PD-L1 Expression, Role, and Significance in Lung Pathology. Ross A Miller, MD FACP FASCP
|
|
|
- Emily Fletcher
- 5 years ago
- Views:
Transcription

1 PD-L1 Expression, Role, and Significance in Lung Pathology Ross A Miller, MD FACP FASCP
2 Background information
 for PD-L1 Near ubiquitous expression in human tissues, with some exceptions PD-L1 expression on cells is induced by proinflammatory states Most notable inducer of PD-L1")
3 PD-1 and PD-L1 expression in tissues PD-L1 Ligand to PD-1 (PD-1 on T cells) Rarely expressed during physiologically normal states Also known as CD274 Encoded by the CD274 gene on chromosome 9 Messenger RNA (mrna) for PD-L1 Near ubiquitous expression in human tissues, with some exceptions PD-L1 expression on cells is induced by proinflammatory states Most notable inducer of PD-L1 expression: interferon gamma (IFN- γ) produced by activated T-cells PD-1: expressed on T cells, binds to its ligand (PD-L1) PD-1 expression on Helper CD4+ T cells and CD8+ T lymphs Tonsil crypt epithelium When PD-1 (expressed on T-cells), binds to its ligand (PD-L1) the immune response is dampened (anergic) T-cell proliferation and cytokine production decreases


4 T-cells Activated T-cells PD-L1 Antigen IFN- γ, and other cytokines PD-1 PD-L1 Cell Death!!! Decreased immune response Cell survival Cell lacking PD-L1 Physiologic goal: prevent overactivation of the immune system and excessive tissue destruction

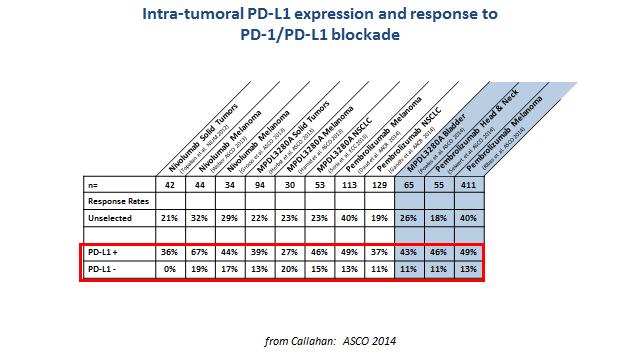
5 Exploitation of the PD-1/PD-L1 pathway Malignant cells can take advantage of the PD-1/PD-L1 Express PD-L1 on their cell surface PD-L1 expression in malignancies often associated with a poor outcome PD-1 Malignant cell Decreased immune response Cell survival

6
7 How does PD-L1 become expressed in Tumor cells???
8 Expression of PD-L1 in tumor cells Inducible PD-L1 expression Pro-inflammatory microenvironment Proposed mechanisms for PD-L1 expression seen in tumors with tumor infiltrating lymphocytes Molecular alterations Independent of inflammatory states So called noninducible or innate expression Examples: loss of PTEN Associated with PD-L1 expression

9 Expression of PD-L1 in tumor cells Regardless of the underlying mechanism (inducible or non-inducible) Malignant cells over expressing PD-L1 seemingly have a propensity to escape the immune system Cell survival and Propagation This process is sometimes referred to as adaptive resistance and this is the basis behind therapy targeting the PD-1/PD-L1 pathway


10 Basis of PD-1/PD-L1 therapy Ab blocking the PD-1/PD- L1 interaction Cell Death!!! However.it is not that simple.

11 T Cell Immune modulation Pardoll DM Nature Rev Cancer 12, 252, 2012
12 Immune modulation Immune system Continuous state of balance Recognizing self Attacking non-self Disruption Autoimmune or immune deficiency states In the normal state Immune checkpoints Activate the immune response Inhibitory feed back to prevent over activation
13 T Cell Immune modulation T cell activation: 2 step process 1 st step: APCs presenting antigens via MHC CD4 + T-cells recognize antigens from MHC class II Helper T cells Th1 (enhance cytotoxic T-cells, Th2 (B cell response), Th17 (autoimmunity and tissue regulation), Treg (suppression of immunity) CD8 + T-cells recognize antigens from MHC class I Cytotoxic T- cell Th1 cells, when activated produce: IL-2 TNF-alpha IFN- γ : Most notable inducer of PD-L1 expression 2nd step: activation of B7/CD28 family of receptors B7/CD28 family of receptors Stimulatory B7-1, B7-2 Some are inhibitory PD-1, PD-L1, DP-L2, CD80, CTLA-4 Pardoll DM Nature Rev Cancer 12, 252, 2012

14 Hiding from the immune system How do cancer cells survive in the immune competent individual? Tumor derived Tregs tend to have higher suppressive activity than Tregs in normally physiologic states Cytotoxic T lymphs have difficulty recognizing Ag on cancer cells via impaired MHC1 pathway mechanisms Cancer cells/the tumor microenvironment tends to produce immunosuppressive cytokines Stimulatory molecules tend to be down regulated Suppressive molecules tend to be up regulated

15 Potential for treatment How do cancer cells survive in the immune competent individual? Tumor derived Tregs tend to have higher suppressive activity than Tregs in normally physiologic states Cytotoxic T lymphs have difficulty recognizing Ag on cancer cells via impaired MHC1 pathway mechanisms Cancer cells/the tumor microenvironment tends to produce immunosuppressive cytokines Stimulatory molecules tend to be down regulated Suppressive molecules tend to be up regulated We could get the patients own immune cells act on the malignant cells Treating the cancer without the harsh side effects of traditional chemotherapy AND If we could stimulate the immune system to recognize malignant cells..
16 Immune modulation Cytokines and immunotherapy IL-2 (produced by activated Th1 cells) Primarily stimulates T cell proliferation discovered by Morgan in 1976 One of the first attempted immunotherapies: IL-2 administered exogenously Expected to result in tumor regression Effective in murine models Some response noted with high-dose therapies (1985): Renal cell carcinomas (14% RR), Melanoma(16% RR) Major toxicity! IL-2 INF-γ and TNF-α capillary leak syndrome and decreased systemic vascular resistance IFN-alpha and imiquimod therapy Limited effectiveness... Some benefit in a limited number of cancers
 Slightly longer progression-free survival Chemo only: 4.6 months Chemo plus phased ipilimumab: 5.")
17 CTLA-4 therapy Anti-CTLA-4: first immune checkpoint inhibitor approved by the FDA (2011) Blocking CTLA-4 prevents downregulation in early stages of T- cell activation 20% of melanoma patients better long term survival Studies in NSCLC (Phase II trail) Slightly longer progression-free survival Chemo only: 4.6 months Chemo plus phased ipilimumab: 5.7 months Tended to be longer in squamous NSCLC (now in Phase III trials) Chemo plus concurrent ipilimumab: 5.5 months Side effects! Rash, colitis, thyroiditis, hepatitis, other auto-immune like reactions
18 Additional stimulatory agents not shown on diagram 4-1BB: Utomilumab (Phase I) and Urelumab (Phase I-II) GITR: MK-4166 (Phase I) Potentials for treatment NSCLC Inhibitory agents PD-L1 inhibitory agents Atezolizumab: approved by FDA Durvalumab: Phase III trial complete Avelumab: Phase III PD-1 inhibitory agents Nivolumab: approved by FDA Pembrolizumab: approved by FDA Pidilizumab: Phase I-II PDR001 Phase I-II Inhibitory agents CTLA-4 inhibitory agents Ipilimumab: Phase III trails Tremelumumab: Phase III trials Inhibitory agent KIR inhibitory agent Lirilumab: Phase I-II Inhibitory agent LAG3 inhibitory agent LAG525: Phase I-II Stimulatory agents OX40 Stimulatory agents MEDI0562: Phase I MEDI6353: Phase I MOXR0916: Phase I
19 PD-1/PD-L1 therapy PD-1 inhibitory agents Nivolumab: approved by FDA Pembrolizumab: approved by FDA Pidilizumab: Phase I-II PDR001 Phase I-II Nivolumab Initial FDA approval was for melanoma Currently, Nivolumab plus ipilimumab is first line therapy, regardless of BRAF V600E mutation status Various studies showed efficacy in NSCLC Some studies showed better responses with increasing PD-L1 expression, some responses were independent of PD-L1 expression FDA approved for the management of advanced NSCLC (and advanced RCC / classical Hodgkin lymphoma Small cell lung cancer Shown effective, PD-L1 expression was not associated with responses in the Checkmate 032 study
20 PD-1/PD-L1 therapy Pembrolizumab Shown active in a variety of solid tumors Melanoma, MMT deficient colorectal cancer, NSCLC, head and neck squamous cell carcinoma Again, numerous studies have showed efficacy in NSCLC Many of these studies were on patients with some PD-L1 expression or showed greater responses with higher levels of PD-L1 expression Small cell carcinoma Phase Ib trials have shown responses in PD-L1 previously treated patients
21 PD-1/PD-L1 therapy PD-L1 inhibitory agents Block PD-1/PD-L1 interactions leaving the PD-1/PD-L2 pathway intact Atezolizumab: approved by FDA Durvalumab: Phase III Avelumab: Phase III Atezolizumab FDA approved for advanced urothelial carcinoma ImVigor 210 trial: slightly better responses with PD-L1 expressin greater than 5% Various studies show efficacy in NSCLC (POPLAR, BIRCH, OAK trials) FDA approved for second-line therapy of NSCLC
22 Side effects of PD-1/PD-L1 therapy Common Fatigue, cough, shortness of breath, nausea, itching, rash, vitiligo, decreased appetite, headache, constipation, joint pain, back pain, diarrhea Others: anemia, cellulitis, lymphocytopenia, sepsis, SJS-TEN, high blood sugar, rhabdomyolysis, others Patients can have immune mediated reactions Pneumonitis, colitis, hepatitis, endocrinopathies, nephritis, skin reacions

23
24 Rational for PD-L1 assessment
25 Conceptually Tumors devoid of PD-L1 Use of PD-1/PD-L1 blockade would be irrelevant as use of blocking agents could not block the pathway. IHC was used to look for PD-L1 + tumors to select patients for blocking agents
26 PD-L1 Immunohistochemistry as a Predictive Biomarker MPDL3280A: Atezolizumab
27 N Engl J Med. 2015;372(21): Keynote-001 Phase 1 study PD-L1 clone: 22C3 (Dako) and using the IHC kit protocol PS: Proportion Score (% of tumor cells staining for PD-L1) ORR: Objective response rate: FDA definition (the proportion of patients with tumor size reduction of a predefined amount and for a minimum time period)
28 PD-L1 clone: 22C3 (Dako) and using the IHC kit protocol
29 Phase II/III: Previously treated advanced stage NSCLC Among patients with at least 50% of tumor cells expressing PD-L1, overall survival was significantly longer with pembrolizumab with docetaxel (median 14 9 months vs 8 2 months; HR 0 54, 95% CI ; p=0 0002) KEYNOTE-024 Reck M et al. N Engl J Med. 2016;375(19): Phase III: 305 patients with previously untreated advanced NSCLC with PD-L1 expression in at least 50% of tumor cells No sensitizing EGFR mutations or ALK translocations Conclusions: pembrolizumab was associated with significantly longer progression-free and overall survival and with fewer adverse events than was platinum-based chemotherapy PD-L1 antibody clone: 22C3 (Merck)
30 October 24 th, 2016 Pembrolizumab became the 1 st immunotherapy drug approved for first line treatment of metastatic NSCLC whose tumor over express PD-L1 (TPS greater than or equal to 50%) Second line with lower levels of PD-L1 expression
31 Nivolumab CheckMate 017 and 057 trials Second-line nivolumab was superior to docetaxel in two subsequent randomized phase III trials of patients with advanced NSCLC who previously received a platinumbased chemotherapy doublet - FDA approval for second line therapy Trails as first line therapy (Nivolumab as a single agent) CheckMate 012: looked at safety and efficacy: 71% had adverse reactions, ORR: 23% CheckMate 026: PD-L1 expression of 5% or greater: the progression-free survival and ORR was longer for the chemotherapy arm but overall survival was better for the nivolumab arm
32 Phase 3 trial comparing nivolumab monotherapy to docetaxel monotherapy in patients with advanced squamous-cell NSCLC in those who had disease progression during or after one prior platinum-containing chemotherapy regimen Patients with stage IIIB or IV Kaplan-Meier curves for progression free survival Time from randomization to the date of first documented tumor progression, death, or last tumor assessment
33 CheckMate 026 ORR Progression free survival Overall Survival Overall Survival at 1 year Nivolumab (months) 14.4 (months) 56.3 Platinum Doublet (months) 13.2 (months) 53.6
34 Bottom line Pembrolizumab was approved for first line therapy (PD-L1 expression greater than 50%) Nivolumab indication: second line therapy Many feel the PD-L1 expression level was set to low in Phase III trial for Nivolumab The goal of a biomarker: Enrich the patient population of who will benefit (select the people most likely to respond) Avoid harm to patients (toxicity) These new drugs are $$$ PD-L1 cutoff for Nivolumab At the time of the study: include as many patients as possible
35 Predictive significance of PD-L1 IHC with nivolumab Checkmate 017: trend toward improved overall survival and overall response rate for patients with PD-L1 expression of 1% or greater Checkmate 057: greater efficacy than docetaxel in subgroups: tumor-membrane expression of PD-L1 (1% or greater, 5% or greater, and 10% or greater) The median overall survival for patients in these subgroups treated with nivolumab was 17.1, 18.2, and 19.4 months, respectively, compared to 9.0, 8.1, and 8.0 months, respectively, with docetaxel Borghaei, NEJM 2015
36 Some of the immunohistochemistry antibody clones and assays for PD-L1 evaluation Drug Antibody Clone Criteria Pembrolizumab PD-1 inhibitory agent Nivolumab PD-1 inhibitory agent 22C3 (Dako) Companion diagnostic (FDA approval) 1st line: PD-L1 at least 50% 2nd Line: PD-L1, 1% or greater 28-8 (Dako) Complementary (FDA approval) 2 nd line: PD-L1 1% or greater Atezolizumab PD-L1 inhibitory agent SP142 (Ventana) Complementary (FDA approval) 2 nd line NSCLC: 50% in tumor cells, or at least 10% in immune cells Durvalumab PD-L1 inhibitory agent SP263 (Ventana) Complementary (FDA Approval) Greater than or equal to 25% Avelumab PD-L1 inhibitory agent (Dako) Greater than or equal to 1% PD-L1 E1L3N: PD-L1 IHC clone: Cell Signaling Technology (Non-FDA approved) ***Laboratory Developed tests (LDTs)*** companion diagnostic: defined as a diagnostic assay required for the use of the associated drug based on clinical efficacy and safety data complementary diagnostic: defined as a diagnostic assay that predicts a favorable outcome of the associated drug by selecting patients based on results of the assay. However, it is not harmful to treat patients with the associated drug in the absence of assay results or if the results are negative. In other words, use of the complementary assay is not required for treatment with the associated drug

37
38 Challenges and Caveats
39 PD-L1 as a biomarker Is not binary... Information presented by Dr. K Kerr at 2017 PPS meeting Used with permission
40

41 Presented by Dr. K Kerr at 2017 PPS meeting Used with permission
42 Things to keep in mind Absent PD-L1 staining does not mean the patient will not respond Various studies show around 10% of patients with negative PD-L1 tumor staining showed response to PD-(L)1 inhibitors Positive PD-L1 expression does not mean the patients will respond to therapy Up to 60% of patients with PD-L1 expression did not respond to therapy Numbers based on studies from: Borghaei et al, NEJM 2015; Rittmeyer A, et al, Lancet 2017; Brahmer J et al, NEJM 2015; Reck M et al, Lancet 2016; Garassino M et al, JTO WCLC 2016; Herbst RS et al, Lancet 2016 PD-L1 expression is tumors is heterogeneous Is our sample representative of the entire tumor? Small clusters of tumor cells on small bx or cell block Resection specimen
 30, 530 538.")

43 Things to keep in mind PD-L1 expression is tumors is heterogeneous Is our sample representative of the entire tumor? Resection specimen Modern Pathology (2017) 30, Immunohistochemical staining for PD-L1 in tissue microarray cores from a series of 79 squamous cell lung cancers and 71 pulmonary adenocarcinomas Substantial inconsistencies for the percentages of cells staining positive for PD-L1 among different tissue microarray cores
44 Some of the immunohistochemistry antibody clones and assays for PD-L1 evaluation Drug Antibody Clone Criteria Pembrolizumab PD-1 inhibitory agent Nivolumab PD-1 inhibitory agent 22C3 (Dako) Companion diagnostic (FDA approval) 1st line: PD-L1 at least 50% 2nd Line: PD-L1, 1% or greater 28-8 (Dako) Complementary (FDA approval) 2 nd line: PD-L1 1% or greater Atezolizumab PD-L1 inhibitory agent SP142 (Ventana) Complementary (FDA approval) 2 nd line NSCLC: 50% in tumor cells, or at least 10% in immune cells Durvalumab PD-L1 inhibitory agent SP263 (Ventana) Greater than or equal to 25% Avelumab PD-L1 inhibitory agent (Dako) Greater than or equal to 1% PD-L1 E1L3N: PD-L1 IHC clone: Cell Signaling Technology (Non-FDA approved) ***Laboratory Developed tests (LDTs)*** companion diagnostic: defined as a diagnostic assay required for the use of the associated drug based on clinical efficacy and safety data complementary diagnostic: defined as a diagnostic assay that predicts a favorable outcome of the associated drug by selecting patients based on results of the assay. However, it is not harmful to treat patients with the associated drug in the absence of assay results or if the results are negative. In other words, use of the complementary assay is not required for treatment with the associated drug
45 Solutions? LDTs and Off-label Screen with LDTs before send-out Select one test based on local oncologists preference Universally accepted, standardized criteria for IHC testing of PD-L1 European approach
46 The French National cancer Institute National validation study of PD-L1 expression using different antibodies and platforms in solid and hematological tumors Not all antibodies and platforms are readily available Provide national guidelines and recommendations regarding antibodies, protocols and scoring systems These studies can only report on technical equivalence there is no guarantee that the same predictive performance will be delivered by an LDT
47 Proposal for Companion Diagnostic Comparability Clearly using each of the companion diagnostics to select one of the several available targeted therapies in the same class is not practical and may be impossible Likewise, having a single test or assay as a sole companion test for all of the multiple therapeutic options within a class is also impractical since the individual therapies have differing modes of action, intended use populations, specificities, safety and efficacy outcomes
48 Compared PD-L1 assays and LDTs with 5 PD-L1 antibodies in a 41-case series PD-L1 clones: 28-8, 22C3, E1L3N, SP142, and SP263 IHC platforms: Ventana BenchMark Ultra, Leica Bond or Dako Autostainer Link 48 IHC platforms. To assesse matching platforms: Dako or Ventana assays were performed with clones 22C3, 28-8, SP263 Conclusions: 22C3, 28-8, and SP263 assays were highly concordant amongst several different centers regarding Similar concordance compared to those 3 assays was demonstrated by 14 of 27 (51.8%) LDTs LDTs using clone SP263 achieved the highest concordance rate across all platforms


49 Some studies comparing different PD-L1 IHC assays Blueprint PD-L1 IHC Assay Comparison Project Hirsch FR et al, JTO 2016 Percentage of PD-L1 stained tumor cells was comparable when the 22C3, 28-8, and SP263 assays were used, whereas the SP142 assay exhibited fewer stained tumor cells JAMA Oncol. doi: /jamaoncol Published online March 9, The assay using the SP142 antibody is an outlier that detected significantly less PD-L1 expression in tumor cells and immune cells. The assay for antibody 22c3 showed slight yet statistically significantly lower staining than either 28-8 or E1L3N 3 of the 4 tests are concordant and reproducible JAMA Oncol. 2017;3(2): monoclonal antibodies (SP142, E1L3N, 9A11,SP263, 22c3, and 28-8) Evidence that most antibodies used for PD-L1 studies are highly similar in their ability to bind PDL1
50 Some limitations of these studies Sample selection, were critical samples utilized Those on the threshold of positivity Were assays adjusted in attempt to achieve validation between each other Adjustment of assays in attempts to establish a universal cut off point How does the staining pattern seen relate to patient outcomes? We are really just comparing staining amongst the antibodies, we are not necessarily correlating with patient responses to immunotherapy Diffrent antibodies and different medications bind to different epitopes...
51 Different Epitopes PD-L1 Clone PD-L1 target (immunogen) Drug FDA approval FDA approved indications 22C3 Clone (mouse) 28-8 Clone (rabbit) SP142 Clone (rabbit) SP263 Clone (rabbit) Human extracellular domain (Phe19-Thr239 fused to human IgG1 Purified recombinant human PD-L1, extracellular domain Phe19-Thr239) Synthetic peptide derived from the C- terminus of human PD-L1 Synthetic peptide from the C-terminus of human PD-L1 protein Pembrolizumab Companion Metastaic NSCLC, Metastatic Melanoma, Classical Hodgkin Lymphoma, MSI-H Solid Tumors, Head and Neck Sq cell ca, Urothelial Carcinoma, Gastric Cancer Nivolumab Complementary NSCLC, Melanoma, Classical Hodgkins Lymphoma, Head and Neck Sq cell ca, Urothelial, RCC, HCC previous treated with sorafenib Atezolizumab Complementary Metastatic NSCLC, Metastatic Urothelial Durvalumab Complementary Locally advanced or metastatic Urothelial carcinoma

52 Immunohistochemistry is not a black box Numerous factors Cold ischemia time Fixation time IASLC Atlas for PD-L hrs for bx hrs for resection Antibody target Vendor kit vs. LDT IHC platform Antibody concentration Antibody incubation conditions Detection system Ille M, et al. Virchows Arch. 2016;468(5): Impact of Fixation time (SP142 Ab) And of course other variables
53 Other considerations.
 or antitumorigenic (M1) properties, helper T-cell subsets, cytotoxic T cells, regulatory T cells, B cells, dendritic cells and myeloid-derived suppressor")
54 The cellular cross-talk between different leukocyte subsets and their predominant contribution to either pro- or antitumor activities, including myeloid lineage leukocytes, tumor-associated macrophages with either protumorigenic (M2) or antitumorigenic (M1) properties, helper T-cell subsets, cytotoxic T cells, regulatory T cells, B cells, dendritic cells and myeloid-derived suppressor cells are shown. R. Salgado et al. Ann Oncol 2015;26: The Author Published by Oxford University Press on behalf of the European Society for Medical Oncology. All rights reserved. For permissions, please journals.permissions@oup.com.

55 Other factors and immune regulatory mechanisms are involved Immune interaction looks more like this Not quite this simple and there may be more Pardoll DM Nature Rev Cancer 12, 252, 2012

56 TC negative and IC+ have similar leukocyte infiltrates to TC+ tumors Both had similar expression of PD-1 and other immune checkpoints Suggest patients who score as PD-L1 by many IHC tests may be immunologically indistinguishable from PD-L1+ patients. Conclusions Relying only on PD-L1 IHC scoring to predict sensitivity to PD-1/PD-L1 blockade may exclude some patients who may respond to anti PD-1 therapy. Defined hot and cold tumors Hot tumors (likely to respond) contain CD8+ T cells expressing PD-1 and TIM3 PD-L1 tumor cells Correlate with high mutational load, smoking history, squamous morphology If the critical factor underlying the response to checkpoint blockade is presence of leukocytes: hybrid IHC/flow cytometry may improve (only) PD-L1 IHC as an immune biomarker More studies needed.
57 Tumor mutational burden and MSI-H/MMR-D Note: FDA is not clearly defined which test/s should be run.i.e PCR based MSI testing, IHC MMR testing, both??? Questions still remain for pathologists FDA News Release: May 23, 2017 Pembrolizumab: FDA approval for patients with unresectable or metastatic solid tumors that have been identified as having a biomarker referred to as microsatellite instability-high (MSI-H) or mismatch repair deficient (dmmr) Based on data from KEYNOTE 016, 164, 012, 028, 158 Trials July 31, 2017 FDA grants nivolumab accelerated approval for MSI-H or dmmr colorectal cancer Approval based on Checkmate 142 Trial
58 Tumor Mutational Burden The CheckMate 026 trial Compared the treatment efficacy of nivolumab versus chemotherapy in first line therapy of advanced nonsmall cell lung cancer (NSCLC) based on the programmed death-ligand 1 (PD-L1) expression. However, there was no strong correlation between treatment response and PD-L1 expression. Subanalysis: Question; could tumor mutation burden (TMB) determine nivolumab treatment response? 312 patients with evaluable TMB data: patients with a high mutation burden had a better progression free survival (9.7 vs 5.8 months; HR,0.62) and objective response rate (46.8% vs 28.3%) compared with the control arm. These findings imply that tumor mutation burden may be considered as a biomarker for nivoluamb in the first line treatment of advanced NSCLC AACR annual meeting 2017: CT082 - Impact of tumor mutation burden on the efficacy of first-line nivolumab in stage IV or recurrent nonsmall cell lung cancer: An exploratory analysis of CheckMate 026
59 Plotted objective response rate for anti-pd-1 or anti-pd-l1 therapy against the median tumor mutational burden Literature review, identified 27 tumor types (meta-analysis study) Observed a significant correlation between tumor mutational burden and objective response rate

60 Accelerated Approval based on the Phase II clinical Trial: KEYNOTE-021 ORR was conducted in subgroups defined by PD-L1 tumor expression (TPS: <1% and 1%) TPS <1% subgroup: ORR was 57% in the pembrolizumab plus PC ORR was 13% in the PC alone arm TPS 1% subgroup: ORR was 54% pembrolizumab plus PC ORR was 38% and in the PC alone arm

 between-group differences were noted in either PD-L1 expression or EGFR mutation")
61 September 8 th, 2017 Phase 3 (PACIFIC study) Comparing durvalumab as consolidation therapy with placebo in patients with stage III, locally advanced, unresectable NSCLC that had not progressed after platinum-based chemoradiotherapy No significant (P<0.05) between-group differences were noted in either PD-L1 expression or EGFR mutation status
62 PD-L1 on cytology samples Various trials looking at therapeutic response and PD-L1 expression were not done or validated in cytology material PD-L1 evaluation is often requested on cytology specimens Appl Immunohistochem Mol Morphol ;25(7): Used 28-8 and 22C3 kits used 85-95% concordance between histology and cytology specimens Limited studies...
 regardless of PD-L1 expression Accelerated approval (based on Keynote-059) is")


63 Primary endpoints (Keynote-061) were OS and PFS in PD-L1 positive patients Secondary outcome measures included OS, PFS, and overall response rate (ORR) regardless of PD-L1 expression Accelerated approval (based on Keynote-059) is contingent on confirmatory trials Ongoing phase III KEYNOTE-062 trial is evaluating pembrolizumab alone and in combination with chemotherapy in the frontline setting for PD-L1 positive advanced gastric or GEJ cancer; phase III KEYNOTE-585 trial is studying the combination of pembrolizumab and chemotherapy in the neoadjuvant and adjuvant settings. However, TPS is not used. So when evaluating PD-L1 we need to know what type of tumor we are evaluating for

64
65 Future Directions


66 The state of current immuotherpaies Lasting and significant responses are only occurring in a subset of patients As we have already discussed, there is far more going on than a single molecule ligand interaction
67 Used CRISPR-Cas9 technology CRISPR: clustered, regularly interspaced, palindromic repeats Exploits a bacterial host defense system and uses the DNA-cutting enzyme Cas9 bound to a RNA guide strand that targets a specific genetic sequence


68 CRISPR-Cas9 Cell transfected with a DNA plasmid wit Cas9protein and guide RNA to target the gene of interest Cas9 cuts the DNA sequence of interest (both strands) A modified portion of DNA can be inserted to insert or replace a DNA sequence Known as homology directed repair (HDR)
69
70 Applied this technology to melanoma cells Used ~123K guide RNA sequences targeting thousands of protein coding genes Looked to see which genetically altered cells could escape the immune system Numerous genes identified that may potentially influence T-cell susceptibility When these genes were silenced -> cells survived after being exposed to T-cells conditioned to respond to tumor antigens Genes most influential had roles in antigen presentation and IFN- γ signaling pathways Correlated with patient tumors Many of these genes were altered in patient tumors
71 Correlated with patient tumors Many of these genes were altered in patient tumors, particularly ones immune to cytotoxic T-cell activity One gene: APLNR Codes for apelin receptor: involved in the JAK-STAT signaling pathway and IFN- γ Melanomas known to be resistant to immunotherapies were sequenced, 7 different mutations were found in the APLNR gene



72 Relevance??? PD-L1 is likely a small piece of the immune therapy puzzle 19 genes were found whose activity correlated cytolytic T-cell activity in 36 human cancer types
1 therapies MSI/MMR Mutational profile, tumor immune profiles, etc PD-L1 expression may be very heterogeneous Expression seen in a")

73 Conclusions PD-L1 expression is only a piece of the puzzle As more is learned, other or additional tests may be used to help select patients for PD-(L)1 therapies MSI/MMR Mutational profile, tumor immune profiles, etc PD-L1 expression may be very heterogeneous Expression seen in a small sample may not reflect expression in the entire tumor There are many different antibodies and assays, a clinically validated assay should be used and the pathologist should be trained on how to interpret the stain they are using Know what the type of tumor you are scoring!
74 Guideline??? There is a CAP/IASLC/AMP consensus guideline on molecular testing for lung cancer Future: separate guideline focused on PD-L1 expression testing in lung cancer is on the way
75 Dynamic and rapidly evolving area in Medicine! Currently Six different anti PD-1 or PD-L1 drugs in use More that 20 agents are in clinical testing Several hundred ongoing clinical trials exploring PD-1/PD-L1 inhibitors in combination with other checkpoint antibodies, vaccines, other therapeutics, surgery, and/or radiation therapy. Be willing to adapt accordingly!
 - Tumor cells: No membranous")
76 Continually evolving field So what should we do??? The best we can while providing the information we know in a concise fashion Talk with your oncology colleagues PD-L1 expression (evaluated by immunohistochemistry) - Tumor cells: No membranous staining versus membranous staining in _% of cells - Associated inflammatory cells: no staining versus positive staining in % of cells Please note: PD-L1 is often heterogeneously expressed in tumors. As such, the PD-L1 expression observed in this particular specimen may not reflect the expression in all portions of the patient s malignancy. There are a number of PD-L1 antibodies and assays available. The assay used to evaluate PD-L1 expression in this sample is a laboratory developed test validated at the Houston Methodist Histology Laboratory using the Ventana SP142 antibody.
77 Sincere thanks to Dr. Cagle, the programming committee and the TSP!, Thanks for your attention Enjoy the meeting!
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Review of NEO Testing Platforms. Lawrence M. Weiss, MD Medical Director, Aliso Viejo
 Review of NEO Testing Platforms Lawrence M. Weiss, MD Medical Director, Aliso Viejo Lawrence Weiss, M.D. Medical Director, Aliso Viejo Dr. Weiss currently serves as NeoGenomics Medical Director, Aliso
Review of NEO Testing Platforms Lawrence M. Weiss, MD Medical Director, Aliso Viejo Lawrence Weiss, M.D. Medical Director, Aliso Viejo Dr. Weiss currently serves as NeoGenomics Medical Director, Aliso
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Lung cancer PD-L1 testing clinical impact
 Lung cancer PD-L1 testing clinical impact Korinna Jöhrens Institute for pathology Carl Gustav Cars Universitätsklinikum Dresden, Germany Medical consultant QuIP Immune therapy with checkpoint-inhibitors
Lung cancer PD-L1 testing clinical impact Korinna Jöhrens Institute for pathology Carl Gustav Cars Universitätsklinikum Dresden, Germany Medical consultant QuIP Immune therapy with checkpoint-inhibitors
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al -
 Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Predictive markers for treatment with Immune checkpoint inhibitors - PD-L1 et al - Lukas Bubendorf Pathology Improved overall survival as a result of combination therapy Predictive biomarkers for the treatment
Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations
 Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Immunotherapy in NSCLC Pathologist role
 Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Immunotherapy in NSCLC Pathologist role Pimpin Incharoen, M.D. Assistant Professor, Thoracic Pathology Department of Pathology, Ramathibodi Hospital Genetic alterations in NSCLC Khono et al, Trans Lung
Predictive Biomarkers for Pembrolizumab. Eric H. Rubin, M.D.
 Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
PD-L1 and Immunotherapy of GI cancers: What do you need to know
 None. PD-L1 and Immunotherapy of GI cancers: What do you need to know Rondell P. Graham September 3, 2017 2017 MFMER slide-2 Disclosure No conflicts of interest to disclose 2017 MFMER slide-3 Objectives
None. PD-L1 and Immunotherapy of GI cancers: What do you need to know Rondell P. Graham September 3, 2017 2017 MFMER slide-2 Disclosure No conflicts of interest to disclose 2017 MFMER slide-3 Objectives
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment
 Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
News from ASCO. Niven Mehra, Medical Oncologist. Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital
 News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
Immune checkpoint inhibitors in NSCLC
 1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano
 Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano Unit of Pathology Fondazione IRCCS Casa Sollievo della Sofferenza San Giovanni Rotondo, Foggia,Italy p.graziano@operapadrepio.it Disclosure
Biomarcatori per la immunoterapia: cosa e come cercare Paolo Graziano Unit of Pathology Fondazione IRCCS Casa Sollievo della Sofferenza San Giovanni Rotondo, Foggia,Italy p.graziano@operapadrepio.it Disclosure
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Immunotherapy in lung cancer. Saurabh maji
 Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we
 9e avondsymposium: "Nieuwe ontwikkelingen in de behandeling van NSCLC" 9 november 2016, UMCG Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we Wim Timens Professor and Chair
9e avondsymposium: "Nieuwe ontwikkelingen in de behandeling van NSCLC" 9 november 2016, UMCG Vernieuwing en diagnostiek bij NSCLC: Immunotherapy: PD-L1 analyse: waar staan we Wim Timens Professor and Chair
Cancer Immunotherapy Patient Forum. for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015
 Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
The role of immune checkpoint inhibitors in non-small cell lung cancer
 Review Article Page 1 of 9 The role of immune checkpoint inhibitors in non-small cell lung cancer Tiffany L. George 1, Erin M. Bertino 2 1 Divisions of Hematology and Medical Oncology, 2 Division of Medical
Review Article Page 1 of 9 The role of immune checkpoint inhibitors in non-small cell lung cancer Tiffany L. George 1, Erin M. Bertino 2 1 Divisions of Hematology and Medical Oncology, 2 Division of Medical
O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal. Gabriela Sousa Oncologia Médica IPO Coimbra
 O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal Gabriela Sousa Oncologia Médica IPO Coimbra Incidência aumenta 3% ao ano Envelhecimento populacional
O DESAFIO DA INOVAÇÃO EM ONCOLOGIA EM PORTUGAL The Challenges of innovative oncology care in Portugal Gabriela Sousa Oncologia Médica IPO Coimbra Incidência aumenta 3% ao ano Envelhecimento populacional
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Keytruda. Keytruda (pembrolizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 9 Last Review Date: November 30, 2018 Keytruda Description Keytruda
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 9 Last Review Date: November 30, 2018 Keytruda Description Keytruda
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immunotherapy in non-small cell lung cancer
 Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Alessandro Inno. IRCCS Ospedale Sacro Cuore Don Calabria Negrar, Verona
 GRUPPO C Coordinatore: Diego Signorelli Ruolo dei checkpoint inhibitors nelle neoplasie polmonari: le evidenze scientifiche e l inserimento dei checkpoint inhibitors nell algoritmo decisionale del NSCLC
GRUPPO C Coordinatore: Diego Signorelli Ruolo dei checkpoint inhibitors nelle neoplasie polmonari: le evidenze scientifiche e l inserimento dei checkpoint inhibitors nell algoritmo decisionale del NSCLC
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Keytruda. Keytruda (pembrolizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 9 Last Review Date: September 20, 2018 Keytruda Description Keytruda
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 9 Last Review Date: September 20, 2018 Keytruda Description Keytruda
The Role of Immuno-Oncology Biomarkers in Lung Cancer
 The Role of Immuno-Oncology Biomarkers in Lung Cancer Vamsidhar Velcheti, MD, FACP Staff Physician, Associate Director Center for Immuno-Oncology Research Taussig Cancer Institute Cleveland Clinic November
The Role of Immuno-Oncology Biomarkers in Lung Cancer Vamsidhar Velcheti, MD, FACP Staff Physician, Associate Director Center for Immuno-Oncology Research Taussig Cancer Institute Cleveland Clinic November
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Non-Small Cell Lung Cancer Webinar. Thursday, September 13, p.m. EDT
 Non-Small Cell Lung Cancer Webinar Thursday, September 13, 2018 1 2 p.m. EDT 1 2 Webinar Faculty Julie R. Brahmer, MD Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Patrick Forde, MD Johns
Non-Small Cell Lung Cancer Webinar Thursday, September 13, 2018 1 2 p.m. EDT 1 2 Webinar Faculty Julie R. Brahmer, MD Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins Patrick Forde, MD Johns
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
The PD-1 pathway of T cell exhaustion
 The PD-1 pathway of T cell exhaustion SAMO 18.3.2016 Overview T cell exhaustion Biology of PD-1 Mechanism Ligands expressed on tumor cell and on non-tumor cells other receptor pairs Biomarkers for apd-1/pd-l1
The PD-1 pathway of T cell exhaustion SAMO 18.3.2016 Overview T cell exhaustion Biology of PD-1 Mechanism Ligands expressed on tumor cell and on non-tumor cells other receptor pairs Biomarkers for apd-1/pd-l1
ICLIO National Conference
 ICLIO National Conference Immuno-oncology In The Clinic Today Lee Schwartzberg, MD, FACP Executive Director, West Cancer Center Chief, Division of Hematology/Oncology University of Tennessee Health Science
ICLIO National Conference Immuno-oncology In The Clinic Today Lee Schwartzberg, MD, FACP Executive Director, West Cancer Center Chief, Division of Hematology/Oncology University of Tennessee Health Science
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Opdivo. Opdivo (nivolumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.53 Subsection: Antineoplastic Agents Original Policy Date: January 16, 2015 Subject: Opdivo Page:
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.53 Subsection: Antineoplastic Agents Original Policy Date: January 16, 2015 Subject: Opdivo Page:
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy
: Biomarkers for Immunotherapy") Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Immunotherapeutic Advances in the Treatment of Metastatic Non-Small Cell Lung Cancer
 Immunotherapeutic Advances in the Treatment of Metastatic Non-Small Cell Lung Cancer Srinivasa R. Sanikommu, MD, and Kathryn F. Mileham, MD Abstract Lung cancer remains the leading cause of cancer-related
Immunotherapeutic Advances in the Treatment of Metastatic Non-Small Cell Lung Cancer Srinivasa R. Sanikommu, MD, and Kathryn F. Mileham, MD Abstract Lung cancer remains the leading cause of cancer-related
Keytruda. Keytruda (pembrolizumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 7 Last Review Date: December 8, 2017 Keytruda Description Keytruda
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.50 Subject: Keytruda Page: 1 of 7 Last Review Date: December 8, 2017 Keytruda Description Keytruda
Clinical Need and diagnostic challenge-the upcoming landscape of checkpointinhibitors
 Clinical Need and diagnostic challenge-the upcoming landscape of checkpointinhibitors ESP/ESMO Marina Chiara GARASSINO Amsterdam 2017 September, 4th 29 European Congress of Pathology Disclosures BMS ROCHE
Clinical Need and diagnostic challenge-the upcoming landscape of checkpointinhibitors ESP/ESMO Marina Chiara GARASSINO Amsterdam 2017 September, 4th 29 European Congress of Pathology Disclosures BMS ROCHE
Biomarkers for Cancer Immunotherapy Debate
 Biomarkers for Cancer Immunotherapy Debate Moderator: Maria Karasarides, PhD AstraZeneca Pro: Daniel S. Chen, MD, PhD Genentech Con: Steve Averbuch, MD Bristol-Myers Squibb Biomarkers to Select Patients
Biomarkers for Cancer Immunotherapy Debate Moderator: Maria Karasarides, PhD AstraZeneca Pro: Daniel S. Chen, MD, PhD Genentech Con: Steve Averbuch, MD Bristol-Myers Squibb Biomarkers to Select Patients
Emerging Tissue and Serum Markers
 Emerging Tissue and Serum Markers for Immune Checkpoint Inhibitors Kyong Hwa Park MD, PhD Medical Oncology Korea University College of Medicine Contents Immune checkpoint inhibitors in clinical practice
Emerging Tissue and Serum Markers for Immune Checkpoint Inhibitors Kyong Hwa Park MD, PhD Medical Oncology Korea University College of Medicine Contents Immune checkpoint inhibitors in clinical practice
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Policy. Medical Policy Manual Approved Revised: Do Not Implement until 6/30/2019. Nivolumab
 Medical Manual Approved Revised: Do Not Implement until 6/30/2019 Nivolumab NDC CODE(S) 00003-3772-XX Opdivo 40 MG/4ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3774-XX Opdivo 100 MG/10ML SOLN (B-M SQUIBB
Medical Manual Approved Revised: Do Not Implement until 6/30/2019 Nivolumab NDC CODE(S) 00003-3772-XX Opdivo 40 MG/4ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3774-XX Opdivo 100 MG/10ML SOLN (B-M SQUIBB
Advances in Pathology and molecular biology of lung cancer. Lukas Bubendorf Pathologie
 Advances in Pathology and molecular biology of lung cancer Lukas Bubendorf Pathologie Agenda The revolution of predictive markers Liquid biopsies PD-L1 Molecular subtypes (non-squamous NSCLC) Tsao AS et
Advances in Pathology and molecular biology of lung cancer Lukas Bubendorf Pathologie Agenda The revolution of predictive markers Liquid biopsies PD-L1 Molecular subtypes (non-squamous NSCLC) Tsao AS et
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management
 Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Histology independent indications in Oncology
 CHMP Oncology Working Party Workshop Histology independent indications in Oncology What have we learnt from the anti PD1- PDL1 story? J Camarero (CHMP alternate ES, OncWP) Disclaimers the views presented
CHMP Oncology Working Party Workshop Histology independent indications in Oncology What have we learnt from the anti PD1- PDL1 story? J Camarero (CHMP alternate ES, OncWP) Disclaimers the views presented
Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018
 Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018 David R. Gandara, MD University of California Davis Comprehensive Cancer Center Disclosures Research Grants: AstraZeneca/Medi,
Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018 David R. Gandara, MD University of California Davis Comprehensive Cancer Center Disclosures Research Grants: AstraZeneca/Medi,
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Agilent companion diagnostics for cancer immunotherapy
 Agilent companion diagnostics for cancer immunotherapy Annika Eklund, PhD Global Product Manager Companion Diagnostics Agilent Technologies Aalborg 1 Agilent Trusted Answers. Together OUR FOCUS life sciences,
Agilent companion diagnostics for cancer immunotherapy Annika Eklund, PhD Global Product Manager Companion Diagnostics Agilent Technologies Aalborg 1 Agilent Trusted Answers. Together OUR FOCUS life sciences,
Tumor Immunity and Immunotherapy. Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School
 Tumor Immunity and Immunotherapy Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School Lecture Outline Evidence for tumor immunity Types of tumor antigens Generation of anti-tumor
Tumor Immunity and Immunotherapy Andrew Lichtman M.D., Ph.D. Brigham and Women s Hospital Harvard Medical School Lecture Outline Evidence for tumor immunity Types of tumor antigens Generation of anti-tumor
IMMUNOTHERAPY FOR THE TREATMENT OF LUNG CANCER
 IMMUNOTHERAPY FOR THE TREATMENT OF LUNG CANCER A guide for patients and caregivers TM Content is consistent with the Oncology Nursing Society Standards and Guidelines. The ONS Seal of Approval does not
IMMUNOTHERAPY FOR THE TREATMENT OF LUNG CANCER A guide for patients and caregivers TM Content is consistent with the Oncology Nursing Society Standards and Guidelines. The ONS Seal of Approval does not
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker
 Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Biomarkers in Imunotherapy: RNA Signatures as predictive biomarker Joan Carles, MD PhD Director GU, CNS and Sarcoma Program Department of Medical Oncology Vall d'hebron University Hospital Outline Introduction
Focus on Immunotherapy as a Targeted Therapy. Brad Nelson, PhD BC Cancer, Victoria, Canada FPON, Oct
 Focus on Immunotherapy as a Targeted Therapy Brad Nelson, PhD BC Cancer, Victoria, Canada FPON, Oct 18 2018 Disclosures I have nothing to disclose that is relevant to this presentation. Immunology @ Deeley
Focus on Immunotherapy as a Targeted Therapy Brad Nelson, PhD BC Cancer, Victoria, Canada FPON, Oct 18 2018 Disclosures I have nothing to disclose that is relevant to this presentation. Immunology @ Deeley
Professor Mark Bower Chelsea and Westminster Hospital, London
 Professor Mark Bower Chelsea and Westminster Hospital, London Cancer immunotherapy & HIV Disclosures: None Lessons for oncology from HIV Awareness and advocacy Activism Rational drug design Prescribing
Professor Mark Bower Chelsea and Westminster Hospital, London Cancer immunotherapy & HIV Disclosures: None Lessons for oncology from HIV Awareness and advocacy Activism Rational drug design Prescribing
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
I farmaci immunoterapici. Stefano Fogli UO Farmacologia Clinica e Farmacogenetica Dipartimento di Medicina Clinica e Sperimentale Università di Pisa
 I farmaci immunoterapici Stefano Fogli UO Farmacologia Clinica e Farmacogenetica Dipartimento di Medicina Clinica e Sperimentale Università di Pisa History of Cancer Immunotherapy Discovery of dendritic
I farmaci immunoterapici Stefano Fogli UO Farmacologia Clinica e Farmacogenetica Dipartimento di Medicina Clinica e Sperimentale Università di Pisa History of Cancer Immunotherapy Discovery of dendritic
Immunotherapy in head and neck cancer and MSI in solid tumors
 Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
Policy. Medical Policy Manual Approved Revised: Do Not Implement Until 3/2/19. Nivolumab (Intravenous)
") Nivolumab (Intravenous) NDC CODE(S) 00003-3772-XX Opdivo 40 MG/4ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3774-XX Opdivo 100 MG/10ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3734-XX Opdivo 240
Nivolumab (Intravenous) NDC CODE(S) 00003-3772-XX Opdivo 40 MG/4ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3774-XX Opdivo 100 MG/10ML SOLN (B-M SQUIBB U.S. (PRIMARY CARE)) 00003-3734-XX Opdivo 240
Disclosures. Immunotherapyin Head & NeckCancer. Actual landscape of systemic treatment in HNSCC. Head andneckcanceris an immunogeneic tumor
 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Emerging biomarkers for immunotherapy in lung cancer
 Emerging biomarkers for immunotherapy in lung cancer Prof Keith M Kerr Department of Pathology Aberdeen University Medical School, Aberdeen Royal Infirmary Aberdeen, UK Why Do We Need Biomarkers for Immunotherapy?
Emerging biomarkers for immunotherapy in lung cancer Prof Keith M Kerr Department of Pathology Aberdeen University Medical School, Aberdeen Royal Infirmary Aberdeen, UK Why Do We Need Biomarkers for Immunotherapy?
Merck Oncology Overview. The Development of MSI-H Cancer Therapy. Development of Anti-Cancer Drugs Forum Tokyo, Japan, 18, February 2017
 Merck Oncology Overview The Development of MSI-H Cancer Therapy Development of Anti-Cancer Drugs Forum Tokyo, Japan, 18, February 217 Andrew Joe, MD Executive Director, Late Stage Oncology Merck & Co.,
Merck Oncology Overview The Development of MSI-H Cancer Therapy Development of Anti-Cancer Drugs Forum Tokyo, Japan, 18, February 217 Andrew Joe, MD Executive Director, Late Stage Oncology Merck & Co.,
Opdivo. Opdivo (nivolumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.53 Subsection: Antineoplastic nts Original Policy Date: January 16, 2015 Subject: Opdivo Page: 1 of
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.21.53 Subsection: Antineoplastic nts Original Policy Date: January 16, 2015 Subject: Opdivo Page: 1 of
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER. Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium
 THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
THE FUTURE OF IMMUNOTHERAPY IN COLORECTAL CANCER Prof. Dr. Hans Prenen, MD, PhD Oncology Department University Hospital Antwerp, Belgium DISCLAIMER Please note: The views expressed within this presentation
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro. Immune checkpoint inhibition in DLBCL
 Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
El contexto molecular de la sobreexpresión de PD-L1 Esther Conde Gallego, MD, PhD
 El contexto molecular de la sobreexpresión de PD-L1 Esther Conde Gallego, MD, PhD Laboratorio de Dianas Terapéuticas Hospital Universitario HM Sanchinarro Madrid, Spain Contents Background PD-L1 expression
El contexto molecular de la sobreexpresión de PD-L1 Esther Conde Gallego, MD, PhD Laboratorio de Dianas Terapéuticas Hospital Universitario HM Sanchinarro Madrid, Spain Contents Background PD-L1 expression
Medical Treatment of Advanced Lung Cancer
 Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Immunotherapy for dmmr metastatic colorectal cancer. Prof.dr. Kees Punt Dept. Medical Oncology AUMC
 Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Immune Checkpoints. PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich
 Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Highlights from AACR 2015: The Emerging Potential of Immunotherapeutic Approaches in Non-Small Cell Lung Cancer
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Lung Cancer Immunotherapy
 Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
Lung Cancer Immunotherapy Luis E. Raez MD FACP FCCP Chief of Hematology/Oncology & Medical Director Memorial Cancer Institute/Memorial Health Care System Clinical Professor of Medicine Herbert Wertheim
New Paradigms for Treatment of. Erminia Massarelli, MD, PHD, MS Clinical Associate Professor
 New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy in NSCLC
 Assay Guiding immunotherapy in NSCLC") VENTANA (SP142) Assay Guiding immunotherapy in NSCLC Hiker s path: VENTANA (SP142) Assay on non-small cell lung cancer tissue Location: Point Conception, CA VENTANA (SP142) Assay Assess NSCLC patient benefit
VENTANA (SP142) Assay Guiding immunotherapy in NSCLC Hiker s path: VENTANA (SP142) Assay on non-small cell lung cancer tissue Location: Point Conception, CA VENTANA (SP142) Assay Assess NSCLC patient benefit
PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER
 PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER Martin Reck Department of Thoracic Oncology LungClinic Grosshansdorf Germany DISCLOSURES Honoraria for
PATIENT SELECTION CORRELATION OF PD-L1 EXPRESSION AND OUTCOME? THE ONCOLOGIST VIEW ON LUNG CANCER Martin Reck Department of Thoracic Oncology LungClinic Grosshansdorf Germany DISCLOSURES Honoraria for
Lights and sheds of early approval of new drugs in clinical routine. Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy
 Lights and sheds of early approval of new drugs in clinical routine Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy RCT 5-10% pts «real» patients are here Clin. Pharm. Ther. 2012
Lights and sheds of early approval of new drugs in clinical routine Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy RCT 5-10% pts «real» patients are here Clin. Pharm. Ther. 2012
Immuno-Oncology Clinical Trials Update: Therapeutic Anti-Cancer Vaccines Issue 7 April 2017
 Delivering a Competitive Intelligence Advantage Immuno-Oncology Clinical Trials Update: Therapeutic Anti-Cancer Vaccines Issue 7 April 2017 Immuno-Oncology CLINICAL TRIALS UPDATE The goal of this MONTHLY
Delivering a Competitive Intelligence Advantage Immuno-Oncology Clinical Trials Update: Therapeutic Anti-Cancer Vaccines Issue 7 April 2017 Immuno-Oncology CLINICAL TRIALS UPDATE The goal of this MONTHLY
2016 Updates in Oncology & Malignant Hematology Brendan Curley, DO
 2016 Updates in Oncology & Malignant Hematology Brendan Curley, DO Disclosures I received final support from ASCO Conquer Cancer foundation in two Merit Awards and one travel award I am on the speakers
2016 Updates in Oncology & Malignant Hematology Brendan Curley, DO Disclosures I received final support from ASCO Conquer Cancer foundation in two Merit Awards and one travel award I am on the speakers
PD-1 Pathway Inhibitors: Immuno-Oncology Agents for Restoring Antitumor Immune Responses
 PD-1 Pathway Inhibitors: Immuno-Oncology Agents for Restoring Antitumor Immune Responses Patrick J. Medina, 1, * and Val R. Adams, 2 1 Department of Pharmacy: Clinical and Administrative Sciences, The
PD-1 Pathway Inhibitors: Immuno-Oncology Agents for Restoring Antitumor Immune Responses Patrick J. Medina, 1, * and Val R. Adams, 2 1 Department of Pharmacy: Clinical and Administrative Sciences, The
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy
 Assay Guiding immunotherapy") VENTANA PD-L1 (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA PD-L1 (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA PD-L1 (SP142) Assay Identify patients most
VENTANA PD-L1 (SP142) Assay Guiding immunotherapy Hiker s path: VENTANA PD-L1 (SP142) Assay on urothelial carcinoma tissue Location: Point Conception, CA VENTANA PD-L1 (SP142) Assay Identify patients most
IMMUNOTHERAPY FOR CANCER A NEW HORIZON. Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust
 IMMUNOTHERAPY FOR CANCER A NEW HORIZON Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust ASCO Names Advance of the Year: Cancer Immunotherapy No recent
IMMUNOTHERAPY FOR CANCER A NEW HORIZON Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust ASCO Names Advance of the Year: Cancer Immunotherapy No recent