Medical treatment non-pancreatic NETs
|
|
|
- Melissa Moore
- 5 years ago
- Views:
Transcription


 Leuven,")
1 Medical treatment non-pancreatic NETs Prof Juan Valle Professor and Honorary Consultant Institute of Cancer Sciences University of Manchester The Christie ENETS Centre of Excellence ESMO Preceptorship on GI neuroendocrine tumours (NETs) Leuven, Belgium, November 2014
2 DISCLOSURES Honoraria: Novartis, Ipsen, Pfizer, Keocyt, SIRTex, Celgene Grant Funding: Novartis, AstraZeneca

3 OVERVIEW Therapies for advanced disease Interferon Somatostatin analogues Chemotherapy Targeted therapies PRRT Liver-directed therapies HAE TACE RE surgery etc.
:375-86 2 Detjen et al Gastroenterology 2000 Apr;118(4):735-48 3 Hofland et al J Clin Endocrinol Metab.")
4 Interferon Mechanism of action Binding to type-i IFN receptors 1 Activation of JAK-STAT pathways 1 Stimulation of T-cells 2 Inducing cell-cycle arrest (in G1 and G0) 2 Inhibit angiogenesis 2 Induce up-regulation of somatostatin receptors 3 1 Platanias Nat Rev Immunol May;5(5): Detjen et al Gastroenterology 2000 Apr;118(4): Hofland et al J Clin Endocrinol Metab Sep;84(9):

5 Interferon in NETs Results Symptomatic improvement 30-70% Biochemical response 50-60% Introduced in By studies 679 patients Doses 3-5MU sc x3/week Toxicities flu-like syndrome Fatigue Myelosuppression Auto-immune disorders Depression Radiological response rate 10% Stable disease 70% Limitations Case series Retrospective Heterogeneous Trial methodology 1 Öberg et al. New Engl J Med 1982;309:129 2 Öberg Best Pract Res Clin Gastroenterology 2012;26:
6 Interferon in NETS phase III studies Study Eligibility n Comment Kölby 1 Midgut, post surgery and HAE 35 Octreotide 100µg bd 200µg tds 230 patients planned initially 5YS: 57% vs. 37% (NS) 33 Octreotide 100µg bd 200µg tds + IFN 3-5MU x3/wk Improved PFS: HR 0.28 [95%CI , p=0.008] 1 Kölby et al Br J Surg Jun;90(6): Faiss et al J Clin Oncol Jul 15;21(14): Arnold et al Clin Gastroenterol Hepatol Aug;3(8):761-71
7 Interferon in NETS phase III studies Study Eligibility n Comment Kölby 1 Faiss 2 Midgut, post surgery and HAE Progressive (within 3-months), welldifferentiated GEP 35 Octreotide 100µg bid 200µg tid 230 patients planned initially 5YS: 57% vs. 37% (NS) 33 Octreotide 100µg bid 200µg tid + IFN 3-5MU x3/wk Improved PFS: HR 0.28 [95%CI , p=0.008] 25 Lanreotide 1mg tid No difference in 1-yr progression rate: 56% in all three arms 27 IFN 5MU x3/wk 28 Lanreotide 1mg tid + IFN 5MU x3/wk No difference in RR Combination arm associated with greater reduction of symptoms (p=0.037) 1 Kölby et al Br J Surg Jun;90(6): Faiss et al J Clin Oncol Jul 15;21(14): Arnold et al Clin Gastroenterol Hepatol Aug;3(8):761-71
8 Interferon in NETS phase III studies Study Eligibility n Comment Kölby 1 Faiss 2 Arnold 3 Midgut, post surgery and HAE Progressive (within 3-months), welldifferentiated GEP Progressive, welldifferentiated, GEP 35 Octreotide 100µg bid 200µg tid 230 patients planned initially 5YS: 57% vs. 37% (NS) 33 Octreotide 100µg bid 200µg tid + IFN 3-5MU x3/wk Improved PFS: HR 0.28 [95%CI , p=0.008] 25 Lanreotide 1mg tid No difference in 1-yr progression rate: 56% in all three arms 27 IFN 5MU x3/wk 28 Lanreotide 1mg tid + IFN 5MU x3/wk No difference in RR Combination arm associated with greater reduction of symptoms (p=0.037) 51 Octreotide 200µg tid 250 patients planned initially OS in combination arm Octreotide 200µg tid + IFN 4.5MU x3/wk vs. 35 mo HR 0.82 [95%CI , NS] 1 Kölby et al Br J Surg Jun;90(6): Faiss et al J Clin Oncol Jul 15;21(14): Arnold et al Clin Gastroenterol Hepatol Aug;3(8):761-71
9 CASTOR DOTATATE 177Lu-DOTA octreotate vs. interferon in non-pancreatic gastrointestinal NETs Study Status: Ongoing (not recruiting) Estimated Primary Completion: Oct, 2016 Design: Randomised, parallel, open study assessing the benefit of Peptide Receptor Radionuclide Therapy (PRRT) versus interferon α-2b Patients with non- pancreatic gastrointestinal NETs, somatostatin analogue-resistant disease, ECOG status 1 N=60 Phase 3 RANDOMISATION 177Lu-octreotate infusions in fixed activities of 7,4 GBq each, given 8-11 weeks apart, IV with an amino acid infusion Interferon α-2b 5MU Units SC every second day Primary endpoint: PFS (RECIST) Sponsor: Jules Bordet Institute 177Lu-octreotate is co-infused over minutes 30 minutes after the beginning of the amino acid solution Secondary endpoints: Treatment response, AEs Key Exclusion Criteria: Resectable disease with curative intent at enrolment Prior treatment with interferon Key Implications: This phase 3 study focuses on patients who have progressed on a somatostatin analogue (non-pancreatic NETS), patients were selected by positive uptake on 68 Ga octreotate PET-CT 1. Randomised Phase III of PRRT Versus Interferon (CASTOR). Available at: CASTOR: Carcinoid Tumours After Failure of Somatostatin Analogues
10 SOMATOSTATIN ANALOGUES The median survival of patients diagnosed with NETs and distant metastases was significantly longer in compared to timeframe (SEER database) * Data from an analysis of 35,825 cases of NETS identified in the SEER registries Yao JC et al. J Clin Oncol 2008;26:




11 G protein SHP1 sst 2 NF-KB JNK PI3K GSK3β p53 Zac1 Apoptosis PDK1 Akt Molecular pathway of SSAs mtor p70s6k direct anti-proliferative effect PTPŋ SHP2 Src MAPK sst 2 Cell growth G protein SHP1 p27 PKG sst 5 G protein cgmp sst 2 and sst 5 binding both down-regulate MAPK sst 2 binding mediates P13K/Akt/mTOR pathway and SHP1 signaling Antiproliferative effect also mediated via protein tyrosine phosphatase (PTPase) modulation Theodoropoulou M et al. Cancer Res 2006;66: Florio T et al. Front Biosci 2008;13: Grozinsky-Glasberg S et al. Neuroendocrinology 2008;87:

12 Proposed mechanism of anti-proliferative effect Anti-proliferative effect of octreotide Binding of the somatostatin receptor on tumour cells Systemic effect Direct anti-proliferative effect Indirect anti-proliferative effect Inhibition of cell cycle Inhibition of growth factor effects Proapoptotic effect Inhibition of growth factor and trophic hormones Inhibition of angiogenesis Immune system modulation Susini C & Buscail L. Ann Oncol 2006;17:
13 Early prospective studies suggesting anti-tumour activity of octreotide Anti-tumour activity of octreotide in patients with progressive GEP-NETs Reference Regimen Response Saltz et al Octreotide sc 3 x 200 μg/d (n=34) SD in 50% of patients for 2 27 months Arnold et al Octreotide sc 3 x 200 μg/d (n=52) SD in 37% of patients for 3 60 months Di Bartolomeo et al Arnold et al Panzuto et al Octreotide sc: 3 x 500 μg/d (n=23) Octreotide sc: 3 x 1000 μg/d (n=35) Octreotide sc 200 μg tid (n=51) OR Octreotide sc 200 μg tid + Interferon-α 4.5 x 106 IU tiw (n=54) Octreotide LAR 30 mg/28d (n=20) Lanreotide SR 60 mg/28d (n=11) SD in 47% of patients for 6 32 months PR in 3% of patients No significant difference between treatment arms SD or PR in 45% at 3 months; 28% at 6 months; 18% at 12 months (PR=2%) SD in 45.2% of patients for 3 6 months 1. Saltz L et al. Cancer 1993;72: Arnold R et al. Gut 1996;38: Di Bartolomeo M et al. Cancer 1996;77: Arnold R et al. Clin Gastroenterol Hepatol 2005;3: Panzuto F et al. Ann Oncol 2006;17: SD=stable disease PR=partial response The tiw=three Christie times/week NHS Foundation Trust

14 Summary of non-randomized clinical trials In recent years, accumulating laboratory and clinical data has supported SSAs role as antiproliferative agents. Further research efforts are underway. CR: complete response; PR: partial response; SD: stable disease; PD: progressive disease Adapted from Strosberg J, et al. World J Gastroenterol. 2010;16:
15 Limitations of small studies Many patients have indolent disease ( stable disease ) anyway disease progression not mandated at study entry for all studies Studies included heterogeneous tumour populations NETs were of different organ sites and biological behaviour Heterogeneity with respect to prior therapies, very few treatment-naïve patients Studies were not designed or powered to evaluate tumour control Lack of placebo-control
16 PROMID: evaluation of the antitumour activity of octreotide LAR Phase III randomised, double-blind, placebo-controlled study Patients with mid-gut NETs treatment-naïve histologically confirmed locally inoperable or metastatic well differentiated measurable (CT/MRI) functioning or nonfunctioning RANDOMISATION (1:1) Octreotide LAR 30mg i.m. every 28 days Placebo i.m. every 28 days Treatment continued until tumour progression or death Months Primary endpoint: Time to progression (blinded central review) Secondary endpoints: objective response rate, OS, quality of life, safety Rinke et al. J Clin Oncol 2009;27:
17 PROMID: Patient demographics Octreotide LAR (n=42) Placebo (n=43) Total (n=85) Median age, years (range) 63.5 (38 79) 61.0 (39 82) 62.0 (38 82) Sex male (%) female (%) Time since diagnosis, months (range) 7.5 ( ) 3.3 ( ) 4.3 ( ) Karnofsky score 80 > % 83.3% 11.6% 88.4% 14.1% 85.9% Carcinoid syndrome* 40.5% 37.2% 38.8% ~60% Nonfunctioning Resection of primary 69.1% 62.8% 65.9% Hepatic tumour load 0% 0 10% 10 25% 25 50% 50% 16.7% 59.5% 7.1% 11.9% 4.8% 11.6% 62.8% 4.7% 9.3% 11.6% 14.1% 61.2% 5.9% 10.6% 8.2% ~75% <10% liver involved Octreoscan positive 76.2% 72.1% 74.1% Ki-67 up to 2% 97.6% 93.0% 95.3% ~95% G1 CgA elevated 61.9% 69.8% 65.9% Rinke et al. J Clin Oncol 2009;27: * not requiring octreotide for symptom control
18 PROMID: Pre-planned interim analysis Progression-free survival Event-driven analysis following 64 events Actual events at time of interim analysis: 67 tumour progressions and 16 deaths 85 patients from the planned 162 were enrolled at the time of the interim analysis Octreotide LAR 30 mg resulted in a median TTP of 14.3 months compared to 6.0 months with placebo, p= Rinke et al. J Clin Oncol 2009;27:
 Resected primary (P<0.")

19 PROMID: Exploratory sub-groups Greatest benefit was seen in patients with Hepatic tumour load 10% (P<0.0009) Resected primary (P<0.0104) KP >80 Octreotide LAR 30mg provided improved TTP Functioning or non-functioning NETs Elevated or non-elevated CgA Any age Arnold R. Presented at ASCO-GI 2009
20 Limitations of PROMID Balance of study arms Longer time since diagnosis in LAR vs. placebo (7.5 vs. 3.3 mo, p=0.0096) In practice, most patients do not have <10% liver involvement Not effective? vs. sub-optimal dose? Vast majority (97.6%) of patients had Ki-67: 2% What about intermediate grade (Ki67: 2-20%) 76% of patients had positive octreotide scan correlation not described No disease progression mandated at study entry: What does stable disease mean?
21 Controlled study of Lanreotide Anti-proliferative Response In NET (CLARINET) N=204 Patients with mid-gut and pancreatic NETs histologically confirmed locally inoperable or metastatic measurable (CT/MRI) well / mod differentiated non-functioning only Prior therapy allowed RANDOMISATION (1:1) Lanreotide Autogel 120 mg s.c. every 28 days Placebo s.c. every 28 days Treatment continued until tumour progression or death Primary end-point: Progression-free survival Secondary endpoints: AE, PK, QoL, CgA ClinicalTrials.gov identifier: NCT Caplin et al N Engl J Med 2014;371:



22 CLARINET study population baseline characteristics Most tumours originated in the pancreas or small intestine Most tumours were stable in size at study entry and most patients have had no previous tumour therapy
23 CLARINET study primary endpoint

24 CLARINET study primary endpoint
25 Differences in study design PROMID CLARINET COOPERATE-2 Somatostatin analogue Octreotide Lanreotide Pasireotide Population Midgut All GEP pnet Progression at baseline No No Yes Prior therapy received 0% 15%? Grade 1 95% 69%? Grade 2 5% 30% (Ki67: 2-10%)?

26 Design: SIG-NET Pasireotide LAR vs. Octreotide LAR metastatic carcinoid tumour Multicentre, randomised, double-blind, parallel group study comparing the efficacy of pasireotide LAR and octreotide LAR in metastatic carcinoid tumour Patients with carcinoid tumours and symptoms (diarrhoea and/or flushing) that are not adequately controlled by somatostatin analogues (SSTa) N=110 RANDOMISATION 1:1 Pasireotide LAR 60 mg IM once every 28 days for 6 months with dose decreased to 40 mg for tolerability (n= 53) Primary endpoint: Symptom response Phase 3 Octreotide LAR 40 mg IM once every 28 days for 6 months with dose decreased to 30 mg for tolerability (n=57) Sponsor: Novartis In addition to LAR treatment, pasireotide SC bid or octreotide SC tid rescue as needed to end of study in 2 treatment groups respectively Secondary endpoints: Symptom response, TRR, DCR, QoL, DoR Key Exclusion Criteria: Patients receiving radiolabeled SSTa within 3 months or cytotoxic chemotherapy or interferon therapy within 4 weeks Patients on anti-diabetics, poorly controlled blood glucose, malabsorption syndrome, cholelithiasis, or diarrhoea Key Implications: Comparison of symptom control in patients with carcinoid syndrome between octreotide LAR (standard arm) and pasireotide (somatostatin analogue with higher affinity for 4 of the 5 somatostatin receptors [especially sst5] compared with octreotide) Although the symptom control was very similar between the two drugs, there appears to be a longer progressionfree survival with pasireotide This needs to be validated in a prospective study (particularly in light of the CLARINET and PROMID studies 1. Efficacy and safety of pasireotide long acting release vs. octreotide long acting release in patients with metastatic carcinoid disease. Available at: 2. SIG-NET clinical study summary. Available at: 3. Wolin E.M., et al. Poster presented at North American NeuroEndocrine Tumour Symposium, Charleston, South Carolina, USA, October 04 05, 2013 SIG-NET: SOM230 InvestiGated in NeuroEndocrine Tumour
27 SIG-NET Pasireotide LAR vs. Octreotide LAR metastatic carcinoid tumour Wolin et al J Clin Oncol 29: 2011 (suppl; abstr 4075) ASCO 2013 Manuscript submitted
: vii124 vii130, 2012")
28 Öberg et al Annals of Oncology 23 (Supplement 7): vii124 vii130, 2012 CHEMOTHERAPY
29 Response rates Tools of the trade chemotherapy in practice Highest with poorly differentiated and anaplastic tumours (70%, cisplatin and etoposide), responses short-lasting Pancreatic NETs: 40-70% with STZ, dacarbazine, 5FU and doxorubicin-based regimens Low RR with midgut carcinoids: 15-30%, lasting 6-8 months (same agents) Patients should be entered into trials, where possible
 regimen N=82 patients (pancreas [49], GI [9], lung [8], ovary [1], UKP [15]) Histological grade predicts response Response rate: low grade 14% intermediate grade 34%")
30 Chemotherapy for non-pancreatic tumours? Streptozocin-5FUcisplatin (FCiSt) regimen N=82 patients (pancreas [49], GI [9], lung [8], ovary [1], UKP [15]) Histological grade predicts response Response rate: low grade 14% intermediate grade 34% high grade 60% (p=0.025) So does mitotic index score (p=0.008) and Ki67 Turner NC et al. Br J Cancer Mar 30;102(7): Öberg et al Annals of Oncology 23 (Supplement 7): vii124 vii130, 2012 Not primary site of tumour!

31 TARGETED THERAPIES
32 RADIANT-2 Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome Core phase (double-blind phase) Patients with advanced (unresectable or metastatic), low/intermediate grade NET; WHO performance status 2 N=429 Phase 3 RANDOMISATION 1 Everolimus 10 mg daily orally plus octreotide 30 mg IM every 28 days Placebo 10 mg daily orally plus octreotide 30 mg IM every 28 days Primary endpoint: PFS (RECIST) Sponsor: Novartis Following core phase, patients to enter in an openlabel extension phase, receiving open-label everolimus Patients with carcinoid syndrome (regardless of the site of primary tumour Progressive disease (within 12 months) G1 and G2 tumours Pavel et al Lancet 2011; 378:

33 RADIANT-2 Patient Demographics Pavel et al Lancet 2011; 378:
34 RADIANT-2 Primary Endpoint results Central Review Primary endpoint PFS Adjusted for two interim analyses, the pre-specified boundary at final analysis was p Local Review Pavel et al Lancet 2011; 378:
35 RADIANT-2 Exploratory subgroup analysis
 Phase I n=28 1 pt with rectal NET; PR Phase II PNET n=66 11pts PR (17%)")
 n=45 2pt PR (4%) PFS 17mth 1 Faivre S, JCO")
36 Early signal of clinical activity of VEGF inhibition in NETs Sunitinib 1 (4/2 weekly) Phase I n=28 1 pt with rectal NET; PR Phase II PNET n=66 11pts PR (17%) PFS 10mth NET n=40 1pt PR PFS 8mth PNET (everolimus alone) n=115 11pt PR (10%) PFS 10mth PNET (everolimus with SSA) n=45 2pt PR (4%) PFS 17mth 1 Faivre S, JCO 2006

 Neutropenia more common with Peg-IFN (14% vs.")
37 Early signal of clinical activity of VEGF inhibition in NETs Randomised phase II study Metastatic carcinoid tumour (GI and lung, not pnet) 1 line of chemo Stable on Octreotide LAR n=44 Bevacizumab 15 mg/kg q3w 18 weeks Peg-IFN 0.5ug/kg qw Bevacizumab + Peg-IFN Until PD Primary endpoint: Response Rate Endpoint % RR (Bev alone) 18% + 77% SD RR (Peg-IFN) 0% + 68% SD Hypertension more common with BEV (18% vs. 0%) Neutropenia more common with Peg-IFN (14% vs. 0%) No differences in fatigue, nausea, vomiting, headache. Yao J C et al. JCO 2008;26:
: 49% at Day 2, 28% at week 18 (p<0.")
38 Early signal of clinical activity of VEGF inhibition in NETs BEV associated with sig. decrease in tumour blood flow (functional CT): 49% at Day 2, 28% at week 18 (p<0.01) No change with Peg-IFN Phase III study ongoing [SWOG S0518, NCT ] Yao J C et al. JCO 2008;26:
39 Design: SWOG-S0518 Octreotide acetate (Sandostatin) Octreotide and IFN-α vs. octreotide and bevacizumab in carcinoid tumour Study Status: Ongoing (not recruiting) Estimated Primary Completion: Jan, 2015 Multicentre, randomised, open-label study comparing octreotide depot and IFN-α vs. octreotide depot and bevacizumab in poor prognosis carcinoid patients Phase 2 study results showed PFS to be superior in bevacizumab group than interferon group at week 18 Patients with metastatic/locally advanced, high-risk NET, Low/intermediate grade NET, Zubrod performance status 0-2 N=400 Phase 3 RANDOMISATION IFN α-2b, 0.5μg/kg, SC, on days 1, 3, 5, 8, 10, 12, 15, 17 and 19, plus octreotide, IM Bevacizumab, 15mg/kg, IV over mins, plus octreotide, IM Primary endpoint: PFS (central review) Sponsor: NCI, SWOG Treatment repeated every 21 days in the absence of disease progression or unacceptable toxicity Secondary endpoints: OS, TTF, OR, AEs Key Exclusion Criteria: Prior interferon, bevacizumab, or any other therapy targeting VEGF or VEGF receptors Concurrent interferon to control carcinoid syndrome Key Implications: All patients in this large phase 3 study receive octreotide and either interferon (based on multiple historical studies) or bevacizumab (based on the BETTER study) 1. Octreotide acetate and recombinant interferon alfa-2b or bevacizumab in treating patients with metastatic or locally advanced, high-risk neuroendocrine tumour. Available at: 2. Protocol Abstract: S0518. Available at: 3. Bevacizumab (Avastin) with octreotide (Sandostatin) for high-risk carcinoid tumours first or second line. Dec NHSC 4. Kulke M H., et al. Poster presented at: American Society of Clinical Oncology (ASCO); June 3-7, 2011; Chicago; IL, USA
40 Specific/selective tyrosine kinase inhibitors (TKIs) in oncology Name Selective Target Cancer (Examples) Afatinib HER2, EGFR NSCLC, squamous cell carcinoma of the head and neck, breast cancer Canertinib EGFR, HER2, 4 Head and neck, breast, and NSCLC, ovarian cancer Cediranib VEGFRs NSCLC, kidney and colorectal cancer CP PDGFRs NSCLC, colon carcinomas, glioblastoma Crizotinib MET NSCLC, anaplastic large cell lymphoma, neuroblastoma Dacomitinib EGFR NSCLC, gastric, head and neck cancer, glioma Erlotinib EGFR NSCLC, pancreatic cancer EMD MET NSCLC EMD MET NSCLC Gefitinib EGFR NSCLC, AML Icotinib EGFR NSCLC Lapatinib HER-2, EGFR Breast cancer Lenvatinib VEGFR2, 3 Approved for thyroid cancer in Japan LY Met, RON NSCLC Neratinib EGFR, HER2 NSCLC, breast cancer PD FGFRs NSCLC, gastric carcinoma, breast cancer Tandutinib FLT3 RCC, CML Tivantinib MET RCC, breast cancer Tivozanib VEGFR1, 2, 3 RCC, breast cancer Vatalanib VEGFR2 NSCLC, DLBCL, colorectal adenocarcinoma Adapted from Hojjat-Farsangi M. Int J Mol Sci Aug 8;15(8):
41 Multi-targeted tyrosine kinase inhibitors (TKIs) in oncology Name Target Molecules (Examples) Cancer (Examples) Amuvatinib ALK, MER, KIT, RET, PDGFRs, FLT3, RAD 51 NSCLC Axitinib VEGFRs, PDGFRs, KIT RCC Cabozantinib (XL184) VEGF, RET, MET, NTRKB, TIE2, AXL Medullary thyroid cancer Dasatinib BCR-ABL, SRC, KIT, PDGFRs, EPH, CSK CML, ALL Foretinib VEGFR2, MET NSCLC, breast, gastric, papillary renal cancer Golvatinib VEGFR2, MET Gastric cancer, HCC, glioblastoma, melanoma Imatinib ABL, KIT, PDGFRs GIST, leukemias MGCD-265 MET, VEGFRs, TIE2, RON NSCLC Nilotinib BCR-ABL, KIT, LCK, EPHA3, 8, DDR1, 2 CML Pazopanib PDGFRs, VEGFRs Advanced RCC, advanced soft tissue sarcoma Ponatinib BCR-ABL, PDGFRα, SRC, KIT, FGFR, VEGFRs CML, philadelphia chromosome positive ALL Regorafenib TIE2, PDGFRs, RET, KIT, B-RAF Metastatic colon cancer Sorafenib VEGFRs, PDGFRs, B-RAF, MEK, ERK Advanced RCC, hepatocellular carcinoma Sunitinib VEGFR2, PDGFRβ, KIT, RET, CSF1R, FLT3 RCC, GIST, pnet Vandetanib EGFR, VEGFRs, RET, Tie-2, FGFR1 Metastatic medullary thyroid cancer Adapted from Hojjat-Farsangi M. Int J Mol Sci Aug 8;15(8):
 functioning (CgA and 5HIAA >1.")
42 SUNLAND sunitinib versus placebo in combination with lanreotide in patients with progressive advanced/metastatic midgut carcinoid tumours Randomised phase II, double-blind, placebo-controlled study Patients with mid-gut NETs well differentiated (G1, G2) functioning (CgA and 5HIAA >1.5xULN) progression within 12 months measurable (CT/MRI) N=104 RANDOMISATION (1:1) Lanreotide 120 mg / 28d + Sunitinib 37.5 mg CDD Lanreotide 120 mg / 28d + placebo Treatment continued until tumour progression or death Primary endpoint: PFS Secondary endpoints: OS, RR, DoR, quality of life, safety Recruiting (CI: Pr Eric Raymond) ClinicalTrials.gov identifier: NCT
43 Sunitinib Following Hepatic Artery Embolisation in Metastatic NET Results Sunitinib days 1 28 in a 42-day cycle, starting 7 days after each HAE and ending 7 days before subsequent HAE (6-weekly) Amongst 39 treated patients: PR: 28 patients (72%) SD: 8 patients (20%) PD: 3 patients (8%) Median PFS, 18 months 2-year OS, 78% % Change in Tumor Measurements Serum VEGF levels increased by an average of 34% (51 pg/ml) Sunitinib 37.5 mg/day by CDD could be administered safely following HAE -100 Strosberg J, et al. Annals of Oncology 2013;23:
44 Other ongoing studies with sunitinib A Randomized Phase II Double-Blind Trial of Sunitinib vs. placebo in combination with Lanreotide in Patients with Progressive Advanced / Metastatic Midgut Carcinoid Tumours - NCT Antitumor Efficacy of Peptide Receptor Radionuclide Therapy With 177 Lutetium -Octreotate Randomized vs. Sunitinib in Unresectable Progressive Well-differentiated Neuroendocrine Pancreatic Carcinoma: First Randomized Phase II - NCT

45 Pathways to New Agents Pavel, M. Neuroendocrinology 2013;97:99 112
46 At a glance Intestinal pnet 6mo-PFS ORR 6mo-PFS ORR Sunitinib (phase III) % 9% Sunitinib (phase II) 73% 2% 70% 11% Pazopanib 68% 0% 81% 19% Sorafenib 40% 10% 61% 10% Axitinib???? Cabozantinib????
")
47 Who benefits most? Biomarkers Unanswered questions (i) Molecular diagnosis
48 Unanswered questions (ii) How do we deal with emerging resistance? Sequencing of therapies Optimal combination Role earlier in the disease? Applicability to other entities Different grade Different site of origin
49 SUMMARY Treatment options less developed for intestinal NETs vs. pancreatic NETs Somatostatin analogues have an established role: control of hormonal secretion Anti-proliferative effect Interferon may be considered for selected patients symptoms uncontrolled with SSAs The role of chemotherapy is less clear, but may be considered for selected patients Targeted therapies show promise: RADIANT-2 study suggests benefit (not licensed or reimbursed) Multiple TKIs under investigation IMPROVED RESEARCH METHODOLOGY AND HIGHER PROFILE OF NETS MEAN EXCITING YEARS AHEAD
50 Thank you
51 BACK-UP SLIDES
 study ECOG PS 0-2 1 prior chemotherapy Prior interferon and prior/concurrent octreotide at a stable dose allowed.")
 Response Rates: Carcinoid: 4/41 (10%); pnet: 4/41 (10%) 6-month PFS: Carcinoid: 8/20 (40%); pnet: 14/23 (61%) Toxicity: Grade 3 4 toxicity occurred in 43% o")
52 Sorafenib inhibits several tyrosine protein kinase receptors (VEGFR and PDGFR) and Raf Kinases (CRaf) A phase II trial of sorafenib in patients (pts) with metastatic neuroendocrine tumors (NET): A Phase II Consortium (P2C) study ECOG PS prior chemotherapy Prior interferon and prior/concurrent octreotide at a stable dose allowed. sorafenib 400 mg po BID Primary endpoint: response RECIST Two cohorts (i.e. Carcinoid and pnet) (separate 2-stage phase II designs). Results: N= 93 pts (50 Carcinoid, 43 pnet) Response Rates: Carcinoid: 4/41 (10%); pnet: 4/41 (10%) 6-month PFS: Carcinoid: 8/20 (40%); pnet: 14/23 (61%) Toxicity: Grade 3 4 toxicity occurred in 43% o skin (20%); GI (7%); fatigue (9%) Conclusions: Sorafenib at 400 mg po BID has modest activity in metastatic neuroendocrine tumors, with frequent grade 3-4 toxicity. T. J. Hobday et al, ASCO JCO 2007;25:18S (abstr 4504)

53 SORNET: Efficacy study of Sorafenib and cyclophosphamide to treat NETs 1 NCT N=22 patients Sorafenib: Phosphoshift measures activation of RAF signal transduction by detecting the phosphorylation of MEK1/2 in cells unstimulated or stimulated using IL3, a specific activator of the RAF signalling pathway in normal monocytes 2 Median PFS: 3 mo (95%CI ); RR: 1/22 (5%) Improved PFS in five patients with an increase in pshift after 7 days of sorafenib vs. those who did not (14.9 months vs 2.8 months; p=0.047). However, pshift did not add value to toxicity-based dosetitration. 1 Quintela-Fandino M et al. BJC 2013;108(6): ) 2 Yagisawa et al Exp Hematol 27:

 N=44")




 All: 91% Carcinoid: 92%")

54 Sorafenib: Sorafenib and bevacizumab combination targeted therapy in advanced NET: A phase II study of Spanish Neuroendocrine Tumour Group (GETNE0801) N=44 patients Histologically-confirmed Measurable advanced NETs Moderately or welldifferentiated NET GEP or lung ECOG PS prior chemo Castellano et al Eur J Cancer (2013) 49, sorafenib 200 mg bid D1-5 qw bevacizumab 5 mg/kg q2w 1 o endpoint: 6-mo PFS 2 o endpoints: PFS, TTP, OS Median PFS: 12.4 mo Median TTP: 14.5 mo ORR: 9.4% DCR: 95%. 6 mo Contd. (discretionary) All: 91% Carcinoid: 92% pnet: 89% Toxicity was an issue: Grade 3-4 adverse events: 64% Dose adjustments: sorafenib (64%) BVZ (36%) 6 patients (15%) withdrew due to adverse events
 in advanced low-grade neuroendocrine carcinoma (LGNEC) Eligibility criteria Patients with either carcinoid or pnet G1-G2 ECOG PS 0-1 Stable dose of depot octreotide (LAR)")
55 Pazopanib small molecule inhibitor of the VEGFR-1, -2, and -3, PDGF-α, PDGF-β, and c-kit tyrosine kinases A prospective, multi-institutional phase II study of GW (pazopanib) and depot octreotide (sandostatin LAR) in advanced low-grade neuroendocrine carcinoma (LGNEC) Eligibility criteria Patients with either carcinoid or pnet G1-G2 ECOG PS 0-1 Stable dose of depot octreotide (LAR) for 2 months No prior VEGF pathway inhibitor treatment 1 prior cytotoxic 2-cohort, 2-stage design N=51 Stratified by cohort Carcinoid: n=20 Pancreatic: n=31 Pazopanib 800 mg PO QD + Octreotide at their prior dose level Efficacy variables: tumour response, toxicity, and survival Adverse Events Grade 3 4 toxicities were relatively rare and included (%): hypertension (14), fatigue (10), neutropenia (8), diarrhoea (6), elevated ALT (6), elevated AST (6), hypertriglyceridaemia (6), nausea (4) Phan AT, et al. J Clin Oncol 2010;28:15S[Abstract 4001]
56 Pazopanib: A prospective, multi-institutional phase II study of GW (pazopanib) and depot octreotide (sandostatin LAR) in advanced low-grade neuroendocrine carcinoma (LGNEC) RECIST best protocol response: ITT population Parameter Overall (N=51)* Carcinoid (n=20) Pancreatic NET (n=31) PR, n (%) 6 (12%) 0 (0%) 6 (19%) SD, n (%) 35 (69%) 14 (70%) 21 (68%) PD, n (%) 6 (12%) 3 (15%) 3 (10%) Unknown 4 (8%) 3 (15%) 1 (3%) PFS 12.7 mo 11.7 mo Treatment with pazopanib and octreotide is feasible Tumor regression in patients with pnet Encouraging PFS durations in both carcinoid and pnet patients Phan AT, et al. J Clin Oncol 2010;28:15S[Abstract 4001]

 Secondary endpoints: PFS, ORR, DoR, TTR, safety, biomarkers assessment Key Implications: Single-arm study exploring the activity of pazopanib (an")
57 PAZONET Pazopanib as single agent in advanced/metastatic GEP NETs Design: Multicentre, open-label study evaluating pazopanib as a single agent in progressive advanced/metastatic GEP NETs patients who have failed chemotherapy, SSA or molecular targeted therapies Patients with well differentiated GEP-NET; ECOG performance status 0-1; life expectancy > 3 months Sponsor: GETNE Open to pnet and non-pnet Heterogeneous prior therapies N=44* N=17 pnet Phase 2 Pazopanib 800 mg (2x400mg) qd Null hypothesis CBR = 50% in favour of CBR = 70% if a total of 28 or more subjects out of 44 experience clinical benefit Primary endpoint: CBR (CR+PR+SD) Secondary endpoints: PFS, ORR, DoR, TTR, safety, biomarkers assessment Key Implications: Single-arm study exploring the activity of pazopanib (an oral, potent multi-target tyrosine kinase inhibitor VEGFR-1, -2, and -3, PDGFR-α and β, and c-kit) The threshold of activity was reached to warrant further investigation; efficacy needs to be confirmed in a prospective phase 3 study

 Progression free survival in months 3 Progression free survival (in months) by 3 subgroups (P =.040) 1. Grande E.")
58 PAZONET Pazopanib as single agent in advanced/metastatic GEP NETs Key Results: Clinical benefit (6-mo PFS) was achieved among 36 patients (SD 33 patients, PR 3 patients) = 85.4% No patient achieved CR, while 6 patients were found to have PD Median PFS: 10 months 1 Pazopanib might be efficacious in patients with refractory NETs Sum of the longest diameter of target lesions decreased over 10% among 32.5% of patients 2 (95%CI: ) P =.722 (95%CI: ) (95%CI: ) (95%CI: ) (95%CI: ) Progression free survival in months 3 Progression free survival (in months) by 3 subgroups (P =.040) 1. Grande E. Poster presented at: European Society for Medical Oncology (ESMO); September 28-October 02, 2012; Vienna, Austria. 2. Pulido EG., et al. Poster presented at: American Society of Clinical Oncology (ASCO); June 1-5, 2012; Chicago; IL, USA 3. Capdevila J., et al. Poster presented at: European Cancer Congress (ECC); September 27 October 1, 2013; Amsterdam, Netherlands 58
59 Pazopanib progressive carcinoid tumours Design: Randomised, double-blind, placebo-controlled, crossover study assessing the efficacy of pazopanib Patients with progressive carcinoid tumour, low/or intermediate grade NET, locally unresectable or metastatic CT, or progressive disease N=165 Phase 2 RANDOMISATION Pazopanib HCL orally every 28 days Placebo orally every 28 days Primary endpoint: PFS (RECIST) Sponsor: NCI Disease progression Cross-over from one arm to another Secondary endpoints: OS, OR, QoL, DoR, TTR Key Exclusion Criteria: Prior treatment with an inhibitor of VEGF or VEGFR Concurrent condition resulting in immune compromise, CNS metastases, GI abnormalities, uncontrolled BP, symptomatic congestive heart failure Pazopanib hydrochloride in treating patients with progressive carcinoid tumours. Available at: Study Status: Ongoing (recruiting) Estimated Primary Completion: Dec, 2016
60 AXITINIB Effect of increasing concentrations of anticancer therapeutic axitinib (targeting VEGFR1 3, PDGFRA-B, and KIT) on QGP-1 Pancreatic Endocrine Tumour cell growth

61 Design: Axitinib Octreotide LAR plus axitinib vs. placebo in non-pancreatic NET Randomised, double-blind, efficacy study to compare octreotide LAR in combination with axitinib vs. placebo Patients with progressive, advanced, well-differentiated NET of non-pancreatic origin, Ki-67 index < 20%; ECOG status: 0-2 N=80 Phase 2 RANDOMISATION Axitinib: orally, 5mg, bid plus Octreotide LAR: IM 30mg, single injection every 28 days Placebo: orally, bid plus Octreotide LAR: IM 30mg, single injection every 28 days Primary endpoint: PFS (RECIST) Sponsor: Grupo Español GETNE Secondary endpoints: OS, ORR, Safety Key Implications: Key Exclusion Criteria: Prior VEGF or VEGFR-targeted therapy Major surgery in <4 weeks or radiation therapy <2 weeks Concomitant CYP3A4 inhibitors/inducers, or oral vitamin K antagonists NETs are known to be highly vascular; this randomised phase 2 study will explore the activity of axitinib (a potent and selective tyrosine kinase inhibitor of vascular endothelial growth factor receptors (VEGFR)-1, VEGFR-2 and VEGFR-3) in non-pancreatic, well-differentiated NETs Available at:
 Secondary endpoints: RR, OS, TTF, AEs Clinicaltrials.")
62 A Phase II Study of Axitinib in Advanced Carcinoid Tumors Strosberg, Lee Moffitt Cancer Centre Axitinib: Eligibility criteria G1-G2 non-pnet aerodigestive NET, UKP and rare subtypes Measurable disease PD within 12 months Prior SSA mandated in mid-gut patients ECOG PS 0-2 N=30 Axitinib 5mg bd Primary endpoint: PFS (RECIST) Secondary endpoints: RR, OS, TTF, AEs Clinicaltrials.gov NCT
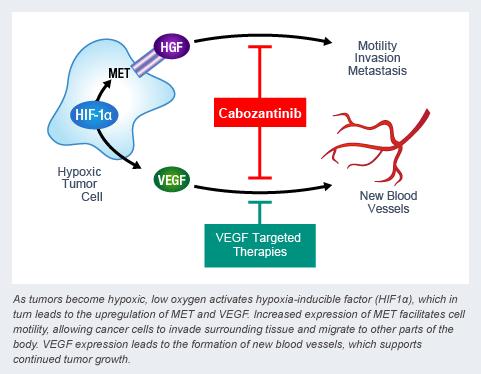
63 CABOZANTINIB

64 In RIP-Tag2 model 1, XL184: Cabozantinib Pre-clinical Eliminated approximately 80% of the tumour vasculature Reduced pericytes and empty basement membrane sleeves Caused widespread intra-tumoural hypoxia and tumour cell apoptosis Slowed regrowth of the tumour vasculature after drug withdrawal. Decreased invasiveness of primary tumours and reduced metastasis Effect of VEGR-blockade amplified 1,2 1. You et al Cancer Res; 71(14); Sennino et al Cancer Discov. Mar 2012; 2(3):
 PD within previous 12")
 Secondary endpoints: OS, AEs, correlates of response Faris et al ASCO 2014 abstr TPS4157 Clinicaltrials.")
65 Cabozantinib inhibits VEGFRs, MET, RET and c-kit An Open-Label, Phase II Study of Cabozantinib (XL184) in Advanced Pancreatic Neuroendocrine and Carcinoid Tumors Massachusetts General Eligibility criteria Well- Moddifferentiated Measurable disease (RECIST) PD within previous 12 months SSA allowed (if stable 2 months ECOG PS 0-1 N=70, parallel cohorts, non-randomised pnet carcinoid Cabozantinib (XL184) 60mg qd Primary endpoint: RR (RECIST) Secondary endpoints: OS, AEs, correlates of response Faris et al ASCO 2014 abstr TPS4157 Clinicaltrials.gov NCT
66
 (others 17) G1 (8) G2 (16) G3 (13) Primary")
 Ahn et al BJC")
67 Korean study Phase II N=37 (Pancreas 12) (CRC 8) (others 17) G1 (8) G2 (16) G3 (13) Primary end-point: response rate 18.9% (24.3% by independent review) Ahn et al BJC 2013;109,
68 Summary Somatostatin analogues remain the cornerstone for treatment of functional tumours Anti-proliferative effects demonstrated in pre-clinical studies Retrospective / prospective studies suggest effect on tumour progression Octreotide LAR delays time to disease progression but not in all patients CLARINET and COOPERATE-2 will enhance our understanding in a wider population Combination studies may explore any additive / synergistic effects
69 Angiogenesis inhibitors Agent (s) Target (s) N Tumor ORR, % Outcomes Comments Bevacizumab + octreotide 1 VEGF 22 Carcinoid months (PFS) 41 Carcinoid months (TTP) VEGFR, PDGFR, RET, FLT3 Sunitinib 2 66 Pancreatic NET months (TTP) Sorafenib 3 VEGFR, PDGF, 50 Carcinoid 7 8 months (PFS) Raf 43 Pancreatic NET months (PFS) Vatalanib 4 VEGFR, PDGFR 11 GEP NET 0 Not reported Ongoing Pazopanib 5 Motesanib 6 VEGFR, PDGFR, VEGFR, PDGFR, RET Carcinoid Pancreatic NET Ongoing 44 LGNET Suspended Atiprimod 7 Unclear 25 LGNET 0 Completed Bevacizumab + VEGF 31 Carcinoid 0 Ongoing 2-methoxyestradiol 8 Sunitinib 9 VEGFR, PDGFR, 74 Pancreatic NET 11.1 months (PFS) Terminated RET, FLT3 ORR = overall response rate; PDGF = platelet-derived growth factor; PDGFR = PDGF receptor; LGNET = low-grade NET. 1. Yao JC, et al. J Clin Oncol 2008:26; Kulke MH, et al. J Clin Oncol 2008:26; Hobday TJ, et al. J Clini Oncol 2007;25:[abstract 4504]. 4. Anthony L, et al. J Clin Oncol 2008;26:[abstract 14624]. 5. NCT Available from 6. NCT Available from 7. Sung MW, et al. J Clin Oncol 2008;26:[abstract 4611]. 8. NCT Available from 9. Raymond E, et al. Oral presentation at the WCGOC. 2009:[abstr O-0013].
: vii124 vii130,")
70 ESMO practice guidelines Öberg et al Annals of Oncology 23 (Supplement 7): vii124 vii130, 2012
71 RADIANT-2 Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with carcinoid syndrome
MEDICAL MANAGEMENT OF METASTATIC GEP-NET
 MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS
 TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology
 Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Review of Gastrointestinal Carcinoid Tumors: Latest Therapies
 Review of Gastrointestinal Carcinoid Tumors: Latest Therapies Arvind Dasari, MD, MS Department of Gastrointestinal Medical Oncology The University of Texas MD Anderson Cancer Center Houston, TX, USA Neuroendocrine
Review of Gastrointestinal Carcinoid Tumors: Latest Therapies Arvind Dasari, MD, MS Department of Gastrointestinal Medical Oncology The University of Texas MD Anderson Cancer Center Houston, TX, USA Neuroendocrine
Background. Capdevila J, et al. Ann Oncol. 2018;29(Suppl 8): Abstract 1307O. 1. Dasari A, et al. JAMA Oncol. 2017;3(10):
: Abstract 1307O. 1. Dasari A, et al. JAMA Oncol. 2017;3(10):") Efficacy of Lenvatinib in Patients With Advanced Pancreatic (pannets) and Gastrointestinal (ginets) WHO Grade 1/2 (G1/G2) Neuroendocrine Tumors: Results of the International Phase II TALENT Trial (GETNE
Efficacy of Lenvatinib in Patients With Advanced Pancreatic (pannets) and Gastrointestinal (ginets) WHO Grade 1/2 (G1/G2) Neuroendocrine Tumors: Results of the International Phase II TALENT Trial (GETNE
NET εντέρου Τι νεότερο/ Νέες μελέτες. Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ
 NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique
 Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique By Professor Kjell Öberg, M.D., Ph.D. Dept. of Endocrine Oncology, University Hospital, Uppsala, Sweden Nashville Oct. 2011 Hallmarks
Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique By Professor Kjell Öberg, M.D., Ph.D. Dept. of Endocrine Oncology, University Hospital, Uppsala, Sweden Nashville Oct. 2011 Hallmarks
Antiangiogenics are effective treatments in NETs
 RENET: A randomized phase III trial comparing REgorafenib to placebo in patients with advanced, progressive, well-differentiated NEuroendocrine Tumors (NETs). Coordinators: Dr Julien Hadoux & Dr David
RENET: A randomized phase III trial comparing REgorafenib to placebo in patients with advanced, progressive, well-differentiated NEuroendocrine Tumors (NETs). Coordinators: Dr Julien Hadoux & Dr David
The Current Champion: Angiogenesis inhibitors
 The Current Champion: Angiogenesis inhibitors Baek-Yeol RYOO University of Ulsan College of Medicine ASAN Medical Center Dept. of Oncology Seoul, Korea Survival probability Sorafenib: Overall Survival
The Current Champion: Angiogenesis inhibitors Baek-Yeol RYOO University of Ulsan College of Medicine ASAN Medical Center Dept. of Oncology Seoul, Korea Survival probability Sorafenib: Overall Survival
Recent developments of oncology in neuroendocrine tumors (NETs)
") Recent developments of oncology in neuroendocrine tumors (NETs) Marc Peeters MD, PhD Coordinator Multidisciplinary Oncological Center Antwerpen (MOCA) Head of the Oncology Department UZA, Professor in
Recent developments of oncology in neuroendocrine tumors (NETs) Marc Peeters MD, PhD Coordinator Multidisciplinary Oncological Center Antwerpen (MOCA) Head of the Oncology Department UZA, Professor in
I. Diagnosis of the cancer type in CUP
 Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
Latest Research: USA I. Diagnosis of the cancer type in CUP II. Outcomes of site-specific therapy of the cancer type in CUP a. Prospective clinical trial b. Retrospective clinical trials 1 Latest Research:
2015: Year in Review Results of Recent Trials
 2015: Year in Review Results of Recent Trials Pamela L. Kunz, MD Assistant Professor of Medicine / GI Oncology Director, Stanford NET Program Stanford University School of Medicine Disclosures Research
2015: Year in Review Results of Recent Trials Pamela L. Kunz, MD Assistant Professor of Medicine / GI Oncology Director, Stanford NET Program Stanford University School of Medicine Disclosures Research
Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal
 Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal Incidence per 100,000 EPIDEMIOLOGY Incidence rates of neuroendocrine tumors by primary tumor site 1.4 1.2 1.0 0.8 0.6
Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal Incidence per 100,000 EPIDEMIOLOGY Incidence rates of neuroendocrine tumors by primary tumor site 1.4 1.2 1.0 0.8 0.6
SUPPLEMENTARY INFORMATION
 Supplementary Table 1. Therapies for non-men1 pancreatic neuroendocrine tumours (NETs) (published after 2011) Somatostatin analogues Tumour type a Intervention Number of participants/information available
Supplementary Table 1. Therapies for non-men1 pancreatic neuroendocrine tumours (NETs) (published after 2011) Somatostatin analogues Tumour type a Intervention Number of participants/information available
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives
 Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
Ongoing and future clinical investigation in GEP NENs
 ESMO PRECEPTORSHIP PROGRAMME Multidisciplinary management, standards of care and future perspectives Lugano, Switzerland 13-14 April 2018 CHAIR: Nicola Fazio, Italy George Pentheroudakis, Greece Ongoing
ESMO PRECEPTORSHIP PROGRAMME Multidisciplinary management, standards of care and future perspectives Lugano, Switzerland 13-14 April 2018 CHAIR: Nicola Fazio, Italy George Pentheroudakis, Greece Ongoing
Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works.
 Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works. Arturo Loaiza-Bonilla, MD, FACP Assistant Professor of Clinical Medicine
Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works. Arturo Loaiza-Bonilla, MD, FACP Assistant Professor of Clinical Medicine
Nuevas alternativas en el manejo de TNE avanzados
 Nuevas alternativas en el manejo de TNE avanzados Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Coordinación científica: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla,
Nuevas alternativas en el manejo de TNE avanzados Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Coordinación científica: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla,
NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες
 NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
Riunione Monotematica A.I.S.F The future of liver diseases. HEPATIC NEOPLASMS The challenge for new drugs
 Riunione Monotematica A.I.S.F. 2016 The future of liver diseases Milan 13 th -15 th October 2016 Centro Congressi Fondazione Cariplo HEPATIC NEOPLASMS The challenge for new drugs Massimo Iavarone Gastroenterology
Riunione Monotematica A.I.S.F. 2016 The future of liver diseases Milan 13 th -15 th October 2016 Centro Congressi Fondazione Cariplo HEPATIC NEOPLASMS The challenge for new drugs Massimo Iavarone Gastroenterology
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Pancreatic NeuroEndocrine Tumors. Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium
 Pancreatic NeuroEndocrine Tumors Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Epidemiology Overall incidence 1.8 to 2.6 SEER, Europe Peak in 5 th and 6 th decade Incidence
Pancreatic NeuroEndocrine Tumors Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Epidemiology Overall incidence 1.8 to 2.6 SEER, Europe Peak in 5 th and 6 th decade Incidence
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust
 GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT )
") An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT02267967) J.M. Xu a, J. Li b, C.M. Bai c, N. Xu d, Z.W. Zhou e, Z.P. Li f, C.C. Zhou g, W. Wang h, J. Li
An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT02267967) J.M. Xu a, J. Li b, C.M. Bai c, N. Xu d, Z.W. Zhou e, Z.P. Li f, C.C. Zhou g, W. Wang h, J. Li
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer
 WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
Angiogenesis and tumor growth
 Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval
 12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval ARMANDO SANTORO Roma 10-6-2016 SORAFENIB APPROVAL 29 OCTOBER 2007 Marketing authorization
12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval ARMANDO SANTORO Roma 10-6-2016 SORAFENIB APPROVAL 29 OCTOBER 2007 Marketing authorization
Jon Trent, MD, PhD. Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center
 Gastrointestinal Stromal Tumor GISTS 2010: After Standard of Care Jon Trent, MD, PhD Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center jtrent@mdanderson.org
Gastrointestinal Stromal Tumor GISTS 2010: After Standard of Care Jon Trent, MD, PhD Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center jtrent@mdanderson.org
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? VEGF Is the Only Angiogenic Factor Present Throughout the Tumor Life Cycle
 Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
David N. Robinson, MD
 David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία. Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018
 Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018 Advisory Board Disclosures Roche, Boeringer, Sanofi, Astra Zeneca,
Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018 Advisory Board Disclosures Roche, Boeringer, Sanofi, Astra Zeneca,
2 nd line Therapy and Beyond NSCLC. Alan Sandler, M.D. Oregon Health & Science University
 2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
Octreotide LAR in neuroendocrine tumours a summary of the experience
 Endocrinology in oncology Review article Octreotide LAR in neuroendocrine tumours a summary of the experience Agnieszka Kolasińska-Ćwikła, MD, PhD Department of Chemotherapy, Oncology Clinic, Maria Sklodowska-Curie
Endocrinology in oncology Review article Octreotide LAR in neuroendocrine tumours a summary of the experience Agnieszka Kolasińska-Ćwikła, MD, PhD Department of Chemotherapy, Oncology Clinic, Maria Sklodowska-Curie
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS
 OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS Dr Mairéad McNamara Senior lecturer, University of Manchester & Honorary Consultant in Medical Oncology, The Christie NHS Foundation Trust
OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS Dr Mairéad McNamara Senior lecturer, University of Manchester & Honorary Consultant in Medical Oncology, The Christie NHS Foundation Trust
GEP NET: algoritmo terapeutico. Dottor Nicola Fazio
 GEP NET: algoritmo terapeutico Dottor Nicola Fazio Basi per il trattamento Caratteristiche del paziente Caratteristiche del tumore P.S., sindrome, comorbidità Differenziazione, Ki-67 Imaging morfologico
GEP NET: algoritmo terapeutico Dottor Nicola Fazio Basi per il trattamento Caratteristiche del paziente Caratteristiche del tumore P.S., sindrome, comorbidità Differenziazione, Ki-67 Imaging morfologico
Recent Advances in Gastrointestinal Cancers
 Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
Evaluation and Management of Neuroendocrine Tumors
 Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
NICaN Pancreatic Neuroendocrine Tumour SACT protocols. 1.0 Dr M Eatock Final version issued
 Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Carcinoma de Tiroide: Teràpies Diana
 Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Le target therapy nei Tumori Neuroendocrini
 Le target therapy nei Tumori Neuroendocrini Take home messages Franco Grimaldi SOC Endocrinologia e Malattie del Metabolismo Nutrizione Clinica Azienda Ospedaliero-Universitaria Santa Maria della Misericordia
Le target therapy nei Tumori Neuroendocrini Take home messages Franco Grimaldi SOC Endocrinologia e Malattie del Metabolismo Nutrizione Clinica Azienda Ospedaliero-Universitaria Santa Maria della Misericordia
Systematic Review of the Role of Targeted Therapy in Metastatic Neuroendocrine Tumors
 At the Cutting Edge Received: February 29, 2016 Accepted: April 12, 2016 Published online: April 16, 2016 Systematic Review of the Role of Targeted Therapy in Metastatic Neuroendocrine Tumors Adrian Lee
At the Cutting Edge Received: February 29, 2016 Accepted: April 12, 2016 Published online: April 16, 2016 Systematic Review of the Role of Targeted Therapy in Metastatic Neuroendocrine Tumors Adrian Lee
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Malignant pleural Mesothelioma: A Year In Review
 Malignant pleural Mesothelioma: A Year In Review Rabab Gaafar,MD Prof. Medical Oncology NCI Cairo University National Cancer Institute Conference 2015 ASCO news in Mesothelioma Introduction ASCO news second
Malignant pleural Mesothelioma: A Year In Review Rabab Gaafar,MD Prof. Medical Oncology NCI Cairo University National Cancer Institute Conference 2015 ASCO news in Mesothelioma Introduction ASCO news second
Metastatic renal cancer (mrcc): Evidence-based treatment
: Evidence-based treatment") Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Medullary Thyroid Carcinoma: New Therapies and Trials
 Medullary Thyroid Carcinoma: New Therapies and Trials Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology, Diabetes, and Metabolism The Ohio State University
Medullary Thyroid Carcinoma: New Therapies and Trials Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology, Diabetes, and Metabolism The Ohio State University
July, ArQule, Inc.
 July, 2012 Safe Harbor This presentation and other statements by ArQule may contain forward-looking statements within the meaning of the Private Securities Litigation Reform Act with respect to clinical
July, 2012 Safe Harbor This presentation and other statements by ArQule may contain forward-looking statements within the meaning of the Private Securities Litigation Reform Act with respect to clinical
OUR EXPERIENCES WITH ERLOTINIB IN SECOND AND THIRD LINE TREATMENT PATIENTS WITH ADVANCED STAGE IIIB/ IV NON-SMALL CELL LUNG CANCER
 & OUR EXPERIENCES WITH ERLOTINIB IN SECOND AND THIRD LINE TREATMENT PATIENTS WITH ADVANCED STAGE IIIB/ IV NON-SMALL CELL LUNG CANCER Interim Data Report of TRUST study on patients from Bosnia and Herzegovina
& OUR EXPERIENCES WITH ERLOTINIB IN SECOND AND THIRD LINE TREATMENT PATIENTS WITH ADVANCED STAGE IIIB/ IV NON-SMALL CELL LUNG CANCER Interim Data Report of TRUST study on patients from Bosnia and Herzegovina
Improving outcomes for NSCLC patients with brain metastases
 Improving outcomes for NSCLC patients with brain metastases Martin Schuler West German Cancer Center, Essen, Germany In Switzerland, afatinib is approved as monotherapy for patients with non-small cell
Improving outcomes for NSCLC patients with brain metastases Martin Schuler West German Cancer Center, Essen, Germany In Switzerland, afatinib is approved as monotherapy for patients with non-small cell
Novel Molecular Molecular Therapies In Hepatocarcinoma Prof Eric
 Novel Molecular Therapies In Hepatocarcinoma Prof. Eric Raymond Department of Médical Oncology Hôpital Beaujon, Clichy Université Paris 7 Denis Diderot INSERM-U728 eric.raymond@bjn.aphp.fr HCC is a highly
Novel Molecular Therapies In Hepatocarcinoma Prof. Eric Raymond Department of Médical Oncology Hôpital Beaujon, Clichy Université Paris 7 Denis Diderot INSERM-U728 eric.raymond@bjn.aphp.fr HCC is a highly
Combining Stroma-Targeted Therapies with Radiation to Prevent Resistance
 Combining Stroma-Targeted Therapies with Radiation to Prevent Resistance Dan G. Duda, DMD, PhD Harvard Medical School New Cancer Targets NCT Conference Sesptember 23, 2013 Conflicts of Interest None Tumor
Combining Stroma-Targeted Therapies with Radiation to Prevent Resistance Dan G. Duda, DMD, PhD Harvard Medical School New Cancer Targets NCT Conference Sesptember 23, 2013 Conflicts of Interest None Tumor
Selection of Appropriate Treatment
 Expert Review in Metastatic Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): Selection of Appropriate Treatment Reference Slide Deck Neuroendocrine Tumors (NETs): A Diverse Group of Malignancies
Expert Review in Metastatic Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): Selection of Appropriate Treatment Reference Slide Deck Neuroendocrine Tumors (NETs): A Diverse Group of Malignancies
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-028 Study
 Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Hot of the press. Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ
 Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
A New Proposal for Metabolic Classification of NENs Stefano Severi IRST Meldola Italy
 RADIONUCLIDE THERAPY AND ALLIED SCIENCE President: Giovanni Paganelli Chairman: Maria Salvato Baltimore USA Domenico Barone Meldola Italy A New Proposal for Metabolic Classification of NENs Stefano Severi
RADIONUCLIDE THERAPY AND ALLIED SCIENCE President: Giovanni Paganelli Chairman: Maria Salvato Baltimore USA Domenico Barone Meldola Italy A New Proposal for Metabolic Classification of NENs Stefano Severi
Novel EGFR TKI Theliatinib: An Open Label, Dose Escalation Phase I Clinical Trial
 Novel EGFR TKI Theliatinib: An Open Label, Dose Escalation Phase I Clinical Trial 2014-309-00CH1 Presenter: Jifang Gong, Beijing Cancer Hospital Lin Shen 1, Li Zhang 2, Hongyun Zhao 2, Wenfeng Fang 2,
Novel EGFR TKI Theliatinib: An Open Label, Dose Escalation Phase I Clinical Trial 2014-309-00CH1 Presenter: Jifang Gong, Beijing Cancer Hospital Lin Shen 1, Li Zhang 2, Hongyun Zhao 2, Wenfeng Fang 2,
A Review in the Treatment Options for Renal Cell Cancer
 A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
A Review in the Treatment Options for Renal Cell Cancer Ali McBride, PharmD, MS BCPS, BCOP Clinical Coordinator Hematology/Oncology Department of Pharmacy The University of Arizona Cancer Center RENAL
I nuovi farmaci: associazione o superamento del trattamento con analoghi
 Milano, 20 giugno 2008 I NETs: a che punto siamo? I nuovi farmaci: associazione o superamento del trattamento con analoghi Nicola Fazio NET: possible targets for novel drugs Angiogenesis VEGF, EGF, IGF,
Milano, 20 giugno 2008 I NETs: a che punto siamo? I nuovi farmaci: associazione o superamento del trattamento con analoghi Nicola Fazio NET: possible targets for novel drugs Angiogenesis VEGF, EGF, IGF,
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Sergio Bracarda MD. Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy
 San Donato Hospital Arezzo, Italy") Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain
 New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
SUPPLEMENTARY INFORMATION
 Supplementary Information S3 TAM- family small molecule kinase inhibitors in development Compound Indication(s) Target Profile Develop Primary Target MERTK TYRO3 Other targets ment Phase Refs Cabozantinib
Supplementary Information S3 TAM- family small molecule kinase inhibitors in development Compound Indication(s) Target Profile Develop Primary Target MERTK TYRO3 Other targets ment Phase Refs Cabozantinib
NEXT GENERATION DRUGS IN KIDNEY CANCER. Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden
 NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
NEXT GENERATION DRUGS IN KIDNEY CANCER Dr Aine O Reilly Karolinska Institutet Stockholm, Sweden KIDNEY CANCER SUBTYPES Papillary Type 1 and 2 Medullary Collecting duct Chromophobe Translocation Clear cell
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer.
 Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Metastatic Renal Cancer Medical Treatment
 Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Advances in Systemic Therapy Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016
 Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016") Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT
 ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse?
 Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Maintenance paradigm in non-squamous NSCLC
 Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Maintenance paradigm in non-squamous NSCLC L. Paz-Ares Hospital Universitario Virgen del Rocío Sevilla Agenda Theoretical basis The data The comparisons Agenda Theoretical basis The data The comparisons
Horizon Scanning Technology Briefing. Sutent (Sunitinib) for first-line and adjuvant treatment of renal cell carcinoma
 for first-line and adjuvant treatment of renal cell carcinoma") Horizon Scanning Technology Briefing National Horizon Scanning Centre Sutent (Sunitinib) for first-line and adjuvant treatment of renal cell carcinoma August 2006: Updated October 2006 This technology
Horizon Scanning Technology Briefing National Horizon Scanning Centre Sutent (Sunitinib) for first-line and adjuvant treatment of renal cell carcinoma August 2006: Updated October 2006 This technology
New Agents for Head and Neck Cancer. Ezra Cohen, MD Associate Professor of Medicine University of Chicago Chicago, IL
 New Agents for Head and Neck Cancer Ezra Cohen, MD Associate Professor of Medicine University of Chicago Chicago, IL Disclosure Dr. Cohen has the following relevant financial relationships with commercial
New Agents for Head and Neck Cancer Ezra Cohen, MD Associate Professor of Medicine University of Chicago Chicago, IL Disclosure Dr. Cohen has the following relevant financial relationships with commercial
Innovaciones en el tratamiento del ca ncer renal. Enrique Grande
 Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
Innovaciones en el tratamiento del ca ncer renal Enrique Grande The enriched inflammatory environment of RCC Chen Z, et al. Nat Rev Cancer 2014 Available agents are expanding across the three eras of arcc
CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY FOR THE RIGHT PATIENT
 Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Daniel Heng, MD, MPH, FRCPC @DrDanielHeng Chair GU Tumour Group, Tom Baker Cancer Centre Clinical Professor, University of Calgary CLINICAL CHALLENGES IN METASTATIC RENAL CELL CARCINOMA: THE RIGHT THERAPY
Why was HOPE 205 a Positive After Years of Negative Studies?
 Why was HOPE 205 a Positive After Years of Negative Studies? Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation Why do we pursue combinations?
Why was HOPE 205 a Positive After Years of Negative Studies? Prof. Dr. med. Viktor Grünwald Klinik für Hämatologie, Hämostaseologie, Onkologie und Stammzelltransplantation Why do we pursue combinations?
Treatment of EGFR mutant advanced NSCLC
 Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Treatment of EGFR mutant advanced NSCLC Raffaele Califano Department of Medical Oncology The Christie and Manchester University Hospital Manchester, UK Outline Data on first-line Overcoming T790M mutation
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
MANAGEMENT OF THYROID MALIGNANCIES
 MANAGEMENT OF THYROID MALIGNANCIES Taofeek K. Owonikoko, MD, PhD Associate Professor Department of Hematology/Medical Oncology Winship Cancer Institute of Emory University Atlanta, GA 1 Disclosures Research
MANAGEMENT OF THYROID MALIGNANCIES Taofeek K. Owonikoko, MD, PhD Associate Professor Department of Hematology/Medical Oncology Winship Cancer Institute of Emory University Atlanta, GA 1 Disclosures Research
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
sunitinib 12.5mg, 25mg, 37.5mg, 50mg hard capsules (Sutent ) SMC No. (698/11) Pfizer Limited
 SMC No. (698/11) Pfizer Limited") sunitinib 12.5mg, 25mg, 37.5mg, 50mg hard capsules (Sutent ) SMC No. (698/11) Pfizer Limited 08 April 2011 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and
sunitinib 12.5mg, 25mg, 37.5mg, 50mg hard capsules (Sutent ) SMC No. (698/11) Pfizer Limited 08 April 2011 The Scottish Medicines Consortium (SMC) has completed its assessment of the above product and
Pancreatic Neuroendocrine Tumours
 UCLH Cancer Collaborative Pancreas Update Meeting 12 th July 2017 Pancreatic Neuroendocrine Tumours Dr. Christos Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior
UCLH Cancer Collaborative Pancreas Update Meeting 12 th July 2017 Pancreatic Neuroendocrine Tumours Dr. Christos Toumpanakis MD PhD FRCP Consultant in Gastroenterology/Neuroendocrine Tumours Hon. Senior
Targeted Therapy in Advanced Renal Cell Carcinoma
 Targeted Therapy in Advanced Renal Cell Carcinoma Brian I. Rini, M.D. Department of Solid Tumor Oncology Glickman Urologic and Kidney Institute Cleveland Clinic Taussig Cancer Institute Cleveland, Ohio
Targeted Therapy in Advanced Renal Cell Carcinoma Brian I. Rini, M.D. Department of Solid Tumor Oncology Glickman Urologic and Kidney Institute Cleveland Clinic Taussig Cancer Institute Cleveland, Ohio
Molecular Targets in Lung Cancer
 Molecular Targets in Lung Cancer Robert Ramirez, DO, FACP Thoracic and Neuroendocrine Oncology November 18 th, 2016 Disclosures Consulting and speaker fees for Ipsen Pharmaceuticals, AstraZeneca and Merck
Molecular Targets in Lung Cancer Robert Ramirez, DO, FACP Thoracic and Neuroendocrine Oncology November 18 th, 2016 Disclosures Consulting and speaker fees for Ipsen Pharmaceuticals, AstraZeneca and Merck
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Guideline A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO)
, Cancer Care Ontario (CCO)") A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Systemic Therapy of Incurable Gastroenteropancreatic Neuroendocrine Tumours S. Singh, D. Sivajohanathan, T.
A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Systemic Therapy of Incurable Gastroenteropancreatic Neuroendocrine Tumours S. Singh, D. Sivajohanathan, T.