Androgen Deprivation Therapy A Question of Timing
|
|
|
- Bathsheba Flynn
- 5 years ago
- Views:
Transcription



")
1 Androgen Deprivation Therapy A Question of Timing James Johnston BSc MBChB FRACS (Urol) Disclosure 1

2 OUTLINE History Watchful waiting Node positive patient Recurrence Intermittent Androgen Suppression Historical 2

3 Historical Historical 3



4 Alan Turing, convicted of homosexual acts in 1952, accepted castration over prison 4


5 John Hunter Circa 1840 The prostate gland, Cowper's glands and the glands along the urethra are in the perfect male large and pulpy, secreting a considerable quantity of slimy mucus which is salty to the taste; while in the castrated animal these are small, flabby, tough and ligamentous and have little secretion. Charles Huggins Born in Halifax, Nova Scotia 21 consecutive men with locally advanced or metastatic disease at the University of Chicago Noticeable improvement in all but 3. Those with small testicles at time of castration had a poor prognosis Nobel Prize

6 Andrew Schally pig to obtain 800ug of LHRH Nobel prize 1977 Androgens 6

7 Androgens Testosterone is the major androgen Estrogen is formed from aromatization in the peripheries and inhibits pituitary production of LH Testosterone plasma half life minutes 7
8 Adrenal Gland DHT Testicles Estrogens Peripheries 8

9 Androgen s Passes in to cell Converted to DHT Interacts with AR Chaperonins released Moves to nucleus Associates with cofactors Androgen response elements in the promoter region of genes Androgen Deprivation Inhibit secretion Inhibit action Cyproterone Flutamide Bicalutamide Enzalutamide Medical Estrogen LHRH agonists LHRH antagonist Ketaconazole Abiraterone Surgical Orchiectomy 9


10 What has changed in prostate cancer PSA Earlier stage at diagnosis The use of medicine compared to surgery People are living longer People with advanced prostate cancer are living longer Side effects Hot Flashes Anemia Muscle Wasting Obesity Osteoporosis / Fracture Sexual dysfunction Gynecomastia Cardiovascular Disease Weakness Cognitive function 10
11 Poll everywhere Go to Pollev.com/jamesjohnst202 Text JAMESJOHNSTO202 to to join then A to E depending on your answer Index patient 1 85 year old man Prostate Cancer 3+4=7 5 out of 12 cores Left and Right Apex and Mid Gland T3 clinically PSA at diagnosis 11 In 3 years time what PSA would prompt you to start ADT A) 22 B) 43 C) 55 D) 63 E) Any PSA, symptomatic mets 11

12 Watchful Waiting Conservative management until progression biochemical progression Local progression Systemic progression Localized prostate cancer with limited life expectancy 12
 Distant metastasis All 0.59 (<0.001) <65 0.47 (0.001) >65 0.77 (0.14) Bill-Axelson et al 2011, NEJM 364;18.")
13 SPCG -4, Scandinavian Study Death from any cause All RR 0.75 (p value 0.007) < (<0.001) > (0.89) Death from prostate cancer All 0.62 (0.01) < (0.008) > (0.41) Distant metastasis All 0.59 (<0.001) < (0.001) > (0.14) Bill-Axelson et al 2011, NEJM 364; Men under 80 Refused or where unsuitable due to cancer or co-morbidities 468 underwent immediate ADT 471 Deferred ADT 8 years follow up Reason for deferred to have ADT New symptomatic disease which threatened serious consequences 13
14 PSA >50 cf to <8-3.5 fold higher chance of dying in both ADT and deferred 7yr cumulative incidence of death - ADT arm 9.2% - Deferred arm 7.9% Although survival may not be significantly better would benefit from imediatte ADT to prevent complications from progressive disease PSA doubling time in those with PSA between 8 and 50 <12months cf to >12 months fold higher risk of dying 7 year cumulative incidence of prostate cancer death 47.6% if PSA DT <12 months cf to 11.4% if PSA DT >12 months 14
15 6 years later, 12 years follow up. % of patients with objective progression Objective progression at 10 years 42% in deferred arm v 30% Appearance of hot spots on bone scan 32 v 16% Time to castrate resistance was similar HR 0.91 deferred to immediate Studer et al 2014 Euro Urol 66; Mortality 80% in deferred arm and 76% in immediate arm had passed away at completion Non PCa mortality 49 v 40% HR 1.15 PCa mortality 25 v 23% HR 1.05 But all cause mortality slightly higher at yr 10 74% v 64% Studer et al 2014 Euro Urol 66;

16 44% never received ADT at end point 31% died without it Studer et al 2014 Euro Urol 66; Metastatic Disease VACURG II 1508 men Stage III/IV Placebo v diethylstilbestrol Patients on placebo never treated with active therapy Therefore immediate vs no therapy Byar et al Cancer 1973; 32: mg dose stopped prematurely due to cardiovascular deaths 16
17 VACURG I Assigned to placebo or orchiectomy No difference in cancer specific survival between groups Patients were allowed to switch to active therapy at symptomatic progression Overall recommendation is that patients with prostate cancer should not be treated until their symptoms require relief Blackard et al Urology 1973; 16: Medical Research Council Prostate Cancer Working Group men with locally advanced or metastatic setting Reduced morbidity Improved survival for M0 patients 54 v 70% favoring early vs deferred No difference in M1 patients 65 v 69% early v delayed Br J Urol 1997; 79:
18 Summary Localized disease with life expectancy less than 10 years In symptomatic metastatic disease give ADT In asymptomatic metastatic disease probably give ADT In non metastatic disease consider initiating ADT when PSA >50 Doubling time <12 months Symptomatic progression Index patient 2 75 year old man Post Radical Prostatectomy T3b, 4+4=8, PSA 18 pre op, margins clear, nodes negative Post op PSA 0.01 In 2 years time what PSA would prompt you to start ADT A) I would have already started it B) 0.03 C) 0.08 D) 0.20 E)

19 Biochemical recurrence post radical prostatectomy 0.2ng/ml or greater with a second confirmatory lab value AUA guidelines 2007 and adopted by EAU Radical Prostate N= & 1997 PSA recurrence N = 315 (15%) Clinical met s 8 years median 5 years median Death Pound et al JAMA ,
20 Natural History Antonarakis et al BJUI 2012; 109: men with progression post radical prostatectomy Johns Hopkins Hospital No salvage or adjuvant therapy prior to metastatic disease Results 8 yr median follow up - 30% developed mets Median metastatic free survival - 10 years Hazard Ratio multivariable analysis Gleason Gleason PSA Dt >15month 1 PSA Dt PSA Dt PSA Dt <3 months 33.3 No difference for stage, margin or time to recurrence (differs from an earlier review by Freedland et al 2005) Antonarakis et al BJUI 2012; 109: 32-9 Freedland et al JAMA 2005; 294(4):
21 Early v late Moul et al 2004 Department of Defense center for for Prostate Disease Research (PSA era) 5382 men underwent radical prostatectomy 1352 men with PSA 0.2ng/ml and post op follow up >6 months Early = after recurrence but before clinical mets Late = no ADT before clinical mets or end of follow up Moul et al J Urol 2004; 171 (14): 1141 Decreased rates of metastasis for Gleason 7 or more & PSADT < 12months, HR 2.12 Moul et al J Urol 2004; 171 (14):
22 Adjuvant vs PSA cut off s: Siddiqui et al 2008 Mayo Clinic Prostatectomy Registry Node negative radical prostatectomy patients who received ADT Adjuvant within 90 days vs ADT at 0.4, or systemic progression Siddiqui et al J Urol 2008; 179: 1830 Improved 10yr BCR free and progression free but not overall survival, If given at PSA less than 0.4 Benefit is lost for those who progress with PSA >0.4 Siddiqui et al J Urol 2008; 179:
23 T3b disease: Siddiqui et al 2011 Mayo Clinic Prostatectomy Registry patients with T3b who underwent adjuvant ADT (within 90 days) Matched 1:1 with T3b who had no adjuvant treatment Margin status, pathological Gleason score, pre op PSA, Age, year of surgery Median follow up 10 years Siddiqui et al BJUI 2011; 107: At 10 years for T3b disease adjuvant ADT show improved BCR free - 60% vs 16% Local recurrence free - 87 v 76% Systemic free % Cancer specific survival - 94 v 87% Not overall survival - 75 v 69% non sig 23
24 EAU Guidelines HIGH RISK Doubling time <3 months T3b Gleason 8-10 Time to recurrence <3 years LOW RISK Doubling time >12 months >3 years Gleason <7 Organ confined, T3a or less Ultrasensitive PSA era Hong et al Urology 2010;76(3): patients 3 year follow up post radical Biochemical recurrence free survival based on PSA nadir Less than % to % 0.02 to % 0.05 or greater % How is it used in calculating doubling time? - not clear 24
25 Index patient 3 72 year old man T2c, 3+4=7, PSA 18 pre op, 2/11 nodes positive 6 months post radical prostatectomy (first PSA), what PSA would prompt you to start ADT A) Undetectable B) 0.05 C) 0.10 D) 0.40 E)
26 Messing Trial 1988 to 1993 Aimed to recruit 240 Messing et al. The lancet oncology 2006; 7: Wong et al men, observational study, SEER data No difference in overall survival for those who received ADT within 120 v those who did not. HR 0.97 Wong et al J Clin Oncol 2008, 27,
27 Touijer et al men observational study MSK 1988 to 2010 Overall survival 60%, Cancer specific survival 72% Freedom from metastasis 65% If not recurred in 5 years then 81% chance of recurrence free Gleason >7 (HR 2.23) 3 or more LN (HR 2.61) Touijer et al Eur Urol 65 (2014) So, in practical terms Post radical prostatectomy node positive patients If they have 3 or more nodes involved and Gleason 8 give ADT Otherwise check the PSA 27
 4.0 B) 6.0 C) 7.")
28 Index patient 4 80 year old man treated with external beam radiation therapy 5 years ago Pre radiation PSA 17, G 3+4=7 6 out of 12 cores, T2b PSA nadir 1.2 Last year the PSA rose to 3.2 Otherwise asymptomatic What PSA would prompt you to start ADT A) 4.0 B) 6.0 C) 7.5 D) 10 28
29 Pinover et al Cancer (4) treated with EBRT in Philadelphia 74Gy (61-80 range) 3D conformal technique Policy was to treat men with ADT if PSA DT < 12 months But some men refuse Observe men with PSA DT >12 months 248 men who demonstrated PSA failure Looked at freedom from distant metastasis PSA DT <12 months PSA nadir 1.5 PSA DT >12 months Gleason score 29
30 Kestin et al 2004 Retrospective comparative study from the USA men with t1-3n0m0 treated with EBRT 66.6 Gy Early ADT = after biochemical failure before clinical failure Late ADT = after clinical failure 5 year outcome Early Late Local failure rate 4% 33% Distant metastasis rate 13% 44% Cancer specific death 9% 24% Death due to any cause 32% 48% Kestin et al Int J Rad Onc, Biol Phys (2) INTERMITTENT THERAPY 30
31 Index patient 5 80 year old man Radical Prostatectomy 3 years earlier Diagnosis PSA 11, pt3b, G 4+4=8, margins clear, node negative PSA post op 0.8 nadir 1 cycle of 9 months cycle PSA nadir to 0.1 with ADT At 2 years post first cycle of intermittent androgen deprivation, what PSA would prompt you start ADT? A) 3.2 B) 5.2 C) 7.0 D)
 240-242 Re exposure of prostate cancer stem cells to androgen can reintroduce apoptotic potential Therefore prolonging time to castrate")
32 Intermittent Androgen Suppression Intermittent androgen suppression is an approach that balances the benefits of early ADT while reducing treatment-related side effects and expense Dr Martin Gleave European Urology 66 (2014) Re exposure of prostate cancer stem cells to androgen can reintroduce apoptotic potential Therefore prolonging time to castrate resistance 32
33 Shionogi model Bruchovsky, Rennie, Coldman Goldenberg et al. Cancer Res 1990; 50 (8): LNCaP prostate tumor model Sato N, Gleave M, Bruchovsky N Rennie S, Goldenberg. Lange P, Sullivan L. J steroid Biochem Mol Biol 1996; 58(2) IAS prolonged time to androgen-independent PSA gene regulation from 26 days to 77 days Klotz, Herr Morse, Whitmore Cancer 1986; 58:

34 A feasibility study 47 locally advanced or metastatic disease 8 of whom had progression following radiation therapy Goldenberg et al Urology (5) An improvement in sense of well being and the recovery of libido and potency in men who reported normal or near normal sexual function before the start of therapy 34
: 1261-9 PR7 trial, National Cancer Institute of Canada")


35 Meta analysis, Magnan et al JAMA Onc 2015 Magnan et al JAMA Oncology 2015; 1 (9): PR7 trial, National Cancer Institute of Canada Non metastatic hormone sensitive Prior radiation therapy Non inferiority trial Median follow up 6.9 years 1386 patients Median survival IAD 8.8 years, CAD 9.1 years Slightly better but not significant quality of scores for intermittent Crook et al N Engl J med 2012;367(10)
36 SWOG, S9346 trial Newly diagnosed Metastatic hormone sensitive Non inferiority trial If PSA dropped to below 4 Randomized to continuous or intermittent therapy 765 continuous androgen deprivation therapy 770 intermittent therapy Median follow up 9.8 years HR 1.10 (0.99 to 1.23) Because non inferiority limit of 1.20 pre set was within 90% confidence interval can not conclude it is non inferior Because lower limit of 90% confidence interval was below 1, then also can not conclude it was significantly inferior either 36
37 Quality of life At 3 and 9 months IAS had improved Erectile function Libido Mental health Physical functioning At 15 months Only improved physical functioning remained Bipolar Androgen Therapy With each cycle testosterone recovery takes longer Keizman et al Prostate (15) Instituting ADT cycle is based on PSA not testosterone Therefore is ADT initiated before testosterone recovered and apoptotic potential regained? Schweizer et al Science Translational Medicine 2015; 7 (269): 269ra2 Pilot study of 16 men with asymptomatic CRPC patients 7 of 14 showed PSA reponse and 5 of 10 showed radiological repsonse 4 men remained on BAT for >1 year 37
38 Take Home Messages This is not a new topic But one that wont go away as prostate cancer management continues to evolve Prostate cancer can kill and is usually due to castrate resistance, therefore considering when to start castration is important Prostate cancer is heterogeneous There is no one size fits all PSA Triggers No prior treatment non metastatic 6-10 No prior treatment metastatic PSA relapse post radical 3-5 PSA relapse after radiation


39 What Next? BATMAN? Newer modalities Haere Ra Farewell 39


40 40
41 Meta analysis Magnan JAMA Oncol (9) IAD not inferior to CAD for survival Some QOL criteria improved Metastatic setting Hussain et al J clin Oncol (24) PSA response is powerful predictor of survival PSA falling to <0.2 by 7-8 months are ideal PSA failing to fall below 4 unlikely to benefit Haere Ra 41
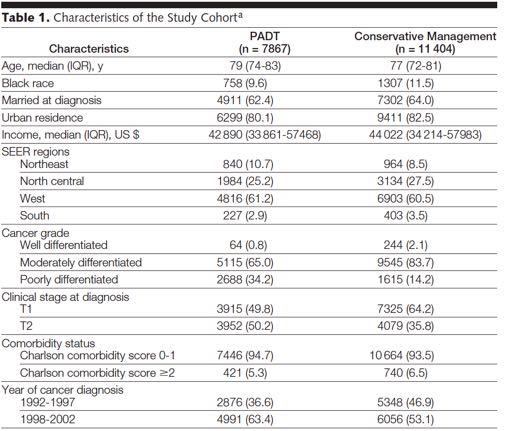
42 Goldenberg et al cancer (5) 1685 Majority of patients require 32 weeks of treatment to reduce PSA Lu Yao et al 2008 JAMA men, SEER 10Yr prostate cancer specific survival 80.1 v 82.6% ADT vs conservative (favoring non ADT use) -?more aggressive disease requiring ADT 10yr overall survival 30.2 v 30.3% Subset of poorly differentiated cancers (g8-10) 10yr p cancer spec survival 59.8% survival vs 54.3%, no difference in overall survival 17.3 v 15.3% Primary ADT = within first 180 days No PSA analysis High use v low use (IVA instrumental variable analysis) 42
43 43
44 Duchesne et al Journal of Clinical Oncology 2015, 33 Suppl TOAD (timing of androgen deprivation therapy) Abstract in Journal of Clinical Oncology 6 yr overall survival 86 v 79% Local disease progression HR 0.51 Distant disease progression HR 0.54 No difference to time to CRPC Two groups of patients proportions are not clear Following BCR after definitive therapy EBRT & RT Localised or metastatic disease not suitable for curative therapy Neoadjuvant No short or long term survival or biochemical recurrence rates 3 RCT, Witjes 1997, Soloway 2002, Klotz 2003 Perhaps reduced positive margin rates by 50% Lee et al
45 Post RP recurrence rad therapy Treating those with PSA <0.5 gives an 80 % chance of being disease free at 5 years Wait and see approach is appropriatte for those with PSA Dt >12 months 6 months of goserelin with SRT improved biochemical progression free survival at 5 years but not survival (GETUG-AFU 16 study ) Salvage Lymph node dissection - complete biochemical response can be achieved Most patients progress after 2 years Ideal patient not worked out yet use selectively 45
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
Hormone therapy works best when combined with radiation for locally advanced prostate cancer
 Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Hormone therapy works best when combined with radiation for locally advanced prostate cancer Phichai Chansriwong, MD Ramathibodi Hospital, Mahidol University Introduction Introduction 1/3 of patients
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease
 Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Radical Prostatectomy: Management of the Primary From Localized to Oligometasta:c Disease Disclosures I do not have anything to disclose Sexual function causes moderate to severe distress 2 years after
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
When PSA fails. Urology Grand Rounds Alexandra Perks. Rising PSA after Radical Prostatectomy
 When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
When PSA fails Urology Grand Rounds Alexandra Perks Rising PSA after Radical Prostatectomy Issues Natural History Local vs Metastatic Treatment options 1 10 000 men / year in Canada 4000 RRP 15-year PSA
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Updates in Prostate Cancer Treatment 2018
 Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Updates in Prostate Cancer Treatment 2018 Mountain States Cancer Conference Elaine T. Lam, MD November 3, 2018 Learning Objectives Understand the difference between hormone sensitive and castration resistant
Timing of Androgen Deprivation: The Modern Debate Must be conducted in the following Contexts: 1. Clinical States Model
 Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Timing and Type of Androgen Deprivation Charles J. Ryan MD Associate Professor of Clinical Medicine UCSF Comprehensive Cancer Center Timing of Androgen Deprivation: The Modern Debate Must be conducted
Intermittent Androgen Suppression - A standard of care or a good second choice?
 Intermittent Androgen Suppression - A standard of care or a good second choice? Dr Nicholas Buchan Uro-oncology Fellow Olympic Medal Standings Gold Silver Bronze USA 9 15 13 Germany 10 13 7 Canada 14 7
Intermittent Androgen Suppression - A standard of care or a good second choice? Dr Nicholas Buchan Uro-oncology Fellow Olympic Medal Standings Gold Silver Bronze USA 9 15 13 Germany 10 13 7 Canada 14 7
Metastatic prostate carcinoma. Lee Say Bob July 2017
 Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
Metastatic prostate carcinoma Lee Say Bob July 2017 Scenario A 58 year old gentleman presents with PSA 200 ng/ml with hard prostate and bone mets. LUTS but upper tracts are normal with normal RP. history
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
Understanding the risk of recurrence after primary treatment for prostate cancer. Aditya Bagrodia, MD
 Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Understanding the risk of recurrence after primary treatment for prostate cancer Aditya Bagrodia, MD Aditya.bagrodia@utsouthwestern.edu 423-967-5848 Outline and objectives Prostate cancer demographics
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia
 Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Paul F. Schellhammer, M.D. Eastern Virginia Medical School Urology of Virginia Norfolk, Virginia Virginia - Chesapeake Bay Landfall: Virginia Beach, April 29 th, 1607 PSA Failure after Radical Prostatectomy
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes
 Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
Naviga2ng the Adverse Effects of ADT: Improving Pa2ent Outcomes E. David Crawford, M.D. Professor of Surgery/ Urology/ Radiation Oncology University of Colorado Greetings from Colorado Disclosures Consultant:
majority of the patients. And taking an aggregate of all trials, very possibly has a modest effect on improved survival.
 Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
Hello. I am Farshid Dayyani. I am Assistant Professor in Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. We will be talking today about prostate cancer for survivorship
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD
 Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
Februray, 2013 The Return of My Cancer -Emerging Effective Therapies Jianqing Lin, MD Why/How my cancer is back after surgery and/or radiation? Undetected micro-metastatic disease (spreading) before local
When radical prostatectomy is not enough: The evolving role of postoperative
 When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
When radical prostatectomy is not enough: The evolving role of postoperative radiation therapy Dr Tom Pickles Clinical Associate Professor, UBC. Chair, Provincial Genito-Urinary Tumour Group BC Cancer
Definition Prostate cancer
 Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
Prostate cancer 61 Definition Prostate cancer is a malignant neoplasm that arises from the prostate gland and the most common form of cancer in men. localized prostate cancer is curable by surgery or radiation
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy. Dr. Matt Andrews Supervisor: Dr. David Bowes
 The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
The Role of Adjuvant vs Salvage Radiation Therapy after Prostatectomy Dr. Matt Andrews Supervisor: Dr. David Bowes Objectives Discuss the evidence for adjuvant radiotherapy (ART) EORTC, SWOG, ARO Current
Initial hormone therapy (and more) for metastatic prostate cancer
 for metastatic prostate cancer") Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Initial hormone therapy (and more) for metastatic prostate cancer Silke Gillessen, MD Medical Oncology Kantonsspital St.Gallen Switzerland silke.gillessen@kssg.ch Conflicts of interest Speakers Bureau
Treatment of Advanced Prostate Cancer
 Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
Treatment of Advanced Prostate Cancer Wm. Kevin Kelly, DO Associate Professor of Medicine and Surgery Yale University Yale University School of Medicine Advanced Prostate Cancer Metastatic Cancer Prostate
PSA is rising: What to do? After curative intended radiotherapy: More local options?
 Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Klinik und Poliklinik für Urologie und Kinderurologie Direktor: Prof. Dr. H. Riedmiller PSA is rising: What to do? After curative intended radiotherapy: More local options? Klinische und molekulare Charakterisierung
Prostate cancer update: Dr Robert Huddart Cancer Clinic London
 Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate cancer update: 2013 Dr Robert Huddart Cancer Clinic London Recent developments Improved imaging New radiotherapy technologies Radiotherapy for advanced disease Intermittent hormone therapy New
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Community care of Prostate Cancer. Shaun Costello Southern Cancer Network
 Community care of Prostate Cancer Shaun Costello Southern Cancer Network Introduction Why is GP follow up of prostate cancer important 4Years In Waikato Faster Cancer Treatment Reporting against the 3
Community care of Prostate Cancer Shaun Costello Southern Cancer Network Introduction Why is GP follow up of prostate cancer important 4Years In Waikato Faster Cancer Treatment Reporting against the 3
Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice
 european urology supplements 5 (2006) 362 368 available at www.sciencedirect.com journal homepage: www.europeanurology.com Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice Antonio
european urology supplements 5 (2006) 362 368 available at www.sciencedirect.com journal homepage: www.europeanurology.com Hormone Therapy for Prostate Cancer: Guidelines versus Clinical Practice Antonio
The Current State of Hormonal Therapy for Prostate Cancer
 The Current State of Hormonal Therapy for Prostate Cancer The Current State of Hormonal Therapy for Prostate Cancer Beth A. Hellerstedt, MD; Kenneth J. Pienta, MD Dr. Hellerstedt is Fellow, Division of
The Current State of Hormonal Therapy for Prostate Cancer The Current State of Hormonal Therapy for Prostate Cancer Beth A. Hellerstedt, MD; Kenneth J. Pienta, MD Dr. Hellerstedt is Fellow, Division of
Clinical Case Conference
 Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
Clinical Case Conference Intermediate-risk prostate cancer 08/06/2014 Long Pham Clinical Case 64 yo man was found to have elevated PSA of 8.65. TRUS-biopies were negative. Surveillance PSA was 7.2 in 3
PROSTATE CANCER SURVEILLANCE
 PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
Case Discussions: Prostate Cancer
 Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Case Discussions: Prostate Cancer Andrew J. Stephenson, MD FRCSC FACS Chief, Urologic Oncology Glickman Urological and Kidney Institute Cleveland Clinic Elevated PSA 1 54 yo, healthy male, family Hx of
Management of Prostate Cancer
 Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Management of Prostate Cancer An ESMO Perspective Alan Horwich Conflicts of Interest Disclosure Alan Horwich I have no personal conflicts of interest relating to prostate cancer. European Incidence and
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
MATERIALS AND METHODS
 Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Primary Triple Androgen Blockade (TAB) followed by Finasteride Maintenance (FM) for clinically localized prostate cancer (CL-PC): Long term follow-up and quality of life (QOL) SJ Tucker, JN Roundy, RL
Risk of renal side effects with ADT. E. David Crawford University of Colorado, Aurora, CO, USA
 Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Risk of renal side effects with ADT E. David Crawford University of Colorado, Aurora, CO, USA ADT: A key treatment for advanced prostate cancer John Hunter 1780-castration 1904: First RP 1938: Acid Phos.
Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer
 Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer Daisaku Hirano, MD Department of Urology Higashi- matsuyama Municipal Hospital, Higashi- matsuyama- city, Saitama- prefecture,
Strategies of Radiotherapy for Intermediate- to High-Risk Prostate Cancer Daisaku Hirano, MD Department of Urology Higashi- matsuyama Municipal Hospital, Higashi- matsuyama- city, Saitama- prefecture,
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE. ELENA CASTRO Spanish National Cancer Research Centre
 VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
VALUE OF PSA AS TUMOUR MARKER OF RELAPSE AND RESPONSE ELENA CASTRO Spanish National Cancer Research Centre Prostate Preceptorship. Lugano 17-18 October 2017 Prostate Specific Antigen (PSA) has a role in:
National Cancer Institute of Canada Clinical Trials Group (NCIC CTG) Trial design:
 Trial design:") Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A PHASE III STUDY OF IRESSA
Prostate Cancer. Dr. Andres Wiernik 2017
 Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
Prostate Cancer Dr. Andres Wiernik 2017 Objectives YES!!! 1. Epidemiology 2. Biology or Natural History of Prostate Cancer 3. Treatment NO!!! 1. Prostate Cancer Screening - controversies Which is the most
The Spa Hotel, Tunbridge Wells Friday 23 rd March Platinum sponsor
 The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
The Spa Hotel, Tunbridge Wells Friday 23 rd March 2018 Platinum sponsor ADT in brachytherapy Adding efficacy or just toxicity C. Salembier Department of Radiotherapy-Oncology Europe Hospitals Brussels
In autopsy, 70% of men >80yr have occult prostate ca
 Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Prostate Cancer UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Two randomized trials showed survival benefit of adding docetaxol to ADT in fit man with very high localized disease
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Evaluation of prognostic factors after radical prostatectomy in pt3b prostate cancer patients in Japanese population
 Japanese Journal of Clinical Oncology, 2015, 45(8) 780 784 doi: 10.1093/jjco/hyv077 Advance Access Publication Date: 15 May 2015 Original Article Original Article Evaluation of prognostic factors after
Japanese Journal of Clinical Oncology, 2015, 45(8) 780 784 doi: 10.1093/jjco/hyv077 Advance Access Publication Date: 15 May 2015 Original Article Original Article Evaluation of prognostic factors after
Embracing Technology & Timing of Salvage Hormones
 Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
Embracing Technology & Timing of Salvage Hormones Andrew Loblaw BSc, MD, MSc, FRCPC, CIP Department of Radiation Oncology Sunnybrook Health Sciences Centre University of Toronto Us Too, Brampton October
Prostate Cancer UK s Best Practice Pathway
 Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
Prostate Cancer UK s Best Practice Pathway TREATMENT Updated August 2018 To be updated in vember Active surveillance What is the patient s stage of disease? Low risk localised PSA < 10 ng/ml and Gleason
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
PORT after RP. Adjuvant. Salvage
 PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
PORT after RP Adjuvant Or Salvage RT after RP 40-50% PSA relapse after RP in HR Definition: PSA should be undetectable within 6 weeks of RP Initial PSA is measured 6-12 weeks after RP AUA defines biochemical
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED PLACEBO-CONTROLLED, DOUBLE-BLIND
Edward P. Gelmann, MD
 Prostate Cancer Edward P. Gelmann, MD Prostate Cancer Etiology and Ep pidemiology Screening Pathology Staging Localized Disease Metastatic Disease normal prostate epithelium GSTP1 CpG island hypermethylation
Prostate Cancer Edward P. Gelmann, MD Prostate Cancer Etiology and Ep pidemiology Screening Pathology Staging Localized Disease Metastatic Disease normal prostate epithelium GSTP1 CpG island hypermethylation
Conceptual basis for active surveillance
 Conceptual basis for active surveillance 1. Screening results in overdiagnosis 2. Clinically insignificant disease can be identified 3. All treatments have significant side effects and cost. 4. Delayed
Conceptual basis for active surveillance 1. Screening results in overdiagnosis 2. Clinically insignificant disease can be identified 3. All treatments have significant side effects and cost. 4. Delayed
EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER
 EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER Abraham Morgentaler, MD Director and Founder Men s Health Boston Associate Clinical Professor Harvard Medical School And the Urology
EVIDENCE SUPPORTING TESTOSTERONE THERAPY IN MEN WITH PROSTATE CANCER Abraham Morgentaler, MD Director and Founder Men s Health Boston Associate Clinical Professor Harvard Medical School And the Urology
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Prostate Cancer: from Beginning to End
 Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer: from Beginning to End Matthew D. Katz, M.D. Assistant Professor Urologic Oncology Robotic and Laparoscopic Surgery University of Arkansas for Medical Sciences Winthrop P. Rockefeller Cancer
Prostate Cancer Incidence
 Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Presentation with lymphadenopathy
 Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Presentation with lymphadenopathy Theo M. de Reijke MD PhD FEBU Department of Urology Academic Medical Center Amsterdam Rationale for RRP in N+ disease Prevention local problems Better survival in limited
Oligometastasis. Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie?
 Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
Körperstereotaxie bei oligo-metastasiertem Prostatakarzinom wann und wie in Kombination mit Systemtherapie? Daniel M. Aebersold 09. Dezember 2016 Oligometastasis JCO, 1995 1 Oligometastasis: Chance for
Adjuvant and Salvage Radiation for Prostate Cancer. Savita Dandapani, MD, PhD
 Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Adjuvant and Salvage Radiation for Prostate Cancer Savita Dandapani, MD, PhD DISCLOSURES I am a consultant for Reflexion, receive funding from Bayer, and on the Speaker s Bureau with Astra Zeneca. Post-prostatectomy
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy
 Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Session 4 Chemotherapy for castration refractory prostate cancer First and second- line chemotherapy October- 2015 ESMO 2004 October- 2015 Fyraftensmøde 2 2010 October- 2015 Fyraftensmøde 3 SWOG 9916 OS
Manipulating Hormones: Androgen Suppression in Prostate Cancer Patients
 Focus on CME at the University of Queen s ManitobaUniversity Manipulating Hormones: Androgen Suppression in ostate Cancer Patients By D. Robert Siemens, MD, FRCSC Case A 62-year old man presents with complaints
Focus on CME at the University of Queen s ManitobaUniversity Manipulating Hormones: Androgen Suppression in ostate Cancer Patients By D. Robert Siemens, MD, FRCSC Case A 62-year old man presents with complaints
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Mary J. Mackenzie, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada BLADDER CANCER A MULTICENTRE, RANDOMIZED
Irreversible Electroporation for the Treatment of Recurrent Prostate Cancer
 Irreversible Electroporation for the Treatment of Recurrent Prostate Cancer after prostatectomy, radiation therapy and HiFU R. Schwartzberg, E. Günther, N. Klein, S. Zapf, R. El-Idrissi, J. Cooper, B.
Irreversible Electroporation for the Treatment of Recurrent Prostate Cancer after prostatectomy, radiation therapy and HiFU R. Schwartzberg, E. Günther, N. Klein, S. Zapf, R. El-Idrissi, J. Cooper, B.
J Clin Oncol 28: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 28 NUMBER 1 JANUARY 1 2010 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Clinical Results of Long-Term Follow-Up of a Large, Active Surveillance Cohort With Localized Prostate Cancer
VOLUME 28 NUMBER 1 JANUARY 1 2010 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Clinical Results of Long-Term Follow-Up of a Large, Active Surveillance Cohort With Localized Prostate Cancer
Debate: Whole pelvic RT for high risk prostate cancer??
 Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Debate: Whole pelvic RT for high risk prostate cancer?? WPRT well, at least it ll get the job done.or will it? Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Using T-stage,
Optimizing Outcomes in Advanced Prostate Cancer
 Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Optimizing Outcomes in Advanced Prostate Cancer Module 3: Focus on Recent CRPC Guidelines and Advanced Hormone-Sensitive Disease Sébastien J. Hotte, MD, MSc (HRM), FRCPC Medical Oncologist and Head, Phase
Prostate Cancer in comparison to Radiotherapy alone:
 Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
Prostate Cancer in comparison to Radiotherapy alone: 1 RTOG 86-10 (2001) 456 patients with > a-goserelin 2 month before RTand during RT + Cyproterone acetate (1 month) vs b-pelvic irradiation (50 gy) +
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Impact of Adjuvant Androgen-Deprivation Therapy on Disease Progression in Patients with Node-Positive Prostate Cancer
 www.kjurology.org http://dx.doi.org/10.4111/kju.2011.52.11.741 Urological Oncology Impact of Adjuvant Androgen-Deprivation Therapy on Disease Progression in Patients with Node-Positive Prostate Cancer
www.kjurology.org http://dx.doi.org/10.4111/kju.2011.52.11.741 Urological Oncology Impact of Adjuvant Androgen-Deprivation Therapy on Disease Progression in Patients with Node-Positive Prostate Cancer
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
2015 myresearch Science Internship Program: Applied Medicine. Civic Education Office of Government and Community Relations
 2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
2015 myresearch Science Internship Program: Applied Medicine Civic Education Office of Government and Community Relations Harguneet Singh Science Internship Program: Applied Medicine Comparisons of Outcomes
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer
 Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
Changes in prostate-specific antigen and hormone levels following withdrawal of prolonged androgen ablation for prostate cancer S Egawa 1 *, H Okusa 1, K Matsumoto 1, K Suyama 1 & S Baba 1 1 Department
Prostate Cancer Local or distant recurrence?
 Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Prostate Cancer Local or distant recurrence? Diagnostic flowchart Vanessa Vilas Boas Urologist VFX Hospital FEBU PSA - only recurrence PSA recurrence: 27-53% of all patients undergoing treatment with curative
Hormonal Treatment and other Options in men with locally Advanced Prostate Cancer. Seoul Veterans Hospital Department of Urology Tae Young Jung
 Hormonal Treatment and other Options in men with locally Advanced Prostate Cancer Seoul Veterans Hospital Department of Urology Tae Young Jung Introduction Watchful waiting / Androgen deprivation therapy
Hormonal Treatment and other Options in men with locally Advanced Prostate Cancer Seoul Veterans Hospital Department of Urology Tae Young Jung Introduction Watchful waiting / Androgen deprivation therapy
Urologic Oncology: Seminars and Original Investigations 30 (2012) 3 15
 3 15") Urologic Oncology: Seminars and Original Investigations 30 (2012) 3 15 Review article The multi-disciplinary management of high-risk prostate cancer Jonathan C. Picard, M.D. a, *, Ali-Reza Golshayan, M.D.
Urologic Oncology: Seminars and Original Investigations 30 (2012) 3 15 Review article The multi-disciplinary management of high-risk prostate cancer Jonathan C. Picard, M.D. a, *, Ali-Reza Golshayan, M.D.
J Clin Oncol 25: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 25 NUMBER 12 APRIL 20 2007 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E Initial Hormonal Management of Androgen-Sensitive Metastatic, Recurrent, or Progressive Prostate Cancer:
VOLUME 25 NUMBER 12 APRIL 20 2007 JOURNAL OF CLINICAL ONCOLOGY A S C O S P E C I A L A R T I C L E Initial Hormonal Management of Androgen-Sensitive Metastatic, Recurrent, or Progressive Prostate Cancer:
PCa Commentary. Prostate Cancer? Where's the Meat? - A Collection of Studies Supporting the Safety of Its Use. Seattle Prostate Institute CONTENTS
 Volume 70 July - August 2011 PCa Commentary SEATTLE PROSTATE INSTITUTE CONTENTS TESTOSTERONE REPLACEMENT in Hypogonadal Men with Treated and Untreated Prostate Cancer? 1 TESTOSTERONE REPLACEMENT in Hypogonadal
Volume 70 July - August 2011 PCa Commentary SEATTLE PROSTATE INSTITUTE CONTENTS TESTOSTERONE REPLACEMENT in Hypogonadal Men with Treated and Untreated Prostate Cancer? 1 TESTOSTERONE REPLACEMENT in Hypogonadal
CLINICAL TRIALS Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer AN OPEN-LABEL, MULTICENTER, RANDOMIZED PHASE II
Prostate cancer: Update from the BCCA
 Prostate cancer: Update from the BCCA Tom Pickles Clinical Professor, UBC Topics 1. Incidence & Utilization rates 2. New developments with External Beam RT IGRT, VMAT and other enhancements Optimizing
Prostate cancer: Update from the BCCA Tom Pickles Clinical Professor, UBC Topics 1. Incidence & Utilization rates 2. New developments with External Beam RT IGRT, VMAT and other enhancements Optimizing
Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer*
 Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
Chinese-German J Clin Oncol DOI 10.1007/s10330-014-0037-9 September 2014, Vol. 13, No. 9, P417 P421 Maximal androgen blockade versus castration alone in patients with metastatic prostate cancer* Abeer
Open clinical uro-oncology trials in Canada
 CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
CLINICAL TRIALS Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Outcomes Following Negative Prostate Biopsy for Patients with Persistent Disease after Radiotherapy for Prostate Cancer
 Clinical Urology Post-radiotherapy Prostate Biopsy for Recurrent Disease International Braz J Urol Vol. 36 (1): 44-48, January - February, 2010 doi: 10.1590/S1677-55382010000100007 Outcomes Following Negative
Clinical Urology Post-radiotherapy Prostate Biopsy for Recurrent Disease International Braz J Urol Vol. 36 (1): 44-48, January - February, 2010 doi: 10.1590/S1677-55382010000100007 Outcomes Following Negative
Radiation with oral hormonal manipulation for non-metastatic, intermediate or high risk prostate cancer in men 70 and older or with comorbidities
 Radiation with oral hormonal manipulation for non-metastatic, intermediate or high risk prostate cancer in men 70 and older or with comorbidities Prostate cancer is predominately a disease of older men,
Radiation with oral hormonal manipulation for non-metastatic, intermediate or high risk prostate cancer in men 70 and older or with comorbidities Prostate cancer is predominately a disease of older men,
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada George Rodrigues, MD, Eric Winquist, MD, Mary J. Mackenzie, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Androgen deprivation therapy: New concepts. Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto
 Androgen deprivation therapy: New concepts Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto Clinical Research funding: 1. Bayer/Algeta 2. Ferring 3. Abbott 4. GSK 5. EMD Serono
Androgen deprivation therapy: New concepts Laurence Klotz Professor of Surgery Sunnybrook HSC University of Toronto Clinical Research funding: 1. Bayer/Algeta 2. Ferring 3. Abbott 4. GSK 5. EMD Serono
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Open clinical uro-oncology trials in Canada Eric Winquist, MD, Mary J. Mackenzie, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada ADRENOCORTICAL MALIGNANCIES CISPLATIN-BASED
Review of Polish and international guidelines on hormonal therapy in localized prostate cancer
 Review article NOWOTWORY Journal of Oncology 2016, volume 66, number 5, 403 407 DOI: 10.5603/NJO.2016.0071 Polskie Towarzystwo Onkologiczne ISSN 0029 540X www.nowotwory.edu.pl Review of Polish and international
Review article NOWOTWORY Journal of Oncology 2016, volume 66, number 5, 403 407 DOI: 10.5603/NJO.2016.0071 Polskie Towarzystwo Onkologiczne ISSN 0029 540X www.nowotwory.edu.pl Review of Polish and international
Advanced Prostate Cancer
 Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Advanced Prostate Cancer SAMO Masterclass 4 th March 2016 Aurelius Omlin Conflicts of interest Advisory Rolle: Astra Zeneca, Astellas, Bayer, Janssen, Pfizer, Sanofi Aventis Research support: TEVA, Janssen
Cancer de la prostate métastatique: prise en charge précoce
 Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Cancer de la prostate métastatique: prise en charge précoce Stéphane Oudard, MD, PhD Georges Pompidou Hospital, Oncology Department, Paris, France stephane.oudard@egp.aphp.fr SAGB.CAB.14.08.0382c 3/02/2016
Early Chemotherapy for Metastatic Prostate Cancer
 Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
Early Chemotherapy for Metastatic Prostate Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Smilow Cancer Center Yale University Medical Center Disclosure Consultant: Sanofi Aventis, Celgene,
PCa Commentary. Volume 79 May June 2014
 1221 Madison Street, 1 st Floor Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 79 May June 2014 CONTENT: Active Surveillance Page 1 Firmagon and Lupron Page 5 ACTIVE SURVEILLANCE:
1221 Madison Street, 1 st Floor Seattle, WA 98104 P 206-215-2480 www.seattleprostate.com PCa Commentary Volume 79 May June 2014 CONTENT: Active Surveillance Page 1 Firmagon and Lupron Page 5 ACTIVE SURVEILLANCE:
ADT vs chemo + ADT as initial treatment for advanced prostate cancer
 ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
ADT vs chemo + ADT as initial treatment for advanced prostate cancer By Hussein Khaled Prof. Medical Oncology Cairo University Possible Levels of Prostate Cancer At Diagnosis Local-Regional Disease Spread
ACTIVE SURVEILLANCE FOR PROSTATE CANCER
 ACTIVE SURVEILLANCE FOR PROSTATE CANCER Dr. Michael J Metcalfe PGY-2 Department of Urological Sciences April 25, 2012 CASE RM 65 year old active Caucasian male, married. PSA= 7.0 T2a Gleason 3+3=6 2/6
ACTIVE SURVEILLANCE FOR PROSTATE CANCER Dr. Michael J Metcalfe PGY-2 Department of Urological Sciences April 25, 2012 CASE RM 65 year old active Caucasian male, married. PSA= 7.0 T2a Gleason 3+3=6 2/6
Non-systemic treatment of low-volume metastatic disease.
 Non-systemic treatment of low-volume metastatic disease. Gert De Meerleer, M.D., Ph.D. Gent University Hospital om behalf of POMP study group Background Patients with metastatic prostate cancer are considered
Non-systemic treatment of low-volume metastatic disease. Gert De Meerleer, M.D., Ph.D. Gent University Hospital om behalf of POMP study group Background Patients with metastatic prostate cancer are considered
STAMPEDE trial (MRC PR08): Arm J overview. Enzalutamide and abiraterone comparison and trial update
: Arm J overview. Enzalutamide and abiraterone comparison and trial update") STAMPEDE trial (MRC PR08): Arm J overview Enzalutamide and abiraterone comparison and trial update Arm J Hypotheses and rationale STAMPEDE: Hypothesis Will addition of enzalutamide and abiraterone to standard-of-care
STAMPEDE trial (MRC PR08): Arm J overview Enzalutamide and abiraterone comparison and trial update Arm J Hypotheses and rationale STAMPEDE: Hypothesis Will addition of enzalutamide and abiraterone to standard-of-care
2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY
 Measure #104 (NQF 0390): Prostate Cancer: Adjuvant Hormonal Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL
Measure #104 (NQF 0390): Prostate Cancer: Adjuvant Hormonal Therapy for High Risk or Very High Risk Prostate Cancer National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL