Surgical Issues in Melanoma
|
|
|
- James Jackson
- 5 years ago
- Views:
Transcription



1 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute
2 Surgical Issues Margins How narrow? Sentinel Lymph Node Biopsy Who Why Completion Lymph Node Dissection Why? Why not? Metastatic Disease (Stage IV) Where does surgery fit?
3 Margin Recommendations:pre-1970* 2 cm Cooling (1966) 5 cm Hadley (1907) Raven (1953) Petersen (1962) Olsen (1966) 8 cm Pack (1953) As wide as possible - Veronesi (1966) 15 cm Petersen (1962) * Wong CK, Dermatologica 141: 215, 1970
4 Randomized Trials: <2 mm French Cooperative Group (n=326) DFS < 2 mm 2 cm Swedish Melanoma Trial Group (n=989) 5 cm 1cm 3 cm WHO #10 (n= 712) 8 vs. 3 local recurrences (NS) Khayat et al, Cancer, 2003 Apr; 97(8): Cohn-Cedermark, Cancer, 2000; 89: 1495 Veronesi U, Arch Surg, 1991 Apr; 126(4):
5 Randomized Trials: Intergroup n=468 Median follow up >10 years 1-4 mm 2 cm 4 cm No difference in local recurrence 2.6% (4cm) vs. 2.1% (2cm) Skin grafts 46% (4cm) vs. 11% (2cm) Risk of LR based on primary tumor

6 Randomized Trials: UK Trial Sweden n=900 n = 936 pts 1cm 3 cm 2 cm 4 cm > 2 mm Thomas et al. NEJM 2004 Gillgren et al, Lancet, November 2011
7 Answer Key: Current (NCCN) Recommendations Melanoma-in-situ Breslow <1mm Breslow mm Breslow mm Breslow >4mm 5 mm 1 cm 1-2 cm 2 cm 2 cm
8 Clinical vs. Pathological Margins
9 Lymph Node Treatment
10 Lymph Node Treatment

11 Regional Lymph Nodes
12 Elective Lymph Node Dissection: WHO #14 All (>1.5mm) mm >4.0mm
13 Intergroup ELND: Overall Survival Balch, Ann Surg Oncol, 2000
14 Sentinel Node
15 Problem: Identification of patients 80% of patients undergoing ELND had negative nodes Others have concomitant systemic spread not cured by ELND Only a subset can benefit from nodal surgery
16
17 MSLT-I Melanoma >1 mm or > Clark IV (primary analysis mm) Randomization Wide excision alone 40% 60% Wide excision + SLN SLN + SLN - CLND for Recurrence Immediate CLND No recurrence: observation Observation


18 MSLT-I prognosis
 Thick ( 3.")
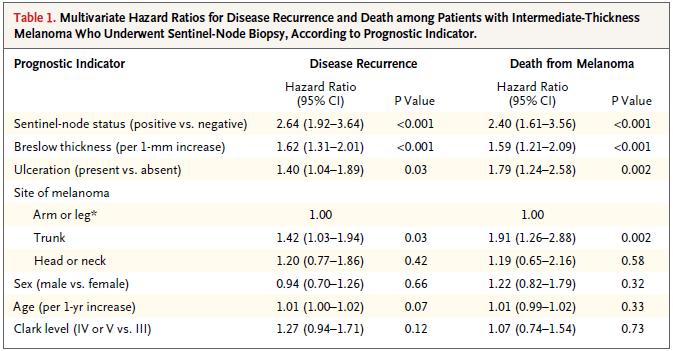
19 SLN Biopsy and Disease-Free Survival: MSLT-I Intermediate Thickness ( mm) Thick ( 3.5mm)

20 Delayed treatment metastatic spread within the regional nodal basin ± 0.5 Mean # Pos. Nodes ± 0.1 SNB Watch & Wait 0 Immediate CLND Delayed CLND

21 Impact of Clinical Recurrence: Morbidity MSLT 1
 Final Dataset Survival (%) 100 75 50 25 0 0 HR: 0.84 P=0.18, 95% CI (0.")

22 Overall Melanoma Related Survival (Breslow mm) Final Dataset Survival (%) HR: 0.84 P=0.18, 95% CI ( ) Group OBS SNB # Event / Total N 97 / / 770 Estimate S(t) ± SE 5-year 10-year 85.7 ± 1.6 % 78.3 ± 2.0% 86.6 ± 1.3 % 81.4 ± 1.5 % Time (years) OBS SNB
23 MSLT-I Melanoma >1 mm or > Clark IV (primary analysis mm) Randomization DSS: Primary Endpoint DFS: Secondary Endpoint Wide excision alone 40% 60% Wide excision + SLN SLN + SLN - Occult Stage III CLND for Recurrence Immediate CLND No recurrence: observation Observation
 Final Dataset 100 Group # Event / Estimate S(t) ± SE % Total N 5-year 10-year OBS, had nodal recur. 48/87 57.5 ± 5.4 41.5 ± 5.6 SNB+ 70 / 193 69.8 ± 4.4 62.1 ± 4.")
24 Morton A 50 Year Odyssey Melanoma Specific Survival Node+ ( mm) Final Dataset 100 Group # Event / Estimate S(t) ± SE % Total N 5-year 10-year OBS, had nodal recur. 48/ ± ± 5.6 SNB+ 70 / ± ± 4.8 Survival (%) HR: % C.I. (0.37, 0.84) Log Rank P=0.006 OBS SNB Time (years)

25 Latent Subgroup Analysis
26 Morton A 50 Year Odyssey Melanoma Specific Survival Node+ ( mm) Final Dataset 100 Group # Event / Estimate S(t) ± SE % Total N 5-year 10-year OBS, had nodal recur. 48/ ± ± 5.6 SNB+ 70 / ± ± 4.8 Survival (%) HR: % C.I. (0.37, 0.84) Log Rank P=0.006 OBS SNB Time (years)

27 Selection for SLN: Thick Melanoma? Overall Survival
28 Melanoma-specific Survival Thin Melanoma?

29 Node-Positive Thin Melanoma: Outcomes

30 Thin Melanoma SLN predictors Problems: SLN population is selected SLN has false negatives SLN has shorter follow up Use clinical nodal recurrence instead

31 Predictors Breslow Clark Ulceration I II III IV V UNK 0.0 Yes No Unknown Gender Primary Site Age Female Male 0.0 Extremity Head/neck Trunk 0.0 < >=70
32 Predicted probabilities of Nodal Recurrence > <50 Female Male < Concordance index = 0.79 Breslow Age Sex Predicted % node recurrence <0.5 >70 female 0.1 <0.5 >70 male 0.4 < female 0.3 < male 0.9 <0.5 <50 female 0.6 <0.5 <50 male >70 female >70 male female male <50 female <50 male >70 female >70 male female male <50 female <50 male 17.4
33 CLND: Rationale and Data
 Stain CLND(+) n (%) 187")
34 MSLT2: Is CLND necessary in SN(+) LN basins? 79-88% of patients have Negative NSN nodes in CLND specimen MSLT-I JWCI Cochran # SN(+) Stain CLND(+) n (%) H&E H&E IHC 22 (11.8%) 39 (12.1%) 19 (21.1%) NSN(-) % 88% 88% 79%
35 Equipoise: Advantages Potential removal of more cancer (10-20%) Complete Staging Information Clinical trial eligibility? Disadvantages Additional surgery Larger incision JP drain Potential complications: Lymphedema Disease may already be systemic Ultrasound may pick up any recurrence at an early time point
36 Is CLND necessary in SN(+) LN basins? RFS MSS Multivariable: HR 1.51, p=0.09
37 JWCI Retro Data


38 DeCOG Trial Randomized 1:1 to CLND or observation Powered to detect 10% absolute survival difference with 80% power No Head/Neck Melanomas Median Breslow 2.4 mm About 2/3 of patients SLN disease <1 mm
39
40 DeCOG Trial: Discussion/Conclusions Better nodal recurrence rate (14.6 vs 8.3%) Not better MSS Based on our findings, complete lymphadenectomy cannot be recommended in melanoma patients with micrometastases. Difficult recruitment - High refusal/dropout Did not achieve target accrual -Decreased statistical power Follow up <3 years
41 MSLT-II and MILND
42 MSLT II: Trial Design Melanoma >1.2 mm or > Clark IV, n=3500 LM/SL: standard and molecular assessment Melanoma: + SLN (Outside Center) n= Observation Randomization n=1926 Stratification: MSLT1 Center Breslow Ulceration SLN H&E vs. PCR Immediate CLND Nodal Ultrasound Recur No Recur Observation Delayed CLND Observation
43 64
44 Accrual: Complete All North Am Europe Australia Target

45 MSLT-II Possible Outcomes Morton SSO PI 5Mar11 45
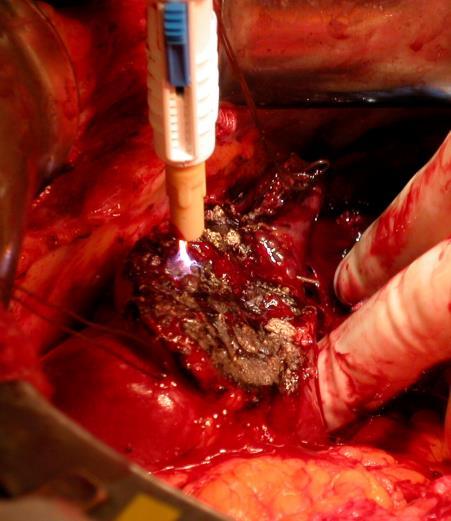
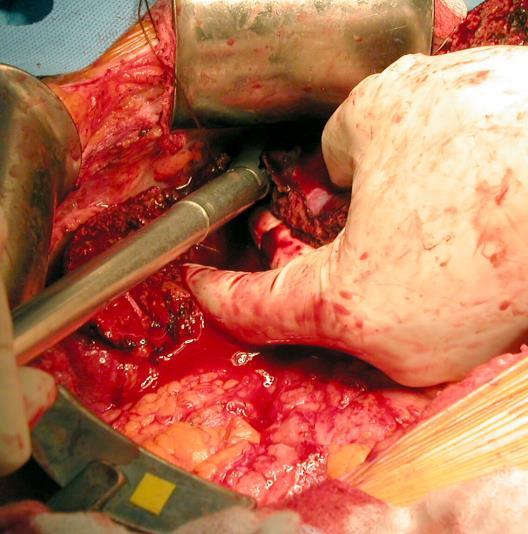
46 Minimally Invasive: MILND
47 Minimally Invasive: MILND
48 Minimally Invasive: MILND

49 Minimally Invasive: MILND

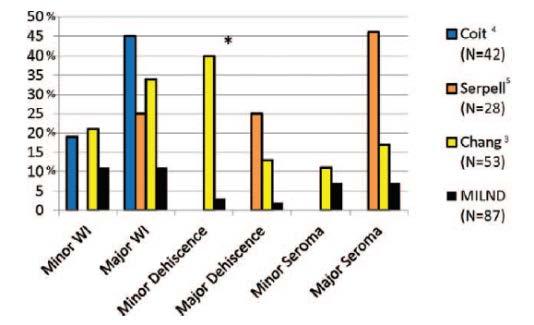
50 Minimally Invasive: MILND
51 Distant Metastases


52 Surgery for Metastatic Melanoma: Heresy? It s too late for surgery, a local therapy Surgery is morbid and complicated Risk/Benefit Ratio very high
53 Meta-analysis of Phase 2 Trials Korn et et al. J Clin Oncol. Feb Feb ,




54 Better Staging 2008 CT scanning Circa
55


56 Vaccines: CancerVax AJCC Stage IV Melanoma Resection of Metastatic Lesions Stratification Factors Site of metastasis: M1a: soft-tissue & nodal mets M1b: visceral mets # individual lesions: 1, 2-3, 4-5 Randomize N=496 BCG + Canvax. BCG + Placebo
 Survival at 5 years Canvaxin TM Placebo 32 39 40% 45% BCG + Placebo n=250 BCG + Canvaxin TM n=246 0.0 HR=1.18 P=0.")
57 MMAIT-IV Overall Survival (Intent To Treat) Overall Survival Median Survival (months) Survival at 5 years Canvaxin TM Placebo % 45% BCG + Placebo n=250 BCG + Canvaxin TM n= HR=1.18 P=0.245 BCG/Pl BCG/Cv Time (months)
58 Morton ACS Stage IV Metastasis Location Soft Tissue Visceral 100 Placebo Median Survival (months) 60 Survival at 5 years 52% Canvaxin 36 43% 100 Placebo Median Survival (Months) 32 Survival at 5 years 39% Canvaxin 29 36% % Survival BCG + Placebo n=108 BCG + Canvaxin TM n=107 % Survival BCG + Placebo n=138 BCG + Canvaxin TM n= HR=1.37 P= HR=1.06 P= Time (months) Time (months)




59 JWCI Metastasectomy Series Lung Small Bowel Adrenal Surgery No Surgery Median OS 29.2 months Tafra, J Thorac CV Surg, 1995 Liver P< Ollila, Arch Surg 1996 Solid Organ Median OS 9.4 months p <.001 Flaherty, Am Surg, 2015 Overall Survival Surgical, n=58 Non-surgical, n=1020 Months Faries, J Am Coll Surg, 2014 Wood, Ann Surg Oncol, 2001
60 Trial Patient Outcomes Over the Years Ipi/PD-1 combo BRAF/MEK combo SWOG PD-1 vemurafenib JWCI Vax Phase 2 MMAIT Vax (Surgery) Ipi + DITC Ipi +/- gp Korn et al. J Clin Oncol. Feb ,
61 Selection! Selection! Selection! Surgery is not appropriate for all patients. True predictive factors are not available Factors for post-resection prognosis are available (TVDT, DFI, Prior Stage III) prognostic predictive




62 Selection Factors Number of Metastases 1 Met: HR=0.537, p= Mets (reference) 2-3 Mets: HR=0.591, p=0.0664
63 Not competition, but collaboration Neoadjuvant trials Biomarker development Adjuvant Surgery Consolidation Selective resection
64 Metastasectomy: Consolidation Liver Stabilization on Prior Therapy P< Melanoma-Specific Survival Overall Survival Surgical, n=58 Non-surgical, n=1020 Months Faries, J Am Coll Surg, 2014 Yes, n=20 No, n=33 p=0.01 Months Faries, et al, JACS, 2014
 41.9 9.4 Overall Survival (p value) 0.")
65 Metastasectomy: Selective Resection Adrenal Surgery No Surgery Curative Surgery Non-Curative Surgery No Surgery Median OS 29.2 months Median OS 9.4 months p <.001 Flaherty, Am Surg, = Censored Treatment Approach Curative Surgery No Surgery Median Survival (mos.) Overall Survival (p value) Flaherty et al, Am Surg, 2014 Non-Curative Surgery No Surgery
66 Ipilimumab with resection 5 year MSS Med. MSS (months) p-value Ipi after Resection 61% (CI 21-62%) Ipi before Resection 42% (CI 30-82%) 47 p=0.37
67 Resection following Ipilimumab: Resection for: n 5 year MSS Isolated Persistent Disease 7 69% (CI 21-91%) Symptomatic 7 53% (CI 17-79%) Progressive 10 14%(0.7-47%)
68 Unresectable
69 Percutaneous Hepatic Perfusion


70

71 Thank you
Nodal Treatment in Melanoma: Snow to MSLT-II
 Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director,
Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director,
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Controversies and Questions in the Surgical Treatment of Melanoma
 Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma
 No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective
 Procedure: An Oncologic Surgeon s Perspective") Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC
 Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018 AJCC
Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018 AJCC
Molecular Enhancement of Sentinel Node Evaluation
 Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy
 Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Rebecca Vogel, PGY-4 March 5, 2012
 Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
Melanoma Surgery Update James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division
 Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Surgical Treatment of Melanoma Across the Disease Spectrum:
 AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
NEW SURGICAL APPROACHES TO MELANOMA THERAPY
 NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
Surgical Oncology Perspective of Melanoma
 Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
Who is the Ideal Candidate for PEG Intron?
 Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
M D..,., M. M P.. P H., H, F. F A.. A C..S..
 Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
Surgery for Melanoma and What s on the Horizon
 and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Adjuvant Therapy of High Risk Melanoma
 Adjuvant Therapy of High Risk Melanoma William Sharfman, MD, FACP Associate Professor of Oncology and Dermatology Johns Hopkins University School of Medicine July 5, 2012 Adjuvant options for Stage IIB/C
Adjuvant Therapy of High Risk Melanoma William Sharfman, MD, FACP Associate Professor of Oncology and Dermatology Johns Hopkins University School of Medicine July 5, 2012 Adjuvant options for Stage IIB/C
Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients
 2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma
 Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature. Sasha Jenkins
 Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Melanoma 10/12/18 Justin J. Baker, M.D.
 Objectives Review Incidence Risk Factors for Development Detection 10/12/18 Justin J. Baker, M.D. Treatment of Surgery Medicine Radiation What is Incidence Cancer of Melanocytes Melanocytes are normal
Objectives Review Incidence Risk Factors for Development Detection 10/12/18 Justin J. Baker, M.D. Treatment of Surgery Medicine Radiation What is Incidence Cancer of Melanocytes Melanocytes are normal
Precision Surgery for Melanoma
 Precision Surgery for Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background 87,110 cases of melanoma estimated in
Precision Surgery for Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background 87,110 cases of melanoma estimated in
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Should we still be performing IHC on all sentinel nodes?
 Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Disclosures. SLNB for Melanoma 25/02/2014 SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION
 8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know
 Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Update on Lymph Node Management in Melanoma
 Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
Metastasectomy for Melanoma What s the Evidence and When Do We Stop?
 Metastasectomy for Melanoma What s the Evidence and When Do We Stop? Vernon K. Sondak, M D Chair, Moffitt Cancer Center Tampa, Florida Focus on Melanoma London, UK October 15, 2013 Disclosures Dr. Sondak
Metastasectomy for Melanoma What s the Evidence and When Do We Stop? Vernon K. Sondak, M D Chair, Moffitt Cancer Center Tampa, Florida Focus on Melanoma London, UK October 15, 2013 Disclosures Dr. Sondak
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA
 ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
ORIGINAL ARTICLE. Clinical Node-Negative Thick Melanoma
 ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
Sentinel Lymph Node Biopsy Is Valuable For All Cancer. Surgery Grand Rounds Debate October 6, 2008 Joel Baumgartner
 Sentinel Lymph Node Biopsy Is Valuable For All Cancer Surgery Grand Rounds Debate October 6, 2008 Joel Baumgartner History Lymphatics first described by Rasmus Bartholin in 1653 Rudolf Virchow postulated
Sentinel Lymph Node Biopsy Is Valuable For All Cancer Surgery Grand Rounds Debate October 6, 2008 Joel Baumgartner History Lymphatics first described by Rasmus Bartholin in 1653 Rudolf Virchow postulated
MELANOMA: THE BEST OF THE YEAR Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone
 MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
Talk to Your Doctor. Fact Sheet
 Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Protocol. This trial protocol has been provided by the authors to give readers additional information about their work.
 Protocol This trial protocol has been provided by the authors to give readers additional information about their work. Protocol for: Faries MB, Thompson JF, Cochran AJ, et al. Completion dissection or
Protocol This trial protocol has been provided by the authors to give readers additional information about their work. Protocol for: Faries MB, Thompson JF, Cochran AJ, et al. Completion dissection or
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Management of the patient with Lymph Node Involvement. Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne
 Management of the patient with Lymph Node Involvement Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne Lymph Node Field Recurrence Most important prognostic factor for early stage melanoma
Management of the patient with Lymph Node Involvement Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne Lymph Node Field Recurrence Most important prognostic factor for early stage melanoma
Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011
 Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011 Most common form of cancer in adults ages 25-29 3-5% of skin cancers but 65-75% of deaths Most common metastasis to small
Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011 Most common form of cancer in adults ages 25-29 3-5% of skin cancers but 65-75% of deaths Most common metastasis to small
VATS Metastasectomy. Inderpal (Netu) S. Sarkaria, MD, FACS
 S. Sarkaria, MD, FACS") VATS Metastasectomy Inderpal (Netu) S. Sarkaria, MD, FACS Vice Chairman, Clinical Affairs Director, Robotic Thoracic Surgery Co-Director, Esophageal and Lung Surgery Institute Disclosures Speaking & Education:
VATS Metastasectomy Inderpal (Netu) S. Sarkaria, MD, FACS Vice Chairman, Clinical Affairs Director, Robotic Thoracic Surgery Co-Director, Esophageal and Lung Surgery Institute Disclosures Speaking & Education:
Sentinel Lymph Node Biopsy: Past and Present Implications for the Management of Cutaneous Melanoma with Nodal Metastasis
 American Journal of Clinical Dermatology (2018) 19 (Suppl 1):S24 S30 https://doi.org/10.1007/s40257-018-0379-0 REVIEW ARTICLE Sentinel Lymph Node Biopsy: Past and Present Implications for the Management
American Journal of Clinical Dermatology (2018) 19 (Suppl 1):S24 S30 https://doi.org/10.1007/s40257-018-0379-0 REVIEW ARTICLE Sentinel Lymph Node Biopsy: Past and Present Implications for the Management
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Radionuclide detection of sentinel lymph node
 Radionuclide detection of sentinel lymph node Sophia I. Koukouraki Assoc. Professor Department of Nuclear Medicine Medicine School, University of Crete 1 BACKGROUND The prognosis of malignant disease is
Radionuclide detection of sentinel lymph node Sophia I. Koukouraki Assoc. Professor Department of Nuclear Medicine Medicine School, University of Crete 1 BACKGROUND The prognosis of malignant disease is
Clinical Case Conference Melanoma
 Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
SENTINEL LYMPH node (SLN) biopsy has become
 biopsy has become") COMMENTARY Sentinel Lymph Node Biopsy for Melanoma: Controversy Despite Widespread Agreement By Kelly M. McMasters, Douglas S. Reintgen, Merrick I. Ross, Jeffrey E. Gershenwald, Michael J. Edwards, Arthur
COMMENTARY Sentinel Lymph Node Biopsy for Melanoma: Controversy Despite Widespread Agreement By Kelly M. McMasters, Douglas S. Reintgen, Merrick I. Ross, Jeffrey E. Gershenwald, Michael J. Edwards, Arthur
Clinical utilities and biological characteristics of melanoma sentinel lymph nodes
 W J C O World Journal of Clinical Oncology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5306/wjco.v7.i2.174 World J Clin Oncol 2016 April
W J C O World Journal of Clinical Oncology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5306/wjco.v7.i2.174 World J Clin Oncol 2016 April
NIH Public Access Author Manuscript J Surg Oncol. Author manuscript; available in PMC 2012 August 1.
 NIH Public Access Author Manuscript Published in final edited form as: J Surg Oncol. 2011 August 1; 104(2): 111 115. doi:10.1002/jso.21903. Does metastasectomy improve survival in patients with Stage IV
NIH Public Access Author Manuscript Published in final edited form as: J Surg Oncol. 2011 August 1; 104(2): 111 115. doi:10.1002/jso.21903. Does metastasectomy improve survival in patients with Stage IV
When Do I Consider Myself Cured?
 The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact
 Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Lymphadenectomy in RCC: Yes, No, Clinical Trial?
 Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis
 Ann Surg Oncol DOI 10.1245/s10434-016-5646-9 ORIGINAL ARTICLE MELANOMAS Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis Giorgos
Ann Surg Oncol DOI 10.1245/s10434-016-5646-9 ORIGINAL ARTICLE MELANOMAS Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis Giorgos
Stage IV Melanoma: Completely Resectable Patients are Scarce
 Ann Surg Oncol DOI 10.1245/s10434-013-2881-1 ORIGINAL ARTICLE MELANOMAS Stage IV Melanoma: Completely Resectable Patients are Scarce K. P. Wevers, MD and H. J. Hoekstra, MD, PhD Division of Surgical Oncology,
Ann Surg Oncol DOI 10.1245/s10434-013-2881-1 ORIGINAL ARTICLE MELANOMAS Stage IV Melanoma: Completely Resectable Patients are Scarce K. P. Wevers, MD and H. J. Hoekstra, MD, PhD Division of Surgical Oncology,
Printed by Martina Huckova on 10/3/2011 3:04:54 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer
 - Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
- Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice. Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin
 1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression
 Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
University of Groningen
 University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
This is a repository copy of Long term follow up of survival in a randomised trial of wide or narrow excision margins in high risk primary melanoma..
 This is a repository copy of Long term follow up of survival in a randomised trial of wide or narrow excision margins in high risk primary melanoma.. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/93871/
This is a repository copy of Long term follow up of survival in a randomised trial of wide or narrow excision margins in high risk primary melanoma.. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/93871/
Dr Rosalie Stephens. Mr Richard Martin. Medical Oncologist Auckland City Hospital Auckland
 Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Is There a Benefit to Sentinel Lymph Node Biopsy in Patients With T4 Melanoma?
 Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
1
 www.clinicaloncology.com.ua 1 Prognostic factors of appearing micrometastases in sentinel lymph nodes in skin melanoma M.N.Kukushkina, S.I.Korovin, O.I.Solodyannikova, G.G.Sukach, A.Yu.Palivets, A.N.Potorocha,
www.clinicaloncology.com.ua 1 Prognostic factors of appearing micrometastases in sentinel lymph nodes in skin melanoma M.N.Kukushkina, S.I.Korovin, O.I.Solodyannikova, G.G.Sukach, A.Yu.Palivets, A.N.Potorocha,
PAPER. Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma
 PAPER Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma Charles R. Scoggins, MD, MBA; Adrianne L. Bowen, MD; Robert C. Martin II, MD, PhD; Michael J. Edwards, MD; Douglas
PAPER Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma Charles R. Scoggins, MD, MBA; Adrianne L. Bowen, MD; Robert C. Martin II, MD, PhD; Michael J. Edwards, MD; Douglas
Melanoma. Tawnya L. Bowles, MD Surgical Oncologist, Medical Director for Melanoma Services; Intermountain Medical Center
 Melanoma Tawnya L. Bowles, MD Surgical Oncologist, Medical Director for Melanoma Services; Intermountain Medical Center Ken Grossmann, MD, PhD Assistant Professor, Department of Medicine, Oncology Division;
Melanoma Tawnya L. Bowles, MD Surgical Oncologist, Medical Director for Melanoma Services; Intermountain Medical Center Ken Grossmann, MD, PhD Assistant Professor, Department of Medicine, Oncology Division;
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
Principles of breast radiation therapy
 ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer. Cheol Min Kang 2018/04/05
 Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin. Suraj Venna
 AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Sentinel Lymph Node Biopsy for Breast Cancer
 Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Sentinel Node Biopsy. Is There Any Role for Axillary Dissection? JCCNB Nov 20, Stephen B. Edge, MD
 Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Sentinel Lymph Node Biopsy in Other Tumours: Sentinel Lymph Node Biopsy in Other Tumours. Methodology. Results. Key Questions to Consider
 Sentinel Lymph Node Biopsy in Other Tumours Dr. Rona Cheifetz Surgical Oncology Update November 24, 2006 Sentinel Lymph Node Biopsy in Other Tumours: An Operation Looking for an Application Dr. Rona Cheifetz
Sentinel Lymph Node Biopsy in Other Tumours Dr. Rona Cheifetz Surgical Oncology Update November 24, 2006 Sentinel Lymph Node Biopsy in Other Tumours: An Operation Looking for an Application Dr. Rona Cheifetz
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation
 Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
After primary tumor treatment, 30% of patients with malignant
 ESTS METASTASECTOMY SUPPLEMENT Alberto Oliaro, MD, Pier L. Filosso, MD, Maria C. Bruna, MD, Claudio Mossetti, MD, and Enrico Ruffini, MD Abstract: After primary tumor treatment, 30% of patients with malignant
ESTS METASTASECTOMY SUPPLEMENT Alberto Oliaro, MD, Pier L. Filosso, MD, Maria C. Bruna, MD, Claudio Mossetti, MD, and Enrico Ruffini, MD Abstract: After primary tumor treatment, 30% of patients with malignant
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
ABSTRACT. Background Sentinel-node biopsy, a minimally invasive procedure for regional melanoma staging, was evaluated in a phase 3 trial.
 The new england journal of medicine established in 1812 february 13, 214 vol. 37 no. 7 Final Trial Report of Sentinel-Node Biopsy versus Nodal Observation in Melanoma D.L. Morton, J.F. Thompson, A.J. Cochran,
The new england journal of medicine established in 1812 february 13, 214 vol. 37 no. 7 Final Trial Report of Sentinel-Node Biopsy versus Nodal Observation in Melanoma D.L. Morton, J.F. Thompson, A.J. Cochran,
Sentinel Node in Malignant Melanoma The Pathologist s Point of View
 Sentinel Node in Malignant Melanoma The Pathologist s Point of View S.J. Diaz-Cano Department of Pathology, Barts and The London School of Medicine, University of London, Barts and The London NHS Trust,
Sentinel Node in Malignant Melanoma The Pathologist s Point of View S.J. Diaz-Cano Department of Pathology, Barts and The London School of Medicine, University of London, Barts and The London NHS Trust,
46. Merkel Cell Carcinoma
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Emerging Approaches for (Neo)Adjuvant Therapy for ER+ Breast Cancer
Adjuvant Therapy for ER+ Breast Cancer") Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
Note: Page numbers of article titles are in boldface type. A Ablative therapy, nonsurgical, for pulmonary metastases of soft tissue sarcoma, 279 280 Adipocytic tumors, atypical lipomatous tumor vs. well-differentiated
MELANOMA LETTER. Surgical Treatment of Primary Melanoma: Where Do We Stand After MSLT-II? THE. From the Editors MSLT-II. SkinCancer.
 THE MELANOMA LETTER A PUBLICATION OF THE SKIN CANCER FOUNDATION DEBORAH S. SARNOFF, MD, President WINTER 2017, Vol. 35 DAN LATORE, Executive Director Surgical Treatment of Primary Melanoma: Where Do We
THE MELANOMA LETTER A PUBLICATION OF THE SKIN CANCER FOUNDATION DEBORAH S. SARNOFF, MD, President WINTER 2017, Vol. 35 DAN LATORE, Executive Director Surgical Treatment of Primary Melanoma: Where Do We