NAACCR Grade 2018 Q & A
|
|
|
- Ralf Briggs
- 5 years ago
- Views:
Transcription
1 NAACCR Grade 2018 Q & A GRADE RULES Q: Can you assign a pathologic grade if bx of highest T AND bx of highest N, where case meets criteria for pathologic staging? A:The grade rules indicate for a pathological grade the tumor must have been resected. We checked with AJCC and they indicated you cannot use the highest T and N to assign a pathological GRADE, you need a surgical resection. It is important to follow the grade rules for collecting grade. They may differ from the rules for assigning TNM stage. Q: What about sites that have individual grade modifiers like Fuhrman Grade, And FIGO? A: Review the grade tables for those sites in the Grade manual. Review the recommended grade systems and any notes which may direct you on coding in certain circumstances. Some of the GYN sites do use FIGO while some do not. Fuhrman grade is no longer used for kidney- see table notes. Q: If a surgical procedure removes the primary site without LND required for path staging do we still assign the pathologic grade? A: YES absolutely. Grade is recorded for every reportable tumor, regardless of eligibility for TNM staging and whether or not you are required to collect TNM stage. Pathological Grade is based on the resection of the primary tumor for most sites. Whether or not lymph nodes or other metastatic sites are biopsied, is not a factor. Great question. Q: If no bx performed; just surgical resection; Do you use code 9? A: Correct for most sites. For most sites, you would code 9 for clinical grade if no biopsy was done prior to resection of the primary tumor. The exception would be a site like bladder or melanoma where the resected tumor is included as part of the clinical assessment. Clinical grade should reflect what the physician knew about the grade prior to treatment. If a biopsy was not performed prior to treatment, then prior to treatment the physician would not know the grade of the tumor. Q: How would one code a grade on a case diagnosed in 2017 and surgery is in 2018? The pathologist used the 2018 cap guidelines for the surgical procedure. Would this affect the grade coding guidelines? 1
2 A: Since the date of diagnosis is 2017, you would collect the grade in the single grade/differentiation data item. Even though the pathologist used the 2018 CAP guidelines, the grade should still be able to be collected, just follow the previous grade rules for the site you have. The version of Grade, SSDI S, Summary Stage, AJCC TNM Stage are all based the year of diagnosis, not when the case was accessioned or treated. Q: If the clinical grade is higher than the pathological grade, the instructions indicate to use the clinical grade, so we lose the pathological grade. If we have fields to collect both clinical & pathologic grade, why would we negate the actual path grade? A: The taskforce discussed this at length with input and guidance from the College of American Pathologist representative, as well as AJCC representatives. The highest microscopically proven grade within the overall tumor is what is prognostically significant and may factor into treatment selection as well as patient outcome. Q: If no residual cancer after surgery do you code 9, unknown grade? A: Not if a grade was established during the clinical timeframe. If you have a grade from the clinical bx, and there is no residual at surgery, then use the clinical grade to code both Clinical Grade and Pathological Grade. Q: If you have a bx w/ melanoma and then a surgery w/ no residual, you grade the bx as clinical, what about the surgery? Do you assign the clinical grade for surgery or 9 for the no residual? A: Use the clinical grade for both. The pathological grade is based in that situation on the microscopic exam of the wide excision and tumor from the clinical timeframe. This reflects TNM Staging for melanoma. The incisional biopsy and excisional biopsy would both be considered information from the Clinical timeframe. And the pathological time frame can include all information from the clinical workup Q: If we do not know whether the grade is clinical or pathological, if there's a surgery, can we assume it as pathological? A: No. Because you don t know if the grade IS from the surgery. Therefore per the 4 th bullet in code 4 for Clinical grade coding guidelines if there is only one grade available and it cannot be determined if it is clinical or pathological, assign it as a clinical grade and code unknown (9) for pathological grade, and blank for post-therapy grade. 2
3 Q: For Slide 22, note 4, would we go by this rule for TURP? A: The grade determined from a TURP would be used in assigning a clinical grade. However, this is not an example of the meaning of the 4 th bullet in Note 4 slide 22. The 4 th bullet in note 4 on slide 22 is describing a situation where you have limited information about a case, likely because the Dx and/or Tx were done elsewhere and you only have a narrative perhaps such as Patient recently moved to Sacramento from Iowa. She is s/p Dx/surgery for newly diagnosed breast cancer. Patient admitted to Outpatient Infusion center for her third cycle of 1 st course chemotherapy for Stage IIIB Infiltrating Breast Ca, SBR9; patient requires fluid and antiemetic support. In this case, you don t know if the SBR9 is from the Bx, the surgery, both, etc. Therefore, collect the SBR9 grade in your clinical grade data item, code the pathological grade to 9, and post-therapy grade is left blank. This is just one example, other scenarios are possible. Q: On the statement about the surgical resection meeting AJCC criteria for cancer site, does that mean, for example, for a prostate ca, if TURP done but not prostatectomy, there is no pathological grade even with surgical resection of psite because of the type? A: That is correct. For most sites resection of the primary tumor is enough to meet the criteria for pathological grade. However, for sites like bladder a partial cystectomy at least is required (because the bladder wall must be able to be assessed, and for prostate, the entire organ must be removed to meet the criteria for pathological stage. Q: Colon: Grade is commonly reported as "low grade" or "high grade" for colorectal primaries in our region. How would Grade be recorded for Colon when reported as such? A: If that is the only grade description used, you would have to code 9 for both clinical and pathological grade. The colon site uses nuclear grade codes 1-4; these cannot be crosswalked to an A-D generic option. However be sure to take each case separately and code per documentation. Q: Can you explain Blank vs Unknown for Grade? A: The Clinical Grade and the Pathological Grade can never be blank. They must always be coded, even if the code is 9, unknown. The Post-Therapy Grade CAN be blank when the post-therapy timeframe is not applicable for case (i.e., the patient did not receive neoadjuvant therapy followed by a surgical resection) Q: If they don t bx the primary site and do a bx of a metastatic site of the breast can we give it a stage 4 even though we don t have a grade for the primary site? A: Yes. Follow the grade rule for collecting grade. Follow the TNM rules for documenting stage. Q: What if path says low to mod diff? 3
4 A: If you re indicating a situation where the grade is reported using both terms low to mod diff, you would code to the higher mod diff term/grade. Also, make sure to read the applicable site-specific notes as well. Q: What if the FNA shows only high grade malignant cells and the resection is a specific type of cancer with a different grade? A: That would depend on the primary site grade instructions. Review the grade table codes and notes for the site you are abstracting and also follow the timeframe rules. If you have a specific example to send in we may be able to provide a more complete answer. Q: What if your State/Hospital does not require AJCC staging? How does AJCC 8th edition apply then? A: The concept of clinical (pre-treatment) and pathological (post surgery) and Post-therapy (surgery after neoadjuvant treatment) grade concepts still apply). Q: What grade would be used for brain primaries? A: WHO grade is the priority when available. The brain and CNS grade tables also include Low and High grade options, along with the generic definitions A-D. Q: Have these changes in terminology and grading schemas been communicated to pathologists globally? I am concerned that we will be coding a LOT of unknowns. A: The SSDI TF spent a great deal of time working with representatives from AJCC and CAP updating the Grade data items. The intent was to ensure that the terminology and grading schemas reflect what physicians are using in the clinical setting and what they are reading about in the current medical literature. Q: For slide 30, 9695/3 Follicular Grade 1 was left out. Is this not one of the applicable histologies or an omission from the other follicular listed? A: YES- GREAT CATCH! I will update my slide! Thank you _ Q: Is the crosswalk in the grade manual? A: Yes it is, pages
5 POST-THERAPY GRADE Q: Can you repeat the POST therapy criteria again, please? A: Post-therapy Grade must be from resection of the primary tumor after neoadjuvant treatment. Both of those criteria must be met to assign a Post-therapy grade. Q: What if after neo-adj there is no residual ca, what do you code for grade? A: If they did a surgical resection of where the tumor had been (i.e. LAR for a rectal primary), then grade would be 9. If they did not do surgery, then post therapy grade would be blank. Either way, pathological grade would be 9. Q: If a patient has neoadjuvant treatment, path grade is always 9? A: Correct. Post-therapy grade will be blank unless the patient received neoajuvant treatment AND the patient had resection of the primary tumor after the neoadjuvant treatment. Q: When you say "Grade Post Therapy" are you referring specifically to neoadjuvant therapy? A: Grade Post-Therapy is referring to the grade identified from resection of the primary tumor following neoadjuvant therapy. If the patient had some form of neoadjuvant therapy, chemotherapy, radiation therapy/combo, etc., which WAS FOLLOWED BY TUMOR RESECTION, the grade from this resection is the post-therapy grade. Q: Is it possible to have a post therapy grade if a post treatment bx is done and grade is given? A: No. The tumor must be resected after the completion of the neoadjuvant treatment. The biopsy is likely being used by the MD to decide upon further adjuvant therapy, or possibly in planning for type of surgical resection Q: A patient had a biopsy followed by surgical resection with residual adjuvant treatment and follow-up bx post treatment. Can you have all three grades coded? A: NEVER. If the patient had bx (clinical grade), followed by surgical resection (pathological grade) you have completed collecting grade. Post therapy grade is assigned when after the bx (clinical grade) the patient then received neoadjuvant treatment which was followed by tumor resection. In this situation you would not have a pathological grade (code 9). 5
6 If criteria for a pathological grade is met, then post-therapy grade criteria is not applicable (data item left blank). As an FYI you can never have a Pathological AJCC stage and a Post-therapy AJCC. You can only have one or the other. Never both. Q: If a patient has neo-adjuvant chemo followed by lumpectomy - would they have clinical and post treatment w/o pathologic grade? A: Assuming a grade was given from an incisional biopsy prior to neoadjuvant treatment, the grade from the incisional bx would be assigned to the clinical grade. The grade from the resected tumor that was taken after neoadjuvant tx would be assigned in post-therapy grade. Pathological grade would be 9. Q: Post-Therapy - will software literally be blank? Or will it state "blank" so it's not actually blank? Blank values were a problem when performing internal abst QC/VE, and running data requests. A: My understanding is the data item will actually be left blank. However, I would recommend you talk with your software vendor to see how they are treating these cases. BREAST Q: If a breast patient has moderately diff ductal carcinoma and high grade DCIS, which grade do we use? The lower grade with the higher histology or higher grade with lower histology? Also for staging? A: Assign the grade based on the invasive component of tumor (Mod-Diff=Code B). However, this would mean you could not use the grade to assign the stage group per Note 8 in the grade table notes. Q: What would clinical grade be for breast, invasive moderately differentiated ductal carcinoma, nuclear grade 2? A: Moderately differentiated is included in the breast grade table for invasive tumors - Code B. I would ignore the nuclear grade 2 term (in breast the nuclear grade terms are only used for an in situ tumor) Q: Grade for breast The manual states you need to include Tubule formation, nuclear pleomorphism, and mitotic count. 3 criteria is required. If the Pathologist only state Gr points are we accepting Grade 1. Notes state all three categories is designated? A: All three do not have to be stated if the SBR grade score is clearly documented. Per note 5: If the SBR/Nottingham score was not documented, HOWEVER, the tubule formation 2, nuclear pleomorphism 2 and mitotic count 3 (numbers for each were documented), then you may add these together to 6
7 calculate the SBR score of 7 which would = G2, Code 2. YOU can calculate the score ONLY when all 3 are documented. Conversely, if the pathologist only states the total score, i.e., SBR 7, then assign the appropriate code for a SBR score of 7; the pathologist already did the math. Q: For invasive breast, is "intermediate" on its own sufficient to assign code 2? A: See resources at Q: How do you code DCIS, micropapillary, solid, of breast? A: Grade would be coded as 9 Q: What if an incisional biopsy is performed and then the patient has a lumpectomy, but no residual tumor is found. Does that mean the initial biopsy was actually excisional (treatment). In that situation would Clinical Grade be 9 and the Pathological grade be based on information from the first procedure? A: No. The intent of the initial biopsy was to diagnose and classify the tumor. It was not meant to be treatment. This is the information the physician used to determine the first treatment (excisional biopsy). We would code the information from initial biopsy in Clinical Grade. The lumpectomy confirmed that there was no residual tumor. After the lumpectomy the physician knew the entire tumor had been removed and the highest grade cells produced by that primary tumor were the ones identified in the initial biopsy. Therefore, Pathological Grade would be the grade identified in the initial biopsy. Q: For 2018 cases, do we leave the old grade field blank or put 9? A: For 2018 and forward cases, leave the old grade data item blank. If the field is not blank for 2018 and forward cases and edit will be triggered. Coding the new grade fields for pre-2018 cases will also result in an edit. Q: Does the clinical grade apply to an excisional biopsy (like in breast) with negative margins? Or would you use the pathological grade? A: For a breast case the grade from an excisional biopsy would be considered/used for the pathological grade. If they did not do some kind of excisional biopsy prior to the excision, then clinical grade would be 9-unknown. Q: What if the clinical grade was Nuclear Grade and Pathological grade is Nottingham grade and Nuclear Grade is higher, do we still pick the higher grade? A: For the clinical grade, assign the appropriate code based on what the nuclear grade is. This is not the preferred grading system, but codes A-D can be used to record the nuclear grade. For the pathological 7
8 grade, the Nottingham grade is the preferred grading system, so you would code the appropriate grade using the preferred grading system. The preferred grading system always takes priority. Q: I abstracted a 2018 breast case, biopsy was positive for invasive ductal carcinoma, nuclear grade III. No SBR/Nottingham grade given. How should clinical grade be coded? A: For Breast, the historic grade (nuclear grade) can be captured in codes A-D. The mapping/crosswalk terms can be used in this case. For Nuclear grade III, this is equivalent to a C. So, for your 2018 case, you may assign a clinical grade of C. Q: Breast - what if only a grade is given, not stated to be SBR grade? Is "grade" equivalent to SBR grade? A: It s hard to say without having an actual description and path report. The statement grade 1, or grade 2, etc., in and of itself is not necessarily equivalent to SBR grade. You would want to review the pathology report further to see if there is additional documentation to indicate they are referring to an SBR or Nottingham grade. You need documentation that they are actually referring to the SBR grade. OR you need documentation they are referring to a generic grade for which codes A-D may be appropriate. If there is no documentation to clarify, Code 9 may be your only option. However, this is not a blanket statement and you must evaluate each case on all documentation available. Q: In the breast if the bx is just "low grade" or "grade 1" would the code be 1 or would it be 9 unknown? A: Low grade cannot be used for an invasive tumor, and you would code as 9. Low grade is reserved for in situ tumors. If all that is stated is grade 1 you need to review the path report to see if there is further information which indicates whether the grade is referencing an SBR or Nottingham grade. Q: Am I correct that breast primaries do not qualify for mapping/crosswalk term use since there are only 3 numeric codes listed in the new table (3-grade system)? A: That is what I stated on the webinar; HOWEVER, THIS WAS AN ERROR. Please note, the conversion or mapping terms list may be used for ANY grade table which includes the generic 4-grade categories A-D. See corrected slide handouts at the end of this Q&A which explains this further. The grade manual directions will also be clarified. GENITOURINARY 8
9 Q: Would you mind reiterating when the updates for the Grade ID 19 will show in the online version (Currently Version 1.1). For example, the use of 1-3 for SCC/Adenoca and L/H for urothelial? A: The updated manual was sent. This will also be reflected in SEER*RSA next week. Q: Please repeat the added note for slide 17. A: Grade G1, G2, G3 are used for Squamous cell carcinoma and Adenocarcinoma. Low Grade and High grade are used for Urothelial carcinomas. Q: Could you please repeat the L & H usage vs 1-3? A: For which site? The rules are different for different sites. For bladder, L & H take precedence for urothelial primaries. For squamous and adenocarcinoma, codes 1-3 take precedence. For sites like colon, low and high are not valid options and would be coded to 9. Q: If State/Hospital does not collect AJCC Stage, how do we know the TURBT (for example) is clinical and not surgical, as TURBT is captured as a surgery? My facility will not be purchasing AJCC 8th edition nor completing the training as it is not applicable. Q: If a patient only has a TURBT, would we use the clinical grade or the pathologic grade? Since they would have resected the primary tumor, but a TURBT is not considered a surgery per AJCC rules. A: A TUBRT is a surgical procedure (and a valid treatment) however it is not a surgical procedure that is considered a definitive tumor resection for the bladder per Grade Rules or TNM rules. It is really more a tumor debulking. The grade from a TURBT would be collected as a Clinical Grade. Example. Cystoscopy with bx positive for squamous cell ca, well differentiated; G1. This is followed by a TURBT revealing squamous cell ca, moderately differentiated; G2. Both of these procedures would be considered part of the clinical workup & timeframe, and the higher grade from the TURBT would be assigned for your clinical grade. Your pathological grade would be code 9; cannot be assessed. Post-therapy grade would be left blank. Q: If an initial prostate bx revealed a gl 6(3+3) and a second biopsy done with a gl 7(3+4) that finalized a treatment plan, which Gleason are you going to use? A: If there is more than one grade identified within the same time frame. Code the higher grade documented. Q: If someone has a bladder primary, but has cytoprostatectomy, prostate ca found incidentally. The clinical grade for the prostate ca, would be 9 correct? 9
10 A: Correct! The prostate cancer was found incidentally on surgical resection for the bladder cancer. So there was no clinical grade, nor clinical staging which are applicable for the prostate primary. Q: Is a pathologic grade coded even if the surgical resection doesn't meet the requirement for AJCC staging for that site? For example, if only a partial cystectomy is done for bladder. A: Yes. FYI a partial cystectomy DOES meet AJCC surgical criteria for bladder. Q: Can the grade manual be updated to include information that specifies when treatment is clinical not pathological? Example, TURBT or TURP, add notes to Bladder or Prostate, that if that is the only "treatment" provided, it is clinical grade and not pathological. A: Yes, we can add something to the grade manual about this. QUICK QUIZ # 7 Q: In the prostate example: Why wouldn't you use 2 in the pathologic grade since you had a clinical grade of 2? (even though you did not have a pathologic term that could be coded) A: Quick Quiz 7 pathological grade is 2 based on the higher clinical grade of Gleason 7. Were you accidentally looking at Quick Quiz 5 for prostate? QUICK QUIZ #6 Q: For Quiz 6 Bladder. After Radical Cystectomy, Final path dx is High grade papillary urothelial ca? A: Yes. Urothelial carcinomas may be either flat or papillary QUICK QUIZ #7 Q: Could you please repeat the answers to quiz #7 prostate, was it 2, 2, blank? A: Yes. Clinical Grade is 2. Pathological grade is 2. Post-therapy grade is blank. Q: Please repeat the rationale for Quiz question #8. QUICK QUIZ # 8 10
11 A: This patient had a biopsy of a liver mass which revealed metastatic ovarian cancer. Grade should be coded only from the primary site, never from a metastatic site. Therefore, our grade code is 9/unknown QUICK QUIZ # 9 Q: Why not the Mod Diff grade for the colon ca with hemicolectomy if we can code to the highest grade known if patient had a resection? A: The highest grade is high grade adenocarcinoma from the hemicolectomy. However, high grade is not a code option in the colon table & the coding notes provide no special allowance or direction in this case. And, while high grade is included in the list of mapping terms, the colon table uses numeric grade codes 1,2,3,4, which cannot be mapped to the A-D codes in the mapping table. Q: For the #9 example, why wouldn't the path grade be a 2 (since you have grade from the biopsy? You have the path grade as a 9 Q: On slide 49 why would you not bring the clinical grade 2 into the pathological grade since there was a resection? Q: Can we use Path grade : High grade? Why did we use path grade 9? A: The clinical grade in this case is lower (moderately differentiated) than the pathological grade (High Grade). So we can t use the rule that states if the clinical grade is higher than pathological grade, to use the clinical grade for both. The path grade is 9 because High grade is not a code option in the table. AND, there are no coding notes in the colon table that indicate we can code high grade to one of the codes in the table. IN ADDITION, the term high grade, while it is included in the mapping terms list, the grade table codes for colon are numeric, and we are not allowed to crosswalk a mapping term to grade definitions with numeric codes. So in this case, code 9, grade cannot be assessed must be recorded. Q: For exercise 9...Does the term "subsequent hemicolectomy" mean secondary treatment and not part of 1st course treatment? A: No the scenario was intended to describe first course treatment. The word subsequent means following or next, etc. Q: Colon, ID 02 - generic 4 grade system is not provided. Quiz #9, surg uses terminology "high grade" but it is not listed. What would the Grade Path be? Or can you use the Mapping/Crosswalk for generic grade? A: Pathological Grade: high grade is not a code option in Grade ID 02 for colon & the coding notes provide no special direction or allowance. Since the grade codes are numeric 1-4, the mapping terms cannot be used. Pathological grade fits no description within the colon code table therefore grade is coded to 9; unknown. QUICK QUIZ #10A 11
12 Q: Could you explain 10A pathologic breast? A: The pathological grade is 1 based on the clinical biopsy which identified the invasive ductal ca, Grade 1. Grade is always collected from the invasive component of a tumor when both in situ and invasive components are present. The surgical resection only revealed some residual DCIS with no remaining invasive tumor. So we use the clinical grade for our pathological grade (which captured the invasive portion of the tumor). QUICK QUIZ #10B Q: What was the grade path for Quick Quiz 10B breast? A: The pathological grade is 1, based on the tumor resection revealing an invasive ductal ca. Our clinical grade was H, for high grade DCIS which is all that was known during the clinical timeframe and diagnostic workup. But on definitive resection of the primary tumor, an invasive component of the tumor was identified. Grade is always coded based on the invasive component of a tumor when both in situ and invasive are present. Q: Quiz 10B - how will this be recorded because it will not be apparent that the bx was DCIS, or is it apparent simply because the High grade is used only for in situ? Not really obvious enough for data analysts. A: For breast the grades L, M, H are only applicable for in situ carcinomas. Q: Why isn't clinical Grade 1, for Quiz question 10B since in Question 10A we ignored the in- situ and assigned both Grade 1? Q: On that last case (10B), it doesn't make sense to pick up the clinical grade since it's higher because we have an option for pathological grade? What's the point of having 3 different types of grade if we can't code it accurately? A: In 10A the clinical bx showed an invasive ductal ca, Grade 1. Then the lumpectomy revealed no remaining invasive tumor, and instead only revealed residual DCIS. The pathological grade of 1 is assigned based on the clinical grade for the invasive tumor. Grade is always assigned based on the invasive component when both are present. Remember the pathological grade timeframe includes all grade information from the clinical timeframe and diagnostic workup THROUGH the completion of the surgical resection of the primary tumor. And you code the highest grade of the two In 10B, the clinical biopsy only showed high grade DCIS, and no invasive component was identified. Therefore our clinical grade can only be assigned based on the microscopic evidence of an in situ cancer 12
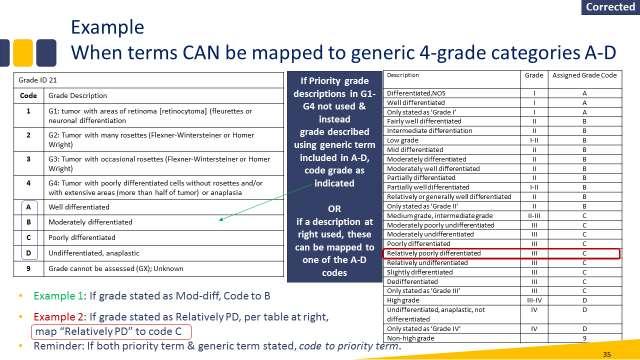
13 (we had no knowledge about the tumor in the clinical timeframe, other then that is was in situ). There was no invasive tumor component identified on the biopsy. Patient then had lumpectomy which revealed the tumor had an invasive component, along with residual DCIS. So for the pathological timeframe we have proof of the invasive component, and grade is always assigned based on the invasive component, if a tumor contains both in situ & invasive. You are collecting grade accurately if you are following the timeframe rules. _ GRADE CONVERSION / MAPPING TERMS Q: Can you please go over the rules for the conversion tables. Q: The mapping is very confusing, how do we know when we should perform mapping to grade? A: CORRECTED INFORMATION: the following differs from what I stated in the webinar. There was a misinterpretation of the grade manual instructions. The grade manual instructions will be updated and clarified. Here are the correct instructions: Terms in the mapping list may apply to any grade table (regardless of whether the priority system is a 2, 3 or 4 grade system) provided the table ALSO includes the generic 4-grade categories A-D. Therefore, when the preferred priority grade is not documented, and grade was stated using some other description, you can review the mapping terms list to see if one of the grade descriptions fits your case and can be mapped to an A-D code in your site grade table. If you find the term or description, code the A-D grade as the table indicates. If the term is not on the list, grade would be coded as 9. I have included corrected and revised slides at the end of this Q&A HANDOUTS, WEB LINKS, GRADE MANUAL, SEER*RSA, EDITS, OTHER MISC Q: Is there a handout for this webinar? Where do we find it A: Yes. Q: Can you provide the slides with the additional rational notes for the Quiz slides A: Yes! See supplemental handout with quiz answers and rationale posted on the NAACCR website. Q: Are we able to order a paper copy of the 2018 Grade Manual? If so, when will it be available? A: The grade manual is available on the NAACCR website. There are no plans to create a paper copy at this time. Q: Is the grade manual final? 13
14 A: It is no longer in Draft form. That means we are no longer taking suggestions on formatting or general feed-back from registrars. However, if something is missing from the manual or something is incorrect, we will have to make changes. Q: Noted that the Grade manual is no longer a draft but final manual. Is there an errata log for this manual? (separate and apart from the SSDI manual?) A: We do not currently have a tracking system for changes, but that will be added for future revisions. Q: Please confirm when and where the recorded version of this presentation will be available for registrars not able to view live versions. A: Q: Where was the alphabetic list for Grade located? A: Immediately following the schema ID list starting on page 14. Q: Which sites do you recommend to down load to your desk top-for the new 2018 sites grade and any other ones? A: See the NAACCR implementation page. You should find links to all of the relevant manuals that have changed or are new for Q: Is software due to go out in summer? A: This is a question for your vendor Q: The required data list v18 on the NAACCR website lists Grade item #440 is required by NPCR. The other Grade items are also required. The CoC does not require item #440 for Grade. Is this an oversight that needs to be updated? A: That is correct. Grade item #440 is required for pre-2018 cases. The new grade data items are required for cases. An edit will be triggered if the new grade data items are used for pre-2018 dx date cases or if the old grade item (#440) is used on 2018 cases. Q: Can you show where grade manual is again on website? A: Q: Where is the 2018 grade manual located? printable? A: See Resources at 14
15 Q: Which manual do we need to review for 2018 cases" SSDI Manual or Grade Manual? A: Use the Grade Manual for the new Grade Data items. Use the SSDI Manual for all other SSDI s. Technically, the new Grade Data items are SSDI s (they are specific to certain sites). However, they are different enough from other SSDI s that we felt they should have their own manual. Q: Is there a way to just print the grading pages for each site? A: You can print specific page from the manual. Q: Will central registries be allowed to use SEER RSA 2018+? A: Absolutely! Q: Are there validations associated with all new grade data fields? Example: A patient with an in situ tumor can only utilize in situ grades? A: At this point we have very few edits related to the new grade fields. I imagine we will add edits that cross check values with behavior, but we don't have any now. Q: Where does the Derived Schema come from? An API? A: Yes Q: Shouldn't item #440 be listed as RH for NPCR and not R? A: RH probably would have been more appropriate since it is required only for pre-2018 cases. Q: Suggestion - add word "Grade" to all of the links for SSDI page so folks know that both SSDI and Grade Manuals, etc. are found at this location. You wouldn't know they were on the SSDI page - unless you know they "go together A: Will do! Q: Will registrars/registries be notified when the grade manual is updated? Will the changes be annotated? Will there be a version number change or a "date updated" included? A: I m not sure about versioning, but we do have a Date Updated included in the footers of the Grade and the SSDI manual. Q: What does SSDI stand for? A: Site Specific Data Item 15
16 Q: Will Registry Plus Online Help be updated with the new 2018 manuals as they are final? Will pre-2018 manuals be available as well? A: I am not sure. Q: After all the majority of changes are made, will there be a re-print of the 8th edition? Or will it only be updated on the on-line version? A: Hopefully, most of the changes have been made and are included in the 3 rd print of the AJCC manual. The 3 rd print is currently available for purchase. I have not heard when the electronic version will be available. Q: SSDI manual appendix A: Could this be a review when abstracting like the purple book and fords manual? A: Yes. It contains a lot of great information. _ Q: Can trainers use this presentation? A: Yes. If you are an NPCR ETC, I am making my presentation available to you on the NPCR SharePoint. _ Q: Is there a code for CE's A: No CE s were requested for this presentation in order for it to be free to everyone Q: Regarding the upcoming 2018 Radiation webinars: will the webinars be recorded so I can review at my convenience? I cannot make either of the live dates. A: All of the 2018 implementation webinars will be posted (including Grade and Radiation). They will be posted to the SUGGESTIONS: - Add word "Grade" to all of the links for SSDI page so folks know that both SSDI and Grade Manuals, etc. are found at this location. You wouldn't know they were on the SSDI page - unless you know they "go together - It would be VERY nice if someone could throw us a bone and grant CE's for these webinars. We are dedicating so much time trying to learn all these new coding systems, we should be rewarded somehow. It's the least they could do. We are stressed enough! GREAT Webinar BTW! It cleared up a lot of questions I had. 16

17 - Curious - Should it be called SSDI? SSDI is usually Social Security Death Index. _ Corrected Slides


18 18
2018 New Grade Coding Rules It s a Good Thing!
 2018 New Grade Coding Rules It s a Good Thing! Presented by Donna M. Hansen, CTR California Cancer Registry NAACCR Webinar May 1, 2018 & May 2, 2018 1 Acknowledgement Special Thanks To: Jennifer Ruhl,
2018 New Grade Coding Rules It s a Good Thing! Presented by Donna M. Hansen, CTR California Cancer Registry NAACCR Webinar May 1, 2018 & May 2, 2018 1 Acknowledgement Special Thanks To: Jennifer Ruhl,
Q: How do you clinically code the N if the nodes are stated to be positive on mammogram/us or other imaging? No biopsy of nodes was done.
 Q&A Breast Webinar Q: One of my investigators is interested in knowing when Oncotype DX data collection was implemented. That data is collected in SSFs 22 and 23. I remember that the SSFs for breast were
Q&A Breast Webinar Q: One of my investigators is interested in knowing when Oncotype DX data collection was implemented. That data is collected in SSFs 22 and 23. I remember that the SSFs for breast were
Change Log V1.3- v1.4
 Change Log V1.3- v1.4 This document shows the changes that were made to the SSDI manual and the Grade manual for the SEER*RSA version 1.4 release on (Date TBD). SSDI Manual Section: General Instructions
Change Log V1.3- v1.4 This document shows the changes that were made to the SSDI manual and the Grade manual for the SEER*RSA version 1.4 release on (Date TBD). SSDI Manual Section: General Instructions
2018 Grade PEGGY ADAMO, RHIT, CTR OCTOBER 11, 2018
 1 2018 Grade PEGGY ADAMO, RHIT, CTR ADAMOM@MAIL.NIH.GOV OCTOBER 11, 2018 2 Acknowledgements Donna Hansen, CCR Jennifer Ruhl, NCI SEER Introduction 3 Histologic Type vs. Grade Credit: Dr. Kay Washington
1 2018 Grade PEGGY ADAMO, RHIT, CTR ADAMOM@MAIL.NIH.GOV OCTOBER 11, 2018 2 Acknowledgements Donna Hansen, CCR Jennifer Ruhl, NCI SEER Introduction 3 Histologic Type vs. Grade Credit: Dr. Kay Washington
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification
 Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation *
 ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
ACOS Inquiry and Response Selected Inquires CS Tumor Size/Extension Evaluation, CS Lymph Nodes Evaluation, CS Metastasis at Diagnosis Evaluation * CS Tumor Size/Extension Evaluation 24842 12/11/2007: Q:
2007 New Data Items. Slide 1. In this presentation we will discuss five new data items that were introduced with the 2007 MPH Coding Rules.
 Slide 1 2007 New Data Items Data Due in: Days In this presentation we will discuss five new data items that were introduced with the 2007 MPH Coding Rules. Slide 2 5 New Data Items Ambiguous Terminology
Slide 1 2007 New Data Items Data Due in: Days In this presentation we will discuss five new data items that were introduced with the 2007 MPH Coding Rules. Slide 2 5 New Data Items Ambiguous Terminology
CANCER REPORTING IN CALIFORNIA: ABSTRACTING AND CODING PROCEDURES California Cancer Reporting System Standards, Volume I
 CANCER REPORTING IN CALIFORNIA: ABSTRACTING AND CODING PROCEDURES California Cancer Reporting System Standards, Volume I Changes and Clarifications 16 th Edition April 15, 2016 Quick Look- Updates to Volume
CANCER REPORTING IN CALIFORNIA: ABSTRACTING AND CODING PROCEDURES California Cancer Reporting System Standards, Volume I Changes and Clarifications 16 th Edition April 15, 2016 Quick Look- Updates to Volume
2018 IMPLEMENTATION UPDATE: WHAT S NEW IN STAGING FOR 2018?
 2018 IMPLEMENTATION UPDATE: WHAT S NEW IN STAGING FOR 2018? SESSION 2 10/20/17 Q&A Please submit all questions concerning webinar content through the Q&A panel. A recording of today s session, the Q&A,
2018 IMPLEMENTATION UPDATE: WHAT S NEW IN STAGING FOR 2018? SESSION 2 10/20/17 Q&A Please submit all questions concerning webinar content through the Q&A panel. A recording of today s session, the Q&A,
MCR: MANAGEMENT OF 2018 CHANGES. By: Maricarmen Traverso-Ortiz MPH, CGG, CTR
 MCR: MANAGEMENT OF 2018 CHANGES By: Maricarmen Traverso-Ortiz MPH, CGG, CTR LEARNING OBJECTIVES Discuss a summary of the new changes for 2018 Overview of how the Maryland Cancer Registry is managing and
MCR: MANAGEMENT OF 2018 CHANGES By: Maricarmen Traverso-Ortiz MPH, CGG, CTR LEARNING OBJECTIVES Discuss a summary of the new changes for 2018 Overview of how the Maryland Cancer Registry is managing and
Kentucky Cancer Registry Spring Training 2017
 Kentucky Cancer Registry Spring Training 2017 What we will cover Coding instructions for grade Case examples addressing some areas of confusion for grade New grade data items coming in 2018 TNM Where to
Kentucky Cancer Registry Spring Training 2017 What we will cover Coding instructions for grade Case examples addressing some areas of confusion for grade New grade data items coming in 2018 TNM Where to
4/10/2018. SEER EOD and Summary Stage. Overview KCR 2018 SPRING TRAINING. What is SEER EOD? Ambiguous Terminology General Guidelines
 SEER EOD and Summary Stage KCR 2018 SPRING TRAINING Overview What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets SEER Summary Stage 2018 Site Specific
SEER EOD and Summary Stage KCR 2018 SPRING TRAINING Overview What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets SEER Summary Stage 2018 Site Specific
Instructions for Coding Grade for 2014+
 Instructions for Coding for 2014+ GRADE, DIFFERENTIATION OR CELL INDICATOR Item Length: 1 NAACCR Item #: 440 NAACCR Name:, Differentiation for solid tumors (Codes 1, 2, 3, 4, 9) and Cell Indicator for
Instructions for Coding for 2014+ GRADE, DIFFERENTIATION OR CELL INDICATOR Item Length: 1 NAACCR Item #: 440 NAACCR Name:, Differentiation for solid tumors (Codes 1, 2, 3, 4, 9) and Cell Indicator for
Seventh Edition Staging 2017 Breast
 Seventh Edition Staging 2017 Breast Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Seventh Edition Staging 2017 Breast Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Q&A for Collecting Cancer Data: Unusual Sites and Histologies Thursday, October 1, 2015
 Q&A for Collecting Cancer Data: Unusual Sites and Histologies Thursday, October 1, 2015 Q1: why can t we use pos pleural effusion to stage t value? A: Pleural effusion in Pleural Mesothelioma does not
Q&A for Collecting Cancer Data: Unusual Sites and Histologies Thursday, October 1, 2015 Q1: why can t we use pos pleural effusion to stage t value? A: Pleural effusion in Pleural Mesothelioma does not
Kyle L. Ziegler, CTR. California Cancer Registry U.C. Davis Health System
 Kyle L. Ziegler, CTR California Cancer Registry U.C. Davis Health System Overview New Data Items Reportability Clarifications New Coding Rules Grade ICD-O-3 Changes Collaborative Stage v0205 2 New Data
Kyle L. Ziegler, CTR California Cancer Registry U.C. Davis Health System Overview New Data Items Reportability Clarifications New Coding Rules Grade ICD-O-3 Changes Collaborative Stage v0205 2 New Data
Q: In order to use the code 8461/3 (serous surface papillary) for ovary, does it have to say the term "surface" on the path report?
 for ovary, does it have to say the term surface on the path report?") Q&A Session for Collecting Cancer Data: Ovary Q: In order to use the code 8461/3 (serous surface papillary) for ovary, does it have to say the term "surface" on the path report? A: We reviewed both the
Q&A Session for Collecting Cancer Data: Ovary Q: In order to use the code 8461/3 (serous surface papillary) for ovary, does it have to say the term "surface" on the path report? A: We reviewed both the
Outline. How to Use the AJCC Cancer Staging Manual, 7 th ed. 7/9/2015 FCDS ANNUAL CONFERENCE ST PETERSBURG, FLORIDA JULY 30, 2015.
 1 How to Use the AJCC Cancer Staging Manual, 7 th ed. FCDS ANNUAL CONFERENCE ST PETERSBURG, FLORIDA JULY 30, 2015 Steven Peace, CTR Outline 2 History, Purpose and Background Purchase and Ordering Information
1 How to Use the AJCC Cancer Staging Manual, 7 th ed. FCDS ANNUAL CONFERENCE ST PETERSBURG, FLORIDA JULY 30, 2015 Steven Peace, CTR Outline 2 History, Purpose and Background Purchase and Ordering Information
Introduction & Descriptors
 AJCC 8 th Edition Staging Introduction & Descriptors Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Introduction & Descriptors Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging. Introduction & Descriptors. Learning Objectives. This webinar is sponsored by
 AJCC 8 th Edition Staging Introduction & Descriptors Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Introduction & Descriptors Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
MCR MINI UPDATE DECEMBER 2017
 Fellow Registrars, MCR staff are very busy in November double checking our data before sending it to the national level, but we still have some important news, tips and resources to share with you. DUE
Fellow Registrars, MCR staff are very busy in November double checking our data before sending it to the national level, but we still have some important news, tips and resources to share with you. DUE
Seventh Edition Staging 2017 Melanoma. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Melanoma Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Seventh Edition Staging 2017 Melanoma Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express written
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012
 Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
Q&A Session NAACCR Webinar Series Collecting Cancer Data: Pancreas January 05, 2012 Q: Will sticky notes be transferrable from the previous electronic version of CS to the updated version? A: It is our
AJCC TNM STAGING UPDATES ARE YOU READY FOR TNM?
 AJCC TNM STAGING UPDATES ARE YOU READY FOR TNM? FCRA Annual Conference Boca Raton, Florida 7/26/2016 Steven Peace, CTR 1 Introduction Order AJCC Cancer Staging Manual, 7 th ed. How To Use - AJCC Cancer
AJCC TNM STAGING UPDATES ARE YOU READY FOR TNM? FCRA Annual Conference Boca Raton, Florida 7/26/2016 Steven Peace, CTR 1 Introduction Order AJCC Cancer Staging Manual, 7 th ed. How To Use - AJCC Cancer
NAACCR Webinar Series 1
 NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
Coding Pitfalls 9/11/14
 Coding Pitfalls 2013 2014 NAACCR Webinar Series September 11, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Coding Pitfalls 2013 2014 NAACCR Webinar Series September 11, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Seventh Edition Staging 2017 Colorectum. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Interactive Staging Bee
 Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging
 Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement
Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement
Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging
 Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement
Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement
5/8/2014. AJCC Stage Introduction and General Rules. Acknowledgements* Introduction. Melissa Pearson, CTR North Carolina Central Cancer Registry
 AJCC Stage Introduction and General Rules Linda Mulvihill Public Health Advisor NCRA Annual Meeting May 2014 National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention
AJCC Stage Introduction and General Rules Linda Mulvihill Public Health Advisor NCRA Annual Meeting May 2014 National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention
AJCC 8 th Edition Staging. Introduction & Descriptors. Learning Objectives. This webinar is sponsored by
 AJCC 8 th Edition Staging Introduction & Descriptors Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Introduction & Descriptors Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
NCDB Vendor Webinar: NCDB Call for Data January 2018 and Upcoming RQRS Revisions
 NCDB Vendor Webinar: NCDB Call for Data January 2018 and Upcoming RQRS Revisions American American College College of of Surgeons 2013 Content 2014 Content cannot be be reproduced or or repurposed without
NCDB Vendor Webinar: NCDB Call for Data January 2018 and Upcoming RQRS Revisions American American College College of of Surgeons 2013 Content 2014 Content cannot be be reproduced or or repurposed without
Major Rule Changes. Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging
 AJCC 8 th Edition Staging Major Rule Changes Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving patient
AJCC 8 th Edition Staging Major Rule Changes Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving patient
DATA STANDARDS AND QUALITY CONTROL MEMORANDUM DSQC #
 DATA STANDARDS AND QUALITY CONTROL MEMORANDUM DSQC #2006-01 CATEGORY: CLARIFICATION SUBJECT: RESCINDMENT - DSQC MEMORANDUM 2002-08 Coding Complex Morphologic Diagnoses (revised 8/02) EFFECTIVE: For Cases
DATA STANDARDS AND QUALITY CONTROL MEMORANDUM DSQC #2006-01 CATEGORY: CLARIFICATION SUBJECT: RESCINDMENT - DSQC MEMORANDUM 2002-08 Coding Complex Morphologic Diagnoses (revised 8/02) EFFECTIVE: For Cases
Quality ID #250 (NQF 1853): Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clinical Care
: Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clinical Care") Quality ID #250 (NQF 1853): Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Quality ID #250 (NQF 1853): Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Process
Lung /4/18. Please submit all questions concerning the webinar content through the Q&A panel.
 Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
Lung NAACCR 2018 2019 WEBINAR SERIES 1 Q&A Please submit all questions concerning the webinar content through the Q&A panel. If you have participants watching this webinar at your site, please collect
FINALIZED SEER SINQ S NOVEMBER 2011
 : 20110133 Multiple primaries/heme & Lymphoid Neoplasms: A patient was diagnosed 7/31/08 with DLBCL (9680/3) (biopsy left supraclav. node), stage IIIB. Treated with chemo. 10/14/10 biopsy right supraclav.
: 20110133 Multiple primaries/heme & Lymphoid Neoplasms: A patient was diagnosed 7/31/08 with DLBCL (9680/3) (biopsy left supraclav. node), stage IIIB. Treated with chemo. 10/14/10 biopsy right supraclav.
NAACR Treatment Webinar Quiz 1
 NAACR Treatment Webinar Quiz 1 1. Which of the following would NOT be considered cancer-directed treatment? a. Hemicolectomy b. Incisional biopsy c. Whole breast radiation d. MRI e. All of the above f.
NAACR Treatment Webinar Quiz 1 1. Which of the following would NOT be considered cancer-directed treatment? a. Hemicolectomy b. Incisional biopsy c. Whole breast radiation d. MRI e. All of the above f.
AJCC 7 th Edition Staging Disease Site Webinar Colorectum
 AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
NAACCR Webinar 2018 SeriesImplementations and Timelines
 NAACCR 2015-2016 Webinar 2018 SeriesImplementations and Timelines August 8, 2017 Session 1 Q&A Please submit all questions concerning webinar content through the Q&A panel. A recording of today s session,
NAACCR 2015-2016 Webinar 2018 SeriesImplementations and Timelines August 8, 2017 Session 1 Q&A Please submit all questions concerning webinar content through the Q&A panel. A recording of today s session,
7 th Edition Staging. AJCC 7 th Edition Staging. Disease Site Webinar. Colorectum. Overview. This webinar is sponsored by
 AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Minor Rule Changes. Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging
 AJCC 8 th Edition Staging Minor Rule Changes Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving patient
AJCC 8 th Edition Staging Minor Rule Changes Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving patient
Commission on Cancer Updates
 Commission on Cancer Updates OBJECTIVES PROVIDE CANCER REGISTRARS WITH INFORMATION ABOUT CURRENT COC 2018 CHANGES DISCUSS CHANGES RELATED TO CANCER REGISTRY DATA COLLECTION DISCUSS CHANGES RELATED TO CANCER
Commission on Cancer Updates OBJECTIVES PROVIDE CANCER REGISTRARS WITH INFORMATION ABOUT CURRENT COC 2018 CHANGES DISCUSS CHANGES RELATED TO CANCER REGISTRY DATA COLLECTION DISCUSS CHANGES RELATED TO CANCER
December 2002 Monthly Memo
 FLORIDA CANCER DATA SYSTEM December 2002 Monthly Memo CODING COMPLEX MORPHOLOGIC DIAGNOSES CODING COMPLEX BREAST HISTOLOGIES Apply these guidelines in priority order. Use the first guideline that applies
FLORIDA CANCER DATA SYSTEM December 2002 Monthly Memo CODING COMPLEX MORPHOLOGIC DIAGNOSES CODING COMPLEX BREAST HISTOLOGIES Apply these guidelines in priority order. Use the first guideline that applies
Measure #250 (NQF 1853): Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clincial Care
: Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clincial Care") Measure #250 (NQF 1853): Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clincial Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage
Measure #250 (NQF 1853): Radical Prostatectomy Pathology Reporting National Quality Strategy Domain: Effective Clincial Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: CLAIMS, REGISTRY DESCRIPTION: Percentage
Q&A Session Collecting Cancer Data: Hematopoietic and Lymphoid Neoplasms Thursday, November 6, 2014
 Q&A Session Collecting Cancer Data: Hematopoietic and Lymphoid Neoplasms Thursday, November 6, 2014 Q: If polycythemia ruba vera (PRV) or essential thrombocythemia (ET) is diagnosed by peripheral smear,
Q&A Session Collecting Cancer Data: Hematopoietic and Lymphoid Neoplasms Thursday, November 6, 2014 Q: If polycythemia ruba vera (PRV) or essential thrombocythemia (ET) is diagnosed by peripheral smear,
AJCC 8 th Edition Staging. Minor Rule Changes. Learning Objectives. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 AJCC 8 th Edition Staging Minor Rule Changes Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving patient
AJCC 8 th Edition Staging Minor Rule Changes Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving patient
You Want ME to Stage that Case???
 You Want ME to Stage that Case??? Jayne Holubowsky, CTR, Director, Virginia Cancer Registry 2 nd DelMarVa-DC Regional Conference October 11, 2018 What s New in the AJCC 8 th Edition Objectives Explain
You Want ME to Stage that Case??? Jayne Holubowsky, CTR, Director, Virginia Cancer Registry 2 nd DelMarVa-DC Regional Conference October 11, 2018 What s New in the AJCC 8 th Edition Objectives Explain
Staging for Residents, Nurses, and Multidisciplinary Health Care Team
 Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Requirements for Abstracted Text
 Slide 1 Requirements for Abstracted Text Principles of Abstracting Lesson 3: Purpose of Text Slide 2 Available Text Fields Place of Diagnosis Immunotherapy Chemotherapy Hormone Therapy Other Therapy Radiation
Slide 1 Requirements for Abstracted Text Principles of Abstracting Lesson 3: Purpose of Text Slide 2 Available Text Fields Place of Diagnosis Immunotherapy Chemotherapy Hormone Therapy Other Therapy Radiation
Coding Pitfalls 9/11/14
 Coding Pitfalls 2013 2014 NAACCR Webinar Series September 11, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Coding Pitfalls 2013 2014 NAACCR Webinar Series September 11, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
FINALIZED SEER SINQ QUESTIONS April July, 2017
 20170040 Source 1: 2016 SEER Manual pgs: 91 Source 2: 2007 MP/H Rules Notes: Lung MP/H Rules/Histology--Lung: What is the histology code for lung cancer case identified pathologically from a metastatic
20170040 Source 1: 2016 SEER Manual pgs: 91 Source 2: 2007 MP/H Rules Notes: Lung MP/H Rules/Histology--Lung: What is the histology code for lung cancer case identified pathologically from a metastatic
OVARY MEASURE SPECIFICATIONS
 Cancer Programs Practice Profile Reports (CP 3 R) OVARY MEASURE SPECIFICATIONS Introduction The Commission on Cancer s (CoC) National Cancer Data Base (NCDB) staff has undertaken an effort to improve the
Cancer Programs Practice Profile Reports (CP 3 R) OVARY MEASURE SPECIFICATIONS Introduction The Commission on Cancer s (CoC) National Cancer Data Base (NCDB) staff has undertaken an effort to improve the
Cancer Programs Practice Profile Reports (CP 3 R) Rapid Quality Reporting System (RQRS)
 Rapid Quality Reporting System (RQRS)") O COLON MEASURE SPECIFICATIONS Cancer Programs Practice Profile Reports (CP 3 R) Rapid Quality Reporting System (RQRS) Introduction The Commission on Cancer s (CoC) National Cancer Data Base (NCDB) staff
O COLON MEASURE SPECIFICATIONS Cancer Programs Practice Profile Reports (CP 3 R) Rapid Quality Reporting System (RQRS) Introduction The Commission on Cancer s (CoC) National Cancer Data Base (NCDB) staff
Format Of ICD-O Terms In Numerical List Each topographic and morphologic term appears only once The first listed term in Bold Type is the Preferred Te
 Florida Cancer Data System International Classification of Diseases for Oncology ICD-O-3 1 Basic Concepts Primary Site/Topography Histology/Morphology Behavior Grade/Immunophenotype 2 ICD-O 3 Structure/Format
Florida Cancer Data System International Classification of Diseases for Oncology ICD-O-3 1 Basic Concepts Primary Site/Topography Histology/Morphology Behavior Grade/Immunophenotype 2 ICD-O 3 Structure/Format
CASEFINDING. KCR Abstractor s Training
 CASEFINDING KCR Abstractor s Training 1 Introduction Casefinding Definition Purpose Methods Sources vs Resources Reportable Cancer Conditions Non-Reportable Conditions Ambiguous Terminology 2 https://www.google.com/search?q=puzzle+pieces&client=firefox-a&hs=mdc&rls=org.mozilla
CASEFINDING KCR Abstractor s Training 1 Introduction Casefinding Definition Purpose Methods Sources vs Resources Reportable Cancer Conditions Non-Reportable Conditions Ambiguous Terminology 2 https://www.google.com/search?q=puzzle+pieces&client=firefox-a&hs=mdc&rls=org.mozilla
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
7/29/ Grade Coding Instructions ICD-O-3 Updates. Outline. Introduction to Coding Grade for 2014+
 2014 Grade Coding Instructions ICD-O-3 Updates 1 I M P L E M E N T A T I O N T I M E L I N E ( S ) 2 0 1 4 F C D S D A M A P P E N D I X H A N D O U T S F C D S A N N U A L C O N F E R E N C E O R L A
2014 Grade Coding Instructions ICD-O-3 Updates 1 I M P L E M E N T A T I O N T I M E L I N E ( S ) 2 0 1 4 F C D S D A M A P P E N D I X H A N D O U T S F C D S A N N U A L C O N F E R E N C E O R L A
NPCR s TNM Stage Calculator
 NPCR s TNM Stage Calculator A Tool for Central Registry Quality Control and Consolidation Assistance NAACCR Annual Meeting June 16, 2016 Jennifer Seiffert Northrop Grumman Under contract to NPCR Joseph
NPCR s TNM Stage Calculator A Tool for Central Registry Quality Control and Consolidation Assistance NAACCR Annual Meeting June 16, 2016 Jennifer Seiffert Northrop Grumman Under contract to NPCR Joseph
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Q&A. Overview. Collecting Cancer Data: Prostate. Collecting Cancer Data: Prostate 5/5/2011. NAACCR Webinar Series 1
 Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
Collecting Cancer Data: Prostate NAACCR 2010-2011 Webinar Series May 5, 2011 Q&A Please submit all questions concerning webinar content through the Q&A panel Overview NAACCR 2010-2011 Webinar Series 1
I.2 CNExT This section was software specific and deleted in 2008.
 CANCER REPORTING IN CALIFORNIA: ABSTRACTING AND CODING PROCEDURES FOR HOSPITALS California Cancer Reporting System Standards, Volume I Changes and Clarifications 8th th Edition Revised May 2008 SECTION
CANCER REPORTING IN CALIFORNIA: ABSTRACTING AND CODING PROCEDURES FOR HOSPITALS California Cancer Reporting System Standards, Volume I Changes and Clarifications 8th th Edition Revised May 2008 SECTION
Interactive Discussion of Part I CS Coding Instructions: Working the Cases
 Interactive Discussion of Part I CS Coding Instructions: Working the Cases April Fritz, RHIT, CTR Donna M. Gress, RHIT, CTR Jennifer Ruhl, RHIT, CCS, CTR This presentation was supported by the Cooperative
Interactive Discussion of Part I CS Coding Instructions: Working the Cases April Fritz, RHIT, CTR Donna M. Gress, RHIT, CTR Jennifer Ruhl, RHIT, CCS, CTR This presentation was supported by the Cooperative
FINALIZED SEER SINQ QUESTIONS January June, 2016
 20160046 MP/H Rules/Multiple primaries/histology--rectum: How many primaries does this person have and what is the correct histology? See discussion. Rectal polyp excised in June, 2012, found to have adenocarcinoma
20160046 MP/H Rules/Multiple primaries/histology--rectum: How many primaries does this person have and what is the correct histology? See discussion. Rectal polyp excised in June, 2012, found to have adenocarcinoma
Pathology Driving Decisions
 Pathology Driving Decisions Part I: Understanding Your Diagnosis and Your Treatment Options May 7, 2018 Presented by: Dr. Matthew Mossanen completed his college and medical school training at UCLA. He
Pathology Driving Decisions Part I: Understanding Your Diagnosis and Your Treatment Options May 7, 2018 Presented by: Dr. Matthew Mossanen completed his college and medical school training at UCLA. He
Coding Pitfalls 9/1/2011. Coding Pitfalls Questions. Fabulous Prizes!!! September 1, NAACCR Webinar Series 1
 Coding Pitfalls 2010 2011 September 1, 2011 NAACCR 2010 2011 Webinar Series Questions Please submit questions about today s presentation through the Q&A (?) panel Fabulous Prizes!!! For the best question
Coding Pitfalls 2010 2011 September 1, 2011 NAACCR 2010 2011 Webinar Series Questions Please submit questions about today s presentation through the Q&A (?) panel Fabulous Prizes!!! For the best question
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Making the Most of Your Cancer Registry
 www.champsods.com Making the Most of Your Cancer Registry Presenter: Toni Hare, Vice President CHAMPS Oncology Data Services Picture of girl here December 11, 2009 Learning Objectives Upon completion of
www.champsods.com Making the Most of Your Cancer Registry Presenter: Toni Hare, Vice President CHAMPS Oncology Data Services Picture of girl here December 11, 2009 Learning Objectives Upon completion of
Summary NAACCR: What you need to know for 2017 Version 1.1. March ICD-O-3 Histologies. Reportability There are no reportability changes in 2017.
 Summary NAACCR: What you need to know for 2017 Version 1.1. March 2017 ICD-O-3 Histologies 2.1 New Terms and Codes Not Yet Implemented ICD-O-3 s and terms effective for 2015 was postponed due to CSv2 software
Summary NAACCR: What you need to know for 2017 Version 1.1. March 2017 ICD-O-3 Histologies 2.1 New Terms and Codes Not Yet Implemented ICD-O-3 s and terms effective for 2015 was postponed due to CSv2 software
1. Laterality, Primary Site E:Lateral & Site conflict Laterality (295) = 0 _ 2 Primary Site (291) = C711 Date of Diagnosis (283) =
 = 0 _ 2 Primary Site (291) = C711 Date of Diagnosis (283) =") Follow-up, Data Quality and Utilization Lesson 8 Page 5: Correcting the Edits Report Instructions: Use the spaces provided to fix the edit by providing the valid value for the incorrect data item. This
Follow-up, Data Quality and Utilization Lesson 8 Page 5: Correcting the Edits Report Instructions: Use the spaces provided to fix the edit by providing the valid value for the incorrect data item. This
Faster Cancer Treatment Indicators: Use cases
 Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
Faster Cancer Treatment Indicators: Use cases 2014 Date: October 2014 Version: Owner: Status: v01 Ministry of Health Cancer Services Final Citation: Ministry of Health. 2014. Faster Cancer Treatment Indicators:
A CENTRAL REGISTRY RELIABILITY STUDY
 A CENTRAL REGISTRY RELIABILITY STUDY Visual Editor TNM & Summary Stage Staging Skill Assessment Donna M. Hansen, CTR Auditor & Education Training Coordinator California Cancer Registry NAACCR June 16,
A CENTRAL REGISTRY RELIABILITY STUDY Visual Editor TNM & Summary Stage Staging Skill Assessment Donna M. Hansen, CTR Auditor & Education Training Coordinator California Cancer Registry NAACCR June 16,
CS Evaluation Fields. Outline of Presentation. Purpose of Evaluation Field. CSv2 Title of Presentation Jan 2011 Lecture Version: 1.
 CS Evaluation Fields Education and Training Team Collaborative Stage Data Collection System Version 02.03.02 (Effective date: 1/1/2011) Outline of Presentation Purpose AJCC TNM Classification Eval data
CS Evaluation Fields Education and Training Team Collaborative Stage Data Collection System Version 02.03.02 (Effective date: 1/1/2011) Outline of Presentation Purpose AJCC TNM Classification Eval data
A patient with recurrent bladder cancer presents with the following history:
 MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
MP/H Quiz A patient with recurrent bladder cancer presents with the following history: 9/23/06 TURB 1/12/07 TURB 4/1/07 TURB 7/12/07 TURB 11/14/07 Non-invasive papillary transitional cell carcinoma from
OSCaR UPDATE. Manager s Update Donald Shipley, MS. Oregon State Cancer Registry
 Oregon State Cancer Registry OSCaR UPDATE VOLUME 8, QUARTER 4 W INTER 2008 Manager s Update Donald Shipley, MS Since the Fall issue of OSCaR Update, the registry staff has completed several significant
Oregon State Cancer Registry OSCaR UPDATE VOLUME 8, QUARTER 4 W INTER 2008 Manager s Update Donald Shipley, MS Since the Fall issue of OSCaR Update, the registry staff has completed several significant
CANCER REPORTING IN CALIFORNIA: ABSTRACTING AND CODING PROCEDURES FOR HOSPITALS California Cancer Reporting System Standards, Volume I
 CANCER REPORTING IN CALIFORNIA: ABSTRACTING AND CODING PROCEDURES FOR HOSPITALS California Cancer Reporting System Standards, Volume I SUMMARY OF YEAR 2004 DATA CHANGES This document will provide a summary
CANCER REPORTING IN CALIFORNIA: ABSTRACTING AND CODING PROCEDURES FOR HOSPITALS California Cancer Reporting System Standards, Volume I SUMMARY OF YEAR 2004 DATA CHANGES This document will provide a summary
Registrar s Guide to Chapter 1, AJCC Seventh Edition. Overview. Learning Objectives. Describe intent and purpose of AJCC staging
 Registrar s Guide to Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers for Disease Control
Registrar s Guide to Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers for Disease Control
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
CERVIX MEASURE SPECIFICATIONS
 Cancer Programs Practice Profile Reports (CP 3 R) CERVIX MEASURE SPECIFICATIONS Introduction The Commission on Cancer s (CoC) National Cancer Data Base (NCDB) staff has undertaken an effort to improve
Cancer Programs Practice Profile Reports (CP 3 R) CERVIX MEASURE SPECIFICATIONS Introduction The Commission on Cancer s (CoC) National Cancer Data Base (NCDB) staff has undertaken an effort to improve
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
The New CP 3 R Application And Revisions To Standard 4.6 Integration Of The NCDB With The Accreditation Process
 The New CP 3 R Application And Revisions To Standard 4.6 Integration Of The NCDB With The Accreditation Process Wednesday, April 29, 2009 at 11 AM Central M. Asa Carter, CTR Manager, Approvals and Standards
The New CP 3 R Application And Revisions To Standard 4.6 Integration Of The NCDB With The Accreditation Process Wednesday, April 29, 2009 at 11 AM Central M. Asa Carter, CTR Manager, Approvals and Standards
Bladder Cancer Knowing the Risks and Warning Signs. Part II: Warning Signs
 Bladder Cancer Knowing the Risks and Warning Signs Part II: Warning Signs May 8, 2018 Presented by: is the Director of Urologic Oncology at MedStar Washington Hospital Center and an Assistant Professor
Bladder Cancer Knowing the Risks and Warning Signs Part II: Warning Signs May 8, 2018 Presented by: is the Director of Urologic Oncology at MedStar Washington Hospital Center and an Assistant Professor
Informational Abstracts: A Guide to Quality Abstracting
 Informational Abstracts: A Guide to Quality Abstracting Presented by NCRA Education Committee Carole Eberle, BS, CTR Louise Schuman, MA, CTR NCRA Education Committee NCRA Strategic Planning and Education
Informational Abstracts: A Guide to Quality Abstracting Presented by NCRA Education Committee Carole Eberle, BS, CTR Louise Schuman, MA, CTR NCRA Education Committee NCRA Strategic Planning and Education
11/3/2016. Outcomes Watching It Grow. What will we discuss? GATRA Annual Conference 2016 Lisa Connor, CTR
 Outcomes Watching It Grow GATRA Annual Conference 2016 Lisa Connor, CTR The abstract begins after case finding The abstract is in progress The abstract is complete The abstract is revisited and nurtured
Outcomes Watching It Grow GATRA Annual Conference 2016 Lisa Connor, CTR The abstract begins after case finding The abstract is in progress The abstract is complete The abstract is revisited and nurtured
Shore Medical Center Site-Specific Study: Colorectal Cancer 2013
 Shore Medical Center Site-Specific Study: Colorectal Cancer Shore Medical Center Site-Specific Study: Colorectal Cancer The following report is the result of a collaborative effort of four physician members
Shore Medical Center Site-Specific Study: Colorectal Cancer Shore Medical Center Site-Specific Study: Colorectal Cancer The following report is the result of a collaborative effort of four physician members
Q&A. Fabulous Prizes. Collecting Cancer Data: Breast 4/4/13. NAACCR Webinar Series Collecting Cancer Data Breast
 Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collecting Cancer Data Breast NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching this webinar
Collaborative Staging
 Slide 1 Collaborative Staging Site-Specific Instructions Prostate 1 In this presentation, we are going to take a closer look at the collaborative staging data items for the prostate primary site. Because
Slide 1 Collaborative Staging Site-Specific Instructions Prostate 1 In this presentation, we are going to take a closer look at the collaborative staging data items for the prostate primary site. Because
Evaluation of Abstracting: Cancers Diagnosed in MCSS Quality Control Report 2005:2. Elaine N. Collins, M.A., R.H.I.A., C.T.R
 Evaluation of Abstracting: Cancers Diagnosed in 2001 MCSS Quality Control Report 2005:2 Elaine N. Collins, M.A., R.H.I.A., C.T.R Jane E. Braun, M.S., C.T.R John Soler, M.P.H September 2005 Minnesota Department
Evaluation of Abstracting: Cancers Diagnosed in 2001 MCSS Quality Control Report 2005:2 Elaine N. Collins, M.A., R.H.I.A., C.T.R Jane E. Braun, M.S., C.T.R John Soler, M.P.H September 2005 Minnesota Department
CS Tumor Size. We re on the Web! Visit us at www2.kumc.edu/kcr
 VOLUME 17 ISSUE 3 July 2013 We re on the Web! Visit us at www2.kumc.edu/kcr July is UV Awareness Month. It is that time of the year again for summer! This is a great opportunity to talk about skin cancer.
VOLUME 17 ISSUE 3 July 2013 We re on the Web! Visit us at www2.kumc.edu/kcr July is UV Awareness Month. It is that time of the year again for summer! This is a great opportunity to talk about skin cancer.
Meeting CoC Standards
 Meeting CoC Standards Chapter 2 Clinical Services Sharon Metzger, CTR Director of Consulting Services Onco, Inc Welcome Thank you for joining us today for our webinar We will take questions and comments
Meeting CoC Standards Chapter 2 Clinical Services Sharon Metzger, CTR Director of Consulting Services Onco, Inc Welcome Thank you for joining us today for our webinar We will take questions and comments
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Collecting Cancer Data: Breast. Prizes! Collecting Cancer Data: Breast 8/4/ NAACCR Webinar Series 1. NAACCR Webinar Series
 Collecting Cancer Data: Breast NAACCR 2008 2009 Webinar Series Prizes! Question of the Month! The participant that submits the best question of the session will receive a fbl fabulous Pi Prize! Shannon
Collecting Cancer Data: Breast NAACCR 2008 2009 Webinar Series Prizes! Question of the Month! The participant that submits the best question of the session will receive a fbl fabulous Pi Prize! Shannon
Data Quality Analysis of Prostate Cancer Site Specific Factors in Metropolitan Detroit SEER Data,
 Data Quality Analysis of Prostate Cancer Site Specific Factors in Metropolitan Detroit SEER Data, 2004-2012 Jeanne Whitlock, MSLS, CTR Julie George, MS Ron Shore, MPH Fawn D. Vigneau, JD, MPH Metropolitan
Data Quality Analysis of Prostate Cancer Site Specific Factors in Metropolitan Detroit SEER Data, 2004-2012 Jeanne Whitlock, MSLS, CTR Julie George, MS Ron Shore, MPH Fawn D. Vigneau, JD, MPH Metropolitan
What s New for 8 th Edition
 What s New for 8 th Edition KCR 2018 SPRING TRAINING Overview What s New New Chapters for 8 th Editions Chapters That Split in 8 th Edition Merged 8 th Edition Chapters Blanks vs Xs How to Navigate Through
What s New for 8 th Edition KCR 2018 SPRING TRAINING Overview What s New New Chapters for 8 th Editions Chapters That Split in 8 th Edition Merged 8 th Edition Chapters Blanks vs Xs How to Navigate Through
Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ).
.") SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
SOLID TUMORS WORKSHOP Cases for review Prostate Cancer Case #1: 75 y/o Male (treated and followed by prostate cancer oncology specialist ). January 2009 PSA 4.4, 20% free; August 2009 PSA 5.2; Sept 2009
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective