A Combined Practice. Why Its Worked. Barriers to Breast Reconstruction. As a breast oncologist the patient gets seemless care
|
|
|
- Nora Melton
- 5 years ago
- Views:
Transcription

1 A Combined Practice A Combined Breast Oncology and Plastic Surgery Practice Why It Works Anne M. Wallace, MD, FACS Director, Comprehensive Breast Health Center Professor of Clinical Surgery, Surgical Oncology and Plastic Surgery UCSD Department of Surgery, Moores Cancer Center Ablative Surgical Oncology Plastic Surgery Focus on breast, melanoma, and oncologic reconstruction while maintaining an aesthetic and general reconstructive practice Have been the Team Leader for the UCSD Breast Program for 20 years Why Its Worked One surgeon, both aspects ablative and reconstruction As a Plastic Surgeon, we know the breast and skin better than any other specialty As a Plastic Surgeon, we follow the patients longer than most As a breast oncologist the patient gets seemless care Barriers to Breast Reconstruction Huge Issue Must understand difficult nature of this field extremely time consuming, very underreimbursed; difficult to achieve patient satisfaction in certain subgroups of body types, etc. Most plastic surgeons are in private practice where reimbursement from insurance does not even begin to pay cost, especially from the BCCTP and medi-cal 1
2 Disparities in Breast Reconstruction Receipt of Breast Reconstruction Data presented at CSPS JCO pts in SEER data, 2260 respondents; 806 patients who received a mastectomy Outcomes receipt of reconstruction 34.6% of 806 patients, 84.5% at time of mastectomy,15.5% later Receipt of Reconstruction by Race: W/AA/Latina-high/Latinalow: 40.9/33.5/41.2/13.5% p < 001 Latina-low tended to be younger, less likely to be high school graduates, and more likely to be without health insurance AA had more comorbidities No difference in stage of disease OSHPD Data Postmastectomy reconstruction rates were determined from the California Office of Statewide Health Planning and Development (OSHPD) inpatient database from 2003 to The proportion of patients undergoing reconstruction rose from 24.8% in 2003 to 29.2% in Do Variations in Provider Discussions Explain Differences in Reconstruction Journal Of American College of Surgeons, April 2008 Data collected from NICCQ, stages I-III 253/626 pts received reconstruction (40.4%) If Discussion of reconstruction not documented, PATIENT LESS LIKELY TO RECEIVE IT 2
3 UCSD Data Of the 1715 operations breast cancer operations 63.6% (N=1091) and 36.4% (N=624) represented breast conservation therapy and mastectomy, respectively. Of the lumpectomy patients, 9.3% (N=168) required reexcision for close or positive margins. (National average by current literature 23%) 78.8% of mastectomy patients underwent breast reconstruction, 4.5% of which were delayed. UCSD same surgeon reconstruction rate 78.8%; Remaining mastectomy patients either did not want reconstruction or had locally advanced disease On multivariate analysis, independent predictors of reconstruction were age, relationship status, and stage of disease, while the effect of race and insurance status were non-significant There was a total recurrence rate of 6.73%. Survival Data from UCSD 615 women treated with mastectomy; 78.8% underwent reconstruction Those pts had higher OS and DFS (8.3% vs 11.3 years, p<0.001 and 6.6 vs 11.5 years, respectively, p<0.001) After controlling for age, race, marital status, payer category, triple negative status, stage of disease and receipt of chemotherapy, radiation therapy and hormone therapy, reconstructed patients still maintained a survival advantage So in an Institution Where A Novel Approach to the Delivery of Breast Care is Made Breast reconstruction rate 78.8% vs national average of 34.6% Positive margin rate 9.8% vs national average of 23% Survival advantage across the board for patients who were reconstructed 3



4 Points to Remember It s the Simple Differences We Make Daily Clear margins is the goal Must accept that taking tissue will leave some change in the effected breast Our goal is to camouflage defect as a much as possible Postoperative correction is very feasible Oncoplastic Techniques For Very Large Defects Central Lumpectomy with inverted T closure A circumareolar, Bennelli-type closure Inferiorly based mammaplasty Other local flaps Basically, volume replacement or volume displacement Any of the above with bracketed localization closure for large periareolar defects 4










5 Inferior Tumor Often Poor Results Preop Radiology localized tumor Mastopexy drawn around Inferior Lower Quadrant tumor Postop 1 year Tumor Involving Nipple Breast Conservation Via Breast Reduction Nipple-Ablation Mastopexy New Nipple Created Later On Patch of Neo-Areolar Skin 5







6 The 12:00 central breast defects are very non-cosmetic when excised primarily BilopedFlap for Central Superior Defect Basic plastic surgery flap-biloped Six days post-op; widely clear margins and NO pulling up of NAC or indentation Asymmetry After Breast Conservation 6






")

7 Preop Flap procedures for local defect Postop Choosing Mastectomy Tumor too diffuse Tumor in multiple quadrants BRCA family Pt will get better cosmetic result with implants (breast small and ptotic) Recurrence Mastectomies have evolved Traditional Skin sparing Nipple sparing 7







8 Traditional Mastectomy Immediate flap After Skin Sparing Mastectomy Skin Sparing Mastectomy Nipple Sparing/ Minimal Skin/ Implant Removal 8




9 There is No subcutaneous fat between ductal tissue and skin Dissection DIRECTLY under skin, completely skinning the undersurface Invert nipple and cut circular rim of tissue out send separately to path Nipple may DIE Editorial in Annals of Surgical Oncology this month STRESSED importance of adequate mastectomy Nipple Sparing Mastectomy Seemless Cancer Care When the Surgeon Does Both Aspects 9






10 1. Example RM, 65 year old female, s/p masto/aug Unhappy with right side nipple too high, bottomed out Now scheduled with me for right side correction and if necessary in OR adjustment of left side Mammogram, PE normal RM, Continued Right side corrected with pocket adjustment, re-do mastopexy to lower NAC, new implant So decision to open left side to place same implant Once implant out on left, palpation of the inside pocket revealed a hard mass on far lateral breast, just anterior to capsule Immediate removal and frozen section Invasive ductal CA; took a wider margin on the spot; scheduled for sentinel lymph node several days later after MRI; Tumor small enough and node negative; thus an intermediate ONCOTYPE score allowed her NO chemotherpy Radiation than proceeded and she is doing very well She later became the donor for my $2 million endowment to establish an integrated fellowship 2. Example Triple Negative Breast Cancer; BRCA+ Had neoadjuvant chemo, Mastectomties, expanders; Post op day 3 implants Continued Was scheduled for fat grafting, upper poles During marking in preop area, pt says Dr. Wallace, I have a lump under my arm. I had not seen her for a month. I examined and there was a 2cm mass in the right axilla Immediate CHANGE in OR plan excisional biopsy, frozen section, followed by ALND when it returned metastatic CA to axilla. Fat grafting aborted as she would now need radiation and would return later for more reconstruction 10







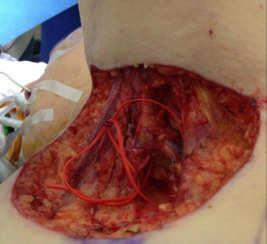
11 3. Example Clear Margins Large cancer forming a U up and across breast Took 5 needles to localize and a breast reduction to close it correctly. 7 cm cancer with clear margins 4. Example ML 68 Year Old Female 2003 had bilateral mastectomies by me for DCIS and a low grade early stage 1 disease Had expander/implant reconstruction, but on the left side had several implant infections. After several implant surgeries, in 2006 we converted her left side to a TRAM flap. She did well until 2012 No history of chemotherapy or radiation February 2012, she Noticed one small bruise Like area on left side. Progressed over 2 months To this. 11



12 ML, Continued She lives in Reno, NV. Biopsy done by my recommendation and it was inconclusive MRI just showed skin thickening All blood work normal; no new meds that cause bruising Clinical picture was still concerning The Answer: Angiosarcoma; Was embedded in the TRAM; no Ductal tissue seen;????? Related to history of implant infection??? Went on to complete resection of the TRAM, Chemotherapy and radiation Came back a year later for a latissimus Flap/ revisions pending.5 Example JC 65 Year Old Female History of nearly 40 year old silicone implants Pelvic pain Primary Care Doc works up with scans; PET/CT eventually done that shows mass under left implant, and PET+ nodes in internal mammary chain, left side Some indistinct nodes in pelvis JC, Continued MRI of breast shows a mass again beneath implant and enlarged IMA nodes Not amenable to core biopsy due to location Implant rupture suspected as well I m referred pt level of expertise that incorporates both aspects - discussed implant removal, identifying and removing mass and removal of internal mammary nodes at that level 12





13 Bilateral capsulectomies done Internal mammary node removal Mass taken with rib fascia Right implant GROSSLY ruptured Left intact, but being pushed and elevated by this mass Ambiguous pathology for 2 weeks; thought to be angiosarcoma; but finally determined to be atypical vascular lesion consistent with an old organized hematoma Care of this pt was facilitated by me knowing both the plastic surgery and the surgical oncology 6. Example BRCA Patients All referred to me Discuss better screening and observation - MRI Discuss chemoprevention tamoxifen, raloxifene, oophrectomy Discuss bilateral mastectomies/reconstruction Follow for years Then DO the mastectomies when the time is right for the patient MASTECTOMIES ARE NOT ALWAYS THE IMMEDIATE ANSWER FOR THESE PATIENTS BRCA +; bilateral preventative Mastectomies, expanders, Implants and fat grating 13










14 Pt BRCA positive 29, BRCA+, Advanced breast cancer treated with chemo first Followed by mastectomies and reconstruction; Despite positive Lymph nodes, etc., she had a great result Triple negative breast cancer Treated first with clinical trial Bilateral mastectomies and Implant reconstruction, nipple sparing PT with bilateral breast cancer; hx Radiation Did Hyperbaric Oxygen First to Help Nipple Survival 14






15 One Pt is a breast augmentation; another is bilateral mastectomies for cancer; Is getting very close to minimal differences in cosmetic outcome Right sided reconstruction ONLY with Mentor MM shaped gel. Nothing done on left; This Implant is fantastic for unilateral reconstruction Because Mentor makes a broader lower profile Shaped implant and it is somewhat softer. Bilateral Tram Flaps after prophylactic mastectomies for family history A Few Additional Comments I do LESS mastectomies than my colleague at UCSD; rvu incentive for general surgeons to do more Efficiency of practice in both the clinic and OR Having a dual practice is obviously better for the patient, but also increases job satisfaction for the surgeon 15











16 Axillary Tumor Recurrence Locally advanced and infiltrating Breast cancer; failed all other modalities Latissimus flap reconstruction Failed TRAM; there is no Implant in this TRAM; Its all Fat necrosis, etc. Contracated implant Since 1995; salvage latissimus Salvage Latissimus Flap 16






17 Chronic 10 month old wound; radiated, necrotic Rib; debridement, rib resection, flap for closure; 6 months later expander placed and fully expanded And Sometimes I Have to Know When NOT to Operate And Manage with my Radiation and Medical Oncology Colleagues PLAN: begin a fellowship for dual trained surgeons with emphasis on both the oncology and the reconstruction Perfect opportunity after an Integrated Plastic Surgery Residency 17
Classification System
 Classification System A graduate of the Breast Oncology training program should be able to care for all aspects of disease and/or provide comprehensive management. When referring to a discipline of training
Classification System A graduate of the Breast Oncology training program should be able to care for all aspects of disease and/or provide comprehensive management. When referring to a discipline of training
The Case FOR Oncoplastic Surgery in Small Breasts. Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA
 The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
The Case FOR Oncoplastic Surgery in Small Breasts Barbara L. Smith, MD, PhD Massachusetts General Hospital Harvard Medical School Boston, MA USA Changing issues in breast cancer management Early detection
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Breast Surgery: Yesterday, Today and Tomorrow
 Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
Contralateral Prophylactic Mastectomy with Immediate Reconstruction: Added Benefits, Added Risks
 Contralateral Prophylactic Mastectomy with Immediate Reconstruction: Added Benefits, Added Risks Grant W. Carlson Wadley R. Glenn Professor of Surgery Divisions of Plastic Surgery & Surgical Oncology Emory
Contralateral Prophylactic Mastectomy with Immediate Reconstruction: Added Benefits, Added Risks Grant W. Carlson Wadley R. Glenn Professor of Surgery Divisions of Plastic Surgery & Surgical Oncology Emory
ONCOPLASTIC BREAST SURGERY AT HOAG WE CAN SAVE YOUR BREASTS
 ONCOPLASTIC BREAST SURGERY AT HOAG WE CAN SAVE YOUR BREASTS Oncoplastic surgery is a new technique that combines oncologic and plastic surgery principles in the same procedure to both remove the tumor
ONCOPLASTIC BREAST SURGERY AT HOAG WE CAN SAVE YOUR BREASTS Oncoplastic surgery is a new technique that combines oncologic and plastic surgery principles in the same procedure to both remove the tumor
Advances in Localized Breast Cancer
 Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Current Strategies in Breast Reconstruction
 Current Strategies in Breast Reconstruction Hani Sbitany, MD Assistant Professor of Surgery University of California, San Francisco Division of Plastic and Reconstructive Surgery 12 th Annual School of
Current Strategies in Breast Reconstruction Hani Sbitany, MD Assistant Professor of Surgery University of California, San Francisco Division of Plastic and Reconstructive Surgery 12 th Annual School of
Breast Reconstruction Surgery
 Breast Reconstruction Surgery I. Policy University Health Alliance (UHA) will reimburse for Breast Reconstruction Surgery when it is determined to be medically necessary and when it meets the medical criteria
Breast Reconstruction Surgery I. Policy University Health Alliance (UHA) will reimburse for Breast Reconstruction Surgery when it is determined to be medically necessary and when it meets the medical criteria
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
So, we already talked about that recognition is the key to optimal treatment and outcome.
 Hi, I m Dr. Anthony Lucci from the University of Texas MD Anderson Cancer Center in Houston. And today, I d like to talk to you about the role of surgery in inflammatory breast cancer patients. So, there
Hi, I m Dr. Anthony Lucci from the University of Texas MD Anderson Cancer Center in Houston. And today, I d like to talk to you about the role of surgery in inflammatory breast cancer patients. So, there
Breast Reconstruction: Current Strategies and Future Opportunities
 Breast Reconstruction: Current Strategies and Future Opportunities Hani Sbitany, MD Assistant Professor of Surgery University of California, San Francisco Division of Plastic and Reconstructive Surgery
Breast Reconstruction: Current Strategies and Future Opportunities Hani Sbitany, MD Assistant Professor of Surgery University of California, San Francisco Division of Plastic and Reconstructive Surgery
Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander.
 Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander. Strong and flexible Bacterially inactivated Provides implant support Breast Reconstruction
Breast Reconstruction Postmastectomy. Using DermaMatrix Acellular Dermis in breast reconstruction with tissue expander. Strong and flexible Bacterially inactivated Provides implant support Breast Reconstruction
Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC
 Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC Objectives Identify breast lesions and masses, and know
Breast Cancer Update 2018 The Latest in Diagnosis and Treatment SARATH K, PALAKODETI, DO, FAACS GENERAL, BREAST, AND COSMETIC SURGEON TOLEDO CLINIC Objectives Identify breast lesions and masses, and know
Mastectomy For Treatment, For Prevention, For Prophylaxis Not as Simple as Following Data
 Mastectomy For Treatment, For Prevention, For Prophylaxis Not as Simple as Following Data Nathalie Johnson, MD FACS Medical Director, Legacy Cancer Institute and Breast Health Centers Objectives Understand
Mastectomy For Treatment, For Prevention, For Prophylaxis Not as Simple as Following Data Nathalie Johnson, MD FACS Medical Director, Legacy Cancer Institute and Breast Health Centers Objectives Understand
Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate surgical options
 across Ontario: Patient indications and appropriate surgical options") A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate
A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Breast cancer reconstruction surgery (immediate and delayed) across Ontario: Patient indications and appropriate
Medical Review Criteria Breast Surgeries
 Medical Review Criteria Breast Surgeries Effective Date: November 8, 2016 Subject: Breast Surgeries Policy: HPHC covers medically necessary breast surgeries including mastectomy, breast reconstruction,
Medical Review Criteria Breast Surgeries Effective Date: November 8, 2016 Subject: Breast Surgeries Policy: HPHC covers medically necessary breast surgeries including mastectomy, breast reconstruction,
Breast cancer: an update
 Breast cancer: an update Dr. Sanjeewa Seneviratne M.D, MRCS, Ph.D. Senior Lecturer and Honorary Consultant Surgeon Department of Surgery Faculty of Medicine, Colombo Plan The problem Screening & early
Breast cancer: an update Dr. Sanjeewa Seneviratne M.D, MRCS, Ph.D. Senior Lecturer and Honorary Consultant Surgeon Department of Surgery Faculty of Medicine, Colombo Plan The problem Screening & early
Updates in Breast Care. Truth or Hype. History of Breast Cancer Surgery. Dr Karen Barbosa 5/3/2017 4/20/2017
 Updates in Breast Care Dr Karen Barbosa 4/20/2017 Truth or Hype Princess Bust Developer Sears, Roebuck and Co. 1897 Promised to make the breast round, firm and beautiful History of Breast Cancer Surgery
Updates in Breast Care Dr Karen Barbosa 4/20/2017 Truth or Hype Princess Bust Developer Sears, Roebuck and Co. 1897 Promised to make the breast round, firm and beautiful History of Breast Cancer Surgery
Surgical Advances in the Treatment of Breast Cancer. Laura Kruper, MD, MSCE Chief, Breast Surgery
 Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery
 Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery Goal The goal of the Breast Surgery rotation is to develop the knowledge, skills and attitudes necessary to evaluate,
Educational Goals and Objectives for Rotations on: Breast, Wound and Plastic Surgery Goal The goal of the Breast Surgery rotation is to develop the knowledge, skills and attitudes necessary to evaluate,
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer. Oncoplastic and Reconstructive Surgery
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Oncoplastic and Reconstructive Surgery Plastic-reconstructive aspects after mastectomy Versions 2002 2017: Audretsch / Bauerfeind
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Oncoplastic and Reconstructive Surgery Plastic-reconstructive aspects after mastectomy Versions 2002 2017: Audretsch / Bauerfeind
National Mastectomy & Breast Reconstruction Audit Datasheet - Mastectomy +/- Immediate Reconstruction
 Patient Registration data Surname Forename NHS/Private Hospital Number Date of birth Postcode Ethnicity Patient-reported outcomes consent Has this patient consented to being sent outcome questionnaires?
Patient Registration data Surname Forename NHS/Private Hospital Number Date of birth Postcode Ethnicity Patient-reported outcomes consent Has this patient consented to being sent outcome questionnaires?
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
THE BREAST CENTER AT MONTEFIORE NYACK HOSPITAL
 THE BREAST CENTER AT MONTEFIORE NYACK HOSPITAL COMPLETE BREAST CARE FROM THE TEAM THAT CARES I don t think I could get better care, more support, or encouragement at any of the bigger hospitals or cancer
THE BREAST CENTER AT MONTEFIORE NYACK HOSPITAL COMPLETE BREAST CARE FROM THE TEAM THAT CARES I don t think I could get better care, more support, or encouragement at any of the bigger hospitals or cancer
Medical Review Criteria Breast Surgeries
 Medical Review Criteria Breast Surgeries Subject: Breast Surgeries Authorization: Prior authorization is required for the following procedures requested for members enrolled in HPHC commercial (HMO, POS,
Medical Review Criteria Breast Surgeries Subject: Breast Surgeries Authorization: Prior authorization is required for the following procedures requested for members enrolled in HPHC commercial (HMO, POS,
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine
 What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
What is Cancer? Petra Ketterl, MD Medical Oncology and Functional Medicine What is Cancer? Layman s terms: cancer starts when cells grow out of control (in any place in the body) and crowd out normal cells
Oncoplastic breast surgery in a Danish perspective II: Reconstructive strategy in oncoplastic breast surgery
 Oncoplastic breast surgery in a Danish perspective II: Reconstructive strategy in oncoplastic breast surgery Michael Rose, MD Department of Surgery and Plastic Surgery, Hospital of Southwest Jutland, Denmark
Oncoplastic breast surgery in a Danish perspective II: Reconstructive strategy in oncoplastic breast surgery Michael Rose, MD Department of Surgery and Plastic Surgery, Hospital of Southwest Jutland, Denmark
Complete breast care from the team that cares. Breast Center
 Breast Center Complete breast care from the team that cares. Imaging Appointment: 845.348.8551 Surgical Consultation: 845.348.8507 nyackhospital.org/breastcenter 1 Complete breast care from the team that
Breast Center Complete breast care from the team that cares. Imaging Appointment: 845.348.8551 Surgical Consultation: 845.348.8507 nyackhospital.org/breastcenter 1 Complete breast care from the team that
BREAST CANCER CARE IN RESOURCE CONSTRAINED REGIONS BBCC 2017 DHAKA. M.J.PAUL MS,DNB, FRCS (Glasg) Professor, Endocrine Surgery CMC Vellore, India
 Professor, Endocrine Surgery CMC Vellore, India") BREAST CANCER CARE IN RESOURCE CONSTRAINED REGIONS BBCC 2017 DHAKA M.J.PAUL MS,DNB, FRCS (Glasg) Professor, Endocrine Surgery CMC Vellore, India BREAST CANCER THE COMING WAVE THE DEMOGRAPHIC CHANGE Increase
BREAST CANCER CARE IN RESOURCE CONSTRAINED REGIONS BBCC 2017 DHAKA M.J.PAUL MS,DNB, FRCS (Glasg) Professor, Endocrine Surgery CMC Vellore, India BREAST CANCER THE COMING WAVE THE DEMOGRAPHIC CHANGE Increase
BREAST CANCER SURGERY. Dr. John H. Donohue
 Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Oncoplastic Breast Surgery
 Disclosures Oncoplastic Breast Surgery Newfoundlander OAGS 2016 Dr Renee Hanrahan General Surgeon Oncologic and Reconstructive Breast Surgeon Objectives What is Oncoplastic Surgery Define Oncoplastic Surgery
Disclosures Oncoplastic Breast Surgery Newfoundlander OAGS 2016 Dr Renee Hanrahan General Surgeon Oncologic and Reconstructive Breast Surgeon Objectives What is Oncoplastic Surgery Define Oncoplastic Surgery
Mitchell Buller, MEng, a Adee Heiman, BA, a Jared Davis, MD, b ThomasJ.Lee,MD, b Nicolás Ajkay, MD, FACS, c and Bradon J. Wilhelmi, MD, FACS b
 Immediate Breast Reconstruction of a Nipple Areolar Lumpectomy Defect With the L-Flap Skin Paddle Breast Reduction Design and Contralateral Reduction Mammoplasty Symmetry Procedure: Optimizing the Oncoplastic
Immediate Breast Reconstruction of a Nipple Areolar Lumpectomy Defect With the L-Flap Skin Paddle Breast Reduction Design and Contralateral Reduction Mammoplasty Symmetry Procedure: Optimizing the Oncoplastic
NIPPLE SPARING MASTECTOMY
 NIPPLE SPARING MASTECTOMY 29th Annual Montefiore-Einstein Controversies in Surgery Symposium Virgilio Sacchini, MD Memorial Sloan-Kettering Cancer Center Professor of Clinical Surgery Weill Cornell Medical
NIPPLE SPARING MASTECTOMY 29th Annual Montefiore-Einstein Controversies in Surgery Symposium Virgilio Sacchini, MD Memorial Sloan-Kettering Cancer Center Professor of Clinical Surgery Weill Cornell Medical
ONCOPLASTIC SURGERY. Dr. Sadir Alrawi Director of Surgical Oncology Services. Dr. Humaa Darr Surgical Oncology Fellow
 Hessa St ONCOPLASTIC SURGERY Dr. Sadir Alrawi Director of Surgical Oncology Services Dr. Humaa Darr Surgical Oncology Fellow Al Sufouh Rd AL SUFOUH AL SUFOUH Sharaf DG Mall of the Emirates Mall Of the
Hessa St ONCOPLASTIC SURGERY Dr. Sadir Alrawi Director of Surgical Oncology Services Dr. Humaa Darr Surgical Oncology Fellow Al Sufouh Rd AL SUFOUH AL SUFOUH Sharaf DG Mall of the Emirates Mall Of the
RUTGERS CANCER INSTITUTE OF NEW JERSEY - ROBERT WOOD JOHNSON MEDICAL SCHOOL INTERDISCIPLINARY BREAST SURGERY FELLOWSHIP CORE EDUCATIONAL OBJECTIVES
 RUTGERS CANCER INSTITUTE OF NEW JERSEY - ROBERT WOOD JOHNSON MEDICAL SCHOOL INTERDISCIPLINARY BREAST SURGERY FELLOWSHIP CORE EDUCATIONAL OBJECTIVES At the completion of Breast Fellowship training, the
RUTGERS CANCER INSTITUTE OF NEW JERSEY - ROBERT WOOD JOHNSON MEDICAL SCHOOL INTERDISCIPLINARY BREAST SURGERY FELLOWSHIP CORE EDUCATIONAL OBJECTIVES At the completion of Breast Fellowship training, the
How To Make a Good Mastectomy for Reconstruction Based on the Anatomy. Zhang Jin, Ph.D MD
 How To Make a Good Mastectomy for Reconstruction Based on the Anatomy Zhang Jin, Ph.D MD Deputy Director and Professor Tianjin Medical University Cancer Institute and Hospital People s Republic of China
How To Make a Good Mastectomy for Reconstruction Based on the Anatomy Zhang Jin, Ph.D MD Deputy Director and Professor Tianjin Medical University Cancer Institute and Hospital People s Republic of China
COPE Library Sample
 Breast Anatomy LOBULE LOBE ACINI (MILK PRODUCING UNITS) NIPPLE AREOLA COMPLEX ENLARGEMENT OF DUCT AND LOBE LOBULE SUPRACLAVICULAR NODES INFRACLAVICULAR NODES DUCT DUCT ACINI (MILK PRODUCING UNITS) 8420
Breast Anatomy LOBULE LOBE ACINI (MILK PRODUCING UNITS) NIPPLE AREOLA COMPLEX ENLARGEMENT OF DUCT AND LOBE LOBULE SUPRACLAVICULAR NODES INFRACLAVICULAR NODES DUCT DUCT ACINI (MILK PRODUCING UNITS) 8420
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation
 Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
INNOVATIVE RECONSTRUCTIVE STRATEGIES IN BREAST CANCER SURGERY
 INNOVATIVE RECONSTRUCTIVE STRATEGIES IN BREAST CANCER SURGERY Jane L. Kakkis, MD, MPH Breast Surgeon, Director Orange Coast Memorial Medical Center, Fountain Valley, CA USA WHEN RADIATION IS NECESSARY
INNOVATIVE RECONSTRUCTIVE STRATEGIES IN BREAST CANCER SURGERY Jane L. Kakkis, MD, MPH Breast Surgeon, Director Orange Coast Memorial Medical Center, Fountain Valley, CA USA WHEN RADIATION IS NECESSARY
Prophylactic Mastectomy & Reconstructive Implications
 Prophylactic Mastectomy & Reconstructive Implications Minas T Chrysopoulo, MD PRMA Center For Advanced Breast Reconstruction Prophylactic Mastectomy Surgical removal of one or both breasts to reduce the
Prophylactic Mastectomy & Reconstructive Implications Minas T Chrysopoulo, MD PRMA Center For Advanced Breast Reconstruction Prophylactic Mastectomy Surgical removal of one or both breasts to reduce the
Therapeutic Mammoplasty in Management of Breast Cancer: A Prospective Clinical Study
 Advances in Breast Cancer Research, 2017, 6, 107-116 http://www.scirp.org/journal/abcr ISSN Online: 2168-1597 ISSN Print: 2168-1589 Therapeutic Mammoplasty in Management of Breast Cancer: A Prospective
Advances in Breast Cancer Research, 2017, 6, 107-116 http://www.scirp.org/journal/abcr ISSN Online: 2168-1597 ISSN Print: 2168-1589 Therapeutic Mammoplasty in Management of Breast Cancer: A Prospective
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node
 Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Lesion Imaging Characteristics Mass, Favoring Benign Circumscribed Margins Intramammary Lymph Node Oil Cyst Mass, Intermediate Concern Microlobulated Margins Obscured Margins Mass, Favoring Malignant Indistinct
Point of view of the surgeons
 NEOADJUVANT THERAPY: WHEN AND HOW? Point of view of the surgeons Dr. M. Danaei Head of Breast Unit Marienhospital Aachen Germany 2 3 Neoadjuvant therapy and overall survival: 4 Neoadjuvant therapy: concept
NEOADJUVANT THERAPY: WHEN AND HOW? Point of view of the surgeons Dr. M. Danaei Head of Breast Unit Marienhospital Aachen Germany 2 3 Neoadjuvant therapy and overall survival: 4 Neoadjuvant therapy: concept
How can surgeons help the Radiation Oncologists?
 How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
How can surgeons help the Radiation Oncologists? Lorna Weir BC Surgical Oncology fall breast cancer update Oct 24, 2009 Disclosure no conflict of interest Outline Introduction OR reports Marking of surgical
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e
 Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 60: Caring for Clients With Breast Disorders Slide 1 Infectious and Inflammatory Breast Disorders: Mastitis Pathophysiology and Etiology
Timby/Smith: Introductory Medical-Surgical Nursing, 9/e Chapter 60: Caring for Clients With Breast Disorders Slide 1 Infectious and Inflammatory Breast Disorders: Mastitis Pathophysiology and Etiology
Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018)
 Test Content Outline (Effective 2018)") Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018) I. Coordination of Care - 26% A. Breast health, screening, early detection, risk assessment and reduction 1. Issues related to
Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018) I. Coordination of Care - 26% A. Breast health, screening, early detection, risk assessment and reduction 1. Issues related to
Skin sparing mastectomy: Technique and suggested methods of reconstruction
 Journal of the Egyptian National Cancer Institute (2014) 26, 153 159 Cairo University Journal of the Egyptian National Cancer Institute www.nci.cu.adu.eg www.sciencedirect.com Full Length Article Skin
Journal of the Egyptian National Cancer Institute (2014) 26, 153 159 Cairo University Journal of the Egyptian National Cancer Institute www.nci.cu.adu.eg www.sciencedirect.com Full Length Article Skin
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction
 Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Breast Cancer Screening and Treatment Mrs Belinda Scott Breast Surgeon Breast Associates Auckland
 Breast Cancer Screening and Treatment 2009 Mrs Belinda Scott Breast Surgeon Breast Associates Auckland BREAST CANCER THE PROBLEM 1.1 million women per year 410,000 deaths each year Increasing incidence
Breast Cancer Screening and Treatment 2009 Mrs Belinda Scott Breast Surgeon Breast Associates Auckland BREAST CANCER THE PROBLEM 1.1 million women per year 410,000 deaths each year Increasing incidence
NIPPLE SPARING PRE-PECTORAL BREAST RECONSTRUCTION
 NIPPLE SPARING PRE-PECTORAL BREAST RECONSTRUCTION 42 yo female healthy athlete Right breast mass. Past medical history: none Family history: aunt with Breast cancer Candidates for nipple-sparing mastectomy
NIPPLE SPARING PRE-PECTORAL BREAST RECONSTRUCTION 42 yo female healthy athlete Right breast mass. Past medical history: none Family history: aunt with Breast cancer Candidates for nipple-sparing mastectomy
Incorporating Nipple-Sparing Mastectomy Into Your Practice. Michael Howard, MD, FACS Karol A Gutowski, MD, FACS
 Incorporating Nipple-Sparing Mastectomy Into Your Practice Michael Howard, MD, FACS Karol A Gutowski, MD, FACS 1 Disclosures Michael Howard, MD Scientific Advisor, EO2 Concepts Karol Gutowski, MD Speaker's
Incorporating Nipple-Sparing Mastectomy Into Your Practice Michael Howard, MD, FACS Karol A Gutowski, MD, FACS 1 Disclosures Michael Howard, MD Scientific Advisor, EO2 Concepts Karol Gutowski, MD Speaker's
Pathology: Grade 1 infiltrating ductal carcinoma with associated DCIS, Lymphvascular invasion present. ER+, PR+. Her 2/ IHC 1+, negative
 GATRA 2016 Breast Case Demographics Name: Autumn Leaf Sex: F Date of Birth: 3/26/75 SSN: 098765432 Race: African American Marital Status: Single Address: 3615 Burnt Hickory Trail, Helen, GA 37285, White
GATRA 2016 Breast Case Demographics Name: Autumn Leaf Sex: F Date of Birth: 3/26/75 SSN: 098765432 Race: African American Marital Status: Single Address: 3615 Burnt Hickory Trail, Helen, GA 37285, White
Ductal Carcinoma-in-Situ: New Concepts and Controversies
 Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Breast Reconstructive Surgery After Mastectomy Page 1 of 8 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Breast Reconstructive Surgery After Mastectomy PRE-DETERMINATION
Breast Reconstructive Surgery After Mastectomy Page 1 of 8 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Breast Reconstructive Surgery After Mastectomy PRE-DETERMINATION
BREAST RECONSTRUCTION FOLLOWING PROPHYLACTIC OR THERAPEUTIC MASTECTOMY FOR BREAST CANCER
 BREAST RECONSTRUCTION FOLLOWING PROPHYLACTIC OR THERAPEUTIC MASTECTOMY FOR BREAST CANCER Effective Date: September 2013 The recommendations contained in this guideline are a consensus of the Alberta Provincial
BREAST RECONSTRUCTION FOLLOWING PROPHYLACTIC OR THERAPEUTIC MASTECTOMY FOR BREAST CANCER Effective Date: September 2013 The recommendations contained in this guideline are a consensus of the Alberta Provincial
National Center of Oncology - Yerevan, Armenia
 - Yerevan, Armenia General Information New breast cancer cases treated per year 450 Breast multidisciplinarity team members 13 Radiologists, surgeons, pathologists, medical oncologists, radiotherapists
- Yerevan, Armenia General Information New breast cancer cases treated per year 450 Breast multidisciplinarity team members 13 Radiologists, surgeons, pathologists, medical oncologists, radiotherapists
Page 1. AHN-JHU Breast Cancer Symposium. Novel Local Regional Clinical Trials. Background. Neoadjuvant Chemotherapy Benefit.
 AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
Tumor Board with Navigation Session #53
 Tumor Board with Navigation Session #53 Moderator: Tina Rizack, MD, MPH With Dennis R Holmes, MD, FACS Reshma Jagsi, MD Jessica Lapise, MS, CGC Gary Levine, MD William Sikov, MD Heather Coelho, RN, BSN,
Tumor Board with Navigation Session #53 Moderator: Tina Rizack, MD, MPH With Dennis R Holmes, MD, FACS Reshma Jagsi, MD Jessica Lapise, MS, CGC Gary Levine, MD William Sikov, MD Heather Coelho, RN, BSN,
ASPS Recommended Insurance Coverage Criteria for Third- Party Payers
 ASPS Recommended Insurance Coverage Criteria for Third- Party Payers Breast Implant Associated Anaplastic Large Cell Lymphoma BACKGROUND Anaplastic Large Cell Lymphoma (ALCL) is a rare type of cancer of
ASPS Recommended Insurance Coverage Criteria for Third- Party Payers Breast Implant Associated Anaplastic Large Cell Lymphoma BACKGROUND Anaplastic Large Cell Lymphoma (ALCL) is a rare type of cancer of
Types of Breast Cancer
 IOWA RADIOLOGY 1 Types of Breast Cancer 515-226-9810 Ankeny Clive Downtown Des Moines IOWA RADIOLOGY 1 Table of Contents Introduction... 1 Ductal Carcinoma... 2 Paget s Disease of the Nipple... 8 Lobular
IOWA RADIOLOGY 1 Types of Breast Cancer 515-226-9810 Ankeny Clive Downtown Des Moines IOWA RADIOLOGY 1 Table of Contents Introduction... 1 Ductal Carcinoma... 2 Paget s Disease of the Nipple... 8 Lobular
Handout for Dr Allison s Lectures on Grossing Breast Specimens:
 Handout for Dr Allison s Lectures on Grossing Breast Specimens: Dr. Kimberly H. Allison Director of Breast Pathology and Breast Pathology Fellowship Director of Residency Training in Pathology Stanford
Handout for Dr Allison s Lectures on Grossing Breast Specimens: Dr. Kimberly H. Allison Director of Breast Pathology and Breast Pathology Fellowship Director of Residency Training in Pathology Stanford
Medical Policy Original Effective Date: Revised Date: Page 1 of 8
 Page 1 of 8 Disclaimer Description Coverage Determination Refer to the member s specific benefit plan and Schedule of Benefits to determine coverage. This may not be a benefit on all plans, or the plan
Page 1 of 8 Disclaimer Description Coverage Determination Refer to the member s specific benefit plan and Schedule of Benefits to determine coverage. This may not be a benefit on all plans, or the plan
Breast Cancer Reconstruction
 Breast Cancer Jerome H. Liu, MD Tom S. Liu, MD Jerome H. Liu, MD Undergraduate: Brown University Medical School: University of California, Los Angeles Residency: UCLA Medical Center Fellowship:UCLA Medical
Breast Cancer Jerome H. Liu, MD Tom S. Liu, MD Jerome H. Liu, MD Undergraduate: Brown University Medical School: University of California, Los Angeles Residency: UCLA Medical Center Fellowship:UCLA Medical
ESSO ACCREDITED TRAINING FELLOWSHIP IN BREAST SURGERY
 ESSO ACCREDITED TRAINING FELLOWSHIP IN BREAST SURGERY 2 TABLE OF CONTENTS 1. BACKGROUND 2. PROGRAM REQUIREMENTS 3. TRAINING OBJECTIVES (Annex 1) 4. TRAINING INSTITUTTIONS (Annex 2) 5. CANDIDATES 6. APPLICATION
ESSO ACCREDITED TRAINING FELLOWSHIP IN BREAST SURGERY 2 TABLE OF CONTENTS 1. BACKGROUND 2. PROGRAM REQUIREMENTS 3. TRAINING OBJECTIVES (Annex 1) 4. TRAINING INSTITUTTIONS (Annex 2) 5. CANDIDATES 6. APPLICATION
HOSPITAL MODELO - LA CORUÑA, Spain
 - LA CORUÑA, Spain General Information New breast cancer cases treated per year 150 Breast multidisciplinarity team members 8 Radiologists, surgeons, pathologists, medical oncologists, radiotherapists
- LA CORUÑA, Spain General Information New breast cancer cases treated per year 150 Breast multidisciplinarity team members 8 Radiologists, surgeons, pathologists, medical oncologists, radiotherapists
Evolution of Breast Surgery
 Evolution of Breast Surgery Natasha Rueth MD Surgical Oncologist Piper Breast Center and Alina Health Surgical Specialists Minneapolis, MN Definitions Radical Mastectomy: Removal of breast, chest muscles,
Evolution of Breast Surgery Natasha Rueth MD Surgical Oncologist Piper Breast Center and Alina Health Surgical Specialists Minneapolis, MN Definitions Radical Mastectomy: Removal of breast, chest muscles,
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
Loco-Regional Management After Neoadjuvant Chemotherapy
 1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
1 Loco-Regional Management After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health Cancer Center at Orlando Health Professor of Surgery,
Breast cancer incidence. Multidisciplinary Management in Breast Cancer. Outline. The Breast 11/10/2014. Incidence of breast cancer in Thailand
 Multidisciplinary Management in Breast Cancer October 8 th,2014 Ongart Somintara,M.D. Surgical Oncologist Department of Surgery, Khon Kaen University Breast cancer incidence USA : 2014 Estimate new case
Multidisciplinary Management in Breast Cancer October 8 th,2014 Ongart Somintara,M.D. Surgical Oncologist Department of Surgery, Khon Kaen University Breast cancer incidence USA : 2014 Estimate new case
Surgical treatment of BRCA mutated patients. Viviana Galimberti MD European Institute of Oncology Milan, Italy
 Surgical treatment of BRCA mutated patients Viviana Galimberti MD European Institute of Oncology Milan, Italy No pharmaceutical company funding was used I declare I have no conflicts of interest as regards
Surgical treatment of BRCA mutated patients Viviana Galimberti MD European Institute of Oncology Milan, Italy No pharmaceutical company funding was used I declare I have no conflicts of interest as regards
surgery choices For Women with Early-Stage Breast Cancer family EDUCATION PATIENT
 surgery choices For Women with Early-Stage Breast Cancer PATIENT & family EDUCATION U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health National Cancer Institute As a woman with
surgery choices For Women with Early-Stage Breast Cancer PATIENT & family EDUCATION U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES National Institutes of Health National Cancer Institute As a woman with
Recent Advances in Breast Cancer Treatment
 Recent Advances in Breast Cancer Treatment Pornchai O-charoenrat MD, PhD, FRCST, FICS Professor Chief, Division of Head-Neck & Breast Surgery Department of Surgery, Siriraj Hospital, THAILAND Recent Advances
Recent Advances in Breast Cancer Treatment Pornchai O-charoenrat MD, PhD, FRCST, FICS Professor Chief, Division of Head-Neck & Breast Surgery Department of Surgery, Siriraj Hospital, THAILAND Recent Advances
Table of contents. Page 2 of 40
 Page 1 of 40 Table of contents Introduction... 4 1. Background Information... 6 1a: Referral source for the New Zealand episodes... 6 1b. Invasive and DCIS episodes by referral source... 7 1d. Age of the
Page 1 of 40 Table of contents Introduction... 4 1. Background Information... 6 1a: Referral source for the New Zealand episodes... 6 1b. Invasive and DCIS episodes by referral source... 7 1d. Age of the
Frederick J. Duffy, Jr., MD, FACS and Brice W. McKane, MD, FACS BREAST RECONSTRUCTION
 Frederick J. Duffy, Jr., MD, FACS and Brice W. McKane, MD, FACS BREAST RECONSTRUCTION BREAST RECONSTRUCTION: A WOMAN S DECISION Options and Information Our approach to breast reconstruction entails a very
Frederick J. Duffy, Jr., MD, FACS and Brice W. McKane, MD, FACS BREAST RECONSTRUCTION BREAST RECONSTRUCTION: A WOMAN S DECISION Options and Information Our approach to breast reconstruction entails a very
Jessa Hospital - Hasselt, Belgium
 - Hasselt, Belgium General Information New breast cancer cases treated per year 336 Breast multidisciplinarity team members 19 Radiologists, surgeons, pathologists, medical oncologists, radiotherapists
- Hasselt, Belgium General Information New breast cancer cases treated per year 336 Breast multidisciplinarity team members 19 Radiologists, surgeons, pathologists, medical oncologists, radiotherapists
Breast Cancer. Common kinds of breast cancer are
 Breast Cancer A breast is made up of three main parts: glands, ducts, and connective tissue. The glands produce milk. The ducts are passages that carry milk to the nipple. The connective tissue (which
Breast Cancer A breast is made up of three main parts: glands, ducts, and connective tissue. The glands produce milk. The ducts are passages that carry milk to the nipple. The connective tissue (which
Breast Cancer. What is breast cancer?
 Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Scan for mobile link. Breast Cancer Breast cancer is a malignant tumor in or around breast tissue. It usually begins as a lump or calcium deposit that develops from abnormal cell growth. Most breast lumps
Groote Schuur Academic Hospital - Cape Town, South Africa
 - Cape Town, South Africa General Information New breast cancer cases treated per year 400 Breast multidisciplinarity team members 7 Radiologists, surgeons, pathologists, medical oncologists, radiotherapists
- Cape Town, South Africa General Information New breast cancer cases treated per year 400 Breast multidisciplinarity team members 7 Radiologists, surgeons, pathologists, medical oncologists, radiotherapists
Surgery for Breast Cancer
 Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Surgery for Breast Cancer 1750 Mastectomy - Petit 1894 Radical mastectomy Halsted Extended, Super radical mastectomy 1948 Modified radical mastectomy Patey 1950-60 WLE & RT Baclesse, Mustakallio 1981-85
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
ONCOLOGIC AND COSMETIC CHALLENGES DO NOT ROUTINELY OPPOSE BREAST CONSERVING SURGERY IN RETRO-AREOLA PRIMARY LESIONS
 ONCOLOGIC AND COSMETIC CHALLENGES DO NOT ROUTINELY OPPOSE BREAST CONSERVING SURGERY IN RETRO-AREOLA PRIMARY LESIONS SURGERY SYMPOSIUM Ines Buccimazza Breast Unit Department of Surgery Nelson R. Mandela
ONCOLOGIC AND COSMETIC CHALLENGES DO NOT ROUTINELY OPPOSE BREAST CONSERVING SURGERY IN RETRO-AREOLA PRIMARY LESIONS SURGERY SYMPOSIUM Ines Buccimazza Breast Unit Department of Surgery Nelson R. Mandela
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy
 Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Malignant Breast disorders
 Malignant Breast disorders RISK FACTORS FOR BREAST CANCER Family Hx.: first- and second-degree relatives with breast cancer and their age at diagnosis. RISK FACTORS FOR BREAST CANCER (cont.) Hormonal Risk
Malignant Breast disorders RISK FACTORS FOR BREAST CANCER Family Hx.: first- and second-degree relatives with breast cancer and their age at diagnosis. RISK FACTORS FOR BREAST CANCER (cont.) Hormonal Risk
University Clinical Center Banja Luka, Breast Center - Banja Luka, Bosnia and Herzegovina
 - Banja Luka, Bosnia and Herzegovina General Information New breast cancer cases treated per year 245 Breast multidisciplinarity team members 23 Radiologists, surgeons, pathologists, medical oncologists,
- Banja Luka, Bosnia and Herzegovina General Information New breast cancer cases treated per year 245 Breast multidisciplinarity team members 23 Radiologists, surgeons, pathologists, medical oncologists,
Measure Definition Benchmark Endorsed By. Measure Definition Benchmark Endorsed By
 Process Risk Assessment Tumor Site: Breast Process Presence or Risk absence Assessment of cancer in first-degree blood relatives documented in patients with invasive breast Presence cancer or absence of
Process Risk Assessment Tumor Site: Breast Process Presence or Risk absence Assessment of cancer in first-degree blood relatives documented in patients with invasive breast Presence cancer or absence of
Breast Cancer: Current Approaches to Diagnosis and Treatment
 Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study
 [ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
[ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
Nipple Sparing Mastectomy: Tips & Tricks. Rebecca Nelson, MD MSc FRCSC Plastic & Reconstructive Surgeon, Burnaby Hospital
 Nipple Sparing Mastectomy: Tips & Tricks Rebecca Nelson, MD MSc FRCSC Plastic & Reconstructive Surgeon, Burnaby Hospital Nipple Sparing Mastectomy (NSM) Introduction & Technique Safety Evidence Indications/Contraindications
Nipple Sparing Mastectomy: Tips & Tricks Rebecca Nelson, MD MSc FRCSC Plastic & Reconstructive Surgeon, Burnaby Hospital Nipple Sparing Mastectomy (NSM) Introduction & Technique Safety Evidence Indications/Contraindications
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity.
 Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
Case Scenario 1: This case has been slightly modified from the case presented during the live session to add clarity. Background: 46 year old married premenopausal female with dense breasts has noticed
BREAST RECONSTRUCTION POST MASTECTOMY
 UnitedHealthcare Commercial Coverage Determination Guideline BREAST RECONSTRUCTION POST MASTECTOMY Guideline Number: SUR057 Effective Date: January 1, 2019 Table of Contents Page INSTRUCTIONS FOR USE...
UnitedHealthcare Commercial Coverage Determination Guideline BREAST RECONSTRUCTION POST MASTECTOMY Guideline Number: SUR057 Effective Date: January 1, 2019 Table of Contents Page INSTRUCTIONS FOR USE...