Radiographic Assessment of Response An Overview of RECIST v1.1
|
|
|
- Diane Rogers
- 5 years ago
- Views:
Transcription
1 Radiographic Assessment of Response An Overview of RECIST v1.1 Stephen Liu, MD Georgetown University May 15 th, 2015
2 Presentation Objectives To understand the purpose of RECIST guidelines To describe the characteristics that are important in selecting target lesions To apply RECIST v1.1 guidelines in assessing response to therapy
3 RECIST Response Evaluation Criteria In Solid Tumors Guidelines published in 2000 Updated guidelines (v1.1) published in 2009 Guidelines are a tool to assess response to treatment
4 Response Critical endpoint for many clinical trials Reflects changes in tumor burden Historically represented drug activity Related to other clinical outcomes Correlation with survival (Paesmans et al 1997, Buyse et al 2000) Criteria for assessing response and progression are critical when RR is the primary endpoint Time to progression and progression free survival are based on assessment of progression
5 Assessing Response Integral part of clinical oncology Systematic observation is a basic principle of oncology Radiographic assessment routinely performed and guides patient care but Inconsistent use of terms like response and progression Reproducibility and comparisons across institutions are challenging No clear rules on how to approach a mixed response
6 Assessing Response Formal guidelines standardize assessment Facilitate comparison within and among trials Goal is consistency and reproducibility
7 Assessing Response Need for a surrogate endpoint was clear For cytotoxic therapy, response rate was an early endpoint Study simulated clinical conditions Establish what is reproducible (not necessarily significant) 12 spheres of varying diameter placed under a soft mattress of foam rubber to represent masses / lymph nodes 16 experienced physicians measured each diameter Consistent results obtained when the product of perpendicular diameters was reduced by 50% Reduction by 25% led to more inconsistency
8 Assessing Response World Health Organization (WHO) First international criteria published in 1979 Standardized reporting of results Defines response and progression Response was a reduction in the product of perpendicular diameters by 50% Was left open to interpretation and led to variations and modified WHO criteria Identification of measurable lesions Number of lesions to measure Progression and mixed responses Accounting for new technology
9 Assessing Response RECIST criteria Collaboration of NCI, EORTC, NCIC International membership Representatives from academia, industry, clinical research, image acquisition Employed a data warehouse 6500 patients, lesions Simulation studies estimate the impact of changes in guidelines
10 Assessing Response RECIST criteria Target and non-target lesions Quantitative assessment of target lesions Qualitative assessment of non-target lesions Updated WHO criteria Fewer measured lesions Updated definitions of progression Unidirectional instead of bidirectional
11 Assessing Response Subsequently validated Exceptions include mesothelioma, lymphoma Updated in 2008 (version 1.1) for further clarification, simplification and standardization
12 RECIST v1.1 Criteria The purpose of RECIST guidelines is to standardize response assessment Most trials assessing response utilize RECIST Understanding RECIST criteria is critical to trial conduct and interpretation of results Eligibility Continuation of effective therapy Discontinuation of ineffective therapy

13 Measurable Disease Measurable disease is more than just measurable Dimensions on a radiology report are not enough!

14 Measurable Disease Measurable disease is more than just measurable Dimensions on a radiology report are not enough!
15 Measurable Disease Tumor lesions Measure in the plane in which images were acquired For body CT, this is typically the axial plane Must be accurately measured in at least one dimension with a minimum size (by long axis) of 10 mm by CT scan 10 mm by caliper measurement on clinical exam 20 mm by chest x-ray Based on a 5mm slice thickness If slice thickness is > 5mm, use 2x the slice thickness as the minimum size
16 Measurable Disease Malignant lymph nodes Must be accurately measured in at least one dimension with a minimum size (by short axis) of 15 mm by CT scan Follow the short axis, not the long axis

17 Lymph Node Short Axis Eisenhauer, EORTC 2008
18 Non-Measurable Disease All other lesions are non-measurable Smaller lesions Leptomeningeal disease Lymphangitic disease of skin or lung Ascites Effusions Inflammatory breast disease Lymph nodes with a short axis < 10mm are considered non-pathological and should not be recorded or followed
19 Non-Measurable Disease Bone lesions Cysts Previously treated lesions Unless there is documented progression in the lesion following prior treatment
20 Modality Image-based assessment preferred to clinical exam Consistency should be maintained Chest X-ray is acceptable but not preferred MRI can be used Preferred for neoadjuvant studies in breast cancer CT is otherwise the preferred modality Ultrasound cannot be used Not reproducible Operator dependent and subjective Obstructed by gas
21 Selecting Target Lesions Careful planning prior to therapy is critical Ensure eligibility Minimize challenges in the future Target lesions Largest and most easily and reproducibly measurable Representative of the disease Non-target lesions Represents all other manifestations of the disease Includes Non-measurable lesions Measurable lesions not selected as target lesions
22 Selecting Target Lesions How to choose your target lesions Radiographic assessment preferred over clinical exam CT preferred over chest X-ray or MRI Use the same modality going forward Remember which diameter to use Tumor lesions always use longest diameter Lymph nodes always use shortest diameter
23 Selecting Target Lesions Each case is unique Select lesions with well-defined edges or margins Choose lesions in a stable position Mesenteric masses will often change position Think ahead Avoid lesions in close proximity that may coalesce Capture the disease distribution Limited to 5 target lesions and 2 per organ

24 Measurable Disease Largest lesion may not be the best lesion Eisenhauer, Eur J Cancer 2008
25 Assessing Response The sum of the diameter for all target lesions will be used to calculate response Each target lesion will be followed If lesion is no longer measurable, it will still be counted Longest diameter should be used, not orientation or slice If visible but too small to measure, use 5mm as the value If a value is provided under 5mm, use the measured value
26 Response Definitions Complete response (CR) Disappearance of all target lesions (LN < 10mm short axis) Partial response (PR) At least a 30% decrease in the sum of diameters of target lesions relative to the baseline sum
27 Response Definitions Complete response (CR) Disappearance of all target lesions (LN < 10mm short axis) Partial response (PR) At least a 30% decrease in the sum of diameters of target lesions relative to the baseline sum Progressive disease (PD) At least a 20% increase (and at least 5mm) in the sum of diameters of target lesions relative to smallest sum on study Appearance of a new lesion is also progression
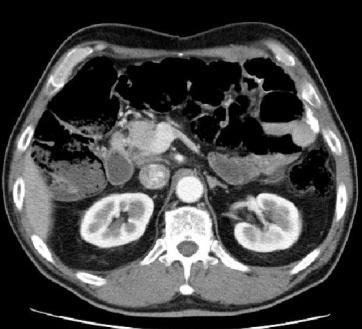
28 Assessing Response 10/31/14 Sum of Target Lesions 6.4 cm Response Baseline Baseline uses long axis for tumor lesions and short axis for malignant lymph nodes
29 Assessing Response 10/31/14 12/15/14 Sum of Target Lesions 6.4 cm 4.0 cm Response Baseline PR Decrease from 6.4 cm to 4.0 cm Reduction of 2.4 cm Reduction of 38% from baseline (unconfirmed PR)
30 Assessing Response 10/31/14 12/15/14 2/2/15 Sum of Target Lesions 6.4 cm 4.0 cm 2.2 cm Response Baseline PR PR Decrease from 6.4 cm to 2.2 cm Reduction of 4.2 cm Reduction of 66% from baseline (confirmed PR)
31 Assessing Response 10/31/14 12/15/14 2/2/15 3/27/15 Sum of Target Lesions 6.4 cm 4.0 cm 2.2 cm 3.2 cm Response Baseline PR PR Decrease from 6.4 cm to 3.2 cm Reduction of 3.2 cm Reduction of 50% from baseline (confirmed PR)
32 Assessing Response 10/31/14 12/15/14 2/2/15 3/27/15 Sum of Target Lesions 6.4 cm 4.0 cm 2.2 cm 3.2 cm Response Baseline PR PR PD Increase from 2.2 cm to 3.2 cm Increase by 1.0 cm Increase by 45% from baseline (PD) PD: At least a 20% increase (and at least 5mm) in the sum of diameters of target lesions relative to smallest sum on study
33 Response Definitions Complete response (CR) Disappearance of all target lesions (LN < 10mm short axis) Partial response (PR) At least a 30% decrease in the sum of diameters of target lesions relative to the baseline sum Progressive disease (PD) At least a 20% increase (and at least 5mm) in the sum of diameters of target lesions relative to smallest sum on study Appearance of a new lesion is also progression Stable disease (SD) Does not qualify for any of the above
34 Lymph Nodes Normal structures Not considered pathologic when short axis < 10mm Short axis diameter still recorded and included in the sum of target lesions In patients with a complete response, normal lymph nodes may persist Sum of lesions may be greater than zero even in a CR

35 Complete Response

36 Lymph Node Normalization Follow-up An abnormally enlarged right external iliac node at Eisenhauer, EORTC 2008
37 Non-Target Lesions No need for measurements Qualitative assessment is required Complete response requires disappearance of all non-target lesions (all LN < 10mm in short axis) Progressive disease on the basis of non-target lesions only when there is unequivocal progression A modest increase in size is not sufficient Change must be sufficient to require a change in therapy
38 New Lesions Represent progression regardless of measurability Should be unequivocal New bone lesions may represent healing or a flare Equivocal lesions should be confirmed If subsequently shown to represent new disease, the date of progression should be the date of the initial scan When a lesion is seen in an anatomic area not included in the baseline scan, it is considered new and will constitute progressive disease Obtaining the proper baseline scan is critical!
39 PET Positive lesion has FDG avidity at least twice that of surrounding tissue on the attenuation corrected images If a PET is negative at baseline and positive at follow up, this is a sign of progressive disease If there is no PET at baseline A new lesion confirmed by CT is progressive disease A new lesion not seen by CT is not progressive disease Increased FDG avidity in a pre-existing site that is not progressing based on CT is not progressive disease
40 Unique Circumstances Lesions that split during treatment Longest diameter of fragmented portions should be added together to calculate the target lesion sum Document the process Lesions that coalesce When a plane exists, use it to measure individual lesions If lesions are truly coalescing, the vector of the longest diameter should be used as the longest diameter of the coalesced lesion and represent the two target lesions
41 Unique Circumstances Lesions that disappear and return Continue to measure and include in the sum Diameter will contribute to PR/PD evaluation If the patient had achieved a complete response and a lesion reappears, this constitutes progressive disease
42 Unique Circumstances Target lesion is now non-evaluable due to necessary changes in technique Seek a baseline exam using the new technique If no alternatives judgment call Delete the lesion from all forms Make the overall interpretation inevaluable Should be discussed with the site and study PI / monitor Try to anticipate before the trial starts
43 Tumor Markers Alone, tumor markers cannot assess response If elevated, they must normalize to meet criteria for a complete response Published guidelines for CA-125 and PSA Should be incorporated into protocols for specific diseases
44 Conclusions Goal is accuracy and reproducibility Strict criteria on measurability 10 mm for tumor lesions 15 mm for lymph nodes (using the short axis) Select target lesions carefully When assessing response PR decrease in sum of diameters by 30% from baseline PD increase in sum of diameters by 20% from nadir (or emergence of unequivocal new lesions) Refer to the published guidelines and the protocol!
Welcome to the RECIST 1.1 Quick Reference
 Welcome to the RECIST 1.1 Quick Reference *Eisenhauer, E. A., et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer 2009;45:228-47. Subject Eligibility
Welcome to the RECIST 1.1 Quick Reference *Eisenhauer, E. A., et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer 2009;45:228-47. Subject Eligibility
RECIST 1.1 Criteria Handout. Medical Imaging. ICONplc.com/imaging
 RECIST 1.1 Criteria Handout Medical Imaging ICONplc.com/imaging 2 Contents Basic Paradigm 3 3 Image Acquisition 44 Measurable Lesions 55 Non-Measurable Lesions. 66 Special Lesion Types 77 Baseline Lesion
RECIST 1.1 Criteria Handout Medical Imaging ICONplc.com/imaging 2 Contents Basic Paradigm 3 3 Image Acquisition 44 Measurable Lesions 55 Non-Measurable Lesions. 66 Special Lesion Types 77 Baseline Lesion
MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES
 MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES Although response is not the primary endpoint of this trial, subjects with measurable disease will be assessed by standard criteria. For the purposes of this
MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES Although response is not the primary endpoint of this trial, subjects with measurable disease will be assessed by standard criteria. For the purposes of this
Radiologic assessment of response of tumors to treatment. Copyright 2008 TIMC, Matthew A. Barish M.D. All rights reserved. 1
 Radiologic assessment of response of tumors to treatment Copyright 2008 TIMC, Matthew A. Barish M.D. All rights reserved. 1 Objective response assessment is important to describe the treatment effect of
Radiologic assessment of response of tumors to treatment Copyright 2008 TIMC, Matthew A. Barish M.D. All rights reserved. 1 Objective response assessment is important to describe the treatment effect of
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL RESPONSE ASSESSMENT LYMPHOMA CHAPTER 11B REVISED: SEPTEMBER 2016
 MANUAL RESPONSE ASSESSMENT LYMPHOMA CHAPTER 11B REVISED: SEPTEMBER 2016") LYMPHOMA Definitions of Response According to Non Hodgkin s Lymphoma (NHL) Criteria Listed below is the new NCI Lymphoma criteria for evaluation and endpoint definitions for Non Hodgkin s Lymphoma response
LYMPHOMA Definitions of Response According to Non Hodgkin s Lymphoma (NHL) Criteria Listed below is the new NCI Lymphoma criteria for evaluation and endpoint definitions for Non Hodgkin s Lymphoma response
Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD
 Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD Section of Pediatric Radiology C.S. Mott Children s Hospital University of Michigan ethans@med.umich.edu Disclosures No relevant
Update on RECIST and Staging of Common Pediatric Tumors Ethan A. Smith, MD Section of Pediatric Radiology C.S. Mott Children s Hospital University of Michigan ethans@med.umich.edu Disclosures No relevant
RECIST 1.1 and SWOG Protocol Section 10
 RECIST 1.1 and SWOG Protocol Section 10 Louise Highleyman, Data Coordinator SWOG Statistics and Data Management Center Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 2009: Revised RECIST guideline
RECIST 1.1 and SWOG Protocol Section 10 Louise Highleyman, Data Coordinator SWOG Statistics and Data Management Center Response Evaluation Criteria in Solid Tumors (RECIST) 1.1 2009: Revised RECIST guideline
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung
 How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
Comparison of RECIST version 1.0 and 1.1 in assessment of tumor response by computed tomography in advanced gastric cancer
 Original Article Comparison of RECIST version 1.0 and 1.1 in assessment of tumor response by computed tomography in advanced gastric cancer Gil-Su Jang 1 *, Min-Jeong Kim 2 *, Hong-Il Ha 2, Jung Han Kim
Original Article Comparison of RECIST version 1.0 and 1.1 in assessment of tumor response by computed tomography in advanced gastric cancer Gil-Su Jang 1 *, Min-Jeong Kim 2 *, Hong-Il Ha 2, Jung Han Kim
Radiological staging of lung cancer. Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh
 Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Radiological staging of lung cancer Shukri Loutfi,MD,FRCR Consultant Thoracic Radiologist KAMC-Riyadh Bronchogenic Carcinoma Accounts for 14% of new cancer diagnoses in 2012. Estimated to kill ~150,000
Programming LYRIC Response in Immunomodulatory Therapy Trials Yang Wang, Seattle Genetics, Inc., Bothell, WA
 PharmaSUG 2017 Paper BB12 Programming LYRIC Response in Immunomodulatory Therapy Trials Yang Wang, Seattle Genetics, Inc., Bothell, WA ABSTRACT The LYmphoma Response to Immunomodulatory therapy Criteria
PharmaSUG 2017 Paper BB12 Programming LYRIC Response in Immunomodulatory Therapy Trials Yang Wang, Seattle Genetics, Inc., Bothell, WA ABSTRACT The LYmphoma Response to Immunomodulatory therapy Criteria
Applying the New irecist Guidelines Radiologic and Clinical Trial Considerations
 Applying the New irecist Guidelines Radiologic and Clinical Trial Considerations Author: K. Luby, Mint Medical www.irecist.com irecist 1 : Guidelines for response criteria for use in trials testing immunotherapeutics
Applying the New irecist Guidelines Radiologic and Clinical Trial Considerations Author: K. Luby, Mint Medical www.irecist.com irecist 1 : Guidelines for response criteria for use in trials testing immunotherapeutics
Evaluation of Lung Cancer Response: Current Practice and Advances
 Evaluation of Lung Cancer Response: Current Practice and Advances Jeremy J. Erasmus I have no financial relationships, arrangements or affiliations and this presentation will not include discussion of
Evaluation of Lung Cancer Response: Current Practice and Advances Jeremy J. Erasmus I have no financial relationships, arrangements or affiliations and this presentation will not include discussion of
8/10/2016. PET/CT Radiomics for Tumor. Anatomic Tumor Response Assessment in CT or MRI. Metabolic Tumor Response Assessment in FDG-PET
 PET/CT Radiomics for Tumor Response Evaluation August 1, 2016 Wei Lu, PhD Department of Medical Physics www.mskcc.org Department of Radiation Oncology www.umaryland.edu Anatomic Tumor Response Assessment
PET/CT Radiomics for Tumor Response Evaluation August 1, 2016 Wei Lu, PhD Department of Medical Physics www.mskcc.org Department of Radiation Oncology www.umaryland.edu Anatomic Tumor Response Assessment
Assessment of Efficacy and Immune Related RECIST criteria
 Assessment of Efficacy and Immune Related RECIST criteria Dr Kenneth O Byrne Princess Alexandra Hospital and Queensland University of Technology, Brisbane, Australia & Trinity College, Dublin, Ireland
Assessment of Efficacy and Immune Related RECIST criteria Dr Kenneth O Byrne Princess Alexandra Hospital and Queensland University of Technology, Brisbane, Australia & Trinity College, Dublin, Ireland
CA 125 definitions agreed by GCIG November 2005
 CA 125 definitions agreed by GCIG November 2005 The GCIG has agreed criteria for defining response and progression of ovarian carcinoma which use the serum marker CA 125, and the situations where these
CA 125 definitions agreed by GCIG November 2005 The GCIG has agreed criteria for defining response and progression of ovarian carcinoma which use the serum marker CA 125, and the situations where these
Cancer will soon become the most common cause of
 From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors Richard L. Wahl 1,2, Heather Jacene 1, Yvette Kasamon 2, and Martin A. Lodge 1 1 Division of Nuclear Medicine,
From RECIST to PERCIST: Evolving Considerations for PET Response Criteria in Solid Tumors Richard L. Wahl 1,2, Heather Jacene 1, Yvette Kasamon 2, and Martin A. Lodge 1 1 Division of Nuclear Medicine,
Update in Lymphoma Imaging
 Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD
 ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD Foundation Medical Partners Southern New Hampshire Health System December 1, 2016 accc-iclio.org Overview
ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD Foundation Medical Partners Southern New Hampshire Health System December 1, 2016 accc-iclio.org Overview
PharmaSUG 2018 Paper AD-02
 PharmaSUG 2018 Paper AD-02 Derivations of Response Status from SDTM Domains using RECIST 1.1 Christine Teng, Merck Research Laboratories, Merck & Co., Inc., Rahway, NJ USA Pang Lei, Merck Research Laboratories,
PharmaSUG 2018 Paper AD-02 Derivations of Response Status from SDTM Domains using RECIST 1.1 Christine Teng, Merck Research Laboratories, Merck & Co., Inc., Rahway, NJ USA Pang Lei, Merck Research Laboratories,
Paradigm shift - from "curing cancer" to making cancer a "chronic disease"
 Current Clinical Practice of Tumor Response Assessment David M. Panicek, MD Department of Radiology Memorial Sloan-Kettering Cancer Center, New York, NY Learning Objectives Review various response assessment
Current Clinical Practice of Tumor Response Assessment David M. Panicek, MD Department of Radiology Memorial Sloan-Kettering Cancer Center, New York, NY Learning Objectives Review various response assessment
Learning Objectives. 1. Identify which patients meet criteria for annual lung cancer screening
 Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Disclosure I, Taylor Rowlett, DO NOT have a financial interest /arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context
Phase II Cancer Trials: When and How
 Phase II Cancer Trials: When and How Course for New Investigators August 9-12, 2011 Learning Objectives At the end of the session the participant should be able to Define the objectives of screening vs.
Phase II Cancer Trials: When and How Course for New Investigators August 9-12, 2011 Learning Objectives At the end of the session the participant should be able to Define the objectives of screening vs.
Revised RECIST Guideline Version 1.1: What Oncologists Want to Know and What Radiologists Need to Know
 Special rticle Pictorial Essay Nishino et al. Revised REIST Guideline Special rticle Pictorial Essay Downloaded from www.ajronline.org by 46.3.203.167 on 11/20/17 from IP address 46.3.203.167. opyright
Special rticle Pictorial Essay Nishino et al. Revised REIST Guideline Special rticle Pictorial Essay Downloaded from www.ajronline.org by 46.3.203.167 on 11/20/17 from IP address 46.3.203.167. opyright
Phase II Cancer Trials: When and How
 Phase II Cancer Trials: When and How Course for New Investigators August 21-23, 2013 Acknowledgment Elizabeth Eisenhauer for some slides! Learning Objectives At the end of the session the participant should
Phase II Cancer Trials: When and How Course for New Investigators August 21-23, 2013 Acknowledgment Elizabeth Eisenhauer for some slides! Learning Objectives At the end of the session the participant should
8/10/2016. PET/CT for Tumor Response. Staging and restaging Early treatment response evaluation Guiding biopsy
 PET/CT for Tumor Response Evaluation August 4, 2016 Wei Lu, PhD Department of Medical Physics www.mskcc.org Department of Radiation Oncology www.umaryland.edu FDG PET/CT for Cancer Imaging Staging and
PET/CT for Tumor Response Evaluation August 4, 2016 Wei Lu, PhD Department of Medical Physics www.mskcc.org Department of Radiation Oncology www.umaryland.edu FDG PET/CT for Cancer Imaging Staging and
10 most frequently made mistakes with RECIST 1.1: how Radiologist can fail - and how to avoid them
 10 most frequently made mistakes with RECIST 1.1: how Radiologist can fail - and how to avoid them Poster No.: C-1689 Congress: ECR 2014 Type: Educational Exhibit Authors: M. Kekelidze, P. Lodise, M. Tozakidou,
10 most frequently made mistakes with RECIST 1.1: how Radiologist can fail - and how to avoid them Poster No.: C-1689 Congress: ECR 2014 Type: Educational Exhibit Authors: M. Kekelidze, P. Lodise, M. Tozakidou,
Blinded, independent, central image review in oncology trials: how the study endpoint impacts the adjudication rate
 Blinded, independent, central image review in oncology trials: how the study endpoint impacts the adjudication rate Poster No.: C-0200 Congress: ECR 2014 Type: Authors: Keywords: DOI: Scientific Exhibit
Blinded, independent, central image review in oncology trials: how the study endpoint impacts the adjudication rate Poster No.: C-0200 Congress: ECR 2014 Type: Authors: Keywords: DOI: Scientific Exhibit
Radiological assessment of neoadjuvent chemotherapy for breast cancer
 XV th Balkan Congress of Radiology Budapest, Hungary, October 12 15, 2017 Radiological assessment of neoadjuvent chemotherapy for breast cancer V. Bešlagić C l i n i c o f R a d i o l o g y, U n i v e
XV th Balkan Congress of Radiology Budapest, Hungary, October 12 15, 2017 Radiological assessment of neoadjuvent chemotherapy for breast cancer V. Bešlagić C l i n i c o f R a d i o l o g y, U n i v e
Liver metastases: treatment planning. PJ Valette
 Liver metastases: treatment planning PJ Valette Liver metastases removal December 2010 April 2011 : after chemotherapy June 2011 : after resection of left lobe mets & portal embol. Sept 2011 : 1 year after
Liver metastases: treatment planning PJ Valette Liver metastases removal December 2010 April 2011 : after chemotherapy June 2011 : after resection of left lobe mets & portal embol. Sept 2011 : 1 year after
Radiological evaluation, with RECIST criteria, of treatment response of non-microcytic lung cancer. Routine follow-up.
 Original article Anales de Radiología México 2015;14:31-42. Radiological evaluation, with RECIST criteria, of treatment response of non-microcytic lung cancer. Routine follow-up. Cuituny-Romero AK 1, Onofre-Castillo
Original article Anales de Radiología México 2015;14:31-42. Radiological evaluation, with RECIST criteria, of treatment response of non-microcytic lung cancer. Routine follow-up. Cuituny-Romero AK 1, Onofre-Castillo
Analysis of Oncology Studies for Programmers and Statisticians
 PharmaSUG 2018 DS06 Analysis of Oncology Studies for Programmers and Statisticians Kevin Lee, Clindata Insight, Moraga, CA ABSTRACT Compared to other therapeutic studies, oncology studies are generally
PharmaSUG 2018 DS06 Analysis of Oncology Studies for Programmers and Statisticians Kevin Lee, Clindata Insight, Moraga, CA ABSTRACT Compared to other therapeutic studies, oncology studies are generally
I9 COMPLETION INSTRUCTIONS
 The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
The I9 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I9 documents comparison review of the baseline screen (C2 Form) with any historical images available. At T1 and
Chikako Suzuki M.D., Ph.D.
 Chikako Suzuki M.D., Ph.D. Main supervisor Lennart Blomqvist M.D. Ph.D Co supervisor Hans Jacobsson M.D. Ph.D., Hirofumi Fujii M.D Ph.D. Department of Molecular Medicine and Surgery, Karolinska Institutet
Chikako Suzuki M.D., Ph.D. Main supervisor Lennart Blomqvist M.D. Ph.D Co supervisor Hans Jacobsson M.D. Ph.D., Hirofumi Fujii M.D Ph.D. Department of Molecular Medicine and Surgery, Karolinska Institutet
Integrating Imaging Criteria Into Trial Endpoints
 Integrating Imaging Criteria Into Trial Endpoints Gregory Goldmacher, MD, PhD, MBA Sr. Director, Translational Biomarkers Merck Research Laboratories CBI Imaging In Clinical Trials 2017 Preview Purpose
Integrating Imaging Criteria Into Trial Endpoints Gregory Goldmacher, MD, PhD, MBA Sr. Director, Translational Biomarkers Merck Research Laboratories CBI Imaging In Clinical Trials 2017 Preview Purpose
Utility of 18 F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer
 Utility of F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer Ngoc Ha Le 1*, Hong Son Mai 1, Van Nguyen Le 2, Quang Bieu Bui 2 1 Department
Utility of F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer Ngoc Ha Le 1*, Hong Son Mai 1, Van Nguyen Le 2, Quang Bieu Bui 2 1 Department
ClinicalTrials.gov Protocol and Results Registration System (PRS) Receipt Release Date: 09/30/2015. ClinicalTrials.gov ID: NCT
 Receipt Release Date: 09/30/2015. ClinicalTrials.gov ID: NCT") ClinicalTrials.gov Protocol and Results Registration System (PRS) Receipt Release Date: 09/30/2015 ClinicalTrials.gov ID: NCT01378962 Study Identification Unique Protocol ID: ML25514 Brief Title: A Study
ClinicalTrials.gov Protocol and Results Registration System (PRS) Receipt Release Date: 09/30/2015 ClinicalTrials.gov ID: NCT01378962 Study Identification Unique Protocol ID: ML25514 Brief Title: A Study
Recommendations for cross-sectional imaging in cancer management, Second edition
 www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Carcinoma of unknown primary origin (CUP) Faculty of Clinical Radiology www.rcr.ac.uk Contents Carcinoma of
www.rcr.ac.uk Recommendations for cross-sectional imaging in cancer management, Second edition Carcinoma of unknown primary origin (CUP) Faculty of Clinical Radiology www.rcr.ac.uk Contents Carcinoma of
I8 COMPLETION INSTRUCTIONS
 The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
The I8 Form is completed for each screening exam at T0, T1, and T2. At T0 (baseline), the I8 Form documents comparison review of the baseline screen (DR Form) with any historical images available. At T1
Denominator Criteria (Eligible Cases): Patient encounter during the performance period (CPT): 78300, 78305, 78306, 78315, 78320
: Patient encounter during the performance period (CPT): 78300, 78305, 78306, 78315, 78320") Quality ID #147: Nuclear Medicine: Correlation with Existing Imaging Studies for All Patients Undergoing Bone Scintigraphy National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS
Quality ID #147: Nuclear Medicine: Correlation with Existing Imaging Studies for All Patients Undergoing Bone Scintigraphy National Quality Strategy Domain: Communication and Care Coordination 2018 OPTIONS
doi: /hepr Response Evaluation Criteria in Cancer of the Liver (RECICL) (2015 Revised version)
 (2015 Revised version)") bs_bs_banner Hepatology Research 2016; 46: 3 9 doi: 10.1111/hepr.12542 Special Report Response Evaluation Criteria in Cancer of the Liver (RECICL) (2015 Revised version) Masatoshi Kudo, Kazuomi Ueshima,
bs_bs_banner Hepatology Research 2016; 46: 3 9 doi: 10.1111/hepr.12542 Special Report Response Evaluation Criteria in Cancer of the Liver (RECICL) (2015 Revised version) Masatoshi Kudo, Kazuomi Ueshima,
C2 COMPLETION INSTRUCTIONS
 The C2 Form is completed for each screening exam at T0, T1, and T2. The C2 Form is to be completed by each of the following ACRIN-NLST study staff: the research associate (study coordinator), CT technologist,
The C2 Form is completed for each screening exam at T0, T1, and T2. The C2 Form is to be completed by each of the following ACRIN-NLST study staff: the research associate (study coordinator), CT technologist,
CDISC Journey in Solid Tumor using RECIST 1.1 Kevin Lee PhUSE conference Oct 14th, 2013
 CDISC Journey in Solid Tumor using RECIST 1.1 Kevin Lee PhUSE conference Oct 14th, 2013 Disclaimer Any views or opinions presented in this presentation are solely those of the author and do not necessarily
CDISC Journey in Solid Tumor using RECIST 1.1 Kevin Lee PhUSE conference Oct 14th, 2013 Disclaimer Any views or opinions presented in this presentation are solely those of the author and do not necessarily
Computed tomography and Modified RECIST criteria for assessment of response in malignant pleural mesothelioma
 Computed tomography and Modified RECIST criteria for assessment of response in malignant pleural mesothelioma Poster No.: C-0729 Congress: ECR 2013 Type: Scientific Exhibit Authors: A. Marin, I. Pozek,
Computed tomography and Modified RECIST criteria for assessment of response in malignant pleural mesothelioma Poster No.: C-0729 Congress: ECR 2013 Type: Scientific Exhibit Authors: A. Marin, I. Pozek,
NIH Public Access Author Manuscript AJR Am J Roentgenol. Author manuscript; available in PMC 2011 July 6.
 NIH Public Access Author Manuscript Published in final edited form as: AJR Am J Roentgenol. 2010 September ; 195(3): W221 W228. doi:10.2214/ajr.09.3928. New Response Evaluation Criteria in Solid Tumors
NIH Public Access Author Manuscript Published in final edited form as: AJR Am J Roentgenol. 2010 September ; 195(3): W221 W228. doi:10.2214/ajr.09.3928. New Response Evaluation Criteria in Solid Tumors
Response Assessment in Clinical Trials: Implications for Sarcoma Clinical Trial Design
 Response Assessment in Clinical Trials: Implications for Sarcoma Clinical Trial Design C. Carl Jaffe Diagnostic Imaging Branch, Cancer Imaging Program, Division of Cancer Treatment and Diagnosis, National
Response Assessment in Clinical Trials: Implications for Sarcoma Clinical Trial Design C. Carl Jaffe Diagnostic Imaging Branch, Cancer Imaging Program, Division of Cancer Treatment and Diagnosis, National
Measuring Response in Solid Tumors: Unidimensional Versus Bidimensional Measurement
 Measuring Response in Solid Tumors: Unidimensional Versus Bidimensional Measurement Keith James, Elizabeth Eisenhauer, Michaele Christian, Monica Terenziani, Donald Vena, Alison Muldal, Patrick Therasse
Measuring Response in Solid Tumors: Unidimensional Versus Bidimensional Measurement Keith James, Elizabeth Eisenhauer, Michaele Christian, Monica Terenziani, Donald Vena, Alison Muldal, Patrick Therasse
Streamlined workflow for review and analysis of oncology patients
 Streamlined workflow for review and analysis of oncology patients Philips IntelliSpace Portal Multi-modality Tumor Tracking application (MMTT) Ekta Dharaiya, MS, Philips Healthcare, Cleveland, OH Cancer
Streamlined workflow for review and analysis of oncology patients Philips IntelliSpace Portal Multi-modality Tumor Tracking application (MMTT) Ekta Dharaiya, MS, Philips Healthcare, Cleveland, OH Cancer
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds
 Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
Dr Claire Smith, Consultant Radiologist St James University Hospital Leeds Imaging in jaundice and 2ww pathway Image protocol Staging Limitations Pancreatic cancer 1.2.4 Refer people using a suspected
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Breast Cancer. What is breast cancer?
 Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation *
 ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
Pre-operative assessment of patients for cytoreduction and HIPEC
 Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
Pre-operative assessment of patients for cytoreduction and HIPEC Washington Hospital Center Washington, DC, USA Ovarian Cancer Surgery New Strategies Bergamo, Italy May 5, 2011 Background Cytoreductive
ROLE OF PET-CT IN BREAST CANCER, GUIDELINES AND BEYOND. Prof Jamshed B. Bomanji Institute of Nuclear Medicine UCL Hospitals London
 ROLE OF PET-CT IN BREAST CANCER, GUIDELINES AND BEYOND Prof Jamshed B. Bomanji Institute of Nuclear Medicine UCL Hospitals London CANCER Key facts Estimated 15.2 million new cases per year in 2015 worldwide
ROLE OF PET-CT IN BREAST CANCER, GUIDELINES AND BEYOND Prof Jamshed B. Bomanji Institute of Nuclear Medicine UCL Hospitals London CANCER Key facts Estimated 15.2 million new cases per year in 2015 worldwide
Larry Tan, MD Thoracic Surgery, HSC. Community Cancer Care Educational Conference October 27, 2017
 Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Larry Tan, MD Thoracic Surgery, HSC Community Cancer Care Educational Conference October 27, 2017 To describe patient referral & triage for the patient with suspected lung cancer To describe the initial
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
THYROID NODULES: THE ROLE OF ULTRASOUND
 THYROID NODULES: THE ROLE OF ULTRASOUND NOVEMBER 2017 DR. DEAN DURANT DEFINITION Thyroid nodule: Focal area within the thyroid gland with echogenicity different from surrounding parenchyma. THYROID NODULES
THYROID NODULES: THE ROLE OF ULTRASOUND NOVEMBER 2017 DR. DEAN DURANT DEFINITION Thyroid nodule: Focal area within the thyroid gland with echogenicity different from surrounding parenchyma. THYROID NODULES
GUIDELINES FOR CANCER IMAGING Lung Cancer
 GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
GUIDELINES FOR CANCER IMAGING Lung Cancer Greater Manchester and Cheshire Cancer Network Cancer Imaging Cross-Cutting Group April 2010 1 INTRODUCTION This document is intended as a ready reference for
PET/CT in Gynaecological Cancers. Stroobants Sigrid, MD, PhD Departement of Nuclear Medicine University Hospital,Antwerp
 PET/CT in Gynaecological Cancers Stroobants Sigrid, MD, PhD Departement of Nuclear Medicine University Hospital,Antwerp Cervix cancer Outline of this talk Initial staging Treatment monitoring/guidance
PET/CT in Gynaecological Cancers Stroobants Sigrid, MD, PhD Departement of Nuclear Medicine University Hospital,Antwerp Cervix cancer Outline of this talk Initial staging Treatment monitoring/guidance
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
What is head and neck cancer? How is head and neck cancer diagnosed and evaluated? How is head and neck cancer treated?
 Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that start in the oral cavity, larynx, pharynx, salivary glands, nasal cavity or paranasal sinuses. They usually begin
Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that start in the oral cavity, larynx, pharynx, salivary glands, nasal cavity or paranasal sinuses. They usually begin
Imaging Tissue Response to Therapeutic Radiation
 1 Imaging Tissue Response to Therapeutic Radiation Sean P. Frigo, Ph.D. Assistant Professor Department of Human Oncology School of Medicine and Public Health University of Wisconsin Madison Slide 1 1 Based
1 Imaging Tissue Response to Therapeutic Radiation Sean P. Frigo, Ph.D. Assistant Professor Department of Human Oncology School of Medicine and Public Health University of Wisconsin Madison Slide 1 1 Based
The oncology specific domains TU, TR and RS: What to know as a statistical analyst
 Your statistical health consultancy CHM staying healthy CRO getting healthy TEMP WORK team health The oncology specific domains TU, TR and RS: What to know as a statistical analyst PhUSE EU Connect 2018,
Your statistical health consultancy CHM staying healthy CRO getting healthy TEMP WORK team health The oncology specific domains TU, TR and RS: What to know as a statistical analyst PhUSE EU Connect 2018,
Cardiopulmonary Imaging Original Research
 Cardiopulmonary Imaging Original Research Downloaded from www.ajronline.org by 46.3.2.112 on 2/11/18 from IP address 46.3.2.112. Copyright ARRS. For personal use only; all rights reserved Nishino et al.
Cardiopulmonary Imaging Original Research Downloaded from www.ajronline.org by 46.3.2.112 on 2/11/18 from IP address 46.3.2.112. Copyright ARRS. For personal use only; all rights reserved Nishino et al.
Short-Term Restaging of Patients with Non-small Cell Lung Cancer Receiving Chemotherapy
 ORIGINAL ARTICLE Short-Term Restaging of Patients with Non-small Cell Lung Cancer Receiving Chemotherapy John F. Bruzzi, FFRRCSI,* Mylene Truong, MD,* Ralph Zinner, MD Jeremy J. Erasmus, MD,* Bradley Sabloff,
ORIGINAL ARTICLE Short-Term Restaging of Patients with Non-small Cell Lung Cancer Receiving Chemotherapy John F. Bruzzi, FFRRCSI,* Mylene Truong, MD,* Ralph Zinner, MD Jeremy J. Erasmus, MD,* Bradley Sabloff,
PLACE LABEL HERE. Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form. RTOG Study No.
 Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form RTOG Study No. 0813 Case # Name RTOG Patient ID INSTRUCTIONS: Submit this form at the appropriate followup
Radiation Therapy Oncology Group Phase II - SBRT - Medically Inoperable I /II NSCLC Follow-up Form RTOG Study No. 0813 Case # Name RTOG Patient ID INSTRUCTIONS: Submit this form at the appropriate followup
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Prevent Cancer Foundation Quantitative Imaging Workshop XIII
 Status of the Quantitative Imaging Profile Lung Nodule Volume Assessment and Monitoring in Low Dose CT Screening Prevent Cancer Foundation Quantitative Imaging Workshop XIII June 13-14, 2016 David S. Gierada,
Status of the Quantitative Imaging Profile Lung Nodule Volume Assessment and Monitoring in Low Dose CT Screening Prevent Cancer Foundation Quantitative Imaging Workshop XIII June 13-14, 2016 David S. Gierada,
Breast Cancer. What is breast cancer?
 Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Emerging Referral Patterns for Whole-Body Diffusion Weighted Imaging (WB-DWI) in an Oncology Center
 in an Oncology Center") Emerging Referral Patterns for Whole-Body Diffusion Weighted Imaging (WB-DWI) in an Oncology Center Poster No.: C-1296 Congress: ECR 2014 Type: Scientific Exhibit Authors: G. Petralia 1, G. Conte 1, S.
Emerging Referral Patterns for Whole-Body Diffusion Weighted Imaging (WB-DWI) in an Oncology Center Poster No.: C-1296 Congress: ECR 2014 Type: Scientific Exhibit Authors: G. Petralia 1, G. Conte 1, S.
Emerging Techniques in Breast Imaging: Contrast-Enhanced Mammography and Fast MRI
 Emerging Techniques in Breast Imaging: Contrast-Enhanced Mammography and Fast MRI Lilian Wang, M.D. Breast Imaging Section Department of Radiology Northwestern Medicine Overview Rationale for new imaging
Emerging Techniques in Breast Imaging: Contrast-Enhanced Mammography and Fast MRI Lilian Wang, M.D. Breast Imaging Section Department of Radiology Northwestern Medicine Overview Rationale for new imaging
AN APPROACH FOR ASSESSMENT OF TUMOR VOLUME FROM MAMMOGRAPHY IN LOCALLY ADVANCED BREAST CANCER. Gupreet Singh
 Malaysian Journal of Medical Sciences, Vol. 15, No. 1, January 2008 (37-41) ORIGINAL ARTICLE AN APPROACH FOR ASSESSMENT OF TUMOR VOLUME FROM MAMMOGRAPHY IN LOCALLY ADVANCED BREAST CANCER Gupreet Singh
Malaysian Journal of Medical Sciences, Vol. 15, No. 1, January 2008 (37-41) ORIGINAL ARTICLE AN APPROACH FOR ASSESSMENT OF TUMOR VOLUME FROM MAMMOGRAPHY IN LOCALLY ADVANCED BREAST CANCER Gupreet Singh
Tool Support for Cancer Lesion Tracking and Quantitative Assessment of Disease Response
 Tool Support for Cancer Lesion Tracking and Quantitative Assessment of Disease Response Mia Levy, MD Vanderbilt University Daniel Rubin, MD Stanford University Tumor Response Assessment Objective criteria
Tool Support for Cancer Lesion Tracking and Quantitative Assessment of Disease Response Mia Levy, MD Vanderbilt University Daniel Rubin, MD Stanford University Tumor Response Assessment Objective criteria
CURRENT CT DOSE METRICS: MAKING CTDI SIZE-SPECIFIC
 CURRENT CT DOSE METRICS: MAKING CTDI SIZE-SPECIFIC Keith Strauss, MSc, FAAPM, FACR Cincinnati Children s Hospital University of Cincinnati College of Medicine Acknowledgments John Boone, PhD Michael McNitt-Grey,
CURRENT CT DOSE METRICS: MAKING CTDI SIZE-SPECIFIC Keith Strauss, MSc, FAAPM, FACR Cincinnati Children s Hospital University of Cincinnati College of Medicine Acknowledgments John Boone, PhD Michael McNitt-Grey,
GROUP 1: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases. Including: Excluding:
 GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
GROUP 1: Including: Excluding: Peripheral tumour with normal hilar and mediastinum on staging CT with no disant metastases Solid pulmonary nodules 8mm diameter / 300mm3 volume and BROCK risk of malignancy
Molecular Imaging in the Development of Cancer Therapeutics. Johannes Czernin
 Molecular Imaging in the Development of Cancer Therapeutics Johannes Czernin Ahmanson Biological Imaging Division University of California Los Angeles Cancer Statistics Cancer Type 5-year Survival Rate
Molecular Imaging in the Development of Cancer Therapeutics Johannes Czernin Ahmanson Biological Imaging Division University of California Los Angeles Cancer Statistics Cancer Type 5-year Survival Rate
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Optimized. clinical pathway. propels high utilization of PET/MR at Pitié-Salpêtrière Hospital
 Optimized propels high utilization of PET/MR at Pitié-Salpêtrière Hospital clinical pathway As one of Europe s largest teaching hospitals, Pitié-Salpêtrière Hospital is renowned for its innovative research
Optimized propels high utilization of PET/MR at Pitié-Salpêtrière Hospital clinical pathway As one of Europe s largest teaching hospitals, Pitié-Salpêtrière Hospital is renowned for its innovative research
Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C.
 Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
Role of Whole-body Diffusion MR in Detection of Metastatic lesions Prof. Dr. NAGUI M. ABDELWAHAB,M.D.; MARYSE Y. AWADALLAH, M.D. AYA M. BASSAM, Ms.C. Cancer is a potentially life-threatening disease,
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University
 objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
objectives Pitfalls and Pearls in PET/CT imaging Kevin Robinson, DO Assistant Professor Department of Radiology Michigan State University To determine the regions of physiologic activity To understand
MEDIASTINAL STAGING surgical pro
 MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
MEDIASTINAL STAGING surgical pro Paul E. Van Schil, MD, PhD Department of Thoracic and Vascular Surgery University of Antwerp, Belgium Mediastinal staging Invasive techniques lymph node mapping cervical
PET/CT for Therapy Assessment in Oncology
 PET/CT for Therapy Assessment in Oncology Rodolfo Núñez Miller, M.D. Nuclear Medicine Section Division of Human Health International Atomic Energy Agency Vienna, Austria Clinical Applications of PET/CT
PET/CT for Therapy Assessment in Oncology Rodolfo Núñez Miller, M.D. Nuclear Medicine Section Division of Human Health International Atomic Energy Agency Vienna, Austria Clinical Applications of PET/CT
SELF-ASSESSMENT MODULE REFERENCE SPR 2018 Oncologic Imaging Course Adrenal Tumors November 10, :00 12:10 p.m.
 SELF-ASSESSMENT MODULE REFERENCE SPR 2018 Oncologic Imaging Course Adrenal Tumors November 10, 2018 10:00 12:10 p.m. Staging Susan E. Sharp, MD 1. In the International Neuroblastoma Risk Group Staging
SELF-ASSESSMENT MODULE REFERENCE SPR 2018 Oncologic Imaging Course Adrenal Tumors November 10, 2018 10:00 12:10 p.m. Staging Susan E. Sharp, MD 1. In the International Neuroblastoma Risk Group Staging
Molecular Imaging and Cancer
 Molecular Imaging and Cancer Cancer causes one in every four deaths in the United States, second only to heart disease. According to the U.S. Department of Health and Human Services, more than 512,000
Molecular Imaging and Cancer Cancer causes one in every four deaths in the United States, second only to heart disease. According to the U.S. Department of Health and Human Services, more than 512,000
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer
 Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Endobronchial Ultrasound in the Diagnosis & Staging of Lung Cancer Dr Richard Booton PhD FRCP Lead Lung Cancer Clinician, Consultant Respiratory Physician & Speciality Director Manchester University NHS
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Measuring Response in Solid Tumors: Comparison of RECIST and WHO Response Criteria
 Jpn J Clin Oncol 2003;33(10)533 537 Measuring Response in Solid Tumors: Comparison of RECIST and WHO Response Criteria Joon Oh Park 1, Soon Il Lee 1, Seo Young Song 1, Kihyun Kim 1, Won Seog Kim 1, Chul
Jpn J Clin Oncol 2003;33(10)533 537 Measuring Response in Solid Tumors: Comparison of RECIST and WHO Response Criteria Joon Oh Park 1, Soon Il Lee 1, Seo Young Song 1, Kihyun Kim 1, Won Seog Kim 1, Chul
COLORECTAL CANCER STAGING in 2010
 COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
COLORECTAL CANCER STAGING in 2010 Robert A. Halvorsen, MD, FACR MCV Hospitals / VCU Medical Center Richmond, Virginia I do not have any relevant financial relationships with any commercial interests COLON
Head and Neck Cancer. What is head and neck cancer?
 Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that usually originate in the squamous cells that line the mouth, nose and throat. Typical symptoms include a persistent
Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that usually originate in the squamous cells that line the mouth, nose and throat. Typical symptoms include a persistent
Innovations in Lung Cancer Diagnosis and Surgical Treatment
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
RADIOLOGIC TECHNOLOGY (526)
") RADIOLOGIC TECHNOLOGY (526) 526-133 DMS General Procedures 2 Radiologic Technology (526) 1 526-130 Introduction to Diagnostic Medical Sonography This course introduces the student to the history of ultrasound
RADIOLOGIC TECHNOLOGY (526) 526-133 DMS General Procedures 2 Radiologic Technology (526) 1 526-130 Introduction to Diagnostic Medical Sonography This course introduces the student to the history of ultrasound
Elastosonography. Prof. Massimo Midiri Direttore Istituto di Radiologia Policlinico Universitario Paolo Giaccone Diagnostica per Immagini, - Palermo
 Elastosonography Prof. Massimo Midiri Direttore Istituto di Radiologia Policlinico Universitario Paolo Giaccone Diagnostica per Immagini, - Palermo everybody has certainly had, at least once in a lifetime,
Elastosonography Prof. Massimo Midiri Direttore Istituto di Radiologia Policlinico Universitario Paolo Giaccone Diagnostica per Immagini, - Palermo everybody has certainly had, at least once in a lifetime,
3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast
 1 Angela Kempen February Case Study February 22, 2012 3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast History of Present Illness: JE is a 45 year-old Caucasian female who underwent
1 Angela Kempen February Case Study February 22, 2012 3D Conformal Radiation Therapy for Mucinous Carcinoma of the Breast History of Present Illness: JE is a 45 year-old Caucasian female who underwent
Targeting and Treating Cancer
 Targeting and Treating Cancer Mark R. Baker, Chief Executive Officer Jefferies Healthcare Conference June 2015 Disclosure Notice This presentation may contain projections and other forward-looking statements
Targeting and Treating Cancer Mark R. Baker, Chief Executive Officer Jefferies Healthcare Conference June 2015 Disclosure Notice This presentation may contain projections and other forward-looking statements
What makes Oncology special? Johanna MURSIC, Indication Programmer PhUSE congress Budapest, October 15 th 2012
 What makes Oncology special? Johanna MURSIC, Indication Programmer PhUSE congress Budapest, October 15 th 2012 Disclaimer The opinions expressed in this presentation and on the following slides are solely
What makes Oncology special? Johanna MURSIC, Indication Programmer PhUSE congress Budapest, October 15 th 2012 Disclaimer The opinions expressed in this presentation and on the following slides are solely
Measure #405: Appropriate Follow-up Imaging for Incidental Abdominal Lesions National Quality Strategy Domain: Effective Clinical Care
 Measure #405: Appropriate Follow-up Imaging for Incidental Abdominal Lesions National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION:
Measure #405: Appropriate Follow-up Imaging for Incidental Abdominal Lesions National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION:
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous