89 Emerging Molecular Diagnostic Tests and Therapies for Melanoma. Aleodor Andea MD
|
|
|
- Hope Parker
- 5 years ago
- Views:
Transcription
1 89 Emerging Molecular Diagnostic Tests and Therapies for Melanoma Aleodor Andea MD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste Chicago, IL 60603
2 89 Emerging Molecular Diagnostic Tests and Therapies for Melanoma Malignant melanoma is the leading cause of death among cutaneous neoplasms. The diagnosis and differentiation of melanoma from benign nevi is currently based on morphology however; in a significant number of cases a definitive diagnosis of melanoma is not possible. Recent molecular studies have revealed genomic differences between melanomas which harbor numerous chromosomal gains and losses and benign nevi which have no detectable chromosomal aberrations. Assays evaluating these abnormalities are ready to be implemented into clinical practice and could become important tools in the diagnosis of this deadly disease. On the therapy side, agents targeting specific pathways active in melanomas are being aggressively investigated with some, including BRAF inhibitors, getting ready for primetime. The session will focus on the utility of comparative genomic hybridization using metaphase chromosomes and microarrays as well as fluorescent in situ-hybridization in establishing a diagnosis of melanoma. In addition, data reflecting the efficacy of the newly FDA approved BRAF inhibitor (vemurafenib) in metastatic melanoma will be presented and the role of BRAF mutation testing discussed. Recognize the categories of melanocytic lesions for which an accurate histologic diagnosis is difficult. Determine appropriate ancillary studies that may help establish a correct diagnosis. Become familiar with new agents used for the treatment of melanoma. FACULTY: Aleodor Andea MD Practicing Pathologists Molecular Pathology Molecular Pathology 1.0 CME/CMLE Credit Accreditation Statement: The American Society for Clinical Pathology (ASCP) is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education (CME) for physicians. This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education (ACCME). Credit Designation: The ASCP designates this enduring material for a maximum of 1 AMA PRA Category 1 Credits. Physicians should only claim credit commensurate with the extent of their participation in the activity. ASCP continuing education activities are accepted by California, Florida, and many other states for relicensure of clinical laboratory personnel. ASCP designates these activities for the indicated number of Continuing Medical Laboratory Education (CMLE) credit hours. ASCP CMLE credit hours are acceptable to meet the continuing education requirements for the ASCP Board of Registry Certification Maintenance Program. All ASCP CMLE programs are conducted at intermediate to advanced levels of learning. Continuing medical education (CME) activities offered by ASCP are acceptable for the American Board of Pathology s Maintenance of Certification Program.
3 Emerging Molecular Diagnostic Tests and Therapies for Melanoma Aleodor Andea, MD Associate Professor of Pathology and Dermatology Director of Dermatopathology Section University of Alabama at Birmingham Birmingham, USA Disclosure information I have no financial or industrial affiliation to disclose. Aleodor A Andea Overview 1. Problems in the diagnosis 2. Molecular alterations (with implications for diagnosis or treatment) 3. Diagnostic assays 4. New therapies 1
4 NEVI Melanoma diagnosis MELANOMA Small Symmetric Well-circumscribed Predominantly nested Uniform No No Present Absent Absent Absent Size Symmetry Circumscription Nested architecture Nests uniformity Pagetoid spread Confluent growth at DEJ Maturation Cytologic atypia Mitoses in dermis Atypical mitoses Large Asymmetric Poorly-circumscribed Predominantly single cells Irregular Prominent Present Absent Severe Present Present ~1 2 million bx/ year in US to rule out melanoma ~3% 6% of bx are melanomas In most cases dx can be made on histopathology 2.3% 25% of cases with diagnostic discrepancies (McGinnin et al, Arch Dermatol 2002, Corona et al, J Clin Oncol 1996, Farmer et al, Hum Pathol 1996, Lodha et al J Cutan Pathol 2008) Reasons for discrepancy Ambiguous lesions with overlapping criteria Atypical Spitz nevi Atypical blue nevi Recurrent melanocytic nevi Nevi in acral, genital or mammary line regions Nevoid melanoma Inter observer variability 2
5 Need for a better test Prevent under/overtreatment of patients Reduce medical costs associated with unnecessary treatment Impact positively on patient care Most common reason for medical malpractice in pathology Kornstein, et al. Arch Pathol and Lab Med, 2007 Gerami, et al, Am J Surg Pathol, 2009 Molecular alterations in melanocytic neoplasms MAP kinase alterations Replicative senescence in melanocytic lesions GROWTH FACTORS MAP Kinase CY YTOPLASM RAS RAF MEK H-Ras, K-Ras, N-Ras A-Raf, B-Raf, C-Raf1 MEK-1, MEK-2 ERK ERK-1, ERK-2 NUCLEUS PROLIFERATION 3
6 GROWTH FACTORS MAP Kinase KIT mutations in 17% of melanomas RAS CY YTOPLASM RAF MEK ERK NUCLEUS PROLIFERATION Curtin et al., N Engl J Med, 2005 MAP Kinase pathway activation in melanocytic lesions GROWTH FACTORS CY YTOPLASM NRAS RAF MEK 30% of melanomas ERK NUCLEUS PROLIFERATION Albino et al., Oncogene 1989 MAP Kinase pathway activation in melanocytic lesions GROWTH FACTORS CY YTOPLASM HRAS RAF MEK Spitz s nevi ERK NUCLEUS PROLIFERATION Bastian B et al, Am J Pathol
7 MAP Kinase pathway activation in melanocytic lesions GROWTH FACTORS RAS CY YTOPLASM B-RAF MEK 40-60% of melanomas, 80% of nevi ERK NUCLEUS PROLIFERATION Davies et al, Nature 2002, Marcia et al. Cancer Res 2002, Curtin et al, N Engl J Med 2005, Pollock et al., Nat Genet 2002 B Raf mutations in melanocytic lesions Lesion % with B-Raf mutation Melanomas 56-80% Nevi Congenital 86% Intradermal 88% Compound 70% Clark s 52-80% Spitz 0% Spitzoid Melanomas 0% Replicative senescence in melanocytic lesions s are protected by telomeres and the enzyme telomerase Greider and Blackburn EH, Nature 1989 Szostak et al, Cell
8 T T T T Mitosis T T T Mitosis T T p53, P53, RB, p16 Checkpoint Cell cycle arrest (Senescence) T T T T Mitosis T T T Mitosis T T Mitosis T Mitosis p53, P53, RB, p16 T T T T T T T T T p53, P53, RB, p16 T Mitosis Mitosis DNA breaks, fusions Cell Crisis Gross chromosomal abnormalities Increase apoptosis Cell Death 6
9 Nevi T T T T Mitosis T T T MAPK -B-RAF -N-RAS -H-RAS Mitosis T T p53, RB, p16 Cell cycle arrest ( Oncogene- Induced Senescence) No chromosomal aberrations T T T T Mitosis Mitosis Mitosis T T T T T Mitosis Melanoma T Mitosis DNA breaks, fusions +/- p53, P53, RB, p16 MAPK -B-RAF -N-RAS -H-RAS Cell cycle arrest (Senescence) Cell Crisis -Re-stabilize telomeres -growth advantage Cell Death Melanoma Gross chromosomal abnormalities Molecular tests differentiating melanoma from nevi IHC Expression microarrays CGH FISH 7
 Ki")




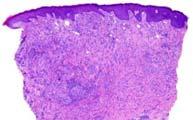
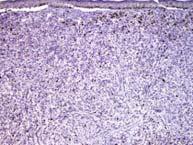
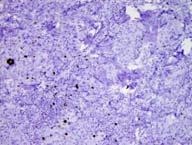


10 Nevus (<5%) Ki 67 Melanoma (>5%) Spindle cell melanoma Ki 67 problems Indeterminate lesion HMB 45/ Cyclin D1 Nevus Melanoma 8


11 HMB 45 problems Combined Nevus Melanoma Spitz Nevus p16 Melanoma Positive in 100% of Spitz nevi Negative in 32-50% of melanomas Stefanaki et al, J Am Acad Dermatol 2007 Expression microarray 9
 Nevi (98%) Problems with tissue microarrays Expensive Require microdissection Difficult to reproduce results Multi marker assays")
12 120 melanocytic lesions FFPE Combimatrix CustomArray Platform Hierarchical clustering Koh et al., Mod Pathol 2009 Melanomas (95%) Nevi (98%) Problems with tissue microarrays Expensive Require microdissection Difficult to reproduce results Multi marker assays Gene espression microarrays Small set of discriminant markers IHC 10


13 Multi marker assays Gene espression microarrays Small set of discriminant markers IHC ARPC2 FN1 RGS1 SPP1 WNT2 Kashani-Sabet et al. PNAS 2009, Haqq et al. PNAS 2005 IHC Top: 0, 1+, 2+, 3+ Algorithm for discrimination 95% specificity 91% sensitivity Bottom: 0, 1+, 2+, 3+ Kashani-Sabet et al. PNAS 2009 Kashani-Sabet et al. PNAS


14 Comparative Genomic Hybridization Screens the entire genome for gains and losses in DNA material in one experiment Variants: Conventional CGH Array based CGH Conventional CGH The ratio of green:red signals along each chromosome is determined 12

15 Array CGH Arrays of genomic bacterial artificial chromosome (BAC) clones CGH in Melanocytic lesions 54 benign nevi 27 Spitz nevi 19 Blue nevi 7 Congenital nevi 132 MM 22 Acral location 108 non Acral Bastian B et al, Am J Pathol
16 Gains: 6p Losses: Gains: 11p: 11% Losses: 1q 7p 7q 8q 9p 9q 10q 10p 7q: 2% 0% 17q 20q 6q 11q The 7 cases were all Spitz nevi (no progression to MM at 7 yrs FU) 96% of cases Bastian B et al, Am J Pathol 2003 Conclusion Potential diagnostic test for ambiguous melanocytic lesions. Chromosomal Aberrations in Ambiguous Melanocytic Lesions Spitz nevi: no abnormalities gains on 11p (12 18%) 18%) Congenital nevi: no abnormalities Cellular blue nevi: no abnormalities Maize Jr, JC et al, Am J Surg Pathol 2005 Bastian B et al, Am J Pathol 2000 Bastian B et al, J Invest Pathol 1999 Bastian B et al, Am J Pathol

17 Disadvantages of CGH Requires 30 50% pure tumor cells Does not allow histologic correlation Cannotdetecttumor tumor subpopulations FISH 15
18 CGH date from melanomas Gerami et al. Am J Surg Pathol q31 (COX2) 4q12 (KIT) 7q34 (BRAF) 6p35 (RREB1) 6q23 (MYB1) 6 cen 7 cen 9p31 (p16) 10 cen 11q13 (CCND1) 17q25 (TK1) 17q21 (RARA) 17 cen 20q13 (ZNF217) Training cohort 301 melanocytic tumors 148 melanomas 153 nevi Validation cohort Unequivocal lesions: 83 melanomas 86 nevi 27 ambiguous cases with clinical follow up 6 cases developed metastases 21 free of disease at > 5 years follow up Gerami et al. Am J Surg Pathol 2009 Gerami et al. Am J Surg Pathol

19 Validation cohort: 72 of 83 melanomas FISH positive 87% sensitivity 82 of 86 nevi FISH negative 95% specificity 4 nevi were FISH positive Gerami et al. Am J Surg Pathol cases with indeterminate histology 6 developed metastases, all FISH positive 100% sensitivity 21 disease free at > 5 years, 15 FISH negative 71% specificity Gerami et al. Am J Surg Pathol Nevi 20 Melanomas 19/20 negative Specificity 95% 18/20 positive Sensitivity 90% 17
 73% 6p25 gain (RREB1) 68% 6p25 gain (RREB1) 82% 6p25 gain (RREB1) 100% 22")
 -3 benign (1 FISH negative) Other potential applications Nevoid melanomas vs Mitotically active")
20 Superficial Lentigo Nodular Acral Spreading Maligna N=22 lentiginous N=70 N=28 N=3 Sensitivity 81% 82% 91% 100% Most common alteration 6p25 gain (RREB1) 73% 6p25 gain (RREB1) 68% 6p25 gain (RREB1) 82% 6p25 gain (RREB1) 100% 22 total lesions - Sensitivity: 60% - Specificity: 33% 12 ambiguous lesions FISH worked in 8 cases -5 malignant (3 FISH positive) -3 benign (1 FISH negative) Other potential applications Nevoid melanomas vs Mitotically active nevi 18
21 Mitotically active nevus N=10 Nevoid melanoma N=10 10/10 cases FISH negative 10/10 cases FISH positive Gerami et al. Am J Surg Pathol 2009 Other potential applications Nevoid melanomas vs Mitotically active nevi Intranodal nevus vs Metastatic Melanoma Metastatic melanoma N=24 Nodal nevus N=17 FISH status 20 cases FISH positive 16 cases FISH negative Sensitivity 83% Specificity 94% 4 FISH negative metastases In 2 the primary melanoma was also FISH negative 1 FISH positive nevus Scott et al. Am J Surg Pathol
22 Other potential applications Nevoid melanomas vs Mitotically active nevi Intranodal nevus vs Metastatic Melanoma Blue nevus vs Blue nevus like metastatic melanoma Blue nevus like metastatic melanoma N=10 Blue nevus N=10 FISH status 9 cases FISH positive 10 cases FISH negative Sensitivity 90% Specificity 100% 6p25 gains Pouryazdanparast et al. Am J Surg Pathol 2009 Other potential applications Nevoid melanomas vs Mitotically active nevi Intranodal nevus vs Metastatic Melanoma Blue nevus vs Blue nevus like metastatic melanoma Micro staging in melanomas with associated nevi 20
23 Conclusion FISH provide additional criteria to help diagnose histologically ambiguous cases This test should be performed in conjunction with standard histopathologic evaluation How to use molecular testing Not in all cases! Only when histology is ambiguous Clinically relevant Trust your clinical judgment Is this final? Sensitivity not great Interpretation is labor intensive Technically challenging Expensive More probes/cutoff points need to be evaluated 21
24 Melanoma treatment FDA approved therapy High dose interleukin 2 Dacarbazine Response rates: 7 20% No improvement in survival New FDA approved drugs Ipilimumab (YERVOY) FDA approval: 3/25/2011 Vemurafenib (ZELBORAF) FDA approval: 8/17/2011 /
25 Ipilimumab Blocks cytotoxic T lymphocyte associated antigen 4 (CTLA4) APC MHC TCR Ag T-cell CD80/86 CD28 Melanoma APC MHC TCR Ag T-cell CD80/86 CTLA-4 Melanoma 23
26 APC MHC TCR Ag T-cell CTLA-4 CD80/86 Anti CTLA-4 AB Melanoma Ipilimumab phase 3 trial Hodi et al. N Eng J Med, 2010, Ipilimumab phase 3 trial Robert et al. N Eng J Med, 2011, 24
27 BRAF V600E inhibitor Vemurafenib MAP Kinase pathway activation in melanocytic lesions GROWTH FACTORS RAS CY YTOPLASM B-RAF MEK 40-60% of melanomas, 90% is V600E ERK NUCLEUS PROLIFERATION MAP Kinase pathway activation in melanocytic lesions GROWTH FACTORS RAS CY YTOPLASM B-RAF MEK Vemurafenib ERK NUCLEUS PROLIFERATION 25
28 PLX4032 (Vemurafenib) Phase I : Complete or partial tumor regression 81% Phase II (BRAF Inhibitor in 2 (BRIM2)): Single arm study 132 patients 2% complete response 53% show a >30% tumor reduction 30% stable disease Flaherty et al. N Eng J Med, 2010, PLX4032 (Vemurafenib) Phase III (BRIM3): 675 patients Vemurafenib vs Dacarbazine 63% reduction in risk of death 74% reduction in risk of death and disease progression Vemurafenib phase 3 trial 26
29 Rash Photosensitivity Hair loss Joint pain Liver problems Arrhythmias Allergic reactions Cutaneous SCC (26%) Side effects Cobas 4800 BRAF V600 Mutation Test FDA approved companion diagnostic test Detects BRAF V600E mutation Real time PCR References Molecular alterations in melanoma 1. Albino AP, Nanus DM, Mentle IR, Cordon Cardo C, McNutt NS, Bressler J et al. Analysis of ras oncogenes in malignant melanoma and precursor lesions: correlation of point mutations with differentiation phenotype. Oncogene 1989;4: Bastian BC, LeBoit PE, Pinkel D. Mutations and copy number increase of HRAS in Spitz nevi with distinctive histopathological features. Am J Pathol 2000;157: Curtin JA, Busam K, Pinkel D, Bastian BC. Somatic activation of KIT in distinct subtypes of melanoma. J Clin Oncol 2006;24: Curtin JA, Fridlyand J, Kageshita T, Patel HN, Busam KJ, Kutzner H et al. Distinct sets of genetic alterations in melanoma. N Engl J Med 2005;353: Davies H, Bignell GR, Cox C, Stephens P, Edkins S, Clegg S et al. Mutations of the BRAF gene in human cancer. Nature 2002;417: Haqq C, Nosrati M, Sudilovsky D, Crothers J, Khodabakhsh D, Pulliam BL et al. The gene expression signatures of melanoma progression. Proc Natl Acad Sci U S A 2005;102: Jaeger J, Koczan D, Thiesen HJ, Ibrahim SM, Gross G, Spang R et al. Gene expression signatures for tumor progression, tumor subtype, and tumor thickness in laser microdissected melanoma tissues. Clin Cancer Res 2007;13: Kashani Sabet M, Rangel J, Torabian S, Nosrati M, Simko J, Jablons DM et al. A multi marker assay to distinguish malignant melanomas from benign nevi. Proc Natl Acad Sci U S A 2009;106: Koh SS, Opel ML, Wei JP, Yau K, Shah R, Gorre ME et al. Molecular classification of melanomas and nevi using gene expression microarray signatures and formalin fixed and paraffin embedded tissue. Mod Pathol 2009;22: Pollock PM, Harper UL, Hansen KS, Yudt LM, Stark M, Robbins CM et al. High frequency of BRAF mutations in nevi. Nat Genet 2003;33:
30 CGH/ FISH in melanoma References 1. Bastian BC, LeBoit PE, Pinkel D. Mutations and copy number increase of HRAS in Spitz nevi with distinctive histopathological features. Am J Pathol 2000;157: Bastian BC, Olshen AB, LeBoit PE, Pinkel D. Classifying melanocytic tumors based on DNA copy number changes. Am J Pathol 2003;163: Bastian BC, Wesselmann U, Pinkel D, Leboit PE. Molecular cytogenetic analysis of Spitz nevi shows clear differences to melanoma. J Invest Dermatol 1999;113: Bastian BC, Xiong J, Frieden IJ, Williams ML, Chou P, Busam K et al. Genetic changes in neoplasms arising in congenital melanocytic nevi: differences between nodular proliferations and melanomas. Am J Pathol 2002;161: Bauer J, Bastian BC. Distinguishing melanocytic nevi from melanoma by DNA copy number changes: comparative genomic hybridization as a research and diagnostic tool. Dermatol Ther 2006;19: Dalton SR, Gerami P, Kolaitis NA, Charzan S, Werling R, LeBoit PE et al. Use of fluorescence in situ hybridization (FISH) to distinguish intranodal nevus from metastatic melanoma. Am J Surg Pathol 2010;34: Gaiser T, Kutzner H, Palmedo G, Siegelin MD, Wiesner T, Bruckner T et al. Classifying ambiguous melanocytic lesions with FISH and correlation with clinical long term follow up. Mod Pathol 2010;23: Gerami P, Jewell SS, Morrison LE, Blondin B, Schulz J, Ruffalo T et al. Fluorescence in situ hybridization (FISH) as an ancillary diagnostic tool in the diagnosis of melanoma. Am J Surg Pathol 2009;33: Gerami P, Mafee M, Lurtsbarapa T, Guitart J, Haghighat Z, Newman M. Sensitivity of fluorescence in situ hybridization for melanoma diagnosis using RREB1, MYB, Cep6, and 11q13 probes in melanoma subtypes. Arch Dermatol 2010;146: CGH/ FISH in melanoma References 10. Gerami P, Wass A, Mafee M, Fang Y, Pulitzer MP, Busam KJ. Fluorescence in situ hybridization for distinguishing nevoid melanomas from mitotically active nevi. Am J Surg Pathol 2009;33: Maize JC, Jr., McCalmont TH, Carlson JA, Busam KJ, Kutzner H, Bastian BC. Genomic analysis of blue nevi and related dermal melanocytic proliferations. Am J Surg Pathol 2005;29: Moore SR, Persons DL, Sosman JA, Bobadilla D, Bedell V, Smith DD et al. Detection of copy number alterations in metastatic melanoma by a DNA fluorescence in situ hybridization probe panel and array comparative genomic hybridization: a southwest oncology group study (S9431). Clin Cancer Res 2008;14: Morey AL, Murali R, McCarthy SW, Mann GJ, Scolyer RA. Diagnosis of cutaneous melanocytic tumours by four colour fluorescence in situ hybridisation. Pathology 2009;41: Newman MD, Lertsburapa T, Mirzabeigi M, Mafee M, Guitart J, Gerami P. Fluorescence in situ hybridization as a tool for microstaging in malignant melanoma. Mod Pathol 2009;22: Newman MD, Mirzabeigi M, Gerami P. Chromosomal copy number changes supporting the classification of lentiginous junctional melanoma of the elderly as a subtype of melanoma. Mod Pathol 2009;22: Pouryazdanparast P, Newman M, Mafee M, Haghighat Z, Guitart J, Gerami P. Distinguishing epithelioid blue nevus from blue nevus like cutaneous melanoma metastasis using fluorescence in situ hybridization. Am J Surg Pathol 2009;33: Ipilimumab References 1. Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med 2010;363: Robert C, Ghiringhelli F. What is the role of cytotoxic T lymphocyte associated antigen 4 blockade in patients with metastatic melanoma? Oncologist 2009;14: Robert C, Thomas L, Bondarenko I, O'Day S, M DJ, Garbe C et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med 2011;364:
31 References Vemurafenib 1. Arkenau HT, Kefford R, Long GV. Targeting BRAF for patients with melanoma. Br J Cancer 2011;104: Capper D, Preusser M, Habel A, Sahm F, Ackermann U, Schindler G et al. Assessment of BRAF V600E mutation status by immunohistochemistry with a mutation specific monoclonal antibody. Acta Neuropathol 2011;122: Chapman PB, Hauschild A, Robert C, Haanen JB, Ascierto P, Larkin J et al. Improved survival with vemurafenib in melanoma with BRAF V600E mutation. N Engl J Med 2011;364: FlahertyKT KT, Puzanov I, KimKB KB, RibasA A, McArthur GA, SosmanJA etal al. Inhibition of mutated, activated BRAF in metastatic melanoma. N Engl J Med 2010;363: Nazarian R, Shi H, Wang Q, Kong X, Koya RC, Lee H et al. Melanomas acquire resistance to B RAF(V600E) inhibition by RTK or N RAS upregulation. Nature 2010;468: Ribas A, Kim KB, Schuchter LM, et al. BRIM 2: an open label, multicenter phase II study of vemurafenib in previousl treated patients with BRAFV600E mutationpositive melanoma. J Clin Oncol 2011; 29:Suppl:8509. abstract. 7. Vultur A, Villanueva J, Herlyn M. Targeting BRAF in advanced melanoma: a first step toward manageable disease. Clin Cancer Res 2011;17: References Other 1. Corona R, Mele A, Amini M, De Rosa G, Coppola G, Piccardi P et al. Interobserver variability on the histopathologic diagnosis of cutaneous melanoma and other pigmented skin lesions. J Clin Oncol 1996;14: Farmer ER, Gonin R, Hanna MP. Discordance in the histopathologic diagnosis of melanoma and melanocytic nevi between expert pathologists. Hum Pathol 1996;27: Greider CW, Blackburn EH. A telomeric sequence in the RNA of Tetrahymena telomerase required for telomere repeat synthesis. Nature 1989;337: Kornstein MJ, Byrne SP. The medicolegal aspect of error inpathology: a searchof jury verdicts and settlements. Arch Pathol Lab Med 2007;131: Lodha S, Saggar S, Celebi JT, Silvers DN. Discordance in the histopathologic diagnosis of difficult melanocytic neoplasms in the clinical setting. J Cutan Pathol 2008;35: Lundblad V, Szostak JW. A mutant with a defect in telomere elongation leads to senescence in yeast. Cell 1989;57: McGinnis KS, Lessin SR, Elder DE, Guerry Dt, Schuchter L, Ming M et al. Pathology review of cases presenting to a multidisciplinary pigmented lesion clinic. Arch Dermatol 2002;138:
Page 1 of 3. We suggest the following changes:
 Page 1 of 3 Loren E. Clarke, M.D. Myriad Genetic Laboratories, Inc. 320 Wakara Way, Salt Lake City, UT 84108 Phone: 801.883.3470 Email: lclarke@myriad.com Date of Request: June 2017 NCCN Guidelines Panel:
Page 1 of 3 Loren E. Clarke, M.D. Myriad Genetic Laboratories, Inc. 320 Wakara Way, Salt Lake City, UT 84108 Phone: 801.883.3470 Email: lclarke@myriad.com Date of Request: June 2017 NCCN Guidelines Panel:
Integrating Fluorescence in situ Hybridization and Genomic Array Results into the Diagnostic Workup of Melanoma
 Integrating Fluorescence in situ Hybridization and Genomic Array Results into the Diagnostic Workup of Melanoma Association for Molecular Pathology United States and Canadian Academy of Pathology Companion
Integrating Fluorescence in situ Hybridization and Genomic Array Results into the Diagnostic Workup of Melanoma Association for Molecular Pathology United States and Canadian Academy of Pathology Companion
MAPK Pathway. CGH Next Generation Sequencing. Molecular Tools in Care of Patients with Pigmented Lesions 7/20/2017
 Molecular Tools in Care of Patients with Pigmented Lesions Tammie Ferringer, MD Geisinger Medical Center, Danville, PA tferringer@geisinger.edu DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Tammie Ferringer,
Molecular Tools in Care of Patients with Pigmented Lesions Tammie Ferringer, MD Geisinger Medical Center, Danville, PA tferringer@geisinger.edu DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Tammie Ferringer,
Michael T. Tetzlaff MD, PhD
 Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Molecular Aspects of Melanocytic Neoplasia. Iwei Yeh MD, PhD University of California, San Francisco
 Molecular Aspects of Melanocytic Neoplasia Iwei Yeh MD, PhD University of California, San Francisco Thanks to: Boris Bastian Timothy McCalmont Philip LeBoit Beth Ruben Jeff North Laura Pincus Thaddeus
Molecular Aspects of Melanocytic Neoplasia Iwei Yeh MD, PhD University of California, San Francisco Thanks to: Boris Bastian Timothy McCalmont Philip LeBoit Beth Ruben Jeff North Laura Pincus Thaddeus
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors
 Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Approximately 2% of the United States population
 Differentiation of Malignant Melanoma From Benign Nevus Using a Novel Genomic Microarray With Low Specimen Requirements Wells M. Chandler, MD; Leslie R. Rowe, MS; Scott R. Florell, MD; Mona S. Jahromi,
Differentiation of Malignant Melanoma From Benign Nevus Using a Novel Genomic Microarray With Low Specimen Requirements Wells M. Chandler, MD; Leslie R. Rowe, MS; Scott R. Florell, MD; Mona S. Jahromi,
I have no relevant conflicts of interest to disclose. John T. Seykora MD PhD Departments of Dermatology & Pathology and Laboratory Medicine
 Molecular Characterization of Stage 1-3 Melanoma: Are we close to accurate prognostication and prediction? I have no relevant conflicts of interest to disclose. John T. Seykora MD PhD Departments of Dermatology
Molecular Characterization of Stage 1-3 Melanoma: Are we close to accurate prognostication and prediction? I have no relevant conflicts of interest to disclose. John T. Seykora MD PhD Departments of Dermatology
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy
 Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is:
 Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Diagnosis of melanocytic proliferations remains one of
 Update on Fluorescence In Situ Hybridization in Melanoma State of the Art Pedram Gerami, MD; Artur Zembowicz, MD, PhD N Context. Recent advances in understanding the molecular basis of melanoma have resulted
Update on Fluorescence In Situ Hybridization in Melanoma State of the Art Pedram Gerami, MD; Artur Zembowicz, MD, PhD N Context. Recent advances in understanding the molecular basis of melanoma have resulted
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
The Enigmatic Spitz Lesion
 The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
STUDY. Sensitivity of Fluorescence In Situ Hybridization for Melanoma Diagnosis Using RREB1, MYB, Cep6, and 11q13 Probes in Melanoma Subtypes
 STUDY Sensitivity of Fluorescence In Situ Hybridization for Melanoma Diagnosis Using RREB1, MYB, Cep6, and 11q13 Probes in Melanoma Subtypes Pedram Gerami, MD; Mariam Mafee, BS; Teekay Lurtsbarapa, MD;
STUDY Sensitivity of Fluorescence In Situ Hybridization for Melanoma Diagnosis Using RREB1, MYB, Cep6, and 11q13 Probes in Melanoma Subtypes Pedram Gerami, MD; Mariam Mafee, BS; Teekay Lurtsbarapa, MD;
Melanocytic lesions on Genital Skin Melanoma vs. Melanocytic Nevus, Revisited. Timothy H. McCalmont, MD University of California, San Francisco
 Melanocytic lesions on Genital Skin Melanoma vs. Melanocytic Nevus, Revisited Timothy H. McCalmont, MD, San Francisco I. IS IT BENIGN OR IS IT MALIGNANT? One of the commonest determinations we make as
Melanocytic lesions on Genital Skin Melanoma vs. Melanocytic Nevus, Revisited Timothy H. McCalmont, MD, San Francisco I. IS IT BENIGN OR IS IT MALIGNANT? One of the commonest determinations we make as
FISH as an effective diagnostic tool for the management of challenging melanocytic lesions
 RESEARCH Open Access FISH as an effective diagnostic tool for the management of challenging melanocytic lesions Mathew W Moore * and Robert Gasparini Abstract Background: The accuracy of melanoma diagnosis
RESEARCH Open Access FISH as an effective diagnostic tool for the management of challenging melanocytic lesions Mathew W Moore * and Robert Gasparini Abstract Background: The accuracy of melanoma diagnosis
Update on Genetic Testing for Melanoma
 Update on Genetic Testing for Melanoma Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania February 18, 2018 AAD
Update on Genetic Testing for Melanoma Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine Hospital of the University of Pennsylvania February 18, 2018 AAD
Normal RAS-RAF (MAPK) pathway signaling
 pathway signaling") BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
BRAF-Mutations in Melanomas L. Mazzucchelli Istituto Cantonale di Patologia, Locarno 77. Annual Meeting Swiss Society of Pathology, Lucerne 2011 Sponsored by Roche Pharma Switzerland Melanoma has increased
There is NO single Melanoma Stain. > 6000 Mutations in Melanoma. What else can be done to discriminate atypical nevi from melanoma?
 Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
6/22/2015. Original Paradigm. Correlating Histology and Molecular Findings in Melanocytic Neoplasms
 6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
Artur Zembowicz, MD, PhD; Sung-Eun Yang, MD; Antonios Kafanas, MD; Stephen R. Lyle, MD, PhD
 Correlation Between Histologic Assessment and Fluorescence In Situ Hybridization Using MelanoSITE in Evaluation of Histologically Ambiguous Melanocytic Lesions Artur Zembowicz, MD, PhD; Sung-Eun Yang,
Correlation Between Histologic Assessment and Fluorescence In Situ Hybridization Using MelanoSITE in Evaluation of Histologically Ambiguous Melanocytic Lesions Artur Zembowicz, MD, PhD; Sung-Eun Yang,
Vernon K. Sondak. Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida
 Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons
 Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons Ben J. Friedman, MD Senior Staff Physician Department of Dermatology Department of Pathology and Laboratory Medicine Henry
Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons Ben J. Friedman, MD Senior Staff Physician Department of Dermatology Department of Pathology and Laboratory Medicine Henry
Melanocytic proliferations in sundamaged
 Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
10/2/17. MELTUMP, SAMPUS, AST.An Algorithmic Approach to Challenging (Often Borderline) Melanocytic Tumors. An Introduction to SNP Arrays
 Melanocytic Tumors. An Introduction to SNP Arrays") MELTUMP, SAMPUS, AST.An Algorithmic Approach to Challenging (Often ) Melanocytic Tumors An Introduction to SNP Arrays Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (11:45-12:30pm, Saturday, 23-09-17) Why do we
MELTUMP, SAMPUS, AST.An Algorithmic Approach to Challenging (Often ) Melanocytic Tumors An Introduction to SNP Arrays Rajiv M. Patel, M.D. RCPA NZ ASM 2017 (11:45-12:30pm, Saturday, 23-09-17) Why do we
Patricia Chevez-Barrrios AAOOP-USCAP /12/2016
 Biomarkers in Ocular Melanoma Patricia Chévez-Barrios, MD Pathology and Genomic Medicine, Houston Methodist Hospital Professor of Pathology and Laboratory Medicine and Ophthalmology, Weill Cornell Medical
Biomarkers in Ocular Melanoma Patricia Chévez-Barrios, MD Pathology and Genomic Medicine, Houston Methodist Hospital Professor of Pathology and Laboratory Medicine and Ophthalmology, Weill Cornell Medical
21/07/2017. The «gray zone» of diagnosis is visible. Nevus Atypical nevus Melanoma. Melanoma ex-blue nevus
 Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
> 6000 Mutations in Melanoma. Tests That Cay Be Employed. FISH for Additions/Deletions. Comparative Genomic Hybridization
 Winter Clinical 2017: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of Colorado
Winter Clinical 2017: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of Colorado
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove)
") Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble at bay
 Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
The Pathology of Neoplasia Part II
 The Pathology of Neoplasia Part II February 2018 PAUL BOGNER, MD A S S O C I A T E P R O F E S S O R O F O N C O L O G Y P A T H O L O G Y A N D D E R M A T O L O G Y Clinical goals of cancer pathology
The Pathology of Neoplasia Part II February 2018 PAUL BOGNER, MD A S S O C I A T E P R O F E S S O R O F O N C O L O G Y P A T H O L O G Y A N D D E R M A T O L O G Y Clinical goals of cancer pathology
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
117 Applying Risk Management Principles to QA in Surgical Pathology: From Principles to Practice. Gregory Flynn MD
 117 Applying Risk Management Principles to QA in Surgical Pathology: From Principles to Practice Gregory Flynn MD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe,
117 Applying Risk Management Principles to QA in Surgical Pathology: From Principles to Practice Gregory Flynn MD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe,
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Which melanoma patients benefit from genetic testing?
 Which melanoma patients benefit from genetic testing? Michael A. Marchetti, MD Assistant Attending, Dermatology Service Memorial Sloan Kettering Cancer Center American Academy of Dermatology Annual Meeting
Which melanoma patients benefit from genetic testing? Michael A. Marchetti, MD Assistant Attending, Dermatology Service Memorial Sloan Kettering Cancer Center American Academy of Dermatology Annual Meeting
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
A diagnostic algorithm for atypical spitzoid tumors: guidelines for immunohistochemical and molecular assessment
 Modern Pathology (2016), 1 15 2016 USCAP, Inc All rights reserved 0893-3952/16 $32.00 1 A diagnostic algorithm for atypical spitzoid tumors: guidelines for immunohistochemical and molecular assessment
Modern Pathology (2016), 1 15 2016 USCAP, Inc All rights reserved 0893-3952/16 $32.00 1 A diagnostic algorithm for atypical spitzoid tumors: guidelines for immunohistochemical and molecular assessment
Corporate Medical Policy
 Corporate Medical Policy BRAF Gene Variant Testing to Select Melanoma or Glioma Patients File Name: Origination: Last CAP Review: Next CAP Review: Last Review: braf_gene_variant_testing_to_select_melanoma_or_glioma_patients_for_targeted_
Corporate Medical Policy BRAF Gene Variant Testing to Select Melanoma or Glioma Patients File Name: Origination: Last CAP Review: Next CAP Review: Last Review: braf_gene_variant_testing_to_select_melanoma_or_glioma_patients_for_targeted_
Conflict of Interest 9/2/2014. Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma
 Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
Pathogenesis and Comparison of Atypical Spitz Nevi vs Benign Spitz, and Childhood Melanoma Martin C. Mihm Jr., M.D., F.A.C.P. Harvard Medical School Brigham and Women s Hospital Dana Farber Cancer Center
One Moment Please. Skin Cancer. Today s Webcast Friday, 09/09/11, Noon. David Carr, MD
 One Moment Please One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast Friday, 09/09/11, Noon 1 New Features Enlarge Slides Links Chapters Polling Use the email function to let
One Moment Please One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast Friday, 09/09/11, Noon 1 New Features Enlarge Slides Links Chapters Polling Use the email function to let
THE SPITZ NEVUS OFTEN POSES
 OBSERVATION ONLINE FIRST Melanoma Mimic A Case of Multiple Pagetoid Spitz Nevi KaLynne Harris, MD; Scott R. Florell, MD; Jason Papenfuss, MD; Wendy Kohlmann, MS, CGC; Mona Jahromi, BS; Joshua D. Schiffman,
OBSERVATION ONLINE FIRST Melanoma Mimic A Case of Multiple Pagetoid Spitz Nevi KaLynne Harris, MD; Scott R. Florell, MD; Jason Papenfuss, MD; Wendy Kohlmann, MS, CGC; Mona Jahromi, BS; Joshua D. Schiffman,
Case Report Comparative genomic hybridization in a case of melanoma that loses expression of S100, HMB45, Melan A and tyrosinase in metastasis
 Int J Clin Exp Pathol 2014;7(1):468-473 www.ijcep.com /ISSN:1936-2625/IJCEP1311022 Case Report Comparative genomic hybridization in a case of melanoma that loses expression of S100, HMB45, Melan A and
Int J Clin Exp Pathol 2014;7(1):468-473 www.ijcep.com /ISSN:1936-2625/IJCEP1311022 Case Report Comparative genomic hybridization in a case of melanoma that loses expression of S100, HMB45, Melan A and
Reviewers' comments: Reviewer #1 (Remarks to the Author):
:") Reviewers' comments: Reviewer #1 (Remarks to the Author): In this study the authors analysed 18 deep penetrating nevi for oncogenic genomic changes (single nucleotide variations, insertions/deletions,
Reviewers' comments: Reviewer #1 (Remarks to the Author): In this study the authors analysed 18 deep penetrating nevi for oncogenic genomic changes (single nucleotide variations, insertions/deletions,
BRAF Gene Mutation Testing To Select Melanoma Patients for BRAF Inhibitor Targeted Therapy. Original Policy Date
 MP 2.04.66 BRAF Gene Mutation Testing To Select Melanoma Patients for BRAF Inhibitor Targeted Therapy Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date
MP 2.04.66 BRAF Gene Mutation Testing To Select Melanoma Patients for BRAF Inhibitor Targeted Therapy Medical Policy Section Medicine Issue 12:2013 Original Policy Date 12:2013 Last Review Status/Date
Conflict of Interest Disclosure
 "NRAS mutation status in advanced melanoma: how much does this really matter to prognosis and therapy?" John Jakob, MD, PhD Department of Melanoma Medical Oncology, The University of Texas M.D. Anderson
"NRAS mutation status in advanced melanoma: how much does this really matter to prognosis and therapy?" John Jakob, MD, PhD Department of Melanoma Medical Oncology, The University of Texas M.D. Anderson
Associate Clinical Professor of Dermatology MUSC
 Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Re-excision of Moderately Dysplastic Nevi: Should we or shouldn t we? John C. Maize, Jr, M.D. Dermatologist and Dermatopathologist Trident Dermatology, Charleston SC Associate Clinical Professor of Dermatology
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is:
 Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Female 18. Deeply pigmented lesion on trunk.?warty naevus?seborrhoeic keratosis?malignant melanoma. The best diagnosis is: A. deep penetrating naevus B. naevoid malignant melanoma C. pigment synthesising
Corporate Medical Policy
 Corporate Medical Policy BRAF Gene Mutation Testing to Select Melanoma or Glioma Patients File Name: Origination: Last CAP Review: Next CAP Review: Last Review: braf_gene_mutation_testing_to_select_melanoma_or_glioma_patients_for_targeted_
Corporate Medical Policy BRAF Gene Mutation Testing to Select Melanoma or Glioma Patients File Name: Origination: Last CAP Review: Next CAP Review: Last Review: braf_gene_mutation_testing_to_select_melanoma_or_glioma_patients_for_targeted_
Time to reconsider Spitzoid neoplasms?
 DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Time to reconsider Spitzoid neoplasms? Carmelo Urso 1 1 Department of Anatomic Pathology, Dermatopathology Section, SM Annunziata Hospital, AUSL Toscana
DERMATOLOGY PRACTICAL & CONCEPTUAL www.derm101.com Time to reconsider Spitzoid neoplasms? Carmelo Urso 1 1 Department of Anatomic Pathology, Dermatopathology Section, SM Annunziata Hospital, AUSL Toscana
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the
 Histopathology (4x) shows a domed papule with melanocytes extending into the") Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the deep dermis. (b) The melanocytes demonstrate abundant
Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the deep dermis. (b) The melanocytes demonstrate abundant
Enlarge Slides. One Moment Please. Skin Cancer. Thomas Olencki, DO David Carr, MD. Today s Webcast Friday, 09/09/11, Noon
 New Features Enlarge Slides Links One Moment Please Chapters Polling Use the email function to let us know what you think One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast
New Features Enlarge Slides Links One Moment Please Chapters Polling Use the email function to let us know what you think One Moment Please Skin Cancer Thomas Olencki, DO David Carr, MD Today s Webcast
Disclosure Information. Lecture Outline. Lecture Outline. Introduction. Molecular Pathology of Cutaneous Melanoma. Nothing to disclose
 Molecular Pathology of Cutaneous Melanoma Disclosure Information Nothing to disclose Jonathan L. Curry, MD Assistant Professor of Pathology and Dermatology University of Texas-MD Anderson Cancer Center
Molecular Pathology of Cutaneous Melanoma Disclosure Information Nothing to disclose Jonathan L. Curry, MD Assistant Professor of Pathology and Dermatology University of Texas-MD Anderson Cancer Center
Melanocytic Tumours. Molecular Biology 02/06/2015. Cutaneous Melanocytic Tumours Introduction. Thomas Brenn. Intermediate Malignancy
 Cutaneous Melanocytic Tumours Introduction Melanocytic Tumours: Update on Epidemiology and Molecular Biology Thomas Brenn Wide clinical and morphological spectrum Ranging from benign naevi to melanoma
Cutaneous Melanocytic Tumours Introduction Melanocytic Tumours: Update on Epidemiology and Molecular Biology Thomas Brenn Wide clinical and morphological spectrum Ranging from benign naevi to melanoma
Management of pediatric melanocytic lesions
 Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 2. Variations on the acquired nevus 3. Dermal melanocytosis
 Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Diagnoses of Cases 1. Lentigo, other melanosis and the acquired nevus 1 1A. Lentigo simplex 4 1B. Psoralens and ultraviolet A (PUVA) lentigo 6 1C. Solar lentigo 8 1D. Café au lait macule 10 1E. Ink-spot
Disclosure Declaration Clinical Utility of Molecular Testing in Malignant Melanoma
 Disclosure Declaration Clinical Utility of Molecular Testing in Malignant Melanoma No Conflict of Interest Allison Cushman-Vokoun, M.D., Ph.D Associate Professor, Department of Pathology and Microbiology
Disclosure Declaration Clinical Utility of Molecular Testing in Malignant Melanoma No Conflict of Interest Allison Cushman-Vokoun, M.D., Ph.D Associate Professor, Department of Pathology and Microbiology
Melanoma 6/2/2011. Classification and Prognosis. Melanoma Statistics. American Cancer Society
 University of Pennsylvania, Ben Franklin in front of Charles Addams Building Melanoma Classification and Prognosis Emphasizing Pathology & History David Elder University of Pennsylvania Melanoma Statistics
University of Pennsylvania, Ben Franklin in front of Charles Addams Building Melanoma Classification and Prognosis Emphasizing Pathology & History David Elder University of Pennsylvania Melanoma Statistics
78 The Power of Peripheral Blood Smears-Apparent Diagnostic Clues (Part 1) Gene Gulati PhD, SH(ASCP)
 Gene Gulati PhD, SH(ASCP)") 78 The Power of Peripheral Blood Smears-Apparent Diagnostic Clues (Part 1) Gene Gulati PhD, SH(ASCP) 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste. 1600 Chicago,
78 The Power of Peripheral Blood Smears-Apparent Diagnostic Clues (Part 1) Gene Gulati PhD, SH(ASCP) 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY FOR CLINICAL PATHOLOGY 33 W. Monroe, Ste. 1600 Chicago,
Copy Number Gains in 11q13 and 8q34 Are Highly Linked to Prognosis in Cutaneous Malignant Melanoma
 The Journal of Molecular Diagnostics, Vol. 13, No. 3, May 2011 Copyright 2011 American Society for Investigative Pathology and the Association for Molecular Pathology. Published by Elsevier Inc. All rights
The Journal of Molecular Diagnostics, Vol. 13, No. 3, May 2011 Copyright 2011 American Society for Investigative Pathology and the Association for Molecular Pathology. Published by Elsevier Inc. All rights
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more
 Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Benign and malignant epithelial lesions: Seborrheic keratosis: A common benign pigmented epidermal tumor occur in middle-aged or older persons more common on the trunk; but extremities, head and neck are
Simulators of melanoma
 Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Simulators of melanoma Philip E. LeBoit, M.D. Depts. of Pathology and Dermatology University of California, San Francisco Simulators of melanoma Simulators of melanoma in situ Melanocytic Non-melanocytic
Rapid BRAF mutation detection in melanoma patients by immunohistochemistry
 http://dx.doi.org/10.17202/juso.2017.4.1 Journal of Universal Science Vol 4(1): 1-5, 2017 Rapid BRAF mutation detection in melanoma patients by immunohistochemistry László FÜLÖP 1, Katalin GÖTZER 1, Erzsébet
http://dx.doi.org/10.17202/juso.2017.4.1 Journal of Universal Science Vol 4(1): 1-5, 2017 Rapid BRAF mutation detection in melanoma patients by immunohistochemistry László FÜLÖP 1, Katalin GÖTZER 1, Erzsébet
Pathology of the skin. 2nd Department of Pathology, Semmelweis University
 Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Pathology of the skin 2nd Department of Pathology, Semmelweis University Histology of the skin Epidermis: Stratum corneum Stratum granulosum Stratum spinosum Stratum basale Dermis: papillary and reticular
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant Melanoma of The Skin - Still A Medical Conundrum?
 SCENIHR Public hearing on the Preliminary Opinion: 'Biological effects of ultraviolet radiation relevant to health with particular reference to sunbeds for cosmetic purposes. Luxembourg, April 12 th, 2016
SCENIHR Public hearing on the Preliminary Opinion: 'Biological effects of ultraviolet radiation relevant to health with particular reference to sunbeds for cosmetic purposes. Luxembourg, April 12 th, 2016
S everal morphological features are frequently used in the
 1194 ORIGINAL ARTICLE Interobserver reproducibility of histological features in cutaneous malignant melanoma C Urso, F Rongioletti, D Innocenzi, C Saieva, D Batolo, S Chimenti, R Filotico, R Gianotti,
1194 ORIGINAL ARTICLE Interobserver reproducibility of histological features in cutaneous malignant melanoma C Urso, F Rongioletti, D Innocenzi, C Saieva, D Batolo, S Chimenti, R Filotico, R Gianotti,
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Rare melanoma: Are the options improving? Dr Neil Steven Consultant in Medical Oncology University Hospital Birmingham University of Birmingham
 Rare melanoma: Are the options improving? Dr Neil Steven Consultant in Medical Oncology University Hospital Birmingham University of Birmingham Classifying melanoma Melanoma (site of origin, thickness,
Rare melanoma: Are the options improving? Dr Neil Steven Consultant in Medical Oncology University Hospital Birmingham University of Birmingham Classifying melanoma Melanoma (site of origin, thickness,
Integrating Fluorescence in situ Hybridization and Genomic Array Results into the Diagnostic Workup of Melanoma
 Integrating Fluorescence in situ Hybridization and Genomic Array Results into the Diagnostic Workup of Melanoma Association for Molecular Pathology United States and Canadian Academy of Pathology Companion
Integrating Fluorescence in situ Hybridization and Genomic Array Results into the Diagnostic Workup of Melanoma Association for Molecular Pathology United States and Canadian Academy of Pathology Companion
BRAF, NRAS and HRAS mutations in spitzoid tumours and their possible pathogenetic significance
 DERMATOPATHOLOGY BJD British Journal of Dermatology BRAF, NRAS and HRAS mutations in spitzoid tumours and their possible pathogenetic significance P.D. Da Forno, J.H. Pringle,* A. Fletcher, M. Bamford,
DERMATOPATHOLOGY BJD British Journal of Dermatology BRAF, NRAS and HRAS mutations in spitzoid tumours and their possible pathogenetic significance P.D. Da Forno, J.H. Pringle,* A. Fletcher, M. Bamford,
Difficulties in the diagnosis of spitzoid melanocytic lesions
 For reprint orders, please contact reprints@expert-reviews.com Difficulties in the diagnosis of spitzoid melanocytic lesions Expert Rev. Dermatol. 5(5), 549 560 (2010) Stephen H Olsen 1, Rajiv M Patel
For reprint orders, please contact reprints@expert-reviews.com Difficulties in the diagnosis of spitzoid melanocytic lesions Expert Rev. Dermatol. 5(5), 549 560 (2010) Stephen H Olsen 1, Rajiv M Patel
5/21/2018. Disclosures. Consulting: Myriad Genetics SciBase. Superficial Atypical Melanocytic Proliferations. SSM, LMM and (some of) their Simulants
 their Simulants") Disclosures Consulting: Myriad Genetics SciBase Superficial Atypical Melanocytic Proliferations SSM, LMM and (some of) their Simulants 1 Melanomas and Nevi. Nevi are important mainly in relation to melanoma
Disclosures Consulting: Myriad Genetics SciBase Superficial Atypical Melanocytic Proliferations SSM, LMM and (some of) their Simulants 1 Melanomas and Nevi. Nevi are important mainly in relation to melanoma
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Clinical validation of a gene expression signature that differentiates benign nevi from malignant melanoma
 J Cutan Pathol 215: 42: 244 252 doi: 1.1111/cup.12475 John Wiley & Sons. Printed in Singapore Journal of Cutaneous Pathology Clinical validation of a gene expression signature that differentiates benign
J Cutan Pathol 215: 42: 244 252 doi: 1.1111/cup.12475 John Wiley & Sons. Printed in Singapore Journal of Cutaneous Pathology Clinical validation of a gene expression signature that differentiates benign
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
BRAF Mutation Analysis
 Last Review Date: October 13, 2017 Number: MG.MM.LA.38aC Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Last Review Date: October 13, 2017 Number: MG.MM.LA.38aC Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Conflicts of Interest
 Challenging Melanocytic Lesions Carlos N. Prieto-Granada M.D. Assistant Professor University of Alabama at Birmingham (UAB) Department of Pathology 2017 AAD Annual Meeting 3/2/17 - Orlando, FL None Conflicts
Challenging Melanocytic Lesions Carlos N. Prieto-Granada M.D. Assistant Professor University of Alabama at Birmingham (UAB) Department of Pathology 2017 AAD Annual Meeting 3/2/17 - Orlando, FL None Conflicts
Response and resistance to BRAF inhibitors in melanoma
 Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
Response and resistance to BRAF inhibitors in melanoma Keith T. Flaherty, M.D. Massachusetts General Hospital Cancer Center Disclosures Roche/Genentech: consultant GlaxoSmithKline: consultant BRAF mutations
Epidemiology. Objectives 8/28/2017
 Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Multiple Primary Melanoma in a Thai Male: A Case Report
 Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Case Report Multiple Primary Melanoma in a Thai Male: A Case Report J Med Assoc Thai 2014; 97 (Suppl. 2): S234-S238 Full text. e-journal: http://www.jmatonline.com Kittisak Payapvipapong MD*, Pinyapat
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT
 Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
Maligna Melanoma and Atypical Fibroxanthoma: An Unusual Collision Tumour G Türkcü 1, A Keleş 1, U Alabalık 1, D Uçmak 2, H Büyükbayram 1 ABSTRACT Two different neoplasia in the same biopsy material called
K Blessing, J J H Grant, D S A Sanders, M M Kennedy, A Husain, P Coburn
 J Clin Pathol 2000;53:591 595 591 Papers Pathology, Aberdeen University, Foresterhill, Aberdeen AB25 2ZD, K Blessing Pathology, Birmingham University, Birmingham B15 2TT, D S A Sanders Pathology, Heartlands
J Clin Pathol 2000;53:591 595 591 Papers Pathology, Aberdeen University, Foresterhill, Aberdeen AB25 2ZD, K Blessing Pathology, Birmingham University, Birmingham B15 2TT, D S A Sanders Pathology, Heartlands
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Metastatic Melanoma. Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds
 Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Metastatic Melanoma Cynthia Kwong February 16, 2017 SUNY Downstate Medical Center Department of Surgery Grand Rounds Case Presentation 77 year old male with previous history of scalp melanoma and thyroid
Advances in Melanoma
 Advances in Melanoma The Blue, the Black and the Ugly 1 Outline History of Melanoma Why be concerned? Skin cancer updates What s old? What s new (and why are Skin Tumor Group med oncs excited again)? What
Advances in Melanoma The Blue, the Black and the Ugly 1 Outline History of Melanoma Why be concerned? Skin cancer updates What s old? What s new (and why are Skin Tumor Group med oncs excited again)? What
Pathological diagnosis of melanocytic tumours: clues and pitfalls # Richard A. Scolyer 1,2,3* and Stanley W. McCarthy 1,2,3
 Pathological diagnosis of melanocytic tumours: clues and pitfalls # Richard A. Scolyer 1,2,3* and Stanley W. McCarthy 1,2,3 1 Tissue Pathology and Diagnostic Oncology, Royal Prince Alfred Hospital, Sydney,
Pathological diagnosis of melanocytic tumours: clues and pitfalls # Richard A. Scolyer 1,2,3* and Stanley W. McCarthy 1,2,3 1 Tissue Pathology and Diagnostic Oncology, Royal Prince Alfred Hospital, Sydney,
Melanoma: Early Detection and Therapeutic Progress
 Melanoma: Early Detection and Therapeutic Progress David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Surgery Thanks to my collaborators, mentors and patients May 19, 2017 Disclosures:
Melanoma: Early Detection and Therapeutic Progress David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Surgery Thanks to my collaborators, mentors and patients May 19, 2017 Disclosures:
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Dr. dr. Primariadewi R, SpPA(K)
") Curriculum Vitae Dr. dr. Primariadewi R, SpPA(K) Education : Medical Doctor from UKRIDA Doctoral Degree from Faculty of Medicine University of Indonesia Pathologist Specialist and Consultant from Faculty
Curriculum Vitae Dr. dr. Primariadewi R, SpPA(K) Education : Medical Doctor from UKRIDA Doctoral Degree from Faculty of Medicine University of Indonesia Pathologist Specialist and Consultant from Faculty
Financial disclosures
 Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Mesenchymal Neoplasms with Melanocytic Differentiation By Konstantinos Linos MD, FCAP, FASDP Bone, Soft Tissue and Dermatopathology Assistant Professor of Pathology Dartmouth-Hitchcock Medical Center Geisel
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New Targeted Therapies in Melanoma
 Vemurafenib and ipilimumab have improved overall survival in patients with metastatic melanoma. Tenzin Norbu Lama. Returning Home (detail). New Targeted Therapies in Melanoma Ragini R. Kudchadkar, MD,
Vemurafenib and ipilimumab have improved overall survival in patients with metastatic melanoma. Tenzin Norbu Lama. Returning Home (detail). New Targeted Therapies in Melanoma Ragini R. Kudchadkar, MD,
A View to the Future: The Development of Targeted Therapy for Melanoma. Michael Davies, M.D., Ph.D.
 A View to the Future: Science to Survivorship Symposium September 26, 2009 The Development of Targeted Therapy for Melanoma Michael Davies, M.D., Ph.D. Assistant Professor, Melanoma Medical Oncology How
A View to the Future: Science to Survivorship Symposium September 26, 2009 The Development of Targeted Therapy for Melanoma Michael Davies, M.D., Ph.D. Assistant Professor, Melanoma Medical Oncology How