Treatment Options in RCC: Past, Present and Future. Pr Stéphane Oudard, MD, PhD Georges Pompidou Hospital Paris, France
|
|
|
- Morgan Mills
- 5 years ago
- Views:
Transcription
1 1 Treatment Options in RCC: Past, Present and Future Pr Stéphane Oudard, MD, PhD Georges Pompidou Hospital Paris, France
2 2 Renal Cell Carcinoma (RCC) 208,500 new cases of kidney cancer are diagnosed this year worldwide 101,900 deaths In the Europe Union 1 46,000 new cases of kidney cancer are diagnosed each year 25-30% of patients have metastatic disease at diagnosis Prognosis: SEER 5-year 5 relative survival rates 71 to 97% if localized, confined by renal capsule (T1-2) 20 to 53% if locally advanced (T3-4, N+) < 10% if distant metastases 1 Levy F et al. Annal Oncol 2004;
3 3 Renal Cell Carcinoma (RCC) Newly diagnosed metastatic RCC have been classified by MSKCC model 1 Low Karnofsky PS (< 80%) Lactate dehydrogenase level > 1.5 time (upper limit of N) Hemoglobin level < lower limit of N High corrected serum calcium level (> 10 mg/dl) Absence of nephrectomy No prognostic factor: OS 22 months 1 prognostic factor : OS 11.9 months > 2 prognostic factors: OS 5.4 months 1 Motzer R et al. J Clin Oncol 1999;17:
 Overexpression of VEGF is often linked to Von Hippel Lindau (VHL) gene mutation (>( 70% clear cell")
4 4 Different tumor types and Rational for Antiangiogenic use Kidney cancer: Highly vasculature tumor Vascularization due to a GF: VEGF (Vascular( Endothelial Growth Factor) Overexpression of VEGF is often linked to Von Hippel Lindau (VHL) gene mutation (>( 70% clear cell carcinoma)
 1 VEGF and PDGF promote tumour angiogenesis that may contribute to tumour hypervascularity in RCC 1 Kaelin WG Jr.")
5 5 Underlying Biology of clear cell RCC Loss of VHL gene function in clear-cell cell RCC results in up-regulated expression of vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF) 1 VEGF and PDGF promote tumour angiogenesis that may contribute to tumour hypervascularity in RCC 1 Kaelin WG Jr. Clin Cancer Res 1994;10:6290s 6295s * DNA-Hypoxia response element *
6 ANGIOGENESIS : A DYNAMIC BALANCE BETWEEN ACTIVATORS AND INHIBITORS HIF ON switch ACTIVATORS Growth factors (VEGF, bfgf, PDGF, PlGF) Angiopoietin 1 Fibrinolytic enzymes (tpa, upa) MMPs Cytokins (TNF, TGF, IL8) ECM proteins (laminin) INHIBITORS MEC proteins Angiopoietin 2 TIMPs Cytokins (IL-10) Angiostatin, Endostatin Thrombospondins Netrin1/Unc5B AGT (serpins) Angiopoietin like 4 OFF 6

7 VEGF Overexpression and Abnormal blood vessels Thurston et al. Science 1999, Vol
8 Metastatic RCC An area of Unmet Medical Need mrcc is generally resistant to standard chemotherapy Nephrectomy mainstay of treatment Cytokine therapy (IL-2 2 or IFN-α) standard of care until now only a minority of patients experience clinical benefit 1 adverse events may be problematic second-line treatment with alternative cytokines produces responses in <5% of patients 2 Alternative agents are urgently needed Current drug treatments are limited, not effective and toxic 1 Bukowski RM. Semin Urol Oncol 2001;19: Escudier B et al. J Clin Oncol 1999;17:
9 Cytokine Therapy in Phase III Trials Regimen No. of Pts % Response Survival Benefit MRCRCC 1 IFN MPA* % 2% Yes Pyrhonen et al 2 Vinblastine IFN + Vinblastine % 16.5% Yes Negrier et al 3 IL-2 IFN IL IFN % 8% 19% No Yang et al 4 High dose IL-2 Low dose IL-2 SQ IL % 11% 10% 1 Lancet 1999;353:14; 2 JCO 1999,17: , 3 NEJM 1998;338:1272; 4 JCO 2003;21:3127; *Medroxyprogesterone No 10
10 Therapeutic Targets in RCC β pvhl α = HIF mtor Bevacizumab Temsirolimus VEGF VEGFR PDGF PDGFR Axitinib Sunitinib Sorafenib Other potential targets: Raf kinase and EGFR Kaelin WG. Nat Rev Cancer 2002;2:
11 12 Sunitinib Mechanism of Action in RCC Loss of VHL Protein Function VEGF PDGF VEGFR VEGF PDGF PDGFR Vascular Endothelial Cell Pericyte/Fibroblast/ Vascular Smooth Muscle Sunitinib Vascular permeability Cell survival, proliferation, migration Vascular formation, maturation Inhibition of RCC pathogenesis and progression
12 Phase II Evaluation of Sunitinib in Metastatic RCC Two Independent, Single-Arm, Multicenter, Phase II Studies 1, 2 (Study 014: N=63; Study 1006: N=106) Patients with Advanced Disease and Failure of of Prior Cytokine Therapy Sunitinib Continue Sunitinib Treatment Unless Progression or or Intolerability Dosing schedule 4 weeks on, 2 week off (4/2) Sunitinib 50mg/day* Sunitinib *Dose reduction permitted (to 37.5mg/day and then to 25mg/day) 1 Motzer et al, JCO 2006;24(1):16-24 ; 2 Motzer et al, JAMA 2006;295:
13 Sunitinib Phase II: Patient Characteristics Study 014 (N=63) Study 1006 (N=105) Pooled Analysis (N=168)* Median age (years) ECOG PS 0/1 (%) 54/45 54/46 54/46 Clear cell/other histology (%) 87/13 100/0 95/5 Prior nephrectomy (%) Prior radiation therapy (%) Number of metastatic sites (%) > *One patient was omitted from the efficacy analysis of study 1006 due to a change in diagnosis 16
14 19 Sunitinib therapy for patients with mrcc: Updated results of two phase II trials (2007) Updated efficacy data for 168 evaluable pts: ORR : 45% (95% CI: 39%, 54%) Median PFS: 8.4 Mo (95%( CI: 7.9, 10.7) Median OS: 22.3 Mo (95% CI: 14.8, 36.0) Median duration of response : 11.6 Mo (95% CI: 9.9, 15.2) Patients alive at 2 years : 48% 20 pts remain on treatment with sunitinib longest pt on the drug for >3.5 years with PR for >3 years 1 pt with a complete response for >2 years Motzer R et al, J Urol 2007
15 20 Progression-Free Survival in Responders and Non- Responders (Studies 014 and 1006) Progression-Free Survival (Months) Responders (N=71) Stable disease 3 3 months (N=41) Stable disease <3 months or progressive disease (N=56) 14.8 (95% CI: ) 7.9 (95% CI: ) 2.1 (95% CI: ) 2.3)
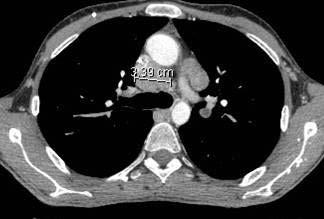


16 21 Interpretation of response in mrcc treated by AA using RECIST Criteria
17 Dynamic contrast enhanced (DCE) imaging 22
18 22 Dynamic contrast enhanced (DCE) imaging Before injection of drug contrast
19 22 Dynamic contrast enhanced (DCE) imaging Before injection of drug contrast VCS
20 22 Dynamic contrast enhanced (DCE) imaging Before injection of drug contrast VCS Aortic vessel
 imaging Before")

21 22 Dynamic contrast enhanced (DCE) imaging Before injection of drug contrast VCS Aortic vessel After drug contrast
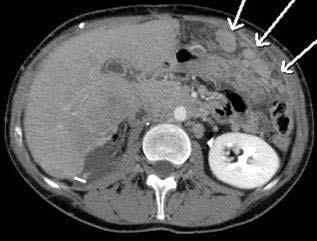
22 Aorte Before treament Metastasis Aorte Metastasis Analyse réalisée à l HEGP, radiologie vasculaire, Pr CA Cuenod/ L Fournier 23
23 Aorte Before treament Metastasis Aorte After treatment Metastasis Analyse réalisée à l HEGP, radiologie vasculaire, Pr CA Cuenod/ L Fournier 23
24 28 Phase 3 Randomized Trial of Sunitinib malate (SU11248) versus Interferon-alfa as First-line Systemic Therapy for Patients with Metastatic Renal Cell Carcinoma RJ Motzer, TE Hutson,, P Tomczak, MD Michaelson, RM Bukowski,, O Rixe, S Oudard, ST Kim, CM Baum, RA Figlin and the SU11248 Study Group Supported by Pfizer Inc MSKCC
25 30 Randomization & Study Treatment N=750 Stratification Factors LDH 1.5 vs >1.5xULN ECOG PS 0 vs 1 Presence vs Absence of Nephrectomy R A N D O M II Z A T II O N Sunitinib (n=375) mg po podaily on on Schedule 4/2 4/2 (4 (4 weeks on/2 weeks off) IFN-α (n=375) 3 MU TIW 1 st st week 6 MU TIW 2 nd nd week 9 MU TIW 3 rd rd week thereafter; SC SC Injection Repeated 6-week 6 cycles Response and safety assessments Dose reduction for toxicity Treatment continued unless progression or intolerance
26 32 Best Response Response (RECIST) Sunitinib (n=374) Investigator Assessment IFN-α (n=373) Independent Central Review Sunitinib (n=365) IFN-α (n=346) No. of patients (%) Objective response* 174 (46) 45 (12) 142 (39) 29 (8) Complete response 5 (1) 4 (1) 0 0 Partial response 169 (45) 41 (11) 142 (39) 29 (8) Stable Disease 152 (41) 205 (55) 146 (40) 165 (48) PD or Not evaluable 48 (13) 123 (33) 77 (21) 152 (44) *Sunitinib vs IFN-α: P<
27 Progression-Free Survival (Independent Central Review) 1.0 Progression-free survival probability Hazard Ratio= % CI (0.439, 0.658) p< Sunitinib Median: 11.0 months (95% CI: ) IFN- α Median: 5.1 months (95% CI: ) No. at Risk Time (Months) Sunitinib:
28 34 Progression-Free Survival by MSKCC Risk Status* MSKCC Risk Factors: 0 (Favorable) Independent Central Review MSKCC Risk Factors: 1 2 (Intermediate) MSKCC Risk Factors: 3 (Poor) Progression-free survival probability Sunitinib (n=143) Median not reached IFN-α (n=121) Median: 8 months (95% CI: 7 NA) Hazard ratio=0.371 (95% CI: ) Hazard ratio=0.388 (95% CI: ) Sunitinib (n=209) Median: 11 months (95% CI: 11 11) IFN-α (n=212) Median: 4 months (95% CI: 3 4) Sunitinib (n=23) Median: 4 months (95% CI: 1 10) IFN-α (n=25) Median: 1 month (95% CI: 1 2) Hazard ratio=0.534 (95% CI: ) Time (months) Time (months) Time (months) *Motzer et al. J Clin Oncol 2002;20: ; excludes 17 pts from IFN-α with missing data
29 35 Patient Baseline Characteristics Predictive of Progression-free Survival for 375 Patients Treated on the Sunitinib arm of the Phase 3 Trial
30 Progression-free Survival According to Risk Factors Derived from Sunitinib Treated Patients Risk Factors 0 N 112 Median PFS (months) % CI (months) Progression-free survival probability ECOG PS (0 vs. 1) Time from diagnosis to treatment ( 1( 1 yr vs. < 1 yr) Corrected calcium ( 10 vs. >10 mg/dl dl) *Outcome by investigator assessment Time (Months) Motzer R, ASCO
31 Overall Survival Overall Survival Probability Hazard Ratio = 0.65 (95% CI: ) P = * Sunitinib (n=375) Median not reached IFN-α (N=375) Median not reached Time (Months) No. at Risk Sunitinib: No. at Risk IFN-α: *The observed p-value did not meet the pre-specified level of significance for this interim analysis 38
32 Treatment-Related Adverse Events Event Fatigue Diarrhea Nausea Stomatitis Hypertension Hand-foot syndrome Ejection fraction decline Pyrexia Chills Myalgia Flu-like like symptoms All grade Sunitinib (%) Grade 3/4 7 5* 3 1 8* 5* <1 0 All grade IFN-α (%) Grade 3/4 11/<1* 0 1 <1 < <1 <1 * Greater frequency, P <
33 40 Laboratory Abnormalities Sunitinib (%) IFN-α (%) Event All grade Grade 3/4 All grade Grade 3/4 Neutropenia 72 11/1* 46 7 Anemia 71 3/<1 64 4/<1 Thrombocytopenia 65 8* 21 0 Lymphopenia * Hypophosphatemia 36 4/< Hyperamylasemia 31 4/1* 28 2/<1 * Greater frequency, P <0.05
34 41 Asthenia Fatigue is often cited as one of the most common reasons for discontinuation of treatment Fatigue is multifactorial A greater risk of fatigue is likely where the patient profile is : Elderly and frail Large tumour burden MANAGEMENT OF FATIGUE Provide counseling on what to expect from treatment and psychological support where feasible Determine whether the patient is suffering from anemia/ hypothyroidism (check every 2-33 cycles), depression For first 2 to 3 cycles provide close support and involvement with patient to counsel and motivate on coping with fatigue At end of 2nd cycle conduct a focused check-up with the patient on the level of fatigue level and impact on quality of life Modify dosage to 37.5mg where fatigue is disruptive to quality of life Enable patient to self monitor after 3rd cycle
35 Endocrine toxicity HYPOTHYROIDISM Frequent event with Sunitinib Sunitinib: Increase TSH level during treatment in 70% of the pts In daily practice Dosage of T4 & TSH before treatment and then every 3 months Supplementation in case of hypothyroïdism Rini BI et al, J Natl Cancer Inst
36 43 Hypertension A full cardiovascular screening should be performed before commencement of treatment to identify any compounding factors to hypertension If Hypertension exists, treat it and delay commencement of treatment until the hypertension is under control MANAGEMENT OF HYPERTENSION Check and control HT before commencing treatment Measure 3 / week during the first 2 cycles Conduct a 2nd full CV screening at 12 weeks Measure 1 / month after the first 2 cycles Adapt HT treatment to reflect the discontinuous treatment cycle, knowing that 2-week 2 off-cycle relieves side effects

37 Hypertension: check blood pressure Azizi M, Chedid A & Oudard S, N Engl J Med
38 45 Cardiac dysfunctions (Sunitinib) Due to mitochondrial injuries and cardiomyocyte apoptosis 11% of pts had cardiovascular event: cardiac heart dysfunction and a coronary artery diseases Sunitinib induces increase in mean systolic and diastolic blood pressure (47%) Associated with asymptomatic LVEF reduction (28%) LVEF is recommended to monitor this side effect especially in at risk patients This toxicity usually resolved upon treatment discontinuation
39 50 Sunitinib is Effective Therapy for Metastatic RCC January 2006: US FDA approval for advanced RCC July 2006: EMEA conditional approval for the treatment of cytokine-refractory advanced and/or metastatic RCC January 2007: EMEA approval for the first-line treatment of advanced and/or metastatic RCC
40 53 Sunitinib Expanded Access Study Patient Characteristics Median age, (range) ECOG PS* Prior nephrectomy Histology* Clear cell Other - - * Missing: PS = 2%, histology = 0.4% n = 2, (19-85) 1985 (84.8%) 308 (13.2%) 2118 (90.5%) 2056 (87.8%) 276 (11.8%)
41 54 Sunitinib Expanded Access Study Patient Characteristics Prior therapy Antiangiogenic Cytokines - - n = 2, (7.1%) 1938 (82.8%) Prior cytokine Rx (n = 1,840) 0 favourable 1-2 intermediate 3 poor 532 (28.9%) 606 (32.9%) 181 (9.8%)



42 Sunitinib cross the brain blood barrier Annal Oncol
43 Exposure-Response of Sunitinib in Metastatic Renal Cell Carcinoma (mrcc): a Population Pharmacokinetic/Pharmacodynamic (PKPD) Approach Objectives Meta-analysis analysis of pharmacokinetic and efficacy data from all clinical studies with single-agent sunitinib in mrcc To evaluate differences in response to sunitinib as a function of individual sunitinib exposures To evaluate relative efficacy of sunitinib 50 mg/day on 4/2 schedule vs mg/day on CD schedule Total number of patients: 237 Treatment naïve 42 / Cytokine Refractory 195 Houk BE, ASCO
44 Probability of PR or CR in mrcc Increased with Mean Daily Sunitinib Exposure Probability of a response 1.0 Mean 95% CI P=0.023 for AUC AUCss sunitinib (ug hr/ml) PR = partial response; CR = complete response 63
45 66 Conclusions In mrcc, sunitinib displays greater efficacy in patients with the highest exposures higher probability of PR with increasing exposure longer TTP and OS with higher exposure greater changes in tumor volume with higher exposure Sunitinib 37.5 mg/day CD appears equally effective as 50 mg/day 4/2 schedule Similar trends displayed with exposure in GIST Ongoing exposure-response response work in breast, lung and colorectal cancer
46 Plasma VEGF level at D0, D28 and D42 for each patient (n = 33 pts) VEGF plasma level (ng/ml de plasma) J0 J28 J42/J0 J28 J42/J0 J28 J42/J0 J28 J42/J0 J28 J42 Cycle 1 Cycle 2 Cycle 3 Cycle 4 Cycle 5 67
47 Axitinib treatment in patients with cytokine-refractory metastatic renal-cell cancer: a phase II study Study design Multicenter phase II study: Axitinib (AG ) 5 mg twice daily Number pts: 52 pts Primay endpoint: OR (RECIST criteria) Results ORR: 44% with 2 CR and 21 PR Stable patients: 22 pts corresponding to a clinical benefit of 86% Median response duration : 23 months Median time to progression: 15.7 months Median overall survival: 29.9 months Toxicity: asthenia, diarrhea, hypertension Rixe O et al, Lancet Oncol

48 Activity of Axitinib using RECIST criteria Rixe O et al, Lancet Oncol
49 Eligibility criteria Histologically/cytologically confirmed, unresectable and/or metastatic disease Clear cell histology Measurable disease Failed one prior systemic therapy in last 8 months ECOG PS 0 or 1 Good organ function (1:1) Randomization n~884 Stratification Motzer criteria Country Sorafenib 400 mg bid Placebo Major endpoints PFS (alpha=0.01) Survival (alpha=0.04) No brain metastasis 73

50 SORAFENIB RESULTS 74
51 Final Results of the phase 3 trial of Sorafenib in Advanced RCC (TARGETs) n=903 patients Sorafenib vs Placebo Final analysis (561 events) 48 % of placebo patients have cross-over over to Sorafenib Median OS (months( months) Sorafenib Placebo Statistical Significance 1st Analysis NR 14.7 NS May nd Analysis NS Nov 2005 Final NS Sept 2006 Censored S June


52 76 Phase III TARGET : Sorafenib toxicity Tolérance Grade 3/4 Hand foot syndrome 6% Diarrhea 5% Neutropenia 13% Hypophosphatemia 13% Hyperamylasemia 12%
53 Phase II Trial of Sorafenib vs IFN as 1st- Line Treatment in mrcc: Study Design Eligibility Criteria Confirmed, unresectable and/or metastatic disease Clear cell histology Measurable disease No prior systemic therapy All MSKCC risk groups No brain metastasis (N=189) R A N D O M I Z A T I O N (n=97) (n=92) Sorafenib 400 mg bid IFN 9 MIU tiw Progression Sorafenib 600 mg bid Primary end points: PFS Escudier B, et al. ASCO Abstract 4501 (Oral presentation) 77
54 Progression-free Survival: Period 1 Independent Assessment Progression-free survival (% patients) Median PFS Sorafenib = 5.7 months IFN = 5.6 months Hazard ratio = 0.88 (95% CI: ) P=0.504 (log-rank test) Time from randomization (months) Patients at risk Sorafenib IFN Escudier B, et al; Presented at the 5th International Symposium on Targeted Anticancer Therapies; Amsterdam,; 8 March 2007 and ASCO
55 79 A Phase 2 trial of intra-patient dose- escalated sorafenib in patients with mrcc Phase 2 second line study n=44 Escalation from 400 mg bid to 800 mg bid 93 % of the patients could be dose escalated 32 pts at 1600 mg CR 16 % (7) PR 39 % (17) SD > 6 months 20 % PFS 8.4 months Well tolerated? Amato R. ASCO 2007, Abstract 5026
56 Growth factors and m-tor m signaling pathway Growth Factors IGF-1, VEGF, ErbB, etc Oxygen, energy, and nutrients Ras/Raf pathway kinases S6 S6K 1 PTEN TSC2 TSC1 PI3-K Akt/PK B Protein Production Cell Growth and Proliferation mtor Ras/Raf Abl ER Angiogenesis RAD001 CCI-779 4E-BP1 elf-4e Normal Cells: role of mtor in angiogenesis and proliferation Deregulation of mtor pathway frequent in different tumor types Cancer cells: RAD001 and CCI-779 Anti-proliferative effect Inhibition of angiogenesis Potentialisation of chemotherapy and targeted drugs 86
57 Temsirolimus Results mtor kinase inhibitor Inhibits translation of several key proteins that regulate cell cycle progression and angiogenesis Global ARCC Trial Temsirolimus vs. IFN Temsirolimus + IFN vs. IFN Modified MSKCC criteria (Poor-Risk Feature Patients) Minimum of 3 following criteria LDH > 1.5 x ULN Hb < LLN Ca ++ > 10 mg/dl Time from diagnosis to first treatment < 1 yr Karnosfky PS Multiple organ sites of metastasis 87
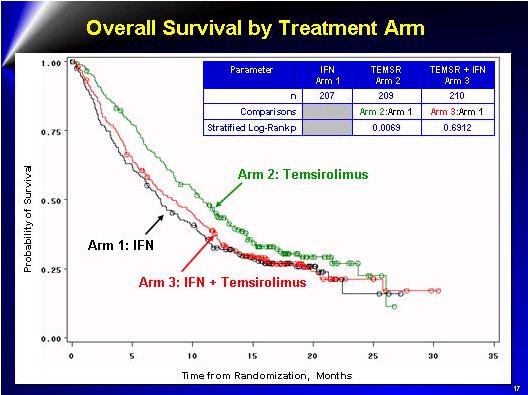
58 88
59 ESTABLISHED IN 1812 July 31, 2003 VOL. 349 (5) A Randomized Trial of Bevacizumab, an Anti Vascular Endothelial Growth Factor Antibody, for Metastatic Renal Cancer N = 79 Phase II 90
60 AVOREN (Bevacizumab): study design IFN-α2a + bevacizumab (n=327) PD RCC patients (n=649) 1:1 IFN-α2a + placebo (n=322) Bevacizumab/placebo 10 mg/kg i.v. q2w until progression IFN-α2a 9 MIU s.c. three times/week (maximum of 52 weeks) (dose reduction allowed) Multinational ex-us study: 101 study sites in 18 countries PD Stratification factors: country and Motzer score PD = progression of disease; i.v. = intravenous; s.c. = subcutaneous P.I. Bernard Escudier 91
61 92 AVOREN study: Tumor response* 100 IFN + placebo (n=289) 100 Bevacizumab + IFN (n=306) Percentage change of sum longest diameter of target lesions % 70% *Patients with measurable disease only; investigator assessed
62 93 Progression-free survival (investigator assessed) Probability of being progression-free Number of patients at risk HR=0.63, p< Median progression-free survival: Bevacizumab + IFN = 10.2 months IFN + placebo = 5.4 months Time (months) IFN + placebo Bevacizumab + IFN
63 Interim analysis of overall survival (251 of 450 scheduled events) Probability of survival Number of patients at risk HR=0.75 (95% CI: ), p<0.0267* Median overall survival: Bevacizumab + IFN = NR IFN + placebo = 19.8 months Time (months) IFN + placebo Bevacizumab + IFN *Stratified by Motzer score and region category; unstratified analysis HR=0.79, p=0.067; prespecified level of significance p=0.0056; Not reached
64 Selected grade 3/4 adverse events* Number of patients (%) Adverse event Any grade 3/4 adverse event Fatigue/asthenia/malaise Proteinuria Hypertension Hemorrhage Venous thromboembolism Gastrointestinal perforation Arterial ischemia *Based on safety population IFN + placebo (n=304) 137 (45) 46 (15) 0 (0) 2 (0.7) 1 (0.3) 2 (0.7) 0 (0) 1 (0.3) Bevacizumab + IFN (n=337) 203 (60( 60) 76 (23( 23) 22 (6.5( 6.5) 13 (3.9( 3.9) 11 (3.3( 3.3) 6 (1.8) 5 (1.5) 4 (1.2) 95
65 96 Side effect with IFN: dose reduction wo lost in efficacy? Clear relationship between IFN dose and toxicity Dose reduction is associated with a better quality of life In the Avoren Study: 40% pts 131/327 have a decrease in IFN in the Bevacizumab + IFN arm Maintenance of the same ORR?
66 100 Treatment Algorithm in mrcc mrcc first line treatment No more indication of IFN For young pts PS=0, one metastatic site, high CAIX : IL + IFN SUTENT for all the other indications TORICEL for modified Motzer prognosis group? AVASTIN + IFN mrcc second line treatment Nexavar If Nexavar first line: Sutent second line Prospective clinical trials: RAD001
67 101 Treatment Algorithm in mrcc Adjuvant therapy: high risk of relapse Ongoing clinical trials (S-TRAC, SORCE, ASSURE) Neoadjuvant therapy: non operable patients, treatment with sutent Surgery possible Indication of nephrectomy in metastatic situation?
68 S-TRAC: Sunitinib Phase III Trial in Adjuvant Renal Cancer Treatment Begin accrual in Europe High-risk patients according to UISS Staging System* N=236 Endpoint: DFS N E P H R E C T O M Y Stratify R A N D O M I S E Sunitinib 50 mg/day 4 weeks on/2 weeks off for 1 year Placebo for 1 year *T3 N0 or NX, M0, Fuhrman s grade 2, ECOG 1 or T4 N0 or NX, M0, any Fuhrman s grade, and any ECOG status or Any T, N1-2, M0, any Fuhrman s grade, and any ECOG status NCT Clinicaltrials.gov 102
69 ASSURE Phase III Trial: Adjuvant Sorafenib Sunitinib Unfavourable REnal Cell Carcinoma ECOG study; currently recruiting Non-metastatic RCC Disease stage II IV N=1,332 N E P H R E C T O M Y Stratify* R A N D O M I S E Sunitinib 50 mg/day 4 weeks on/2 weeks off Total = 9 cycles Sorafenib 400 mg twice daily for 6 weeks Total = 9 cycles Placebo twice daily for 6 weeks Total = 9 cycles Primary endpoint: DFS at 5 years Duration: 1 year *UISS (II V); Histologic subtype clear-cell/non-clear cell Biopsy at recurrence NCT Clinicaltrials.gov 103
70 SORCE Phase III Trial: SOrafenib in Patients with Resected Primary Renal CEll Carcinoma Patients with high and intermediate risk resected RCC Planned N=1,656 N E P H R E C T O M Y Stratify R A N D O M I S E Sorafenib 400 mg twice daily for 3 years (n=621) Sorafenib 400 mg twice daily for 1 year followed by placebo for 2 years (n=621) Placebo for 3 years (n=414) 1º end point: Disease-free survival 2º end points: RCC-specific survival time, toxicity, QOL and biomarkers Duration: 1 vs. 3 years NCT Clinicaltrials.gov 104
71 105 CARMENA TRIAL: Impact of the radical nephrectomy on the outcome in mrcc n=576 Metastatic RCC Biopsy, Clear Cell RCC R A N D O M I Z A T I O N 1:1 RN and then SUTENT 50 mg PO/J 4 S / 2 S SUTENT 50 mg PO/J 4 S / 2 S PI : Pr Arnaud Mejean
72 PREINSUT study: Sunitinib before and after nephrectomy in mrcc Eligibility criteria Clear cell carcinoma Operable tumor ECOG PS 0 or 1 Normal organic fonctions Mesurable metastases No brain met Tissu bank Exploratory Phase II, N =100 pts, 16 centers in France 2 cycles Sunitinib 50 mg/d (4 wk ON /2 wk OFF) Nephrectomy : week 12 After 2 wk of cicatrisation, Sunitinib 50 mg/j until progression or unacceptable toxicity Follow-up: 2 years Promotion: INCa/PHRC
73 107 Neoadjuvant strategy: T3N2M0 possibility of surgery after two cycles of Sutent Pre chir 1 Post Sutent 2 cycles Post chir 1 Post Sutent 5 cycles




74 107 Neoadjuvant strategy: T3N2M0 possibility of surgery after two cycles of Sutent Pre chir 1 Post Sutent 2 cycles Post chir 1 Post Sutent 5 cycles
75 108 Neoadjuvant strategy for patients with only one kidney left: possibility of conservative surgery after two cycles of Sutent Radical Nephrectomy Partial Nephrectomy
76 108 Neoadjuvant strategy for patients with only one kidney left: possibility of conservative surgery after two cycles of Sutent Radical Nephrectomy Sutent Partial Nephrectomy
77 108 Neoadjuvant strategy for patients with only one kidney left: possibility of conservative surgery after two cycles of Sutent Radical Nephrectomy Sutent Partial Nephrectomy
78 110 What is next? Sunitinib schedule regimen? Intermittent treatment or continuous How circumvent angiogenic-resistance? Targeted drugs + cytokines? Higher RR, higher toxicities, which dose intensity? Horizontal drug combinations? Inhibition of KDR, PDGFR and EGFR Vertical drug combinations? Inhibition of HIF, VEGF and KDR
79 111 Vertical Combinations: : Inhibition of VEGF at different levels HIF TOR Inhibiteur (CCI- 779) HSP-90 antagoniste (17-AAG) VEGF Bevacizumab, VEGF Trap KDR SU11248, BAY , AG
80 Horizontal Combinations: : Inhibition of VEGF at different levels β pvhl α HIF Bevacizumab, VEGF Trap VEGF PDGF TGFα KFR PDGFR EGFR SU11248, BAY , AG SU11248, BAY , AG Erlotinib, Gefitinib, CCI-779, BAY
81 113 Conclusions Mechanism-directed RCC therapy based on tumor-specific molecular feature is validated Sunitinib significantly improves RR and PFS versus IFN in first line setting Sorafenib significantly improves PFS versus placebo in second line setting Temsirolimus significantly improves PFS and survival versus IFN in modified poor risk population Bevacizumab and IFN significantly improves RR and PFS versus IFN in first line setting Sunitinib is the new standard reference for the first-line treatment of mrcc New drugs seem to be interesting (Axitinib( Axitinib, pazopamib,, etc ) There is a potential benefit of subsequent anti-angiogenic angiogenic therapies
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Targeted Therapy in Advanced Renal Cell Carcinoma
 Targeted Therapy in Advanced Renal Cell Carcinoma Brian I. Rini, M.D. Department of Solid Tumor Oncology Glickman Urologic and Kidney Institute Cleveland Clinic Taussig Cancer Institute Cleveland, Ohio
Targeted Therapy in Advanced Renal Cell Carcinoma Brian I. Rini, M.D. Department of Solid Tumor Oncology Glickman Urologic and Kidney Institute Cleveland Clinic Taussig Cancer Institute Cleveland, Ohio
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
David N. Robinson, MD
 David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
Angiogenesis Targeted Therapies in Renal Cell Carcinoma
 Angiogenesis Targeted Therapies in Renal Cell Carcinoma John S. Lam, MD Department of Urology David Geffen School of Medicine University of California-Los Angeles Patient Case CC: Abdominal pain VS: T
Angiogenesis Targeted Therapies in Renal Cell Carcinoma John S. Lam, MD Department of Urology David Geffen School of Medicine University of California-Los Angeles Patient Case CC: Abdominal pain VS: T
Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents
 in the Era of Targeted Agents") Conflict of Interest Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents None Patrick Medina, PharmD, BCOP Associate Professor University of Oklahoma OKC, OK Learning Objectives Epidemiology
Conflict of Interest Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents None Patrick Medina, PharmD, BCOP Associate Professor University of Oklahoma OKC, OK Learning Objectives Epidemiology
Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce
 in the elderly ( 65y): Position of a SIOG Taskforce") Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce Medical treatment of metastatic RCC in the elderly ( 65y): Members of the SIOG Taskforce
Medical treatment of metastatic renal cell carcinoma (mrcc) in the elderly ( 65y): Position of a SIOG Taskforce Medical treatment of metastatic RCC in the elderly ( 65y): Members of the SIOG Taskforce
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Medical Management of Renal Cell Carcinoma
 Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
Medical Management of Renal Cell Carcinoma Lin Mei, MD Hematology-Oncology Fellow Hematology, Oncology and Palliative Care Virginia Commonwealth University Educational Objectives Background of RCC (epidemiology,
A Review in the Treatment Options for Renal Cell Cancer
 A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
Targeted and immunotherapy in RCC
 Targeted and immunotherapy in RCC Treatment options Surgery (radical VS partial nephrectomy) Thermal ablation therapy Surveillance Immunotherapy Molecular targeted therapy Molecular targeted therapy Targeted
Targeted and immunotherapy in RCC Treatment options Surgery (radical VS partial nephrectomy) Thermal ablation therapy Surveillance Immunotherapy Molecular targeted therapy Molecular targeted therapy Targeted
New strategies and future of target therapy in advanced kidney cancer
 New strategies and future of target therapy in advanced kidney cancer VHL Gene Inactivation VHL Complex Disrupted VHL Protein HIF1-a, HIF2-a Accumulation VEGF PDGF TGF-α, CXCR4 Angiogenesis Endothelial
New strategies and future of target therapy in advanced kidney cancer VHL Gene Inactivation VHL Complex Disrupted VHL Protein HIF1-a, HIF2-a Accumulation VEGF PDGF TGF-α, CXCR4 Angiogenesis Endothelial
Metastatic Renal Cancer Medical Treatment
 Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Metastatic renal cancer (mrcc): Evidence-based treatment
: Evidence-based treatment") Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Sequential Therapy in Renal Cell Carcinoma*
 Sequential Therapy in Renal Cell Carcinoma* Bernard Escudier, MD, Marine Gross Goupil, MD, Christophe Massard, MD, and Karim Fizazi, MD, PhD Because of the recent approval of several drugs for the treatment
Sequential Therapy in Renal Cell Carcinoma* Bernard Escudier, MD, Marine Gross Goupil, MD, Christophe Massard, MD, and Karim Fizazi, MD, PhD Because of the recent approval of several drugs for the treatment
Dose individualization of sunitinib in mrcc: Toxicity-adjusted dose or Therapeutic drug monitoring
 Dose individualization of sunitinib in mrcc: Toxicity-adjusted dose or Therapeutic drug monitoring Alison Zhang 1, Peter Fox 1, Sally Coulter 4, Val Gebski 5, Bavanthi Balakrishnar 1, Christopher Liddle
Dose individualization of sunitinib in mrcc: Toxicity-adjusted dose or Therapeutic drug monitoring Alison Zhang 1, Peter Fox 1, Sally Coulter 4, Val Gebski 5, Bavanthi Balakrishnar 1, Christopher Liddle
Linee guida terapeutiche oncologiche. Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona
 Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Linee guida terapeutiche oncologiche Francesco Massari U.O.C. di Oncologia Medica d.u. Azienda Ospedaliera Universitaria Integrata Verona 1 YOUNG SPECIALIST RENAL CARE Verona, 07-08 Marzo 2014 Clinical
Renal Cell Cancer. Clinical case study 1 & 2. Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland
 Renal Cell Cancer Clinical case study 1 & 2 Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland 1 Case study 1 - RCC and Lung Metastases Case study 1: Patient History Male, 63 years old Mild
Renal Cell Cancer Clinical case study 1 & 2 Petri Bono MD PhD Helsinki University Hospital Helsinki, Finland 1 Case study 1 - RCC and Lung Metastases Case study 1: Patient History Male, 63 years old Mild
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA. Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA
 UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
Horizon Scanning Technology Briefing. Sutent (Sunitinib) for first-line and adjuvant treatment of renal cell carcinoma
 for first-line and adjuvant treatment of renal cell carcinoma") Horizon Scanning Technology Briefing National Horizon Scanning Centre Sutent (Sunitinib) for first-line and adjuvant treatment of renal cell carcinoma August 2006: Updated October 2006 This technology
Horizon Scanning Technology Briefing National Horizon Scanning Centre Sutent (Sunitinib) for first-line and adjuvant treatment of renal cell carcinoma August 2006: Updated October 2006 This technology
Prognostic Factors: Does It Really Matter if New Drugs for Targeted Therapy Will Be Used?
 european urology supplements 8 (2009) 478 482 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prognostic Factors: Does It Really Matter if New Drugs for Targeted Therapy Will
european urology supplements 8 (2009) 478 482 available at www.sciencedirect.com journal homepage: www.europeanurology.com Prognostic Factors: Does It Really Matter if New Drugs for Targeted Therapy Will
REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO
 REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO Alain Ravaud, MD.PhD Bordeaux. France DISCLOSURES Consultant for: Pfizer, Novartis, GlaxoSmithKline, Roche, Bristol-Myers Squibb Institutional
REAL WORLD PRACTICE: ADJUVANT THERAPY READY FOR PRIME TIME? PRO Alain Ravaud, MD.PhD Bordeaux. France DISCLOSURES Consultant for: Pfizer, Novartis, GlaxoSmithKline, Roche, Bristol-Myers Squibb Institutional
Treatment Algorithm and Therapy Management in mrcc. Manuela Schmidinger Medical University of Vienna Austria
 Treatment Algorithm and Therapy Management in mrcc Manuela Schmidinger Medical University of Vienna Austria A Paradigm Shift in the Treatment of mrcc 1. Sunitinib 2. Sorafenib 3. Bevacizumab+IFN-alpha
Treatment Algorithm and Therapy Management in mrcc Manuela Schmidinger Medical University of Vienna Austria A Paradigm Shift in the Treatment of mrcc 1. Sunitinib 2. Sorafenib 3. Bevacizumab+IFN-alpha
Angiogenesis and tumor growth
 Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
Tratamiento adyuvante y neoadyuvante del cáncer renal en Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet.
 Tratamiento adyuvante y neoadyuvante del cáncer renal en 2017 Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet. Barcelona Pronóstico del CR mediante un sistema integrado en 468 pts
Tratamiento adyuvante y neoadyuvante del cáncer renal en 2017 Xavier Garcia del Muro Solans Institut Català d Oncologia Hospitalet. Barcelona Pronóstico del CR mediante un sistema integrado en 468 pts
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game?
 Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Sequencing of therapies in mrcc. Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC
 Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
Sequencing of therapies in mrcc Ari Hakimi MD Assistant Professor Urology Service, Department of Surgery MSKCC Old Paradigm Sequencing approved agents VEGF TKI Sunitinib Pazopanib Axitinib TKI TKI MTORi
CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY FOR THE RIGHT PATIENT
 Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
The Therapeutic Landscape in Advanced Renal Cell Carcinoma
 The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
The Therapeutic Landscape in Advanced Renal Cell Carcinoma Cora Sternberg, MD, FACP Chairman, Department of Medical Oncology San Camillo-Forlanini Hospital Rome, Italy What best describes the change in
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
I Kid(ney) You Not: Updates on Renal Cell Carcinoma
 You Not: Updates on Renal Cell Carcinoma") Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Disclosures I Kid(ney) You Not: Updates on Renal Cell Carcinoma Nothing to disclose Renee McAlister, PharmD, BCOP Clinical Pharmacist, GU/Melanoma Vanderbilt Ingram Cancer Center September 29, 2018 Objectives
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? VEGF Is the Only Angiogenic Factor Present Throughout the Tumor Life Cycle
 Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Innovaciones en el tratamiento del ca ncer renal. Enrique Grande
 Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Current Status of Studies on Targeted Therapy for Renal Cell Carcinoma
 294 Chin J Clin Oncol (2008) 5: 294~298 DOI 10.1007/s11805-008-0294-x Current Status of Studies on Targeted Therapy for Renal Cell Carcinoma Shaoqi Wang 1 Shaoxiang Wang 2 Juan Wang 1 1 Department of Oncology,
294 Chin J Clin Oncol (2008) 5: 294~298 DOI 10.1007/s11805-008-0294-x Current Status of Studies on Targeted Therapy for Renal Cell Carcinoma Shaoqi Wang 1 Shaoxiang Wang 2 Juan Wang 1 1 Department of Oncology,
pan-canadian Oncology Drug Review Final Clinical Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013
 for metastatic Renal Cell Carcinoma March 7, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Axitinib (Inlyta) for metastatic Renal Cell Carcinoma March 7, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients
 Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Cytoreductive Nephrectomy
 Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Positioning Antiangiogenesis Drugs and Other Agents in Renal Cell Cancer Treatment
 Positioning Antiangiogenesis Drugs and Other Agents in Renal Cell Cancer Treatment Ahmad Awada, MD, PhD Medical Oncology Clinic Institut Jules Bordet Université Libre de Bruxelles (U.L.B.) Brussels, Belgium
Positioning Antiangiogenesis Drugs and Other Agents in Renal Cell Cancer Treatment Ahmad Awada, MD, PhD Medical Oncology Clinic Institut Jules Bordet Université Libre de Bruxelles (U.L.B.) Brussels, Belgium
Sergio Bracarda MD. Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy
 San Donato Hospital Arezzo, Italy") Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea
 Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care
 vs standard of care") A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care Martin H. Voss 1, Thomas Hutson 2, Arif Hussain 3, Ulka
A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care Martin H. Voss 1, Thomas Hutson 2, Arif Hussain 3, Ulka
Nursing s Role in the Management of New Oral Chemotherapy Agents
 Nursing s Role in the Management of New Oral Chemotherapy Agents Mechelle Barrick BSN, RN, OCN, CCRP Clinical Research Nurse Coordinator Greater Baltimore Medical Center mbarrick@gbmc.org THE NURSES ROLE
Nursing s Role in the Management of New Oral Chemotherapy Agents Mechelle Barrick BSN, RN, OCN, CCRP Clinical Research Nurse Coordinator Greater Baltimore Medical Center mbarrick@gbmc.org THE NURSES ROLE
Efficacy and Toxicity of Sunitinib in Metastatic Renal Cell Carcinoma Patients in Egypt
 DOI:http://dx.doi.org/10.7314/APJCP.2015.16.5.1971 Efficacy and Toxicity of Sunitinib in Egyptian Patients with Metastatic Renal Cell Carcinoma RESEARCH ARTICLE Efficacy and Toxicity of Sunitinib in Metastatic
DOI:http://dx.doi.org/10.7314/APJCP.2015.16.5.1971 Efficacy and Toxicity of Sunitinib in Egyptian Patients with Metastatic Renal Cell Carcinoma RESEARCH ARTICLE Efficacy and Toxicity of Sunitinib in Metastatic
E2804 The BeST Trial
 E2804 The BeST Trial A randomized Phase II Study of VEGF, RAF Kinase and MTOR Combination Targeted Therapy with Bevacizumab, Sorafenib and Temsirolimus in Advanced Renal Cell Carcinoma Investigators Keith
E2804 The BeST Trial A randomized Phase II Study of VEGF, RAF Kinase and MTOR Combination Targeted Therapy with Bevacizumab, Sorafenib and Temsirolimus in Advanced Renal Cell Carcinoma Investigators Keith
Invented name/name: Avastin International non-proprietary name/common name: bevacizumab TYPE II VARIATION: EMEA/H/C/000582/II/0015
 Invented name/name: Avastin International non-proprietary name/common name: bevacizumab TYPE II VARIATION: EMEA/H/C/000582/II/0015 Extension of indication to include: Avastin in combination with interferon
Invented name/name: Avastin International non-proprietary name/common name: bevacizumab TYPE II VARIATION: EMEA/H/C/000582/II/0015 Extension of indication to include: Avastin in combination with interferon
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Multidisciplinary approach for renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 20 April, Antalya, Turkey RCC European Union 60.000 new diagnoses/year 26.000 Cancer related deaths
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015
 Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
Emerging Biomarkers of VEGF and mtor Inhibitors in 2015 Laurence Albiges Institut Gustave Roussy, France Fourteenth International Kidney Cancer Symposium Miami, Florida, USA November 6-7, 2015 www.kidneycancersymposium.com
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma
 for Metastatic Renal Cell Carcinoma") pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
What can we expect from running phase III trials: will all of them alter the current treatment algorithm?
 What can we expect from running phase III trials: will all of them alter the current treatment algorithm? 8 th European International Kidney Cancer Symposium Budapest, May 2013 Martin Gore PhD FRCP Royal
What can we expect from running phase III trials: will all of them alter the current treatment algorithm? 8 th European International Kidney Cancer Symposium Budapest, May 2013 Martin Gore PhD FRCP Royal
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Final appraisal determination Bevacizumab (first-line), sorafenib (first- and second-line),
, sorafenib (first- and second-line),") NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Final appraisal determination Bevacizumab (first-line), sorafenib (first- and secondline), sunitinib (second-line) and temsirolimus (firstline) for
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Final appraisal determination Bevacizumab (first-line), sorafenib (first- and secondline), sunitinib (second-line) and temsirolimus (firstline) for
Renal Cell Carcinoma: Status of Medical and Surgical Therapy. Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation
 Renal Cell Carcinoma: Status of Medical and Surgical Therapy Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation Metastatic Renal Cell Carcinoma: Evolution of Current Therapeutic Approaches
Renal Cell Carcinoma: Status of Medical and Surgical Therapy Ronald M. Bukowski Emeritus Physician Cleveland Clinic Foundation Metastatic Renal Cell Carcinoma: Evolution of Current Therapeutic Approaches
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Integrating novel therapy in advanced renal cell carcinoma
 Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
Integrating novel therapy in advanced renal cell carcinoma Tian Zhang, MD Assistant Professor of Medicine GU Oncology Duke Cancer Institute March 11, 2017 Disclosures Research Funding Janssen Pfizer Consultant
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Second - Line Debate: Axitinib
 Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
Renal Cell Cancer: Present and Future. Bernard Escudier, Gustave Roussy
 Renal Cell Cancer: Present and Future Bernard Escudier, Gustave Roussy [HKIOF May 2017] Sponsored by Bristol- Myers Squibb OPDIVO Hong Kong prescribing information is available upon request Disclosures
Renal Cell Cancer: Present and Future Bernard Escudier, Gustave Roussy [HKIOF May 2017] Sponsored by Bristol- Myers Squibb OPDIVO Hong Kong prescribing information is available upon request Disclosures
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
The Use of Inhibitors of Angiogenesis in Patients with Inoperable Locally Advanced or Metastatic Renal Cell Cancer: Guideline Recommendations
 Evidence-Based Series #3-8-4: Section 1 The Use of Inhibitors of Angiogenesis in Patients with Inoperable Locally Advanced or Metastatic Renal Cell Cancer: Guideline Recommendations S. Hotte, T. Waldron,
Evidence-Based Series #3-8-4: Section 1 The Use of Inhibitors of Angiogenesis in Patients with Inoperable Locally Advanced or Metastatic Renal Cell Cancer: Guideline Recommendations S. Hotte, T. Waldron,
Cancer Cell Research 14 (2017)
") Available at http:// www.cancercellresearch.org ISSN 2161-2609 Efficacy and safety of bevacizumab for patients with advanced non-small cell lung cancer Ping Xu, Hongmei Li*, Xiaoyan Zhang Department of
Available at http:// www.cancercellresearch.org ISSN 2161-2609 Efficacy and safety of bevacizumab for patients with advanced non-small cell lung cancer Ping Xu, Hongmei Li*, Xiaoyan Zhang Department of
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016
 for Metastatic Renal Cell Carcinoma September 1, 2016") pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Metastatic Renal Cell Carcinoma September 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report
Scottish Medicines Consortium
 Scottish Medicines Consortium sorafenib 200mg tablets (Nexavar ) (No. 321/06) Bayer Plc 6 October 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
Scottish Medicines Consortium sorafenib 200mg tablets (Nexavar ) (No. 321/06) Bayer Plc 6 October 2006 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and advises
CLINICAL POLICY Department: Medical Management Document Name: Inlyta Reference Number: NH.PHAR.100 Effective Date: 05/12
 Page: 1 of 5 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
Page: 1 of 5 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
10/15/2012. Overcoming Endocrine Therapy Resistance. The Problem in ER+ Tumors is Endocrine Therapy Resistance
 Overcoming Endocrine Therapy Resistance Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Slide Credits: Hope Rugo, MD The Problem in ER+ Tumors is Endocrine Therapy Resistance
Overcoming Endocrine Therapy Resistance Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Slide Credits: Hope Rugo, MD The Problem in ER+ Tumors is Endocrine Therapy Resistance
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
ADVISORY COMMITTEE BRIEFING MATERIALS: AVAILABLE FOR PUBLIC RELEASE
 Tivozanib Hydrochloride in Advanced Renal Cell Carcinoma ADVISORY COMMITTEE BRIEFING MATERIALS: AVAILABLE FOR PUBLIC RELEASE AVEO PHARMACEUTICALS, INC. 75 Sidney Street Cambridge, MA 02139 Tel: (617) 299-5000
Tivozanib Hydrochloride in Advanced Renal Cell Carcinoma ADVISORY COMMITTEE BRIEFING MATERIALS: AVAILABLE FOR PUBLIC RELEASE AVEO PHARMACEUTICALS, INC. 75 Sidney Street Cambridge, MA 02139 Tel: (617) 299-5000
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Clinical Biomarker in Kidney Cancer. Maria Nirvana Formiga, M.D., Ph.D.
 Clinical Biomarker in Kidney Cancer Maria Nirvana Formiga, M.D., Ph.D. Disclosures I am on the Speaker s Bureau with Pfizer and Bayer Clinical trials of BMS and Pfizer Kidney Cancer 70% new cases in developed
Clinical Biomarker in Kidney Cancer Maria Nirvana Formiga, M.D., Ph.D. Disclosures I am on the Speaker s Bureau with Pfizer and Bayer Clinical trials of BMS and Pfizer Kidney Cancer 70% new cases in developed
PFIZER INC. THERAPEUTIC AREA AND FDA APPROVED INDICATIONS: See USPI
 PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
PFIZER INC. These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert. For publications based on this study, see associated bibliography.
Phase II Cancer Trials: When and How
 Phase II Cancer Trials: When and How Course for New Investigators August 9-12, 2011 Learning Objectives At the end of the session the participant should be able to Define the objectives of screening vs.
Phase II Cancer Trials: When and How Course for New Investigators August 9-12, 2011 Learning Objectives At the end of the session the participant should be able to Define the objectives of screening vs.
NEXT GENERATION DRUGS IN KIDNEY CANCER. Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden
 NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
Reference No: Author(s) Approval date: June Committee. Operational Date: July Review:
 Approval date: June Committee. Operational Date: July Review:") Reference No: Title: Author(s) Systemic anti-cancer therapy (SACT) guidelines for renal cell cancer Dr Alison Clayton Consultant Medical Oncologist & Dr Jane Hurwitz Consultant Medical Oncologist, Cancer
Reference No: Title: Author(s) Systemic anti-cancer therapy (SACT) guidelines for renal cell cancer Dr Alison Clayton Consultant Medical Oncologist & Dr Jane Hurwitz Consultant Medical Oncologist, Cancer
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Long Term Results in GIST Treatment
 Long Term Results in GIST Treatment Dr. Laurentia Gales Prof. Dr. Rodica Anghel, Dr. Xenia Bacinschi Institute of Oncology Prof Dr Al Trestioreanu Bucharest 25 th RSRMO October 15-17 Sibiu Background Gastrointestinal
Long Term Results in GIST Treatment Dr. Laurentia Gales Prof. Dr. Rodica Anghel, Dr. Xenia Bacinschi Institute of Oncology Prof Dr Al Trestioreanu Bucharest 25 th RSRMO October 15-17 Sibiu Background Gastrointestinal
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Malignant pleural Mesothelioma: A Year In Review
 Malignant pleural Mesothelioma: A Year In Review Rabab Gaafar,MD Prof. Medical Oncology NCI Cairo University National Cancer Institute Conference 2015 ASCO news in Mesothelioma Introduction ASCO news second
Malignant pleural Mesothelioma: A Year In Review Rabab Gaafar,MD Prof. Medical Oncology NCI Cairo University National Cancer Institute Conference 2015 ASCO news in Mesothelioma Introduction ASCO news second
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer
 Non-Small Cell Lung Cancer") Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Atezolizumab Adjuvant Study: Medical Oncologist Perspective. Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center
 Atezolizumab Adjuvant Study: Medical Oncologist Perspective Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center Trial overview Key issues Outline Challenges with neoadjuvant therapy Placebo control
Atezolizumab Adjuvant Study: Medical Oncologist Perspective Sumanta K. Pal, MD City of Hope Comprehensive Cancer Center Trial overview Key issues Outline Challenges with neoadjuvant therapy Placebo control
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
Axitinib in renal cell carcinoma: now what do we do?
 Renal Cell Carcinoma Axitinib in renal cell carcinoma: now what do we do? Ian D. Davis Monash University Eastern Health Clinical School, Level 2, Box Hill, Victoria 3128, Australia Correspondence to: Ian
Renal Cell Carcinoma Axitinib in renal cell carcinoma: now what do we do? Ian D. Davis Monash University Eastern Health Clinical School, Level 2, Box Hill, Victoria 3128, Australia Correspondence to: Ian
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Characterization of Patients with Poor-
 Characterization of Patients with Poor- Risk Metastatic Renal Cell Carcinoma Hamieh L 1 *, McKay RR 1 *, Lin X 2, Simantov R 2, Choueiri TK 1 *Equal contributions 1 Dana-Farber Cancer Institute, Boston,
Characterization of Patients with Poor- Risk Metastatic Renal Cell Carcinoma Hamieh L 1 *, McKay RR 1 *, Lin X 2, Simantov R 2, Choueiri TK 1 *Equal contributions 1 Dana-Farber Cancer Institute, Boston,
Therapeutic effects and associated adverse events of multikinase inhibitors in metastatic renal cell carcinoma: A meta-analysis
 EXPERIMENTAL AND THERAPEUTIC MEDICINE 9: 2275-2280, 2015 Therapeutic effects and associated adverse events of multikinase inhibitors in metastatic renal cell carcinoma: A meta-analysis QINXIANG TAN 1*,
EXPERIMENTAL AND THERAPEUTIC MEDICINE 9: 2275-2280, 2015 Therapeutic effects and associated adverse events of multikinase inhibitors in metastatic renal cell carcinoma: A meta-analysis QINXIANG TAN 1*,
Synopsis. Study Phase and Title: Study Objectives: Overall Study Design
 Synopsis Study Phase and Title: Study Objectives: Overall Study Design Phase III randomized sequential open-label study to evaluate the efficacy and safety of sorafenib followed by pazopanib versus pazopanib
Synopsis Study Phase and Title: Study Objectives: Overall Study Design Phase III randomized sequential open-label study to evaluate the efficacy and safety of sorafenib followed by pazopanib versus pazopanib
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Phase II Cancer Trials: When and How
 Phase II Cancer Trials: When and How Course for New Investigators August 21-23, 2013 Acknowledgment Elizabeth Eisenhauer for some slides! Learning Objectives At the end of the session the participant should
Phase II Cancer Trials: When and How Course for New Investigators August 21-23, 2013 Acknowledgment Elizabeth Eisenhauer for some slides! Learning Objectives At the end of the session the participant should
Current experience in immunotherapy for metastatic renal cell carcinoma
 Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
METRIC Study Key Eligibility Criteria
 The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).