Management of pt1 polyps. Maria Pellise
|
|
|
- Alicia Crawford
- 5 years ago
- Views:
Transcription
1 Management of pt1 polyps Maria Pellise






")

2 Early colorectal cancer Malignant polyp Screening programmes SM Invasive adenocar cinoma Advances in diagnostic & therapeutic endoscopy pt1 polyps % of large-bowel polyps removed in general diagnostic colonoscopy practice 10% of detected cancers (British BCSP) Logan RF etal. Gut 2012; You NC, Ann Surg 2007; Williams et al. Colorectal Dise 2013

3 Early Cancers Classification According to Depth of Invasion Tis T1 T1sm T2 m1 m2 m3 sm1 sm2 sm3 Epithelial Layer Lamina Propria Muscularis Mucosae Submucosa Muscularis Propria Lymphatic involvment ENDOSCOPIC TREATMENT

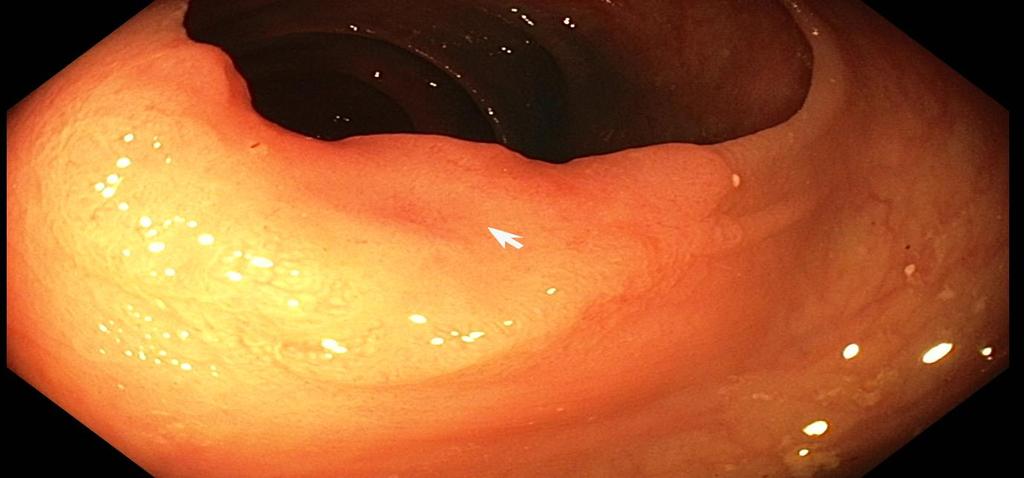
4 M, 57yo, FIT + 10mm rectal sessile polyp; 8cm from anal verge mpellise@clinic.cat


5 Invasive adenocarcinoma within a tubular adenoma Tumor size: 8mm Adenoma size: 9mm Depth of submucosal invasion: 2mm Low grade histology (moderatelly differenciated) Absence of lymphovascular invasion Absence of perineural invasion Negative margin ptnm Staging: pt1 mpellise@clinic.cat



6 Recurrence can be lethal BANKER Recurrence rate: 1 5% GAMBLER SURGERY Morbidity Anastomotic leak - mortality rate up to 3-6% Costs FOLLOW-UP Under-staging Local recurrence Systemic recurrence mpellise@clinic.cat

7 Management of pt1 polyps No RCT Heterogeneity and deficiencies in reporting histology Heterogeneity and deficiencies in reporting endoscopic data Surgical series Different outcomes measures Clinical significant outcomes are rare events



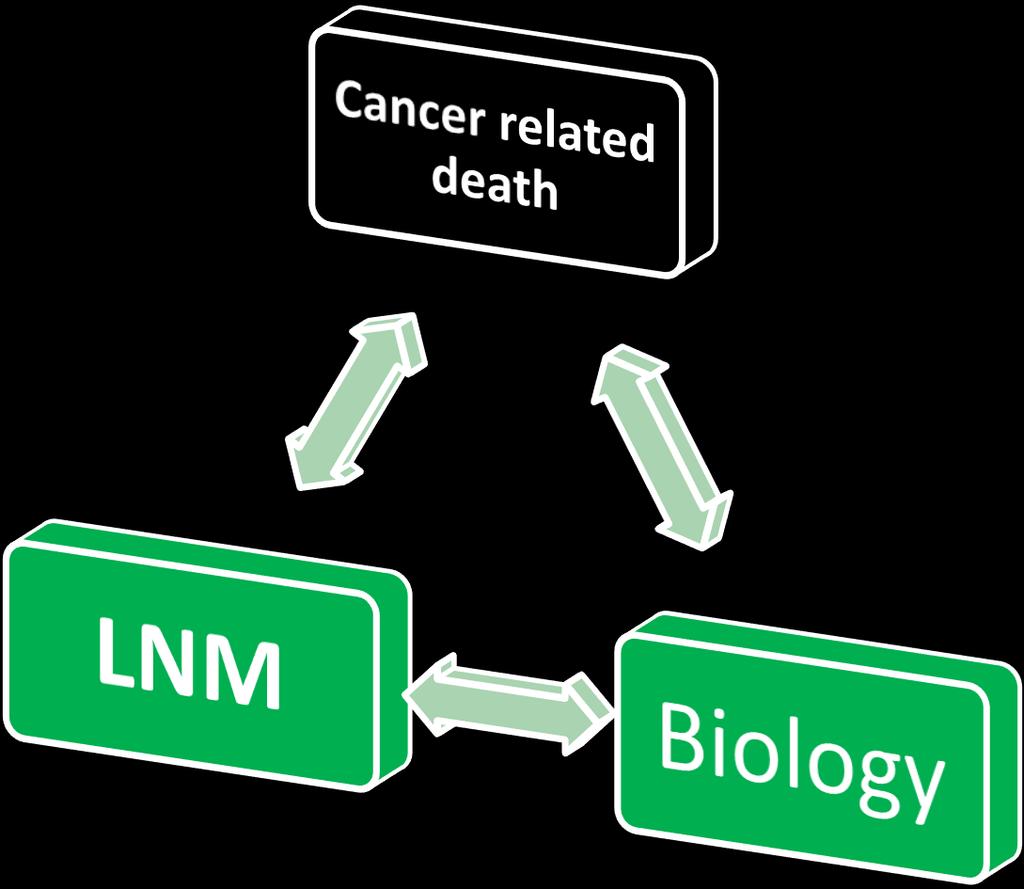
8 Cancer related death Local recurrence Lymphatic spread Vascular spread Intermediate endpoint Incidence of synchronous LNM in pt1= 6 12% mpellise@clinic.cat
9 Risk factors for LNM in pt1 surgical series: poor differentiation lymphovascular invasion presence of positive (R1) or unable to determine (Rx) resection margins deep submucosal invasion (i.e., 1,000 μ m/sm2 3 in non-pedunculated tumors, and Haggitt 4 in pedunculated tumors) presence of intense tumor budding Rectal location Sessile or flat morphology Clusters of undifferentiated cells mpellise@clinic.cat

10 Systematic review Risk of LNM Bosch et al. Endoscopy 2013


11 Accuracy for predicting LNM Bosch et al. Endoscopy 2013
12 Indications for additional treatment NCCN ESMO JSCCR Tumor differentiation + (grade 3,4) + (grade 3) + (poorly di; signet ring;mucinous) Lymphatic invasion Vascular invasion Resection margin (vertical) Submucosal depth invasion + (Level 4) + (> 1mm) Tumor budding + (grade 2 or 3) Network NCC. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Rectal Cancer (Version ). 2017, DOI: Labianca R, Nordlinger B, Beretta GD et al. Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO 2013; 24 Suppl 6: vi64-72 Watanabe T, Muro K, Ajioka Y et al. Japanese Society for Cancer of the Colon and Rectum (JSCCR) guidelines 2016 for the treatment of colorectal cancer. International journal of clinical oncology 2017,


13 Artificial intelligence predictive model Ichimasa K et al. Endosocpy 2018


14 It is not clear that surgery of a pt1 completely resected with high risk for LNM decreases mortality mpellise@clinic.cat









15

16 Dutch T1 CRC working group Retrospective cohort study. Patients with T1 CRC diagnosed between 2000 and 2014 in 1 academic and 12 non-academic hospitals. Netherlands Cancer Registry. Median follow-up time of 36.5 months (interquartile range ) Patients with pt1 CRC Hospitals N=2253 Patients included N= pedunculated 905 sessile or flat morphology high-risk T1 CRC if one or more: poor differentiation, deep submucosal invasion (i.e., 1,000 μ m/sm2 3 in non-pedunculated tumors, and Haggitt 4 in pedunculated tumors), lymphovascular invasion, positive (R1) or unable to determine (Rx) resection margins. R0 resectionwas defined as a cancer-free resection margin irrespective of distance in millimeters. Endoscopic resection only Wait and see N= 519 Endoscopic resection of pt1crc N= 925 Macroscopic complete resection N= 877 Secondary surgery N= 358 Primary surgical resection N=758 Including TAMIS N =105 Low risk N= 121 High risk N= 198 Unknown N= 200 High risk N= 602 Including N= 282 of secondary surgeries Backes Y et al. Am J Gastro 2017; Overwater et al. Gut 2018; Bakes Y Gastroenterol 2018 Surgical resection and low risk or undefinable risk N= 440 Including secondary surgeries low risk N=19; unknown N=57

17 Dutch T1 CRC working group Endoscopic resection before surgical resection of a high-risk T1 CRC has no adverse effect. Of all T1 CRCs treated with surgical resection, still 5% develops a local or distant recurrence. CRC-related death among patients with recurrence: 41.7% The decision to conduct a wait-and-see policy in high-risk T1 CRC should be cautiously made given the poor prognosis when cancer recurs Previous biopsies of the scar negative for cancerous tissue did not guarantee recurrence free survival. There is an increasing need for identification of malignant polyps before endoscopic resection to guide resection technique and optimise specimen handling Backes Y et al. Am J Gastro 2017; Overwater et al. Gut 2018; Bakes Y Gastroenterol 2018

18 Scottish screening programme N= 485 Follow up =50 months (minimum 16 months). Cancer related death = 1.3%-2.8% ONLY! Systemic recurrence > local recurrence ¾ undergo surgery have no evidence of residual tumor independent predictors of residual tumour, disease recurrence and cancer-related death: evidence of lymphovascular invasion Incomplete excision Therapeutic technique Richards CH, Gut 2018
")


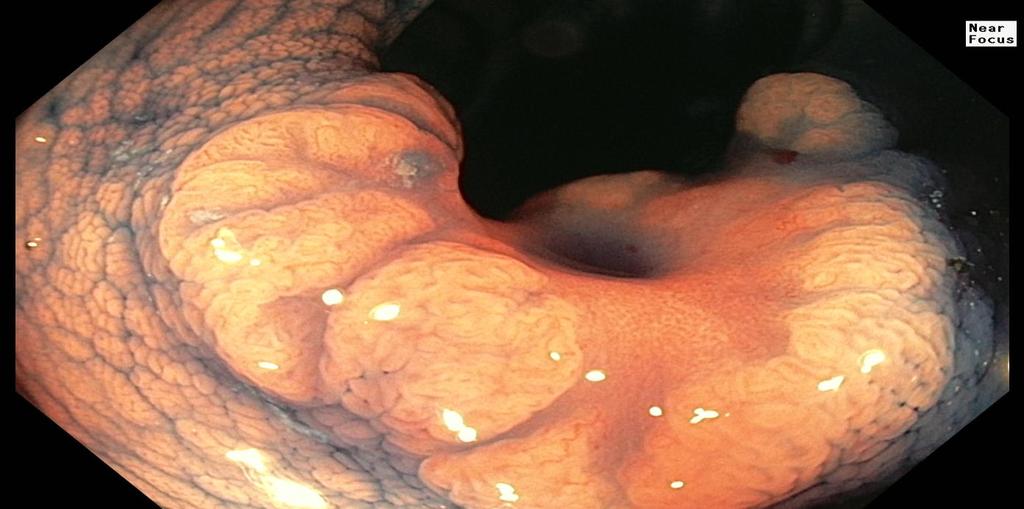
19 F, 65, FIT(+) sigmoid



20 M, 65, FIT+ Sigmoid colon pt1 good prognosis. Margin < 1mmL
21





22 Polypoid Paris classification Pedunculated: 0-Ip Sessile: 0-Is Mixed: 0-Isp % sm invasion 11-15mm: 8% 16-20mm: 17% >20mm: more Non polypoid Slightly elevated Totally flat Slightly depressed Lambert R, Lightdale C. Gastrointest Endosc 2003;58 suppl6 Lambert R et al. Endoscopy 2005;37: Kudo et al. Gastrointest endosc 2008;63:suppl mm: 2% 16-20mm: 10% 6-10mm:44% 11-15mm: 67% 16-20mm: 90%

23 Burgess et al. Gastroenterol 2018


24 Superficial focal interrogation: Pit & Microvascular pattern



")
25 Sano, Dig Endosc 2006 Kudo S, J Clin Pathol 1994 Japan NBI Expert Team (JNET) (2016) Sumimoto GIE 2017



26 NBI International Colorectal Endoscopic classification (NICE) Type 1 Type 2 Type 3 Color Vessels Surface Most likely histology Hyperplastic Adenoma Deep submucosal invasion
27 58 endoscopists 17 centers Polyps > 10mm Prediction of deep SM invasion Elegible participants n=1650 Participants included n=1634 Lesions included n=2136 Excluded n=16 No histology n=4 Non-deep invasion No NICE 3 n=2004 Deep invasion NICE 3 n=132 Non-deep invasion Deep invasion n= % n=37 1.9% n= % n= % No histology n=7 mpellise@clinic.cat Puig et al. under revision

28 NICE classification p<0.001 Depressed area NO p<0.001 YES Pedunculated p=0.007 YES NO Non-deep invasion Deep invasion Similar results for LNM risks LST-G nodular mixed type p<0.001 Ulceration p=0.026 NO YES NO YES 93% 1% 8.6% 9.7% 13% 44% n=1812 n=93 n=93 n=31 n=80 n=14 Puig et al. Under revision





29 NICE classification Endoscopic treatment Uncertain (personalize) Surgery 0,7% Depressed area LST-G nodular mixed type NO NO YES YES Pedunculated YES Ulceration NO NO YES 1% 9% 10% 13% 44% 93% 12,5% 86,8% NICE type 2 with depressed areas, NICE type 2 nodular mixed type NICE type 3 nonpedunculated polyps without ulceration Puig et al. under revision

30 Final Remarks (Too) Many open questions! Imperative need for: standardisation of histological criteria, endoscopic description Multidisciplinary consensus protocols Large prospective cohort studies Prospective randomised controlled trials? Improve identification of malignant polyps before endoscopic resection: In large polyps in small polyps Talk to your pathologist! Talk to your surgeon!
31 Thank you!!
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD
 SNARE THE CASE FOR EMR AND ESD") THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
THE BIG, AWKWARD, FLAT POLYP THAT CAN T BE REMOVED WITH A (SINGLE) SNARE THE CASE FOR EMR AND ESD Surgical Oncology Network meeting Dr. Eric Lam MD FRCPC October 14, 2017 DISCLOSURES None OBJECTIVES Appreciate
Large polyps: EMR, ESD, TEM and segmental resection. Terry Phang 2017 SON fall update
 Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Large polyps: EMR, ESD, TEM and segmental resection Terry Phang 2017 SON fall update Key Points: Large polyps No RCT re: Recurrence, complications Piecemeal vs en bloc: EMR vs ESD Partial vs full-thickness:
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
The Paris classification of colonic lesions
 The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
The Paris classification of colonic lesions Training to improve the interobserver agreement among international experts Sascha van Doorn, MD, PhD-student in CRC-reserach group of Evelien Dekker Introduction
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions
 Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
Diagnostic accuracy of pit pattern and vascular pattern in colorectal lesions Digestive Disease Center, Showa University Northern Yokohama Hospital Department of Pathology Yoshiki Wada, Shin-ei Kudo, Hiroshi
ESD for EGC with undifferentiated histology
 ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
ESD for EGC with undifferentiated histology Jun Haeng Lee, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea Biopsy: M/D adenocarcinoma ESD: SRC >>
Formula One Study. Assessment criteria of pathological parameters. Ver.2. UK Japan Joint Study for Risk Factors of Lymph Node
 APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
APPENDIX 01: Assessment criteria Formula One Study UK Japan Joint Study for Risk Factors of Lymph Node Metastasis in Submucosal Invasive (pt1) Colorectal Cancer Assessment criteria of pathological parameters
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Endoscopic Corner CASE 1. Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R
 170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
170 Endoscopic Corner Kimtrakool S Aniwan S Linlawan S Muangpaisarn P Sallapant S Rerknimitr R CASE 1 A 54-year-old woman underwent a colorectal cancer screening. Her fecal immunochemical test was positive.
Treatment Strategy for Non-curative Resection of Early Gastric Cancer. Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea
 Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Treatment Strategy for Non-curative Resection of Early Gastric Cancer Jun Haneg Lee. Sungkyunkwan University, Samsung Medical Center, Seoul Korea Classic EMR/ESD data analysis style Endoscopic resection
Colon Polyps: Detection, Inspection and Characteristics
 Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Colon Polyps: Detection, Inspection and Characteristics Stephen Kim, M.D. Assistant Professor of Medicine Interventional Endoscopy Services UCLA Division of Digestive Diseases September 29, 2018 1 Disclosures
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
COLON: Innovations 3 steps, 3 parts..
 COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
COLON: Innovations 3 steps, 3 parts.. Detection: I see an abnormality (usually a polyp) Characterization: Is this abnormality neoplastic? (for example: an adenoma) Treatment: it is neoplastic. Can I treat
Pathology in Slovenian CRC screening programme: Organisation and quality assurance. Snježana Frković Grazio and Matej Bračko
 Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia
 Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
Chromoendoscopy and Endomicroscopy for detecting colonic dysplasia Ralf Kiesslich I. Medical Department Johannes Gutenberg University Mainz, Germany Cumulative cancer risk in ulcerative colitis 0.5-1.0%
EMR, ESD and Beyond. Peter Draganov MD. Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida
 EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
EMR, ESD and Beyond Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated by Endoscopy
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
05/07/2018. What colorectal cancer screening is all about. Not so simple pathology: issues from the screening programme
 Not so simple pathology: issues from the screening programme Professor Neil A Shepherd Gloucester & Cheltenham, UK What colorectal cancer screening is all about. detecting early stage cancer D 25% A 8%
Not so simple pathology: issues from the screening programme Professor Neil A Shepherd Gloucester & Cheltenham, UK What colorectal cancer screening is all about. detecting early stage cancer D 25% A 8%
Paris classification (2003) 삼성의료원내과이준행
 삼성의료원내과이준행") Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Paris classification (2003) 삼성의료원내과이준행 JGCA classification - Japanese Gastric Cancer Association - Type 0 superficial polypoid, flat/depressed, or excavated tumors Type 1 polypoid carcinomas, usually attached
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER?
 CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
Dysplasia 4/19/2017. How do I practice Chromoendoscopy for Surveillance of Colitis? SCENIC: Polypoid Dysplasia in UC. Background
 SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
SCENIC: Polypoid in UC Definition How do I practice for Surveillance of Colitis? Themos Dassopoulos, M.D. Director, BSW Center for IBD Themistocles.Dassopoulos@BSWHealth.org Tel: 469-800-7189 Cell: 314-686-2623
Bowel Screening Colonoscopy in Glasgow How well are we doing? How well should we be doing? How can we evidence and improve performance?
 Bowel Screening Colonoscopy in Glasgow 2017 How well are we doing? How well should we be doing? How can we evidence and improve performance? Bowel Screening Standards - Scotland Definitions Completion
Bowel Screening Colonoscopy in Glasgow 2017 How well are we doing? How well should we be doing? How can we evidence and improve performance? Bowel Screening Standards - Scotland Definitions Completion
IN THE DEVELOPMENT and progression of colorectal
 Digestive Endoscopy 2014; 26 (Suppl. 2): 73 77 doi: 10.1111/den.12276 Treatment strategy of diminutive colorectal polyp
Digestive Endoscopy 2014; 26 (Suppl. 2): 73 77 doi: 10.1111/den.12276 Treatment strategy of diminutive colorectal polyp
Large Colorectal Adenomas An Approach to Pathologic Evaluation
 Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Anatomic Pathology / LARGE COLORECTAL ADENOMAS AND PATHOLOGIC EVALUATION Large Colorectal Adenomas An Approach to Pathologic Evaluation Elizabeth D. Euscher, MD, 1 Theodore H. Niemann, MD, 1 Joel G. Lucas,
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Short and longterm outcomes after endoscopic resection of malignant polyps.
 Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Short and longterm outcomes after endoscopic resection of malignant polyps. Short and longterm outcomes High risk features Lymph node metastasis Lymph node metastases sm1 sm2 sm3 Son 2008 3.1 % 14.9% 25.0
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications
 Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Adenoma and Malignant Colorectal Polyp: Pathological Considerations and Clinical Applications Authors: *Emil Salmo, 1 Najib Haboubi 2 1. Department of Histopathology, The Pennine Acute Hospitals NHS Trust,
Do any benign polyps require an operation?
 Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
Do any benign polyps require an operation? Kevin Waschke MD.,CM., FRCPC, FASGE McGill University Health Center President Elect Canadian Association of Gastroenterology Colonoscopy Education Day - Tuesday
Emerging Interventions in Endoscopy. Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital
 Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Emerging Interventions in Endoscopy Margaret Vance Nurse Consultant in Gastroenterology St Mark s Hospital Colon Cancer Colon cancer is common. 1 in 20 people in the UK will develop the disease 19 000
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma
 Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Polypectomy and Local Resections of the Colorectum Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth
Seventh Edition Staging 2017 Colorectum. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
The malignant colorectal polyp
 The malignant colorectal polyp Dr Ian Brown Envoi Pathology Envoi data reproduced from J Clin Path 2015 article Definition Adenocarcinoma found in an endoscopically resected polypoidal tumour Submucosal
The malignant colorectal polyp Dr Ian Brown Envoi Pathology Envoi data reproduced from J Clin Path 2015 article Definition Adenocarcinoma found in an endoscopically resected polypoidal tumour Submucosal
Rectal EMR: Techniques and Tips
 Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
Rectal EMR: Techniques and Tips Dr Paul Urquhart Epworth Eastern Eastern Health (Head of Endoscopy) The context of EMR Basic Technique Recurrence Perforation Bleeding Introduction 1 I don t treat rectal
How to characterize dysplastic lesions in IBD?
 How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
How to characterize dysplastic lesions in IBD? Name: Institution: Helmut Neumann, MD, PhD, FASGE University Medical Center Mainz What do we know? Patients with IBD carry an increased risk of developing
Endoscopic Submucosal Dissection ESD
 Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
Endoscopic Submucosal Dissection ESD Peter Draganov MD Professor of Medicine Division of Gastroenterology, Hepatology and Nutrition University of Florida Gastrointestinal Cancer Lesion that Can be Treated
ADENOMAS WITH ADENOCARCINOMA: A STUDY EVALUATING THE RISK OF RESIDUAL CANCER AND LYMPH NODE METASTASIS
 253SJS102210.1177/1457496913482253S. E. Steigen, et al.adenomas with adenocarcinomas and risk factors Scandinavian Journal of Surgery 102: 90 95, 2013 ADENOMAS WITH ADENOCARCINOMA: A STUDY EVALUATING THE
253SJS102210.1177/1457496913482253S. E. Steigen, et al.adenomas with adenocarcinomas and risk factors Scandinavian Journal of Surgery 102: 90 95, 2013 ADENOMAS WITH ADENOCARCINOMA: A STUDY EVALUATING THE
Page 1. Is the Risk This High? Dysplasia in the IBD Patient. Dysplasia in the Non IBD Patient. Increased Risk of CRC in Ulcerative Colitis
 Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Screening for Colorectal Neoplasia in Inflammatory Bowel Disease Francis A. Farraye MD, MSc Clinical Director, Section of Gastroenterology Co-Director, Center for Digestive Disorders Boston Medical Center
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Felix W. Leung 1,2,3. Editorial
 Editorial Incomplete resection after macroscopic radical endoscopic resection of T1 colorectal cancer should a paradigm-changing approach to address the risk be considered? Felix W. Leung 1,2,3 1 Sepulveda
Editorial Incomplete resection after macroscopic radical endoscopic resection of T1 colorectal cancer should a paradigm-changing approach to address the risk be considered? Felix W. Leung 1,2,3 1 Sepulveda
How to treat early gastric cancer? Endoscopy
 How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
How to treat early gastric cancer? Endoscopy Presented by Pierre H. Deprez Institution Cliniques universitaires Saint-Luc, Brussels Université catholique de Louvain 2 3 4 5 6 Background Diagnostic or therapeutic
Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate
 Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate Authors Yasuhiro Abe 1,HaruakiNabeta 1, Ryota Koyanagi 1, Taro Nakamichi 1, Hayato Hirashima 1, Alan Kawarai
Extended cold snare polypectomy for small colorectal polyps increases the R0 resection rate Authors Yasuhiro Abe 1,HaruakiNabeta 1, Ryota Koyanagi 1, Taro Nakamichi 1, Hayato Hirashima 1, Alan Kawarai
PAPER. Review of Results After Endoscopic and Surgical Therapy
 Rectal Carcinoid Tumors PAPER Review of Results After Endoscopic and Surgical Therapy Mary R. Kwaan, MD, MPH; Joel E. Goldberg, MD; Ronald Bleday, MD Objective: To assess whether endoscopic treatment can
Rectal Carcinoid Tumors PAPER Review of Results After Endoscopic and Surgical Therapy Mary R. Kwaan, MD, MPH; Joel E. Goldberg, MD; Ronald Bleday, MD Objective: To assess whether endoscopic treatment can
Malignant colorectal polyps: venous invasion and
 774 Gut, 1991,32, 774-778 Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy Department of Pathology J M Geraghty Endoscopy Unit C B Williams and ICRF Colorectal
774 Gut, 1991,32, 774-778 Malignant colorectal polyps: venous invasion and successful treatment by endoscopic polypectomy Department of Pathology J M Geraghty Endoscopy Unit C B Williams and ICRF Colorectal
Expert panel observations
 Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Expert panel observations Professor Neil A Shepherd Gloucester and Cheltenham, UK Gloucestershire Cellular Pathology Laboratory Three big issues in BCSP pathology serrated pathology & what do we do about
Histopathologic risk factors for lymph node metastasis in patients with T1 colorectal cancer
 ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 https://doi.org/10.4174/astr.2017.93.5.266 Annals of Surgical Treatment and Research Histopathologic risk factors for lymph node metastasis in patients
ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 https://doi.org/10.4174/astr.2017.93.5.266 Annals of Surgical Treatment and Research Histopathologic risk factors for lymph node metastasis in patients
When is local excision appropriate for early rectal cancer?
 Surg Today (2014) 44:2000 2014 DOI 10.1007/s00595-013-0766-3 REVIEW ARTICLE When is local excision appropriate for early rectal cancer? Kotaro Maeda Yoshikazu Koide Hidetoshi Katsuno Received: 12 July
Surg Today (2014) 44:2000 2014 DOI 10.1007/s00595-013-0766-3 REVIEW ARTICLE When is local excision appropriate for early rectal cancer? Kotaro Maeda Yoshikazu Koide Hidetoshi Katsuno Received: 12 July
BC CRC Update Malignant Polyp Who Needs Surgery
 BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
BC CRC Update Malignant Polyp Who Needs Surgery Anthony MacLean, MD, FRCSC, FACS, FASCRS Colorectal Surgeon Foothills Medical Centre Clinical Associate Professor of Surgery and Oncology University of Calgary
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
위암내시경진단 (2019) - 융기형위암을중심으로 성균관대학교의과대학내과이준행
 - 융기형위암을중심으로 성균관대학교의과대학내과이준행") 위암내시경진단 (2019) - 융기형위암을중심으로 성균관대학교의과대학내과이준행 위암내시경진단 (2019) 위암검진에대한짧지않은 comment 융기형암은융기되어있는가? 함몰형암은함몰되어있는가? Semi-pedunculated polyp Sentinel polyp or EGJ cancer? IIa + IIc 위암검진에대한짧지않은 comment 성균관대학교의과대학내과이준행
위암내시경진단 (2019) - 융기형위암을중심으로 성균관대학교의과대학내과이준행 위암내시경진단 (2019) 위암검진에대한짧지않은 comment 융기형암은융기되어있는가? 함몰형암은함몰되어있는가? Semi-pedunculated polyp Sentinel polyp or EGJ cancer? IIa + IIc 위암검진에대한짧지않은 comment 성균관대학교의과대학내과이준행
Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens
 ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
ISPUB.COM The Internet Journal of Pathology Volume 12 Number 1 Morphologic Criteria of Invasive Colonic Adenocarcinoma on Biopsy Specimens C Rose, H Wu Citation C Rose, H Wu.. The Internet Journal of Pathology.
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus
 Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Histopathology of Endoscopic Resection Specimens from Barrett's Esophagus Br J Surg 38 oct. 1950 Definition of Barrett's esophagus A change in the esophageal epithelium of any length that can be recognized
Difficult Polypectomy 2015 Tool of the Trade
 Difficult Polypectomy 2015 Tool of the Trade Jonathan Cohen, MD FACG FASGE Clinical Professor of Medicine NYU Langone School of Medicine Improving Therapeutics in the Colon Improved detection of polyp
Difficult Polypectomy 2015 Tool of the Trade Jonathan Cohen, MD FACG FASGE Clinical Professor of Medicine NYU Langone School of Medicine Improving Therapeutics in the Colon Improved detection of polyp
Update on Colonic Serrated (and Conventional) Adenomatous Polyps
 Adenomatous Polyps") Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
Update on Colonic Serrated (and Conventional) Adenomatous Polyps Maui, HI 2018 Robert D. Odze, MD, FRCPC Chief, Division of GI Pathology Professor of Pathology Brigham and Women s Hospital Harvard Medical
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Gastric Polyps. Bible class
 Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Gastric Polyps Bible class 29.08.2018 Starting my training in gastroenterology, some decades ago, my first chief always told me that colonoscopy may seem technically more challenging but gastroscopy has
Missed Lesions at Endoscopy. Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand
 Missed Lesions at Endoscopy Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand Missed Lesions at Endoscopy Is there a problem? With Gastroscopy
Missed Lesions at Endoscopy Dr Russell Walmsley, MD, FRCP, FRACP Gastroenterologist WDHB Chair Endoscopy Guidance Group for New Zealand Missed Lesions at Endoscopy Is there a problem? With Gastroscopy
European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition
 SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
SE116 European guidelines for quality assurance in colorectal cancer screening and diagnosis. First Edition Quality assurance in pathology in colorectal cancer screening and diagnosis Co-Funded by the
Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations
 Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Virchows Arch (2011) 458:1 19 DOI 10.1007/s00428-010-0977-6 REVIEW AND PERSPECTIVE Quality assurance in pathology in colorectal cancer screening and diagnosis European recommendations Phil Quirke Mauro
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases
 Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Diagnostic and Therapeutic Approaches to Dysplasia in Inflammatory Bowel Diseases Parakkal Deepak, M.B.B.S., M.S. Assistant Professor of Medicine Division of Gastroenterology John T. Milliken Department
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Experience and challenges of implementing optical diagnosis into clinical practice UK and European Perspective
 Experience and challenges of implementing optical diagnosis into clinical practice UK and European Perspective WEO Image Enhanced Endoscopy San Diego, USA Dr James East Consultant Gastroenterologist Honorary
Experience and challenges of implementing optical diagnosis into clinical practice UK and European Perspective WEO Image Enhanced Endoscopy San Diego, USA Dr James East Consultant Gastroenterologist Honorary
Current status of gastric ESD in Korea. Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea
 Current status of gastric ESD in Korea Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea Contents Brief history of gastric ESD in Korea ESD/EMR for gastric adenoma
Current status of gastric ESD in Korea Jun Haeng Lee. Department of Medicine Sungkyunkwanuniversity School of Medicie, Seoul, Korea Contents Brief history of gastric ESD in Korea ESD/EMR for gastric adenoma
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Clinicopathological Characteristics of Superficial Type
 Diagnostic and Therapeutic Endoscopy, 1995, Vol. 2, pp. 99-105 Reprints available directly from the publisher Photocopying permitted by license only (C) 1995 Harwood Academic Publishers GmbH Printed in
Diagnostic and Therapeutic Endoscopy, 1995, Vol. 2, pp. 99-105 Reprints available directly from the publisher Photocopying permitted by license only (C) 1995 Harwood Academic Publishers GmbH Printed in
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Clinical Study Endoscopic Submucosal Dissection for Early Colorectal Neoplasms: Clinical Experience in a Tertiary Medical Center in Taiwan
 Gastroenterology Research and Practice Volume 2013, Article ID 891565, 7 pages http://dx.doi.org/10.1155/2013/891565 Clinical Study Endoscopic Submucosal Dissection for Early Colorectal Neoplasms: Clinical
Gastroenterology Research and Practice Volume 2013, Article ID 891565, 7 pages http://dx.doi.org/10.1155/2013/891565 Clinical Study Endoscopic Submucosal Dissection for Early Colorectal Neoplasms: Clinical
The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions
 Acta Medica Marisiensis 2016;62(2):182-186 DOI: 10.1515/amma-2016-0004 RESEARCH ARTICLE The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions Boeriu Alina
Acta Medica Marisiensis 2016;62(2):182-186 DOI: 10.1515/amma-2016-0004 RESEARCH ARTICLE The Usefulness Of Narrow Band Imaging Endoscopy For The Real Time Characterization Of Colonic Lesions Boeriu Alina
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Predict, Resect and discard : Yes we can! (at least in some hands)
") Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
Diminutive polyps : Real time endoscopic histology Predict, Resect and discard : Yes we can! (at least in some hands) Robert Benamouzig Hôpital Avicenne AP-HP & Paris 13 University France Why it is important?
2015 Winter School 대장종양성병변의진단과치료. Dong Kyung Chang. Sungkyunkwan University, School of Medicine Samsung Medical Center
 2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
2017 gastroenterology Winter School 77 2015 Winter School 대장종양성병변의진단과치료 Dong Kyung Chang Sungkyunkwan University, School of Medicine Samsung Medical Center Colon Polyps (Epithelial origin) Neoplastic Premalignant
Advanced techniques for resection of large polyps. John G. Lee, MD February 2, 2018
 Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Advanced techniques for resection of large polyps John G. Lee, MD February 2, 2018 Background 1cm - large polyp on screening 2cm - large for polypectomy 3cm giant polyp 10-15% of polyps can t be removed
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Early rectal cancer: the European Association for Endoscopic Surgery (EAES) clinical consensus conference
 clinical consensus conference") DOI 10.1007/s00464-015-4067-3 and Other Interventional Techniques CONSENSUS STATEMENT Early rectal cancer: the European Association for Endoscopic Surgery (EAES) clinical consensus conference Mario Morino
DOI 10.1007/s00464-015-4067-3 and Other Interventional Techniques CONSENSUS STATEMENT Early rectal cancer: the European Association for Endoscopic Surgery (EAES) clinical consensus conference Mario Morino
Factors for Endoscopic Submucosal Dissection in Early Colorectal Neoplasms: A Single Center Clinical Experience in China
 ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
ORIGINAL ARTICLE Clin Endosc 2015;48:405-410 http://dx.doi.org/10.5946/ce.2015.48.5.405 Print ISSN 2234-2400 On-line ISSN 2234-2443 Open Access Factors for Endoscopic Submucosal Dissection in Early Colorectal
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS
 PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
PATHOLOGY GROUP GUIDELINES FOR THE EXAMINATION AND REPORTING OF COLORECTAL CANCER SPECIMENS Produced by: Address: Yorkshire Cancer Network Pathology Group Arthington House, Cookridge Hospital, Hospital
WEO CRC SC Meeting. Barcelona, Spain October 23, 2015
 WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
Barrett s Esophagus: Ablate Everyone?
 Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Nicholas J. Shaheen, MD, MPH, FACG Barrett s Esophagus: Ablate Everyone? Nicholas J. Shaheen, MD, MPH, FACG Center for Esophageal Diseases and Swallowing University of North Carolina Greetings from UNC,
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Adenoma to Carcinoma Pathway
 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions
 Showa Univ J Med Sci 12(3), 253-258, September 2000 Original Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions Masaaki MATSUKAWA, Mototsugu FUJIMORI, Takahiko KOUDA,
Showa Univ J Med Sci 12(3), 253-258, September 2000 Original Incidence and Management of Hemorrhage after Endoscopic Removal of Colorectal Lesions Masaaki MATSUKAWA, Mototsugu FUJIMORI, Takahiko KOUDA,
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working Group chair: Michal F. Kaminski, Poland
 Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working chair: Michal F. Kaminski, Poland Population Interventions Comparator Outcome Additional evidence 1.1 Rate of adequate
Supporting Information 2. ESGE QIC Lower GI Delphi voting process: Round 1 Working chair: Michal F. Kaminski, Poland Population Interventions Comparator Outcome Additional evidence 1.1 Rate of adequate
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Durham E-Theses. Improving the Management of Large Colorectal Polyps CHATTREE, AMIT
 Durham E-Theses Improving the Management of Large Colorectal Polyps CHATTREE, AMIT How to cite: CHATTREE, AMIT (2015) Improving the Management of Large Colorectal Polyps, Durham theses, Durham University.
Durham E-Theses Improving the Management of Large Colorectal Polyps CHATTREE, AMIT How to cite: CHATTREE, AMIT (2015) Improving the Management of Large Colorectal Polyps, Durham theses, Durham University.
The Natural History of Right-Sided Lesions
 The Natural History of Right-Sided Lesions Jasper L.A. Vleugels Dept of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands. None Disclosures Agenda Is there evidence that
The Natural History of Right-Sided Lesions Jasper L.A. Vleugels Dept of Gastroenterology and Hepatology, Academic Medical Center, Amsterdam, the Netherlands. None Disclosures Agenda Is there evidence that
Romanian Journal of Morphology and Embryology 2006, 47(3):
:") Romanian Journal of Morphology and Embryology 26, 7(3):239 23 ORIGINAL PAPER Predictive parameters for advanced neoplastic adenomas and colorectal cancer in patients with colonic polyps a study in a tertiary
Romanian Journal of Morphology and Embryology 26, 7(3):239 23 ORIGINAL PAPER Predictive parameters for advanced neoplastic adenomas and colorectal cancer in patients with colonic polyps a study in a tertiary
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Local recurrence after endoscopic resection of colorectal tumors
 Int J Colorectal Dis (2009) 24:225 230 DOI 10.1007/s00384-008-0596-8 ORIGINAL ARTICLE Local recurrence after endoscopic resection of colorectal tumors Kinichi Hotta & Takahiro Fujii & Yutaka Saito & Takahisa
Int J Colorectal Dis (2009) 24:225 230 DOI 10.1007/s00384-008-0596-8 ORIGINAL ARTICLE Local recurrence after endoscopic resection of colorectal tumors Kinichi Hotta & Takahiro Fujii & Yutaka Saito & Takahisa
Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer
 498 Original article Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer Authors C. Kunisaki 1, M. Takahashi 2, Y. Nagahori 3, T. Fukushima 3, H. Makino
498 Original article Risk factors for lymph node metastasis in histologically poorly differentiated type early gastric cancer Authors C. Kunisaki 1, M. Takahashi 2, Y. Nagahori 3, T. Fukushima 3, H. Makino
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom
 Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Principles of diagnosis, work-up and therapy The Gastroenterologist s role
 Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Principles of diagnosis, work-up and therapy The Gastroenterologist s role Dr. Christos G. Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior Lecturer University
Earlyoesophagealcancer. dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia
 Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Earlyoesophagealcancer dr. Nina Zidar Institute of Pathology Faculty ofmedicine University of Ljubljana Slovenia Early carcinoma of oesophagus = tumor limited to mucosa or submucosa, not extending into
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Predictive relevance of lymphovascular invasion in T1 colorectal cancer before endoscopic treatment
 Original article Predictive relevance of lymphovascular invasion in T1 colorectal cancer before endoscopic treatment Authors Kazuya Inoki 1,4, Taku Sakamoto 1, Hiroyuki Takamaru 1, Masau Sekiguchi 1, Masayoshi
Original article Predictive relevance of lymphovascular invasion in T1 colorectal cancer before endoscopic treatment Authors Kazuya Inoki 1,4, Taku Sakamoto 1, Hiroyuki Takamaru 1, Masau Sekiguchi 1, Masayoshi
Endoscopic submucosal dissection of malignant non-pedunculated colorectal lesions
 Endoscopic submucosal dissection of malignant non-pedunculated colorectal lesions Authors Carl-Fredrik Rönnow 1,JacobElebro 2,ErvinToth 3, Henrik Thorlacius 1 Institutions 1 Department of Clinical Sciences,
Endoscopic submucosal dissection of malignant non-pedunculated colorectal lesions Authors Carl-Fredrik Rönnow 1,JacobElebro 2,ErvinToth 3, Henrik Thorlacius 1 Institutions 1 Department of Clinical Sciences,