Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
|
|
|
- Philomena Thornton
- 5 years ago
- Views:
Transcription
1 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016
2 17th Annual Advances in Oncology September 30-October 1, 2016 Sacramento, CA Anna Orlowski, J.D. End of Life Option Act: Medical Legal Considerations. No relevant financial relationships in the past twelve months by presenter or spouse/partner. The speaker will directly disclosure the use of products for which are not labeled (e.g., off label use) or if the product is still investigational.
3 Early Stage Breast Cancer Extended adjuvant endocrine therapy Anthracyclines in HER2- breast cancer Platinum in TNBC Capecitabine for residual disease Dual HER2 blockade Metastatic Breast Cancer Endocrine monotherapy versus combination therapy Endocrine resistance and PI3K inhibition Role of T-DM1 in HER2+ disease Checkpoint inhibitors in TNBC
4 Early Stage Breast Cancer
5 Long term recurrence risks after use of endocrine therapy for only 5 years EBCTCG: Data from 91 trials on each individual with ER+ disease allocated only 5 years of endocrine therapy N= 46,000 women who were alive and disease free at 5 years Main finding: Even after 5 years of endocrine therapy, recurrences continue steadily, at least to year 20; significant even for T1N0 disease Pan H et al, 2016 ASCO Annual Meeting, abstract 505
6 EBCTCG: Long term recurrence risks after 5 years of endocrine therapy Slide 12 Pan H et al, 2016 ASCO Annual Meeting, abstract 505
, and improves survival by 39% at 64 months f/u (HR 0.61; p < 0.")
7 Benefits of extended adjuvant endocrine therapy MA.17: After 5 years of tamoxifen, the addition of 5 years of adjuvant letrozole reduces breast cancer recurrence by 43% compared to placebo (HR 0.57; p < 0.001), and improves survival by 39% at 64 months f/u (HR 0.61; p < 0.001) 1,2 ATLAS/aTTOM: Compared to 5 years of tamoxifen, 10 years of tamoxifen reduces breast cancer mortality by 15% in all years and by 25% starting at year 10. 3,4 1. Goss P et al. NEJM 2003;349(19): Jin H et al. J Clin Oncol 2012;30(7): Davies C et al. Lancet 2013;381: Gray RG et al. J Clin Oncol 2013;31 (suppl;abstr 5).
8 MA.17R Trial Study Design n=1918 randomized phase III Letrozole 2.5 mg po daily +/- Tamoxifen any duration AI 4.5 to 6 Years R Hormone receptor positive Postmenopausal and disease-free 1:1 Placebo 5 years Goss P, et al. ASCO 2016, LBA1

9 MA.17R Disease-free survival Median f/u 6.3 years Goss P, et al. ASCO 2016, LBA1

10 MA.17R DFS by pre-specified subgroups Goss P, et al. ASCO 2016, LBA1
11 MA.17R MA.17R is the first study to show benefit of extending AI use beyond 5 years 34% reduction in disease recurrence. There were no significant differences between the placebo group and the letrozole group related to most measures of quality of life. Bone health remains an issue. Biomarkers/multi-gene signatures are needed to determine which patients are most at risk for late recurrences
 2 However, no comparison to combination or sequential anthracycline and taxane regimen.")
12 1 Can anthracyclines be omitted in patients with high risk lymph node negative or node positive, HER2- negative breast cancer? TC x 4 vs AC x 4 demonstrated OS superior for TC (HR =0.69; p=0.032) 2 However, no comparison to combination or sequential anthracycline and taxane regimen. TC x 6, often used in clinical practice, became the standard to compare with TaxAC regimens 1 Blum JL et al, ASCO 2016, abstract Jones S et al, J Clin Oncol 2009;27:
13 ABC Trials Study Design HER2 - Lymph node + High Risk LNn = 4,130 phase III R Arm 1 (TaxAC) TAC q 3 wk x 6 cycles or AC q 3 wk x 4 cycles paclitaxel q 1 wk x 12 or AC q 2 wk x 4 cycles paclitaxel q 1 wk x 12 or AC q 2 wk x 4 cycles paclitaxel q 2 wk x 4 Arm 2 Docetaxel/cyclophosphamide (TC) TC x 6 cycles * High risk lymph node negative defined as pt2-t3 pn0; or pt1c if pn0 then must be either ER and PR negative; ER+ or PR+ and either Grade 3 or Oncotype Dx Recurrence Score > 31 for USOR and > 25 for B-46I/07132 and B-49
14 ABC Trials: Invasive Disease Free Survival The primary aim: Determine if invasive disease free survival with TC is non-inferior compared to TaxAC, defined by HR of less than 1.18 Blum JL et al, ASCO 2016, abstract 1000

15 Slide 17 Blum JL et al, ASCO 2016, abstract 1000
16 Triple Negative Breast Cancer has Worse Outcome if Residual Disease Present after Neoadjuvant Chemotherapy TNBC pts (n=255) compared with non-tnbc pts (n=863) had higher pcr rates (22% vs 11%) However, TNBC pts had lower 3-yr PFS and OS rates If pcr was achieved, TNBC pts and non-tnbc pts had similar outcome If residual disease present, TNBC pts had worse outcome compared with non-tnbc pts Liedtke C et al. J Clin Oncol 2008;26:
17 GeparSixto Neoadjuvant Study Design TNBC regimen n = 315 phase II TNBC R Paclitaxel 80 mg/m2 q 1 wk x 18 Non-pegylated liposomal doxorubicin 20 mg/m2 q 1wk x 18 Bevacizumab 15 mg/kg q 3 wk Paclitaxel 80 mg/m2 q 1 wk x 18 Non-pegylated liposomal doxorubicin 20 mg/m2 q 1wk x 18 Bevacizumab 15 mg/kg q 3 wk Carboplatin AUC 1.5 q wk x 18 S U R G E R Y pcr, % PMCb PM P Value TNBC (n = 315) gbrca wild type (n = 241) gbrca mutant (n = 50) von Minckwitz G et al. SABCS Abstract S2-04.

18 GeparSixto: DFS advantage demonstrated with carboplatin in TNBC von Minckwitz G et al. SABCS Abstract S2-04.


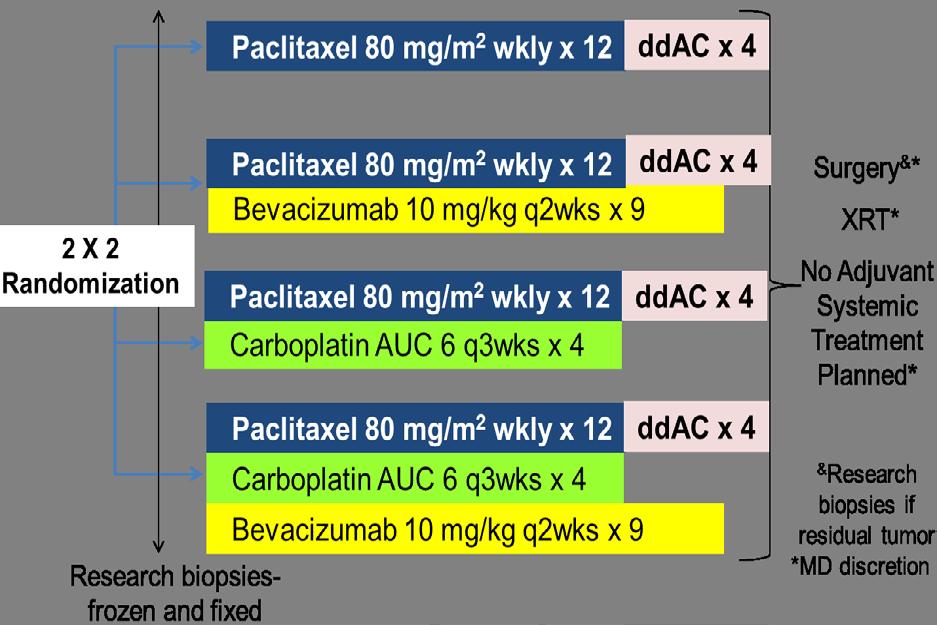
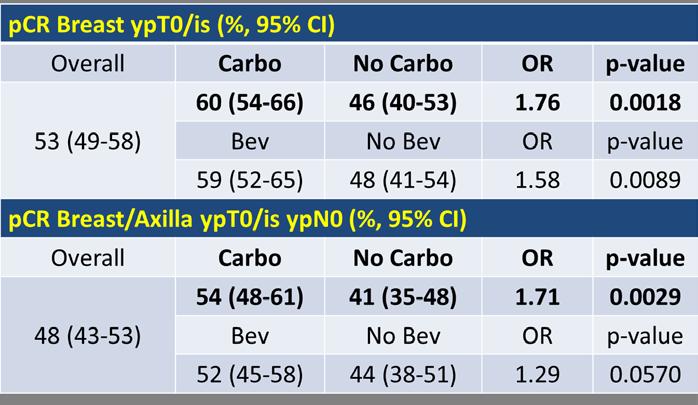
19 CALGB 40603: phase II trial neoadjuvant chemo/bev +/- carbo +/- bev pcr rate in TNBC Sikov, JCO 2015
20 CALGB 40603: No DFS advantage with carboplatin in TNBC Sikov WM, et al. J Clin Oncol. 2015;33:13-21.
21 Platinum therapy in early stage TNBC Prospective randomized data are conflicting regarding use of pathologic CR as surrogate for DFS on a trial level, though underpowered to show this. Studies consistently show that achieving a pathologic CR is prognostic on an individual patient level. The routine addition of a platinum agent to ACT-based neoadjuvant therapy for patients with early stage TNBC should not be considered a standard of care. However, higher pcr rates associated with the addition of carboplatin may be beneficial for some patients. Incorporation of robust correlative studies in future trials is needed to identify TNBC patients who will benefit from platinum.
22 NRG-BR003 - Randomized Phase III Trial of Adjuvant Therapy Comparing Doxorubicin Plus Cyclophosphamide Followed by Weekly Paclitaxel with or without Carboplatin for Node-Positive or High-Risk Node-Negative Triple-Negative Invasive Breast Cancer N = 990 Resected LN+ or High Risk LN- ER/PR/HER2- Early stage BC Primary endpoint: IDFS R AC q 2 wks x 4 followed by paclitaxel q 1 wk x 12 AC q 2 wks x 4 followed by paclitaxel q 1 wk x 12 plus carboplatin AUC 5 q 3 wk x 4
23 Residual disease after neoadjuvant chemotherapy and surgery: CREATE-X n = 910 phase III HER2-, Stage I-IIIB NAC Surgery Pathology Non-pCR or node + R Control Standard Therapy Standard Therapy + Capecitabine 2500 mg/m 2 /d d 1-14 q 3 wk x 8 Stratified by ER status, age, neoadjuvant chemotherapy, use of 5- FU, institution, node status Standard therapy: HR+: Hormone therapy HR-: No further systemic treatment 1. Toi M, et al. SABCS Abstract S Ohtani S, et al. SABCS Abstract P
24 CREATE-X: 5-Yr Efficacy Capecitabine achieved significantly higher 5-yr DFS and OS in HER2- BC pts with residual disease Characteristic, % Capecitabine (n = 440) No Capecitabine (n = 445) 5-yr DFS yr OS HR (95% CI) 0.70 ( ) 0.60 ( ) P Value <.01 Toi M, et al. SABCS Abstract S1-07.
25 Capecitabine may have benefit in high risk populations CREATE-X subgroup analysis suggests the benefit was predominantly in the TNBC subgroup (HR 0.58). Other studies have shown benefits of (neo)adjuvant capecitabine added to standard chemotherapy in TNBC subgroups (ABCSG-24; FinnXX), but did not achieve their primary endpoints, so were negative overall. Results of CREATE-X should be confirmed in an adjuvant study that would evaluate high risk population of TNBC patients.
26 EA1131: A randomized phase III post-operative trial of platinum agent chemotherapy vs. capecitabine in patients with residual triple-negative breast cancer (TNBC) following neoadjuvant chemotherapy Accrual goal 750 TNBC Stage II/III NAC Surgery Pathology > 1 cm residual disease Tissue submission PAM 50 analysis R Cisplatin 75 mg/m 2 d1 q 3 wk x 4 cycles or Carboplatin AUC 6 d1 q 3 wk x 4 cycles Capecitabine 1000 mg/m 2 /d d1-14 q 3 wk x 6 cycles * Choice of platinum agent will be per treating physician discretion Primary endpoint: IDFS in patients with basal-like TNBC Secondary endpoints: IDFS in patients with non basal-like TNBC, OS, RFS
27 Metastatic Breast Cancer
28 Endocrine monotherapy in first line metastatic setting Postmenopausal patients with HR+ metastatic breast cancer without prior exposure to AIs, or those with late relapses, recommendation is for non-steroidal AI monotherapy (ASCO guidelines). Phase II FIRST trial results suggest fulvestrant may be superior to non-steroidal AI as front-line therapy. fulvestrant (500mg) (F) vs anastrazole (A) n = 205 postmenopausal, HR+ pts TTP: F 23.4 mo A 13.1 mo HR 0.66 p= 0.01 OS: F 55.1 mo A 48.4 mo HR 0.70 p=0.04 Confirmatory phase III FALCON trial ongoing Ellis M, et al, J Clin Oncol 2015; Robertson J et al, SABC 2010, abstract S1-3 Robertson J, et al, J Clin Oncol 2009;27:
29 Endocrine combination therapy in first line metastatic setting Preclinical studies identified luminal ER positive subtype as being palbociclib-sensitive with synergy demonstrated between palbociclib and anti-estrogens. 1 PALOMA-I, randomized phase II study of palbociclib plus letrozole vs letrozole alone as first-line therapy for HR+ advanced breast cancer 2 Addition of palbociclib to letrozole demonstrated 10- month improvement in PFS over letrozole alone (HR 0.49; p = ) and acceptable safety profile Accelerated FDA approval granted 1. Finn et al, Breast Cancer Research 2009; 2. Finn et al, Lancet Oncol 2015.
30 PALOMA 2 Study Design Prospective, randomized, double-blind, placebo-controlled phase III trial n = 666 phase Postmenopausal HR+ HER2- advanced breast cancer No prior treatment for advanced disease AI resistant patients excluded R Palbociclib 125 mg daily (3/1 schedule) + Letrozole 2.5 mg daily Placebo (3/1 schedule) + Letrozole 2.5 mg daily Finn R et al, ASCO 2016, Abstract 507
 Finn R et al, ASCO 2016,")
31 PALOMA 2 PFS Investigator-Assessed (ITT Population) Finn R et al, ASCO 2016, Abstract 507

32 PALOMA 2 Finn R et al, ASCO 2016, Abstract 507
33 PALOMA-2 Safety Most common AE was neutropenia: 80% in palbociclib plus letrozole arm vs 6% in placebo plus letrozole. SAEs occurred in < 1% of pts, except febrile neutropenia in 1.6% in the palbociclib plus letrozole arm vs 0 in placebo arm. Grade 3/4 non-hematologic AEs uncommon in both arms. Deliverabilty was > 90% in palbociclib arm and 94% in placebo arm Finn R et al, ASCO 2016, Abstract 507
34 PALOMA 3: Palbociclib and fulvestrant in endocrine resistant metastatic breast cancer PALOMA 3 phase III trial (n=512) evaluated palbociclib plus fulvestrant versus fulvestrant alone in patients with HR+ advanced breast cancer that had progressed on prior endocrine therapy Palbociclib plus fulvestrant demonstrated significant increase in PFS, 9.2 mo vs 3.8 mo (HR 0.42; p < 0.001), similar toxicity profile as observed in PALOMA-1 Basis for FDA approval of palbociclib with fulvestrant Turner NC, et al. NEJM 2015;373:
35 Sequencing endocrine therapies in the metastatic setting for postmenopausal patients 1 st line options: nonsteroidal AI monotherapy fulvestrant monotherapy (await FALCON) non-steroidal AI plus CDK 4/6 inhibitor (PALOMA-2) non-steroidal AI plus fulvestrant (SWOG 0226) If use non-steroidal AI plus CDK 4/6 inhibitor upfront, then challenging to determine subsequent lines of therapy after progression If use non-steroidal AI monotherapy upfront, then can use fulvestrant plus CDK 4/6 inhibitor 2 nd line and exemestane +/- everolimus 3 rd line
36 PI3K inhibition in endocrine resistant metastatic breast cancer: BELLE-2 Study n = 1147 phase III Postmenopausal HR+ HER2- advanced breast cancer with progression on/after AI therapy R Buparlisib 100 mg/day + Fulvestrant 500 mg Placebo + Fulvestrant 500 mg Baselga J, et al. SABCS Abstract S6-01.
37 BELLE-2: PFS results and efficacy by PI3KCA mutation in ctdna Median PFS, Mos n Buparlisib + Fulvestrant (n = 576) Placebo + Fulvestrant (n = 571) Overall population 1, PI3K-activated pts ctdna PIK3CA mutant ctdna PIK3CA nonmutant HR (95% CI) 0.78 ( ) 0.76 ( ) 0.56 ( ) 1.05 ( ) PFS significantly longer with use of buparlisib + fulvestrant in the overall population but not significantly extended in pt population with a known PI3K activation status (threshold p =.01 in trial design) Buparlisib + fulvestrant extended PFS in pts with PIK3CA mutations in circulating tumor DNA versus fulvestrant alone, but not in pts with non-mutant PIK3CA. P Value < <
38 TH3RESA: Study Design N = 602 Phase 3 Pts with HER2+ advanced breast cancer, 2 prior anti- HER2 therapies R T-DM1 3.6 mg/kg q3w IV Therapy of Physician s Choice PD PD T-DM1 Optional crossover. Wildiers H, et al. SABCS Abstract S5-05.
39 TH3RESA: Final OS analysis Median OS significantly improved with use of T-DM1 vs physician-selected therapy in pretreated pts with HER2+ MBC: 22.7 months vs 15.8 months HR 0.68 (95% CI: ; P =.0007) 44.9% of TPC arm pts received T-DM1 crossover therapy T-DM1 is preferred treatment for patients whose metastatic disease has progressed after treatment with a combination of a taxane based chemotherapy and trastuzumab, with or without pertuzumab. Wildiers H, et al. SABCS Abstract S5-05.
40 Immunotherapy in TNBC Cancer cells can use PD1/PDL1 pathway to evade the immune system by expressing PDL1 and down regulating immune responses. Blocking the interaction of PD1 and PDL1 releases the stop on T cells and allows T cell mediated immune responses against tumor cells. There is higher expression of PDL1 mrna in TNBC compared to non-tnbc. TNBCs have high mutational burden and may produce neoantigens leading to an immune response. 20 to 30% of TNBCs are associated with tumor infiltrating lymphocytes (TILs) which can facilitate an immune response.
41 Immune checkpoint blockade in metastatic TNBC Pembrolizumab ant-pd-1 antibody blocks interaction PD- 1 receptor and its ligands PD-L1 and PD-L2 Phase 1B trial in metastatic TNBC KEYNOTE-012 n = 32; 46.9% had > 3 prior line of therapy all tumors positive for PD-L1 expression pembrolizumab 10 mg/kg IV every 2 weeks response rate 18.5% (CR 1 pt; PR 4 pts) median duration of response not reached (range 15 to 40 months) trend toward more clinical benefit with increasing PD-L1 expression Buisseret L et al, Annals of Onc 2015 ;26 : 6-9.

 and without (57%)")
42 Immune checkpoint blockade with chemotherapy in metastatic TNBC Atezolizumab anti-pdl1 antibody blocks PD-L1/PD-1 and PD-L1/B7.1 interaction. Phase 1-b evaluated atezolizumab in combination with weekly nabpaclitaxel in metastatic TNBC pts Up to 3 prior lines of chemotherapy Responses seen in pts with (77%) and without (57%) PD-L1 expression Adams S et al. ASCO 2016, abstract 1007.
43 Conclusions Early Stage Breast Cancer Extended adjuvant AI therapy for 10 years improves DFS in HR+ postmenopausal BC patients. Adjuvant anthracyclines improve DFS in LN positive and high risk LN negative HER2- early stage BC patients. The role of platinum in early stage TNBC is not yet defined. Trials are ongoing to determine who will benefit. Capecitabine for TNBC patients with residual disease after surgery improved OS in one study and needs confirmation. Advanced breast cancer CDK 4/5 inhibition plus endocrine therapy improves DFS in advanced HR+ BC, but which line of therapy, which patients? T-DM1 improves OS in HER2+ advanced breast cancer in 2 nd line therapy and beyond. Checkpoint inhibition in TNBC can provide durable responses and is being tested further. Some PDL-1 expression appears better than none.
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017
 TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy
 Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Triple Negative Breast Cancer: Part 2 A Medical Update
 Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Recent Update in Management of Breast Cancer: Medical Oncology. Jin Hee Ahn, M.D., PhD. 23-April-2015
 2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
ASCO 2017 BREAST CANCER HIGHLIGHTS
 Post-ASCO 24 th June 2017, Dolce La Hulpe, Belgium ASCO 2017 BREAST CANCER HIGHLIGHTS Martine J. Piccart-Gebhart, MD, PhD Jules Bordet Institute, Brussels, Belgium Université Libre de Bruxelles Breast
Post-ASCO 24 th June 2017, Dolce La Hulpe, Belgium ASCO 2017 BREAST CANCER HIGHLIGHTS Martine J. Piccart-Gebhart, MD, PhD Jules Bordet Institute, Brussels, Belgium Université Libre de Bruxelles Breast
Systemic Therapy for Locally Advanced Breast Cancer
 Systemic Therapy for Locally Advanced Breast Cancer Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology National University Cancer Institute, Singapore Clinical Care Senior Principal
Systemic Therapy for Locally Advanced Breast Cancer Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology National University Cancer Institute, Singapore Clinical Care Senior Principal
Overcoming resistance to endocrine or HER2-directed therapy
 Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Triple-Negative Breast Cancer
 June 2017 Triple-Negative Breast Cancer Amir Sonnenblick, MD, PhD Sharett institute of oncology Hadassah-Hebrew university medical center, Jerusalem, Israel This presentation is the intellectual property
June 2017 Triple-Negative Breast Cancer Amir Sonnenblick, MD, PhD Sharett institute of oncology Hadassah-Hebrew university medical center, Jerusalem, Israel This presentation is the intellectual property
Breast cancer treatment
 Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Triple Negative Breast Cancer. Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008
 Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016
 Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016 Yes! Age disparities vary by tumor subtype Genomic risk prediction data in young women Adjuvant systemic therapy
Any News in EBC? Ann H. Partridge, MD, MPH Dana-Farber Cancer Institute November 11, 2016 Yes! Age disparities vary by tumor subtype Genomic risk prediction data in young women Adjuvant systemic therapy
Disease Update: Metastatic Breast Cancer
 Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Early Stage Disease. Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center
 SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Role of chemotherapy in BRCA and Triple negative breast cancer. Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos
 Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
HER2-positive Breast Cancer
 HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Manejo do câncer de mama RH+ na adjuvância: o que há de novo?
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari
 Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari Neoadjuvant Treatment A window of opportunity Rational: Historically proposed to enable breast-conserving surgery
Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari Neoadjuvant Treatment A window of opportunity Rational: Historically proposed to enable breast-conserving surgery
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives
 Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer
 TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer Marta Bonotto Department of Oncology University Hospital of Udine TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive
TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer Marta Bonotto Department of Oncology University Hospital of Udine TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive
Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici
 Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici Laura Orlando UOC Oncologia & Breast Unit Brindisi Verona 22/04/2016 Summary Studi con
Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici Laura Orlando UOC Oncologia & Breast Unit Brindisi Verona 22/04/2016 Summary Studi con
DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA
 Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
2014 San Antonio Breast Cancer Symposium Review
 2014 San Antonio Breast Cancer Symposium Review HER2 Positive Disease 01-10-2015 Elisavet Paplomata, MD Assistant Professor Hematology & Medical Oncology Emory University Winship Cancer Institute S6-01
2014 San Antonio Breast Cancer Symposium Review HER2 Positive Disease 01-10-2015 Elisavet Paplomata, MD Assistant Professor Hematology & Medical Oncology Emory University Winship Cancer Institute S6-01
Targeting CDK 4/6. Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine
 2016.04.30 GBCC Education Symposium Targeting CDK 4/6 Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine Contents Cyclins -CDKs in cell cycle control CDK 4/6 in breast cancer Preclinical
2016.04.30 GBCC Education Symposium Targeting CDK 4/6 Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine Contents Cyclins -CDKs in cell cycle control CDK 4/6 in breast cancer Preclinical
NeoadjuvantTreatment In BC When, How, Who?
 NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
Predicting outcome in metastatic breast cancer
 Predicting outcome in metastatic breast cancer Aleix Prat, MD, PhD Medical Oncology Department Translational Genomics and Targeted Therapeutics in Solid Tumors Monday, 15 th January, Manchester, UK Disclosures
Predicting outcome in metastatic breast cancer Aleix Prat, MD, PhD Medical Oncology Department Translational Genomics and Targeted Therapeutics in Solid Tumors Monday, 15 th January, Manchester, UK Disclosures
Update in the treatment of Her2- overexpressing breast cancers. Fabrice ANDRE Institut Gustave Roussy Villejuif, France
 Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Novel Chemotherapy Agents for Metastatic Breast Cancer. Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX
 Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer
 Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it?
 Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland
 What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Multimedia Appendix 6 Educational Materials Table of Contents. Intervention Educational Materials Audio Script (version 1)
") Multimedia Appendix 6 Educational Materials Table of Contents Intervention Educational Materials... 1 Audio Script (version 1)... 1 Text (version 1)... 5 Slides (version 1)... 17 Audio Script (version
Multimedia Appendix 6 Educational Materials Table of Contents Intervention Educational Materials... 1 Audio Script (version 1)... 1 Text (version 1)... 5 Slides (version 1)... 17 Audio Script (version
Triple Negative Breast Cancer
 GASCO 2016 San Antonio Breast Cancer Symposium Review Triple Negative Breast Cancer Amelia Zelnak, MD, MSc Atlanta Cancer Care Northside Hospital Cancer Institute Disclosures: consultant for Novartis,
GASCO 2016 San Antonio Breast Cancer Symposium Review Triple Negative Breast Cancer Amelia Zelnak, MD, MSc Atlanta Cancer Care Northside Hospital Cancer Institute Disclosures: consultant for Novartis,
PRO: Pathologic Complete Response Does Predict Outcome for Early Stage Breast Cancer Patients
 PRO: Pathologic Complete Response Does Predict Outcome for Early Stage Breast Cancer Patients Amelia B. Zelnak, M.D., M.Sc. Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute
PRO: Pathologic Complete Response Does Predict Outcome for Early Stage Breast Cancer Patients Amelia B. Zelnak, M.D., M.Sc. Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute
Updates From San Antonio Breast Cancer Symposium 2017
 Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER. Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx
 OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
Systemic Therapy Considerations in Inflammatory Breast Cancer
 Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
A vision for HER2 future
 School of Medical Oncology Department of Medical and Biological Sciences - University of Udine Department of Oncology - University Hospital of Udine A vision for HER2 future Current therapeutic algorithm
School of Medical Oncology Department of Medical and Biological Sciences - University of Udine Department of Oncology - University Hospital of Udine A vision for HER2 future Current therapeutic algorithm
Non-Anthracycline Adjuvant Therapy: When to Use?
 Northwestern University Feinberg School of Medicine Non-Anthracycline Adjuvant Therapy: When to Use? William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for
Northwestern University Feinberg School of Medicine Non-Anthracycline Adjuvant Therapy: When to Use? William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for
Update on New Perspectives in Endocrine-Sensitive Breast Cancer. James R. Waisman, MD
 Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012
 Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Metastatic Breast Cancer What is new? Subtypes and variation?
 Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
Breast : ASCO Abstracts for Review
 Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Novel Preoperative Therapies for HER2-Positive Breast Cancer. Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center
 Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Overview of nab-paclitaxel in Breast Cancer
 Overview of nab-paclitaxel in Breast Cancer William J. Gradishar MD FASCO FACP Betsy Bramsen Professor of Breast Oncology Robert H. Lurie Comprehensive Cancer Center Northwestern University Feinberg School
Overview of nab-paclitaxel in Breast Cancer William J. Gradishar MD FASCO FACP Betsy Bramsen Professor of Breast Oncology Robert H. Lurie Comprehensive Cancer Center Northwestern University Feinberg School
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice
 Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Treatment of Metastatic Breast Cancer. Prof RCCoombes Imperial College London
 Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Breast Cancer: ASCO Poster Review
 Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
10/15/2012. Inflammatory Breast Cancer vs. LABC: Different Biology yet Subtypes Exist
 Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Systemic therapy: HER-2 update. Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven
 Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Systemic therapy: HER-2 update Hans Wildiers Multidisciplinair Borst Centrum/Algemene medische oncologie UZ Leuven New drugs Strategic issues Specific anti-her2 drugs Lapa$nib /Nera$nib Baselga & Swain,
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Post-ESMO 2012: Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich T.Rordorf, SAMO Luzern 1
 Post-ESMO 2012: Breast Cancer Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich 1 Neoadjuvant treatment (in Her-2 positive disease) neoadjuvant trials abstracts: breast sparing surgery, biomarkers,
Post-ESMO 2012: Breast Cancer Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich 1 Neoadjuvant treatment (in Her-2 positive disease) neoadjuvant trials abstracts: breast sparing surgery, biomarkers,
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones
 ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?
 as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?") 1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
BREAST CANCER SLIDE DECK 2017 Selected abstracts from:
 BREAST CANCER SLIDE DECK 2017 Selected abstracts from: 2017 ASCO ANNUAL MEETING 2 6 June 2017 Chicago, USA Supported by Eli Lilly and Company. Eli Lilly and Company has not influenced the content of this
BREAST CANCER SLIDE DECK 2017 Selected abstracts from: 2017 ASCO ANNUAL MEETING 2 6 June 2017 Chicago, USA Supported by Eli Lilly and Company. Eli Lilly and Company has not influenced the content of this
Chemotherapy With or Without Targeted Drugs* in Metastatic Breast Cancer
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Chemotherapy With or Without Targeted Drugs* in Metastatic Breast Cancer * Substances without published evidence based on at
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Chemotherapy With or Without Targeted Drugs* in Metastatic Breast Cancer * Substances without published evidence based on at
Emerging Approaches for (Neo)Adjuvant Therapy for ER+ Breast Cancer
Adjuvant Therapy for ER+ Breast Cancer") Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
BREAST CANCER RISK REDUCTION (PREVENTION)
") BREAST CANCER RISK REDUCTION (PREVENTION) Articles Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled
BREAST CANCER RISK REDUCTION (PREVENTION) Articles Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled
When is Chemotherapy indicated in Advanced Luminal Breast Cancer?
 When is Chemotherapy indicated in Advanced Luminal Breast Cancer? Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology Clinical Care National University Cancer Institute, Singapore
When is Chemotherapy indicated in Advanced Luminal Breast Cancer? Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology Clinical Care National University Cancer Institute, Singapore
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Dilemmas in Adjuvant Chemotherapy Is adjuvant chemotherapy effective in ER+
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Dilemmas in Adjuvant Chemotherapy Is adjuvant chemotherapy effective in ER+
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer
 The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA
 Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Considerations in Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Metronomic chemotherapy for breast cancer
 Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
4, :00 PM 9:00 PM
 Consensus or Controversy? Clinical Investigators Provide Their Perspectives on Practical Issues and Research Questions in the Management of Breast Cancer Robert W Carlson, MD John Crown, MD Charles E Geyer
Consensus or Controversy? Clinical Investigators Provide Their Perspectives on Practical Issues and Research Questions in the Management of Breast Cancer Robert W Carlson, MD John Crown, MD Charles E Geyer
Mechanisms of hormone drug resistance
 Mechanisms of hormone drug resistance Ljiljana Stamatović Institute for Oncology and Radiology of Serbia Tenth UMOS Conference, Belgrade, 16-17 th May 2015. Hormone receptor-positive breast cancer (HR+
Mechanisms of hormone drug resistance Ljiljana Stamatović Institute for Oncology and Radiology of Serbia Tenth UMOS Conference, Belgrade, 16-17 th May 2015. Hormone receptor-positive breast cancer (HR+
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Page. Objectives: Hormone Therapy Resistance: Challenges and Opportunities. Research Support From Merck
 Hormone Therapy Resistance: Challenges and Opportunities Pamela. N. Munster, MD University of California, San Francisco Financial Disclosures Research Support From Merck Objectives: Understanding the current
Hormone Therapy Resistance: Challenges and Opportunities Pamela. N. Munster, MD University of California, San Francisco Financial Disclosures Research Support From Merck Objectives: Understanding the current
SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER
 SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER Sunil Shrestha 1*, Ji Yuan Yang, Li Shuang and Deepika Dhakal Clinical School of Medicine, Yangtze University, Jingzhou, Hubei Province, PR. China Department
SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER Sunil Shrestha 1*, Ji Yuan Yang, Li Shuang and Deepika Dhakal Clinical School of Medicine, Yangtze University, Jingzhou, Hubei Province, PR. China Department
Nadia Harbeck Breast Center University of Cologne, Germany
 Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
Advanced HER2+ Breast Cancer: New Options and How to Deploy Them. José Baselga MD, PhD
 Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和
 資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
Systemic Therapy of HER2-positive Breast Cancer
 Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
Highlights in breast cancer
 CONGRESS HIGHLIGHTS SPECIAL EDITION 309 Highlights in breast cancer W. Lybaert, MD In this article, the most important new studies presented at ESMO 2017 in Madrid in early (EBC) and metastatic breast
CONGRESS HIGHLIGHTS SPECIAL EDITION 309 Highlights in breast cancer W. Lybaert, MD In this article, the most important new studies presented at ESMO 2017 in Madrid in early (EBC) and metastatic breast
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid
 Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Treatment of Early-Stage HER2+ Breast Cancer
 Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Adjuvant Systemic Therapy in Early Stage Breast Cancer
 Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND!
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
Current Optimal Sequence and Duration of Endocrine Treatment
 [Symposium 7] Present and Future of Endocrine Therapy 07 Apr, 2018@GBCC Current Optimal Sequence and Duration of Endocrine Treatment Breast Oncology Center The Cancer Institute Hospital of JFCR Shinji
[Symposium 7] Present and Future of Endocrine Therapy 07 Apr, 2018@GBCC Current Optimal Sequence and Duration of Endocrine Treatment Breast Oncology Center The Cancer Institute Hospital of JFCR Shinji
ASCO and San Antonio Updates
 ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
Breast Cancer Immunotherapy. Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy
 Breast Cancer Immunotherapy Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy Conflict of Interest I have the following financial relationships to disclose:
Breast Cancer Immunotherapy Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy Conflict of Interest I have the following financial relationships to disclose:
UK Interdisciplinary Breast Cancer Symposium. Should lobular phenotype be considered when deciding treatment? Michael J Kerin
 UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
Adjuvant chemotherapy in older breast cancer patients: how to decide?
 Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY. Dr. Carlos Garbino
 EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
FoROMe Lausanne 6 février Anita Wolfer MD-PhD Cheffe de clinique Département d Oncologie, CHUV
 FoROMe Lausanne 6 février 2014 Anita Wolfer MD-PhD Cheffe de clinique Département d Oncologie, CHUV Epithelial Ovarian Cancer (EOC) Epidemiology Fifth most common cancer in women and forth most common
FoROMe Lausanne 6 février 2014 Anita Wolfer MD-PhD Cheffe de clinique Département d Oncologie, CHUV Epithelial Ovarian Cancer (EOC) Epidemiology Fifth most common cancer in women and forth most common
COME HOME Innovative Oncology Business Solutions, Inc.
 Innovative Oncology Business Solutions, Inc. Breast Cancer Diagnostic/Therapeutic Pathway V11, April 2015 Required Structured Data Fields: ICD9 Code Stage Staging Components Performance Status Treatment
Innovative Oncology Business Solutions, Inc. Breast Cancer Diagnostic/Therapeutic Pathway V11, April 2015 Required Structured Data Fields: ICD9 Code Stage Staging Components Performance Status Treatment