The Role of the Medical Oncologist in the Treatment of Prostate Cancer. Alireza saadat hematologist and oncologist
|
|
|
- Eleanore McKinney
- 5 years ago
- Views:
Transcription
1 The Role of the Medical Oncologist in the Treatment of Prostate Cancer Alireza saadat hematologist and oncologist
2 When should you see an oncologist? High risk localized disease Rising PSA after local therapy Hormone sensitive disease Endocrine Resistant Disease
3 Natural History of Metastatic Prostate Cancer Castration Tumor Volume and Activity Secondary Hormonal Rx Chemo Rx Time
4 CASTRATE-SENSITIVE, NON- METASTATIC Rising PSA after primary therapy Biochemical recurrence Stage D0 If prostatectomy, consider XRT PSA doubling time predictor of risk for metastasis PSADT < 12 months Androgen ablation therapy standard of care Data supporting intermittent therapy Clinical trials
5 Side effects of ADT ADT is associated with a wide range of side effects that can significantly impair quality of life. Loss of lean body mass, increased body fat, and decreased muscle strength. Sexual dysfunction Loss of libido in men receiving GnRH agonists usually develops within the first several months and is followed by erectile dysfunction.
6 Side effects of ADT Loss of bone mineral density, which can result in bone fracture due to osteoporosis. This effect may be compounded by the presence of bone metastases. Vasomotor instability, which is manifested by hot flashes. Gynecomastia, decreased body hair, and smaller penile and/or testicular size. Fatigue or lack of energy. Behavioral and neurologic effects. Cardiovascular and metabolic abnormalities.
7 CASTRATE-SENSITIVE, METASTATIC Metastasis typically bone and nodes Wide variation in natural history Depends on extent of osseous mets Presence of visceral mets Grade of tumor PSADT Good risk Time to progression 3-5+ years Poor risk Time to progression 1-3 years Standard of care is AAT Evidence supporting intermittent AAT
8 CASTRATE-RESISTANT, NON- METASTATIC Defined as rising PSA on LHRH therapy Castrate testosterone level Negative scans No symptoms of disease Variable natural history Time to metastasis 1-3+ years PSADT helpful - < 9 months predicts mets within 2 years Treatment is second-line AAT Antiandrogens Ketoconazole/Zytiga
9 Castrate Resistant, Metastatic (Pre-Taxotere) Good prognosis (asymptomatic, low volume ) Standard Taxotere chemotherapy Antiandrogens, ketoconazole/zytiga Immunotherapy (Provenge, sipuleucel-t) Investigational therapies Poor prognosis (symptomatic, aggressive) Standard Taxotere chemotherapy Investigational chemotherapy combinations
10 CASTRATE-RESISTANT, METASTATIC (Post-Taxotere) Jevtana (Cabazitaxel) FDA approved Zytiga (Abiraterone) FDA approved MDV3100 Other emerging drugs
11 Abiraterone Androgens produced in the testis can cause autocrine/paracrine signaling that results in tumor progression Abiraterone is an orally administered small molecule that irreversibly inhibits the products of the CYP17 gene (including both 17,20-lyase and 17-alpha-hydroxylase). doing so, abiraterone blocks the synthesis of androgens in the tumor as well as in the testis and adrenal glands. Patients treated with abiraterone are at risk for adrenal insufficiency and require concurrent steroid replacement therapy.
12 Abiraterone abiraterone plus prednisone prolonged overall survival compared with prednisone alone in men who had previously been treated with docetaxel and in those who were chemotherapy naïve. Abiraterone is approved for patients who have metastatic castrate resistant prostate cancer. Abiraterone is generally well tolerated, although fluid retention, hypokalemia and hypertension may require treatment.
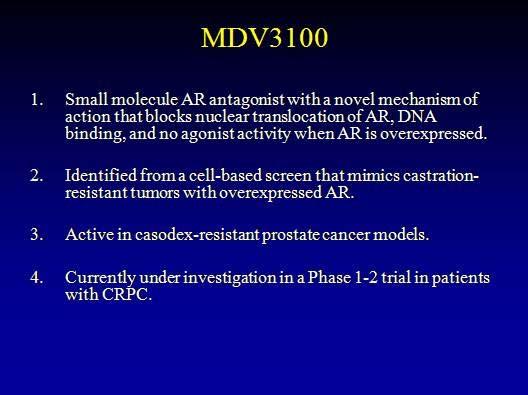
13 Enzalutamide Enzalutamide is an orally administered agent that acts at multiple sites in the androgen receptor signaling pathway, including blocking the binding of androgen to the androgen receptor, inhibition of nuclear translocation of the androgen receptor, and inhibition of the association of the androgen receptor with nuclear DNA. Unlike abiraterone, concurrent treatment with steroids is not required. In a phase III trial in men who had received prior docetaxel - based chemotherapy, enzalutamide significantly increased median survival compared with placebo.
14 Enzalutamide A second phase III trial is evaluating enzalutamide in chemotherapy naïve patients (NCT ). Treatment with enzalutamide has rarely been associated with seizures, and its use is contraindicated in patients with a seizure disorder. Enzalutamide is approved for men with metastatic, castration-resistant prostate cancer who have received treatment with docetaxel. There are no data on the efficacy of enzalutamide in men who have previously been treated with abiraterone.
15 Sipuleucel-T Sipuleucel-T is a dendritic cell vaccine that is prepared from peripheral blood mononuclear cells obtained by leukapheresis. These cells are exposed ex vivo to a novel recombinant protein immunogen, which consists of prostatic acid phosphatase (PAP) fused to human granulocyte macrophage colony-stimulating factor. These activated cells are then infused back into the patient approximately three days after the original harvesting. In randomized trials, sipuleucel-t prolonged overall survival compared with placebo in men with minimally symptomatic, metastatic prostate cancer.
16 Sipuleucel-T There are no data on the effectiveness of sipuleucel-t in men whose only evidence of disease is an elevated PSA or in those with symptomatic metastatic disease. Treatment is contraindicated in patients who are on steroids or opioids for cancer-related pain, and should be used with caution in patients with liver metastases. Although sipuleucel-t prolonged overall survival, it did not significantly increase progression-free survival or affect the serum PSA.











17 Docetaxel HRPC Trials TAX N=1006 Randomize Mitoxantrone 12 mg/m 2 Prednisone 10 mg q day Q 21 days up to 10 cycles Docetaxel 30 mg/m 2 /wk Prednisone 10 mg q day 5 on; 1 off x 6 cycles Docetaxel 75 mg/m 2 Prednisone 10 mg q day Q 21 days up to 10 cycles SWOG N=770 *Warfarin and aspirin Randomize Mitoxantrone 12 mg/m 2 Prednisone 5 mg bid Q 21 days Docetaxel 60 mg/m 2 d 2 Estramustine 280 mg d1-5* Dexamethasone 20 mg, tid d 1 & 2 1. Tannock et al. N Engl J Med 2004:351; Petrylak et al. N Engl J Med 2004;351:
18 Overall Survival 100% 80% D+E M+P # at Risk # of Deaths Median in Months % HR: 0.80 (95% CI 0.67, 0.97), p = % 20% 0% Months Petrylak et NEJM 2004
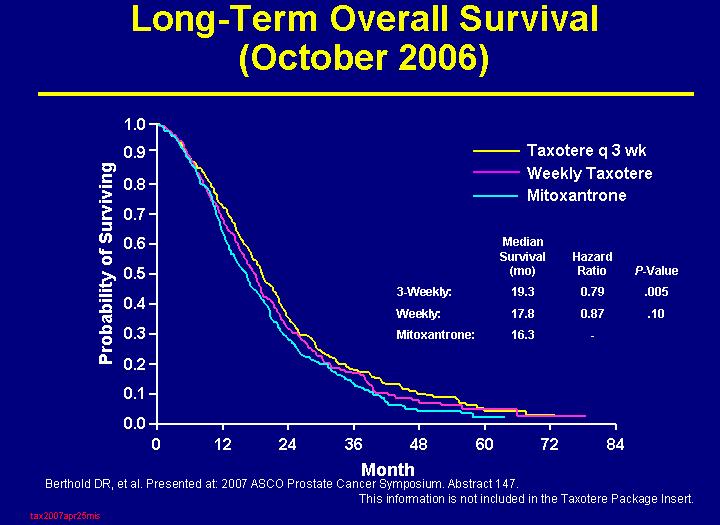
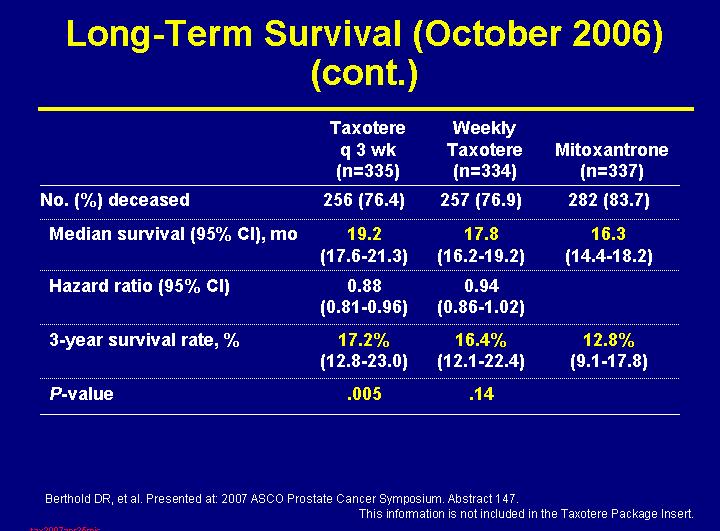
19 Overall Survival TAX 327 Probability of Surviving Median survival Hazard (mos) ratio P-value Combined: D 3 wkly: D wkly: Mitoxantrone 16.4 Docetaxel 3 wkly Docetaxel wkly Mitoxantrone Months Tannock et al. N Engl J Med 2004:351;
20
21
22 Evidence for Angiongenis as a Target for Prostate Cancersis Microvessel density correlates with prognosis in radical prostatetectomy specimens Elevated levels of VEGF correlate with prognosis in CRPCa bfgf expresse in epithelial and stromal cells
23 CALGB 9040: Randomized Double Blinded Placebo controlled Phase III Trial Comparing Docetaxel + Prednisone with or without Bevacizumab in men with HRPC Eligibility Metastatic PC T <50 ng/ml No prior chemo Adequate hem, renal & liver function Stratification Halabi nomogram RANDOMIZE Arm A Dexamethasone Docetaxel Prednisone Placebo* Arm B Dexamethasone Docetaxel Prednisone Bevacizumab* 8 mg po x 3 doses 75 mg/m 2 on d1 q21d 10 mg po daily IV on day 1 q 21 days 8 mg po x 3 doses 75 mg/m 2 on d1 q 21d 10 mg po daily 15 mg/kg IV on day 1q 21d N = 1020 patients CALGB, ECOG, NCIC
24 CALGB Study Primary endpoint of improvement in median survival from 19 in docetaxel arm to 23 months in docetaxel/bevizcuzimab arm not met Press Release Roche 2010
25 Structure of Thalidomide and the 2nd-Generation IMiDs




26 MAINSAIL TRIAL Screening Metastatic CRPC Chemo-naïve Disease Progression CRPC Patients N= 1,015 Randomize 1:1 Docetaxel/Prednisone + Lenalidomide Until Progression or Toxicity N ~ 500 Docetaxel/Prednisone + Placebo Until Progression or Toxicity N ~ 500 Follow-Up: For Survival For Other Treatments Up to five years
27 TROPIC: Phase III Registration Study 146 Sites in 26 Countries mcrpc patients who progressed during and after treatment with a docetaxel based regimen (N=755) Stratification factors ECOG PS (0, 1 vs. 2) Measurable vs. non measurable disease cabazitaxel 25 mg/m² q 3 wk + prednisone* for 10 cycles (n=378) *Oral prednisone/prednisolone: 10 mg daily. Primary endpoint: OS Secondary endpoints: Progression free survival (PFS), response rate, and safety mitoxantrone 12 mg/m² q 3 wk + prednisone* for 10 cycles (n=377) Inclusion: Patients with measurable disease must have progressed by RECIST; otherwise must have had new lesions or PSA progression 2
28 Primary Endpoint: Overall Survival Proportion of OS (%) 100 (ITT Analysis) Median OS (months) Hazard Ratio 95% CI P value MP CBZP < Number at risk 0 0 months 6 months 12 months 18 months 24 months 30 months MP CBZP
29 On-Study Laboratory Abnormalities Safety Population MP (n=371) CBZP (n=371) All Grades (%) Grade 3 (%) All Grades (%) Grade 3 (%) Hematology Anemia Leukopenia Neutropenia Thrombocytopenia Biochemistry Alkaline Phosphatase ALAT ASAT Hyperbilirubinemia Creatinine
30 Total Deaths During Study Safety Population MP (n=371) CBZP (n=371) Total deaths during study 275 (74.1%) 227 (61.2%) Due to progression 253 (68.2%) 197 (53.1%) Due to AEs 7 (1.9%) 18 (4.9%) Due to other reasons 15 (4.0%) 12 (3.2%) 3


31 APPENDICULAR AND AXIAL METASTASIS
32 Skeletal-Related Events Pathologic fracture Spinal cord compression/vertebral body collapse Radiation or surgery to bone Change in antineoplastic therapy


33 Bone Metastases Can Have Serious Consequences


34 The Cycle of Bone Destruction: Osteoblastic Effects
35 SKELETAL RELATED EVENTS SRE Fracture, need for XRT, cord compression, pain, hypercalcemia Zometa (Zoledronic acid) Potent bisphosphonate given IV every 3-4 weeks Inhibits osteoclasts 35% reduction in SREs, postponement to time to first SRE Side-effects (nephrotoxicity, ONJ, flu-like symptoms) Xgeva (Denosumab) Rank ligand inhibitor (osteoclast inhibitor) given SQ every 3-4 weeks Slightly better reduction in SREs and time to first SRE than zometa Side-effects (hypocalcemia, ONJ) Both FDA-approved for castrate-resistant, bone mets ASCO no superiority of either drug
36 Zometa 039: Skeletal-Related Event (SRE) Prevention Study Bone metastases with progressive disease after ADT (N=639) Randomize Standard Care + ZOMETA Standard Care + Placebo Endpoint: SRE
37 Proportion of Patients With SRE (-HCM) at Month 15 by Treatment (Intent-to-Treat Patients) Proportion of Patients With SRE % * 34% 45% ZOMETA 8/4 mg ZOMETA 4 mg Placebo *P<.05 vs placebo
38 Time to First SRE ( HCM) by Treatment % Patients Without the Event ZOMETA 4 mg Median Time, Days* NR Placebo Time After the Start of Study Drug (Days) *P=.011 ZOMETA 4 mg vs placebo
39
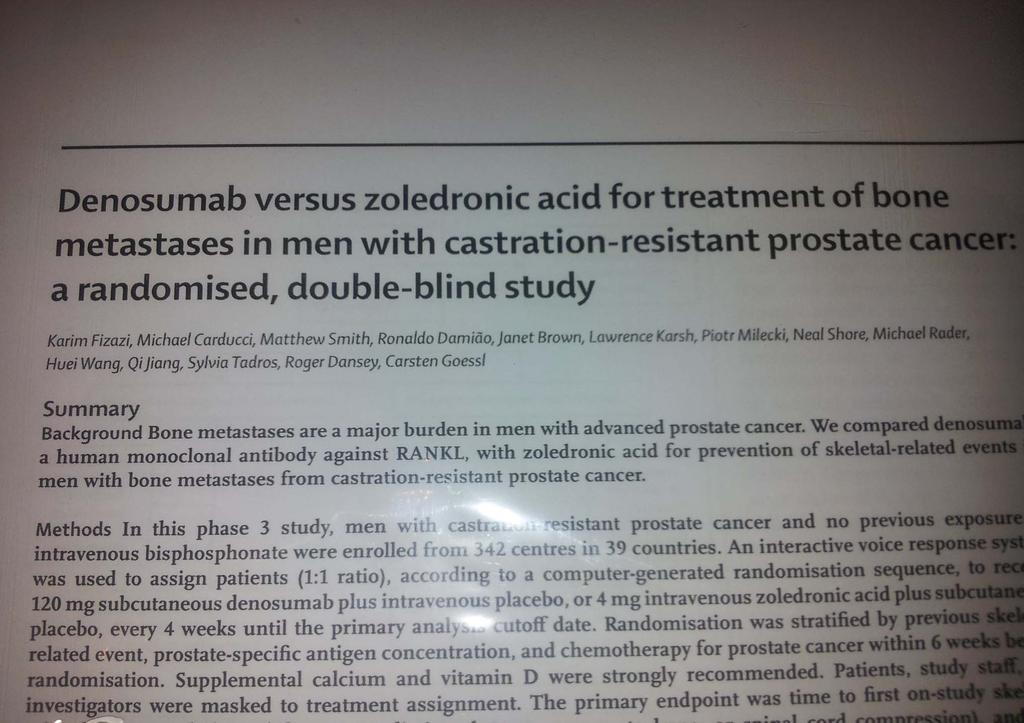
40 Study Design: International, Randomized, Double- Blind, Active-Controlled Study Key Inclusion Hormone-refractory (castration resistant) prostate cancer and bone metastases Key Exclusion Current or prior IV bisphosphonate treatment Denosumab 120 mg SC and Placebo IV* every 4 weeks (N = 950) Zoledronic acid 4 mg IV* and Placebo SC every 4 weeks (N = 951) Calcium and Vitamin D supplemented in both treatment groups Accrual period from May 2006 to December 2008 Analysis cut-off date October 2009 *Per protocol and Zometa label, IV product dose adjusted for baseline creatinine clearance and subsequent dose intervals determined by serum creatinine. No SC dose adjustments made due to increased serum creatinine.
41 Time to First On-Study SRE Proportion of Subjects Without SRE HR 0.82 (95% CI: 0.71, 0.95) P = (Non-inferiority) P = (Superiority) Denosumab Zoledronic acid KM Estimate of Median Months % Risk Reduction Study Month Subjects at risk: Zoledronic Acid Denosumab

42
43 Ligand activated androgen receptor signaling remains a driver in CRPC Hypothesis: Hormone-refractory prostate cancer (HRPC) frequently remains driven by a ligand-activated androgen receptor (AR). This disease is not truly hormone refractory
44 Biological evidence for a continued hormone driver in CRPC High intratumoral androgens despite castration Castration resistance: AR amplification/ mutations in CRPC increase AR activity AR mrna expression alone resistance in isogenic lines Aberrant activation of the androgen receptor
45 Abiraterone Clinical Trials Abiraterone vs placbo in patients with CRPC prior to docetaxel Abiraterone/prednisone vs placebo/prednisone in CPRC patients post chemotherapy. Close to accrual
46
47 AFFIRM Phase 3 Registration Trial of MDV3100 in Post-Chemotherapy CRPC Patients 2 MDV mg QD R 1 Placebo QD Primary Endpoint: 25% survival increase (12 to 15 months) Sample size: ~1170 (780 and 390) Statistics: 85% Power; p=0.05, two-sided Biomarkers: CTC enumeration and profiling with outcome Scher, H. (North America) and De Bono, J. Co-PI, Medivation
48 Conclusions Standard of care for CRPCA is docetaxel/prednisone Novel phase IIII studies are combining docetaxel with novel targeted agents Carbazitaxel is approved as a second line therapy for castration resistant prostate cancer New biological approaches are being evaluated in the second line setting
49 Prostate Cancer The Future Immunotherapy or Vaccine therapy Provenge GVAX Others in development Satraplatin-an oral chemotherapy agent Targeted agents such as erlotinib, bevacizumab
50 THANK YOU!
51 PATIENT CASE A 68 yo man had T3, PSA 15, grade 8 cancer and underwent XRT and 2 years ADT with PSA going to undetectable. One year after completing ADT, his PSA begins to rise and reaches 2.5 ng/dl in 12 months. He is anxious but asymptomatic. What term is used to describe his prostate cancer? What assessment should be done? a) Serum testosterone level b) Calculate PSA doubling time C) Bone scan d) CT ab/pelvis/cxr e) All the above (correct answer)
52 Testosterone level is normal at 190. PSADT is ~6 months. Bone scan and CT scans do not show obvious mets. What are the correct treatment options? a) Continued monitoring with PSA q 3 months b) Repeat XRT to prostate c) LHRH agonist given continuously or intermittently d) Taxotere chemotherapy e) Casodex alone
53 Lupron is started every 3 months. PSA falls to 0.4 after 6 months but then rises to 5.5 over next 9 months. Repeat bone scan shows 4 new osseous lesions in the pelvis and spine c/w mets. CT shows enlarged pelvic nodes. He remains asymptomatic other than hot flashes. What term is used to describe his prostate cancer? What are the correct treatment options? a) Taxotere chemotherapy b) Add casodex 50 mg/d c)zytiga d)provenge e) Start zometa or xgeva f) b and e (correct)
54 Casodex is added to Lupron. Zometa is started monthly. PSA continues to rise. He reports mild low back pain relieved with advil. What are the correct treatment options? a) Another antiandrogen b) Ketoconazole c) Provenge d) Taxotere chemotherapy e)zytiga f) b or c (correct)
55 The pt undergoes treatment with Provenge which is well-tolerated. His PSA continues to rise rapidly. His back pain worsens and is requiring hydrocodone for relief. Scans show 4 new osseous lesions and larger nodes. CT shows new left hydronephrosis. What are the correct treatment options? a) Referral to Urologist for management of hydro b) XRT to L-spine c)taxotere d)all the above (correct)
56 Urologist stents left ureter. He receives XRT to L- spine with good palliation of pain. He is then treated with Taxotere for 8 cycles with a 50% drop in his PSA. Treatment stopped due to worsening fatigue. His PSA begins to increase within the next 6-7 months. Repeat scans show 3 new bone lesions. What are the correct treatment options? a) Repeat Taxotere b) Jevtana (Cabazitaxel) c)zytiga (Abiraterone) d)investigational drug e)all the above (correct answer)
57 Questions Prostate cancer after hormone ablation is A) Still hormone responsive B) Does not respond to chemotherapy C) Spreads to the bone in 90% of pateints D) A and C
58 Question 2 A significant complication of treatments targeting bone (bisphosphophonates and denosamab) is A) Osteonecrosis of the jaw B) Hand foot syndrome C) Rash D) Diarrhea
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
 www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
www.drpaulmainwaring.com Figure 1 Androgen action Harris W P et al. (2009) Nat Clin Pract Urol doi:10.1038/ncpuro1296 Figure 2 Mechanisms of castration resistance in prostate cancer Harris W P et al. (2009)
Prostate Cancer 2009 MDV Anti-Angiogenesis. Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy. Docetaxel/Epothilone
 Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Prostate Cancer 2009 Anti-Angiogenesis MDV 3100 Anti-androgen Radiotherapy Surgery Androgen Deprivation Therapy Docetaxel/Epothilone Abiraterone DC therapy Bisphosphonates Denosumab Secondary Hormonal
Current Chemotherapy for Castration Resistant Prostate Cancer
 Current Chemotherapy for Castration Resistant Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine at Columbia University Medical Center/NY Presbyterian Hospital Disclosure Consultant: Sanofi Aventis,
Current Chemotherapy for Castration Resistant Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine at Columbia University Medical Center/NY Presbyterian Hospital Disclosure Consultant: Sanofi Aventis,
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일
 New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
New Treatment Modalities and Clinical Trials for HRPC 계명의대 김천일 Castrate-Resistant Prostate Cancer (CRPC) Current standard therapy Androgen receptor (AR) in CRPC New systemic therapies Hormonal therapy
Advances in Chemotherapy for Castration Resistant Prostate Cancer
 Advances in Chemotherapy for Castration Resistant Prostate Cancer Daniel P. Petrylak, MD Director, Genitourinary Oncology Co Director, Signal Transduction Program Yale Comprehensive Cancer Center Sequencing
Advances in Chemotherapy for Castration Resistant Prostate Cancer Daniel P. Petrylak, MD Director, Genitourinary Oncology Co Director, Signal Transduction Program Yale Comprehensive Cancer Center Sequencing
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in nonorchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
A Forward Look at Options for. In Prostate Cancer
 A Forward Look at Options for Prostate Cancer Charles J Ryan, MD Associate Professor of Medicine Helen Diller Family Comprehensive Cancer Center University of California, San Francisco UC 1 SF UC SF Castration
A Forward Look at Options for Prostate Cancer Charles J Ryan, MD Associate Professor of Medicine Helen Diller Family Comprehensive Cancer Center University of California, San Francisco UC 1 SF UC SF Castration
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Until 2004, CRPC was consistently a rapidly lethal disease.
 Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Until 2004, CRPC was consistently a rapidly lethal disease. the entry in systemic disease is declared on a an isolated PSA recurrence after local treatment so!!! The management of CRPC and MCRPC is different
Advanced Prostate Cancer
 Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Advanced Prostate Cancer January 13, 2017 Sindu Kanjeekal MD FRCPC Medical Oncology and Hematology Regional Systemic Quality Lead Erie St Clair Adjunct Professor Schulich School of Medicine and University
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Philip Kantoff, MD Dana-Farber Cancer Institute
 CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
CHEMOTHERAPY FOR MCRPC Philip Kantoff, MD Dana-Farber Cancer Institute Harvard Medical School 1 Disclosure of Financial Relationships With Any Commercial Interest Name Nature of Financial Commercial Interests
Strategic decisions for systemic treatment. metastatic castration resistant prostate cancer (mcrpc)
") Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Strategic decisions for systemic treatment metastatic castration resistant prostate cancer (mcrpc) SAMO Luzern 14.09.2012 Richard Cathomas Onkologie Kantonsspital Graubünden richard.cathomas@ksgr.ch mcrpc
Management of castrate resistant disease; after first line hormone therapy fails
 Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Management of castrate resistant disease; after first line hormone therapy fails Dr. Syed A Hussain Clinical Senior Lecturer and Consultant in Medical Oncology University of Liverpool and Clatterbridge
Index Patients 3& 4. Guideline Statements 10/11/2014. Enzalutamide Reduced the Risk of Death
 //4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
//4 Prolonged Radiographic Progression-Free Survival Reduced the Risk of Death Overall ITT Population Estimated median rpfs, months (9% CI): : NYR (.8 NYR); placebo:.9 (.7.4) rpfs (%) ( Enza 9 8 7 4 8
When exogenous testosterone therapy is. adverse responses can be induced.
 Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Theoretical tips It has been reasoned that discontinuation of ADT in non orchiectomized patients may have detrimental effect on patients with CRPC as discontinuation of ADT can result in renewed release
Novel treatment for castration-resistant prostate cancer
 Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
Novel treatment for castration-resistant prostate cancer Cora N. Sternberg, MD, FACP Chair, Department of Medical Oncology San Camillo and Forlanini Hospitals Rome, Italy Treatment options for patients
ADT vs chemo + ADT as initial treatment for advanced prostate cancer
 ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia
 In Oncologia") SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract on Prostate Cancer) In Oncologia Divisione di Oncologia Medica Unità Tumori Genitourinari SESSIONE PLATINUM SERIES (Best Papers Poster o Abstract
ASCO 2012 Genitourinary tumors
 ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
ASCO 2012 Genitourinary tumors Post ASCO Bern 14-06-2012 Dr. med. Richard Cathomas leitender Arzt Onkologie, KSGR, Chur Renal cell cancer Changes in first line treatment? Prostate cancer 3 positive phase
8/31/ ) Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases
 Intermittent androgen deprivation in androgen-sensitive PCa. 1) Alpharadin (Ra223) in CRPC with bone metastases") Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Bruce J. Roth, M.D. Clinical Trials: Medivation, Oncogenix 1) Alpharadin (Ra223) in CRPC with bone metastases 2) Enzalutamide (MDV-31) in CRPC and prior docetaxel 3) Abiraterone in chemo-naïve CRPC 4)
Evolution of Chemotherapy for. Cancer
 Evolution of Chemotherapy for Hormone Refractory Prostate t Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology Princess Margaret Hospital and University of Toronto In 1985, two
Evolution of Chemotherapy for Hormone Refractory Prostate t Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology Princess Margaret Hospital and University of Toronto In 1985, two
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC)
") Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Sequencing Strategies in Metastatic Castration Resistant Prostate Cancer (MCRPC) Amit Bahl Consultant Oncologist Bristol Cancer Institute Clinical Director Spire Specialist Care Centre UK Disclosures Advisory
Management of castration resistant prostate cancer after first line hormonal therapy fails
 Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Management of castration resistant prostate cancer after first line hormonal therapy fails Simon Crabb Senior Lecturer in Medical Oncology University of Southampton WHAT ARE THE AIMS OF TREATMENT? Cure?
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc
 SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
SOGUG meeting New drugs after docetaxel chemotherapy in patient with mcrpc Stéphane OUDARD, MD, PhD Head of the Oncology department Georges Pompidou Hospital, Paris France University Rene Descartes, Paris
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223
 SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
SYSTEMIC THERAPIES FOR CRPC: Chemotherapy and Radium-223 ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 4-5 October 2018 Disclosures Participation in advisory boards:
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents
 Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Androgens and prostate cancer: insights from abiraterone acetate and other novel agents Ian Davis Ludwig Institute for Cancer Research Austin Health, Melbourne, Australia Supported in part by an Australian
Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT
![Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT](/thumbs/71/65630457.jpg "Saad et al [12] Metastatic CRPC. Bhoopalam et al [14] M0 PCa on ADT <1 yr vs >1 yr ADT") Evolution of Treatment Options for Patients with and Bone Metastases Trials of Treatments for Castration-Resistant Prostrate Cancer Mentioned in This Review Bisphosphonates (Zometa) 4 mg IV 8 mg IV ( to
Evolution of Treatment Options for Patients with and Bone Metastases Trials of Treatments for Castration-Resistant Prostrate Cancer Mentioned in This Review Bisphosphonates (Zometa) 4 mg IV 8 mg IV ( to
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Recent Progress in Management of Advanced Prostate Cancer
 Review Article [1] April 15, 2005 By Philip W. Kantoff, MD [2] Androgen-deprivation therapy, usually with combined androgen blockade, is standard initial treatment for advanced prostate cancer. With failure
Review Article [1] April 15, 2005 By Philip W. Kantoff, MD [2] Androgen-deprivation therapy, usually with combined androgen blockade, is standard initial treatment for advanced prostate cancer. With failure
Management Options in Advanced Prostate Cancer: What is the Role for Sipuleucel-T?
 Clinical Medicine Insights: Oncology Consise Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Management Options in Advanced Prostate Cancer: What is
Clinical Medicine Insights: Oncology Consise Review Open Access Full open access to this and thousands of other papers at http://www.la-press.com. Management Options in Advanced Prostate Cancer: What is
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW
 LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Abiraterone for the treatment of metastatic castration-resistant prostate cancer that has progressed on or after a docetaxel-based chemotherapy regimen Disease
SAMPLE ONLY. Your Health Matters. Advanced Prostate Cancer and its Treatment A Patient Guide. Please order from Documents and Media: 415/
 Your Health Matters Advanced Prostate Cancer and its Treatment A Patient Guide UCSF Genitourinary Medical Oncology Program Charles Ryan, MD, UCSF Patient Advocates Please order from Documents and Media:
Your Health Matters Advanced Prostate Cancer and its Treatment A Patient Guide UCSF Genitourinary Medical Oncology Program Charles Ryan, MD, UCSF Patient Advocates Please order from Documents and Media:
SUMMARY. 3. Emerging understanding of mechanisms of resistance to current treatments
 SUMMARY 1. Discuss the active agents in prostate cancer currently available in Australia 2. Celebrate the growing role for Prostate Medical Oncologists in Multi Disc Teams active treaments overall survival
SUMMARY 1. Discuss the active agents in prostate cancer currently available in Australia 2. Celebrate the growing role for Prostate Medical Oncologists in Multi Disc Teams active treaments overall survival
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
Medical Treatments for Prostate Cancer
 Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Bone Metastases. Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital
 Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Bone Metastases Sukanda Denjanta, M.Sc., BCOP Pharmacy Department, Chiangrai Prachanukroh Hospital 1 Outline Pathophysiology Signs & Symptoms Diagnosis Treatment Spinal Cord Compression 2 General Information
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
CME Baseline Curriculum Report
 CME Baseline Curriculum Report October 14, 2010 For CME Activity: Managing Advanced Prostate Cancer in the Community Setting: A Case-based Curriculum Supported by an independent educational grant from
CME Baseline Curriculum Report October 14, 2010 For CME Activity: Managing Advanced Prostate Cancer in the Community Setting: A Case-based Curriculum Supported by an independent educational grant from
Advanced Prostate Cancer. SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin
 Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Advanced Prostate Cancer SAMO Masterclass 17 th of March 2017 PD Dr. med. Aurelius Omlin aurelius.omlin@kssg.ch Conflicts of Interest Research Support: TEVA, Janssen Advisory Rolle: Astra Zeneca, Astellas,
Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy).
.") Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
Thanks to: The Medical Educator Consortium Luis Raez, MD, Florida International University 15th ed. Prostate Cancer Management: From Early Chemical Recurrence to HRPC (excluding Immunotherapy). Mayer Fishman,
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
LUNCH AND LEARN. April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology
 LUNCH AND LEARN April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology Medical Therapy for Prostate Cancer Androgen (testosterone) is required for the growth of both normal prostate and prostate cancers
LUNCH AND LEARN April 17, 2018 David R. Wilkinson M.D. Gulfshore Urology Medical Therapy for Prostate Cancer Androgen (testosterone) is required for the growth of both normal prostate and prostate cancers
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Second line hormone therapies. Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017
 Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Second line hormone therapies Dr Lisa Pickering Consultant Medical Oncologist ESMO Preceptorship Singapore 2017 Disclosures Institutional Research Support/P.I. Employee Consultant Major Stockholder Speakers
Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T
 Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T Schelhammer PF, Chodak G, Whitmore JB, Sims R, Frohlich MW, Kantoff PW. Lower baseline prostate-specific antigen is associated with a greater
Lower Baseline PSA Predicts Greater Benefit From Sipuleucel-T Schelhammer PF, Chodak G, Whitmore JB, Sims R, Frohlich MW, Kantoff PW. Lower baseline prostate-specific antigen is associated with a greater
PCa Commentary. Volume 74 March April 2012
 1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2490 www.seattleprostate.com PCa Commentary Volume 74 March April 2012 CONTENTS 1 AN ALTERNATIVE TO LUPRON 2 MDV3100 Phase III AFFIRM Trial Demonstrates
1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2490 www.seattleprostate.com PCa Commentary Volume 74 March April 2012 CONTENTS 1 AN ALTERNATIVE TO LUPRON 2 MDV3100 Phase III AFFIRM Trial Demonstrates
2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC
 Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Ronald de Wit Erasmus MC Cancer Institute The Netherlands 2014 Treatment Paradigms in mcrpc Docetaxel in hormone sensitive PC Disclosures Sanofi ; research grant support, consultancy and speaker fees Astellas;
Evolution or revolution in the treatment of prostate cancer
 Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
Evolution or revolution in the treatment of prostate cancer de Johann Sebastian de Bono, MB, ChB, FRCP, MSc, PhD Professor of Experimental Cancer Medicine Department of Medicine/ Drug Development Unit
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
Group Sequential Design: Uses and Abuses
 Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Group Sequential Design: Uses and Abuses Susan Halabi Department of Biostatistics and Bioinformatics, Duke University October 23, 2015 susan.halabi@duke.edu What Does Interim Data Say? 2 Group Sequential
Elderly men with prostate cancer + ADT
 Elderly men with prostate cancer + ADT Background and Rationale ADT and Osteoporosis Proportion of Patients With Fractures 1-5 Yrs After Cancer Diagnosis 21 18 +6.8%; P
Elderly men with prostate cancer + ADT Background and Rationale ADT and Osteoporosis Proportion of Patients With Fractures 1-5 Yrs After Cancer Diagnosis 21 18 +6.8%; P
Castrate-resistant prostate cancer: Bone-targeted agents. Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France
 Castrate-resistant prostate cancer: Bone-targeted agents Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation in advisory boards or as a speaker for: Amgen, Astellas,
Castrate-resistant prostate cancer: Bone-targeted agents Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation in advisory boards or as a speaker for: Amgen, Astellas,
ACTUALIZACIONES EN TRATAMIENTOS DIRIGIDOS AL HUESO. COMBINACIÓN CON OTRAS ESTRATEGIAS TERAPÉUTICAS.
 ACTUALIZACIONES EN TRATAMIENTOS DIRIGIDOS AL HUESO. COMBINACIÓN CON OTRAS ESTRATEGIAS TERAPÉUTICAS. ÁLVARO PINTO Servicio de Oncología Médica Hospital Universitario La Paz IdiPAZ, Madrid INTRODUCTION High
ACTUALIZACIONES EN TRATAMIENTOS DIRIGIDOS AL HUESO. COMBINACIÓN CON OTRAS ESTRATEGIAS TERAPÉUTICAS. ÁLVARO PINTO Servicio de Oncología Médica Hospital Universitario La Paz IdiPAZ, Madrid INTRODUCTION High
Joelle Hamilton, M.D.
 Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Joelle Hamilton, M.D. www.urologycentersalabama.com Case Presentation: CRPC, Rising PSA 70 yo healthy, fit, active man post RALP 8 years prior with rising PSA Rising PSA from 0.02 nadir to 3.4 thus ADT
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE. Daan De Maeseneer, Medisch Oncoloog
 PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
PLAATS VAN DE CHEMOTHERAPIE IN DE BEHANDELING VAN EEN PROSTAATCARCINOOM: EEN UPDATE Daan De Maeseneer, Medisch Oncoloog 1 Overview DEAT PSA/Tumor Burden METASTASES INITIAL DIAGNOSIS & THERAPY ADT CRP SREs/
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey
 Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Modern Screening and Treatment of Advanced Prostate Cancer John Tuckey Commonest male cancer - 2939 per year Third male cancer death 670 per year More die with it than of it but More people die of prostate
Policy. not covered Sipuleucel-T. Considerations Sipuleucel-T. Description Sipuleucel-T. be medically. Sipuleucel-T. covered Q2043.
 Cellular Immunotherapy forr Prostate Cancer Policy Number: 8.01.53 Origination: 11/2010 Last Review: 11/2014 Next Review: 11/2015 Policy BCBSKC will provide coverage for cellular immunotherapy for prostate
Cellular Immunotherapy forr Prostate Cancer Policy Number: 8.01.53 Origination: 11/2010 Last Review: 11/2014 Next Review: 11/2015 Policy BCBSKC will provide coverage for cellular immunotherapy for prostate
Perspective on endocrine and chemotherapy agents. Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr. Sternberg has received research funding for
Treatment of Prostate cancer and why I refuse to know my PSA. Outline of Presentation
 Treatment of Prostate cancer and why I refuse to know my PSA Ian F Tannock MD, PhD, DSc Princess Margaret Hospital and University of Toronto Outline of Presentation 1. Requirements for screening to be
Treatment of Prostate cancer and why I refuse to know my PSA Ian F Tannock MD, PhD, DSc Princess Margaret Hospital and University of Toronto Outline of Presentation 1. Requirements for screening to be
Bone-targeted therapies for prostate cancer in Institut Gustave Roussy Villejuif, France
 Bone-targeted therapies for prostate cancer in 2012 Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards or speaker for: Amgen, Astellas-Medivation,
Bone-targeted therapies for prostate cancer in 2012 Pr Karim Fizazi, MD, PhD Institut Gustave Roussy Villejuif, France Disclosure Participation to advisory boards or speaker for: Amgen, Astellas-Medivation,
INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER
 INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER Daniel George, MD Professor of Medicine and Surgery Director of Genitourinary Oncology Program Duke Cancer Institute 1 Disclosures Consultant:
INTERGRATING NON- HORMONAL THERAPIES INTO PROSTATE CANCER Daniel George, MD Professor of Medicine and Surgery Director of Genitourinary Oncology Program Duke Cancer Institute 1 Disclosures Consultant:
Immunotherapy Therapy for Prostate Cancer
 2006 Prostate Health Education Network African American Prostate Cancer Disparity Summit Immunotherapy Therapy for Prostate Cancer Glen W. McWilliams, MD Chief of Urology James J. Peters VAMC Assistant
2006 Prostate Health Education Network African American Prostate Cancer Disparity Summit Immunotherapy Therapy for Prostate Cancer Glen W. McWilliams, MD Chief of Urology James J. Peters VAMC Assistant
Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, Nasdaq: DNDN
 Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, 2009 Nasdaq: DNDN PROVENGE sipuleucel-t is an autologous active cellular immunotherapy that activates
Summary of Phase 3 IMPACT Trial Results Presented at AUA Meeting Webcast Conference Call April 28, 2009 Nasdaq: DNDN PROVENGE sipuleucel-t is an autologous active cellular immunotherapy that activates
Patients Living Longer: The Promise of Newer Therapies
 Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
Patients Living Longer: The Promise of Newer Therapies David M. Nanus, MD! Chief, Division of Hematology and Medical Oncology! Weill Cornell Medicine! New York Presbyterian Hospital!! Demographics 180,890
Ripamonti C, et al. ASCO 2012 (Abstract 9005)
") ZOOM: A Prospective, Randomized Trial of Zoledronic Acid for Long-term Treatment in Patients With Bone-Metastatic Breast Cancer After 1 Year of Standard Zoledronic Acid Treatment D. Amadori, M. Aglietta,
ZOOM: A Prospective, Randomized Trial of Zoledronic Acid for Long-term Treatment in Patients With Bone-Metastatic Breast Cancer After 1 Year of Standard Zoledronic Acid Treatment D. Amadori, M. Aglietta,
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Tubulin-binding drug In prostate cancer
 Tubulin-binding drug In prostate cancer Dr Christophe Massard Institut Gustave Roussy, Department of Cancer Medicine christophe.massard@igr.fr TAT Meeting, Paris, 2011 U981 Chemotherapy in Prostate Cancer
Tubulin-binding drug In prostate cancer Dr Christophe Massard Institut Gustave Roussy, Department of Cancer Medicine christophe.massard@igr.fr TAT Meeting, Paris, 2011 U981 Chemotherapy in Prostate Cancer
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Name of Policy: Cellular Immunotherapy for Prostate Cancer
 Name of Policy: Cellular Immunotherapy for Prostate Cancer Policy #: 432 Latest Review Date: July 2014 Category: Medical Policy Grade: A Background/Definitions: As a general rule, benefits are payable
Name of Policy: Cellular Immunotherapy for Prostate Cancer Policy #: 432 Latest Review Date: July 2014 Category: Medical Policy Grade: A Background/Definitions: As a general rule, benefits are payable
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE
 mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE IL CARCINOMA PROSTATICO, UNA MALATTIA ETEROGENEA? RAZIONALE E RISULTATI DEL TRATTAMENTO CHEMIOTERAPICO ASSOCIATO ALL
mcrpc 2014 TRA EVOLUZIONE E RIVOLUZIONE: COME ORIENTARSI NEL LABIRINTO DELLE TERAPIE IL CARCINOMA PROSTATICO, UNA MALATTIA ETEROGENEA? RAZIONALE E RISULTATI DEL TRATTAMENTO CHEMIOTERAPICO ASSOCIATO ALL
Chemohormonal Therapy For Prostate Cancer. What is old, is new again!
 Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Chemohormonal Therapy For Prostate Cancer What is old, is new again! Mount Tremblant January 20, 2017 Kala S. Sridhar MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital Head, GU Medical Oncology
Dendritic Cell Based Cancer Vaccine Development
 Dendritic Cell Based Cancer Vaccine Development November 10, 2005 CVCWG Meeting Rob Hershberg, MD, PhD Chief Medical Officer 1 Meeting the challenges of developing cancer vaccines-- APC8015 (Provenge TM
Dendritic Cell Based Cancer Vaccine Development November 10, 2005 CVCWG Meeting Rob Hershberg, MD, PhD Chief Medical Officer 1 Meeting the challenges of developing cancer vaccines-- APC8015 (Provenge TM
What will change for men with advanced prostate cancer in the next 24 months? ESO Observatory: Perspective on endocrine and chemotherapy agents
 Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Perspective on endocrine and chemotherapy agents Cora N. Sternberg Department of Medical Oncology San Camillo & Forlanini Hospitals Rome, Italy Disclosures Dr.Sternberg has received research funding for
Navigating Prostate Cancer Therapy. Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA
 Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
Navigating Prostate Cancer Therapy Nevin Murray MD Clinical Professor of Medicine, UBC Medical Oncologist, BCCA Disclosures In compliance with accreditation, we require the following disclosures to the
The Changing Landscape of Treatment Options For Metastatic Castrate-Resistant Prostate Cancer
 The Changing Landscape of Treatment Options For Metastatic Castrate-Resistant Prostate Cancer Challenges and Solutions for Physicians and Patients Carole Alison Chr vala, PhD INTRODUCTION Prostate cancer
The Changing Landscape of Treatment Options For Metastatic Castrate-Resistant Prostate Cancer Challenges and Solutions for Physicians and Patients Carole Alison Chr vala, PhD INTRODUCTION Prostate cancer
American Urological Association (AUA) Guideline
 Guideline") 1 Approved by the AUA Board of Directors May 2018 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2018 by the American Urological
1 Approved by the AUA Board of Directors May 2018 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2018 by the American Urological
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
New Treatment Options for Prostate Cancer
 New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
New Treatment Options for Prostate Cancer Moderator: Jeremy P. Goldberg, President, JPG Healthcare LLC Panelists: Philip Kantoff, MD, Director, Lank Center for Genitourinary Oncology, Dana- Farber Cancer
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
HOW I DO IT. Introduction. BARKIN J. How I Do It: Managing bone health in patients with prostate cancer. Can J Urol 2014;21(4):
:") HOW I DO IT How I Do It: Managing bone health in patients with prostate cancer Jack Barkin, MD Department of Surgery, University of Toronto, Humber River Hospital, Toronto, Ontario, Canada BARKIN J. How
HOW I DO IT How I Do It: Managing bone health in patients with prostate cancer Jack Barkin, MD Department of Surgery, University of Toronto, Humber River Hospital, Toronto, Ontario, Canada BARKIN J. How
Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia
 Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia 5-year prostate cancer specific survival rates have improved from 67% to 99% between 1974 and 2000 Excellent survival
Paul F. Schellhammer, MD, FACS Professor Eastern Virginia Medical School Norfolk, Virginia 5-year prostate cancer specific survival rates have improved from 67% to 99% between 1974 and 2000 Excellent survival
Secondary Hormonal therapies in mcrpc
 Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Secondary Hormonal therapies in mcrpc Ravindran Kanesvaran Consultant,Division of Medical Oncology National Cancer Centre Singapore 1 Disclosures Research Support/P.I. Sanofi Consultant Major Stockholder
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer. Dr. Simon Yu Nov 18, 2017
 GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research
GU Guidelines Update Meeting: M0 Castrate Resistant Prostate Cancer Dr. Simon Yu Nov 18, 2017 Faculty/Presenter Disclosure Faculty: Dr. Simon Yu Relationships with commercial interests: Grants/Research