancer Davis A Romney, MD Ironwood Cancer and Research Centers Feb 18, 2014 Overview Start with the basics: Definition of cancer Most common cancers in men Prostate, lung, and colon cancers Cancer
Translating Evidence Into Policy The Case of Prostate Cancer Screening. Ruth Etzioni Fred Hutchinson Cancer Research Center
 Translating Evidence Into Policy The Case of Prostate Cancer Screening Ruth Etzioni Fred Hutchinson Cancer Research Center Prostate Cancer Mortality in the US 2011 Prostate Cancer Mortality in the US 2011
Translating Evidence Into Policy The Case of Prostate Cancer Screening Ruth Etzioni Fred Hutchinson Cancer Research Center Prostate Cancer Mortality in the US 2011 Prostate Cancer Mortality in the US 2011
PSA & Prostate Cancer Screening
 PSA & Prostate Cancer Screening DR JONATHAN REES MD MRCS MRCGP Do you think we should have a national screening programme for Prostate Cancer using PSA? YES it s an outrage, women have breast cancer screening
PSA & Prostate Cancer Screening DR JONATHAN REES MD MRCS MRCGP Do you think we should have a national screening programme for Prostate Cancer using PSA? YES it s an outrage, women have breast cancer screening
Prostate Cancer Screening Where are we? Prof. Bob Steele Professor of Surgery, University of Dundee Independent Chair, UK NSC
 Prostate Cancer Screening Where are we? Prof. Bob Steele Professor of Surgery, University of Dundee Independent Chair, UK NSC 1990 Screening The detection of disease in asymptomatic people in order to
Prostate Cancer Screening Where are we? Prof. Bob Steele Professor of Surgery, University of Dundee Independent Chair, UK NSC 1990 Screening The detection of disease in asymptomatic people in order to
The Evolving Role of PSA for Prostate Cancer. The Evolving Role of PSA for Prostate Cancer: 10/30/2017
 The Evolving Role of PSA for Prostate Cancer Adele Marie Caruso, DNP, CRNP Adult Nurse Practitioner Perelman School of Medicine at the University of Pennsylvania November 4, 2017 The Evolving Role of PSA
The Evolving Role of PSA for Prostate Cancer Adele Marie Caruso, DNP, CRNP Adult Nurse Practitioner Perelman School of Medicine at the University of Pennsylvania November 4, 2017 The Evolving Role of PSA
Prostate Cancer Screening: Con. Laurence Klotz Professor of Surgery, Sunnybrook HSC University of Toronto
 Prostate Cancer Screening: Con Laurence Klotz Professor of Surgery, Sunnybrook HSC University of Toronto / Why not PSA screening? Overdiagnosis Overtreatment Risk benefit ratio unfavorable Flaws of PSA
Prostate Cancer Screening: Con Laurence Klotz Professor of Surgery, Sunnybrook HSC University of Toronto / Why not PSA screening? Overdiagnosis Overtreatment Risk benefit ratio unfavorable Flaws of PSA
The Royal Marsden. Prostate case study. Presented by Mr Alan Thompson Consultant Urological Surgeon
 Prostate case study Presented by Mr Alan Thompson Consultant Urological Surgeon 2 Part one Initial presentation A 62 year old male solicitor attends your GP surgery. He has rarely seen you over the last
Prostate case study Presented by Mr Alan Thompson Consultant Urological Surgeon 2 Part one Initial presentation A 62 year old male solicitor attends your GP surgery. He has rarely seen you over the last
Helping you make better-informed decisions 1-5
 Helping you make better-informed decisions 1-5 The only test that provides an accurate assessment of prostate cancer aggressiveness A prognostic medicine product for prostate cancer. A common diagnosis
Helping you make better-informed decisions 1-5 The only test that provides an accurate assessment of prostate cancer aggressiveness A prognostic medicine product for prostate cancer. A common diagnosis
Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease
 Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease Jeffrey A. Cadeddu, MD Professor, Department of Urology UT Southwestern Medical Center Vice-Chair, AUA/ASTRO/SUO
Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease Jeffrey A. Cadeddu, MD Professor, Department of Urology UT Southwestern Medical Center Vice-Chair, AUA/ASTRO/SUO
Applying the Principles of Disease Screening to Prostate Cancer
 PUBLIC HEALTH Applying the Principles of Disease Screening to Prostate Cancer Maria Paiva, BSP, PharmD, BCPS 1,2 Mary H. H. Ensom, B. Sc. (Pharm), PharmD, FASHP, FCCP, FCSHP, FCAHS 1,3 1 Faculty of Pharmaceutical
PUBLIC HEALTH Applying the Principles of Disease Screening to Prostate Cancer Maria Paiva, BSP, PharmD, BCPS 1,2 Mary H. H. Ensom, B. Sc. (Pharm), PharmD, FASHP, FCCP, FCSHP, FCAHS 1,3 1 Faculty of Pharmaceutical
Prostate Cancer Screening Clinical Practice Guidelines
 NATIONAL CLINICAL PRACTICE GUIDELINES Prostate Cancer Screening Clinical Practice Guidelines Reviewed/Approved by the National Guideline Directors November 2017 Next Review/Approval: November 2019 Developed
NATIONAL CLINICAL PRACTICE GUIDELINES Prostate Cancer Screening Clinical Practice Guidelines Reviewed/Approved by the National Guideline Directors November 2017 Next Review/Approval: November 2019 Developed
10/2/2018 OBJECTIVES PROSTATE HEALTH BACKGROUND THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION
 THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION Lenette Walters, MS, MT(ASCP) Medical Affairs Manager Beckman Coulter, Inc. *phi is a calculation using the values from PSA, fpsa and p2psa
THE PROSTATE HEALTH INDEX PHI*: BETTER PROSTATE CANCER DETECTION Lenette Walters, MS, MT(ASCP) Medical Affairs Manager Beckman Coulter, Inc. *phi is a calculation using the values from PSA, fpsa and p2psa
Pre-test. Prostate Cancer The Good News: Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest
 Pre-test Matthew R. Cooperberg, MD, MPH UCSF 40 th Annual Advances in Internal Medicine Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest 1. I do not offer routine PSA screening, and
Pre-test Matthew R. Cooperberg, MD, MPH UCSF 40 th Annual Advances in Internal Medicine Prostate Cancer Screening 2012: Putting the PSA Controversy to Rest 1. I do not offer routine PSA screening, and
Response to United States Preventative Services Task Force draft PSA Screening recommendation: Donald B. Fuller, M.D. Genesis Healthcare Partners
 Response to United States Preventative Services Task Force draft PSA Screening recommendation: Donald B. Fuller, M.D. Genesis Healthcare Partners October 2011 Cancer Incidence Statistics, 2011 CA: A Cancer
Response to United States Preventative Services Task Force draft PSA Screening recommendation: Donald B. Fuller, M.D. Genesis Healthcare Partners October 2011 Cancer Incidence Statistics, 2011 CA: A Cancer
Questions and Answers About the Prostate-Specific Antigen (PSA) Test
 Test") CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Questions and Answers
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Questions and Answers
PSA screening. To screen or not to screen, that s the question Walid Shahrour FRCSC, MDCM, BSc Assistant professor Northern Ontario School of Medicine
 PSA screening To screen or not to screen, that s the question Walid Shahrour FRCSC, MDCM, BSc Assistant professor Northern Ontario School of Medicine Conflict of Interest Declaration: Nothing to Disclose
PSA screening To screen or not to screen, that s the question Walid Shahrour FRCSC, MDCM, BSc Assistant professor Northern Ontario School of Medicine Conflict of Interest Declaration: Nothing to Disclose
Prostate Cancer: from Beginning to End
 Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
AllinaHealthSystems 1
 2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
BLADDER PROSTATE PENIS TESTICLES BE YO ND YO UR CA NC ER
 BLADDER PROSTATE PENIS TESTICLES THE PROSTATE IS A SMALL, WALNUT-SIZED GLAND THAT IS PART OF THE MALE REPRODUCTIVE SYSTEM. IT RESTS BELOW THE BLADDER, IN FRONT OF THE RECTUM AND SURROUNDS PART OF THE URETHRA.
BLADDER PROSTATE PENIS TESTICLES THE PROSTATE IS A SMALL, WALNUT-SIZED GLAND THAT IS PART OF THE MALE REPRODUCTIVE SYSTEM. IT RESTS BELOW THE BLADDER, IN FRONT OF THE RECTUM AND SURROUNDS PART OF THE URETHRA.
PSA Screening for Prostate Cancer at Western Medical Clinic Kardy Fedorowich University of Manitoba Max Rady College of Medicine
 PSA Screening for Prostate Cancer at Western Medical Clinic Kardy Fedorowich University of Manitoba Max Rady College of Medicine Abstract While PSA screening for prostate cancer remains a widely used tool
PSA Screening for Prostate Cancer at Western Medical Clinic Kardy Fedorowich University of Manitoba Max Rady College of Medicine Abstract While PSA screening for prostate cancer remains a widely used tool
SHARED DECISION MAKING FOR PROSTATE CANCER SCREENING
 SHARED DECISION MAKING FOR PROSTATE CANCER SCREENING 16 TH A N N U A L M A S S A C H U S E T T S P R O S T A T E C A N C E R S Y M P O S I U M Mary McNaughton-Collins, MD, MPH Foundation Medical Director
SHARED DECISION MAKING FOR PROSTATE CANCER SCREENING 16 TH A N N U A L M A S S A C H U S E T T S P R O S T A T E C A N C E R S Y M P O S I U M Mary McNaughton-Collins, MD, MPH Foundation Medical Director
PROSTATE CANCER SURVEILLANCE
 PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
Page 1. Selected Controversies. Cancer Screening! Selected Controversies. Breast Cancer Screening. ! Using Best Evidence to Guide Practice!
 Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Cancer Screening!! Using Best Evidence to Guide Practice! Judith M.E. Walsh, MD, MPH! Division of General Internal Medicine! Womenʼs Health Center of Excellence University of California, San Francisco!
Managing Prostate Cancer in General Practice
 Managing Prostate Cancer in General Practice Tuesday 18 th September 2018 Presenters: Prof Jon Emery Assoc Prof Declan Murphy The education has been developed in partnership with Cancer Council Victoria,
Managing Prostate Cancer in General Practice Tuesday 18 th September 2018 Presenters: Prof Jon Emery Assoc Prof Declan Murphy The education has been developed in partnership with Cancer Council Victoria,
Screening for Abdominal Aortic Aneurysm: Systematic Review and Meta-analysis
 Screening for Abdominal Aortic Aneurysm: Systematic Review and Meta-analysis Date: September 6 th, 2015 Revisions: October 29 rd, 2015 McMaster Evidence Review and Synthesis Centre Team: Donna Fitzpatrick-Lewis,
Screening for Abdominal Aortic Aneurysm: Systematic Review and Meta-analysis Date: September 6 th, 2015 Revisions: October 29 rd, 2015 McMaster Evidence Review and Synthesis Centre Team: Donna Fitzpatrick-Lewis,
Outcomes With "Watchful Waiting" in Prostate Cancer in US Now So Good, Active Treatment May Not Be Better
 1 sur 5 19/09/2009 07:02 www.medscape.com From Medscape Medical News Outcomes With "Watchful Waiting" in Prostate Cancer in US Now So Good, Active Treatment May Not Be Better Zosia Chustecka September
1 sur 5 19/09/2009 07:02 www.medscape.com From Medscape Medical News Outcomes With "Watchful Waiting" in Prostate Cancer in US Now So Good, Active Treatment May Not Be Better Zosia Chustecka September
Title: Prostate Specific Antigen (PSA) for Prostate Cancer Screening: A Clinical Review
 for Prostate Cancer Screening: A Clinical Review") Title: Prostate Specific Antigen (PSA) for Prostate Cancer Screening: A Clinical Review Date: November 26, 2007 Context and policy issues: Prostate cancer is the most common tumor in men, and is one of
Title: Prostate Specific Antigen (PSA) for Prostate Cancer Screening: A Clinical Review Date: November 26, 2007 Context and policy issues: Prostate cancer is the most common tumor in men, and is one of
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Screening for asymptomatic bacteriuria in pregnancy (2018)
") Screening for asymptomatic bacteriuria in pregnancy (2018) Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Use of Slide Deck These slides are made available publicly
Screening for asymptomatic bacteriuria in pregnancy (2018) Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Use of Slide Deck These slides are made available publicly
Prostate-Specific Antigen testing in men between 40 and 70 years in Brazil: database from a check-up program
 ORIGINAL ARTICLE Vol. 40 (6): 745-752, November - December, 2014 doi: 10.1590/S1677-5538.IBJU.2014.06.05 Prostate-Specific Antigen testing in men between 40 and 70 years in Brazil: database from a check-up
ORIGINAL ARTICLE Vol. 40 (6): 745-752, November - December, 2014 doi: 10.1590/S1677-5538.IBJU.2014.06.05 Prostate-Specific Antigen testing in men between 40 and 70 years in Brazil: database from a check-up
4.5% 4.0% 3.5% 3.0% 2.5% 2.0% 1.5% 1.0% 0.5% 0.0% < >80 Current Age (Yrs)
") Biomedical Engineering for Global Health Lecture Twelve Prostate Cancer Early Detection Prostate Cancer: Statistics Prostate gland contributes enzymes, nutrients and other secretions to semen. United States:
Biomedical Engineering for Global Health Lecture Twelve Prostate Cancer Early Detection Prostate Cancer: Statistics Prostate gland contributes enzymes, nutrients and other secretions to semen. United States:
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Reducing overtreatment of prostate cancer by radical prostatectomy in Eastern Ontario: a population-based cohort study
 Reducing overtreatment of prostate cancer by radical prostatectomy in Eastern Ontario: a population-based cohort study Luke Witherspoon MD MSc, Johnathan L. Lau BSc, Rodney H. Breau MD MSc, Christopher
Reducing overtreatment of prostate cancer by radical prostatectomy in Eastern Ontario: a population-based cohort study Luke Witherspoon MD MSc, Johnathan L. Lau BSc, Rodney H. Breau MD MSc, Christopher
The balance of harms and benefits of screening for prostate cancer: the apples and oranges problem solved
 The balance of harms and benefits of screening for prostate cancer: the apples and oranges problem solved Harold C. Sox, MD, MACP The Patient-Centered Outcomes Research Institute April 2,2016 Declarations
The balance of harms and benefits of screening for prostate cancer: the apples and oranges problem solved Harold C. Sox, MD, MACP The Patient-Centered Outcomes Research Institute April 2,2016 Declarations
Screening for prostate cancer (Review)
") Ilic D, Neuberger MM, Djulbegovic M, Dahm P This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2013, Issue 1 http://www.thecochranelibrary.com
Ilic D, Neuberger MM, Djulbegovic M, Dahm P This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2013, Issue 1 http://www.thecochranelibrary.com
Facing Prostate Cancer Surgery? Learn about minimally invasive da Vinci Surgery
 Facing Prostate Cancer Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Prostate Cancer Your prostate is a walnut-sized gland that is part of the male reproductive system. The prostate
Facing Prostate Cancer Surgery? Learn about minimally invasive da Vinci Surgery The Condition: Prostate Cancer Your prostate is a walnut-sized gland that is part of the male reproductive system. The prostate
Navigating the Stream: Prostate Cancer and Early Detection. Ifeanyi Ani, M.D. TPMG Urology Newport News
 Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Navigating the Stream: Prostate Cancer and Early Detection Ifeanyi Ani, M.D. TPMG Urology Newport News Understand epidemiology of prostate cancer Discuss PSA screening and PSA controversy Review tools
Cancer Screening: Evidence, Opinion and Fact Dialogue on Cancer April Ruth Etzioni Fred Hutchinson Cancer Research Center
 Cancer Screening: Evidence, Opinion and Fact Dialogue on Cancer April 2018? Ruth Etzioni Fred Hutchinson Cancer Research Center Three thoughts to begin 1. Cancer screening is a good idea in principle Detect
Cancer Screening: Evidence, Opinion and Fact Dialogue on Cancer April 2018? Ruth Etzioni Fred Hutchinson Cancer Research Center Three thoughts to begin 1. Cancer screening is a good idea in principle Detect
Washington, DC, November 9, 2009 Institute of Medicine
 Holger Schünemann, MD, PhD Chair, Department of Clinical Epidemiology & Biostatistics Michael Gent Chair in Healthcare Research McMaster University, Hamilton, Canada Washington, DC, November 9, 2009 Institute
Holger Schünemann, MD, PhD Chair, Department of Clinical Epidemiology & Biostatistics Michael Gent Chair in Healthcare Research McMaster University, Hamilton, Canada Washington, DC, November 9, 2009 Institute
Submission To Health Select Committee: Early Detection and Treatment of Prostate Cancer
 August 2009 1 Submission To Health Select Committee: Early Detection and Treatment of Prostate Cancer This submission is from the, PO Box 12700, Thorndon Wellington, 6011. Contact person Sarah Perry, Health
August 2009 1 Submission To Health Select Committee: Early Detection and Treatment of Prostate Cancer This submission is from the, PO Box 12700, Thorndon Wellington, 6011. Contact person Sarah Perry, Health
Effective Health Care Program
 Comparative Effectiveness Review Number 146 Effective Health Care Program Therapies for Clinically Localized Prostate Cancer: Update of a 2008 Systematic Review Executive Summary Background Prostate cancer
Comparative Effectiveness Review Number 146 Effective Health Care Program Therapies for Clinically Localized Prostate Cancer: Update of a 2008 Systematic Review Executive Summary Background Prostate cancer
The Challenge of Cancer Screening Part One Prostate Cancer and Lung Cancer Screening
 The Challenge of Cancer Screening Part One Prostate Cancer and Lung Cancer Screening The Challenge of Cancer Screening Part One Prostate Cancer and Lung Cancer Screening By Marsha Fountain, RN, MSN The
The Challenge of Cancer Screening Part One Prostate Cancer and Lung Cancer Screening The Challenge of Cancer Screening Part One Prostate Cancer and Lung Cancer Screening By Marsha Fountain, RN, MSN The
16:30-18:30 WS #67: Urology Forum - Prostate Cancer, Stones, Renal Tumours, Voiding Dysfunction (120 minutes, not repeated) -
 -") Dr Anna Lawrence Urologist Auckland Dr Andrew Williams Urologist Auckland Madhu Koya Urologist Auckland Andrew Lienert Urologist Auckland Dr Louise Tomlinson Consultant Gynaecologist Auckland 16:30-18:30
Dr Anna Lawrence Urologist Auckland Dr Andrew Williams Urologist Auckland Madhu Koya Urologist Auckland Andrew Lienert Urologist Auckland Dr Louise Tomlinson Consultant Gynaecologist Auckland 16:30-18:30
NICE BULLETIN Diagnosis & treatment of prostate cancer
 Diagnosis & treatment of prostate cancer NICE provided the content for this booklet which is independent of any company or product advertised Diagnosis and treatment of prostate cancer Introduction In
Diagnosis & treatment of prostate cancer NICE provided the content for this booklet which is independent of any company or product advertised Diagnosis and treatment of prostate cancer Introduction In
EAU 2009: US Study Shows No Mortality Benefit From Prostate Cancer Screening, But European Study Suggests There May Be One
 From Medscape Medical News : www.medscape.com/viewarticle/589786 EAU 2009: US Study Shows No Mortality Benefit From Prostate Cancer Screening, But European Study Suggests There May Be One By Roxanne Nelson
From Medscape Medical News : www.medscape.com/viewarticle/589786 EAU 2009: US Study Shows No Mortality Benefit From Prostate Cancer Screening, But European Study Suggests There May Be One By Roxanne Nelson
Decision-Analytic Modeling of PSA Screening an ONCOTYROL Project
 Decision-Analytic Modeling of PSA Screening an ONCOTYROL Project EUFEP, Baden, June 24-26, 2009 Uwe Siebert, MD, MPH, MSc, ScD Professor of Public Health (UMIT) Adjunct Professor of Health Policy and Management
Decision-Analytic Modeling of PSA Screening an ONCOTYROL Project EUFEP, Baden, June 24-26, 2009 Uwe Siebert, MD, MPH, MSc, ScD Professor of Public Health (UMIT) Adjunct Professor of Health Policy and Management
Updates In Cancer Screening: Navigating a Changing Landscape
 Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Updates In Cancer Screening: Navigating a Changing Landscape Niharika Dixit, MD I have no conflict of interest. 1 Why Should You Care Trends in Cancer Incidence by Site United States. Siegal Et al: CA
Quality-of-Life Effects of Prostate-Specific Antigen Screening
 Quality-of-Life Effects of Prostate-Specific Antigen Screening Eveline A.M. Heijnsdijk, Ph.D., Elisabeth M. Wever, M.Sc., Anssi Auvinen, M.D., Jonas Hugosson, M.D., Stefano Ciatto, M.D., Vera Nelen, M.D.,
Quality-of-Life Effects of Prostate-Specific Antigen Screening Eveline A.M. Heijnsdijk, Ph.D., Elisabeth M. Wever, M.Sc., Anssi Auvinen, M.D., Jonas Hugosson, M.D., Stefano Ciatto, M.D., Vera Nelen, M.D.,
Prostate Cancer. Axiom. Overdetection Is A Small Issue. Reducing Morbidity and Mortality
 Overdetection Is A Small Issue (in the context of decreasing prostate cancer mortality rates and with appropriate, effective, and high-quality treatment) Prostate Cancer Arises silently Dwells in a curable
Overdetection Is A Small Issue (in the context of decreasing prostate cancer mortality rates and with appropriate, effective, and high-quality treatment) Prostate Cancer Arises silently Dwells in a curable
ADVICE TO PATIENTS REQUESTING PSA MEASUREMENT
 Frequently-Asked Questions What is the aim of this leaflet? Prostate cancer is a serious condition. The PSA test, which can give an early indication of prostate cancer, is available to you if you want
Frequently-Asked Questions What is the aim of this leaflet? Prostate cancer is a serious condition. The PSA test, which can give an early indication of prostate cancer, is available to you if you want
Resolving the PSA testing controversy. Professor Villis Marshall AC Professor Bruce Armstrong AM Professor Mark Frydenberg
 Resolving the PSA testing controversy Professor Villis Marshall AC Professor Bruce Armstrong AM Professor Mark Frydenberg Professor Villis Marshall AC Introduc)on Guidelines aim to inform tes)ng for the
Resolving the PSA testing controversy Professor Villis Marshall AC Professor Bruce Armstrong AM Professor Mark Frydenberg Professor Villis Marshall AC Introduc)on Guidelines aim to inform tes)ng for the
Fellow GU Lecture Series, Prostate Cancer. Asit Paul, MD, PhD 02/20/2018
 Fellow GU Lecture Series, 2018 Prostate Cancer Asit Paul, MD, PhD 02/20/2018 Disease Burden Screening Risk assessment Treatment Global Burden of Prostate Cancer Prostate cancer ranked 13 th among cancer
Fellow GU Lecture Series, 2018 Prostate Cancer Asit Paul, MD, PhD 02/20/2018 Disease Burden Screening Risk assessment Treatment Global Burden of Prostate Cancer Prostate cancer ranked 13 th among cancer