Intravesical Therapy for Bladder Cancer
|
|
|
- Janis Horton
- 5 years ago
- Views:
Transcription
, University of Toronto Director, Uro-Oncology, Mount Sinai Hospital Director, Uro-Oncology Fellowship Program,")
1 Intravesical Therapy for Bladder Cancer Alexandre R. Zlotta, MD, PhD, FRCSC Professor, Department of Surgery (Urology), University of Toronto Director, Uro-Oncology, Mount Sinai Hospital Director, Uro-Oncology Fellowship Program, University of Toronto Staff, Division of Surgical Oncology, Princess Margaret Hospital, University Health Network Toronto, Ontario
2 Key Learning Objectives By participating in this session, health care professionals will: Learn about the recent advances in intravesical therapy for non-muscle invasive bladder cancer Examine new data regarding differences in BCG strains, EMDA for BCG failures, imaging of residual disease and new predictive markers and risk stratification including histological variants


3 Intravesical Therapy for Bladder Cancer Alexandre R Zlotta, MD PhD FRCSC Professor, University of Toronto, Toronto, Ontario, Canada Mount Sinai and Princess Margaret Hospitals, University Health Network
4 Disclosures Advisor, grants Sanofi-Aventis Sanofi-Pasteur Amgen Astellas- CUA grants

5 BCG works but there are BCG failures!!!! Recurrence rates: 33-74% Progression rates: 7-49% Toronto experience: 1/3 recurrence without progression, 1/3 no rec no progression, 1/3 progression

6 A prospective randomized single-institution trial with treatment of 142 high-risk NMIBC patients with BCG Connaught or Tice

7 Patients and BC characteristics
8 Recurrence-free survival Progression-free survival
9 CONCLUSIONS Treatment with BCG Connaught prevented recurrences more efficiently than BCG Tice. Comparison of the immunogenicity of the two strains in mice indicated superior immunogenicity of BCG Connaught.


10 Can we identify the cats from the lions?
11
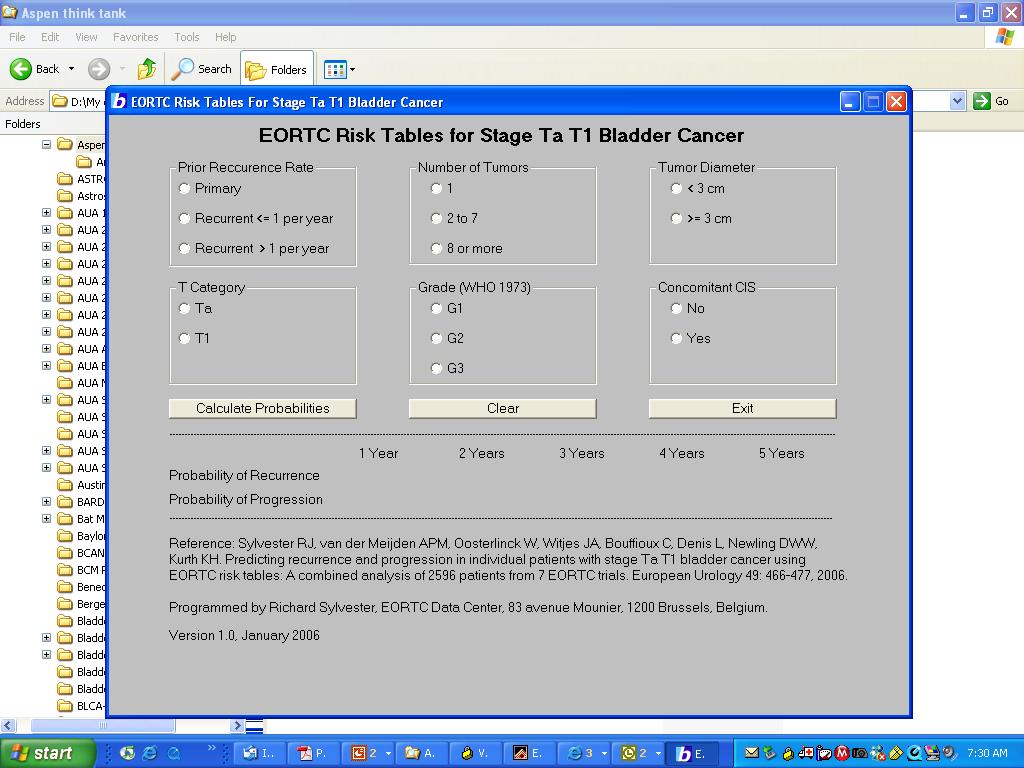
12 Results of multivariate analysis Most Important Prognostic Factors Recurrence Progression Nb of tumors Carcinoma in situ Prior rec rate Grade Tumor size T category (Sylvester et al, 2006)
")
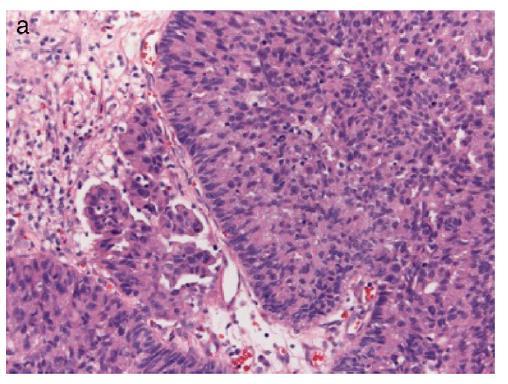
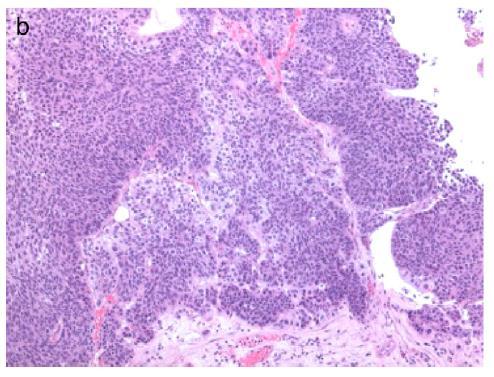
13 T1m (minimal) T1e (extensive) pt1e: Invasion > 0.5 mm

14 New substaging New substaging T1a,b,c substaging T1a,b,c substaging
:")
15 J Urol 2013; 189 (6):
16

17 Uni and multivariable analyses bladder cancer specific survival
18 RESULTS AND MESSAGE Progression rates at 10 yr ranged from 17% to 52%. Most important prognostic factors for progression: age, tumor size, and concomitant CIS Most important prognostic factors for BCa-specific survival and OS: age and tumor size. T1G3 patients 70 yr with tumors 3 cm and concomitant CIS should be treated more aggressively because of the high risk of progression
19 Clinical Outcomes of ct1 Micropapillary Bladder Cancer Willis et al, MD Anderson J Urol patients with micropapillary bladder cancer, including 72 staged with ct1n0m0 40 received primary intravesical BCG 26 underwent up-front radical cystectomy Of patients who received BCG 75%, 45% and 35% experienced disease recurrence, progression and lymph node metastasis, respectively!!!!! 5 year survival BCG: 60% 5 year survival cystectomy: 100% 5 year survival delayed cyst after recurrence: 60% 5 year survival delayed cyst after progression: 24%
20

21 Intravesical chemotherapy The Renaissance
22 The International Bladder Cancer Group emphasizes the importance of distinguishing recurrence from treatment failure Recurrence refers to reappearance of disease (any grade, T category, or CIS) after completion of therapy Treatment failure is defined as any recurrence or progression that occurs during intravesical therapy.
23 Intravesical Gemcitabine Author Dalbagni Dalbagni Bartoletti Mohanty Di Lorenzo Addeo Treatment modality IV Gemcitabine IV Gemcitabine IV Gemcitabine IV Gemcitabine IV Gemcitabine IV Gemcitabine n= n=high risk n='failure s' F/U (mo) (0-35) weeks (6-22) Efficacy and Comment 50% CR with a 1 year RFS of 21%. 37% needed a cystectomy Phase I stage of above study with 7/18 (39%) CR Recurrence in 32.5% of BCG failures vs. 21% BCG naïve group 43.7% of high risk failures developed recurrence vs. 25% of intermediate risk failures 60% CR. 3 patients (8.75%) progressed (all G3pT1 previously) Recurrence and 2-yr DFS better for GC vs BCG (p=0.002 and p<0.008, respectively) Recurrence free 72% GC vs. 61% MMC. DFS in favour of GC (p=0.0021)
24
25
26 Overall Survival Cancer Specific Survival
27 Intravesical Docetaxel/Paclitaxel/ BCG interferon Author Treatment modality n= n=high risk N=failures F/U (mo) McKiernan IV Docetaxel weeks Laudano IV Docetaxel Barlow IV Docetaxel Bassi IV Paclitaxel week McKiernan IV Paclitaxel weeks Joudi BCG + Interferon-α Efficacy and Comment Phase I study with a mean of 3 previous courses BCG. 56% CR but only 22% durability Long term follow-up of McKiernan [24]. 61% failed treatment. Median DFS 13.3 months Maintenance regime with 10/13 (77%) CR and 6 (46%) disease free at end of follow-up Phase I tolerability study. Nine (60%) patientshad no CIS on post treatment biopsy Only 28% (n=5 )had no evidence of disease at 6 week post treatment evaluation Of BCG failure group, 45% disease free vs. 59% BCG
 or had tumor recurrence after prior BCG (BCG-F), Joudi et al, 2006")
28 Recurrence rates in patients receiving intravesical BCG and IFN characterized by whether they never received BCG (BCG-N) or had tumor recurrence after prior BCG (BCG-F), Joudi et al, 2006
29 Thermochemotherapy/phototherapy Author Treatment modality n= N high risk N 'failures' F/U (mo) Efficacy and Comment Witjes Thermochemot herapy % CR and 51% disease free after mean 27mo f/u Nativ Thermochemot herapy (2-74) Overall DFS 85% and 56% after 1 and 2 years but decreased efficacy if no maintenance Halachmi Waidelich Berger Breyer Thermochemot herapy Photodynamic therapy Photodynamic therapy MMC + Gemcitabine (2-49) 36 (12-51) 23.7 (1-73) KM estimated probability of recurrence 50.7% at 2-yrs for BCG failure cohort vs 42.9% 3/5 CIS patients and 4/19 with papillary tumours disease free In BCG failure group, 4/10 (40%) recurrence free with mean f/u 11.8 months % CR

30 More than 80% of pts previously treated with BCG Almost half of all those who received CHT showed no evidence of disease at 2 years

31
32 Device assisted instillations: EMDA (di Stasi Lancet Oncol 2006)
33 Methods 81 mg BCG infused over 120 min once a week for 2 weeks, followed by 40 mg electromotive mitomycin (intravesical electric current 20 ma for 30 min) once a week as one cycle for three cycles (n=107) Maintenance in the combo arm: 40 mg electromotive mitomycin once a month for 2 months, followed by 81 mg BCG once a month as one cycle for three cycles
34 OVERALL TREATMENT EFFICACY Recurrence BCG alone (n=105) BCG/MMC (n=107) P value Patients (%) 61/105 (58.1) 45/107 (42.1) Median disease- mos (CI) 21 (15-54) 69 (55-86) Progression to muscle invasive disease Patients (%) 23/105 (21.9) 10/107 (9.4) Median time to progr. (CI) 16.0 ( ) 37.5 ( ) Mortality Death from any cause (%) 34/105 (32.4) 23/107 (21.5) Death from bladder ca (%) 17/105 (16.2) 6/107 (5.6)
35
36 BACKGROUND In July 2012: Sanofi Pasteur announced it was halting production of ImmuCyst, BCG Connaught strain after inspectors found mould in the sterile manufacturing area of the Toronto plant following a flood. The Toronto facility was the only one in the world manufacturing ImmuCyst, the market leader in many countries including the UK, US and Canada This halt led to a severe worldwide shortage of BCG as other manufacturers struggled to keep up with demand.
37 Multiple simultaneous problems! Although the problem appeared to be improving slowly MSD, OncoTICE manufacturer announced that it expected severely reduced OncoTICE supplies throughout 2015 due to a combination of increased demand and a manufacturing issue. Sanofi Pasteur indicated that ImmuCyst should be available from the second quarter of Production of the RIVM BCG strain by Medac (Germany) has been on hold for some time during the fourth quarter of 2014
38 Clinical recommendations 1. BCG maintenance can be stopped after 1 yr- Patients in years 2 and 3 of maintenance without CIS can be reassured that this option is safe in terms of progression although there is a slightly higher risk of recurrence 2. Patients with CIS could be offered a reduced dose of BCG for years 2 and if possible, patients should be offered a one-third dose of BCG for induction and maintenance courses up to 1 yr. Based on a randomised EORTC trial which showed no difference in progression rates between fulldose and one-third dose BCG. Recurrence rates, however, will be higher.
39 4. if administering one-third dose BCG is not possible for practical reasons Induction course of MMC that should be followed by maintenance Optimal MMC maintenance regimen unknown, but following confirmation of response at cystoscopy, monthly instillation from months 3 12 would be a pragmatic option.s
40 5. patients should not be offered only a single BCG instillation instead of three instillations for each BCG maintenance cycle because this has been shown to be less effective
41 6. in circumstances in which BCG supplies have run out or are insufficient to allow reduced doses Patients with lowest risk high-risk NMIBC (HG Ta) can be offered an induction course of MMC followed by maintenance High-risk NMIBC patients with T1 or CI should be offered intravesical chemotherapy using DAT with thermotherapy- DISCUSSION EMDA in Canada? If already failed MMC or no access, gemcitabine 2000 mg in 50 ml once a week for 6 wk. In case of local toxicity, dose reduced to 1000 mg in 50 ml.
Management options for high-risk, BCG-refractory NMIBC. Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center
 Management options for high-risk, BCG-refractory NMIBC Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center Bladder Cancer in U.S. 4 th most common cancer in men 9 th
Management options for high-risk, BCG-refractory NMIBC Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center Bladder Cancer in U.S. 4 th most common cancer in men 9 th
Non Muscle Invasive Bladder Cancer. Primary and Recurrent TCC 4/10/2010. Two major consequences: Strategies: High-Risk NMI TCC
 Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Controversies in the management of Non-muscle invasive bladder cancer
 Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Issues in the Management of High Risk Superficial Bladder Cancer
 Issues in the Management of High Risk Superficial Bladder Cancer MICHAEL A.S. JEWETT DIVISION OF UROLOGY, DEPARTMENT OF SURGICAL ONCOLOGY, PRINCESS MARGARET HOSPITAL & THE UNIVERSITY OF TORONTO 1 Carcinoma
Issues in the Management of High Risk Superficial Bladder Cancer MICHAEL A.S. JEWETT DIVISION OF UROLOGY, DEPARTMENT OF SURGICAL ONCOLOGY, PRINCESS MARGARET HOSPITAL & THE UNIVERSITY OF TORONTO 1 Carcinoma
Reviewing Immunotherapy for Bladder Carcinoma In Situ
 Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience. Paul Gellhaus Assistant Clinical Professor
 Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience Paul Gellhaus Assistant Clinical Professor Iowa??? none Disclosures Caveats Dr. Michael O Donnell
Non-Muscle Invasive Bladder Cancer BCG Failures: University of Iowa Hospitals and Clinics Experience Paul Gellhaus Assistant Clinical Professor Iowa??? none Disclosures Caveats Dr. Michael O Donnell
Risk Adapted Treatment of Non-muscle Invasive Bladder Cancer. Eila C. Skinner, MD
 Risk Adapted Treatment of Non-muscle Invasive Bladder Cancer Eila C. Skinner, MD Professor, Department of Urology Stanford University SWIU Winter Meeting January, 2015 Goals Minimize treatment for patients
Risk Adapted Treatment of Non-muscle Invasive Bladder Cancer Eila C. Skinner, MD Professor, Department of Urology Stanford University SWIU Winter Meeting January, 2015 Goals Minimize treatment for patients
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D.
 Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
CUA guidelines on the management of non-muscle invasive bladder cancer
 Original cua guidelines research CUA guidelines on the management of non-muscle invasive bladder cancer Wassim Kassouf, MD, CM, FRCSC; * Samer L. Traboulsi, MD; * Girish S. Kulkarni, MD, FRCSC; Rodney
Original cua guidelines research CUA guidelines on the management of non-muscle invasive bladder cancer Wassim Kassouf, MD, CM, FRCSC; * Samer L. Traboulsi, MD; * Girish S. Kulkarni, MD, FRCSC; Rodney
Novel therapeutic strategies for NMIBC. Peter Black Vancouver Prostate Centre University of British Columbia
 Novel therapeutic strategies for NMIBC Peter Black Vancouver Prostate Centre University of British Columbia Financial and Other Disclosures I have the following financial interests or relationships to
Novel therapeutic strategies for NMIBC Peter Black Vancouver Prostate Centre University of British Columbia Financial and Other Disclosures I have the following financial interests or relationships to
BCG Unresponsive Disease A Roadmap for Drug Development and Integra;on of Novel Therapies
 BCG Unresponsive Disease A Roadmap for Drug Development and Integra;on of Novel Therapies Seth P. Lerner, MD, FACS Professor of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College of
BCG Unresponsive Disease A Roadmap for Drug Development and Integra;on of Novel Therapies Seth P. Lerner, MD, FACS Professor of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College of
BCG Failure or BCG Unresponsive: Defining and Managing Difficult Patients
 BCG Failure or BCG Unresponsive: Defining and Managing Difficult Patients Michael S. Cookson, MD, Professor and Chair Department of Urology University of Oklahoma Non-muscle Invasive Bladder Cancer Bladder
BCG Failure or BCG Unresponsive: Defining and Managing Difficult Patients Michael S. Cookson, MD, Professor and Chair Department of Urology University of Oklahoma Non-muscle Invasive Bladder Cancer Bladder
The Role of Bacillus Calmette-Guérin in the Treatment of Non Muscle-Invasive Bladder Cancer
 EUROPEAN UROLOGY 57 (2010) 410 429 available at www.sciencedirect.com journal homepage: www.europeanurology.com Collaborative Review Bladder Cancer The Role of Bacillus Calmette-Guérin in the Treatment
EUROPEAN UROLOGY 57 (2010) 410 429 available at www.sciencedirect.com journal homepage: www.europeanurology.com Collaborative Review Bladder Cancer The Role of Bacillus Calmette-Guérin in the Treatment
Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer
 Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer Andrew J. Stephenson, MD, FRCSC, FACS Director, Urologic Oncology Associate Professor of Surgery Glickman Urological and Kidney
Neoadjuvant vs. Adjuvant Chemotherapy for Muscle-Invasive Bladder Cancer Andrew J. Stephenson, MD, FRCSC, FACS Director, Urologic Oncology Associate Professor of Surgery Glickman Urological and Kidney
Intravesical gemcitabine in combination with mitomycin C as salvage treatment in recurrent non-muscle-invasive bladder cancer
 Intravesical gemcitabine in combination with mitomycin C as salvage treatment in recurrent non-muscle-invasive bladder cancer Patrick A. Cockerill, John J. Knoedler, Igor Frank, Robert Tarrell and Robert
Intravesical gemcitabine in combination with mitomycin C as salvage treatment in recurrent non-muscle-invasive bladder cancer Patrick A. Cockerill, John J. Knoedler, Igor Frank, Robert Tarrell and Robert
Contemporary management of high-grade T1 bladder cancer Arnulf Stenzl
 Contemporary management of high-grade T1 bladder cancer Arnulf Stenzl Dep. of Urology, Eberhard-Karls University, Tuebingen, Germany Treatment options in HG T1 BCa TUR-BT Primary and second resection (T0-status)
Contemporary management of high-grade T1 bladder cancer Arnulf Stenzl Dep. of Urology, Eberhard-Karls University, Tuebingen, Germany Treatment options in HG T1 BCa TUR-BT Primary and second resection (T0-status)
Management of High-Risk Non-Muscle Invasive Bladder Cancer. Seth P. Lerner, MD, FACS
 Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
CUA guidelines on the management of non-muscle invasive bladder cancer
 Original cua guidelines research CUA guidelines on the management of non-muscle invasive bladder cancer Wassim Kassouf, MD, CM, FRCSC; * Samer L. Traboulsi, MD; * Girish S. Kulkarni, MD, FRCSC; Rodney
Original cua guidelines research CUA guidelines on the management of non-muscle invasive bladder cancer Wassim Kassouf, MD, CM, FRCSC; * Samer L. Traboulsi, MD; * Girish S. Kulkarni, MD, FRCSC; Rodney
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
BCG Unresponsive NMIBC: What s Available?
 BCG Unresponsive NMIBC: What s Available? Michael S. Cookson, MD, MMHC, FACS Professor and Chair Department of Urology University of Oklahoma TwiLer @uromc Professional Practice Gap Gap 1: There is incomplete
BCG Unresponsive NMIBC: What s Available? Michael S. Cookson, MD, MMHC, FACS Professor and Chair Department of Urology University of Oklahoma TwiLer @uromc Professional Practice Gap Gap 1: There is incomplete
Contents of Online Supporting Information. etable 1. Study characteristics for trials of intravesical therapy vs. TURBT alone
 Contents of Online Supporting Information etable 1. Study characteristics for trials of intravesical therapy vs. TURBT alone etable 2. Study characteristics of head to head trials of intravesical therapy
Contents of Online Supporting Information etable 1. Study characteristics for trials of intravesical therapy vs. TURBT alone etable 2. Study characteristics of head to head trials of intravesical therapy
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of intravesical microwave hyperthermia with intravesical chemotherapy for superficial
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of intravesical microwave hyperthermia with intravesical chemotherapy for superficial
T1HG Bladder Cancer What is the Best Therapy?
 T1HG Bladder Cancer What is the Best Therapy? Ashish M. Kamat, MD, MBBS, FACS Professor of Urology Director, Urologic Oncology Fellowship Guidelines for T1HG Bladder Cancer AUA Recommendation: BCG induction
T1HG Bladder Cancer What is the Best Therapy? Ashish M. Kamat, MD, MBBS, FACS Professor of Urology Director, Urologic Oncology Fellowship Guidelines for T1HG Bladder Cancer AUA Recommendation: BCG induction
Critical Evaluation of Early Post-operative Single Instillation Therapy in NMIBC
 Critical Evaluation of Early Post-operative Single Instillation Therapy in NMIBC Levent N. Türkeri MD, PhD Professor of Urology Acıbadem University Faculty of Medicine Istanbul Conflict of Interest No
Critical Evaluation of Early Post-operative Single Instillation Therapy in NMIBC Levent N. Türkeri MD, PhD Professor of Urology Acıbadem University Faculty of Medicine Istanbul Conflict of Interest No
Bladder Cancer Canada November 21st, Bladder Cancer 2018: A brighter light at the end of the cystoscope
 Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Bladder Cancer Canada November 21st, 2018 Bladder Cancer 2018: A brighter light at the end of the cystoscope Chris Morash MD FRCSC Associate Professor, University of Ottawa Head, Urological Oncology Bladder
Optimising the management of non-muscle invasive bladder cancer from diagnosis to cure. Dr Richard Savdie Uro-Oncology Fellow BSc MBBS FRACS
 Optimising the management of non-muscle invasive bladder cancer from diagnosis to cure Dr Richard Savdie Uro-Oncology Fellow BSc MBBS FRACS Objectives 1. Explore best practice diagnostic techniques 2.
Optimising the management of non-muscle invasive bladder cancer from diagnosis to cure Dr Richard Savdie Uro-Oncology Fellow BSc MBBS FRACS Objectives 1. Explore best practice diagnostic techniques 2.
UC San Francisco UC San Francisco Previously Published Works
 UC San Francisco UC San Francisco Previously Published Works Title Multi-institutional analysis of sequential intravesical gemcitabine and mitomycin C chemotherapy for non-muscle invasive bladder cancer
UC San Francisco UC San Francisco Previously Published Works Title Multi-institutional analysis of sequential intravesical gemcitabine and mitomycin C chemotherapy for non-muscle invasive bladder cancer
RITE Thermochemotherapy in the treatment of BCG refractory NMIBC
 RITE Thermochemotherapy in the treatment of BCG refractory NMIBC Ben Ayres Consultant Urological Surgeon St George s Hospital London 1 Financial and Other Disclosures Off-label use of drugs, devices, or
RITE Thermochemotherapy in the treatment of BCG refractory NMIBC Ben Ayres Consultant Urological Surgeon St George s Hospital London 1 Financial and Other Disclosures Off-label use of drugs, devices, or
Management of Difficult Cases of Non-Muscle Invasive Bladder Cancer
 Management of Difficult Cases of Non-Muscle Invasive Bladder Cancer 1 Bladder Cancer Recurrence is common Progression is uncommon Progression is more important than recurrence There are indicators of recurrence
Management of Difficult Cases of Non-Muscle Invasive Bladder Cancer 1 Bladder Cancer Recurrence is common Progression is uncommon Progression is more important than recurrence There are indicators of recurrence
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
NMIBC. Piotr Jarzemski. Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland
 NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
european urology 52 (2007)
") european urology 52 (2007) 1123 1130 available at www.sciencedirect.com journal homepage: www.europeanurology.com Urothelial Cancer Long-Term Intravesical Adjuvant Chemotherapy Further Reduces Recurrence
european urology 52 (2007) 1123 1130 available at www.sciencedirect.com journal homepage: www.europeanurology.com Urothelial Cancer Long-Term Intravesical Adjuvant Chemotherapy Further Reduces Recurrence
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
The Clinical Impact of the Classification of Carcinoma In Situ on Tumor Recurrence and their Clinical Course in Patients with Bladder Tumor
 Original Article Japanese Journal of Clinical Oncology Advance Access published December 17, 2010 Jpn J Clin Oncol 2010 doi:10.1093/jjco/hyq228 The Clinical Impact of the Classification of Carcinoma In
Original Article Japanese Journal of Clinical Oncology Advance Access published December 17, 2010 Jpn J Clin Oncol 2010 doi:10.1093/jjco/hyq228 The Clinical Impact of the Classification of Carcinoma In
Management of Superficial Bladder Cancer Douglas S. Scherr, M.D.
 Management of Superficial Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of Superficial Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
EUROPEAN UROLOGY 56 (2009)
") EUROPEAN UROLOGY 56 (2009) 247 256 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority Bladder Cancer Editorial by Guido Dalbagni on pp. 257 258 of this issue
EUROPEAN UROLOGY 56 (2009) 247 256 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority Bladder Cancer Editorial by Guido Dalbagni on pp. 257 258 of this issue
September 10, Dear Dr. Clark,
 September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
September 10, 2015 Peter E. Clark, MD Chair, NCCN Bladder Cancer Guidelines (Version 2.2015) Associate Professor of Urologic Surgery Vanderbilt Ingram Cancer Center Nashville, TN 37232 Dear Dr. Clark,
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
Who is the Ideal Candidate for PEG Intron?
 Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Disclosures. The Importance of Pathology? Pathologic, Morphologic and Clinical Features. Pathologic Reproducibility
 The Importance of Pathology? Seth P. Lerner, MD, FACS Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine Support for research Disclosures Photocure, Imalux,
The Importance of Pathology? Seth P. Lerner, MD, FACS Beth and Dave Swalm Chair in Urologic Oncology Scott Department of Urology Baylor College of Medicine Support for research Disclosures Photocure, Imalux,
/05/ /0 Vol. 174, 86 92, July 2005 THE JOURNAL OF UROLOGY. Printed in U.S.A. Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION
 0022-5347/05/1741-0086/0 Vol. 174, 86 92, July 2005 THE JOURNAL OF UROLOGY Printed in U.S.A. Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000162059.64886.1c BACILLUS CALMETTE-GUERIN
0022-5347/05/1741-0086/0 Vol. 174, 86 92, July 2005 THE JOURNAL OF UROLOGY Printed in U.S.A. Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000162059.64886.1c BACILLUS CALMETTE-GUERIN
Update on bladder cancer diagnosis and management
 7 Update on bladder cancer diagnosis and management RICHARD T. BRYAN Although the basis of the diagnosis and management of urothelial bladder cancer has remained unchanged for two decades or more, there
7 Update on bladder cancer diagnosis and management RICHARD T. BRYAN Although the basis of the diagnosis and management of urothelial bladder cancer has remained unchanged for two decades or more, there
Effective Health Care Program
 Comparative Effectiveness Review Number 153 Effective Health Care Program Emerging Approaches to Diagnosis and Treatment of Non Muscle-Invasive Bladder Cancer Executive Summary Background Bladder cancer
Comparative Effectiveness Review Number 153 Effective Health Care Program Emerging Approaches to Diagnosis and Treatment of Non Muscle-Invasive Bladder Cancer Executive Summary Background Bladder cancer
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of electrically-stimulated intravesical chemotherapy for superficial bladder
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of electrically-stimulated intravesical chemotherapy for superficial bladder
Predicting Response to Intravesical Immunotherapy (BCG) in NMIBC
 in NMIBC") Predicting Response to Intravesical Immunotherapy (BCG) in NMIBC Ashish M. Kamat, MD, MBBS, FACS Professor of Urologic Oncology Wayne B. Duddlesten Professor of Cancer Research President, International
Predicting Response to Intravesical Immunotherapy (BCG) in NMIBC Ashish M. Kamat, MD, MBBS, FACS Professor of Urologic Oncology Wayne B. Duddlesten Professor of Cancer Research President, International
MANAGING PATIENTS WITH NON-MUSCLE INVASIVE BLADDER CANCER: OLD DISEASE, NEW IDEAS
 MANAGING PATIENTS WITH NON-MUSCLE INVASIVE BLADDER CANCER: OLD DISEASE, NEW IDEAS This symposium took place on 12 th March 2016 as part of the European Association of Urology Congress 2016 in Munich, Germany
MANAGING PATIENTS WITH NON-MUSCLE INVASIVE BLADDER CANCER: OLD DISEASE, NEW IDEAS This symposium took place on 12 th March 2016 as part of the European Association of Urology Congress 2016 in Munich, Germany
Open clinical uro-oncology trials in Canada
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
Improving Patient Outcomes: Optimal BCG Treatment Regimen to Prevent Progression in Superficial Bladder Cancer
 european urology supplements 5 (2006) 654 659 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review Improving Patient Outcomes: Optimal BCG Treatment Regimen to Prevent Progression
european urology supplements 5 (2006) 654 659 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review Improving Patient Outcomes: Optimal BCG Treatment Regimen to Prevent Progression
INTRAVESICAL THERAPY AND FOLLOW-UP OF SUPERFICIAL TRANSITIONAL CELL CARCINOMA OF THE BLADDER
 Clinical Urology Brazilian Journal of Urology Official Journal of the Brazilian Society of Urology Vol. 26 (3): 242-249, May - June, 2000 INTRAVESICAL THERAPY AND FOLLOW-UP OF SUPERFICIAL TRANSITIONAL
Clinical Urology Brazilian Journal of Urology Official Journal of the Brazilian Society of Urology Vol. 26 (3): 242-249, May - June, 2000 INTRAVESICAL THERAPY AND FOLLOW-UP OF SUPERFICIAL TRANSITIONAL
Maintenance Therapy with Intravesical Bacillus Calmette Guérin in Patients with Intermediate- or High-risk Non-muscle-invasive
 Jpn J Clin Oncol 2013;43(3)305 313 doi:10.1093/jjco/hys225 Advance Access Publication 9 January 2013 Maintenance Therapy with Intravesical Bacillus Calmette Guérin in Patients with Intermediate- or High-risk
Jpn J Clin Oncol 2013;43(3)305 313 doi:10.1093/jjco/hys225 Advance Access Publication 9 January 2013 Maintenance Therapy with Intravesical Bacillus Calmette Guérin in Patients with Intermediate- or High-risk
14th Meeting of the EAU Section of Oncological Urology (ESOU)
") Is Bacillus Calmette-Guerin (BCG) still the best adjuvant treatment after Trans Urethral Resection (TUR) for Ta-T1 high grade (G3) bladder cancer M. Brausi, Modena (IT) Introduction Bacillus Calmette-Guerin
Is Bacillus Calmette-Guerin (BCG) still the best adjuvant treatment after Trans Urethral Resection (TUR) for Ta-T1 high grade (G3) bladder cancer M. Brausi, Modena (IT) Introduction Bacillus Calmette-Guerin
The Impact of Blue Light Cystoscopy with Hexaminolevulinate (HAL) on Progression of Bladder Cancer ANewAnalysis
 on Progression of Bladder Cancer ANewAnalysis") Bladder Cancer 2 (2016) 273 278 DOI 10.3233/BLC-160048 IOS Press Research Report 273 The Impact of Blue Light Cystoscopy with Hexaminolevulinate (HAL) on Progression of Bladder Cancer ANewAnalysis Ashish
Bladder Cancer 2 (2016) 273 278 DOI 10.3233/BLC-160048 IOS Press Research Report 273 The Impact of Blue Light Cystoscopy with Hexaminolevulinate (HAL) on Progression of Bladder Cancer ANewAnalysis Ashish
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
 A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
Sequential Intravesical Gemcitabine and Docetaxel for the Salvage Treatment of Non-Muscle Invasive Bladder Cancer
 Bladder Cancer 1 (2015) 65 72 DOI 10.3233/BLC-150008 IOS Press Research Report 65 Sequential Intravesical Gemcitabine and Docetaxel for the Salvage Treatment of Non-Muscle Invasive Bladder Cancer Ryan
Bladder Cancer 1 (2015) 65 72 DOI 10.3233/BLC-150008 IOS Press Research Report 65 Sequential Intravesical Gemcitabine and Docetaxel for the Salvage Treatment of Non-Muscle Invasive Bladder Cancer Ryan
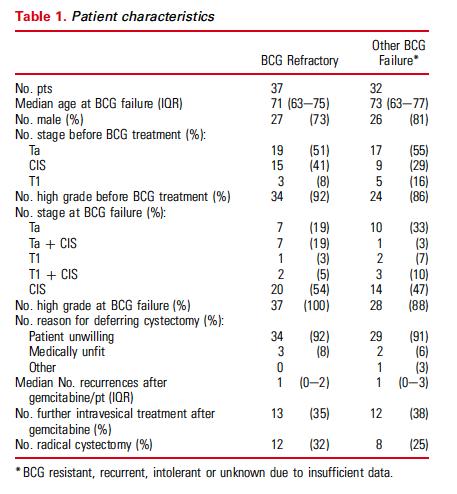
Intravesical Gemcitabine for High Risk, Nonmuscle Invasive Bladder Cancer after Bacillus Calmette-Guerin Treatment Failure
 Intravesical Gemcitabine for High Risk, Nonmuscle Invasive Bladder Cancer after Bacillus Calmette-Guerin Treatment Failure Itay A. Sternberg, Guido Dalbagni,* Ling Y. Chen, Sherri M. Donat, Bernard H.
Intravesical Gemcitabine for High Risk, Nonmuscle Invasive Bladder Cancer after Bacillus Calmette-Guerin Treatment Failure Itay A. Sternberg, Guido Dalbagni,* Ling Y. Chen, Sherri M. Donat, Bernard H.
Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer Center Contemporary Experience
 International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
Chemotherapy Treatment Algorithms for Urology Cancer
 Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Chemotherapy Treatment Algorithms for Urology Cancer Chemoradiation for bladder cancer; Chemotherapy algorithm for non TCC bladder cancer Squamous cell carcinoma; Chemotherapy Algorithm for Non Transitional
Mixed low and high grade non muscle invasive bladder cancer: a histological subtype with favorable outcome
 DOI 10.1007/s00345-014-1383-5 Original Article Mixed low and high grade non muscle invasive bladder cancer: a histological subtype with favorable outcome Tina Schubert Matthew R. Danzig Srinath Kotamarti
DOI 10.1007/s00345-014-1383-5 Original Article Mixed low and high grade non muscle invasive bladder cancer: a histological subtype with favorable outcome Tina Schubert Matthew R. Danzig Srinath Kotamarti
Early radical cystectomy in NMIBC Marko Babjuk
 Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Early radical cystectomy in NMIBC Marko Babjuk Dept. of Urology, 2nd Faculty of Medicine, Hospital Motol, Praha, Czech Republic We Are The European Association of Urology We Are Urologists, residents,
Organ-sparing treatment of invasive transitional cell bladder carcinoma
 Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
ROBOTIC VS OPEN RADICAL CYSTECTOMY
 ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
ROBOTIC VS OPEN RADICAL CYSTECTOMY A REVIEW Colin Lundeen December 14, 2016 Objectives Review the history of radical cystectomy Critically analyze recent RCTs comparing open radical cystectomy (ORC) to
Point-Counterpoint: Radiation & Bladder Cancer
 Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Radiation Plays a Major Role in Certain Stages of Bladder Cancer ~ David C. Beyer, MD Radiation Therapy; no role in management of bladder cancer Robert E. Donohue M.D. Denver VAMC University of Colorado
Naim B Farah 1*, Rami Ghanem 2 and Mahmoud Amr 3
 Farah et al. BMC Urology 2014, 14:11 RESEARCH ARTICLE Open Access Treatment efficacy and tolerability of intravesical Bacillus Calmette-Guerin (BCG) - RIVM strain: induction and maintenance protocol in
Farah et al. BMC Urology 2014, 14:11 RESEARCH ARTICLE Open Access Treatment efficacy and tolerability of intravesical Bacillus Calmette-Guerin (BCG) - RIVM strain: induction and maintenance protocol in
The Effects of Intravesical Chemoimmunotherapy with Gemcitabine and Bacillus Calmette Guérin in Superficial Bladder Cancer: a Preliminary Study
 The Journal of International Medical Research 2009; 37: 1823 1830 The Effects of Intravesical Chemoimmunotherapy with Gemcitabine and Bacillus Calmette Guérin in Superficial Bladder Cancer: a Preliminary
The Journal of International Medical Research 2009; 37: 1823 1830 The Effects of Intravesical Chemoimmunotherapy with Gemcitabine and Bacillus Calmette Guérin in Superficial Bladder Cancer: a Preliminary
Radical Cystectomy Often Too Late? Yes, But...
 european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
THE USE OF HALF DOSE BCG FOR INTRAVESICAL IMMUNOTHERAPY IN NON MUSCLE INVASIVE BLADDER CANCER
 THE USE OF HALF DOSE BCG FOR INTRAVESICAL IMMUNOTHERAPY IN NON MUSCLE INVASIVE BLADDER CANCER Mihály Zoltán Attila 1, Rusu Cristian Bogdan 2, Mihály Orsolya Maria 3, Bolboacă Sorana Daniela 4, Bungărdean
THE USE OF HALF DOSE BCG FOR INTRAVESICAL IMMUNOTHERAPY IN NON MUSCLE INVASIVE BLADDER CANCER Mihály Zoltán Attila 1, Rusu Cristian Bogdan 2, Mihály Orsolya Maria 3, Bolboacă Sorana Daniela 4, Bungărdean
Treatment of Invasive Bladder Cancer in the Elderly and Frail Pa9ent
 Treatment of Invasive Bladder Cancer in the Elderly and Frail Pa9ent Jehonathan H Pinthus MD, Ph.D, FRCSC Associate Professor Department of Surgery/Urology McMaster University Life expectancy Current age
Treatment of Invasive Bladder Cancer in the Elderly and Frail Pa9ent Jehonathan H Pinthus MD, Ph.D, FRCSC Associate Professor Department of Surgery/Urology McMaster University Life expectancy Current age
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Objectives. Results. Patients and Methods. Conclusions. associated percentages were used to analyse treatment variables.
 Current clinical practice gaps in the treatment of intermediate- and high-risk non-muscleinvasive bladder cancer (NMIBC) with emphasis on the use of bacillus Calmette- Guérin (BCG): results of an international
Current clinical practice gaps in the treatment of intermediate- and high-risk non-muscleinvasive bladder cancer (NMIBC) with emphasis on the use of bacillus Calmette- Guérin (BCG): results of an international
The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
 30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Clinical Study of G3 Superficial Bladder Cancer without Concomitant CIS Treated with Conservative Therapy
 Jpn J Clin Oncol 2002;32(11)461 465 Clinical Study of G3 Superficial Bladder Cancer without Concomitant CIS Treated with Conservative Therapy Takashi Saika, Tomoyasu Tsushima, Yasutomo Nasu, Ryoji Arata,
Jpn J Clin Oncol 2002;32(11)461 465 Clinical Study of G3 Superficial Bladder Cancer without Concomitant CIS Treated with Conservative Therapy Takashi Saika, Tomoyasu Tsushima, Yasutomo Nasu, Ryoji Arata,
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Research Report. Keywords: Bladder Cancer, BCG failure, virtual clinical trial, mitomycin C
 Bladder Cancer 1 (2015) 143 150 DOI 10.3233/BLC-150020 IOS Press Research Report 143 Novel Simulation Model of Non-Muscle Invasive Bladder Cancer: A Platform for a Virtual Randomized Trial of Conservative
Bladder Cancer 1 (2015) 143 150 DOI 10.3233/BLC-150020 IOS Press Research Report 143 Novel Simulation Model of Non-Muscle Invasive Bladder Cancer: A Platform for a Virtual Randomized Trial of Conservative
Emerging Approaches for (Neo)Adjuvant Therapy for ER+ Breast Cancer
Adjuvant Therapy for ER+ Breast Cancer") Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer
 Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Bladder Preservation Strategies for Muscle Invasive Bladder Cancer Jeff M. Michalski, MD, MBA, FACR, FASTRO The Carlos A. Perez Distinguished Professor of Radiation Oncology Department of Radiation Oncology
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Guidelines for the Management of Bladder Cancer
 Guidelines for the Management of Bladder Cancer Date Approved by Network Governance July 2012 Date for Review July 2015 Changes Between Version 3 and 4 Sections 5.2 and 8 updated Page 1 of 9 1. Scope of
Guidelines for the Management of Bladder Cancer Date Approved by Network Governance July 2012 Date for Review July 2015 Changes Between Version 3 and 4 Sections 5.2 and 8 updated Page 1 of 9 1. Scope of
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Lymphadenectomy in RCC: Yes, No, Clinical Trial?
 Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Panel: A Case-based Approach to the Management of Bladder Cancer
 Panel: A Case-based Approach to the Management of Bladder Cancer ~ Moderator: Robert Donohue, MD Panel: David C. Beyer, MD E. David Crawford, MD Donald L. Lamm, MD Paul D. Maroni, MD TCC Cases Robert E.
Panel: A Case-based Approach to the Management of Bladder Cancer ~ Moderator: Robert Donohue, MD Panel: David C. Beyer, MD E. David Crawford, MD Donald L. Lamm, MD Paul D. Maroni, MD TCC Cases Robert E.
SUPERFICIAL BLADDER CANCER MANAGEMENT
 A CME Webcast/TELECONFERENCE Case by Case: CRITICAL ISSUES IN SUPERFICIAL BLADDER CANCER MANAGEMENT An Interactive Case Format with Instant Audience Polling APRIL-MAY 2005 CME Program Slide Book Sponsored
A CME Webcast/TELECONFERENCE Case by Case: CRITICAL ISSUES IN SUPERFICIAL BLADDER CANCER MANAGEMENT An Interactive Case Format with Instant Audience Polling APRIL-MAY 2005 CME Program Slide Book Sponsored
Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016
 BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
Debate: Adjuvant vs. Neoadjuvant Therapy for Urothelial Cancer
 Debate: Adjuvant vs. Neoadjuvant Therapy for Urothelial Cancer Kala Sridhar, MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital GU Medical Oncology Site Group Head Associate Professor, University
Debate: Adjuvant vs. Neoadjuvant Therapy for Urothelial Cancer Kala Sridhar, MD, MSc, FRCPC Medical Oncologist, Princess Margaret Hospital GU Medical Oncology Site Group Head Associate Professor, University
A patient with recurrent bladder cancer presents with the following history:
 MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
CHEMO-RADIOTHERAPY FOR BLADDER CANCER. Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre
 CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
CHEMO-RADIOTHERAPY FOR BLADDER CANCER Dr Darren Mitchell Consultant Clinical Oncologist Northern Ireland Cancer Centre AIMS Muscle invasive disease Current Gold-Standard Rationale behind Chemo-Radiotherapy
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS
Haematuria and Bladder Cancer
 Haematuria and Bladder Cancer Dr Pardeep Kumar Consultant Urological Surgeon Haematuria 3 Haematuria Macroscopic vs Microscopic Painful vs Painless Concurrent abdo pain/urinary symptoms Previous testing?
Haematuria and Bladder Cancer Dr Pardeep Kumar Consultant Urological Surgeon Haematuria 3 Haematuria Macroscopic vs Microscopic Painful vs Painless Concurrent abdo pain/urinary symptoms Previous testing?
Clinical Practice Recommendations for the Management of Non Muscle Invasive Bladder Cancer
 european urology supplements 7 (2008) 651 666 available at www.sciencedirect.com journal homepage: www.europeanurology.com Clinical Practice Recommendations for the Management of Non Muscle Invasive Bladder
european urology supplements 7 (2008) 651 666 available at www.sciencedirect.com journal homepage: www.europeanurology.com Clinical Practice Recommendations for the Management of Non Muscle Invasive Bladder
CAN INTRAVESICAL BACILLUS CALMETTE-GUÉRIN REDUCE RECURRENCE IN PATIENTS WITH SUPERFICIAL BLADDER CANCER? A META-ANALYSIS OF RANDOMIZED TRIALS
 ADULT UROLOGY CAN INTRAVESICAL BACILLUS CALMETTE-GUÉRIN REDUCE RECURRENCE IN PATIENTS WITH SUPERFICIAL BLADDER CANCER? A META-ANALYSIS OF RANDOMIZED TRIALS RUI FA HAN AND JIAN GANG PAN ABSTRACT Objectives.
ADULT UROLOGY CAN INTRAVESICAL BACILLUS CALMETTE-GUÉRIN REDUCE RECURRENCE IN PATIENTS WITH SUPERFICIAL BLADDER CANCER? A META-ANALYSIS OF RANDOMIZED TRIALS RUI FA HAN AND JIAN GANG PAN ABSTRACT Objectives.
Original Article APMC-276
 Original Article APMC-276 The Clinical Value of Immediate Second Transurethral Resection in Patients with High Grade Non-Muscle Inasive Bladder Cancer (HG-NMIBC) Syed Saleem Abbas Jafri, Zafar Iqbal Khan
Original Article APMC-276 The Clinical Value of Immediate Second Transurethral Resection in Patients with High Grade Non-Muscle Inasive Bladder Cancer (HG-NMIBC) Syed Saleem Abbas Jafri, Zafar Iqbal Khan
Urinary Bladder Cancer
 Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Fellow GU Lecture Series, 2018 Urinary Bladder Cancer Asit Paul, MD, PhD 01/31/2018 Overview Non-muscle invasive bladder cancer Muscle invasive bladder cancer Bladder sparing chemo-radiation therapy T4b
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015
 Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
Alicia K. Morgans, MD Assistant Professor of Medicine Division of Hematology/Oncology Vanderbilt University Medical Center January 24, 2015 Overview Background Perioperative chemotherapy in MIBC Neoadjuvant
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance