Maintenance Therapy for Advanced NSCLC: Which Patients, Which Approach?
|
|
|
- Paul Phelps
- 5 years ago
- Views:
Transcription
1 Maintenance Therapy for Advanced NSCLC: Which Patients, Which Approach? Mark A. Socinski, MD Visiting Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Associate Clinical Director, Lung SPORE Co-Director, UPMC Lung Cancer Center of Excellence and Lung and Thoracic Malignancies Program University of Pittsburgh
2 Defining Maintenance Therapy Treatment beyond initial 4 (maybe 6) cycles of first line chemo doublet-based therapy with goal of maintaining best response with minimal toxicity Continuation maintenance: use of one or more agents given in first-line therapy Switch maintenance: initiation of a different agent that was not given in first-line therapy National Comprehensive Cancer Network website. Accessed 3/31/10.
 vs.")
3 The Dawn of Maintenance Therapy in NSCLC ECOG 4599 First-line Adv. NSCLC nonsquamous cell (N = 878) R A N D Sandler, N Engl J Med Carbo/pac 6 cycles Carbo/pac 6 cycles + bevacizumab q3wk RR: 15% (chemo) vs. 35% (chemo/bev) if no PD Observe until PD Maint bev until PD
4 Switch Maintenance Therapy
5 Immediate vs. Delayed Docetaxel Primary Endpoint: Overall Survival Adv. NSCLC Chemonaïve PS 0-2 N = 562 First-Line Chemo Gemcitabine/Carbo Every 3 wks x 4 cycles Gemcitabine 1000 mg/m2 IV d1, 8 q21 Carboplatin AUC 5 IV d1 q21 if no progression R A N D N = % drop off 95% of pts. received chemo Immediate Docetaxel 75mg/m 2 on Day 1, every 21 days until PD or maximum of 6 cycles Delayed Docetaxel Best supportive care, then start therapy at PD 75mg/m 2 on Day 1, every 21 days, until PD or maximum of 6 cycles 63% of pts. received chemo Fidias, J Clin Oncol 2009
6 Immediate vs. Delayed Second-Line Docetaxel Efficacy Progression-Free Survival Overall Survival Median 2 vs 4 mo p = HR=0.63 Median 9.1 vs 12.5 mo p = 0.08 HR=0.80 Fidias, J Clin Oncol 27: , 2009
7 Survival for Patients Actually Receiving Docetaxel on Immediate and Delayed Arms (Fidias) Immediate Delayed MST (months) N
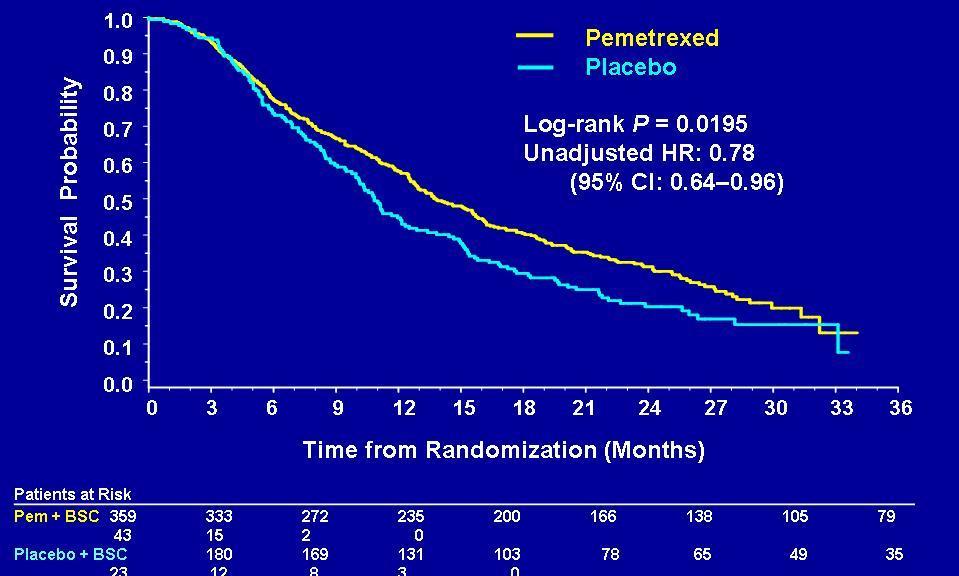
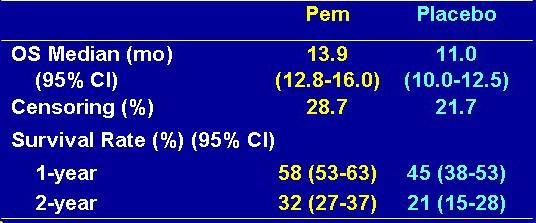
8 JMEN: Maintenance Pemetrexed vs. Placebo after First-Line Chemotherapy Does going on maintenance pemetrexed after four cycles of firstline chemo improve progression-free survival (PFS)? Advanced NSCLC No progression after 4 cycles of first line chemo (not including pemetrexed) N = 663 N = 441 R A N D N = 222 Maintenance pemetrexed IV every 3 weeks B12 and folate supplementation Maintenance placebo IV every 3 weeks B12 and folate supplementation Belani, Proc ASCO 2009
9 PFS Probability (%) Survival Probability (%) PFS and OS PFS OS (ITT Population) Pemetrexed: 4.04 mos (95% CI: ) Placebo: 1.97 mos (95% CI: ) HR = (95% CI: ) p < Pemetrexed 13.4 mos Placebo 10.6 mos HR = 0.79 (95% CI: ) p = Time (mos) 24% censored Time (mos) Ciuleanu, Lancet 2011
10 Survival Probability (%) JMEN: OS by Histology Non-Squamous (n = 481) SCC (n = 182) HR = 0.70 (95% CI: ) HR = 1.07 (95% CI: ) p =.002 p = Pemetrexed 15.5 mos Placebo 10.3 mos Pemetrexed 9.9 mos Placebo 10.8 mos Time (mos) Time (mos) Belani et al, 2009.
11 Erlotinib Maintenance Therapy in Advanced NSCLC: SATURN 1 st Line Adv NSCLC N = 1949 Tissue collected Platinum-based doublet chemo x 4 cycles if no prog R A N D N = 889 Erlotinib 150 mg PO daily Until Progresssion Placebo150 mg PO daily Until Progression 54% dropped off Primary Endpoint: PFS (All, and EGFR IHC positive) Capuzzo, ASCO 2009, WCLC 2009; Lancet 2010
12 PFS probability SATURN Trial Progression-Free Survival (by Intent to Treat) Erlotinib Placebo PFS at 12 wks (%) PFS at 24 wks (%) HR=0.71 ( ) Log-rank p< Erlotinib (n=437) Placebo (n=447) Time (weeks) *PFS is measured from time of randomization into the maintenance phase; assessments were every 6 weeks; ITT = intent-to-treat population
13 SATURN Trial Progression-Free Survival in Clinical Subgroups All HR (95% CI) n 0.71 ( ) 884 Male Female 0.78 ( ) ( ) 230 Caucasian Asian 0.75 ( ) ( ) 128 Adenocarcinoma Squamous-cell 0.60 ( ) ( ) 359 Never smoker Former smoker Current smoker 0.56 ( ) ( ) ( ) Favours erlotinib HR Favours placebo
14 OS probability SATURN Trial Overall Survival (by Intent to Treat) HR=0.81 ( ) Log-rank p= Erlotinib (n=438) Placebo (n=451) Time (months) *OS is measured from time of randomisation into the maintenance phase; ITT = intent-to-treat population
15 SATURN Trial Quality of Life/Symptom Progression HR (95% CI) p Time to deterioration in QoL (FACT-L) 0.96 ( ) Time to pain 0.61 ( ) Time to cough 0.77 ( ) Time to dyspnea 0.75 ( ) Time to analgesic use 0.66 ( ) FACT-L = Functional Assessment of Cancer Therapy Lung questionnaire; QoL = quality of life
16 PFS probability PFS according to EGFR mutation status EGFR mutation+ EGFR wild-type HR=0.10 ( ) Log-rank p< Erlotinib (n=22) Placebo (n=27) HR=0.78 ( ) Log-rank p= Erlotinib (n=199) Placebo (n=189) Time (weeks) Time (weeks) Interaction p<0.001
17 OS probability OS according to EGFR mutation status EGFR mutation+ EGFR wild-type 1.0 HR=0.83 ( ) Log-rank p= HR=0.77 ( ) Log-rank p= Erlotinib (n=199) Median 11.3 Placebo (n=189) Median Erlotinib (n=22) Median NR Placebo (n=27)* Median Time (months) Time (months) *Note that 67% of patients with EGFR mutation+ disease in the placebo arm received a second-line EGFR TKI
18 PFS probability PFS according to KRAS mutation status KRAS mutation+ KRAS wild-type HR=0.77 ( ) Log-rank p= Erlotinib (n=49) Placebo (n=41) HR=0.70 ( ) Log-rank p= Erlotinib (n=205) Placebo (n=198) Time (weeks) Time (weeks) Interaction p=0.95
19 OS probability Prognosis of patients with SD after first-line chemotherapy in SATURN Placebo: SD on 1st-line chemotherapy (n=235) Placebo: CR/PR on 1st-line chemotherapy (n=210) Time (months)
20 OS probability OS according to response to first-line chemotherapy (ITT population) Stable Disease CR/PR HR=0.72 ( ) Log-rank p= HR=0.94 ( ) Log-rank p= Erlotinib (n=252) Erlotinib (n=184) 0.4 Placebo (n=235) 0.4 Placebo (n=210) Time (months) Time (months) Multivariate HR for OS in SD population 0.71, p= Measured from time of randomisation into the maintenance phase
21 OS probability OS in patients with SD on first-line chemotherapy according to histology 1.0 Squamous 1.0 Non-squamous 0.8 HR=0.67 ( ) 0.8 HR=0.76 ( ) Log-rank p= Log-rank p= Erlotinib (n=97) Placebo (n=93) 0.6 Erlotinib (n=155) Placebo (n=142) Time (months) Time (months) Measured from time of randomisation into the maintenance phase
22 OS probability OS in EGFR wild-type group with SD on first-line chemotherapy Erlotinib (n=114) Placebo (n=103) HR=0.65 ( ) Log-rank p= Time (months) Measured from time of randomisation into the maintenance phase
23 Erlotinib Confers Survival Benefit Even for Patients with Response Rates of Nearly 0% Survival distribution function 1.00 Male Smokers with Squamous-Cell NSCLC 0.75 HR = % CI = p = Erlotinib median = 5.5 months (n=100) Placebo median = 3.4 months (n=57) Survival time (months) Clark, Clin Lung Ca, 2006
24 % Patients NOT Receiving Second Line Treatment in Observation Arms Study # Pts. w CR/PR/SD at end of 1 st line HR for OS # Pts. Obs Arm NOT Receiving Same Rx Fidias (JCO 2009) % Ciuleanu (Lancet 2009) (non-scca) 80% Cappuzzu (Lancet Oncol 2010) %
25 Continuation Maintenance Therapy
26 Gemcitabine Maintenance vs. Best Supportive Care Stage IIIB/IV NSCLC Chemo-naïve PS 0-2 (N=352) First-line chemo Gemcitabine/Cisplatin x3 cycles If no PD Gemcitabine: 1250 mg/m 2 IV d 1, 8, q 21 d R A N D 2:1 Ongoing gem until PD, + BSC (N = 138) BSC (N = 68) Cisplatin: 80 mg/m 2 IV d 1, q 21 d TTP: 6.6 vs 5 mo (3.6 vs 2.0 mo during maintenance) for gemcitabine maintenance therapy vs best supportive care, respectively; P<.001 No difference in OS Brodowicz T, et al, Lung Cancer. 2006;52(2):
27 Gemcitabine Maintenance after First Line Carbo/Gemcitabine Stage IIIB/IV NSCLC Chemo-naïve PS 0-2 (N=519) First-line chemo Gemcitabine/Carbo x4 cycles Gemcitabine: 1000 mg/m 2 IV d 1, 8, q 21 d Carboplatin: AUC 5 IV d 1, q 21 d If no PD R A N D 1:1 N = 255 (51% drop off) Ongoing gem until PD, + BSC BSC Median age 67 64% of patients performance status 2 (56% PS2-3 during maintenance) Belani, ASCO 2010, #7506


28 Gemcitabine Continuation Maintenance after First Line Carbo/Gemcitabine: Efficacy PFS OS Belani, ASCO 2010, #7506
29 PARAMOUNT: Phase III Trial of Pemetrexed Maintenance in Nonsquamous NSCLC Eligibility: Stage IIIB/IV NSCLC Nonsquamous No prior therapy Prior radiation allowed (N=900) Pemetrexed 500 mg/m 2 Cisplatin 75 mg/m 2 q21d 4 cycles Primary endpoint: PFS Secondary endpoints: OS, patient reported outcomes, safety, response (OS data not yet mature) CR PR SD R A N D O M I Z E Pemetrexed BSC Placebo BSC PD Paz-Ares. ASCO (abstr CRA7510) & ASCO 2012 (A#LBA7507).
30 Survival Probability PARAMOUNT: PFS from Randomization PFS: Primary Efficacy Endpoint PFS: Reassessed at Time of Final OS Survival Probability Pemetrexed Placebo Unadjusted HR: 0.62 ( ) Time (Months) Patients at Risk Pem + BSC Plac+ BSC Patients at Risk Pemetrexed Placebo Unadjusted HR: 0.60 ( ) Time (Months) Pem +BSC Plac + BSC Paz-Ares. ASCO (abstr CRA7510) & ASCO 2012 (A#LBA7507).
31 PARAMOUNT: OS from Randomization
 Induction Response SD (n=280) Pre-randomization PS 1 (n=366) Pre-randomization PS 0 (n=170) Non-smoker (n=116) Smoker (n=419) Male (n=313) Female (n=226) Age <70 (n=447) Age 70")
32 PARAMOUNT: Subgroup PFS Hazard Ratios PFS results were internally consistent; benefit was seen across all subgroups All Randomized Patients (N=539) Stage IV (n=489) Stage IIIB (n=50) Induction Response CR/PR (n=242) Induction Response SD (n=280) Pre-randomization PS 1 (n=366) Pre-randomization PS 0 (n=170) Non-smoker (n=116) Smoker (n=419) Male (n=313) Female (n=226) Age <70 (n=447) Age 70 (n=92) Age <65 (n=350) Age > 65 (n=189) Other Histologic Diagnosis (n=32) Large Cell Carcinoma (n=36) Adenocarcinoma (n=471) Treatment Hazard Ratio (95% CI) Paz-Ares et al, Favors Pemetrexed Favors Placebo

33 PARAMOUNT: OS by Induction Response

34 Efficacy of Maintenance Therapy Results of Recent Phase III Studies Reference n Therapy Primary End Point PFS (HR) OS (HR) Fidias et al, Docetaxel OS Ciuleanu et al, Pemetrexed PFS Belani et al, Gemcitabine OS Cappuzzo et al, Erlotinib PFS Miller et al, Pérol et al, Erlotinib + Bevacizumab Erlotinib vs. Gemcitabine PFS PFS Takeda et al, Gefitinib OS Paz-Ares et al, Pemetrexed PFS Zhang et al, Gefitinib PFS PFS = progression-free survival; OS = overall survival; HR = hazard ratio; NR = not reported.
35 Comparing Maintenance Therapy Strategies Continuation vs. Maintenance Single Agents vs. Combinations Chemotherapy vs. Targeted Therapies
36 IFCT-GFPC 0502 study design Cisplatin gemcitabine x 4 cycles N=834 PD: off Objective response or stable disease 44% dropoff R* N=464 A B Maintenance treatment Observation N=155 Gemcitabine N=154 PD PD Progression: 2 nd line Pemetrexed Pemetrexed NSCLC Stage IIIB wet IV PS 0-1, years Asymptomatic brain mets allowed Tumor tissue EGFR IHC EGFR mutation C N=155 Erlotinib Primary endpoint: PFS PD Pemetrexed Induction chemo: cisplatin 80mg/m 2 d1 + gemcitabine 1,250mg/m 2 d1, d8 Arm B: gemcitabine 1,250mg/m 2 d1, d8 /3 wks Arm C: erlotinib 150mg daily Pérol, J Clin Oncol 2012 *Stratification factors: gender histology: adenocarcinoma vs other histology smoking status: non-smokers vs current/former smokers center response vs stabilization to induction chemotherapy EGFR = epidermal growth factor receptor IHC = immunohistochemistry; PD = progressive disease
37 IFCT Trial: PFS Benefit with Gemcitabine (Continuation Maintenance Therapy) Pérol, J Clin Oncol 2012
38 IFCT Trial: PFS Benefit with Erlotinib (Switch Maintenance Therapy) Pérol, J Clin Oncol 2012
39 Overall Survival: Maintenance Therapy with Gemcitabine or Erlotinib vs. Observation Gemcitabine (continuation) Erlotinib (switch) No OS benefit, arguably from equalizing effect of subsequent effective therapy Pérol, J Clin Oncol 2012
40 2 nd /3 rd Line Therapies in IFCT-GFPC 0502 Maintenance Arm OBS (n=155) Gem (n=154) Erlotinib (n=155) 2 nd line pemetrexed (%) RR to 2 nd line pemetrexed (%) nd line other (%) rd line Treatment (%) Most commonly used 3 rd line agent Erlotinib Erlotinib Docetaxel Perol M et al J Clin Oncol epub Sept 4, 2012
41 AVAPERL: Continuation Maintenance Therapy with Pemetrexed vs. Pemetrexed/Bevacizumab First-line Adv. NSCLC Non-squamous N = 362 R A N D O M I Z E Cisplatin/Pemetrexed with Bevacizumab 4 cycles Cisplatin/pemetrexed with Bevacizumab 4 cycles If no PD Bev Maint Rx Pem/Bev Maint Rx Median progression-free survival: 6.6 vs months, favoring combination (HR = 0.50; p< 0.001) No new safety issues ESMO 2011


42 AVAPERL: Efficacy Progression-Free Surv from Maintenance Overall Survival
43 Erlotinib Maintenance Therapy Trials in Advanced NSCLC: ATLAS 1 st Line Adv NSCLC Bev Eligible N = 1150 Primary Endpoint: PFS Platinum-based doublet chemo + bevacizumab x 4 cycles if no prog R A N D 1:1 N = 743 (35% drop off) Bev 15 mg/m2 IV Q21d + Erlotinib 150 mg PO daily Until Progression Bev 15 mg/m2 IV Q21d + Placebo150 mg PO daily Until Progression Miler, Proc ASCO 2009

44 Proportion Without Event ATLAS Trial Progression-Free Survival Bev + Placebo (n=373) Bev + Erlotinib (n=370) HR=0.722 ( ) Log-rank P= No. of patients at risk: Progression-Free Survival (months) Bev+Placebo Bev+Erlotinib Miler, Proc ASCO 2009
45 Kabbinivar, Proc ASCO 2010 ATLAS Trial Overall Survival
46 POINT BREAK Trial: ECOG 4599 vs. ABC/ Patel Regimen Primary investigator: Dr. Jyoti Patel, Northwestern First-line Adv. NSCLC Non-squamous N= 939 R A N D O M I Z E Primary endpoint: Overall survival Carboplatin/paclitaxel Bevacizumab 4* cycles Carboplatin/pemetrexed Bevacizumab 4* cycles If no PD Bev Maint Rx Pem/Bev Maint Rx N = 590 (37% drop off)


47 PointBreak: Overall Results From First Line Progression-Free Survival Overall Survival More neuropathy, alopecia w/paclitaxel; more heme toxicity w/pem Patel, Chicago Multidisciplinary Symposium in Thoracic Onc


48 PointBreak: Results From Maintenance (63%) Progression-Free Survival Overall Survival Pem/Bev combination appears more effective in maintenance setting Patel, Chicago Multidisciplinary Symposium in Thoracic Onc
49 ECOG 5508 Trial of Maintenance Therapy Options in Advanced NSCLC Principal Investigator: Suresh Ramalingam Advanced NSCLC bev eligible PS 0-1 Carbo AUC 6 Paclitaxel 200 mg/m2 Bevacizumab 15 mg/kg IV day 1 q 21days x 4 cycles if no PD R A N D O M I Z E Bevacizumab 15 mg/kg q21days to PD Pem 500 mg/m2 q21days to PD Pem 500 mg/m2 Bevacizumab 15 mg/kg q21days to PD PD = progressive disease

50 Rates of Crossover and Administration of Any 2 nd Line Agent in The Major Maintenance Trials Edelman et al. J Thorac Oncol 7:1331, International Association for the Study of Lung Cancer. Published by Lippincott Williams & Wilkins, Inc. 2
51 Considerations in Evaluating the Role of Maintenance Therapy in Advanced NSCLC Exposure to effective agents and 2 nd line therapy was compromised on control arms of many trials Patients on control arms had to wait for RECIST defined PD before therapy could be instituted These two factors may have predisposed the control arms on many trials to have poorer survival When 2 nd line therapy defined in the trial design (Perol), survival is equivalent It is probably exposure not timing that benefits patients Do we improve QoL without undue toxicity?
52 QoL in Maintenance Therapy Author Year Instrument Overall Specific Findings Fidias 2008 LCSS Ciuleanu 2009 LCSS Cappuzzo 2009 FACT-L Better (not sign 0.76) No difference TTD No difference TTD - Delayed in worsening of 2/6 symptoms (pain, hemoptysis) Delayed time to pain & analgesic use (HR 0.96) No diff in time to cough and dyspnea Miller Perol nr nr Paz Ares 2011 EQ5D No difference - Zhang 2011 FACT-L Better Delayed median time to worsening in lung cancer symptoms TTD time to deterioration in QoL
53 Toxicity in Switch Maintenance Trials EJC Zhang et al. Chest 140 July, 2011
54 Conclusions - Management after 4-6 Cycles of Therapy Continuation or switch maintenance appear comparable Maximize benefit from each agent before discontinuing it (favor continuation over switch in patients doing well) In bev-eligible patients, PFS but not OS appears better with combinations than bev alone Duration of maintenance unclear (pay attention to gr 1-2 toxicities which adversely effect QoL) Survival benefit with erlotinib is NOT limited to EGFR mutants and is only maintenance agent studied with bev A treatment break is still reasonable and can be therapeutic IF patients get treated later Maintenance an option.but not a mandate
55 So What Do I Do In My Practice In non-squames after 4 cycles If I use bev, I generally continue it until PD If I use pem with bev, I think I may do more bev alone If I do not use bev, I generally use Pem-based therapy and give the option of continuation Pem or OBS but reassess q4 cycles In squames after 4 cycles I generally offer a treatment break but if SD PD I recommend maintenance with erlotinib or doectaxel
Maintenance paradigm in non-squamous NSCLC
 Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Slide 1. Slide 2 Maintenance Therapy Options. Slide 3. Maintenance Therapy in the Management of Non-Small Cell Lung Cancer. Maintenance Chemotherapy
 Slide 1 Maintenance Therapy in the Management of Non-Small Cell Lung Cancer Frances A Shepherd, MD FRCPC Scott Taylor Chair in Lung Cancer Research Princess Margaret Hospital, Professor of Medicine, University
Slide 1 Maintenance Therapy in the Management of Non-Small Cell Lung Cancer Frances A Shepherd, MD FRCPC Scott Taylor Chair in Lung Cancer Research Princess Margaret Hospital, Professor of Medicine, University
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse?
 Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf
 MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
MAINTENANCE TREATMENT CHEMO MAINTENANCE OR TARGETED OF BOTH? Martin Reck Department of Thoracic Oncology LungenClinic Grosshansdorf OUTLINE Background and Concept Switch Maintenance Continuation Maintenance
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer
 Non-Small Cell Lung Cancer") Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Maintenance Treatment for Advanced NSCLC. Yvonne Summers PhD, FRCP ESMO Preceptorship Programme March 2017
 Maintenance Treatment for Advanced NSCLC Yvonne Summers PhD, FRCP ESMO Preceptorship Programme March 2017 Milestones in the Palliative Systemic Treatment of NSCLC 1990 2000 2010 2015 Platinum based Chemotherapy
Maintenance Treatment for Advanced NSCLC Yvonne Summers PhD, FRCP ESMO Preceptorship Programme March 2017 Milestones in the Palliative Systemic Treatment of NSCLC 1990 2000 2010 2015 Platinum based Chemotherapy
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Maintenance Treatment of Advanced NSCLC
 Maintenance Treatment of Advanced NSCLC Giorgio V. Scagliotti University of Torino Department of Clinical & Biological Sciences giorgio.scagliotti@unito.it UNIVERSTY OF TORINO DEPT. OF OF Maintenance /Consolidation/Sequencing
Maintenance Treatment of Advanced NSCLC Giorgio V. Scagliotti University of Torino Department of Clinical & Biological Sciences giorgio.scagliotti@unito.it UNIVERSTY OF TORINO DEPT. OF OF Maintenance /Consolidation/Sequencing
Sao Paulo, Abril 2014
 Tratamento de Manutencao e outros Sao Paulo, Abril 2014 Rogerio C. Lilenbaum, M.D. Professor of Medicine Yale Cancer Center Chief Medical Officer Smilow Cancer Hospital What Is Maintenance Therapy? Use
Tratamento de Manutencao e outros Sao Paulo, Abril 2014 Rogerio C. Lilenbaum, M.D. Professor of Medicine Yale Cancer Center Chief Medical Officer Smilow Cancer Hospital What Is Maintenance Therapy? Use
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC. Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy
 PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
PROGNOSTIC AND PREDICTIVE BIOMARKERS IN NSCLC Federico Cappuzzo Istituto Toscano Tumori Ospedale Civile-Livorno Italy Prognostic versus predictive Prognostic: In presence of the biomarker patient outcome
1st line chemotherapy and contribution of targeted agents
 ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER 1st line chemotherapy and contribution of targeted agents Yi-Long Wu Guangdong Lung Cancer Institute Guangdong General Hospital Guangdong Academy
ESMO PRECEPTORSHIP PROGRAMME NON-SM ALL-CELL LUNG CANCER 1st line chemotherapy and contribution of targeted agents Yi-Long Wu Guangdong Lung Cancer Institute Guangdong General Hospital Guangdong Academy
2 nd line Therapy and Beyond NSCLC. Alan Sandler, M.D. Oregon Health & Science University
 2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
11/21/2009. Erlotinib in KRAS Mt patients. Bevacizumab in Squamous patients
 Decision-Making in Non-Small Cell Lung Cancer (NSCLC): Moving from Empiric to Personalized & Molecular-based Therapy David R. Gandara, MD University of California Davis Cancer Center Disclosures Research
Decision-Making in Non-Small Cell Lung Cancer (NSCLC): Moving from Empiric to Personalized & Molecular-based Therapy David R. Gandara, MD University of California Davis Cancer Center Disclosures Research
Personalized maintenance therapy in advanced non-small cell lung cancer
 China Lung Cancer Research Highlight Personalized maintenance therapy in advanced non-small cell lung cancer Kazuhiro Asami, Kyoichi Okishio, Tomoya Kawaguchi, Shinji Atagi Department of Clinical Oncology,
China Lung Cancer Research Highlight Personalized maintenance therapy in advanced non-small cell lung cancer Kazuhiro Asami, Kyoichi Okishio, Tomoya Kawaguchi, Shinji Atagi Department of Clinical Oncology,
1st-line Chemotherapy for Advanced disease
 SESSION 3: ADVANCED NSCLC 1st-line Chemotherapy for Advanced disease JY DOUILLARD MD PhD Professor Emeritus in Medical Oncology Chief Medical Officer (CMO) ESMO Lugano CH Percent Survival HISTORICAL BASIS
SESSION 3: ADVANCED NSCLC 1st-line Chemotherapy for Advanced disease JY DOUILLARD MD PhD Professor Emeritus in Medical Oncology Chief Medical Officer (CMO) ESMO Lugano CH Percent Survival HISTORICAL BASIS
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
ASCO Highlights Lung Cancer
 ASCO Highlights Lung Cancer Anne S. Tsao, M.D. Director, Mesothelioma Program Assistant Professor July 11, 2009 The University of Texas MD ANDERSON CANCER CENTER Department of Thoracic/Head & Neck Medical
ASCO Highlights Lung Cancer Anne S. Tsao, M.D. Director, Mesothelioma Program Assistant Professor July 11, 2009 The University of Texas MD ANDERSON CANCER CENTER Department of Thoracic/Head & Neck Medical
in combination with cisplatin as first-line doublet 3 as maintenance agent following non-pemetrexed platinum doublet 4
 Overall survival (OS) results from PARAMOUNT study of maintenance plus best supportive care (BSC) versus plus BSC, immediately after induction with - Cisplatin, in patients with advanced Nonsquamous Non-small
Overall survival (OS) results from PARAMOUNT study of maintenance plus best supportive care (BSC) versus plus BSC, immediately after induction with - Cisplatin, in patients with advanced Nonsquamous Non-small
EGFR MUTATIONS: EGFR PATHWAY AND SELECTION OF FIRST-LINE THERAPY WITH TYROSINE KINASE INHIBITORS
 EGFR MUTATIONS: EGFR PATHWAY AND SELECTION OF FIRST-LINE THERAPY WITH TYROSINE KINASE INHIBITORS Federico Cappuzzo Istituto Clinico Humanitas IRCCS Rozzano-Italy The EGFR/HER Family Ligand binding domain
EGFR MUTATIONS: EGFR PATHWAY AND SELECTION OF FIRST-LINE THERAPY WITH TYROSINE KINASE INHIBITORS Federico Cappuzzo Istituto Clinico Humanitas IRCCS Rozzano-Italy The EGFR/HER Family Ligand binding domain
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? VEGF Is the Only Angiogenic Factor Present Throughout the Tumor Life Cycle
 Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Background. Azzoli CG et al. J Clin Oncol 2009; 2 Sandler A et al. NEJM 2006; 3
 A Randomized, Open-Label, Phase III, Superiority Study of Pemetrexed(Pem) + Carboplatin(Cb) + Bevacizumab(Bev) Followed by Maintenance Pem + Bev versus Paclitaxel (Pac)+Cb+Bev Followed by Maintenance Bev
A Randomized, Open-Label, Phase III, Superiority Study of Pemetrexed(Pem) + Carboplatin(Cb) + Bevacizumab(Bev) Followed by Maintenance Pem + Bev versus Paclitaxel (Pac)+Cb+Bev Followed by Maintenance Bev
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Antiangiogenici in combinazione a chemioterapia in prima linea: bevacizumab
 Micro-ambiente tumorale. Antiangiogenici e immunoterapia: miti e realtà Milano, 11 Ottobre 2016 Antiangiogenici in combinazione a chemioterapia in prima linea: bevacizumab Francesco Grossi U.O.S. Tumori
Micro-ambiente tumorale. Antiangiogenici e immunoterapia: miti e realtà Milano, 11 Ottobre 2016 Antiangiogenici in combinazione a chemioterapia in prima linea: bevacizumab Francesco Grossi U.O.S. Tumori
ESMO THE CHRISTIE PRECEPTORSHIP PROGRAMME. 1 st line chemotherapy for advanced NSCLC. Benjamin BESSE, MD, PhD Head Dpt of Cancer Medicine
 ESMO THE CHRISTIE PRECEPTORSHIP PROGRAMME 1 st line chemotherapy for advanced NSCLC Benjamin BESSE, MD, PhD Head Dpt of Cancer Medicine 2017 PD-L1 50% Pembrolizuma b [I,A] Courtesy of J.Remon Adapted from
ESMO THE CHRISTIE PRECEPTORSHIP PROGRAMME 1 st line chemotherapy for advanced NSCLC Benjamin BESSE, MD, PhD Head Dpt of Cancer Medicine 2017 PD-L1 50% Pembrolizuma b [I,A] Courtesy of J.Remon Adapted from
Nivolumab: esperienze italiane nel carcinoma polmonare avanzato
 NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC avanzato: quali novità nel 2018? Negrar, 30 Ottobre 2018 Nivolumab: esperienze italiane nel carcinoma polmonare avanzato Francesco Grossi UOC Oncologia Medica Fondazione IRCCS Ca Granda Ospedale
NSCLC: Terapia medica nella fase avanzata. Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza
 NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
NSCLC: Terapia medica nella fase avanzata Paolo Bidoli S.C. Oncologia Medica H S. Gerardo Monza First-line Second-line Third-line Not approved CT AND SILENT APPROVAL Docetaxel 1999 Paclitaxel Gemcitabine
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Maintenance therapies in advanced non-small-cell lung cancer
 Review Maintenance therapies in advanced non-small-cell lung cancer Advanced non-small-cell lung cancer is treated with upfront platinum doublet chemotherapy, which produces moderate survival improvements.
Review Maintenance therapies in advanced non-small-cell lung cancer Advanced non-small-cell lung cancer is treated with upfront platinum doublet chemotherapy, which produces moderate survival improvements.
Is there a role for maintenance therapy in advanced non-small-cell lung cancer?
 Review Is there a role for maintenance therapy in advanced non-small-cell lung cancer? Cesare Gridelli*1, Paolo Maione1, Antonio Rossi1, Clorinda Schettino1, Maria Anna Bareschino1, Paola Claudia Sacco1,
Review Is there a role for maintenance therapy in advanced non-small-cell lung cancer? Cesare Gridelli*1, Paolo Maione1, Antonio Rossi1, Clorinda Schettino1, Maria Anna Bareschino1, Paola Claudia Sacco1,
Cytotoxic Maintenance Therapy in Advanced NSCLC: Update State of the Art or State of Confusion
 Cytotoxic Maintenance Therapy in Advanced NSCLC: Update State of the Art or State of Confusion Corey J Langer MD, FACP Director Thoracic Oncology Abramson Cancer Center Professor of Medicine Hematology-Oncology
Cytotoxic Maintenance Therapy in Advanced NSCLC: Update State of the Art or State of Confusion Corey J Langer MD, FACP Director Thoracic Oncology Abramson Cancer Center Professor of Medicine Hematology-Oncology
1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC
 1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC Dr Ross Soo, FRACP National University Cancer Institute, Singapore National University Health System Cancer Science
1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC Dr Ross Soo, FRACP National University Cancer Institute, Singapore National University Health System Cancer Science
Histology: Its Influence on Therapeutic Decision Making
 Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
Histology: Its Influence on Therapeutic Decision Making Mark A. Socinski, MD Professor of Medicine and Thoracic Surgery Director, Lung Cancer Section, Division of Hematology/Oncology Co-Director, UPMC
VEGF-Inhibitors in NSCLC. Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany
 VEGF-Inhibitors in NSCLC Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Conflicts of interest Advisory Board: AstraZeneca Bristol-Myers Squibb Daiichi Sankyo Eli Lilly Merck
VEGF-Inhibitors in NSCLC Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Conflicts of interest Advisory Board: AstraZeneca Bristol-Myers Squibb Daiichi Sankyo Eli Lilly Merck
Combined Modality Therapy State of the Art. Everett E. Vokes The University of Chicago
 Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
INMUNOTERAPIA I. Dra. Virginia Calvo
 INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
INMUNOTERAPIA I Dra. Virginia Calvo LBA62. Health-related quality of life (HRQoL) for Pembrolizumab or placebo plus Carboplatin and Paclitaxel or nab-paclitaxel in patients with metastatic squamous NSCLC:
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
LUNG CANCER TREATMENT: AN OVERVIEW
 LUNG CANCER TREATMENT: AN OVERVIEW KONSTANTINOS N. SYRIGOS, M.D., Ph.D. Αναπλ. Καθηγητής Παθολογίας-Ογκολογίας, Ιατρικής Σχολής Αθηνών. Διευθυντής Ογκολογικής Μονάδας, Νοσ. «Η Σωτηρία». Visiting Professor
LUNG CANCER TREATMENT: AN OVERVIEW KONSTANTINOS N. SYRIGOS, M.D., Ph.D. Αναπλ. Καθηγητής Παθολογίας-Ογκολογίας, Ιατρικής Σχολής Αθηνών. Διευθυντής Ογκολογικής Μονάδας, Νοσ. «Η Σωτηρία». Visiting Professor
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
PRACTICE GUIDELINE SERIES
 ELLIS et al. PRACTICE GUIDELINE SERIES The role of the epidermal growth factor receptor tyrosine kinase inhibitors as therapy for advanced, metastatic, and recurrent nonsmall-cell lung cancer: a Canadian
ELLIS et al. PRACTICE GUIDELINE SERIES The role of the epidermal growth factor receptor tyrosine kinase inhibitors as therapy for advanced, metastatic, and recurrent nonsmall-cell lung cancer: a Canadian
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW. Erlotinib for the third or fourth-line treatment of NSCLC January 2012
 Disease background LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Erlotinib for the third or fourth-line treatment of NSCLC January 2012 Lung cancer is the second most common cancer in the UK (after breast),
Disease background LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Erlotinib for the third or fourth-line treatment of NSCLC January 2012 Lung cancer is the second most common cancer in the UK (after breast),
Two Cycles of Chemoradiation: 2 Cycles is Enough. Concurrent Chemotherapy / RT Regimens
 1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
Strategies in the therapy of advanced NSCLC SAMO Winter-Conference 2008 on Chest tumors
 Strategies in the therapy of advanced NSCLC SAMO Winter-Conference 2008 on Chest tumors Miklos Pless Medical Oncology Kantonsspital Winterthur 2 Setting the stage. 1995: Chemotherapy works! Meta-Analysis
Strategies in the therapy of advanced NSCLC SAMO Winter-Conference 2008 on Chest tumors Miklos Pless Medical Oncology Kantonsspital Winterthur 2 Setting the stage. 1995: Chemotherapy works! Meta-Analysis
Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC)
") Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC) Suresh S. Ramalingam, MD Director of Thoracic Oncology Associate Professor Emory University Atlanta,
Exploring Personalized Therapy for First Line Treatment of Advanced Non-Small Cell Lung Cancer (NSCLC) Suresh S. Ramalingam, MD Director of Thoracic Oncology Associate Professor Emory University Atlanta,
Second-line treatment for advanced NSCLC
 UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Life was so simple back in 2008 Di
UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY Life was so simple back in 2008 Di
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Overview of Lung Cancer :Perspectives from Cancer Genotype. Ji-Youn Han, MD, PhD. Center for Lung Cancer National Cancer Center
 Overview of Lung Cancer :Perspectives from Cancer Genotype Ji-Youn Han, MD, PhD. Center for Lung Cancer National Cancer Center Histologic classification of lung cancer Therapeutic plateau reached with
Overview of Lung Cancer :Perspectives from Cancer Genotype Ji-Youn Han, MD, PhD. Center for Lung Cancer National Cancer Center Histologic classification of lung cancer Therapeutic plateau reached with
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
LUNG CANCER. Başak Oyan-Uluç, MD Yeditepe University Hospital Medical Oncology. Best of ASCO, İstanbul
 LUNG CANCER Başak Oyan-Uluç, MD Yeditepe University Hospital Medical Oncology Best of ASCO, İstanbul 2012 23.6.2012 Treatment of Metastatic NSCLC EGFR targetted treatments 1st line: EGFR-mutated: Afatinib
LUNG CANCER Başak Oyan-Uluç, MD Yeditepe University Hospital Medical Oncology Best of ASCO, İstanbul 2012 23.6.2012 Treatment of Metastatic NSCLC EGFR targetted treatments 1st line: EGFR-mutated: Afatinib
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
NSCLC with squamous histology: Current treatment and new options on horizon
 NSCLC with squamous histology: Current treatment and new options on horizon Prof. Yasser A.Kader Professor of Oncology Faculty of Medicine, Cairo University 2015 Lung Cancer: Incidence and Mortality New
NSCLC with squamous histology: Current treatment and new options on horizon Prof. Yasser A.Kader Professor of Oncology Faculty of Medicine, Cairo University 2015 Lung Cancer: Incidence and Mortality New
2012 Chicago Multidisciplinary Symposium in Thoracic Oncology September 6-8, 2012 Friday, September 7, News Briefing 7:15 a.m.
 2012 Chicago Multidisciplinary Symposium in Thoracic Oncology September 6-8, 2012 Friday, September 7, News Briefing 7:15 a.m. Central time Moderated by Heather Wakelee, MD Stanford University Stanford,
2012 Chicago Multidisciplinary Symposium in Thoracic Oncology September 6-8, 2012 Friday, September 7, News Briefing 7:15 a.m. Central time Moderated by Heather Wakelee, MD Stanford University Stanford,
Sequencing in EGFR-Mutated NSCLC: Does Order Matter?
 Sequencing in EGFR-Mutated NSCLC: Does Order Matter? Maximilian J. Hochmair, MD Otto Wagner Hospital Vienna, Austria Disclosures Honoraria: AstraZeneca, AbbVie, Pfizer, Boehringer Ingelheim, Roche, MSD,
Sequencing in EGFR-Mutated NSCLC: Does Order Matter? Maximilian J. Hochmair, MD Otto Wagner Hospital Vienna, Austria Disclosures Honoraria: AstraZeneca, AbbVie, Pfizer, Boehringer Ingelheim, Roche, MSD,
K-Ras signalling in NSCLC
 Targeting the Ras-Raf-Mek-Erk pathway Egbert F. Smit MD PhD Dept. Pulmonary Diseases Vrije Universiteit VU Medical Centre Amsterdam, The Netherlands K-Ras signalling in NSCLC Sun et al. Nature Rev. Cancer
Targeting the Ras-Raf-Mek-Erk pathway Egbert F. Smit MD PhD Dept. Pulmonary Diseases Vrije Universiteit VU Medical Centre Amsterdam, The Netherlands K-Ras signalling in NSCLC Sun et al. Nature Rev. Cancer
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER. Virginie Westeel Chest Disease Department University Hospital Besançon, France
 PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
INNOVATION IN LUNG CANCER MANAGEMENT. Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy
 INNOVATION IN LUNG CANCER MANAGEMENT Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy FIRST-LINE THERAPY FOR METASTATIC NSCLC IN 216 Stratification for EGFR, ALK
INNOVATION IN LUNG CANCER MANAGEMENT Federico Cappuzzo Department of Oncology-Hematology, AUSL della Romagna, Ravenna, Italy FIRST-LINE THERAPY FOR METASTATIC NSCLC IN 216 Stratification for EGFR, ALK
Second-line treatment for advanced NSCLC
 Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY DISCLOSURE OF INTEREST Speaker Bureau: Eli Lilly, MSD, BI, BMS, Roche, AZ UNIVERSITY
Second-line treatment for advanced NSCLC Silvia Novello silvia.novello@unito.it UNIVERSITY OF TORINO DEPARTMENT OF ONCOLOGY DISCLOSURE OF INTEREST Speaker Bureau: Eli Lilly, MSD, BI, BMS, Roche, AZ UNIVERSITY
New Options for Achieving Individualized Approaches to Non-Small Cell Lung Cancer (NSCLC) Management
 Management") New Options for Achieving Individualized Approaches to Non-Small Cell Lung Cancer (NSCLC) Management Ramaswamy Govindan, MD Director Professor of Medicine Director, Thoracic Oncology Program Department
New Options for Achieving Individualized Approaches to Non-Small Cell Lung Cancer (NSCLC) Management Ramaswamy Govindan, MD Director Professor of Medicine Director, Thoracic Oncology Program Department
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer.
 Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Stage III NSCLC: Overview
 Locally Advanced NSCLC: New Concepts in Combined Modality Therapy NSCLC: Stage Distribution Randeep Sangha, MD Visiting Assistant Professor UC Davis Cancer Center Sacramento, CA Stage III NSCLC: Overview
Locally Advanced NSCLC: New Concepts in Combined Modality Therapy NSCLC: Stage Distribution Randeep Sangha, MD Visiting Assistant Professor UC Davis Cancer Center Sacramento, CA Stage III NSCLC: Overview
Monoclonal Antibodies in the Management of Non-Small Cell Lung Cancer (NSCLC): 2016 Update Angioinhibitors and EGFR MAbs
: 2016 Update Angioinhibitors and EGFR MAbs") Monoclonal Antibodies in the Management of Non-Small Cell Lung Cancer (NSCLC): 2016 Update Angioinhibitors and EGFR MAbs Corey J Langer, MD, FACP Director Thoracic Oncology Abramson Cancer Center Professor
Monoclonal Antibodies in the Management of Non-Small Cell Lung Cancer (NSCLC): 2016 Update Angioinhibitors and EGFR MAbs Corey J Langer, MD, FACP Director Thoracic Oncology Abramson Cancer Center Professor
Changing demographics of smoking and its effects during therapy
 Changing demographics of smoking and its effects during therapy Egbert F. Smit MD PhD. Dept. Pulmonary Diseases, Vrije Universiteit Medical Centre, Amsterdam, The Netherlands Smoking prevalence adults
Changing demographics of smoking and its effects during therapy Egbert F. Smit MD PhD. Dept. Pulmonary Diseases, Vrije Universiteit Medical Centre, Amsterdam, The Netherlands Smoking prevalence adults
Tratamiento de la enfermedad avanzada en cáncer de pulmón
 Tratamiento de la enfermedad avanzada en cáncer de pulmón S. Ponce Aix! S. Oncología Médica Hospital Universitario 12 de Octubre Madrid Survival by stage NSCLC Stage Distribution NSCLC Stage 5-year Survival
Tratamiento de la enfermedad avanzada en cáncer de pulmón S. Ponce Aix! S. Oncología Médica Hospital Universitario 12 de Octubre Madrid Survival by stage NSCLC Stage Distribution NSCLC Stage 5-year Survival
Personalized Medicine for Advanced NSCLC in East Asia
 Personalized Medicine for Advanced NSCLC in East Asia - Update treatment strategy for NSCLC based on Japanese clinical practice guideline - Masahiro Tsuboi, M.D., Ph.D. Associate-professor, School of Medicine,
Personalized Medicine for Advanced NSCLC in East Asia - Update treatment strategy for NSCLC based on Japanese clinical practice guideline - Masahiro Tsuboi, M.D., Ph.D. Associate-professor, School of Medicine,
Lung cancer is the leading cause of cancer-related death in the
 ORIGINAL ARTICLE Bevacizumab Maintenance in Patients with Advanced Non Small-Cell Lung Cancer, Clinical Patterns, and Outcomes in the Eastern Cooperative Oncology Group 4599 Study Results of An Exploratory
ORIGINAL ARTICLE Bevacizumab Maintenance in Patients with Advanced Non Small-Cell Lung Cancer, Clinical Patterns, and Outcomes in the Eastern Cooperative Oncology Group 4599 Study Results of An Exploratory
Immunoterapia di 1 linea Evidenze e Prospettive Future
 Immunoterapia di 1 linea Evidenze e Prospettive Future Sara Pilotto Oncologia Medica, Dipart. di Medicina, Università di Verona, A.O.U.I. Verona sara.pilotto@univr.it Negrar, 30 ottobre 2018 Disclosures
Immunoterapia di 1 linea Evidenze e Prospettive Future Sara Pilotto Oncologia Medica, Dipart. di Medicina, Università di Verona, A.O.U.I. Verona sara.pilotto@univr.it Negrar, 30 ottobre 2018 Disclosures
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Data on first-line Overcoming T790M
Medical Oncology: State of the Art Therapy in Advanced NSCLC: 2011 looking toward 2015
 Medical Oncology: State of the Art Therapy in Advanced NSCLC: 2011 looking toward 2015 David R. Gandara, MD University of California Davis Cancer Center Algorithm for Therapy of Advanced Stage NSCLC: 2009
Medical Oncology: State of the Art Therapy in Advanced NSCLC: 2011 looking toward 2015 David R. Gandara, MD University of California Davis Cancer Center Algorithm for Therapy of Advanced Stage NSCLC: 2009
Cancer Cell Research 14 (2017)
") Available at http:// www.cancercellresearch.org ISSN 2161-2609 Efficacy and safety of bevacizumab for patients with advanced non-small cell lung cancer Ping Xu, Hongmei Li*, Xiaoyan Zhang Department of
Available at http:// www.cancercellresearch.org ISSN 2161-2609 Efficacy and safety of bevacizumab for patients with advanced non-small cell lung cancer Ping Xu, Hongmei Li*, Xiaoyan Zhang Department of
Joachim Aerts Erasmus MC Rotterdam, Netherlands. Drawing the map: molecular characterization of NSCLC
 Joachim Aerts Erasmus MC Rotterdam, Netherlands Drawing the map: molecular characterization of NSCLC Disclosures Honoraria for advisory board/consultancy/speakers fee Eli Lilly Roche Boehringer Ingelheim
Joachim Aerts Erasmus MC Rotterdam, Netherlands Drawing the map: molecular characterization of NSCLC Disclosures Honoraria for advisory board/consultancy/speakers fee Eli Lilly Roche Boehringer Ingelheim
Treatment of EGFR-Mutation+ NSCLC in 1st- and 2nd-Line
 Treatment of EGFR-Mutation+ NSCLC in 1st- and 2nd-Line Martin Reck David F. Heigener Department of Thoracic Oncology Hospital Grosshansdorf Germany Identification of driver mutation in tumor specimens
Treatment of EGFR-Mutation+ NSCLC in 1st- and 2nd-Line Martin Reck David F. Heigener Department of Thoracic Oncology Hospital Grosshansdorf Germany Identification of driver mutation in tumor specimens
Platinum-containing first-line chemotherapy has improved
 Original Article PARAMOUNT: Descriptive Subgroup Analyses of Final Overall Survival for the Phase III Study of Maintenance Pemetrexed versus Placebo Following Induction Treatment with Pemetrexed Plus Cisplatin
Original Article PARAMOUNT: Descriptive Subgroup Analyses of Final Overall Survival for the Phase III Study of Maintenance Pemetrexed versus Placebo Following Induction Treatment with Pemetrexed Plus Cisplatin
Ludger Sellmann 1, Klaus Fenchel 2, Wolfram C. M. Dempke 3,4. Editorial
 Editorial Improved overall survival following tyrosine kinase inhibitor treatment in advanced or metastatic non-small-cell lung cancer the Holy Grail in cancer treatment? Ludger Sellmann 1, Klaus Fenchel
Editorial Improved overall survival following tyrosine kinase inhibitor treatment in advanced or metastatic non-small-cell lung cancer the Holy Grail in cancer treatment? Ludger Sellmann 1, Klaus Fenchel
Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement. Reference Slides Introduction
 Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement Reference Slides Introduction EML4-ALK Fusion Oncogene Key Driver in 3% to 7% NSCLC Inversion or Translocation
Do You Think Like the Experts? Refining the Management of Advanced NSCLC With ALK Rearrangement Reference Slides Introduction EML4-ALK Fusion Oncogene Key Driver in 3% to 7% NSCLC Inversion or Translocation
Treatment of advanced NSCLC in the elderly. Cesare Gridelli Division of Medical Oncology S.G. Moscati Hospital Avellino (Italy)
") Treatment of advanced NSCLC in the elderly Cesare Gridelli Division of Medical Oncology S.G. Moscati Hospital Avellino (Italy) Most cancer patients are aged >65 years Ovary Breast NHL Corpus uteri Leukaemias
Treatment of advanced NSCLC in the elderly Cesare Gridelli Division of Medical Oncology S.G. Moscati Hospital Avellino (Italy) Most cancer patients are aged >65 years Ovary Breast NHL Corpus uteri Leukaemias
Angiogenesis and tumor growth
 Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Nivolumab (Opdivo) for Non-Small Cell Lung Cancer April 1, 2016
 for Non-Small Cell Lung Cancer April 1, 2016") pan-canadian Oncology Drug Review Initial Clinical Guidance Report Nivolumab (Opdivo) for Non-Small Cell Lung Cancer April 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Initial Clinical Guidance Report Nivolumab (Opdivo) for Non-Small Cell Lung Cancer April 1, 2016 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007
 Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007 Bruce E. Johnson, MD Dana-Farber Cancer Institute, Brigham and Women s Hospital, and Harvard
Biomarkers of Response to EGFR-TKIs EORTC-NCI-ASCO Meeting on Molecular Markers in Cancer November 17, 2007 Bruce E. Johnson, MD Dana-Farber Cancer Institute, Brigham and Women s Hospital, and Harvard
Lung Cancer: Personalized Approaches to Non-Small Cell and Small Cell Lung Cancer
 Lung Cancer: Personalized Approaches to Non-Small Cell and Small Cell Lung Cancer Speaker: Bruce E. Johnson, MD Chief Clinical Research Officer, Dana-Farber Cancer Institute Professor of Medicine, Harvard
Lung Cancer: Personalized Approaches to Non-Small Cell and Small Cell Lung Cancer Speaker: Bruce E. Johnson, MD Chief Clinical Research Officer, Dana-Farber Cancer Institute Professor of Medicine, Harvard
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
First line erlotinib for NSCLC patients not selected by EGFR mutation: keep carrying the TORCH or time to let the flame die?
 Perspective First line erlotinib for NSCLC patients not selected by EGFR mutation: keep carrying the TORCH or time to let the flame die? Jared Weiss Multidisciplinary Thoracic Oncology Program, Lineberger
Perspective First line erlotinib for NSCLC patients not selected by EGFR mutation: keep carrying the TORCH or time to let the flame die? Jared Weiss Multidisciplinary Thoracic Oncology Program, Lineberger
Is the Neo-adjuvant Approach Better than Adjuvant Approach? Comparative Levels of Evidence: Randomized Trials
 Is the Neo-adjuvant Approach Better than Approach? Virginie Westeel University Hospital Besançon, France Perspectives in Lung Cancer Amsterdam, 5-6 March 2010 Comparative Levels of Evidence: Randomized
Is the Neo-adjuvant Approach Better than Approach? Virginie Westeel University Hospital Besançon, France Perspectives in Lung Cancer Amsterdam, 5-6 March 2010 Comparative Levels of Evidence: Randomized
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
EGFR Mutation-Positive Acquired Resistance: Dominance of T790M
 Treatment of EGFR Mutation-Positive Acquired Resistance: T790M+ or T790M- H. Jack West, MD Swedish Cancer Institute, Seattle, WA EGFR Mutation-Positive Acquired Resistance: Dominance of T790M Yu, Clin
Treatment of EGFR Mutation-Positive Acquired Resistance: T790M+ or T790M- H. Jack West, MD Swedish Cancer Institute, Seattle, WA EGFR Mutation-Positive Acquired Resistance: Dominance of T790M Yu, Clin
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Collaborative Practice in the Management of Patients With Cancer. Non-Small Cell Lung Cancer: Management of Patients on Cytotoxic Chemotherapy
 Collaborative Practice in the Management of Patients With Cancer Non-Small Cell Lung Cancer: Management of Patients on Cytotoxic Chemotherapy Program Chair Beth Eaby-Sandy, MSN, CRNP, OCN Abramson Cancer
Collaborative Practice in the Management of Patients With Cancer Non-Small Cell Lung Cancer: Management of Patients on Cytotoxic Chemotherapy Program Chair Beth Eaby-Sandy, MSN, CRNP, OCN Abramson Cancer
Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung
 Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung Noemi Reguart,MD, PhD Hospital Clinic de Barcelona Barcelona, Spain SC-CRP-02660 Conversations in Oncology 2018 is a standalone
Successes and Challenges in Treating Squamous Cell Carcinoma of the Lung Noemi Reguart,MD, PhD Hospital Clinic de Barcelona Barcelona, Spain SC-CRP-02660 Conversations in Oncology 2018 is a standalone
EGFR Tyrosine Kinase Inhibitors Prolong Overall Survival in EGFR Mutated Non-Small-Cell Lung Cancer Patients with Postsurgical Recurrence
 102 Journal of Cancer Research Updates, 2012, 1, 102-107 EGFR Tyrosine Kinase Inhibitors Prolong Overall Survival in EGFR Mutated Non-Small-Cell Lung Cancer Patients with Postsurgical Recurrence Kenichi
102 Journal of Cancer Research Updates, 2012, 1, 102-107 EGFR Tyrosine Kinase Inhibitors Prolong Overall Survival in EGFR Mutated Non-Small-Cell Lung Cancer Patients with Postsurgical Recurrence Kenichi
Optimal Application of Adjuvant Therapy in NSCLC
 Optimal Application of Adjuvant Therapy in NSCLC Heather Wakelee, MD Stanford University, Stanford Cancer Institute Post 1995 Meta-Analysis : NSCLC Randomized Adjuvant Platinum Trials Trial Stage n Chemo
Optimal Application of Adjuvant Therapy in NSCLC Heather Wakelee, MD Stanford University, Stanford Cancer Institute Post 1995 Meta-Analysis : NSCLC Randomized Adjuvant Platinum Trials Trial Stage n Chemo
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Quale sequenza terapeutica nella malattia EGFR+
 Trattamento della malattia avanzata oncogene-addicted Quale sequenza terapeutica nella malattia EGFR+ Chiara Bennati AUSL della Romagna Ravenna, Italy A matter of fact Outline Can we improve PFS/OS with
Trattamento della malattia avanzata oncogene-addicted Quale sequenza terapeutica nella malattia EGFR+ Chiara Bennati AUSL della Romagna Ravenna, Italy A matter of fact Outline Can we improve PFS/OS with