Introduction. Agenda. Pathogenesis. Pathogenesis and Clinical Implications. Pathogenesis and Clinical Implications
|
|
|
- Gavin Reynolds
- 5 years ago
- Views:
Transcription
1 Surface Epithelial Tumors of the Ovary Part II Invasive Carcinomas Moderator Robert J. Kurman, M.D. Discussants Kathleen R. Cho, M.D. Anais Malpica, M.D. Patricia A. Shaw, M.D. Robert A. Soslow, M.D. C. Blake Gilks, M.D. Agenda Introduction Overview of presentations New model of pathogenesis with clinical implications Molecular pathology with morphological correlation Grading Two tier Three tier Histotyping Panel and Audience Discussion of unknown cases Pathogenesis Introduction Robert J. Kurman, M.D. The Johns Hopkins University School of Medicine Since serous borderline tumors are rarely associated with invasive serous carcinomas it is generally believed that they are unrelated But some SBTs recur as carcinomas And mucinous, endometrioid, and clear cell carcinomas are often associated with their respective carcinomas How can these disparate findings be reconciled? Pathogenesis and Clinical Implications Most ovarian cancers present in an advanced stage and survival is poor Survival for stage I tumors is reported to be greater than 90% Accordingly a great effort has been made to detect ovarian cancer when it is stage I Pathogenesis and Clinical Implications So far this effort, using CA 125 as a tumor marker and vaginal ultrasound, has been unsuccessful Why? Can something be done to improve this?
2 Molecular Pathology of Ovarian Carcinoma with Morphological Correlation Kathleen R. Cho, M.D. Molecular Genetics The major histotypes of ovarian carcinomas have distinctive, albeit partially overlapping, molecular signatures Genetic alterations in ovarian carcinomas deregulate specific cell signaling pathways Ovarian cancer treatment will likely evolve to include drugs that inhibit the signaling pathways known to be activated in a given tumor ( personalized medicine ) Molecular Genetics (Endometrioid carcinomas as example) Does histologic type matter? Does tumor grade matter? What role can practicing pathologists expect to play in stratifying ovarian cancer patients into appropriate treatment groups? Grading of Ovarian Carcinoma Two Approaches Anais Malpica, M.D. Patricia A. Shaw, M.D. Grading Historically there has been no uniformly accepted grading system Shimizu et al have proposed a three tier system modeled after the Elston grading system for breast carcinoma Applicable to all histological types of ovarian cancer Malpica et al have proposed a two tier system Applicable only to serous carcinoma Histotyping of Ovarian Carcinoma Robert A. Soslow, M.D.
3 Histotyping Once borderline tumors are excluded does histotyping have any clinical relevance? How do we distinguish borderline endometrioid and clear cell borderline tumors from their respective carcinomas? How do we distinguish endometrioid from serous carcinomas when they are poorly differentiated? What exactly constitutes clear cell carcinoma? Case Discussion Panel and Audience Unknown cases posted on the ISGYP and USCAP websites Histotyping and grading Pathogenesis of Ovarian Cancer Lessons from Morphology and Molecular Biology A Proposed Model with Clinical Implications Robert J Kurman, M.D. Key Issues Epithelial carcinomas of the ovary can be divided into two categories designated Type I and Type II Type I carcinomas are slow growing, indolent tumors that develop from atypical proliferative (borderline) tumors Type II carcinomas are rapidly growing, aggressive tumors which develop de novo Understanding the pathogenesis of Type I and Type II carcinomas provides clues for new approaches to early detection and treatment Histological Classification of Ovarian Tumors Serous Borderline Tumors The Birth of Borderline FIGO Classification Tumors of the Ovary Cystomas (a) Benign cystadenomas (b) Cystadenomas with proliferating activity of the epithelial cells and nuclear abnormalities but with no infiltrative destructive growth (low potential malignancy) (c) Cystadencarcinomas WHO Classification Ovarian Tumours Surface Epithelial-Stromal Tumors Benign Cystadenoma Adenofibroma Of borderline malignancy (carcinomas of LMP) Cystadenoma Adenofibroma Malignant Adenocarcinoma Surface papillary carcinoma Malignant adenofibroma The borderline group was carved out of the carcinoma category and defined as a noninvasive group of tumors displaying cellular proliferation and cytologic atypia Kottmeier H In Carcinoma of the cervix, endometrium and ovary. Year Book Publishers, Chicago, 1962 pp
4 Why was Borderline Created? To account for Intermediate behavior between cystadenomas and frankly invasive carcinomas Inability to predict the outcome of an individual tumor Histological Classification of Ovarian Tumors WHO Classification Ovarian Tumours Surface Epithelial-Stromal Tumors Benign Cystadenoma Adenofibroma Of borderline malignancy (carcinomas of LMP) Cystadenoma Adenofibroma Malignant Adenocarcinoma Surface papillary carcinoma Malignant adenofibroma WHO Classification Ovarian Tumours Surface Epithelial-Stromal Tumors Benign Cystadenoma Adenofibroma Borderline Tumor Cystadenoma Adenofibroma Malignant Adenocarcinoma Surface papillary carcinoma Adenocarcinofibroma (malignant adenofibroma) Dualistic Model of Ovarian Carcinogenesis Type I Type II Dualistic Model of Ovarian Carcinogenesis Type I Type II Low-grade High-grade Low-grade Arise from precursor lesions in a stepwise fashion Cystadenomas Borderline Tumors High-grade Arise de novo Shih and Kurman Am J Pathol 164:1511, 2004 Shih and Kurman Am J Pathol 164:1511, 2004 Dualistic Model of Ovarian Carcinogenesis Type I Type II Dualistic Model of Ovarian Carcinogenesis Type I Type II Low-grade Arise from precursor lesions in a stepwise fashion Cystadenomas Borderline Tumors Typically present as stage I High-grade Arise de novo Typically present as advanced stage Low-grade Arise from precursor lesions in a stepwise fashion Cystadenomas Borderline Tumors Typically present as stage I Slow growing, indolent High-grade Arise de novo Typically present as advanced stage Rapid growing, aggressive Shih and Kurman Am J Pathol 164:1511, 2004 Shih and Kurman Am J Pathol 164:1511, 2004
5 Dualistic Model of Ovarian Carcinogenesis Type I Type II Dualistic Model of Ovarian Carcinogenesis Type I Type II Low-grade Arise from precursor lesions in a stepwise fashion Cystadenomas Borderline Tumors Typically present as stage I Slow growing, indolent Generally remain low-grade High-grade Arise de novo Typically present as advanced stage Rapid growing, aggressive Shih and Kurman Am J Pathol 164:1511, 2004 Low-grade Arise from precursor lesions in a stepwise fashion Cystadenomas Borderline Tumors Typically present as stage I Slow growing, indolent Often remain low-grade Can progress to high-grade High-grade Arise de novo Typically present as advanced stage Rapid growing, aggressive Shih and Kurman Am J Pathol 164:1511, 2004 A Classification of Ovarian Carcinoma Based on Clinical, Pathologic, and Molecular Features Type I Low-grade micropapillary serous carcinoma Mucinous carcinoma Endometrioid carcinoma Clear cell carcinoma Malignant Brenner tumor Type II High-grade serous carcinoma MMMT (carcinosarcoma) The Pathogenesis of Ovarian Cancer Traditional View Ovarian cancer is regarded as a single disease and treated with one approach The reason is because most ovarian cancer is serous carcinoma Shih and Kurman Am J Pathol 164:1511, 2004 Serous Carcinogenesis - Current View Well differentiated carcinoma progresses to poorly differentiated serous carcinoma Carcinoma begins in the ovary (stage I), spreads to the pelvic (stage II) and abdominal cavities (stage III) and beyond (stage IV) Well diff Poorly diff Mod diff Poorly diff Relationship of BOTs to Invasive Carcinoma SBTs are rarely associated with invasive carcinoma SBTs are a distinct entity unrelated to invasive carcinoma MBTs are frequently associated with invasive carcinoma Are some BOTs precursors and others not?







6 Can SBTs be divided into benign and malignant subtypes? The Pathogenesis of Ovarian Cancer Hierarchical Branching Atypical Proliferative Serous Tumor Nonhierarchical Branching Micropapillary Serous Carcinoma, Noninvasive Recent advances in understanding the pathogenesis of ovarian carcinomas come from studies of serous and mucinous borderline tumors Tumors with a hierarchical pattern had significantly better outcome than those with a nonhierarchical pattern Burks et al Am J Surg Pathol 20: , 1996 Noninvasive Micropapillary Serous Carcinoma Noninvasive MPSC with focus of early invasion Invasive Low-grade MPSC Grade 1 nuclei The Proposal that Noninvasive Micropapillary Tumors were Noninvasive Carcinomas Microsoft The Controversy Noninvasive tumors with a micropapillary pattern are variants of a borderline tumor and should not be classified as a noninvasive carcinoma because there is no significant difference in the outcome of typical stage I SBTs compared to stage I noninvasive MPSCs




 1979")
7 True but The Controversy As reported in the literature there is also no significant difference in the outcome of typical stage I SBTs compared to Bona fide invasive stage I carcinoma which is >90% The Controversy There is no significant difference in the outcome of typical advanced stage SBTs compared to MPSCs if stratified into implant type Specifically, invasive implants determine behavior True but virtually all studies have shown that MPSCs are significantly more often associated with invasive implants What are Invasive Implants? Sharp line between implant and underlying tissue Looks like primary SBT Noninvasive Implant Irregular infiltration into underlying tissue Looks like well differentiated serous carcinoma Courtesy Debra Bell Invasive Implant Vaginal Recurrence (1993) Primary tumor Invasive implant Recurrent carcinoma All look the same

 Reports of invasive implants associated with typical borderline tumors")
 Patient with bilateral typical SBTs with implants in parametrium and pelvic peritoneum One")
8 If something looks like a duck, walks like a duck, and quacks like a duck It is a duck! Invasive implants are low-grade serous carcinomas Are Typical SBTs Ever Associated with Invasive Implants? for all practical purposes they are not Typical SBTs are benign tumors that have the potential to undergo malignant transformation to a low-grade micropapillary serous carcinoma (noninvasive or invasive) Reports of invasive implants associated with typical borderline tumors almost certainly missed occult areas of carcinoma (noninvasive or invasive MPSC) in the primary SBT even when the tumor was adequately sampled (1 block/cm of the greatest tumor dimension) Patient with bilateral typical SBTs with implants in parametrium and pelvic peritoneum One block/cm of greatest tumor dimension Implant in Parametrium Peritoneal Implant Invasive Implant Invasive Implant



 vs Group 2")
 83 months Shvartsman")
9 Bilateral Typical SBTs Sampling 1 block/cm Additional sections from the SBTs Invasive Low-grade MP Serous Carcinomas Grade 1 nuclei Additional sections from the SBTs Up to 75% of low-grade invasive MPSCs are associated with SBTs Over 90% of these SBTs display a micropapillary pattern Conclusion - SBTs with a micropapillary pattern (noninvasive MPSCs) are the immediate precursors of low-grade invasive MPSCs Smith Sedhev et al Amer J Surg Pathol 27:725-36,2003 Malpica et al Amer J Surg Pathol 28: ,2004 Behavior of Advanced Stage LG- Invasive MPSCs Compared to SBTs that Recur as LG-Invasive MPSCs Group 1 - LG-Invas MPSC (n=112) vs Group 2 - SBTs recurring as LG Invas MPSC (n=41) Survival Group 1-82 months Survival Group months Survival Group 2 (from relapse as MPSC to death) 83 months Shvartsman et al Unpublished data
 CA SBT * Low-grade Serous Ca 31/51 (61%) 15/22 (68%) 2/25 (8%) 1/12 (8%) are characterized by distinctive molecular genetic changes * Includes Atypical Prolif Tumor and")
 98/140 (70%) ** I-M Shih et al **p53* Includes mutation Atypical rate")
10 In addition to clincal and pathologic differences Frequency of KRAS/BRAF and p53 Mutations in Ovarian Serous Tumors Tumor KRAS/BRAF p53 Low-grade (invasive micropapillary serous) CA High-grade (conventional serous) CA SBT * Low-grade Serous Ca 31/51 (61%) 15/22 (68%) 2/25 (8%) 1/12 (8%) are characterized by distinctive molecular genetic changes * Includes Atypical Prolif Tumor and noninvasive MPSC I-M Shih et al Frequency of KRAS/BRAF and p53 Mutations in Ovarian Serous Tumors Tumor SBT * Low-grade Serous Ca KRAS/BRAF 31/51 (61%) 15/22 (68%) p53 2/25 (8%) 1/12 (8%) Gene expression profiles in SBT, LG MPSC and HG serous carcinoma Low-grade High-grade Normal High-grade Serous Ca ** 1/140 ( <1%) 98/140 (70%) ** I-M Shih et al **p53* Includes mutation Atypical rate Proliferative is 82% Tumor on purified and noninvasive epithelial MPSC cells from tumor samples Gilks et al., Gyncol Oncol, 96:684, 2005 Hampton et al., Oncogene, 24:1053, 2005 Birrer et al., Cancer Res, 65:10602, 2005 SBT and LG MPSC have similar profiles distinct from HG ser CA What is the Pathogenesis of Low-grade Micropapillary Serous Carcinoma? Serous Cystadenoma Containing a Small Atypical Proliferative Serous Tumor (APST) Borderline tumor Cyst Before After (Cancer Res, 64:6915, 2004)











11 Mutations of KRAS and BRAF Precede the Development of APSTs Pathogenesis of Low Grade Micropapillary Serous Carcinoma APST Noninvasive LG MPSC Noninvasive LG MPSC with focus of invasion Invasive LG MPSC 3 mm Serous cystadenoma adjacent to APST BRAF mutation Codon 599, T1796A APST in Serous cystadenoma BRAF mutation Codon 599, T1796A (Cancer Res, 64:6915, 2004) The Usual Type of Serous Carcinoma What is the Origin of High-grade Serous carcinoma? Grade 3 nuclei Is high-grade and rarely associated with SBTs High-grade Serous Carcinoma Pathogenesis Development of Conventional (high-grade) serous carcinoma The precursors of highgrade serous carcinomas are not well characterized It has been proposed that they develop de novo Bell DA, Scully RE Cancer 73: ,1994 From the surface epithelium or inclusion cysts Tumor 7mm Ovary Mutation of p53 is a very early event in the development of high-grade serous carcinoma Courtesy Jeff Boyd




 Developing from an Atypical Proliferative")

12 Low-grade pathway Dual Pathways of Serous Carcinogenesis Early Events Low-grade pathway High-grade pathway Low-grade serous carcinoma High-grade serous carcinoma Borderline Low-grade carcinoma xxxxxxxxxxxxxxx High-grade pathway xxxxxxxxxxxxxxx High-grade carcinoma KRAS or BRAF Mutation p53 Mutation Grade is a Defining Feature of Invasive Serous Carcinomas Serous carcinoma can be divided into two distinct types Low-grade micropapillary serous carcinoma High-grade serous carcinoma High-grade carcinoma High-grade pathway Not an issue of progression, these are distinct and separate tumor types High-grade Serous Carcinoma (HG Ser CA) Developing from an Atypical Proliferative Serous Tumor (APST) Grading of Serous Carcinoma Low-grade serous carcinoma Case A Case B High-grade serous carcinoma (Reiko et al., in press) Identical KRAS mutation in APST and HG Ser CA No p53 mutation
 Survival of stage I MBTs is 100% Survival of advanced stage MBTs")
 It is now known that PMP results from a ruptured mucinous appendiceal adenoma Ovarian involvement")

?")
13 Progression in the Type I Pathway Serous Tumors Cystadenoma APST Noninvasive MPSC HG Ser CA Invasive MPSC Very rare event Mucinous Borderline Tumors (MBTs) Survival of stage I MBTs is 100% Survival of advanced stage MBTs reported in the literature is 50% but Over 80% of advanced stage MBTs reported are associated with pseudomyxoma peritonei (PMP) It is now known that PMP results from a ruptured mucinous appendiceal adenoma Ovarian involvement is secondary Advanced Stage (MBTs)? Ovarian Tumor Several studies have now shown that what appear to be ovarian MBTs are in fact metastatic carcinomas typically from the upper GI tract (biliary tree and pancreas) or cervix Cervical Tumor Ovarian Tumor Advanced Stage (MBTs)? Once MBTs associated with PMP (>80%) are eliminated from consideration and Metastatic carcinomas involving the ovaries that masquerade as MBTs are excluded HPV 16 in situ hybridization

14 Advanced Stage (MBTs)? There are none! The Relationship of MBTs to Mucinous Carcinoma Molecular Studies Molecular genetic studies using KRAS mutations as a marker Approximately 50% of mucinous carcinomas, MBTs and mucinous cystadenomas have KRAS mutations of codon 12 and 13 Using laser capture microdissection the identical KRAS mutation is present in all three of the tumor components in the same case (mucinous cystadenoma, MBT and mucinous carcinoma) Mok SC, et al Cancer Res 53:1489, 1993 Relationship of MBTs to Mucinous Carcinoma Clinical, morphologic, and molecular data suggest there is a progression Mucinous Adenoma zzzz Atypical Prolif Tumor Intraepith Ca Microinva Ca Mucinous Ca Mucinous Carcinoma Mean size of both primary mucinous carcinomas and MBTs is 18 cm Majority of primary mucinous carcinomas are well differentiated and unilateral at presentation Primary mucinous carcinomas are often focal developing within MBTs and mucinous cystadenomas Survival for stage I is >90% Borderline Endometrioid and Clear Cell Tumors The Relationship of Endometrioid Adenocarcinoma To Endometrioid Borderline Tumors Not a single well documented case associated with malignant behavior reported since the category was introduced by FIGO in 1971 and incorporated into the WHO classification in 1973 Frequently associated with their respective carcinomas Endometriosis Courtesy Kathy Cho Atypical Endometriosis Genetic Alterations: Borderline Endometrioid Tumor PTEN, K-Ras, -catenin Microsatellite Instability Low-grade Endometrioid Adenocarcinoma
15 Endometrioid Carcinoma Frequently presents as a well differentiated stage Ia tumor associated with an atypical proliferative endometrioid tumor/adenofibroma Survival for these tumors is close to 100% Advanced stage tumors are relatively uncommon when classified using strict criteria Clear Cell Carcinoma Poorly understood because it has not been well characterized In literature and based on personal experience clear cell carcinoma includes Solid endometrioid carcinomas with extensive secretory change Poorly differentiated carcinomas containing cells with clear cytoplasm Classic clear cell carcinoma (tubulocystic, papillary and solid patterns) Summary of Type I Tumors Low-grade Develop in a slow, stepwise fashion from Cystadenomas Atypical proliferative (borderline) tumors Similar to Type I endometrial carcinomas - complex hyperplasia and complex atypical hyperplasia precursors Typically present as stage I Are generally Indolent and remain low-grade Some progress Summary of Type II Tumors High-grade adenocarcinoma Includes high-grade serous carcinoma, MMMT, adenocarcinoma NOS, and undifferentiated carcinoma Preliminary molecular data suggests they are similar Arise de novo Present in advanced stage Highly aggressive Dualistic Model of Ovarian Carcinogenesis Screening for Ovarian Cancer TypeI & TypeII Tumors Clinical Implications Looking to the future Understanding pathogenesis clarifies misconceptions in the current approaches to early detection Ovarian cancer is not a single disease Appreciation of diverse molecular pathways of carcinogenesis will permit more customized approaches to detection

16 Goal of Early Detection Detect stage I ovarian carcinoma Survival of stage I disease is > 90% 75-80% of ovarian carcinoma presents as advanced stage disease implying 20-25% are stage I Most patients will be successfully treated by surgery There will be limited need for cytotoxic chemotherapy Detection of Stage I Ovarian Cancer The vast majority of ovarian cancers are serous carcinomas but how many are stage I? Carcinomas Stage Distribution (n=220) Carcinomas Stage Distribution (n=220) Cell Type Stage I Stage II-IV Cell Type Stage I Stage II-IV Serous 4% 96% Serous 4% 96% Mucinous 83% 17% Mucinous 83% 17% Endometrioid 53% 47% Endometrioid 53% 47% Clear cell 36% 64% Clear cell 36% 64% Brenner 100% 0% Brenner 100% 0% Seidman et al Int J Gynecol Pathol 23:41,2003 Seidman et al Int J Gynecol Pathol 23:41,2003 Bilaterality and Size Serous carcinomas tend to be small (in the ovary) and bilateral at presentation The bulk of the tumor is often outside of the ovary High-grade Serous Carcinoma






17 High-grade Serous Carcinoma Detection of Stage I Ovarian Serous Carcinoma Since ovarian carcinomas are small, even when there is extraovarian spread They will not be detected by pelvic exam or transvaginal ultrasound Is it possible to detect stage I serous carcinoma? Courtesy R Bristow Is Ovarian Serous Carcinoma Ever Stage I? Thoroughly staged, stage I serous carcinoma sent for consultation because of microscopic lesion in the omentum thought to represent mesothelial hyperplasia Ovary Omentum Omentum






18 Ovary p53 Omentum p53 Ovary Ki-67 Omentum Ki-67 Is Ovarian Serous Carcinoma Ever Stage I? Hardly ever! Other Problems Not all ovarian serous carcinomas start in the ovary Serous carcinomas identical to those in the ovary can develop after bilateral salpingo oophorectomy These are primary peritoneal serous carcinomas which at diagnosis are stage II or III Other Problems Not all ovarian serous carcinomas start in the ovary Small serous carcinomas detected in the fimbria of women with BRCA mutations undergoing prophylactic oophorectomy Not previously recognized because fallopian tubes are not routinely serially sectioned? These tumors are stage II ovarian carcinomas at diagnosis Problems in the Detection of Stage I Ovarian Serous Carcinoma Summary Serous carcinomas that start in the ovary spread rapidly Lead time is brief and nearly always present in advanced stage Cervix model does not apply Some serous carcinomas start in the peritoneum or fallopian tube These are advanced stage at diagnosis
19 Detection of Stage I Ovarian Serous Carcinoma (Type II) Bottom Line It will be virtually impossible to detect stage I serous carcinoma using presently available technology Implications for Treatment of High-grade Serous Carcinoma (Type II Tumor) The most important predictor of outcome (more important than stage) is whether the tumor has been adequately debulked (optimal cytoreduction) Over time this has shifted from <2cm to <1.5 cm to <1cm Implications for Treatment of Serous Carcinoma (Type II Tumor) A Paradigm Shift Successful treatment will depend on detection of minimal (microscopic to 1 cm) ovarian serous carcinoma (stage is irrelevant) Using a panel of sensitive and specific molecular markers that precede development of morphologically recognizable precursors Treatment will be instituted based on marker detection only Classification of Ovarian Tumors Why do SBTs have an intermediate behavior? Because they are a heterogeneous group mainly benign (atypical proliferative) and a small number of noninvasive low-grade MPSCs which can implant (so-called invasive implants but in fact are metastatic low-grade carcinomas) Evolution in our Understanding of Ovarian Carcinogenesis Creation of the borderline category was an important achievement that focused our attention on a subset of tumors that had previously been buried in the category of carcinoma Over the last 30 years significant advances have elucidated our understanding of these tumors Evolution in our Understanding of Ovarian Carcinogenesis The borderline category and the concept that there is a group of tumors whose behavior is unpredictable has now outlived its usefulness and needs to be replaced
 Borderline kathcho@umich.edu Molecular Pathology of Ovarian Carcinoma with Morphological Correlation Kathleen R. Cho, M.")
20 Classification of Ovarian Tumors Cystadenoma/adenofibroma Atypical proliferative tumor Noninvasive (intraepithelial) carcinoma Invasive carcinoma (Type I) Low-grade micropapillary serous Mucinous Endometrioid Clear cell Malignant Brenner tumor High-grade carcinoma (Type II) Borderline Molecular Pathology of Ovarian Carcinoma with Morphological Correlation Kathleen R. Cho, M.D. Comprehensive Cancer Center and Departments of Pathology and Internal Medicine University of Michigan Medical School Key Issues The major histotypes of ovarian carcinomas have distinctive, albeit partially overlapping, molecular signatures Major Types of Ovarian Carcinoma Genetic alterations in ovarian carcinomas deregulate specific cell signaling pathways Serous (50%) Mucinous (10%) Ovarian cancer treatment will likely evolve to include drugs that inhibit the signaling pathways known to be activated in a given tumor ( personalized medicine ) Endometrioid (20%) Clear cell (10%) Treatment Guidelines for Ovarian Carcinoma Standard therapy is surgical debulking followed by chemotherapy (carboplatin + paclitaxel) In contrast to endometrial carcinoma, Rx is NOT histotype dependent Treatment of recurrent/drug-resistant disease remains a major challenge References: 1) National Comprehensive Cancer Network, NCCN Clinical Practice Guidelines in Oncology, ) RF Ozols, Challenges for chemotherapy in ovarian cancer. Ann Oncol 17(Supp 5), 2006 On the horizon Personalized medicine using drugs that target specific molecular defects in tumor cells Ovarian carcinomas have characteristic genetic alterations, but the frequency with which a given gene is mutated varies substantially with: Histologic type Tumor grade What role will pathologists play in determining the specific molecular defects in ovarian cancer cells?
 Clear cell (?) Reference: 1) Bell DA. Origins and Molecular Pathology of Ovarian Cancer.")
21 Major Types of Ovarian Carcinoma: Characteristic Genetic Alterations (Selected) OvCA Samples Highthroughput analysis of RNA and DNA Serous (p53) Mucinous (K-RAS) What are we learning about ovarian cancer? Endometrioid (CTNNB1, PTEN, K-RAS, p53) Clear cell (?) Reference: 1) Bell DA. Origins and Molecular Pathology of Ovarian Cancer. Mod Pathol, 18:S19-32, 2005 Gene Expression Profiling of Ovarian Carcinomas Affymetrix oligonucleotide microarrays U133A array: approximately 22,000 probe sets (14,500 genes) Data Processing: quantile normalization to adjust for differences in probe intensity across different chips Statistical Analyses: Principal component analysis First two principal components for 103 human samples, all probe-sets, log-transformed data Clear Cell (N=8) Endometrioid (N=37) Mucinous (N=13) Serous (N=41) Normal (N=4) First Principal Component Ovarian Endometrioid Adenocarcinoma (OEA) Tumor Progression Model Ovarian carcinomas arise through a multistep process in which clonal selection acts on cells with somatic mutations and altered gene expression to allow outgrowth of progeny with increasingly aggressive growth properties Endometriosis Atypical Endometriosis Endometriosis with Epithelial Hyperplasia Endometrioid Adenocarcinoma Genetic Alterations: Tumor suppressor genes (PTEN, p53) DNA mismatch repair genes (MSH2, MSH6, MLH1, MLH3) Oncogenes (K-RAS, CTNNB1/ -catenin) The genes mutated in cancer frequently encode proteins that function in conserved signaling pathways
 The Wnt signaling pathway is frequently deregulated in cancers Wnt Signaling Overview Nucleus TCF Target Genes Wnt/ -catenin/tcf Pathway Defects Ovarian")
 All OEAs evaluated for mutations in CTNNB1 ( -cat) exon 3 Other Wnt/ -cat/tcf Pathway Defects in Ovarian Endometrioid Adenocarcinomas: APC Results Missense mutations found in 18 OEAs (25%) OEAs")
 OE-32T CGA TGA (Codon 1114) OE-18T OE-29T TOV-112D (ß-cat) B OSE CTNNB1 or APC mutations present in 26% of OEAs WNT PATHWAY DEFECTS: CORRELATION WITH LOW TUMOR GRADE")
22 Wnt Signaling: Importance and overview Cytoplasm Wnt signaling plays major roles in: Cell proliferation Differentiation Morphogenesis -catenin plays a central role in the signal transduction pathway to the nucleus (canonical pathway) The Wnt signaling pathway is frequently deregulated in cancers Wnt Signaling Overview Nucleus TCF Target Genes Wnt/ -catenin/tcf Pathway Defects Ovarian Endometrioid Adenocarcinomas (OEAs) 72 primary OEAs collected (CHTN, UM, Kumamoto U.) All OEAs evaluated for mutations in CTNNB1 ( -cat) exon 3 Other Wnt/ -cat/tcf Pathway Defects in Ovarian Endometrioid Adenocarcinomas: APC Results Missense mutations found in 18 OEAs (25%) OEAs with CTNNB1 mutations show nuclear accumulation of -cat by immunohistochemical staining OE-2T OE-28T 75 Kd 50 Kd 35 Kd 13T 15T 32T SW626 A C G T A C G T A C G T A C G T Mutant Wild Type Mutant Wild Type OE-32T CGA TGA (Codon 554) OE-32T CGA TGA (Codon 1114) OE-18T OE-29T TOV-112D (ß-cat) B OSE CTNNB1 or APC mutations present in 26% of OEAs WNT PATHWAY DEFECTS: CORRELATION WITH LOW TUMOR GRADE AND STAGE Activating Mutations (PIK3CA) -cat or APC mut -cat or APC wt Grade Grade 2 or p = 1.2 X 10-6 (Fisher s exact) Inactivating Mutations -cat or APC mut -cat or APC wt Stage 1 or Stage 3 or p = 1.5 X 10-5 Modified from : DA Altomare and JR Testa (Oncogene, 2005)
23 Mutational analysis of PTEN (n=72) and corresponding mutations of CTNNB1 and K-RAS in OEAs Tumor PTEN mutation CTNNB1 mutation K-RAS mutation ID (exons 1-9) (exon 3) (codons 12 and 13) OE-13T del T, exon 4, frameshift TCT TGT None OE-19T GAG TAG, exon 1, nonsense TCT TAT None OE-31T TAT AAT, exon 5 (Tyr Asn) None None OE-48T ACT CCT, exon 5 (Thr Pro) GGA GAA None OE-54T ACG AGG, exon 5 (Thr Arg) GAC GCC None OE-55T del ACTT, exon 8, frameshift TCT TTT None OE-63T CAG TAG, exon 6, nonsense None None OE-75T GAT GGT, exon 5 (Gly Asp) None None Mutational analysis of PIK3CA (n=72) and corresponding mutations of PTEN and CTNNB1 in OEAs Tumor ID PIK3CA mutation PTEN mutation CTNNB1 mutation OE-21T H1047R, exon 20 None GGA GAA (Gly34Glu) OE-31T H1047R, exon 20 TAT AAT, exon 5 (Tyr Asn) None OE-55T E542K, exon 9 del ACTT, exon 8, frameshift TCT TTT (Ser37Phe) OE-71T E542K, exon 9 None GGA GAA (Gly34Glu) OE-75T H1047R, exon 20 GAT GGT, exon 5 (Gly Asp) None Mutations in the Wnt/ -cat/tcf and PI3K/Pten/Akt Pathways Frequently Co-Occur in OEAs Correlation of PTEN and/or PIK3CA mutation with Wnt/ -cat/tcf pathway defects in OEAs PTEN or PIK3CA mutation Wild type PTEN and PIK3CA Wnt/ -cat/tcf pathway DEFECTIVE Wnt/ -cat/tcf pathway INTACT p=.0024 two-sided Fisher s exact test Second Principal Component First two principal components for 99 tumors, all probe-sets, log-transformed data P 3 P P OE First Principal Component P 3 3 P P Green = CTNNB1 mut Blue = APC mut P = Pten mut 3 = PIK3CA mut Second Principal Component First two principal components for 99 tumors, all probe-sets, log-transformed data P 3 P P OE First Principal Component P 3 3 P P Green = CTNNB1 mut Blue = APC mut P = Pten mut 3 = PIK3CA mut IARC TP53 DATABASE 8% 7% 7% 0% The Majority Of TP53 Mutations Are Missense Mutations Germline 6% 72% missense frameshift nonsense silent other splice 9% 7% Somatic 4% 2% 5% 73% IARC TP53 DATABASE Mut. frequency Missense mut. Missense Mutations are Clustered in the DNA-binding Domain N- -C Transactivation (1-42; 43-62) Proline-rich (65-97) 245 DNA binding ( ) 282 Oligomerisation ( ) Regulation ( ) 1 % 2.3 % 80 % 3.4 % 0. 3% 50.8 % 45.4 % 82.1 % 36.4 % 72.7 % September p53.iarc.fr September p53.iarc.fr

24 TP53 Mutations in OEAs: Exons 5-8 p53 Mutations in OEAs: Association with High Tumor Grade and Stage 32 mutations identified (n=72) 81% missense Remainder nonsense or frameshift 5 additional tumors showed intense and diffuse nuclear accumulation of p53 protein Presumptive missense mutations outside of region sequenced Mutant p53 Wild type p53 Mutant p53 Wild type p53 Grade 1 Grade 2 or Stage 1 or 2 Stage 3 or p =.0009 p = 3 X p53 Mutations in OEAs: Negative Association with Wnt/ -Cat and/or PI3K/Pten Pathway Defects Mutant p53 Wild type p53 Wnt/ -cat and/or PI3K/Pten Pathway DEFECT p = 1.5 X 10-6 Wnt/ -cat and PI3K/Pten Pathways INTACT Second Principal Component First two principal components for 99 tumors, all probe-sets, log-transformed data P 3 P P OE First Principal Component P 3 3 P P Green = CTNNB1 mut Blue = APC mut P = Pten mut 3 = PIK3CA mut p53 mutation Second Principal Component First two principal components for 99 tumors, all probe-sets, log-transformed data P 3 P P OE First Principal Component P 3 3 P P Green = CTNNB1 mut Blue = APC mut P = Pten mut 3 = PIK3CA mut p53 mutation Second Principal Component First two principal components for 99 tumors, all probe-sets, log-transformed data OS OM OC OE First Principal Component

25 Conclusions Why does any of this matter? The findings support subdivision of ovarian endometrioid adenocarcinomas into two subgroups Low grade OEAs are characterized by frequent Wnt/ -cat/tcf and PI3K/Pten pathway defects, infrequent p53 mutations, favorable outcome High grade OEAs are characterized by frequent p53 mutations, infrequent Wnt/ -cat/tcf and PI3K/Pten pathway defects, poorer outcome High grade OEAs have a similar gene expression profile to ovarian serous carcinomas (both have frequent p53 mutations) Powis, G. et al. Clin Cancer Res 2006;12: Copyright 2006 American Association for Cancer Research What can pathologists do to help? Current morphological classification provides useful information Within a given histotype, specific molecular alterations are associated with tumor grade Immunostaining for signaling pathway components, properly interpreted, can substitute for selected mutational analyses Nuclear accumulation of -catenin (vs. membranous) Loss of Pten (increased pakt, ps6) Nuclear accumulation of p53 Serous Carcinoma Based on the cytologic atypia (primary parameter) and mitotic index (secondary parameter) o Two types High grade (marked variation [ 3:1] in nuclear size and shape with irregular chromatin and variable presence of macronucleoli, and a mitotic index >12 mitoses per 10 high power fields) Low grade (uniform round or oval nuclei with evenly distributed chromatin and variable At present, it seems that ovarian cancer represents a heterogeneous group of diseases o Different histologic parameters may needed to determine the biological behavior of different tumors Histologic grade has been found to be an important prognostic factor in cases of ovarian carcinoma o However, there is no system that is universally used for grading these neoplasms Grading of Ovarian Cancer Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center International Society of Gynecological Pathologists Symposium 2007 Bibliography 1. Lee KR and Scully RE. Mucinous tumors of the ovary. A clinicopathologic study of 196 borderline tumors (of intestinal type) and carcinomas, including an evaluation of 11 cases with pseudomyxoma peritonei. Am J Surg Pathol 2000; 24: Lee KR, Tavassoli FA, Prat J, et al. Surface epithelialstromal tumors, Tumors of the Ovary and Peritoneum. In: WHO Classification of Tumors, Pathology and Genetics, Tumors of the Breast and Female Genital Organs. Eds. Tavassoli, FA and Devilee, P. IARCPress Lyon, Washington, D.C., USA, 2003; pp Malpica A, Deavers MT, Lu K, et al. Grading ovarian serous carcinoma using a two-tier system. Am J Surg Pathol. 2004; 28: Malpica, et al. Inter-observer and intra-observer variability of a two-tier system for grading ovarian serous carcinoma. Am J Surg Pathol (in press). 5. Riopel MA, Ronnett BM, Kurman RJ. Evaluation of diagnostic criteria and behavior of ovarian intestinaltype mucinous tumors. Atypical proliferative (borderline) tumors and intraepithelial, microinvasive, invasive, and metastatic carcinomas. Am J Surg Pathol. 1999; 23: Robey SS, Silva EG, Gershenson DM, et al. Transitional cell carcinoma in high-grade high-stage ovarian carcinoma. Cancer. 1989; 63: Silva, EG, Robey-Cafferty, SS, Smith TL, Gershenson, DM. Ovarian carcinomas with transitional cell carcinoma pattern. Am J Clin Pathol. 1990; 93: Silva EG and Gershenson DM. Standardized histologic grading of epithelial ovarian cancer: Elusive after all presence of nucleoli and a mitotic index of up 12 mitoses per 10 high power fields) Endometrioid Carcinoma Based on the amount of solid component o Three grades Grade 1, up to 5% solid component (nonmorular) Grade 2, >5 to 50% solid component (nonmorular) Grade 3, more than 50% solid component (non-morular) Mucinous Carcinoma Based on the presence and type of invasion o Two types Non-invasive (intraglandular) Invasive Expansile Infiltrative Clear Cell Carcinoma High grade carcinoma Transitional Cell Carcinoma High grade carcinoma Undifferentiated Carcinoma High grade carcinoma

26 these years. (Editorial) Gynecologic Oncology. 1998; 70:1. 9. Singer G, Kurman RJ, Chang H-W, Cho SKR, Shih l-m. Diverse tumorigenic pathways in ovarian serous carcinoma. Am J Pathol. 2002; 160: Gilks CB. Subclassification of ovarian surface epithelial tumors based on correlation of histologic and molecular pathologic data. Int J Gynecol Pathol. 2004; 23: International Society of Gynecological Pathologists Symposium 2007 Grading of Ovarian Cancer Anaís Malpica, M.D. Department of Pathology Grading of Ovarian Cancer Introduction Traditionally ovarian cancer has been considered one disease Diverse grading systems have been used to grade these neoplasms regardless of the tumor histotype Grading of Ovarian Cancer The FIGO grading system Based on architectural features, grade of the tumor depends on the ratio of glandular or papillary structures to solid tumor Grade 1, < 5% solid Grade 2, 5% to 50% solid Grade 3, >50% solid Grading of Ovarian Cancer The WHO system Based on the pathologist s impression of both architectural and cytologic features Categories not defined according to a quantitative method Grading of Ovarian Cancer Ovarian carcinoma appears to be a heterogeneous group of tumors, rather than a single disease Therefore, a universal grading system for this heterogeneous group most likely would not accommodate the inherent differences among these diverse tumors



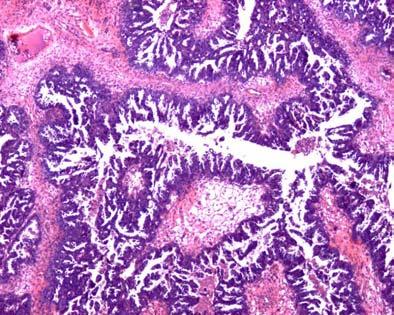
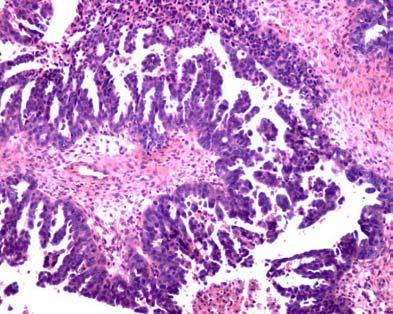
27 Grading of Ovarian Cancer Considering this heterogeneity, it would be more appropriate to use different parameters in order to grade the cases within each histologic type Grading of Ovarian Cancer Serous Carcinoma The recently proposed two-tier grading system (M.D. Anderson grading system) has emerged as a good method to segregate serous carcinomas that have different molecular, pathogenetic, histologic, immunohistochemical, and clinical features Serous Carcinoma The two-tier grading system (M.D. Anderson grading system) is based primarily on the assessment of nuclear atypia with the mitotic rate used as a secondary feature Two grades: Low High Low Grade Serous Carcinoma Definition A serous carcinoma characterized by the presence of uniform cells with mild to moderate nuclear atypia, and usually a low mitotic index ( 12 mitoses per 10 HPFs)





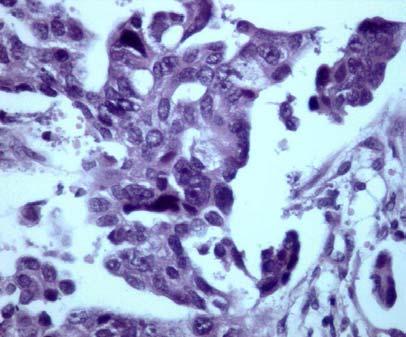
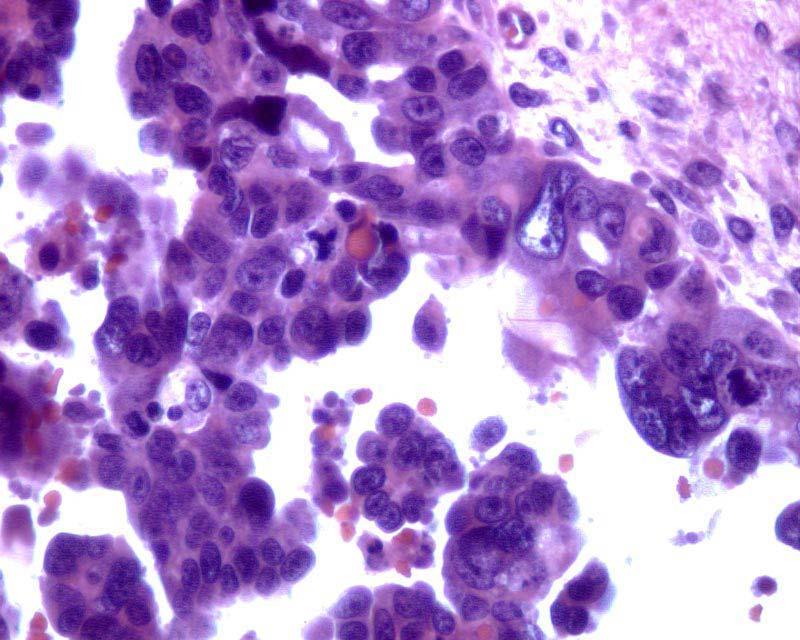
28 High Grade Serous Carcinoma Definition A serous carcinoma characterized by the presence of pleomorphic cells with marked nuclear atypia ( 3:1 variation in size and shape), and a high mitotic index (>12 mitoses per 10 HPFs)
29

 f/u Transformation to low grade serous carcinoma in 6.")
30 Low vs. High Grade Serous Carcinoma Differences in Pathogenesis: Morphologic Evidence Association with a serous neoplasm of low malignant potential 60% of the low grade serous carcinomas 2% of the high grade serous carcinomas Malpica A et al, 2004 Low vs. High Grade Serous Carcinoma Differences in Pathogenesis: Morphologic Evidence Association with serous tumor of low malignant potential 276 pts with serous LMP and long-term ( 5-year) f/u Transformation to low grade serous carcinoma in 6.8% of pts Interval range, 7 to 288 months (58% 60 months) Longacre TA et al, 2005 Low vs. High Grade Serous Carcinoma Differences in Pathogenesis: Molecular Evidence Ovarian Tumorigenesis Model Type I, tumors that arise in a stepwise manner from borderline (low malignant potential) tumors Low grade serous carcinoma, prototypic type I tumor BRAF and KRAS mutations Singer G et al, 2002 Low vs. High Grade Serous Carcinoma Differences in Pathogenesis: Molecular Evidence Ovarian Tumorigenesis Model Type II, de novo development (as yet no recognizable precursor lesion identified) High grade serous carcinoma, prototypic type II tumor p53 mutation Low vs. High Grade Serous Carcinoma: Immunohistochemical Differences Antibody p53 Bcl-2 MIB1, mean index Her-2 neu Low Grade Serous Ca 18% 5% 23.0% 4.5% High Grade Serous Ca 64% 26% 55.4% 36% Singer G et al, 2002 C-Kit 4.5% 30% O Neill CJ et al, 2005

31 Low vs. High Grade Serous Carcinoma: Differences in Biologic Behavior Low grade serous carcinoma appears to be less responsive to conventional chemotherapy than high grade serous carcinoma Patients with low grade serous carcinoma have a longer overall survival than patients with high grade serous carcinoma Gershenson DM, et al, 2006 Low vs. High Grade Serous Carcinoma: Frequently Asked Questions What is the incidence of low grade serous carcinoma? Uncommon tumor Less than 10% of ovarian serous carcinomas (MDACC unpublished data) 1/102 cases of advanced stage ovarian cancer (Gilks CB, 2004) Is the term low grade serous carcinoma used in a standard fashion? No Some gynecological pathologists use this term to designate the micropapillary/cribriform variant of a serous tumor of low malignant potential Low vs. High Grade Serous Carcinoma: Frequently Asked Questions What is the reproducibility of the two-tier grading system for ovarian serous carcinoma? Overall kappa among 9 different observers = The inter-observer kappas ranged from to in the first round of the review and from to in the second review Malpica A et al, in press 2007 Low vs. High Grade Serous Carcinoma: Frequently Asked Questions What is the reproducibility of the two-tier grading system for ovarian serous carcinoma? Eight of 9 participants had an intra-grader kappa ranging from to (excellent agreement) One participant had an intra-grader kappa of (good agreement) Malpica A et al, in press 2007 Endometrioid Carcinoma Endometrioid Carcinoma Grading system similar to the FIGO grading system used for endometrial endometrioid adenocarcinoma Grade 1 : less than 5% solid areas





32 Endometrioid Carcinoma Endometrioid Carcinoma Grade 2 : 5 to 50% solid areas Grade 3 : more than 50% solid areas Endometrioid Carcinoma Survival rate of patients with grade 1 or 2 tumors is higher than those with grade 3 tumors Clear Cell Carcinoma By definition a high grade carcinoma The WHO recommendation is not to grade Kline RC et al, 1990 Clear Cell Carcinoma Clear Cell Carcinoma A high incidence of stage I disease Poor response to platinum-based therapy Controversial results regarding the survival of patients with this type of tumor when compared to patients with serous carcinoma
 cases are high grade WHO criteria Low grade Uniformly enlarged nuclei, with mild alteration of the polarity and mild differences in shape, contour, and chromatin distribution Infrequent mitoses")
 Marked atypia of the")
33 Transitional Cell Carcinoma Transitional Cell Carcinoma The WHO recommendation is to grade according to the criteria used for transitional cell carcinoma of the urinary tract In reality, most (if not all) cases are high grade WHO criteria Low grade Uniformly enlarged nuclei, with mild alteration of the polarity and mild differences in shape, contour, and chromatin distribution Infrequent mitoses High grade Marked variation in nuclear polarity, size, shape, and chromatin distribution Frequent mitoses Transitional Cell Carcinoma Ovarian carcinomas with more than 50% of a TCC component appear to have a better response to chemotherapy Especially if the TCC component is also predominant in the metastases Mucinous Carcinoma Non-invasive carcinoma (Intraepithelial) Marked atypia of the epithelium Invasive carcinoma Expansile or confluent type Confluent glandular pattern uninterrupted by normal ovarian stroma occupying an area measuring more than 5 mm in diameter (The Johns Hopkins group criterion) or more than 10 mm 2 (WHO criterion) Infiltrative type Small glands, nest of cells or individual cells infiltrating the stroma in an area measuring more than 5 mm in diameter (The Johns Hopkins group criterion) or more than 10 mm 2 (WHO criterion)

 Infiltrative stromal invasion appears to")
 Undifferentiated Carcinoma Grading of Ovarian Cancer By")

 and mitotic index (secondary")
34 Mucinous Carcinoma Prognosis Intraepithelial mucinous carcinoma Risk of recurrence for stage I cases: 5.8% Invasive carcinoma 5-year survival of 91% for stage I cases; advanced stage cases all died of disease (Riopel MA et al, 1999) Infiltrative stromal invasion appears to be more aggressive than expansile invasion (Lee KR and Scully RE, 2000 and Rodriguez IM and Prat J, 2002) Undifferentiated Carcinoma Grading of Ovarian Cancer By definition a high grade carcinoma The 5-year survival of patients with undifferentiated carcinoma is worse than that of patients with serous carcinoma or transitional cell carcinoma Summary Serous Carcinoma Categories: High grade Low grade Criteria: Degree of cytologic atypia (primary feature) and mitotic index (secondary feature) Endometrioid Carcinoma Categories: Grades 1, 2, and 3 Criterion: amount of solid component
 Grading of Ovarian Cancer Summary Mucinous Carcinoma Criteria: Invasion Glandular crowding without intervening ovarian stroma")
35 Grading of Ovarian Cancer Summary Mucinous Carcinoma Categories: Non-invasive (intraepithelial) Invasive Expansile or confluent vs. infiltrative Criteria: Marked cytologic atypia (non-invasive carcinoma) Grading of Ovarian Cancer Summary Mucinous Carcinoma Criteria: Invasion Glandular crowding without intervening ovarian stroma in an area measuring more than 5 mm in diameter (confluent or expansile pattern) Small glands, clusters of cells or individual cells in the stroma in an area measuring more than 5 mm in diameter (infiltrative pattern) Grading of Ovarian Cancer Summary Transitional cell carcinoma Categories: Almost always high grade Criteria: WHO criteria for urothelial carcinoma High grade carcinomas (by definition) Clear cell carcinoma Undifferentiated carcinoma International Society of Gynecological Pathologists San Diego 2007 Key Issues Grading of Ovarian Cancer Dr. Patricia Shaw University Health Network University of Toronto Toronto, Canada Review of the three-tiered tiered grading system as developed by Dr. Silverberg and colleagues Does this system fulfill the criteria desired in a grading system? Clinical relevance Applicability to all major histological types Inter-observer reproducibility










36 An ideal grading system should be: Applicable to all histological types EOC Clinically relevant Reproducible - Intra- and inter-observer Easy to apply in clinical setting Widely adopted Dr. Silverberg and colleagues developed a 3-tiered system: Shimizu et al. Gynecologic Oncology 1998 Shimizu et al. Cancer 1998 Silverberg. International Journal of Gynecological Pathology 2000 Architectural Grade Glandular Papillary Solid Architectural Grade Papillary Solid Nuclear Grade Grade 1 Grade 2 Grade 3 Mitotic Count Score Score MF/10 HPF > 24
37 Architectural Grade and Survival Are these features clinically relevant? And to all major histological subtypes? Type Stage I-II Stage III-IV p-value p-value Serous Endometrioid 0.04 NS Mucinous NS Clear cell NS NS TCC -- NS All Shimizu Gynecol Oncol 1998 Nuclear Grade and Survival Mitotic Count Score and Survival Type Stage I-II Stage III-IV p-value p-value Serous Endometrioid NS Mucinous Clear cell NS TCC NS NS All Type Stage I-II Stage III-IV p-value p-value Serous Endometrioid NS Mucinous Clear cell NS NS TCC NS NS All NS Shimizu Gynecol Oncol 1998 Shimizu Gynecol Oncol 1998 Silverberg Grading System* Score Architecture Nuclear Grade Mitotic Activity (per 10 HPF) 1 Glandular Papillary Solid 3 >24 Is this grading system clinically relevant? And for all major histological subtypes? Total Score Silverberg Grade Shimizu Cancer 1998
38 Silverberg Grade and Survival Type Stage I-II Stage III-IV p-value p-value Serous Endometrioid NS Mucinous Clear cell NS NS TCC NS All Prognostic Factors: Stage I-II I II Ovarian Cancer (Multivariate) Significant: Silverberg grade (p=0.0001) Performance status (p=0.0004) Not significant: FIGO grade Age Histologic sub-type Shimizu Gynecol Oncol 1998 Prognostic Factors: Stage III-IV IV Ovarian Cancer (Multivariate) Significant: Silverberg grade Response to chemotherapy Post-surgical residual disease Performance status Histological subtypes - Mucinous/TCC Not Significant: FIGO grade Age Is this grading system reproducible? Shimizu et al Sato et al (Yes) Validation of Silverberg System by others: Mayr and Diebold 2000 Sato et al 2002 Shaw et al 2002 Gilks et al 2006 Histological Features of Hereditary Ovarian Carcinoma BRCA1/2 Control p-value GOG Grade % 8% 2 50% 51% 3 50% 41% Silverberg Grade % 2 25% 45% 3 75% 40% Shaw et al. Int J Gynecol Pathol 2002


39 Key Issues Histotyping ovarian cancers Robert A. Soslow, MD Review morphology, immunophenotype, genotype and differential diagnosis* Emphasize endometrioid and clear cell tumors Suggest refinements to diagnostic criteria Rationale for histotyping Distinct disease entities BRCA1 and 2 Tumor progression from: Endometriosis Borderline tumor Diagnostic criteria for carcinoma Carcinoma grading Therapeutic relevance WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction WHO critique WHO approach Morphologically based, but not entirely objective Problems Mucinous carcinoma Poorly differentiated endometrioid carcinoma Transitional cell carcinoma Mixed epithelial carcinoma Hendrickson MR, Longacre TA. Classification of surface epithelial neoplasms of the ovary Pathology (Phila). 1: , 1993
. 1:189-254, 1993 Serous carcinoma: morphology Hendrickson MR, Longacre TA.")
40 Hendrickson MR, Longacre TA. Classification of surface epithelial neoplasms of the ovary Pathology (Phila). 1: , 1993 Hendrickson MR, Longacre TA. Classification of surface epithelial neoplasms of the ovary Pathology (Phila). 1: , 1993 Serous carcinoma: morphology Hendrickson MR, Longacre TA. Classification of surface epithelial neoplasms of the ovary Pathology (Phila). 1: , 1993 Overview Problems Architecture Glandular Cribriform Microcystic Trabecular Cytology Clear cells Signet ring cells Spindle cells Serous carcinoma: immunophenotype All serous WT1 (>70%) Low-grade serous ER/PR High-grade serous P53 (overexpression, >70%) P16 Variable ER/PR Variable loss of BRCA1 Serous carcinoma: genotype Low grade serous BRAF mutation K-ras mutation High grade serous P53 mutation BRCA1 or 2 abnormalities (sporadic) BRCA1 or 2 mutation (familial) Singer G, et al. Am J Surg Pathol 29:218-24, 2005 Shaw PA, et al. Int J Gynecol Pathol 21:407-11, 2002








41 Familial Serous carcinoma: pathogenesis Inclusion cyst BRCA-1 mutation Dysplasia BRCA-1 abnl Sporadic BRAF K-ras Surface Epithelium Borderline tumor (BT) High grade serous carcinoma: pathogenesis TP53 mutation High grade carcinoma TP53 mutation Micropapillary BT Low grade carcinoma Singer G, et al. Am J Surg Pathol 29:218-24, 2005 Low grade serous carcinoma: pathogenesis Serous carcinoma: differential diagnosis Glandular, cribriform, microcystic, trabecular: Mucinous, endometrioid, clear cell, transitional Clear cells, signet ring cells: Clear cell, endometrioid, mucinous Ovarian carcinoma classification: serous Broad range of histologic features Slit-like spaces, irregular luminal contours Frequent WT1 Low-grade: serous borderline tumor, BRAF/K-ras, ER/PR High-grade: tubal intraepithelial carcinoma, p53, p16, loss of BRCA1, BRCA1 or 2 family Other entities are excluded Serous tumors: prevalence 80-85% of ovarian carcinomas 95% of stage III-IV ovarian carcinoma Low stage serous carcinomas are rare ~25% of stage I/II carcinomas are serous ~25% of stage I/II serous carcinomas are stage I Leitao MM, et al. Am J Surg Pathol 28:147-59, 2004 Seidman JD, et al. Int J Gynecol Pathol 23:41-4, 2004
 Negative racemase and -catenin (GI ddx)")

")
 Leitao MM, et al.")
42 (Intestinal) Mucinous tumors: morphology Overview Problems Primary versus metastasis Paucity of intracytoplasmic mucin/prevalence of extracellular mucin Borderline tumor versus carcinoma Mucinous tumors: immunophenotype Immunophenotype CK7>20 (GI ddx) Negative racemase and -catenin (GI ddx) Negative p16 (Endocervical ddx) Negative ER (Endometrioid ddx) Retained SMAD4/DPC4 (Pancreatic ddx) Negative mesothelin and fascin (Pancreatic ddx) Mucinous carcinoma: pathogenesis Mucinous carcinoma: pathogenesis Mucinous cystadenoma Intestinal mucinous BT K-ras Intestinal mucinous carcinoma Mucinous tumors: borderline versus carcinoma Expansile invasion Large cribriform glands Extensive gland fusion Complex papillary architecture Destructive invasion Am J Surg Pathol 23:617-35, 1999, 24: , 2000, 26:139-52, 2002, 22: , 1998 Low stage ovarian carcinomas (n=140) Diagnosis changed to borderline (30%) 70% were mucinous or endometrioid Mucinous tumors: differential diagnosis Exclude metastasis Scant intracytoplasmic mucin Endometrioid Extracellular mucin Pseudomyxoma peritonei Low grade serous carcinoma (cribriform) Leitao MM, et al. Am J Surg Pathol 28:147-59, 2004
43 Mucinous tumors: features favoring metastasis Bilateral disease Surface involvement Destructive stromal invasion Nodular growth pattern Single cells/signet ring cells Vascular invasion Am J Surg Pathol Mar; 27(3): Ovarian carcinoma classification: intestinal mucinous Intracytoplasmic mucin, expansile invasion Intestinal mucinous borderline tumor CK7>20, retained SMAD4 Negative racemase, -catenin, ER, p16, mesothelin, fascin K-ras Other entities are excluded: exclude metastasis Mucinous tumors: prevalence Only <3% of all ovarian carcinomas >2/3 are stage I ~15% of all stage I tumors Leitao MM, et al. Am J Surg Pathol 28:147-59, 2004 Seidman JD, et al. Am J Surg Pathol 27(7):985-93, 2003 Riopel MA, et al. Am J Surg Pathol 23(6):617-35, 1999 Seromucinous tumors Definition and synonyms Similarities with low grade serous tumors Architecture Clinical profile Differences with intestinal mucinous tumors Morphology Clinical profile Similarities with endometrioid tumors Endometriosis Endometrioid tumors: morphology Overview Problems Architecture: Cribriform Trabecular Papillary Cytology: Intracytoplasmic mucin Clear cells High nuclear grade Borderline tumor versus carcinoma Endometrioid tumors: immunophenotype ER/PR -catenin Not WT1 P53 in high grade examples
 Sporadic MSI PTEN")


 Diagnosis changed to borderline (30%) 70% were mucinous or")

 Low grade, stage I endometrioid carcinoma with")
44 Endometrioid tumors: genotype CTNNB-1 ( -catenin) PTEN Microsatellite instability (MSI) Familial Endometrioid carcinoma: pathogenesis Endometriosis (clonal) Sporadic MSI PTEN CTNNB1 Complex atypical hyperplasia/endometrioid BT?MSI?PTEN Low grade carcinoma Endometrioid carcinoma: pathogenesis Endometrioid carcinoma: pathogenesis Endometrioid tumors: borderline versus carcinoma Expansile invasion Large cribriform glands Extensive gland fusion Complex papillary architecture Destructive invasion Am J Surg Pathol 24: , 2000; Am J Surg Pathol 27:1253-9, 2003 Low stage ovarian carcinomas (n=140) Diagnosis changed to borderline (30%) 70% were mucinous or endometrioid (70%) Leitao MM, et al. Am J Surg Pathol 28:147-59, 2004 Endometrioid tumors: invasion patterns 13 grade 1 and 2 endometrioid carcinomas (8 IA, 5 IC); median F/U 81 mos: 9 expansile (9/9 NED) 4 expansile and destructive* (3/4 NED) Low grade, stage I endometrioid carcinoma with expansile invasion: VERY limited malignant potential Chen S, et al. Mod Pathol 18:903-11, 2005
45 Endometrioid tumors: differential diagnosis Cribriform, papillary, trabecular: Serous, transitional Intracytoplasmic mucin, clear cells, high nuclear grade: Metastasis, mucinous, clear cell, serous Ovarian carcinoma classification: endometrioid Endometrial-like, metaplasias, secretory change, expansile invasion Endometriosis, endometrioid borderline tumor, endometrioid uterine carcinoma ER/PR, -catenin; not WT1 CTNNB-1 ( -catenin), PTEN, MSI-H Other entities are excluded Endometrioid tumors: prevalence 10% of ovarian carcinomas Most common stage I carcinoma (~50%) Most endometrioid carcinomas are Stage I or II (>2/3) Leitao MM, et al. Am J Surg Pathol 28:147-59, 2004 Seidman JD, et al. Int J Gynecol Pathol 23:41-4, 2004 Clear cell tumors: morphology Overview Problems Architecture: Papillary Solid Cytology: Clear cytoplasm Oxyphilic variant Borderline tumor versus carcinoma Clear cell tumors: diagnostic reproducibility, immunophenotype, lessons learned Clear cell carcinomas have a limited and distinctive architectural repertoire and immunophenotype Mixed epithelial tumors containing clear cells (MET-C) are not reproducibly diagnosed MET-Cs are seldom clear cell carcinomas most are serous carcinomas Interobserver agreement Han G, et al. USCAP 2007, abstract Han G, et al. USCAP 2007, abstract




46 Clear cell immunophenotype WT1 ER BRCA1 CCC 10% 10% 100% SC 90% 90% 64% MET-C CC 90% 90% 60% Clear cell tumors: immunophenotype Immunophenotype Paucity of ER/PR Lack of WT1 Variable p53 expression Low proliferation rate MET-C SC 90% 90% 40% Han G, et al. USCAP 2007, abstract Clear cell tumors: genotype Mutations: PTEN TGF beta R2 K-RAS MSI-H Clear cell carcinoma: pathogenesis Endometriosis Atypical endometriosis or Endometrioid carcinoma (Clear cell borderline tumor) Clear cell carcinoma Clear cell carcinoma: pathogenesis Clear cell tumors: borderline versus carcinoma Adenofibromatous Destructive invasion greater than microinvasion: carcinoma What counts as invasion? Pure borderline tumors are almost never encountered Papillary Essentially always considered carcinoma Importance of cytologic characteristics Nuclear grade? Ddx with papillary endometrioid carcinoma and serous borderline tumor Sangoi AR, et al. USCAP 2007, abstract Asad H, Soslow RA, unpublished
International Society of Gynecological Pathologists Symposium 2007
 International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
International Society of Gynecological Pathologists Symposium 2007 Anais Malpica, M.D. Department of Pathology The University of Texas M.D. Anderson Cancer Center Grading of Ovarian Cancer Histologic grade
Molecular Pathology of Ovarian Carcinoma with Morphological Correlation
 Molecular athology of Ovarian Carcinoma with Morphological Correlation Kathleen R. Cho, M.D. Comprehensive Cancer Center and Departments of athology and Internal Medicine University of Michigan Medical
Molecular athology of Ovarian Carcinoma with Morphological Correlation Kathleen R. Cho, M.D. Comprehensive Cancer Center and Departments of athology and Internal Medicine University of Michigan Medical
Current Concept in Ovarian Carcinoma: Pathology Perspectives
 Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
Current Concept in Ovarian Carcinoma: Pathology Perspectives Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine Current Concept in Ovarian
Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor
 of the Ovary Arising in an Atypical Proliferative Serous Tumor") Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor Robert J Kurman, M.D. Johns Hopkins University School of Medicine Case History A 53 year
Case # 4 Low-Grade Serous Carcinoma (Macropapillary) of the Ovary Arising in an Atypical Proliferative Serous Tumor Robert J Kurman, M.D. Johns Hopkins University School of Medicine Case History A 53 year
Ovarian carcinoma classification. Robert A. Soslow, MD
 Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Ovarian carcinoma classification Robert A. Soslow, MD soslowr@mskcc.org WHO classification Serous Mucinous Endometrioid Clear cell Transitional Squamous Mixed epithelial Undifferentiated Introduction Rationale
Low-grade serous neoplasia. Robert A. Soslow, MD
 Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Low-grade serous neoplasia Robert A. Soslow, MD soslowr@mskcc.org Outline Orientation Ovarian tumor overview Non serous borderline tumors Serous borderline tumors Clinical summary Morphologic description
Bibliography. Serous Tumors of the Ovary. Nomenclature
 Bibliography Serous Tumors of the Ovary Nomenclature 1. Allison KH, Swisher EM, Kerkering KM, et al. Defining an appropriate threshold for the diagnosis of serous borderline tumor of the ovary: when is
Bibliography Serous Tumors of the Ovary Nomenclature 1. Allison KH, Swisher EM, Kerkering KM, et al. Defining an appropriate threshold for the diagnosis of serous borderline tumor of the ovary: when is
of 20 to 80 and subsequently declines [2].
![of 20 to 80 and subsequently declines [2].](/thumbs/80/81450506.jpg "of 20 to 80 and subsequently declines [2].") - - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
- - According to the 2014 World Health Organization (WHO) classification and tumor morphology, primary ovarian tumors are subdivided into three categories: epithelial (60%), germ cell (30%), and sex-cord
Borderline tumors. Borderline tumors. Serous borderline tumor are NOT benign. Low grade serous carcinoma: pathogenesis. Serous carcinoma: pathogenesis
 Serous borderline tumor are NOT benign Robert A. Soslow, MD Memorial Sloan-Kettering Cancer Center soslowr@mskcc.org Borderline tumors Serous BTs and seromucinous BTs are both histopathologically borderline
Serous borderline tumor are NOT benign Robert A. Soslow, MD Memorial Sloan-Kettering Cancer Center soslowr@mskcc.org Borderline tumors Serous BTs and seromucinous BTs are both histopathologically borderline
Clinical History USCAP Specialty Conference. Gynecologic Pathology Case 3
 2010 USCA Specialty Conference Gynecologic athology Case Kathleen R. Cho, M.D. Department of athology Clinical History 46 yo woman presented with bilateral ovarian masses and elevated CA-125 TAH/BSO, pelvic
2010 USCA Specialty Conference Gynecologic athology Case Kathleen R. Cho, M.D. Department of athology Clinical History 46 yo woman presented with bilateral ovarian masses and elevated CA-125 TAH/BSO, pelvic
Section 1. Biology of gynaecological cancers: our current understanding
 Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Section 1 Biology of gynaecological cancers: our current understanding Chapter 1 Morphological sub-types of ovarian carcinoma: new developments and pathogenesis W Glenn McCluggage 1 Introduction In most
Mucinous Tumors of the Ovary Beirut, Lebanon. Anaís Malpica, M.D. Professor Department of Pathology
 Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
Mucinous Tumors of the Ovary Beirut, Lebanon Anaís Malpica, M.D. Professor Department of Pathology Primary Mucinous Tumors of the Ovary Cystadenoma Borderline (Tumor of Low Malignant Potential/Atypical
Mody. AIS vs. Invasive Adenocarcinoma of the Cervix
 Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
Common Problems in Gynecologic Pathology Michael T. Deavers, M.D. Houston Methodist Hospital, Houston, Texas Common Problems in Gynecologic Pathology Adenocarcinoma in-situ (AIS) of the Cervix vs. Invasive
SEROUS TUMORS. Dr. Jaime Prat. Hospital de la Santa Creu i Sant Pau. Universitat Autònoma de Barcelona
 SEROUS TUMORS Dr. Jaime Prat Hospital de la Santa Creu i Sant Pau Universitat Autònoma de Barcelona Serous Borderline Tumors (SBTs) Somatic genetics Clonality studies have attempted to dilucidate whether
SEROUS TUMORS Dr. Jaime Prat Hospital de la Santa Creu i Sant Pau Universitat Autònoma de Barcelona Serous Borderline Tumors (SBTs) Somatic genetics Clonality studies have attempted to dilucidate whether
The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas. W Glenn McCluggage Belfast, Northern Ireland
 The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland Enterprise Interest None OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS
The Diagnostic Challenges of Low Grade and High Grade Tubo-Ovarian Serous Carcinomas W Glenn McCluggage Belfast, Northern Ireland Enterprise Interest None OVARIAN SEROUS CARCINOMA (OSC) RECENT DEVELOPMENTS
Low-Grade Serous Ovarian Tumors Debra A. Bell, MD Mayo Clinic and Mayo Medical School Rochester, MN
 1 Low-Grade Serous Ovarian Tumors Debra A. Bell, MD Mayo Clinic and Mayo Medical School Rochester, MN It is very appropriate to discuss low-grade ovarian serous neoplasms in a symposium in honor of Dr.
1 Low-Grade Serous Ovarian Tumors Debra A. Bell, MD Mayo Clinic and Mayo Medical School Rochester, MN It is very appropriate to discuss low-grade ovarian serous neoplasms in a symposium in honor of Dr.
Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center
 Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center Ovarian cancer is not a single disease Ovarian Epithelial Tumors: Histological Spectrum* Type Frequency Histology High-Grade
Ovarian cancer: 2012 Update Srini Prasad MD Univ Texas MD Anderson Cancer Center Ovarian cancer is not a single disease Ovarian Epithelial Tumors: Histological Spectrum* Type Frequency Histology High-Grade
Case presentation 04/13/2017. Genomic/morphological classification of endometrial carcinoma
 Genomic/morphological classification of endometrial carcinoma Robert A. Soslow, MD soslowr@mskcc.org architecture.about.com Case presentation 49 year old woman with vaginal bleeding Underwent endometrial
Genomic/morphological classification of endometrial carcinoma Robert A. Soslow, MD soslowr@mskcc.org architecture.about.com Case presentation 49 year old woman with vaginal bleeding Underwent endometrial
5/26/2016. Pelvic Serous Carcinoma: 2014 W.H.O. Update. Outline of Talk. Changes to 2014 WHO system for pelvic serous tumors
 Pelvic Serous Carcinoma: 2014 W.H.O. Update Outline of Talk Practical Implications for Pathologists Changes to 2014 WHO system for pelvic serous tumors High grade serous carcinoma versus low grade serous
Pelvic Serous Carcinoma: 2014 W.H.O. Update Outline of Talk Practical Implications for Pathologists Changes to 2014 WHO system for pelvic serous tumors High grade serous carcinoma versus low grade serous
Ovarian Clear Cell Carcinoma
 Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
Ovarian Clear Cell Carcinoma Rouba Ali-Fehmi, MD Professor of Pathology The Karmanos Cancer Institute, Wayne State University School of Medicine 50 year old woman with chief complaint of shortness of breath
The Origin of Pelvic Low-Grade Serous Proliferative Lesions
 The Origin of Pelvic Low-Grade Serous Proliferative Lesions Ovarian Atypical Proliferative (Borderline) Serous Tumors, Noninvasive Implants and Endosalpingiosis Robert J. Kurman, M.D. Kurman RJ, Vang R,
The Origin of Pelvic Low-Grade Serous Proliferative Lesions Ovarian Atypical Proliferative (Borderline) Serous Tumors, Noninvasive Implants and Endosalpingiosis Robert J. Kurman, M.D. Kurman RJ, Vang R,
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors (neoplasms) 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal
Interpretation of p53 Immunostains. P53 Mutations are Ubiquitous in High Grade Serous Carcinoma. Diffuse strong positive nuclear staining
 Stains for Tumor Classification p53 p16 WT1 HMGA2 P53 Mutations are Ubiquitous in High Grade Serous Carcinoma Source Ahmed et al Australian Ovarian Cancer Study Cancer Genome Atlas Research Network Cases
Stains for Tumor Classification p53 p16 WT1 HMGA2 P53 Mutations are Ubiquitous in High Grade Serous Carcinoma Source Ahmed et al Australian Ovarian Cancer Study Cancer Genome Atlas Research Network Cases
Case 1. Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno
 Luca Mazzucchelli Istituto cantonale di patologia Locarno") Case 1 Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno SAMO Interdisciplinary Workshop on Gynecological Tumors Lucern, October
Case 1 Pathology of gynecological cancer. What do we need to know (Case 1) Luca Mazzucchelli Istituto cantonale di patologia Locarno SAMO Interdisciplinary Workshop on Gynecological Tumors Lucern, October
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Low-grade appendiceal mucinous neoplasm (LAMN) High-grade appendiceal mucinous neoplasm (HAMN) Adenocarcinoma
Original contribution
 Human Pathology (2012) 43, 747 752 www.elsevier.com/locate/humpath Original contribution The presence and location of epithelial implants and implants with epithelial proliferation may predict a higher
Human Pathology (2012) 43, 747 752 www.elsevier.com/locate/humpath Original contribution The presence and location of epithelial implants and implants with epithelial proliferation may predict a higher
3/24/2017. Disclosure of Relevant Financial Relationships. Mixed Epithelial Endometrial Carcinoma. ISGyP Endometrial Cancer Project
 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME disclose any relevant financial relationship
Bases biológicas del cáncer de ovario en el siglo XXI
 Bases biológicas del cáncer de ovario en el siglo XXI Iñigo Espinosa, M.D. Clínica Universidad de Navarra Epithelial Ovarian Tumors WHO 1973-2014 Serous Mucinous Endometrioid Clear cell Transitional Squamous
Bases biológicas del cáncer de ovario en el siglo XXI Iñigo Espinosa, M.D. Clínica Universidad de Navarra Epithelial Ovarian Tumors WHO 1973-2014 Serous Mucinous Endometrioid Clear cell Transitional Squamous
Invited Re vie W. Molecular genetics of ovarian carcinomas. Histology and Histo pathology
 Histol Histopathol (1 999) 14: 269-277 http://www.ehu.es/histol-histopathol Histology and Histo pathology Invited Re vie W Molecular genetics of ovarian carcinomas J. Diebold Pathological Institute, Ludwig-Maximilians-University
Histol Histopathol (1 999) 14: 269-277 http://www.ehu.es/histol-histopathol Histology and Histo pathology Invited Re vie W Molecular genetics of ovarian carcinomas J. Diebold Pathological Institute, Ludwig-Maximilians-University
Patologia Molecular del Carcinoma de Ovario
 Curso de Patologia Molecular XXVI Congreso Nacional de la SEAP Cadiz Patologia Molecular del Carcinoma de Ovario Jaime Prat Barcelona Ovarian Epithelial Tumors WHO 1999 and 2003 Serous Mucinous Endometrioid
Curso de Patologia Molecular XXVI Congreso Nacional de la SEAP Cadiz Patologia Molecular del Carcinoma de Ovario Jaime Prat Barcelona Ovarian Epithelial Tumors WHO 1999 and 2003 Serous Mucinous Endometrioid
Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran
 ORIGINAL ARTICLE Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran Katayoun Ziari, Ebrahim Soleymani, and
ORIGINAL ARTICLE Survival Analysis and Prognosis for Patients with Serous and Mucinous Borderline Ovarian Tumors: 14-Year Experience from a Tertiary Center in Iran Katayoun Ziari, Ebrahim Soleymani, and
Atypical Hyperplasia/EIN
 EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
EIN Atypical Hyperplasia/EIN Based on scientific and diagnostic advances, in 2014 the WHO moved that the precursor lesion for endometrioid carcinoma be atypical hyperplasia/ein, rather than what was previously
Mousa. Najat kayed &Renad Al-Awamleh. Nizar Alkhlaifat
 6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
6 Mousa Najat kayed &Renad Al-Awamleh Nizar Alkhlaifat P a g e 1 This sheet written based on record 13 on website Cover slide( 95-117 ) No need to go back to slide FALLOPIAN TUBE PATHOLOGY In general fallopian
Serous Borderline Tumors of the Ovary: Implants, Manifestations, Biology & New Insights in Progression
 Serous Borderline Tumors of the Ovary: Implants, Manifestations, Biology & New Insights in Progression Stanley J. Robboy, MD Professor of Pathology Professor of Obstetrics & Gynecology Vice Chairman for
Serous Borderline Tumors of the Ovary: Implants, Manifestations, Biology & New Insights in Progression Stanley J. Robboy, MD Professor of Pathology Professor of Obstetrics & Gynecology Vice Chairman for
ACCME/Disclosures. Cribriform Lesions of the Prostate. Case
 Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
Cribriform Lesions of the Prostate Ming Zhou, MD, PhD Departments of Pathology and Urology New York University Langone Medical Center New York, NY Ming.Zhou@NYUMC.ORG ACCME/Disclosures The USCAP requires
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to
Molecular Subtyping of Endometrial Cancer: A ProMisE ing Change
 Molecular Subtyping of Endometrial Cancer: A ProMisE ing Change Charles Matthew Quick, M.D. Associate Professor of Pathology Director of Gynecologic Pathology University of Arkansas for Medical Sciences
Molecular Subtyping of Endometrial Cancer: A ProMisE ing Change Charles Matthew Quick, M.D. Associate Professor of Pathology Director of Gynecologic Pathology University of Arkansas for Medical Sciences
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden
 and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden") What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
What s (new) and Important in Reporting of Uterine Cancers Katherine Vroobel The Royal Marsden Maastricht Pathology 2018 Wednesday 20 th June Endometrioid adenocarcinoma High grade carcinomas (common)
3 cell types in the normal ovary
 Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal cells
Ovarian tumors 3 cell types in the normal ovary Surface (coelomic epithelium) the origin of the great majority of ovarian tumors 90% of malignant ovarian tumors Totipotent germ cells Sex cord-stromal cells
A Survay on Appendiceal Involvement in Ovarian Mucinous Tumors
 http://www.ijwhr.net Open Access doi 10.15296/ijwhr.2018.33 Original Article International Journal of Women s Health and Reproduction Sciences Vol. 6, No. 2, April 2018, 199 203 ISSN 2330-4456 A Survay
http://www.ijwhr.net Open Access doi 10.15296/ijwhr.2018.33 Original Article International Journal of Women s Health and Reproduction Sciences Vol. 6, No. 2, April 2018, 199 203 ISSN 2330-4456 A Survay
Objectives. Atypical Glandular Cells. Atypical Endocervical Cells. Reactive Endocervical Cells
 2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
2013 California Society of Pathologists 66 th Annual Meeting San Francisco, CA Atypical Glandular Cells to Early Invasive Adenocarcinoma: Cervical Cytology and Histology Christina S. Kong, MD Associate
JMSCR Vol 05 Issue 11 Page November 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.78 A Histomorphological Study of Carcinoma
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 71.58 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i11.78 A Histomorphological Study of Carcinoma
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS
 ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
ENODMETRIAL CARCINOMA: SPECIAL & NOT SO SPECIAL VARIANTS Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu Stanford University, Stanford,
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience
 Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Endometrial Metaplasia, Hyperplasia & Other Cancer Mimics: a Consultant s Experience Pacific Northwest Society of Pathologists Vancouver, B.C. September 26, 2015 Teri A. Longacre, M.D. longacre@stanford.edu
Important Recent Advances in Gynaecological Pathology
 Important Recent Advances in Gynaecological Pathology Sanjiv Manek Consultant Gynaecological Pathologist Oxford, UK In recent years there have been a significant number of changes in gynaecological pathology
Important Recent Advances in Gynaecological Pathology Sanjiv Manek Consultant Gynaecological Pathologist Oxford, UK In recent years there have been a significant number of changes in gynaecological pathology
ACCME/Disclosures. Risk of Gyne Ca in HBOC. Molecular basis of HBOC. Hereditary Ovarian and Breast Cancer Syndrome
 Hereditary Ovarian and Breast Cancer Syndrome C. Blake Gilks, MD Dept of Pathology Vancouver General Hospital University of British Columbia Blake.gilks@vch.ca The USCAP requires that anyone in a position
Hereditary Ovarian and Breast Cancer Syndrome C. Blake Gilks, MD Dept of Pathology Vancouver General Hospital University of British Columbia Blake.gilks@vch.ca The USCAP requires that anyone in a position
Clonal evolution of human cancers
 Clonal evolution of human cancers -Pathology-based microdissection and genetic analysis precisely demonstrates molecular evolution of neoplastic clones- Hiroaki Fujii, MD Ageo Medical Laboratories, Yashio
Clonal evolution of human cancers -Pathology-based microdissection and genetic analysis precisely demonstrates molecular evolution of neoplastic clones- Hiroaki Fujii, MD Ageo Medical Laboratories, Yashio
Gynecologic Cancers are many diseases. Speaker Disclosure: Gynecologic Cancer Care in the Age of Precision Medicine. Controversies in Women s Health
 Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Controversies in Women s Health Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Controversies in Women s Health Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Gestione dei tumori borderline iniziali e avanzati nelle donne in età fertile
 Gestione dei tumori borderline iniziali e avanzati nelle donne in età fertile Pierandrea De Iaco pierandrea.deiaco@aosp.bo.it SSD ONCOLOGIA GINECOLOGICA AOU SANT ORSOLA-MALPIGHI BOLOGNA Borderline ovarian
Gestione dei tumori borderline iniziali e avanzati nelle donne in età fertile Pierandrea De Iaco pierandrea.deiaco@aosp.bo.it SSD ONCOLOGIA GINECOLOGICA AOU SANT ORSOLA-MALPIGHI BOLOGNA Borderline ovarian
Histological Typing Of Cancer And Precancer Of The Oral Mucosa
 Histological Typing Of Cancer And Precancer Of The Oral Mucosa 1 / 7 2 / 7 3 / 7 Histological Typing Of Cancer And Within the last decade, histologic grading has become widely accepted as a powerful indicator
Histological Typing Of Cancer And Precancer Of The Oral Mucosa 1 / 7 2 / 7 3 / 7 Histological Typing Of Cancer And Within the last decade, histologic grading has become widely accepted as a powerful indicator
Stage IIIC transitional cell carcinoma and serous carcinoma of the ovary have similar outcomes when treated with platinum-based chemotherapy
 Original Investigation 33 Stage IIIC transitional cell carcinoma and serous carcinoma of the ovary have similar outcomes when treated with platinum-based chemotherapy Gökhan Boyraz, Derman Başaran, Mehmet
Original Investigation 33 Stage IIIC transitional cell carcinoma and serous carcinoma of the ovary have similar outcomes when treated with platinum-based chemotherapy Gökhan Boyraz, Derman Başaran, Mehmet
Gynecologic Cancers are many diseases. Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine. Speaker Disclosure:
 Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Gynecologic Cancer Care in the Age of Precision Medicine Gynecologic Cancers in the Age of Precision Medicine Advances in Internal Medicine Lee-may Chen, MD Department of Obstetrics, Gynecology & Reproductive
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens
 How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
How to Recognize Gynecologic Cancer Cells from Pelvic Washing and Ascetic Specimens Wenxin Zheng, M.D. Professor of Pathology and Gynecology University of Arizona zhengw@email.arizona.edu http://www.zheng.gynpath.medicine.arizona.edu/index.html
Select problems in cystic pancreatic lesions
 Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Disclosure Select problems in cystic pancreatic lesions Five Prime Therapeutics shareholder Adicet Bio shareholder Bristol-Meyer Squibb advisory board grace.kim@ucsf.edu Pancreatic cystic lesions Intraductal
Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance
 & 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
& 2006 USCAP, Inc All rights reserved 0893-3952/06 $30.00 www.modernpathology.org Intraductal carcinoma of the prostate on needle biopsy: histologic features and clinical significance Charles C Guo 1 and
Syllabus. Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix. Appendiceal tumors. Summary provided Complete presentation
 2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
2016 Current Issues in Surgical Pathology Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Syllabus Summary provided Complete presentation sanjay.kakar@ucsf.edu Sanjay Kakar, MD University
Case year old female presented with asymmetric enlargement of the left lobe of the thyroid
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 Diagnosis 2/21/2011 TGB
 Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
Case 4 22 year old female presented with asymmetric enlargement of the left lobe of the thyroid gland. No information available relative to a prior fine needle aspiration biopsy. A left lobectomy was performed.
64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus
 Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Case 6 64 YO lady THBSO for prolapse At gross : A 3 cm endometrial polyp in the fundus Numerous irregular, large glands with leaf-like pattern Large glands with broad-based papillary infolding into the
Dall istologia alla caratterizzazione biomolecolare
 Il carcinoma ovarico: approccio multidisciplinare e prospettive terapeutiche Dall istologia alla caratterizzazione biomolecolare Anna Pesci Ospedale SC Don Calabria, Negrar anna.pesci@sacrocuore.it Ovarian
Il carcinoma ovarico: approccio multidisciplinare e prospettive terapeutiche Dall istologia alla caratterizzazione biomolecolare Anna Pesci Ospedale SC Don Calabria, Negrar anna.pesci@sacrocuore.it Ovarian
Page # 1. Endometrium. Cellular Components. Anatomical Regions. Management of SIL Thomas C. Wright, Jr. Most common diseases:
 Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
Endometrium Pathology of the Endometrium Thomas C. Wright Columbia University, New York, NY Most common diseases: Abnormal uterine bleeding Inflammatory conditions Benign neoplasms Endometrial cancer Anatomical
MPH Quiz. 1. How many primaries are present based on this pathology report? 2. What rule is this based on?
 MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
MPH Quiz Case 1 Surgical Pathology from hysterectomy performed July 11, 2007 Final Diagnosis: Uterus, resection: Endometrioid adenocarcinoma, Grade 1 involving most of endometrium, myometrial invasion
Borderline Ovarian Tumours. Andreas Obermair Brisbane
 Borderline Ovarian Tumours Andreas Obermair Brisbane Definition First described in 1929 Cellular features of malignancy Cellular atypia Mitotic activity No stromal invasion An entity per se??? (or precursor
Borderline Ovarian Tumours Andreas Obermair Brisbane Definition First described in 1929 Cellular features of malignancy Cellular atypia Mitotic activity No stromal invasion An entity per se??? (or precursor
Case Report Ovarian Seromucinous Borderline Tumor and Clear Cell Carcinoma: An Unusual Combination
 Case Reports in Obstetrics and Gynecology Volume 2015, Article ID 690891, 5 pages http://dx.doi.org/10.1155/2015/690891 Case Report Ovarian Seromucinous Borderline Tumor and Clear Cell Carcinoma: An Unusual
Case Reports in Obstetrics and Gynecology Volume 2015, Article ID 690891, 5 pages http://dx.doi.org/10.1155/2015/690891 Case Report Ovarian Seromucinous Borderline Tumor and Clear Cell Carcinoma: An Unusual
05/07/2018. Types of challenges. Challenging cases in uterine pathology. Case 1 ` 65 year old female Post menopausal bleeding Uterine Polyp
 Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Types of challenges Challenging cases in uterine pathology Nafisa Wilkinson Gynaecological Pathologist UCLH London Lack of complete history often, NO clinical history at all! Cases from other centres often
Presenter: Yeh-Han Wang M.D.
 Korea-Taiwan-Japan Joint Meeting for Gynecological Pathology Mini-lecture Female Adnexal Tumor of Probable Wolffian Origin (FATWO) in Taiwan: A Small Case Series and Literature Review Presenter: Yeh-Han
Korea-Taiwan-Japan Joint Meeting for Gynecological Pathology Mini-lecture Female Adnexal Tumor of Probable Wolffian Origin (FATWO) in Taiwan: A Small Case Series and Literature Review Presenter: Yeh-Han
6/5/2010. Outline of Talk. Endometrial Alterations That Mimic Cancer & Vice Versa: Metaplastic / reactive changes. Problems in Biopsies/Curettages
 Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Outline of Talk Endometrial Alterations That Mimic Cancer & Vice Versa: Problems in Biopsies/Curettages Metaplastic / reactive changes Mucinous change Microglandular hyperplasia-like change Squamous metaplasia
Adenocarcinoma of Mullerian origin: review of pathogenesis, molecular biology, and emerging treatment paradigms
 Cobb et al. Gynecologic Oncology Research and Practice (2015) 2:1 DOI 10.1186/s40661-015-0008-z REVIEW Adenocarcinoma of Mullerian origin: review of pathogenesis, molecular biology, and emerging treatment
Cobb et al. Gynecologic Oncology Research and Practice (2015) 2:1 DOI 10.1186/s40661-015-0008-z REVIEW Adenocarcinoma of Mullerian origin: review of pathogenesis, molecular biology, and emerging treatment
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Biology Response Controversies and Advances
 Biology Response Controversies and Advances in BRCA related ovarian cancer Lessons learned and future directions Michael Friedlander The Prince of Wales Hospital and Royal Hospital for Women Sydney BREAST-CANCER
Biology Response Controversies and Advances in BRCA related ovarian cancer Lessons learned and future directions Michael Friedlander The Prince of Wales Hospital and Royal Hospital for Women Sydney BREAST-CANCER
David Nunns on behalf of the Gynae Guidelines Group Date:
 Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Borderline tumours of the ovary management and follow-up Author: Contact Name and Job Title Directorate & Speciality
Title of Guideline (must include the word Guideline (not protocol, policy, procedure etc) Borderline tumours of the ovary management and follow-up Author: Contact Name and Job Title Directorate & Speciality
Neoplasia 2018 Lecture 2. Dr Heyam Awad MD, FRCPath
 Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
Neoplasia 2018 Lecture 2 Dr Heyam Awad MD, FRCPath ILOS 1. List the differences between benign and malignant tumors. 2. Recognize the histological features of malignancy. 3. Define dysplasia and understand
CASE 4 21/07/2017. Ectopic Prostatic Tissue in Cervix. Female 31. LLETZ for borderline nuclear abnormalities
 Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Female 31 CASE 4 LLETZ for borderline nuclear abnormalities PSA Ectopic Prostatic Tissue in Cervix AJSP 2006;30;209-215 usually incidental microscopic finding usually in ectocervical stroma? developmental
Case Report Clinicopathologic study of endometrial dedifferentiated endometrioid adenocarcinoma: a case report
 Int J Clin Exp Pathol 2012;5(1):77-82 www.ijcep.com /ISSN: 1936-2625/IJCEP1111016 Case Report Clinicopathologic study of endometrial dedifferentiated endometrioid adenocarcinoma: a case report Yan Shen
Int J Clin Exp Pathol 2012;5(1):77-82 www.ijcep.com /ISSN: 1936-2625/IJCEP1111016 Case Report Clinicopathologic study of endometrial dedifferentiated endometrioid adenocarcinoma: a case report Yan Shen
Pathology of the female genital tract
 Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Pathology of the female genital tract Common illnesses of the female genital tract Before menarche Developmental anomalies Tumors (ovarial teratoma) Amenorrhea Fertile years PCOS, ovarian cysts Endometriosis
Pathobiology of ovarian carcinomas
 Chinese Journal of Cancer Review Mojgan Devouassoux-Shisheboran 1 and Catherine Genestie 2 Abstract Ovarian tumors comprise a heterogeneous group of lesions, displaying distinct tumor pathology and oncogenic
Chinese Journal of Cancer Review Mojgan Devouassoux-Shisheboran 1 and Catherine Genestie 2 Abstract Ovarian tumors comprise a heterogeneous group of lesions, displaying distinct tumor pathology and oncogenic
Epithelial Ovarian Cancer 8/2/2013. Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer?
 Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer? Ann E. Smith Sehdev, MD Director, Center for Gynecologic Pathology Cascade Pathology, Portland, Oregon Ann E. Smith Sehdev has no
Tu-be or Not Tu-be: Is the Fallopian Tube the Source of Ovarian Cancer? Ann E. Smith Sehdev, MD Director, Center for Gynecologic Pathology Cascade Pathology, Portland, Oregon Ann E. Smith Sehdev has no
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box?
 When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
When Immunostains Can Get You in Trouble: Gynecologic Pathology p16: Panacea or Pandora s Box? Teri A. Longacre, MD Stanford Medicine Stanford California pi6 in Gynecologic Pathology: Panacea or Pandora
Mucinous Adenocarcinoma Involving the Ovary: Comparative Evaluation of the Classification Algorithms using Tumor Size and Laterality
 J Korean Med Sci 2010; 25: 220-5 ISSN 1011-8934 DOI: 10.3346/jkms.2010.25.2.220 Mucinous Adenocarcinoma Involving the Ovary: Comparative Evaluation of the Classification Algorithms using Tumor Size and
J Korean Med Sci 2010; 25: 220-5 ISSN 1011-8934 DOI: 10.3346/jkms.2010.25.2.220 Mucinous Adenocarcinoma Involving the Ovary: Comparative Evaluation of the Classification Algorithms using Tumor Size and
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital
 Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Joseph Misdraji, M.D. GI pathology Unit Massachusetts General Hospital jmisdraji@partners.org Adenoma Low-grade appendiceal mucinous neoplasm High-grade appendiceal mucinous neoplasm Adenocarcinoma Serrated
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1)
") Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Prostate Pathology: Prostate Carcinoma, variants and Gleason Grading (Part 1) Jae Y. Ro, MD, PhD June 7, 2012 Ten Leading Cancer Types for the Estimated New Cancer Cases and Deaths By Sex, United States,
Endosalpingiosis. Case report
 Case report Endosalpingiosis Michael D. Holmes, M.D. Howard S. Levin M.D. Department of Pathology Lester A. Ballard, Jr., M.D. Department of Gynecology Endosalpingiosis, a term referring to tuballike epithelium
Case report Endosalpingiosis Michael D. Holmes, M.D. Howard S. Levin M.D. Department of Pathology Lester A. Ballard, Jr., M.D. Department of Gynecology Endosalpingiosis, a term referring to tuballike epithelium
Diagnostically Challenging Cases in Gynecologic Pathology
 Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Diagnostically Challenging Cases in Gynecologic Pathology Eric C. Huang, M.D., Ph.D. Department of Pathology and Laboratory Medicine University of California, Davis Medical Center Case 1 Presentation 38
Neoplasias Quisticas del Páncreas
 SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
SEAP -Aproximación Práctica a la Patología Gastrointestinal- Madrid, 26 de mayo, 2006 Neoplasias Quisticas del Páncreas Gregory Y. Lauwers, M.D. Director, Service Massachusetts General Hospital Harvard
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis
 In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
In situ and Invasive Endocervical Carcinoma: Problems and Pitfalls in Diagnosis Rouba Ali-Fehmi,MD The Karmanos Cancer Institute, Wayne State University School of Medicine Global incidence of cervical
Borderline Ovarian Mucinous Tumors: Consensus Points and Persistent Controversies Regarding Nomenclature, Diagnostic Criteria, and Behavior
 Borderline Ovarian Mucinous Tumors: Consensus Points and Persistent Controversies Regarding Nomenclature, Diagnostic Criteria, and Behavior Brigitte M. Ronnett, M.D.; C. Blake Gilks, M.D., Maria J. Merino,
Borderline Ovarian Mucinous Tumors: Consensus Points and Persistent Controversies Regarding Nomenclature, Diagnostic Criteria, and Behavior Brigitte M. Ronnett, M.D.; C. Blake Gilks, M.D., Maria J. Merino,
Primary Mucinous Ovarian Cancer (PMOC) Michael Frumovitz
 Michael Frumovitz") Primary Mucinous Ovarian Cancer (PMOC) Michael Frumovitz Epithelial Subtypes Serous Endometrioid Mucinous Transitional Clear Cell Mixed Undifferentiated Squamous Ovarian Surface Epithelium Naora et al.,
Primary Mucinous Ovarian Cancer (PMOC) Michael Frumovitz Epithelial Subtypes Serous Endometrioid Mucinous Transitional Clear Cell Mixed Undifferentiated Squamous Ovarian Surface Epithelium Naora et al.,
Gynecologic Cytopathology: Glandular lesions
 Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Gynecologic Cytopathology: Glandular lesions Lin Wai Fung (MSc, MPH, CMIAC) 17/4/2014 Glandular lesions of the uterus Endocervix Endometrium Normal endocervical cells Sheets, strips well-preserved architecture:
Prof. Dr. Aydın ÖZSARAN
 Prof. Dr. Aydın ÖZSARAN Adenocarcinomas of the endometrium Most common gynecologic malignancy in developed countries Second most common in developing countries. Adenocarcinomas, grade 1 and 2 endometrioid
Prof. Dr. Aydın ÖZSARAN Adenocarcinomas of the endometrium Most common gynecologic malignancy in developed countries Second most common in developing countries. Adenocarcinomas, grade 1 and 2 endometrioid
Background. Background. Background. Background 2/2/2015. Endometriosis-Associated Ovarian Cancer: Malignant Transformation of Endometriosis
 Endometriosis-Associated Ovarian Cancer: Malignant Transformation of Endometriosis I have no disclosures. Marcela G. del Carmen, MD, MPH Associate Professor Division of Gynecologic Oncology EOC is gynecologic
Endometriosis-Associated Ovarian Cancer: Malignant Transformation of Endometriosis I have no disclosures. Marcela G. del Carmen, MD, MPH Associate Professor Division of Gynecologic Oncology EOC is gynecologic
KRAS: ONE ACTOR, MANY POTENTIAL ROLES IN DIAGNOSIS
 UNIVERSITÀ DEGLI STUDI DI PALERMO Scuola di Specializzazione in Biochimica Clinica Direttore Prof. Marcello Ciaccio KRAS: ONE ACTOR, MANY POTENTIAL ROLES IN DIAGNOSIS Loredana Bruno KRAS gene Proto-oncogene
UNIVERSITÀ DEGLI STUDI DI PALERMO Scuola di Specializzazione in Biochimica Clinica Direttore Prof. Marcello Ciaccio KRAS: ONE ACTOR, MANY POTENTIAL ROLES IN DIAGNOSIS Loredana Bruno KRAS gene Proto-oncogene
ACCME/Disclosures. Case History 4/13/2016. USCAP GU Specialty Conference Case 3. Ann Arbor, MI
 USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
USCAP GU Specialty Conference Case 3 March 2016 L. Priya Kunju, M.D. University of Michigan Health System Ann Arbor, MI University of Michigan Health System ACCME/Disclosures The USCAP requires that anyone
GOBLET CELL CARCINOID. Hanlin L. Wang, MD, PhD University of California Los Angeles
 GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
GOBLET CELL CARCINOID Hanlin L. Wang, MD, PhD University of California Los Angeles hanlinwang@mednet.ucla.edu Goblet cell carcinoid (GCC) is a unique type of mixed endocrine-exocrine neoplasm, almost exclusively
Published Ahead of Print on September 28, 2012 as /theoncologist
 The Oncologist Gynecologic Oncology Diagnosis, Treatment, and Follow-Up of Borderline Ovarian Tumors DANIELA FISCHEROVA, a MICHAL ZIKAN, a PAVEL DUNDR, b DAVID CIBULA a a Gynecological Oncology Center,
The Oncologist Gynecologic Oncology Diagnosis, Treatment, and Follow-Up of Borderline Ovarian Tumors DANIELA FISCHEROVA, a MICHAL ZIKAN, a PAVEL DUNDR, b DAVID CIBULA a a Gynecological Oncology Center,
USCAP 2013: THE ORIGINS OF OVARIAN CANCER: MUCINOUS TUMORS
 USCAP 2013: THE ORIGINS OF OVARIAN CANCER: MUCINOUS TUMORS Russell Vang, M.D. Associate Professor Division of Gynecologic Pathology The Johns Hopkins Hospital Table of contents: Powerpoint handout Text
USCAP 2013: THE ORIGINS OF OVARIAN CANCER: MUCINOUS TUMORS Russell Vang, M.D. Associate Professor Division of Gynecologic Pathology The Johns Hopkins Hospital Table of contents: Powerpoint handout Text
Ovarian serous tumors of low malignant potential
 ORIGINAL ARTICLE Lymph Node Involvement in Ovarian Serous Tumors of Low Malignant Potential (Borderline Tumors) Pathology, Prognosis, and Proposed Classification Jesse K. McKenney, MD, Bonnie L. Balzer,
ORIGINAL ARTICLE Lymph Node Involvement in Ovarian Serous Tumors of Low Malignant Potential (Borderline Tumors) Pathology, Prognosis, and Proposed Classification Jesse K. McKenney, MD, Bonnie L. Balzer,
Institute of Pathology First Faculty of Medicine Charles University. Ovary
 Ovary Barrett esophagus ph in vagina between 3.8 and 4.5 ph of stomach varies from 1-2 (hydrochloric acid) up to 4-5 BE probably results from upward migration of columnar cells from gastroesophageal junction
Ovary Barrett esophagus ph in vagina between 3.8 and 4.5 ph of stomach varies from 1-2 (hydrochloric acid) up to 4-5 BE probably results from upward migration of columnar cells from gastroesophageal junction
Gynecologic Malignancies. Kristen D Starbuck 4/20/18
 Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial
Gynecologic Malignancies Kristen D Starbuck 4/20/18 Outline Female Cancer Statistics Uterine Cancer Adnexal Cancer Cervical Cancer Vulvar Cancer Uterine Cancer Endometrial Cancer Uterine Sarcoma Endometrial