6/22/2015. Original Paradigm. Correlating Histology and Molecular Findings in Melanocytic Neoplasms
|
|
|
- Dustin O’Connor’
- 5 years ago
- Views:
Transcription




1 6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant to Abbott Molecular, Neogenomics, Myriad Genomics, and Derm Tech Int. Clonal Chromosomal Aberrations Original Paradigm Melanoma Nevi 95% Only 20% of Spitz Nevi Common Gains 6p, 7q, 17q, Isolated Gain 20q, 4q,8q, in 11p 1q, 11q Common Deletions 9p, 10, 21q Melanoma Cohort 3 (n=169) Melanocytic nevi n Common Nevus 25 Dysplastic Nevus 42 Spitz Nevus 14 Nevus on Acral Skin 3 Blue Nevus 2 86 Sensitivity=86.7% Specificity=95.4% Melanomas n Head & Neck 30 Trunk 27 Extremity 23 Glabrous Skin
2 Slide 1 6 1)start by saying what you want to go over a)briefly review CGH and some of the early studies on melanoma b)review the original study and development of the FISH assay c)get into the newer FISH probes Pedram Gerami, 10/19/2011
Inclusion criteria: Diagnosis of AST 5 years follow up no adverse event or tumor spread beyond a sentinel lymph node or less than 5 years of follow up if there")
Age 2)Sex 3)Anatomic site 4)Breslow depth 5)Mitotic count 6)Clark Level 7)Ulceration status 8)Presence or")
3 Multi-center collaborative study on Spitz tumors involving Northwestern Univ, UCSF, Univ of Michigan, MD Anderson, Memorial Sloan Kettering and Sydney Melanoma Unit Study Design 1)Multi-center retrospective case controlled study 2)Inclusion criteria: Diagnosis of AST 5 years follow up no adverse event or tumor spread beyond a sentinel lymph node or less than 5 years of follow up if there was evidence of tumor spread beyond the sentinel lymph node 3)FISH evaluation with probes targeting 6p25, 6q23, Cep 6, 11q13, 9p21, and 8q24 was performed on all cases blinded to the clinical outcome Data Collection and Analysis The following data points were collected for each case: 1)Age 2)Sex 3)Anatomic site 4)Breslow depth 5)Mitotic count 6)Clark Level 7)Ulceration status 8)Presence or Absence of kamino bodies 9)Expansile nodular growth 10)Epidermal Consumption 11)Epithelioid versus spindle morphology 12)Complete clinical follow up including sentinel node status 13)FISH data Summary of clinical, histological, and molecular data by clinical stage Clinical N Avera Sex Average Ulceratio Average Average % Patients Average Stage ge n with Ratio Breslow Mitotic Clark FU Time Age (M:F:NA) Status (Y: Positive (months) (mm) Rate Level N) (Yrs) (/mm 2 ) FISH M: 31F: 2.3 7Y: 57N NA 6 1a 13 1b 45 1x M: 4 F: 1NA 3.2 4Y: 4N M: 1F 6.6 1Y: 2N *NA- not available Frequency of FISH results for good (1a,1b,1x) vs. bad (2,4) outcome Spitzoid patients Patient outcome FISH result Good (1a,1b,1x) Bad (2,4) Fisher s exact test 6P Positive Negative q Positive Negative P Cep 6 Positive Negative q Positive Negative P Positive 3 9 < Negative q Positive Negative FISH outcome FISH old probe set Positive < Negative 49 0 Positive Negative 49 5 FISH new probe set Cytogenetic risk Positive 9 11 < Negative 55 0 Low risk 55 0 < Intermediate 6 2 High risk 3 9 2
4 Comparison of the frequency of each chromosomal copy number aberration by outcome groups Group 1 vs. 2 and 4 Group 1 and 2 vs. 4 FISH (# of positives / Group Group Fisher Group Group Fisher # of negatives ) exact test exact 1a/1b/1x 2/4 1a/1b/1x 4 test /2 6P25 8/56 5/ /61 2/ q23 8/56 1/ /63 0/ P/Cep 6 2/62 1/ /70 1/ q13 8/56 5/ /61 2/ P21 3/61 9/2 < /63 3/ q24 1/63 1/ /71 1/ FISH + probe set 1 or 15/49 11/0 < /49 3/ * FISH + probe set 1 ** 15/49 6/ /53 2/ FISH + probe set 2 9/55 11/0 < /55 3/ *** Cytogenetic risk**** 55/6/3 0/2/9 < /8/9 0/0/ ( # of low/ # of intermediate/# of high) Multivariate Analysis Comparing Variables for Group 1 versus Group 2 through 4 Variable Estimate Odds Ratio 95% CI for OR p-value Mitotic F9P (+ vs. -) Footnote: backward elimination method was used to derive the final multivariable models < Multivariate Analysis Comparing Variables for Group 1 and 2 versus Group 4 Variable Estimate Odds Ratio 95% CI for OR p-value F9P (+ vs. -) Footnote: backward elimination method was used to derive the final multivariable models 3
5 4





6 5
9 of 11 cases")
 4 of 9")





7 Recurring Themes Among ASTs With Ree Aggressive Clinical Course : 1)9 of 11 cases with disease progression beyond the sentinel had homozygous 9p21 deletions 2) 4 of 9 patients with ASTs with homozygous 9p21 deletion developed recurrent in transit metastasis in the skin in addition to sentinel and non-sentinel lymph node involvement all of whom are still alive. One patient with up to 8 years of follow up. 3)Distant metastasis and death from disease from ASTs uncommon but when it does happen most cases likely to have homozygous 9p21 deletion and likely to occur with a more protracted course compared to conventional melanomas 36 6



8


 1 17 F Positive 12 3 3 M Not available,")



9 Heirarchy of Risk for Distant Metastasis in Melanocytic Neoplasms with Spitzoid Morphology Conventional Melanoma Most taggressive Spitzoid Melanoma with Homozygous 9p21 Deletion Intermediate 43 ASTs with no evidence of copy number aberrations Low Risk ASTs with 6q23 Deletion Low Risk ASTs with 3p21 Deletion/BAPomas Low Risk ASTs with 11p gains Low Risk Clinical Follow up for atypical Spitz tumors with 6q23 deletions Case # Age Sex Sentinel node biopsy result Follow up time (mo) 1 17 F Positive M Not available, Doing well 3 with no evidence of disease on follow up 5 5 F Not done F Not available, Doing well 18 with no evidence of disease on follow up 8 7 M Not available, Doing well with no evidence of disease on follow up M Positive F Positive NA Not done F Positive NA Positive F Negative F Not done F Negative F Not available, Doing well 3 with no evidence of disease on follow up 21 4 F Negative M Positive M Negative M Negative 3 A B C D E F 8


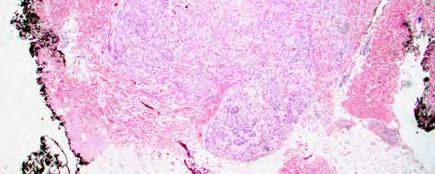
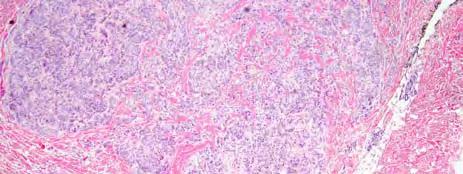
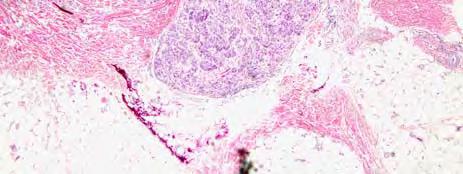
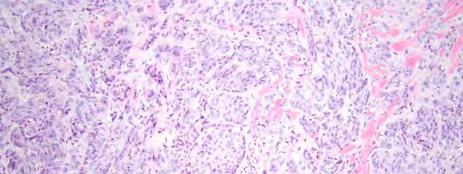
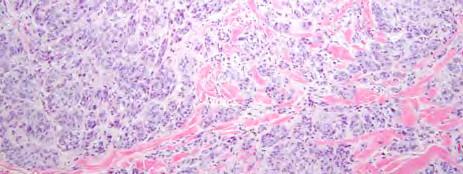
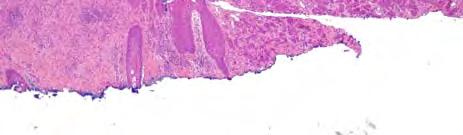
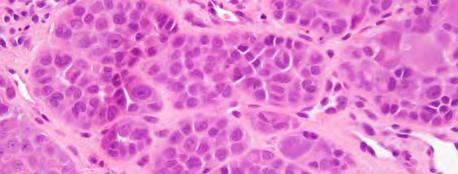
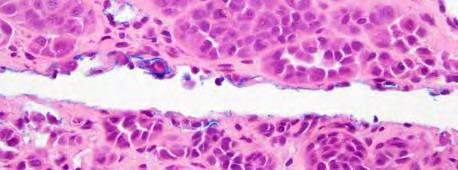
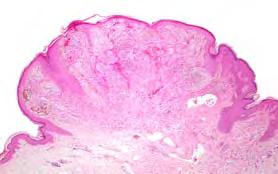
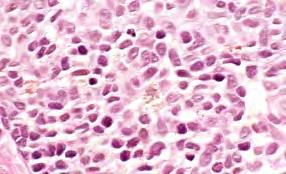
10 8 year old male with non-changing pink papule 9









11 Chromosomal Aberrations New Paradigm Melanoma Common Gains 6p, 7q, 17q, 20q, 4q,8q, 1q, 11q Spitz tumors 95% Chimeric Fusion Proteins: Ros, AlK, NTRK1, BRAF, RET Isolated Gain in 11p, can havae gains in 7q Common Deletions 9p, 10, 21q 3p21, 6q23, heterozygous loss of 9p21 Change in diameter from 3 to 5 mm in 3 month period 10

 Sentinel node positive (41 events) Where we started:")

 Class 2 (high risk) Adopted by")


12 Molecular Assays for Staging Melanoma MSLT-1: Twice as many node-negative patients died compared to node-positive Initial Report 2006 Final Report 2014 Sentinel node negative (83 events) Sentinel node positive (41 events) Where we started: Gene expression profiling in uveal melanoma 15-gene expression profile test Prospective clinical validation study 1 Strong separation of metastatic risk by class % metastasis free p< Months Class 1 (low risk) Class 2 (high risk) Adopted by >95% of ocular oncologists as standard of care Achieved a market penetration of 70% Transformed care by enabling personalized treatment planning 2 Morton, N Engl J Med, 2006; Morton, N Engl J Med, Onken, 2012, Ophthalmology 2 Aaberg, 2014, Clinical Ophthalmology 66 11

 Age, median yrs (range) 61 (23-89) 58 (18-94) Follow-up, median yrs (range) 4.9 (0.0-13.7) 5.7 (0.0-11.")
 1mm 46 (28%) 45 (43%) > 1mm 101 (62%) 58 (56%) Mitotic Index 1/mm 2 43 (26%) 29 (28%) > 1/mm 2 82 (50%) 53 (51%) Ulceration Absent 104 (63%) 65 (63%) Present 46 (28%) 28 (27%) Growth Pattern")

13 Cellular functions represented in GEP signature Migration/chemotaxis/ metastasis Chemokine/secreted molecules Gap junction/cellular adhesion CXCL14 SPP1 CLCA2 S100A9 S100A8 CCL14 MGP SPP1 GJA1 DSC1 PPL Differentiation/ proliferation Cell surface receptors Structural proteins CRABP2 SPRRIB BTG1 TACST D2 CLCA2 ROBO1 MGP SPP1 CST6 Lymphocytic invasion LTA4H Angiogenesis regulator CXCL14 Transcription factor TRIM29 Extracellular functions KRT6B KRT14 67 Gerami, Clin Cancer Res 2013 Validation Study #1: Background demographics Characteristics Training Set (n = 164) Validation Set (n = 104) Age, median yrs (range) 61 (23-89) 58 (18-94) Follow-up, median yrs (range) 4.9 ( ) 5.7 ( ) AJCC Stage n (%) n (%) 0 15 (9%) 0 (0%) I 63 (38%) 56 (54%) II 67 (41%) 34 (33%) III 18 (11%) 12 (11%) IV 1 (1%) 2 (2%) Breslow Thickness Median mm (range) 1.86 ( ) 1.4 ( ) 1mm 46 (28%) 45 (43%) > 1mm 101 (62%) 58 (56%) Mitotic Index 1/mm 2 43 (26%) 29 (28%) > 1/mm 2 82 (50%) 53 (51%) Ulceration Absent 104 (63%) 65 (63%) Present 46 (28%) 28 (27%) Growth Pattern Superficial spreading 75 (46%) 56 (54%) Nodular 47 (29%) 25 (24%) Desmoplastic/lentigo maligna/ acral lentiginous 25 (15%) 10 (10%) Gerami, Clin Cancer Res 2015 Censor date: May GEP Accuracy: Disease-free survival prediction all cases n=164 Training Set n=104 p< yr DFS Class 1 = 91% Class 2 = 25% ROC = Accuracy = 83% Sensitivity = 85% Validation Set n=104 5 yr DFS Class 1 = 97% Class 2 = 31% ROC = Accuracy = 86% Sensitivity = 89% GEP is an independent predictor of metastasis for Stage I and II melanoma Cox regression analysis comparing GEP to commonly assessed predictive factors revealed: GEP is a stronger predictor of metastatic recurrence than AJCC stage in multivariate analysis: HR 95% CI p-value AJCC GEP test GEP is also independent of Breslow s thickness, ulceration, mitosis and age Gerami, Clin Cancer Res 2015 Censor Date: May, Gerami, Clin Cancer Res 2015 Censor date: May, Validation Study #2: Baseline Demographics (n=217) SLNB positive SLNB negative Characteristics (n=58) (n=159) Age, median years (range) 57 (23-94) 63 (31-89) Time to metastasis, median years (range) 1.0 (0-7.6) 1.8 (0-8.7) Follow-up in cases without metastatic event, median years (range) 2.5 ( ) 6.1 (0-13.7) Regional plus distant metastasis (n) Distant metastasis only (n) AJCC Stage (n) I n/a 46 II n/a 112 III 58 0 IV n/a 1 Breslow Thickness Median mm (range) 4.0 (0.8-16) 2.3 (0.4-14) < 1mm 4 27 > 1mm Mitotic Index (n) < 1/mm > 1/mm Ulceration (n) absent present Gerami, JAAD in press 2015 Censor date: May
 SLN Results GEP Results")





14 SLNB Status Disease-Free, Distant Metastasis-free and Overall Survival SLNB OR GEP Prognostic Prediction DFS DMFS OS SLNB vs. GEP 1 st and 2 nd Validation Studies with SLNB procedure Patients with SLN Procedure (n=217) SLN Results GEP Results SLN positive = 58 SLN negative = 159 Class 2 = 141 Class 1 = 76 Met = 37 Met = 70 Met = 91 Met = 16 GEP Class Non = 21 Non = 89 Non = 50 Non = 60 PPV = 64% NPV = 56% PPV = 65% NPV = 79% DFS = Disease Free Survival; DMFS = Distant Metastasis-Free Survival; OS = Overall Survival Gerami, JAAD in press 2015 Censor date: May Disease-Free, Distant Metastasis-free and Overall Survival SLNB AND GEP Prognostic Prediction GEP Prognostic Data Improves Prediction Over SLNB Negative Status for Overall Survival DFS Class 1/SLN Class 1/SLN+ Class 2/SLN Class 2/SLN+ DMFS Class 1/SLN Class 1/SLN+ Class 2/SLN Class 2/SLN+ OS Class 1/SLN Class 1/SLN+ Class 2/SLN Class 2/SLN+ OS SLNB 100% 75% SLNB- 50% 25% SLNB+ n=217 p= % Time (years) SLNB- (n=159) SLNB+ (n=58) Events yr OS 71% 62% % su urviving % survival GEP in SLNB- Patients 100% 75% Class 1/ SLNB- 50% 25% Class 2/ SLNBn=159 p< % Time (years) Class 1/SLNB- (n=67) Class 2/SLNB- (n=92) Events yr OS 91% 55% DFS = Disease Free Survival; DMFS = Distant Metastasis-Free Survival; OS = Overall Survival Gerami, JAAD in press 2015 Censor date: May Gerami, JAAD in press 2015 Censor date: May JandJan 2003 DP


15 January 2013 Primary Dermal Cutaneous Metastasis 14


 13")
")

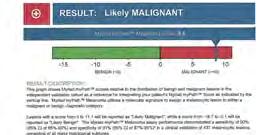
16 mrna Expression for Diagnosis of Melanocytic Neoplasms From Myriad Evaluated 859 total lesions by mrna expression profiling focusing on 23 genes Gene Signature 1) 13 immune related genes 2) 1 cell differentiation gene 3) 9 housekeeping genes Training set of 464 and Validation set of
17 91 16
2/6/2018. Original Paradigm. Clonal Chromosomal A berrations. Only 20% of Spitz Nevi 95% 6p, 7q, 17q, 20q, 4q,8q, 1q, 11q. Isolated Gain in 11p
 Molecular Diagnostics for Melanocytic Neoplasms: Moving towards a Revolution in the Management of Melanocytic Neoplasms Pedr am Gerami MD Associate Professor of Dermatology, Pathology and Pediatrics at
Molecular Diagnostics for Melanocytic Neoplasms: Moving towards a Revolution in the Management of Melanocytic Neoplasms Pedr am Gerami MD Associate Professor of Dermatology, Pathology and Pediatrics at
> 6000 Mutations in Melanoma. Tests That Cay Be Employed. FISH for Additions/Deletions. Comparative Genomic Hybridization
 Winter Clinical 2017: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of Colorado
Winter Clinical 2017: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of Colorado
Update on Lymph Node Management in Melanoma
 Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
True or False? Nearly twice as many SLNB negative compared to SLNB positive patients will ultimately die of metastatic melanoma.
 qrt-pcr Based Methods for Prognosis of Melanoma Pedr am Gerami MD Pr ofessor of Dermatology, Pathology and Pediatrics Nor thwestern University Dir ector Melanoma Program, Northwestern Skin Cancer Institute
qrt-pcr Based Methods for Prognosis of Melanoma Pedr am Gerami MD Pr ofessor of Dermatology, Pathology and Pediatrics Nor thwestern University Dir ector Melanoma Program, Northwestern Skin Cancer Institute
I have no relevant conflicts of interest to disclose. John T. Seykora MD PhD Departments of Dermatology & Pathology and Laboratory Medicine
 Molecular Characterization of Stage 1-3 Melanoma: Are we close to accurate prognostication and prediction? I have no relevant conflicts of interest to disclose. John T. Seykora MD PhD Departments of Dermatology
Molecular Characterization of Stage 1-3 Melanoma: Are we close to accurate prognostication and prediction? I have no relevant conflicts of interest to disclose. John T. Seykora MD PhD Departments of Dermatology
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Gene Expression Profiling in Malignancies: New Insights into Cancer Care
 Gene Expression Profiling in Malignancies: New Insights into Cancer Care Surgical Grand Rounds February 8, 2017 Martin Fleming, M.D. Chief, Division of Surgical Oncology West Cancer Center University of
Gene Expression Profiling in Malignancies: New Insights into Cancer Care Surgical Grand Rounds February 8, 2017 Martin Fleming, M.D. Chief, Division of Surgical Oncology West Cancer Center University of
Vernon K. Sondak. Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida
 Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Vernon K. Sondak Department of Cutaneous Oncology Moffitt Cancer Center Tampa, Florida Australasian Melanoma Conference 2016 Sydney, NSW, Australia October 29, 2016 Disclosures Dr. Sondak is a compensated
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy
 Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Update on Spitzoid and Blue nevus-like melanocytic lesions Emphasis on molecular studies informing diagnosis, prognosis and therapy Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology,
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is:
 Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Case 26 Male 37. Right jawline 5mm nodule?keloid. The best diagnosis is: A. Desmoplastic Spitz naevus B. Atypical Spitz Tumour C. Spitzoid melanoma D. Deep penetrating naevus E. Spitz naevus Case 26: M
Michael T. Tetzlaff MD, PhD
 Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department of Translational and
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology
 Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Genetic Testing: When should it be ordered? Julie Schloemer, MD Dermatology Outline Germline testing CDKN2A BRCA2 BAP1 Somatic testing Gene expression profiling (GEP) BRAF Germline vs Somatic testing
Which melanoma patients benefit from genetic testing?
 Which melanoma patients benefit from genetic testing? Michael A. Marchetti, MD Assistant Attending, Dermatology Service Memorial Sloan Kettering Cancer Center American Academy of Dermatology Annual Meeting
Which melanoma patients benefit from genetic testing? Michael A. Marchetti, MD Assistant Attending, Dermatology Service Memorial Sloan Kettering Cancer Center American Academy of Dermatology Annual Meeting
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors
 Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Melanoma and the genes: Molecular alterations informing the diagnosis of melanocytic tumors Michael T. Tetzlaff MD, PhD Associate Professor Department of Pathology, Section of Dermatopathology Department
Dermatopathology. Dr. Rafael Botella Estrada. Hospital La Fe de Valencia
 Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Dermatopathology Dr. Rafael Botella Estrada. Hospital La Fe de Valencia Melanoma and mimics Dr. Martin Mihm Malignant lesions result from the accumulation of mutations Class I lesions (benign) Class II
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
MAPK Pathway. CGH Next Generation Sequencing. Molecular Tools in Care of Patients with Pigmented Lesions 7/20/2017
 Molecular Tools in Care of Patients with Pigmented Lesions Tammie Ferringer, MD Geisinger Medical Center, Danville, PA tferringer@geisinger.edu DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Tammie Ferringer,
Molecular Tools in Care of Patients with Pigmented Lesions Tammie Ferringer, MD Geisinger Medical Center, Danville, PA tferringer@geisinger.edu DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY Tammie Ferringer,
Molecular Enhancement of Sentinel Node Evaluation
 Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Melanoma Update: 8th Edition of AJCC Staging System
 Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
Melanoma Update: 8th Edition of AJCC Staging System Rosalie Elenitsas, M.D. Professor of Dermatology Director, Dermatopathology University of Pennsylvania DISCLOSURE OF RELATIONSHIPS WITH INDUSTRY None
David B. Troxel, MD. Common Medicolegal Situations: Misdiagnosis of Melanoma
 Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Common Medicolegal Situations: Misdiagnosis of Melanoma David B. Troxel, MD Medical Director, The Doctors Company, Napa, California Clinical Professor Emeritus, University of California at Berkeley Past
Molecular Aspects of Melanocytic Neoplasia. Iwei Yeh MD, PhD University of California, San Francisco
 Molecular Aspects of Melanocytic Neoplasia Iwei Yeh MD, PhD University of California, San Francisco Thanks to: Boris Bastian Timothy McCalmont Philip LeBoit Beth Ruben Jeff North Laura Pincus Thaddeus
Molecular Aspects of Melanocytic Neoplasia Iwei Yeh MD, PhD University of California, San Francisco Thanks to: Boris Bastian Timothy McCalmont Philip LeBoit Beth Ruben Jeff North Laura Pincus Thaddeus
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
There is NO single Melanoma Stain. > 6000 Mutations in Melanoma. What else can be done to discriminate atypical nevi from melanoma?
 Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
Las Vegas Fall Clinical 2016: The Assessment and Diagnosis of Melanoma Whitney A. High, MD, JD, MEng Associate Professor, Dermatology & Pathology Director of Dermatopathology (Dermatology) University of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
Melanocytic proliferations in sundamaged
 Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
Atypical Spitzoid Tumor: What Does It Mean And How Should It Be Managed? Melanocytic proliferations in sundamaged skin Jane L. Messina, Jane L. Messina MD International Melanoma Pathology Working Group
The Enigmatic Spitz Lesion
 The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
The Enigmatic Spitz Lesion The Dawn of Spitz S Spitz Sophie Spitz Melanomas of Childhood ; Am J Pathol 1948 1910-1956 13 children (18 mo - 12 yrs) 12/13 had a benign clinical course Sophie Spitz Born 1910
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018
 Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Melanocytic Lesions: Use of Immunohistochemistry and Special Studies Napa Valley 2018 Victor G. Prieto, MD, PhD Professor Depts. of Pathology and Dermatology University of Texas - MD Anderson Cancer Center
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Controversies and Questions in the Surgical Treatment of Melanoma
 Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Gene Expression Profiling for Melanoma
 Medical Policy Manual Genetic Testing, Policy No. 29 Gene Expression Profiling for Melanoma Next Review: April 2019 Last Review: April 2018 Effective: June 1, 2018 IMPORTANT REMINDER Medical Policies are
Medical Policy Manual Genetic Testing, Policy No. 29 Gene Expression Profiling for Melanoma Next Review: April 2019 Last Review: April 2018 Effective: June 1, 2018 IMPORTANT REMINDER Medical Policies are
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy
 Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Clinical Case Conference Melanoma
 Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre
 Skin Cancer Volume 2013, Article ID 904701, 7 pages http://dx.doi.org/10.1155/2013/904701 Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre Vera Teixeira, 1
Skin Cancer Volume 2013, Article ID 904701, 7 pages http://dx.doi.org/10.1155/2013/904701 Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre Vera Teixeira, 1
ORIGINAL ARTICLE. Clinical Node-Negative Thick Melanoma
 ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma.
 Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Melanoma UpToDate: Introduction: Risk Factors: 1. Opdivo + Ipilumimab is now the first line therapy for metastatic melanoma. Median age = 50 yrs Incidence is rising - Sun exposure: UVB (290-320nm) > UVA
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases
 Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
Malignant Melanoma in Turkey: A Single Institution s Experience on 475 Cases Faruk Tas, Sidika Kurul, Hakan Camlica and Erkan Topuz Institute of Oncology, Istanbul University, Istanbul, Turkey Received
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA
 ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Nodal Treatment in Melanoma: Snow to MSLT-II
 Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director,
Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director,
Talk to Your Doctor. Fact Sheet
 Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Gene Expression Profiling for Cutaneous Melanoma
 Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Applies to all products administered or underwritten by Blue Cross and Blue Shield of Louisiana and its subsidiary, HMO Louisiana, Inc.(collectively referred to as the Company ), unless otherwise provided
Rebecca Vogel, PGY-4 March 5, 2012
 Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
University of Groningen
 University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble at bay
 Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
Pitfalls in the diagnosis of melanocytic tumors Timothy McCalmont, MD University of California, San Francisco Ways to get into trouble, ideas on avoiding trouble, and diagnostic approaches to keep trouble
Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons
 Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons Ben J. Friedman, MD Senior Staff Physician Department of Dermatology Department of Pathology and Laboratory Medicine Henry
Molecular Methods in the Diagnosis and Prognostication of Melanoma: Pros & Cons Ben J. Friedman, MD Senior Staff Physician Department of Dermatology Department of Pathology and Laboratory Medicine Henry
Gene Expression Profiling for Cutaneous Melanoma
 Gene Expression Profiling for Cutaneous Melanoma Policy Number: 2.04.146 Last Review: 8/1/2018 Origination: 08/2018 Next Review: 8/1/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
Gene Expression Profiling for Cutaneous Melanoma Policy Number: 2.04.146 Last Review: 8/1/2018 Origination: 08/2018 Next Review: 8/1/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision
 Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
The Pathology of Neoplasia Part II
 The Pathology of Neoplasia Part II February 2018 PAUL BOGNER, MD A S S O C I A T E P R O F E S S O R O F O N C O L O G Y P A T H O L O G Y A N D D E R M A T O L O G Y Clinical goals of cancer pathology
The Pathology of Neoplasia Part II February 2018 PAUL BOGNER, MD A S S O C I A T E P R O F E S S O R O F O N C O L O G Y P A T H O L O G Y A N D D E R M A T O L O G Y Clinical goals of cancer pathology
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Dr. Brent Doolan, BSc MBBS MPH
 Impact of partial biopsies on the need for complete excisional surgery in the management of cutaneous melanomas: A multi-centre review Dr. Brent Doolan, BSc MBBS MPH Peter MacCallum Cancer Centre, Melbourne
Impact of partial biopsies on the need for complete excisional surgery in the management of cutaneous melanomas: A multi-centre review Dr. Brent Doolan, BSc MBBS MPH Peter MacCallum Cancer Centre, Melbourne
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Is There a Benefit to Sentinel Lymph Node Biopsy in Patients With T4 Melanoma?
 Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
Management of pediatric melanocytic lesions
 Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Open Journal of Clinical & Medical Case Reports Management of pediatric melanocytic lesions Volume 3 (2017) Issue 8 ISSN 2379-1039 Jin Kim, BS; Emmanuel Gabriel MD, PhD; Weiguo Liu MD, PhD; Lin Lin MD,
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective
 Procedure: An Oncologic Surgeon s Perspective") Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Disclosures. SLNB for Melanoma 25/02/2014 SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION
 8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
Who is the Ideal Candidate for PEG Intron?
 Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature. Sasha Jenkins
 Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
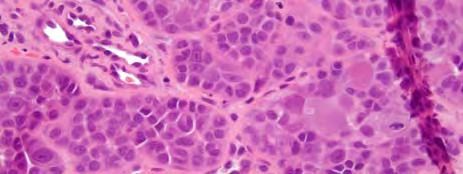
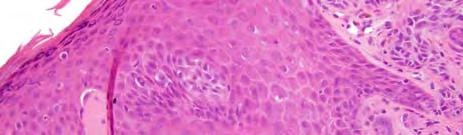
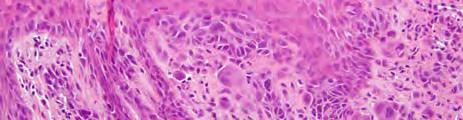
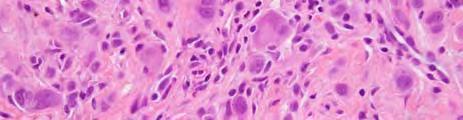
Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the
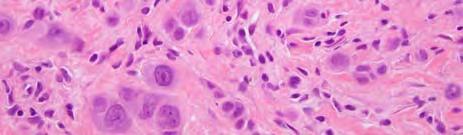
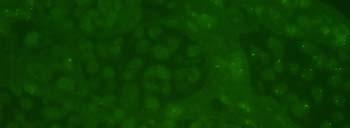
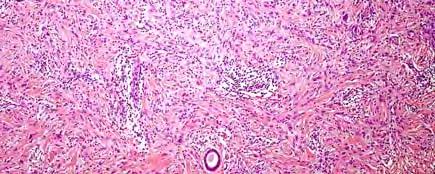
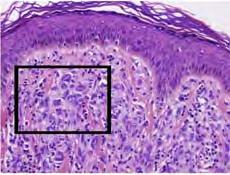
 Histopathology (4x) shows a domed papule with melanocytes extending into the") Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the deep dermis. (b) The melanocytes demonstrate abundant
Supplementary Figure 1. Spitzoid Melanoma with PPFIBP1-MET fusion. (a) Histopathology (4x) shows a domed papule with melanocytes extending into the deep dermis. (b) The melanocytes demonstrate abundant
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Rare melanoma: Are the options improving? Dr Neil Steven Consultant in Medical Oncology University Hospital Birmingham University of Birmingham
 Rare melanoma: Are the options improving? Dr Neil Steven Consultant in Medical Oncology University Hospital Birmingham University of Birmingham Classifying melanoma Melanoma (site of origin, thickness,
Rare melanoma: Are the options improving? Dr Neil Steven Consultant in Medical Oncology University Hospital Birmingham University of Birmingham Classifying melanoma Melanoma (site of origin, thickness,
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
Challenges in Melanoma Diagnosis and Management
 Challenges in Melanoma Diagnosis and Management Winter Clinical Dermatology Conference - Hawaii Darrell S. Rigel, MD MS Clinical Professor of Dermatology New York University Medical Center DISCLOSURE OF
Challenges in Melanoma Diagnosis and Management Winter Clinical Dermatology Conference - Hawaii Darrell S. Rigel, MD MS Clinical Professor of Dermatology New York University Medical Center DISCLOSURE OF
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Desmoplastic Melanoma: Clinical Behavior and Management Implications
 Desmoplastic Melanoma: Clinical Behavior and Management Implications Collier S. Pace, MD, a Jyoti P. Kapil, MD, b Luke G. Wolfe, MS, c Brian J. Kaplan, MD, c and James P. Neifeld, MD c a Division of Plastic
Desmoplastic Melanoma: Clinical Behavior and Management Implications Collier S. Pace, MD, a Jyoti P. Kapil, MD, b Luke G. Wolfe, MS, c Brian J. Kaplan, MD, c and James P. Neifeld, MD c a Division of Plastic
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma
 Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Radionuclide detection of sentinel lymph node
 Radionuclide detection of sentinel lymph node Sophia I. Koukouraki Assoc. Professor Department of Nuclear Medicine Medicine School, University of Crete 1 BACKGROUND The prognosis of malignant disease is
Radionuclide detection of sentinel lymph node Sophia I. Koukouraki Assoc. Professor Department of Nuclear Medicine Medicine School, University of Crete 1 BACKGROUND The prognosis of malignant disease is
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Page 1 of 3. We suggest the following changes:
 Page 1 of 3 Loren E. Clarke, M.D. Myriad Genetic Laboratories, Inc. 320 Wakara Way, Salt Lake City, UT 84108 Phone: 801.883.3470 Email: lclarke@myriad.com Date of Request: June 2017 NCCN Guidelines Panel:
Page 1 of 3 Loren E. Clarke, M.D. Myriad Genetic Laboratories, Inc. 320 Wakara Way, Salt Lake City, UT 84108 Phone: 801.883.3470 Email: lclarke@myriad.com Date of Request: June 2017 NCCN Guidelines Panel:
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Gene Expression Profiling for Cutaneous Melanoma Page 1 of 28 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Gene Expression Profiling for Cutaneous Melanoma Professional
Gene Expression Profiling for Cutaneous Melanoma Page 1 of 28 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Gene Expression Profiling for Cutaneous Melanoma Professional
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Clinical utilities and biological characteristics of melanoma sentinel lymph nodes
 W J C O World Journal of Clinical Oncology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5306/wjco.v7.i2.174 World J Clin Oncol 2016 April
W J C O World Journal of Clinical Oncology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5306/wjco.v7.i2.174 World J Clin Oncol 2016 April
Epidemiology. Objectives 8/28/2017
 Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Should we still be performing IHC on all sentinel nodes?
 Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Malignant tumors of melanocytes: Part 1. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
Malignant tumors of melanocytes: Part 1 Deba P Sarma, MD., Omaha The melanocytic tumor is one of the most difficult and confusing areas in Dematopathology. It is true that most (95%) of such lesions are
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin. Suraj Venna
 AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
21/07/2017. The «gray zone» of diagnosis is visible. Nevus Atypical nevus Melanoma. Melanoma ex-blue nevus
 Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
Update on the Clinico- Pathological and Molecular Diagnosis of Melanocytic Lesions None to declare Conflicts of interest Belfast pathology Arnaud de la Fouchardière MD, PhD Lyon, France What is new? Today
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma
 No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer. Cheol Min Kang 2018/04/05
 Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
المركب النموذج--- سبيتز وحمة = Type Spitz's Nevus, Compound SPITZ NEVUS 1 / 7
 SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma
SPITZ NEVUS 1 / 7 Epidemiology An annual incidence rate of 1.4 cases of Spitz nevus per 100,000 individuals has been estimated in Australia, compared with 25.4 per 100,000 individuals for cutaneous melanoma