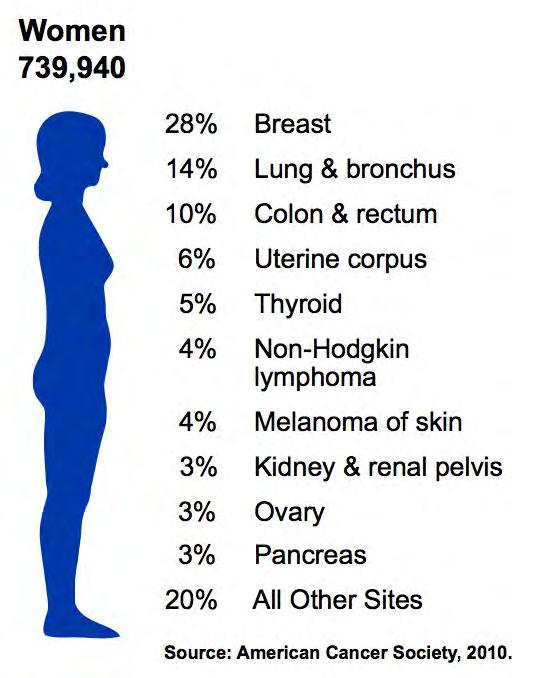
New Cancer Cases By Site Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3%
|
|
|
- Miranda Hampton
- 5 years ago
- Views:
Transcription
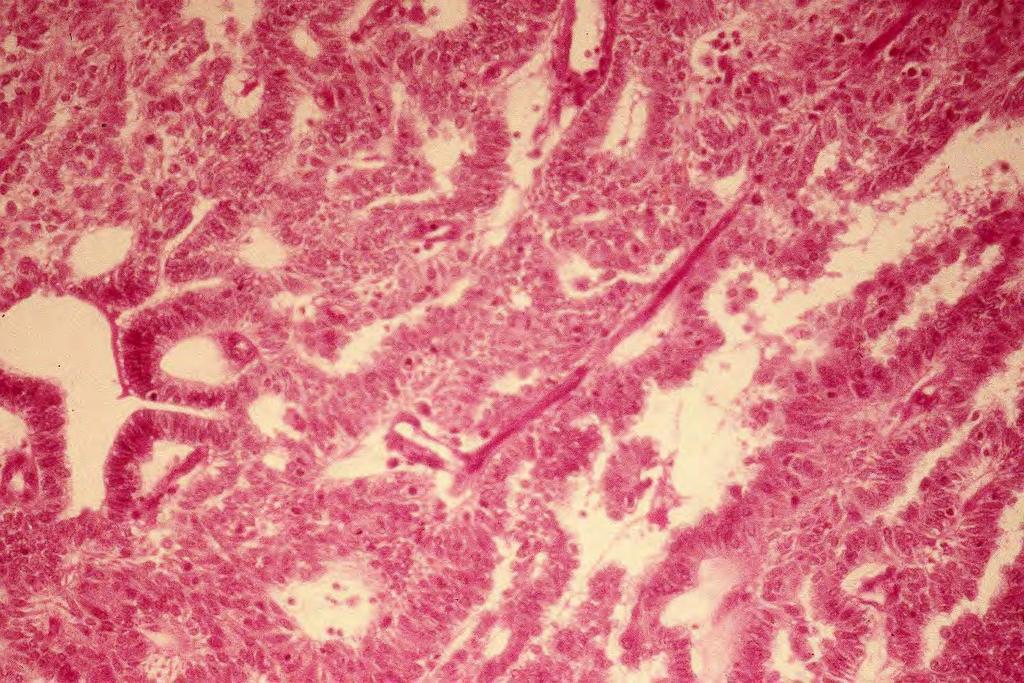
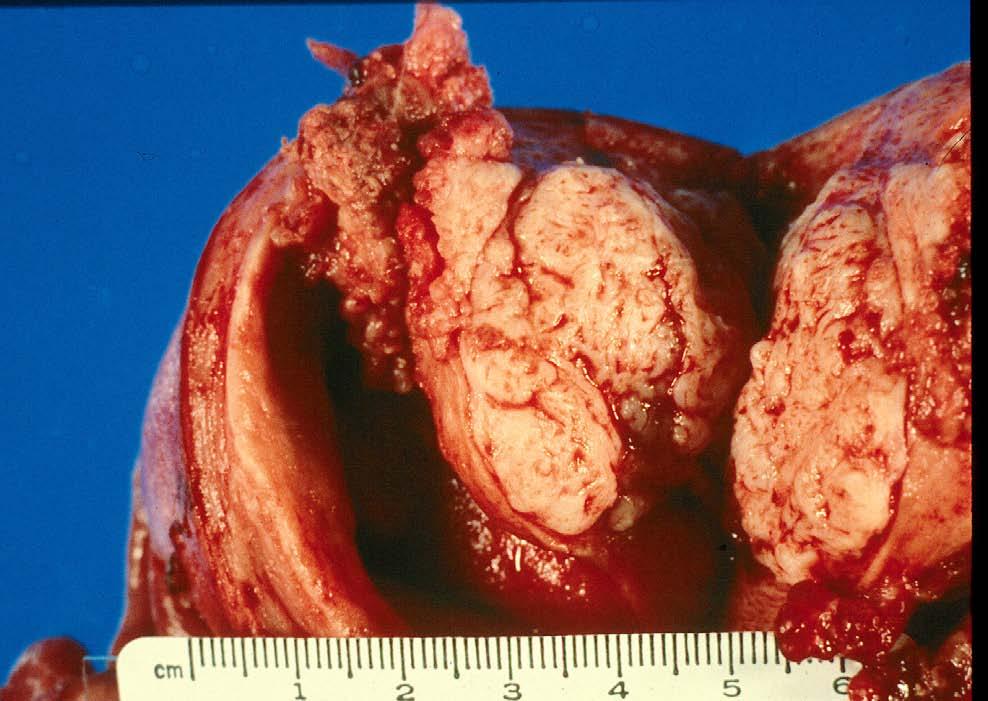
1 Uterine Malignancy

2 New Cancer Cases By Site 2010 Breast 28% Lung 14% Colo-Rectal 10% Uterus 6% Thyroid 5% Lymphoma 4% Ovary 3%
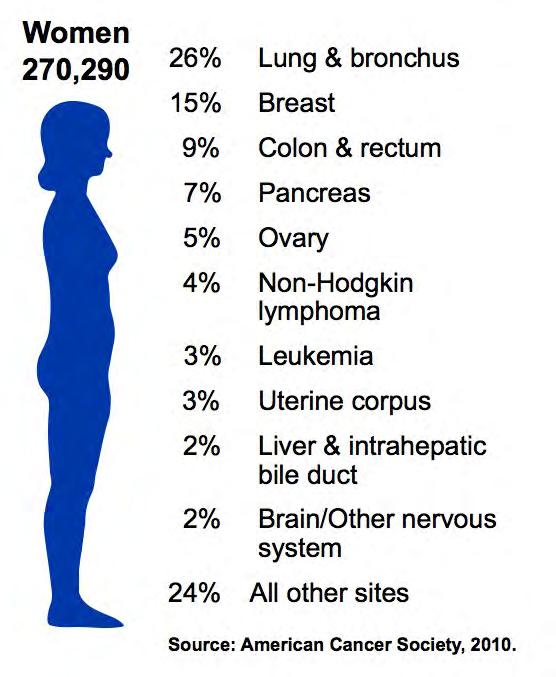
3 Cancer Deaths By Site 2010 Lung 26% Breast 15% Colo-Rectal 9% Pancreas 7% Ovary 5% Lymphoma 4% Leukemia 3% Uterus 3%
4 Gynecologic Malignancies ,000 40,000 35,000 30,000 25,000 20,000 15,000 10,000 5, ,470 21,880 13,850 7,950 12,200 4,210 3, Uterus Ovary Cervix Vulva New Deaths
5 Uterine Cancer Median age at Diagnosis 60 years
6 Uterine Malignancy Age Distribution Pt, 2000
7 Uterine Cancer 75% Postmenopausal 25% Perimenopausal/Premenopausal 5% Aged 40 or younger
8 Endometrial Cancer Type I Type II Clinical Features Risk Factors Unopposed estrogen Age Race White > Black White = Black Differentiation Well differentiated Poorly differentiated Histology Endometrioid Non-endometrioid Stage I/II III/IV Prognosis Favorable Not favorable Ploidy Diploid Aneuploid

9 Uterine Cancer Risk Factors Obesity Nulliparity Late menopause Unopposed estrogen Hereditary 5% associated with HPNCC (10% for women younger than 50)

10 Uterine Cancer Etiology Estrogen Driven Obese, postmenopausal Non-estrogen Driven Older, not obese
11 Post Menopausal Vaginal Bleeding
12 Postmenopausal Bleeding Etiology Factor Percentage Exogenous estrogen 30 Endometritis/vaginits 30 Endometrial Cancer 15 Polyps (endom./ cx.) 10 Endometrial hyperplasia 5 Misc.(sarcoma/ Cx ca./ 10 trauma, caruncle
13 Endometrial Cancer Screening No cost effective screening method. Prompt evaluation of symptomatic patients is essential.
14 Endometrial Cancer Precursors Estrogen Dependent Proliferative endometrium Hyperpalsia Hyperplasia with atypia (EIN) Cancer
15 Uterine Malignancy Diagnosis Endometrial biopsy Dilation and curettage Hysteroscopy Histologic type and grade Presence or absence of vaginal metastases Rule out primary endocervical carcinoma
16 Uterine Cancer Histology Endometrioid Papillary serous Clear cell Undifferntiated Sarcoma Mixed Mesodermal Sarcoma Leiomyosarcoma Stromal Sarcoma
17 Uterine Cancer Staging
18 Pre-treatment Evaluation May or may not alter staging of the disease Should impact decision making regarding therapy
19 F.I.G.O. International Federation of Gynecology & Obstetrics Universally available Clinical vs. Surgical Once established, the stage is not changed Should have prognostic significance Aids in worldwide outcome reporting May assist in treatment decisions
20 F.I.G.O. Clinical Staging Physical exam Chest radiograph Intravenous pyelogram Barium enema Sigmoidoscopy/cystoscopy
21 Diagnostic Tests Cannot alter staging Computed tomography Magnetic resonance imaging (MRI) PET scan Bone scan
22 Staging Gynecologic Malignancies Clinical Surgical Cervix GTN Vagina Ovary Uterine Vulva
23 Uterine Malignancy Surgical Staging
24 Endometrial Cancer Staging FIGO 2009 Stage I The carcinoma is confined to the corpus uteri IA No or < ½ myometrial invasion IB Invasion ½ of the myometrium Stage II Tumor involves the cervical stroma, but does not extend beyond the uterus Stage III Local and/or regional spread of the tumor IIIA Tumor invades the serosa of the corpus uteri and/or adnexae IIIB Vaginal and/or parametrial involvement IIIC Metastases to the pelvic and/or para-aortic lymph nodes IIIC1 Positive pelvic lymph nodes IIIC2 Positive para-aortic lymph nodes with or without positive pelvic lymph nodes Stage IV Tumor invades the bladder and/or bowel mucosa IVA Tumor invades bladder and/or bowel mucosa IVB Distant metastases, including intra-abdominal metastases and/or inguinal lymph nodes Note: All tumors are Graded 1,2 or 3. Endocervical gland involvement is to be considered Stage I. Positive cytology has to be reported separately without changing stage.
25 FIGO 2009 Updated Endometrial Cancer Staging Myometrial invasion is consolidated into two groups IA and IB Stage IIA cervical mucosal involvement deleted Stage not altered by (+) cytology IIIA Node involvement segregated into pelvic and aortic
 peritoneal cytology?")
26 Uterine Cancer Prognostic Factors Histologic type Histologic grade Depth of myometrial invasion (+) peritoneal cytology? Node metastases Extra-uterine disease

27
28

29
30 Uterine Malignancies UKSM,W 7/82-7/ Patients
31 Uterine Malignancies Histology % Adenocarcinoma Sarcoma Pt, 2000
32 Uterine Malignancies Stage Distribution I II III IV Not Spec. 783 Pt, 2000
33 Uterine Malignancies Distribution by Grade 24% 15% 32% 29% Grade I Grade II Grade III Not Spec. 783 Pt. 2000
34 Uterine Malignancies Extrauterine Disease 80 % No Yes Not Spec Pt, 2000
35 Uterine Cancer Therapy

36 Uterine Malignancy Pre-treatment Assessment Physical exam & pre-op evaluation CXR EKG CBC, comprehensive metabolic panel CT scan is of no benefit if surgery is planned
37 Uterine Malignancy Treatment Options Surgical staging Hysterectomy, BSO, and peritoneal cytology, pelvic lymphadenectomy, aortic node sampling Abdominal, laparoscopic, robotic Postop treatment is based on pathologic risk factors
38 Uterine Cancer Surgical Preparation Medical clearance Bowel prep (usually not) DVT prophylaxis Prophylactic antibiotics
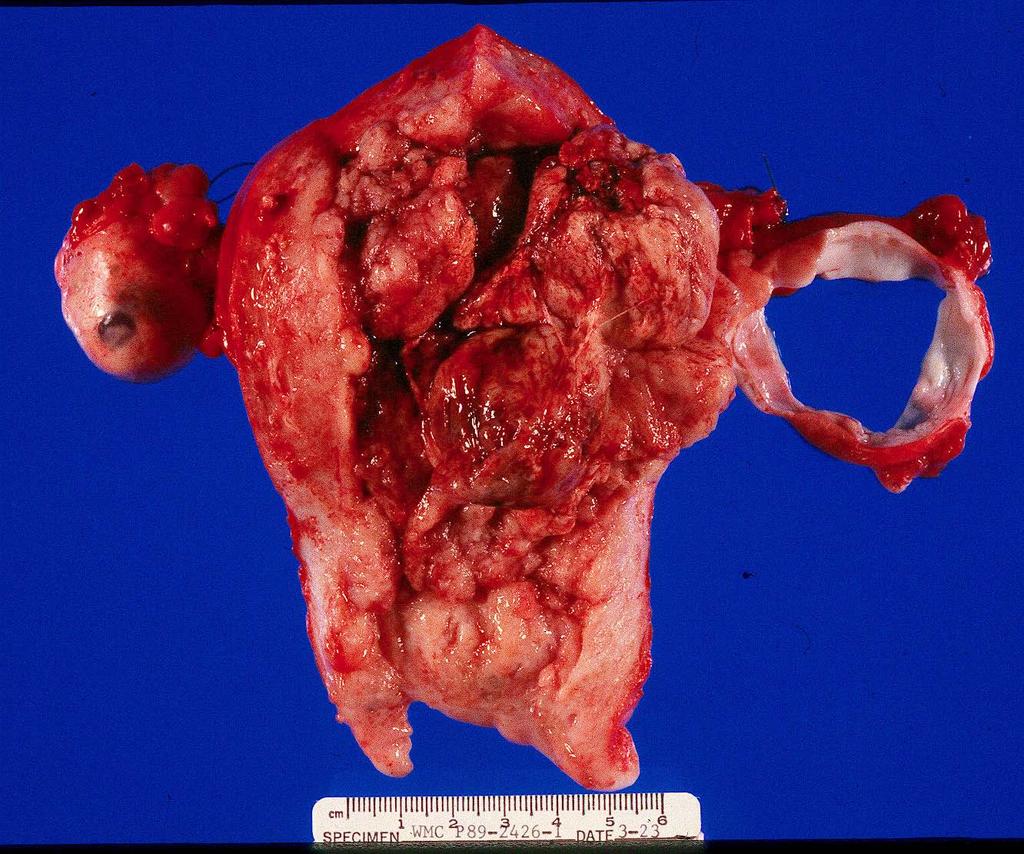
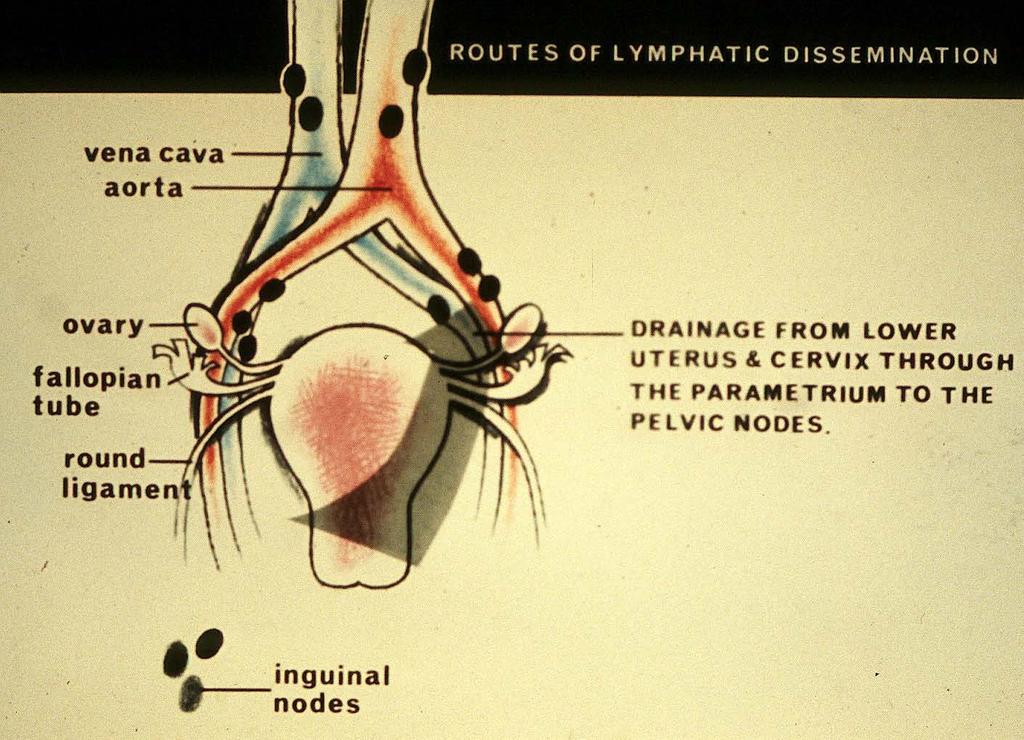
39 Uterine Cancer Pattern of Spread Direct extension Myometrium Parametrium Peritoneal surface Lymphatic Vascular
40
41
42

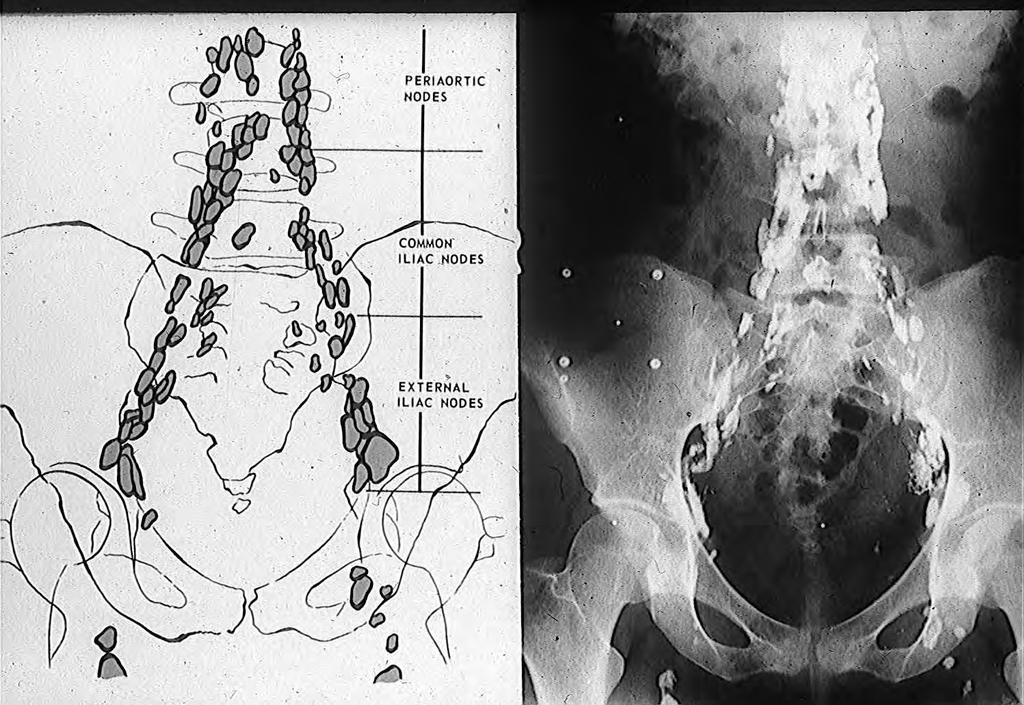
43 Ext Iliac art. Obt. nerve Ureter Ext. Iliac vein

44 Vena cava Aorta

45 Postoperative Treatment Observation Pelvic radiation Combination chemotherapy & radiation Systemic chemotherapy Hormone therapy
46 Uterine Cancer Post-operative Pelvic Radiation Therapy Grade III lesions with any invasion Deeply invasive Grade II? Cervical stromal invasion Serosal involvement? Positive pelvic nodes
47
48 Uterine Cancer Post-operative Systemic or Combination Therapy Positive peritoneal cytology? Gross peritoneal disease / omentum Adnexal involvement Distant metastases
49 Uterine Malignancies Status Last Seen Alive, NED 50 Alive w/dis % Dead w/dis Dead wo/dis Lost to FU Pt, 2000
50 Uterine Malignancy Survival I II III IV Not Spec. 783 Pt, 2000 % NED
51 Uterine Malignancy Survival By Grade Pt, I II III Not Spec. % NED
52 Uterine Cancer Post-treatment Surveillance Pelvic exam and Pap q 3 mos. for 1 yr. Pelvic exam and Pap q 4 mos. for 1 yr. Exams q 6 mos. For final 3 years. 50 % of vaginal/pelvic recurrences are curable with radiation therapy Expensive radiographic f/u is of little benefit
53 Uterine Sarcomas
54 Uterine Sarcomas Mesenchymal Tumors Endometrial Stromal and related tumors Endometrial stromal Sarcoma Smooth muscle tumors Leiomyosarcoma Mixed Epithelial & Mesenchymal Tumors Carcinosarcoma Malignant mixed tumors Adenosarcoma
55
56
57
58 The End
59
60
61 Uterine Cancer
62 Cancer Deaths By Site 2000 Lung 25% Breast 15% Colo-Rectal 11% Ovary 5% Pancreas 5% Lymphoma 4%
63
64

65 Prognostic Factors Histology Lesion size Histologic grade Stage / Extent of disease Node status Age & physical condition of patient
66 Endometrial Carcinoma FIGO Staging Stage IA G123 Tumor limited to endometrium Stage IB G123 Invasion to less than one-half the myometrium Stage IC G123 Invasion to more than one-half the myometrium Stage IIA G123 Endocervical glandular involvement only Stage IIB G123 Cervical stromal invasion Stage IIIA G123 Tumor invades serosa and/or adnexa, and/or (+) peritoneal cytology Stage IIIB G123 Vaginal metastases Stage IIIC G123 Metastases to pelvic and/or paraaortic nodes Stage IVA G123 Tumor invasion of bladder or bowel mucosa Stage IVB G123 Distant metastases including intra-abdominal and/or inguinal nodes Histopathology- Tumor Grading G1 5% or less of a nonsquamous or nonmorular solid growth pattern G2 6%-50% of a nonsquamous or nonmorular solid growth pattern G3 More than 50% of a nonsquamous or nonmorular solid growth pattern Nuclear atypia, inappropriate for the architectural grade, raises the degree of grade 1 or grade 2 tumors by one grade. In serous adenocarcinomas, clear cell adenocarcinomas, and squamous cell carcinomas, nuclear grading takes precedent.
67 Uterine Malignancies Grade Distribution I II III Not Spec Pt, 2000
68
69
70
71 Endometrial Cancer Staging FIGO 2009 Stage I The carcinoma is confined to the corpus uteri IA No or < ½ myometrial invasion IB Invasion ½ of the myometrium Stage II Tumor involves the cervical stroma, but does not extend beyond the uterus Stage III Local and/or regional spread of the tumor IIIA Tumor invades the serosa of the corpus uteri and/or adnexae IIIB Vaginal and/or parametrial involvement IIIC Metastases to the pelvic and/or para-aortic lymph nodes IIIC1 Positive pelvic lymph nodes IIIC2 Positive para-aortic lymph nodes with or without positive pelvic lymph nodes Stage IV Tumor invades the bladder and/or bowel mucosa IVA Tumor invades bladder and/or bowel mucosa IVB Distant metastases, including intra-abdominal metastases and/or inguinal lymph nodes Note: All tumors are Graded 1,2 or 3. Endocervical gland involvement is to be considered Stage I. Positive cytology has to be reported separately without changing stage.
72 FIGO 2009 Updated Endometrial Cancer Staging Myometrial invasion is consolidated into two groups IA and IB Stage IIA cervical mucosal involvement deleted Stage not altered by (+) cytology IIIA Node involvement segregated into pelvic and aortic
 Adenosarcomas Carcinosarcomas (formerly malignant mixed mullerian tumors,")
73 Uterine Sarcoma Staging FIGO 2009 Leiomysarcomas and Endometrial Stromal Sarcomas (ESS) Adenosarcomas Carcinosarcomas (formerly malignant mixed mullerian tumors, MMMT)
74 Leiomyosarcomas and Endometrial Stromal Sarcomas (ESS) FIGO Staging 2009 Stage I Stage II Stage III Stage IV IA IB IIA IIB IIIA IIIB IIIC IVA IVB Tumor limited to the uterus 5 cm > 5 cm. Tumor extends beyond the uterus, within the pelvis Adnexal involvement Involvement of other pelvic tissue Tumor invades abdominal tissues (not just protruding into the abdomen One site > one site Metastases to pelvic or para-aortic lymph nodes Tumor with Bladder and/or rectum invasion Distant metastases
75 Stage I Stage II Stage III Stage IV IA IB IC IIA IIB IIIA IIIB IIIC IVA IV B Uterine Adenosarcoma FIGO 2009 Staging Tumor limited to uterus Tumor limited to endometrium/endocervix with no myometrial invasion ½ myometrial invasion > ½ myometrial invasion Tumor extends beyond the uterus, within the pelvis Adnexal involvement Involvement of other pelvic tissues Tumor invades abdominal tissues (not just protruding into the abdomen) One site > one site Metastasis to pelvic and/or para-aortic lymph nodes Tumor with Bladder and/or rectum invasion Distant metastasis
76 Carcinosarcomas Should be staged as carcinomas of the endometrium
77 Uterine Cancer Prognostic Factors Histologic type Histologic grade Depth of myometrial invasion (+) peritoneal cytology? Node metastases Extra-uterine disease

78 Uterine Cancer Staging F.I.G.O. Stage I A - Limited to endometrium B - Invades 1/2 myometrium C - Invades > 1/2 myometrium Stage II A - Endocervical gland involvement B - Cervical stromal invasion
79 Uterine Cancer Staging F.I.G.O. Stage III A - Involves serosa, adnexa, or (+) cytology B - Vaginal Metastases C - (+) pelvic or para-aortic nodes Stage IV A - Invades bladder or bowel mucosa B - Distant metastases, abdomen, or inguinal nodes
80 Uterine Malignancies Depth Of Mymetrial Invasion None /Super Inner 1/2 Outer 1/ Serosa Not Spec Pt, 2000
81 Uterine Malignancies Peritoneal Cytology 31% 11% 58% Neg. Pos. Not Done 783 Pt. 2000


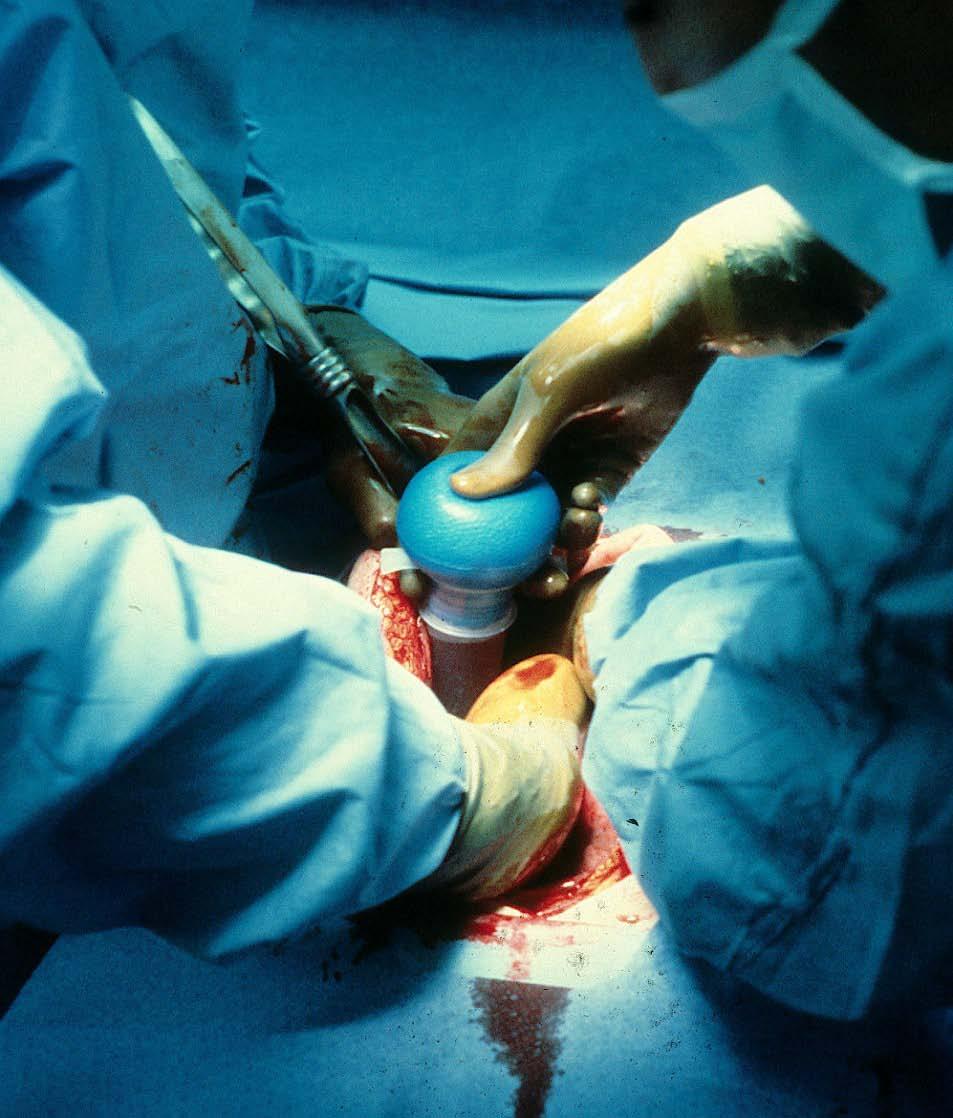
82 Uterine Cancer Surgical Therapy and Staging Midline incision Peritoneal cytology Right and left paracolic gutters and pelvis Explore upper abdomen para-aortic +/or pre-caval node sampling Pelvic node dissection TAH/BSO
83 Uterine Malignancies Post-operative Therapy None % Radiation Chemo. Hormone Not Spec Pt, 2000
84 Uterine Malignancy Survival By Depth of Myometrial Invasion Pt, % NED None/Sup Inner 1/2 Outer 1/2 Serosa Not Spec.
85 Uterine Malignancy Survival By (+) Peritoneal Cytology Neg. Pos. Not Done Pt, 2000 % NED
86 Uterine Malignancy Survival By Post-Operative Therapy Pt, % NED 63 None XRT
87 Uterine Cancer Post-op hormone therapy??
Staging and Treatment Update for Gynecologic Malignancies
 Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Staging and Treatment Update for Gynecologic Malignancies Bunja Rungruang, MD Medical College of Georgia No disclosures 4 th most common new cases of cancer in women 5 th and 6 th leading cancer deaths
Endometrial Cancer. Incidence. Types 3/25/2019
 Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
Endometrial Cancer J. Anthony Rakowski DO, FACOOG MSU SCS Board Review Coarse Incidence 53,630 new cases yearly 8,590 deaths yearly 4 th most common malignancy in women worldwide Most common GYN malignancy
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
3/25/2019. Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates
 Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates") J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
J. Anthony Rakowski D.O., F.A.C.O.O.G. MSU SCS Board Review Coarse Rare uterine cancers ~3% Leiomyosarcoma Carcinosarcoma (MMMT) Endometrial Stromal Sarcomas Aggressive tumors High Mortality Rates Signs
Staging. Carcinoma confined to the corpus. Carcinoma confined to the endometrium. Less than ½ myometrial invasion. Greater than ½ myometrial invasion
 5 th of June 2009 Background Most common gynaecological carcinoma in developed countries Most cases are post-menopausal Increasing incidence in certain age groups Increasing death rates in the USA 5-year
5 th of June 2009 Background Most common gynaecological carcinoma in developed countries Most cases are post-menopausal Increasing incidence in certain age groups Increasing death rates in the USA 5-year
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
2009 USCAP Gyn Pathology Evening Session Case #3. Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA
 2009 USCAP Gyn Pathology Evening Session Case #3 Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA rzaino@psu.edu Clinical history Middle aged woman with an exophytic mass of
2009 USCAP Gyn Pathology Evening Session Case #3 Richard J. Zaino, MD Hershey Medical Center Penn State University Hershey, PA rzaino@psu.edu Clinical history Middle aged woman with an exophytic mass of
What is endometrial cancer?
 Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
Uterine cancer What is endometrial cancer? Endometrial cancer is the growth of abnormal cells in the lining of the uterus. The lining is called the endometrium. Endometrial cancer usually occurs in women
ARROCase: Locally Advanced Endometrial Cancer
 ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
ARROCase: Locally Advanced Endometrial Cancer Charles Vu, MD (PGY-3) Faculty Advisor: Peter Y. Chen, MD, FACR Beaumont Health (Royal Oak, MI) November 2016 Case 62yo female with a 3yr history of vaginal
Type I. Type II. Excess estrogen Lynch Endometrioid adenocarcinoma PTEN. High grade More aggressive Serous, Clear Cell p53
 Type I Excess estrogen Lynch Endometrioid adenocarcinoma PTEN Type II High grade More aggressive Serous, Clear Cell p53 Stage I IA IB Stage II Stage III IIIA IIIB IIIC IIIC1 IIIC2 Stage IV IVA IVB nodes
Type I Excess estrogen Lynch Endometrioid adenocarcinoma PTEN Type II High grade More aggressive Serous, Clear Cell p53 Stage I IA IB Stage II Stage III IIIA IIIB IIIC IIIC1 IIIC2 Stage IV IVA IVB nodes
Janjira Petsuksiri, M.D
 GYN malignancies Janjira Petsuksiri, M.D Outlines Cervical cancer Endometrial cancer Ovarian cancer Vaginal cancer Vulva cancer 2 CA Cervix Epidemiology - Second most common female cancer Risk factors
GYN malignancies Janjira Petsuksiri, M.D Outlines Cervical cancer Endometrial cancer Ovarian cancer Vaginal cancer Vulva cancer 2 CA Cervix Epidemiology - Second most common female cancer Risk factors
Gynaecology NSSG (Lancs & South Cumbria) Uterine Cancer Guidelines (V4.0)
 Uterine Cancer Guidelines (V4.0)") Gynaecology NSSG (Lancs & South Cumbria) Uterine Cancer Guidelines (V4.0) ** VALID ON DATE OF PRINTING ONLY all guidelines available on the Strategic Clinical Network website : GMLSC SCN Date first published
Gynaecology NSSG (Lancs & South Cumbria) Uterine Cancer Guidelines (V4.0) ** VALID ON DATE OF PRINTING ONLY all guidelines available on the Strategic Clinical Network website : GMLSC SCN Date first published
Cervical Cancer: 2018 FIGO Staging
 Cervical Cancer: 2018 FIGO Staging Jonathan S. Berek, MD, MMS Laurie Kraus Lacob Professor Stanford University School of Medicine Director, Stanford Women s Cancer Center Senior Scientific Advisor, Stanford
Cervical Cancer: 2018 FIGO Staging Jonathan S. Berek, MD, MMS Laurie Kraus Lacob Professor Stanford University School of Medicine Director, Stanford Women s Cancer Center Senior Scientific Advisor, Stanford
Uterine Malignancies. Collecting Cancer Data: Uterine Malignancies 10/7/2010. NAACCR Webinar Series 1. Questions. Fabulous Prizes!!!
 Uterine October 7, 2010 NAACCR 2010-2011 Webinar Series Session 1 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes!!! 3 NAACCR 2010-2011 Webinar
Uterine October 7, 2010 NAACCR 2010-2011 Webinar Series Session 1 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes!!! 3 NAACCR 2010-2011 Webinar
NAACCR Webinar Series /7/17
 COLLECTING CANCER DATA: UTERUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
COLLECTING CANCER DATA: UTERUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Gynecologic Malignancies. Kristen D Starbuck 4/20/18
 Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
The International Federation of Gynecology and Obstetrics (FIGO) updated the staging
 updated the staging") Continuing Education Column Revised FIGO Staging System Hee Sug Ryu, MD Department of Obstetrics and Gynecology, Ajou University School of Medicine E - mail : hsryu@ajou.ac.kr J Korean Med Assoc 2010;
Continuing Education Column Revised FIGO Staging System Hee Sug Ryu, MD Department of Obstetrics and Gynecology, Ajou University School of Medicine E - mail : hsryu@ajou.ac.kr J Korean Med Assoc 2010;
ARRO Case: Early-stage Endometrial Cancer
 ARRO Case: Early-stage Endometrial Cancer Ankit Modh, MD (PGY-4) Faculty Advisor: Mohamed A Elshaikh, MD Department of Radiation Oncology Henry Ford Cancer Institute Case Presentation 70 y/o African American
ARRO Case: Early-stage Endometrial Cancer Ankit Modh, MD (PGY-4) Faculty Advisor: Mohamed A Elshaikh, MD Department of Radiation Oncology Henry Ford Cancer Institute Case Presentation 70 y/o African American
One of the commonest gynecological cancers,especially in white Americans.
 Gynaecology Dr. Rozhan Lecture 6 CARCINOMA OF THE ENDOMETRIUM One of the commonest gynecological cancers,especially in white Americans. It is a disease of postmenopausal women with a peak incidence in
Gynaecology Dr. Rozhan Lecture 6 CARCINOMA OF THE ENDOMETRIUM One of the commonest gynecological cancers,especially in white Americans. It is a disease of postmenopausal women with a peak incidence in
Uterus Malignancies /5/15
 Collecting Cancer Data: Uterus 2014-2015 NAACCR Webinar Series February 5, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Uterus 2014-2015 NAACCR Webinar Series February 5, 2015 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer
 THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
THIS DOCUMENT North of Scotland Cancer Network Clinical Management Guideline for Endometrial Cancer Based on WOSCAN CMG with further extensive consultation within NOSCAN UNCONTROLLED WHEN PRINTED DOCUMENT
Cervical cancer presentation
 Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Carcinoma of the cervix: Carcinoma of the cervix is the second commonest cancer among women worldwide, with only breast cancer occurring more commonly. Worldwide, cervical cancer accounts for about 500,000
Adjuvant Therapies in Endometrial Cancer. Emma Hudson
 Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Adjuvant Therapies in Endometrial Cancer Emma Hudson Endometrial Cancer Most common gynaecological cancer Incidence increasing in Western world 1-2% cancer deaths 75% patients postmenopausal 97% epithelial
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type)
") Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
Chapter 2: Initial treatment for endometrial cancer (including histologic variant type) CQ01 Which surgical techniques for hysterectomy are recommended for patients considered to be stage I preoperatively?
The new FIGO classification in endometrial carcinoma
 The new FIGO classification in endometrial carcinoma Poster No.: C-1073 Congress: ECR 2012 Type: Educational Exhibit Authors: A. IGLESIAS CASTAÑON, M. Arias Gonzales, J. Mañas Uxó, 1 2 1 2 2 2 B. NIETO
The new FIGO classification in endometrial carcinoma Poster No.: C-1073 Congress: ECR 2012 Type: Educational Exhibit Authors: A. IGLESIAS CASTAÑON, M. Arias Gonzales, J. Mañas Uxó, 1 2 1 2 2 2 B. NIETO
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER CERVIX Site Group: Gynecology Cervix Author: Dr. Stephane Laframboise 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING AND
STUMPed for a Diagnosis Contemporary Management of Uterine Sarcomas
 UCSF Helen Diller Family Comprehensive Cancer Center Disclosures I have no financial disclosures STUMPed for a Diagnosis Contemporary Management of Uterine Sarcomas Lee-may Chen, MD Department of Obstetrics,
UCSF Helen Diller Family Comprehensive Cancer Center Disclosures I have no financial disclosures STUMPed for a Diagnosis Contemporary Management of Uterine Sarcomas Lee-may Chen, MD Department of Obstetrics,
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
Current staging of endometrial carcinoma with MR imaging
 Current staging of endometrial carcinoma with MR imaging Poster No.: C-1436 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Magalhaes, H. Donato, C. B. Marques, P. Gomes, F. Caseiro Alves; Coimbra/PT
Current staging of endometrial carcinoma with MR imaging Poster No.: C-1436 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Magalhaes, H. Donato, C. B. Marques, P. Gomes, F. Caseiro Alves; Coimbra/PT
receive adjuvant chemotherapy
 Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
Women with high h risk early stage endometrial cancer should receive adjuvant chemotherapy Michael Friedlander The Prince of Wales Cancer Centre and Royal Hospital for Women The Prince of Wales Cancer
29 Cancer of the Uterine Corpus
 29 Cancer of the Uterine Corpus Robbert Soeters INTRODUCTION Malignancies affecting the uterine corpus are endometrial adenocarcinoma and uterine sarcomas. ENDOMETRIAL ADENOCARCINOMA Endometrial adenocarcinoma
29 Cancer of the Uterine Corpus Robbert Soeters INTRODUCTION Malignancies affecting the uterine corpus are endometrial adenocarcinoma and uterine sarcomas. ENDOMETRIAL ADENOCARCINOMA Endometrial adenocarcinoma
Gynecologic Oncologist. Surgery Chemotherapy Radiation Therapy Hormonal Therapy Immunotherapy. Cervical cancer
 Gynecologic Oncology Pre invasive vulvar, vaginal, & cervical disease Vulvar Cervical Endometrial Uterine Sarcoma Fallopian Tube Ovarian GTD Gynecologic Oncologist Surgery Chemotherapy Radiation Therapy
Gynecologic Oncology Pre invasive vulvar, vaginal, & cervical disease Vulvar Cervical Endometrial Uterine Sarcoma Fallopian Tube Ovarian GTD Gynecologic Oncologist Surgery Chemotherapy Radiation Therapy
Page # 1. Endometrium. Cellular Components. Anatomical Regions. Management of SIL Thomas C. Wright, Jr. Most common diseases:
 Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Cervical Cancer 3/25/2019. Abnormal vaginal bleeding
 Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Cervical Cancer Abnormal vaginal bleeding Postcoital, intermenstrual or postmenopausal Vaginal discharge Pelvic pain or pressure Asymptomatic In most patients who are not sexually active due to symptoms
Case 1. Gynaecology Case Presentation. Objectives. Disclosures 22/10/ year old female Clinical history: Assess right ovarian cyst
 Gynaecology Case Presentation Organ Imaging 2016 University of Toronto Sarah Johnson 39 year old female Clinical history: Assess right ovarian cyst Clinically diagnosed endometriosis Started fertility
Gynaecology Case Presentation Organ Imaging 2016 University of Toronto Sarah Johnson 39 year old female Clinical history: Assess right ovarian cyst Clinically diagnosed endometriosis Started fertility
PORTEC-4. Patient seqnr. Age at inclusion (years) Hospital:
 Hospital:") May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
May 2016 Randomisation Checklist Form 1, page 1 of 2 Patient seqnr. Age at inclusion (years) Hospital: Eligible patients should be registered and randomised via the Internet at : https://prod.tenalea.net/fs4/dm/delogin.aspx?refererpath=dehome.aspx
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES CASE 1: FEMALE REPRODUCTIVE
 Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
Please complete prior to the webinar. HOSPITAL REGISTRY WEBINAR FEMALE REPRODUCTIVE SYSTEM EXERCISES PHYSICAL EXAMINATION CASE 1: FEMALE REPRODUCTIVE 3/5 Patient presents through the emergency room with
UTERINE SARCOMAS CURRENT THERAPEUTIC OPTIONS
 Review Journal of Translational Medicine and Research, volume 19, no. 1-2, 2014 UTERINE SARCOMAS CURRENT THERAPEUTIC OPTIONS N. Bacalbaæa 1, A. Traistaru 2, I. Bãlescu 3 1 Carol Davila University of Medicine
Review Journal of Translational Medicine and Research, volume 19, no. 1-2, 2014 UTERINE SARCOMAS CURRENT THERAPEUTIC OPTIONS N. Bacalbaæa 1, A. Traistaru 2, I. Bãlescu 3 1 Carol Davila University of Medicine
ENDOMETRIAL CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre)
") ENDOMETRIAL CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Source: UpToDate 2017, ASCO/CCO/Alberta provincial guidelines, NCCN Reviewed by: Dr. Sarah Glaze (Gynecologic
ENDOMETRIAL CANCER Updated Apr 2017 by: Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Source: UpToDate 2017, ASCO/CCO/Alberta provincial guidelines, NCCN Reviewed by: Dr. Sarah Glaze (Gynecologic
New FIGO Staging of Uterine malignancies with MR Imaging: Correlation with Surgical and Histopathologic Findings
 New FIGO Staging of Uterine malignancies with MR Imaging: Correlation with Surgical and Histopathologic Findings Poster No.: C-1548 Congress: ECR 2011 Type: Educational Exhibit Authors: J. Takahama, A.
New FIGO Staging of Uterine malignancies with MR Imaging: Correlation with Surgical and Histopathologic Findings Poster No.: C-1548 Congress: ECR 2011 Type: Educational Exhibit Authors: J. Takahama, A.
Endometrial Cancer. Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines
 Gynecological Cancer Treatment Guidelines") Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines Endometrial Cancer Emad R. Sagr, MBBS, FRCSC Consultant Gynecology Oncology Security forces Hospital, Riyadh Epidemiology
Saudi Gynecology Oncology Group (SGOG) Gynecological Cancer Treatment Guidelines Endometrial Cancer Emad R. Sagr, MBBS, FRCSC Consultant Gynecology Oncology Security forces Hospital, Riyadh Epidemiology
SCBT.MR MRI of Uterine Malignancy. Susan M. Ascher, MD, FSCBT.MR Georgetown University School of Medicine Washington, DC
 2 0 1 6 SCBT.MR MRI of Uterine Malignancy Susan M. Ascher, MD, FSCBT.MR Georgetown University School of Medicine Washington, DC aschers@gunet.georgetown.edu MUST READS Sala E, et al. The added role of
2 0 1 6 SCBT.MR MRI of Uterine Malignancy Susan M. Ascher, MD, FSCBT.MR Georgetown University School of Medicine Washington, DC aschers@gunet.georgetown.edu MUST READS Sala E, et al. The added role of
Index. B Bilateral salpingo-oophorectomy (BSO), 69
, 69") A Advanced stage endometrial cancer diagnosis, 92 lymph node metastasis, 92 multivariate analysis, 92 myometrial invasion, 92 prognostic factors FIGO stage, 94 histological grade, 94, 95 histologic cell
A Advanced stage endometrial cancer diagnosis, 92 lymph node metastasis, 92 multivariate analysis, 92 myometrial invasion, 92 prognostic factors FIGO stage, 94 histological grade, 94, 95 histologic cell
Index. Cytoplasm, nonepithelial malignant tumor features 70
 Accurette device 23 Adenosarcoma, differential diagnosis 80, 81 Arias-Stella reaction 65 Atypical endocervical cells 8 Atypical endometrial cells 8 Atypical glandular cells (AGC) 8, 9 Atypical glandular
Accurette device 23 Adenosarcoma, differential diagnosis 80, 81 Arias-Stella reaction 65 Atypical endocervical cells 8 Atypical endometrial cells 8 Atypical glandular cells (AGC) 8, 9 Atypical glandular
North of Scotland Cancer Network Clinical Management Guideline for Carcinoma of the Uterine Cervix
 THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
THIS DOCUMENT North of Scotland Cancer Network Carcinoma of the Uterine Cervix UNCONTROLLED WHEN PRINTED DOCUMENT CONTROL Prepared by A Kennedy/AG Macdonald/Others Approved by NOT APPROVED Issue date April
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
CPC on Cervical Pathology
 CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
CPC on Cervical Pathology Dr. W.K. Ng Senior Medical Officer Department of Clinical Pathology Pamela Youde Nethersole Eastern Hospital Cervical Smear: High Grade SIL (CIN III) Cervical Smear: High Grade
 TOC NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level evidence,
TOC NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level evidence,
Atypical Hyperplasia/EIN
 EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
UTERINE SARCOMA EXAMPLE OF A UTERINE SARCOMA USING PROPOSED TEMPLATE
 UTERINE SARCOMA EXAMPLE OF A UTERINE SARCOMA USING PROPOSED TEMPLATE Case: Adenosarcoma with heterologous elements and stromal overgrowth o TAH, BSO, omentectomy, staging biopsies of cul-de-sac, bladder
UTERINE SARCOMA EXAMPLE OF A UTERINE SARCOMA USING PROPOSED TEMPLATE Case: Adenosarcoma with heterologous elements and stromal overgrowth o TAH, BSO, omentectomy, staging biopsies of cul-de-sac, bladder
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป
 ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
ICRT รศ.พญ.เยาวล กษณ ชาญศ ลป Brachytherapy การร กษาด วยร งส ระยะใกล Insertion การสอดใส แร Implantation การฝ งแร Surface application การวางแร physical benefit of brachytherapy - very high dose of radiation
This protocol is intended to assist pathologists in providing
 Protocol for the Examination of Specimens From Patients With Carcinomas of the Endometrium A Basis for Checklists Steven G. Silverberg, MD, for the Members of the Cancer Committee, College of American
Protocol for the Examination of Specimens From Patients With Carcinomas of the Endometrium A Basis for Checklists Steven G. Silverberg, MD, for the Members of the Cancer Committee, College of American
Ovarian Cancer Includes Epithelial, Fallopian Tube, Primary Peritoneal Cancer, and Ovarian Germ Cell Tumors
 Ovarian Cancer Includes Epithelial, Fallopian Tube, Primary Peritoneal Cancer, and Ovarian Germ Cell Tumors Overview Ovarian epithelial cancer, fallopian tube cancer, and primary peritoneal cancer are
Ovarian Cancer Includes Epithelial, Fallopian Tube, Primary Peritoneal Cancer, and Ovarian Germ Cell Tumors Overview Ovarian epithelial cancer, fallopian tube cancer, and primary peritoneal cancer are
64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus
 Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
A randomised trial of non-selective versus selective adjuvant Therapy in high risk Apparent stage 1 Endometrial Cancer QA MANUAL
 A randomised trial of non-selective versus selective adjuvant Therapy in high risk Apparent stage 1 Endometrial Cancer QA MANUAL For Surgical Specimen Processing and Microscopy Central Pathology Quality
A randomised trial of non-selective versus selective adjuvant Therapy in high risk Apparent stage 1 Endometrial Cancer QA MANUAL For Surgical Specimen Processing and Microscopy Central Pathology Quality
Sarah Burton. Lead Gynae Oncology Nurse Specialist Cancer Care Cymru
 Sarah Burton Lead Gynae Oncology Nurse Specialist Cancer Care Cymru Gynaecological Cancers Cervical Cancers Risk factors Presentation Early sexual activity Multiple sexual partners Smoking Human Papiloma
Sarah Burton Lead Gynae Oncology Nurse Specialist Cancer Care Cymru Gynaecological Cancers Cervical Cancers Risk factors Presentation Early sexual activity Multiple sexual partners Smoking Human Papiloma
ENDOMETRIAL CANCER: A GUIDE FOR PATIENTS
 ENDOMETRIAL CANCER: A GUIDE FOR PATIENTS PATIENT INFORMATION BASED ON ESMO CLINICAL PRACTICE GUIDELINES This guide for patients has been prepared by Reliable Cancer Therapies (RCT) as a service to patients,
ENDOMETRIAL CANCER: A GUIDE FOR PATIENTS PATIENT INFORMATION BASED ON ESMO CLINICAL PRACTICE GUIDELINES This guide for patients has been prepared by Reliable Cancer Therapies (RCT) as a service to patients,
JMSCR Vol 05 Issue 11 Page November 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.78 A Histomorphological Study of Carcinoma
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.78 A Histomorphological Study of Carcinoma
Invasive Cervical Cancer: Squamous Cell, Adenocarcinoma, Adenosquamous
 Note: If available, clinical trials should be considered as preferred treatment options for eligible patients (www.mdanderson.org/gynonctrials). Other co-morbidities are taken into consideration prior
Note: If available, clinical trials should be considered as preferred treatment options for eligible patients (www.mdanderson.org/gynonctrials). Other co-morbidities are taken into consideration prior
Risk group criteria for tailoring adjuvant treatment in patients with endometrial cancer : a validation study of the GOG criteria
 Risk group criteria for tailoring adjuvant treatment in patients with endometrial cancer : a validation study of the GOG criteria Suk-Joon Chang, MD, Hee-Sug Ryu MD Gynecologic Cancer Center Department
Risk group criteria for tailoring adjuvant treatment in patients with endometrial cancer : a validation study of the GOG criteria Suk-Joon Chang, MD, Hee-Sug Ryu MD Gynecologic Cancer Center Department
Endometrium. Protocol applies to all carcinomas of the endometrium. Procedures Cytology (No Accompanying Checklist) Biopsy Curettage Hysterectomy
 Biopsy Curettage Hysterectomy") Endometrium Protocol applies to all carcinomas of the endometrium. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Endometrium Protocol applies to all carcinomas of the endometrium. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Cancer of the corpus uteri
 DOI: 10.1002/ijgo.12612 FIGO CANCER REPORT 2018 Cancer of the corpus uteri Frédéric Amant 1,2,3, * Mansoor Raza Mirza 4 Martin Koskas 5 Carien L. Creutzberg 6 1 Division of Gynecologic Oncology, University
DOI: 10.1002/ijgo.12612 FIGO CANCER REPORT 2018 Cancer of the corpus uteri Frédéric Amant 1,2,3, * Mansoor Raza Mirza 4 Martin Koskas 5 Carien L. Creutzberg 6 1 Division of Gynecologic Oncology, University
Uterine Cervix. Protocol applies to all invasive carcinomas of the cervix.
 Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Endometrial cancer. Szabolcs Máté MD. I. St. Department of Obstetrics and Gyneacology.
 Endometrial cancer Szabolcs Máté MD. I. St. Department of Obstetrics and Gyneacology dr.mate.szabolcs@gmail.com Epidemiology Developing countries Cervical cancer is the most common gyn. malignant tumor
Endometrial cancer Szabolcs Máté MD. I. St. Department of Obstetrics and Gyneacology dr.mate.szabolcs@gmail.com Epidemiology Developing countries Cervical cancer is the most common gyn. malignant tumor
CARCINOMA CERVIX. Dr. PREETHI REDDY. B. M S OBG II yr POST GRADUATE.
 CARCINOMA CERVIX Dr. PREETHI REDDY. B M S OBG II yr POST GRADUATE. Introduction Cervical cancer is the second most common female malignancy worldwide. It is responsible for 4,66,000 deaths annually worldwide
CARCINOMA CERVIX Dr. PREETHI REDDY. B M S OBG II yr POST GRADUATE. Introduction Cervical cancer is the second most common female malignancy worldwide. It is responsible for 4,66,000 deaths annually worldwide
Case Scenario 1. History
 History Case Scenario 1 A 53 year old white female presented to her primary care physician with post-menopausal vaginal bleeding. The patient is not a smoker and does not use alcohol. She has no family
History Case Scenario 1 A 53 year old white female presented to her primary care physician with post-menopausal vaginal bleeding. The patient is not a smoker and does not use alcohol. She has no family
Endometrial cancer. Cathrine Holland
 Endometrial cancer athrine Holland Abstract Endometrial cancers are the most common gynaecological malignancies in the UKwith approximately 4500 new cases occur each year and the incidence is rising. Increasingly
Endometrial cancer athrine Holland Abstract Endometrial cancers are the most common gynaecological malignancies in the UKwith approximately 4500 new cases occur each year and the incidence is rising. Increasingly
See NS R. Version Continue
 dis RT ± No pro otherapy/rt National Comprehensive Cancer Network N0-1 Resectable tomy ain RI ne an N2 N3 ADJUVANT RT ± chemotherapy c See Margins Stage IIIB ( Surgery ± chemo (categ ±RT Thoracoto Version
dis RT ± No pro otherapy/rt National Comprehensive Cancer Network N0-1 Resectable tomy ain RI ne an N2 N3 ADJUVANT RT ± chemotherapy c See Margins Stage IIIB ( Surgery ± chemo (categ ±RT Thoracoto Version
5 Mousa Al-Abbadi. Ola Al-juneidi & Obada Zalat. Ahmad Al-Tarefe
 5 Mousa Al-Abbadi Ola Al-juneidi & Obada Zalat Ahmad Al-Tarefe Abnormal Uterine Bleeding (AUB) AUB is a very common scenario or symptom where women complain of menorrhagia (heavy and/or for long periods),
5 Mousa Al-Abbadi Ola Al-juneidi & Obada Zalat Ahmad Al-Tarefe Abnormal Uterine Bleeding (AUB) AUB is a very common scenario or symptom where women complain of menorrhagia (heavy and/or for long periods),
Hitting the High Points Gynecologic Oncology Review
 Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
Hitting the High Points is designed to cover exam-based material, from preinvasive neoplasms of the female genital tract to the presentation, diagnosis and treatment, including surgery, chemotherapy, and
Guidelines for Assigning Summary Stage 2000
 Guidelines for Assigning Summary Stage 2000 Mary Lewis, CTR National Program of Cancer Registries 2014 NCRA Annual Meeting May 17, 2014 National Center for Chronic Disease Prevention and Health Promotion
Guidelines for Assigning Summary Stage 2000 Mary Lewis, CTR National Program of Cancer Registries 2014 NCRA Annual Meeting May 17, 2014 National Center for Chronic Disease Prevention and Health Promotion
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
The Good Uterine Sarcomas: What Do You Need to Know
 The Good Uterine Sarcomas: What Do You Need to Know Anais Malpica, M.D. Departments of Pathology and Gynecologic Oncology The University of Texas M.D. Anderson Cancer Center Matthew Powell, M.D. Division
The Good Uterine Sarcomas: What Do You Need to Know Anais Malpica, M.D. Departments of Pathology and Gynecologic Oncology The University of Texas M.D. Anderson Cancer Center Matthew Powell, M.D. Division
ENDOMETRIAL CANCER. Endometrial cancer is a great concern in UPDATE. For personal use only. Copyright Dowden Health Media
 For mass reproduction, content licensing and permissions contact Dowden Health Media. UPDATE ENDOMETRIAL CANCER Are lymphadenectomy and external-beam radiotherapy valuable in women who have an endometrial
For mass reproduction, content licensing and permissions contact Dowden Health Media. UPDATE ENDOMETRIAL CANCER Are lymphadenectomy and external-beam radiotherapy valuable in women who have an endometrial
Annual report of Gynecologic Oncology Committee, Japan Society of Obstetrics and Gynecology, 2013
 bs_bs_banner doi:10.1111/jog.12360 J. Obstet. Gynaecol. Res. Vol. 40, No. 2: 338 348, February 2014 Annual report of Gynecologic Oncology Committee, Japan Society of Obstetrics and Gynecology, 2013 Daisuke
bs_bs_banner doi:10.1111/jog.12360 J. Obstet. Gynaecol. Res. Vol. 40, No. 2: 338 348, February 2014 Annual report of Gynecologic Oncology Committee, Japan Society of Obstetrics and Gynecology, 2013 Daisuke
Jacqui Morgan March 6, 2019
 Jacqui Morgan March 6, 2019 Case 1 25yo, G2P1 Here for WWE, no problems, healthy, needs refill on OCPs. Pap- Abnormal Glandular Cells-NOS Now What?? Case 1 Colposcopy What findings? Case 1 ECC Cervical
Jacqui Morgan March 6, 2019 Case 1 25yo, G2P1 Here for WWE, no problems, healthy, needs refill on OCPs. Pap- Abnormal Glandular Cells-NOS Now What?? Case 1 Colposcopy What findings? Case 1 ECC Cervical
Adenocarcinoma of the Endometrium: An Institutional Review
 Pieter Baltens, 1580. Feast of St. George. From the collection of Dr. Gordon and Adele Gilbert of St. Petersburg, Florida. Adenocarcinoma of the Endometrium: An Institutional Review Denis Cavanagh, MD;
Pieter Baltens, 1580. Feast of St. George. From the collection of Dr. Gordon and Adele Gilbert of St. Petersburg, Florida. Adenocarcinoma of the Endometrium: An Institutional Review Denis Cavanagh, MD;
MRI for cervical and endometrial cancers. Dr Robert Bleehen Consultant Radiologist Cardiff & Vale UHB
 MRI for cervical and endometrial cancers Dr Robert Bleehen Consultant Radiologist Cardiff & Vale UHB RCR 06(1) RCR 06(1) Technique Pelvic multiphased-array coil Fasting? Buscopan? ABDOMEN!!! Cx:+/- HR
MRI for cervical and endometrial cancers Dr Robert Bleehen Consultant Radiologist Cardiff & Vale UHB RCR 06(1) RCR 06(1) Technique Pelvic multiphased-array coil Fasting? Buscopan? ABDOMEN!!! Cx:+/- HR
Algorithms for management of Cervical cancer
 Algithms f management of Cervical cancer Algithms f management of cervical cancer are based on existing protocols and guidelines within the ESGO comunity and prepared by ESGO Educational Committe as a
Algithms f management of Cervical cancer Algithms f management of cervical cancer are based on existing protocols and guidelines within the ESGO comunity and prepared by ESGO Educational Committe as a
THE RISK OF HYSTEROSCOPY IN SERIOUS ENDOMETRIAL DISEASES. Mary Girlie Z. Veloso, MD FPOGS, DMAS, Obstetrics - Gynecology
 THE RISK OF HYSTEROSCOPY IN SERIOUS ENDOMETRIAL DISEASES Mary Girlie Z. Veloso, MD FPOGS, DMAS, Obstetrics - Gynecology ABSTRACT Objective: The aim of this review article is to compare varied studies on
THE RISK OF HYSTEROSCOPY IN SERIOUS ENDOMETRIAL DISEASES Mary Girlie Z. Veloso, MD FPOGS, DMAS, Obstetrics - Gynecology ABSTRACT Objective: The aim of this review article is to compare varied studies on
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER
 UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
Most common cancer Africans & Asians more prone because of poor socioeconomic condition Drastic decline in west as more detection of preinvasive
 CANCER CERVIX Most common cancer Africans & Asians more prone because of poor socioeconomic condition Drastic decline in west as more detection of preinvasive leison by PAP Smears. Etiology: Age - 2 peaks
CANCER CERVIX Most common cancer Africans & Asians more prone because of poor socioeconomic condition Drastic decline in west as more detection of preinvasive leison by PAP Smears. Etiology: Age - 2 peaks
Gynecological Cancers in Primary Care
 Gynecological Cancers in Primary Care Nora M. Lersch MSN CRNP AOCNP Division of Gynecological Oncology Objectives Identify the incidence of ovarian, cervical, vulvar and endometrial cancer Identify common
Gynecological Cancers in Primary Care Nora M. Lersch MSN CRNP AOCNP Division of Gynecological Oncology Objectives Identify the incidence of ovarian, cervical, vulvar and endometrial cancer Identify common
Newton Wellesley Hospital 2013
 Newton Wellesley Hospital 20 Standard 4.6 Assessment and Evaluation of Treatment Planning Endometrial Cancer Each year a physician member of the cancer committee conducts a study to ensure that diagnostic
Newton Wellesley Hospital 20 Standard 4.6 Assessment and Evaluation of Treatment Planning Endometrial Cancer Each year a physician member of the cancer committee conducts a study to ensure that diagnostic
Imaging of endometrial and cervical cancer
 Insights Imaging (2010) 1:309 328 DOI 10.1007/s13244-010-0042-7 REVIEW Imaging of endometrial and cervical cancer Shilpa Patel & Sidath H. Liyanage & Anju Sahdev & Andrea G. Rockall & Rodney H. Reznek
Insights Imaging (2010) 1:309 328 DOI 10.1007/s13244-010-0042-7 REVIEW Imaging of endometrial and cervical cancer Shilpa Patel & Sidath H. Liyanage & Anju Sahdev & Andrea G. Rockall & Rodney H. Reznek
Chapter 8 Adenocarcinoma
 Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
Page 80 Chapter 8 Adenocarcinoma Overview In Japan, the proportion of squamous cell carcinoma among all cervical cancers has been declining every year. In a recent survey, non-squamous cell carcinoma accounted
Essex & East Suffolk Gynae Cancer Supra-Network
 Essex & East Suffolk Gynae Cancer Supra-Network Gynaecological Cancers Referral, Diagnosis and Management Guidelines Constitution Version Number 9.0 Author Members of the NSSG Date Written August 2010
Essex & East Suffolk Gynae Cancer Supra-Network Gynaecological Cancers Referral, Diagnosis and Management Guidelines Constitution Version Number 9.0 Author Members of the NSSG Date Written August 2010
Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy
 Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy Stephanie Yap, M.D. University Gynecologic Oncology Northside Cancer Institute Our Learning Objectives Review survival rates,
Gynecologic Cancer Surveillance and Survivorship: Informing Practice and Policy Stephanie Yap, M.D. University Gynecologic Oncology Northside Cancer Institute Our Learning Objectives Review survival rates,
PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT
 PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT QUESTION #1 WHICH OF THE FOLLOWING IS NOT A RISK FACTOR FOR CERVICAL CANCER? A. HIGH RISK HPV B. CIGARETTE SMOKING C.
PRE TEST CERVICAL SCREENING MANAGEMENT COLPOSCOPY PATHOLOGIC DIAGNOSIS AND TREATMENT QUESTION #1 WHICH OF THE FOLLOWING IS NOT A RISK FACTOR FOR CERVICAL CANCER? A. HIGH RISK HPV B. CIGARETTE SMOKING C.
Disclosure. Case. Mixed Tumors of the Uterine Corpus and Cervix. I have nothing to disclose
 Mixed Tumors of the Uterine Corpus and Cervix Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Department of Pathology Brigham and Women s Hospital Boston, MA UCSF Current Issues in Anatomic
Mixed Tumors of the Uterine Corpus and Cervix Marisa R. Nucci, M.D. Division of Women s and Perinatal Pathology Department of Pathology Brigham and Women s Hospital Boston, MA UCSF Current Issues in Anatomic
GENERAL DATA. Sex : female Age : 40 years old Marriage status : married
 GENERAL DATA Sex : female Age : 40 years old Marriage status : married CHIEF COMPLAINT Bilateral ovarian tumors discovered by sonography accidentally PRESENT ILLNESS 2003-06-26 :bilateral ovarian tumors
GENERAL DATA Sex : female Age : 40 years old Marriage status : married CHIEF COMPLAINT Bilateral ovarian tumors discovered by sonography accidentally PRESENT ILLNESS 2003-06-26 :bilateral ovarian tumors
Relapse Patterns and Outcomes Following Recurrence of Endometrial Cancer in Northern Thai Women
 DOI:http://dx.doi.org/10.7314/APJCP.2015.16.9.3861 Relapse Patterns and Outcomes Following Recurrence of Endometrial Cancer in Northern Thai Women RESEARCH ARTICLE Relapse Patterns and Outcomes Following
DOI:http://dx.doi.org/10.7314/APJCP.2015.16.9.3861 Relapse Patterns and Outcomes Following Recurrence of Endometrial Cancer in Northern Thai Women RESEARCH ARTICLE Relapse Patterns and Outcomes Following
Coversheet for Network Site Specific Group Agreed Documentation
 Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Coversheet for Network Site Specific Group Agreed Documentation This sheet is to accompany all documentation agreed by Pan Birmingham Cancer Network Site Specific Groups. This will assist the Network Governance
Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva Malignant melanoma sho
 Carcinoma Vulva & Vagina Subdivisi Onkologi Ginekologi Bagian Obgin FK USU Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva
Carcinoma Vulva & Vagina Subdivisi Onkologi Ginekologi Bagian Obgin FK USU Vulvar Carcinoma. Definition: Cases should be classified as carsinoma of the vulva when the primary site growth is in the vulva
Michael G. Kelly, MD Gynecologic Oncologist University of Colorado Cancer Center
 Michael G. Kelly, MD Gynecologic Oncologist University of Colorado Cancer Center 50 yo healthy postmenopausal female with BMI = 35 with screening PAP smear = AGUS. What is the next step? (1) Colposcopy
Michael G. Kelly, MD Gynecologic Oncologist University of Colorado Cancer Center 50 yo healthy postmenopausal female with BMI = 35 with screening PAP smear = AGUS. What is the next step? (1) Colposcopy
Gynecological sarcoma
 Gynecological sarcoma Therapy of the gynecological sarcoma Treatment gynecologist s update view Frédéric Amant MD PhD Gynecologic Oncology, KU Leuven, Belgium Center Gynecologic Oncology Amsterdam (CGOA),
Gynecological sarcoma Therapy of the gynecological sarcoma Treatment gynecologist s update view Frédéric Amant MD PhD Gynecologic Oncology, KU Leuven, Belgium Center Gynecologic Oncology Amsterdam (CGOA),
MRI in Cervix and Endometrial Cancer
 28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
28th Congress of the Hungarian Society of Radiologists RCR Session Budapest June 2016 MRI in Cervix and Endometrial Cancer DrSarah Swift St James s University Hospital Leeds, UK Objectives Cervix and endometrial
Management of Endometrial Hyperplasia
 Management of Endometrial Hyperplasia I have nothing to disclose. Stefanie M. Ueda, M.D. Assistant Clinical Professor UCSF Division of Gynecologic Oncology Female Malignancies in the United States New
Management of Endometrial Hyperplasia I have nothing to disclose. Stefanie M. Ueda, M.D. Assistant Clinical Professor UCSF Division of Gynecologic Oncology Female Malignancies in the United States New
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
Vaginal intraepithelial neoplasia
 Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the
Vaginal intraepithelial neoplasia The terminology and pathology of VAIN are analogous to those of CIN (VAIN I-III). The main difference is that vaginal epithelium does not normally have crypts, so the