Dyslipidemia and the Use of Statins. Troy L Randle, DO, FACC, FACOI
|
|
|
- Dwayne Pierce
- 6 years ago
- Views:
Transcription
1 Dyslipidemia and the Use of Statins Troy L Randle, DO, FACC, FACOI
2
3
4 Objective: Identify CV risk. Determine what dyslipidemia (dyslipoproteinemia) is Decrease CV risk and optimize lipid levels for your patients at higher risk using statins.

5
6

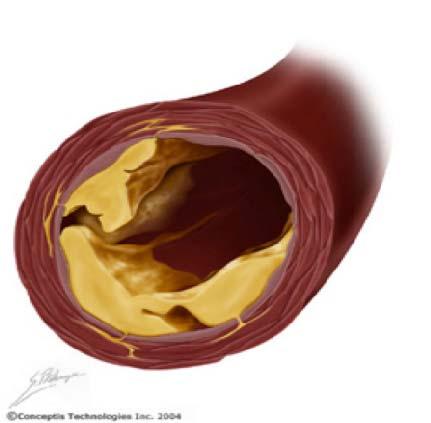
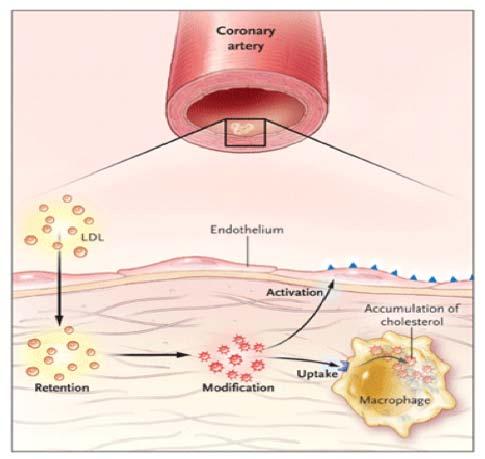
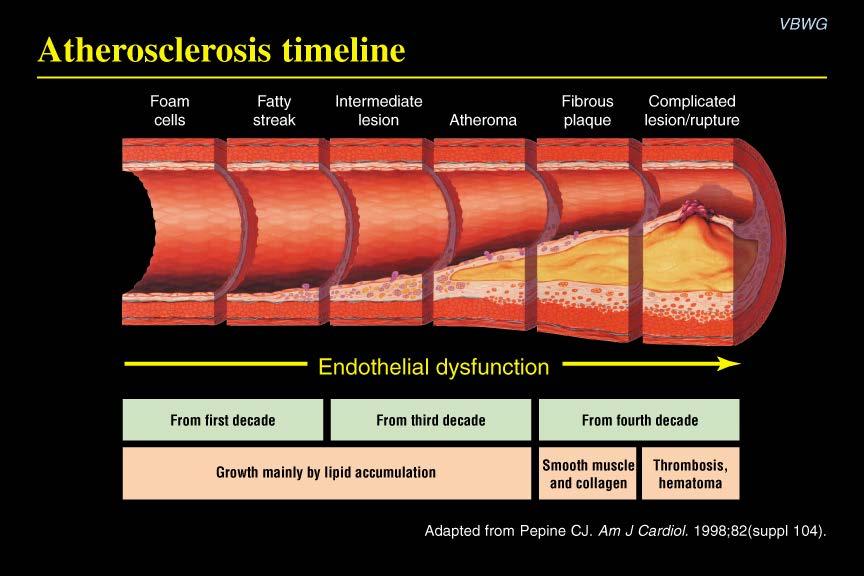
7 Atherothrombosis: A Progressive Process Normal Fatty Streak Fibrous Plaque Occlusive Atherosclerotic Plaque Plaque Rupture/ Fissure & Thrombosis Unstable Angina MI Coronary Death Clinically Silent Effort Angina Claudication Stroke Critical Leg Ischemia Increasing Age Courtesy of P Ganz.

8 Lesion growth

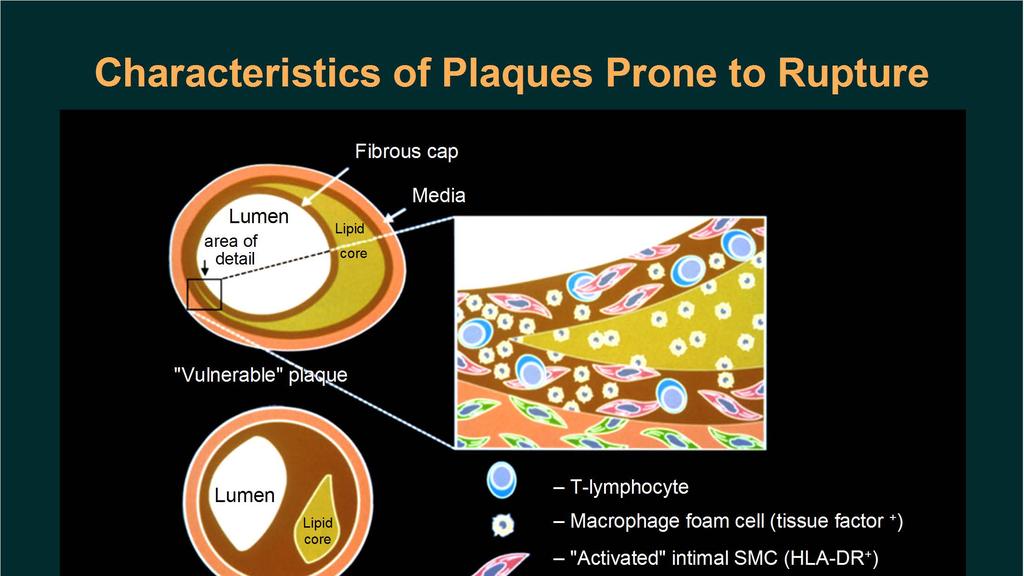
9 Mechanism of Plaque Disruption in Atherothrombosis


10 Thrombotic occlusion Final Result Normal blush
11 Framingham Risk Score (FRS) for 10 yr CHD Risk Qx Calculate df Dysmetabolic Syndrome Cardio-Metabolic Syndrome (MetS)
12 Refining Risk Assessment Coronary artery calcium, ankle-brachial index, high-sensitivity CRP (hs CRP), and family history were independent predictors of incident CHD/CVD in intermediate-risk individuals. Coronary artery calcium provided superior discrimination and risk reclassification compared with other risk markers. Yebeah J et al. JAMA August 22/ ; 308 (8):
13 NCEP III Guidelines: Clinical ID of the Metabolic Syndrome* Risk factor Defining Level Abdominal Obesity Waist Circumference Men >40 in Women >35 in Triglycerides (TG) > 150mg/dL HDL C Men <40mg/dL Women <50mg/dL Blood pressure Fasting glucose >130/>85mmHg >100mg/dL *Diagnosis is dependent on 3 or more factors NCEP ATP III. JAMA May ; 285:


14 Metabolic Pathways Underlying Pre-Diabetes and Metabolic Syndrome Grundy, S. M. J Am Coll Cardiol 2012;59: Copyright 2012 American College of Cardiology Foundation. Restrictions may apply.
15
16 Secondary Prevention Guidelines* Recently updated by the AHA & ACC. First update since 2001 based on new evidence that intensive therapy can significantly reduce recurrent events and CVA. * Smith C S et al. AHA/ACC Guidelines for secondary prevention for patients with coronary and other atherosclerotic vascular disease: 2006 Update: Endorsed by the National Heart, Lung and Blood Institute. J Am Coll Cardiol May ; 47: * Maiese M L. ACC/AHA Update Secondary-Prevention Guidelines Heartbeat June 2006; # Heartbeats
17 How to read a lipid panel in 6 quick steps 1. Look at the triglyceride (TG) level. If it is >500 mg/dl, treatment is indicated, and TG reduction takes precedence over all other lipid concentrations. If TG is <500 mg/dl, go to Step Look at the low-density lipoprotein cholesterol (LDL-C) level. If it is >190 mg/dl, drug therapy is indicated regardless of other findings. At lower levels, the need for therapy is based on the patient s overall risk of cardiovascular disease (CVD). Therapeutic lifestyle changes (TLC) recommendations are always indicated. 3. Look at high-density lipoprotein cholesterol (HDL-C). Increased risk is present if it is <50 mg/dl, the threshold for women and <40mg/dL in men. Do not assume that high HDL-C always means low CVD risk.
18 How to read a lipid panel in 6 quick steps 4. Calculate the total cholesterol (TC)/HDL-C ratio (a surrogate of apob/apoa-i ratio). Increased risk is present if it is > Calculate the non-hdl-c level (TC minus HDL-C). If it is >130 mg/dl or >100 mg/dl in very-high-risk patients, therapy is warranted. Newer data reveal that this calculation is always equal to, or better than, LDL-C at predicting CVD risk. Non-HDL-C is less valuable if TG is >500 mg/dl. 6. Calculate the TG/HDL-C ratio to estimate the size of LDL. If the ratio is >3.8, the likelihood of small LDL is 80%. (Small LDL usually has very high LDL-P.)
19 Cholesterol Management per NCEP III Guidelines PRIMARY GOAL: LDL-C SECONDARY GOAL: Non HDL-C JAMA 2001; 285:
20 LDL-C LDL-C is the number one surrogate for Apo B (the transport vehicle that gets cholesterol into the vessel wall) per NCEP ATP III guidelines (If Apo B is controlled it is unlikely that atherogenisis can occur). In patients with TG (> 130mg/dL) or low HDL-C (< 40mg/dL) TG/HDL axis disorders, LDL-C is simply not as good a surrogate for Apo B as non-hdl-c.
21 Non-HDL-C Provides a measure of all the cholesterol in atherogenic particles including LDL-C, Apo B, LP(a) and TG-rich particles in VLDL, VLDL remnants and intermediately dense lipoproteins. Introduced as the secondary target of therapy in patients with high TG (> 200mg/dL) per NCEP ATP III guidelines. JAMA 2001; 285:
22 NCEP III Non HDL-C Goal Non-HDL-C = TC - HDL-C Goal Non-HDL-C is 30mg > LDL-C goal Must be remembered that LDL-C and non HDL-C goals are NCEP surrogates for the number 1 lipid risk factor which is Apo B lipoprotein. Neither non-hdl-c or especially LDL-C approaches Apo B or LDL-P (via NMR) measurements as the most accurate predictors of risk.
23 Non HDL-C When TG are elevated, non HDL-C is a much better surrogate of the all important Apo B level than is LDL-C. LDL-C is a calculation (TC-[HDL-C + VLDL-C] and VLDL-C is estimated by labs using a formula TG/5).
24 Non HDL-C Among statin-treated patients, on-treatment levels of LDL-C, non HDL-C, and apob were each associated with risk of future major cardiovascular events. The strength of this association was greater for non HDL-C than for LDL-C and apob. JAMA June ;307(12):
25 Abnormalities of the TG/HDL-C Axis Increasing prevalence (T2DM/MetS). Treatment errors are frequently made by looking only at the LDL-C level (particularly in diabetics) which are frequently normal or only slightly elevated and subsequently not treated. Frequently associated with elevated Apo B and increased LDL-C particle (LDL-P) concentrations if the LDL particles are small.
26 Bottom Line NCEP states: Normalize LDL-C and non-hdl-c to appropriate goals based on risk the higher the risk the more aggressive the therapy. If you don t want to risk your patient s lives on lipid surrogates, order an apob or the NMR lipid profile for the LDL-P (particle number). Perfect world: Framingham offspring study goals.
27 Cholesterol: How low? Lower seems to be better but how far is yet to be determined. Studies continue to show improved outcomes the lower we go.
28
29
30
31
32
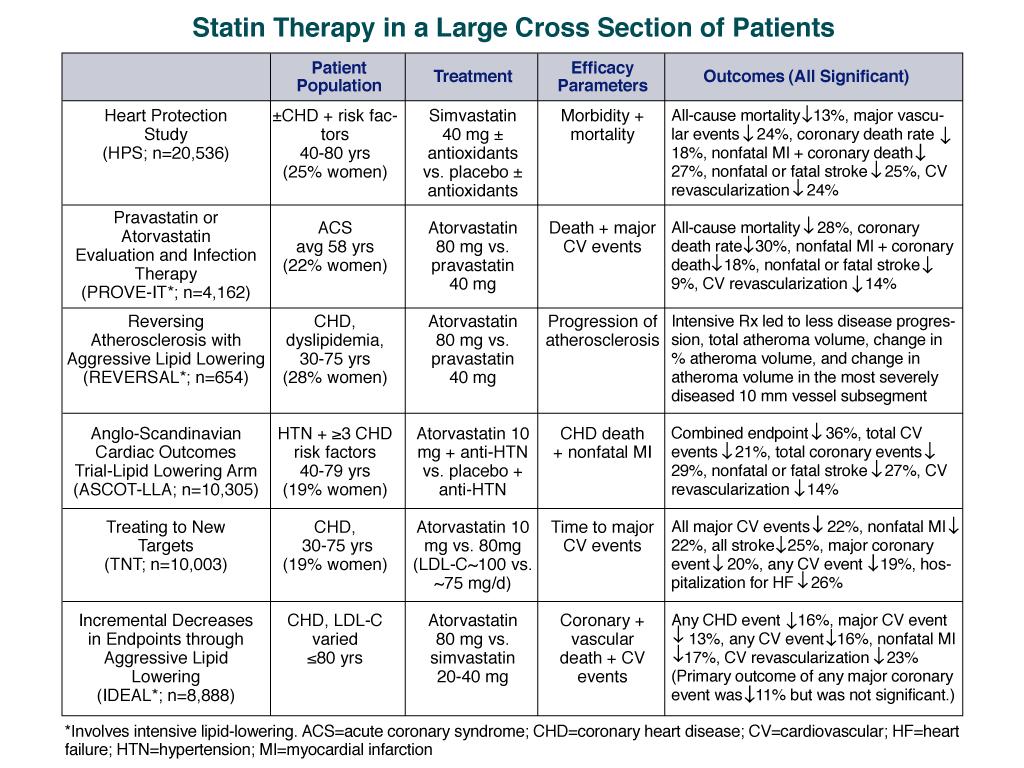
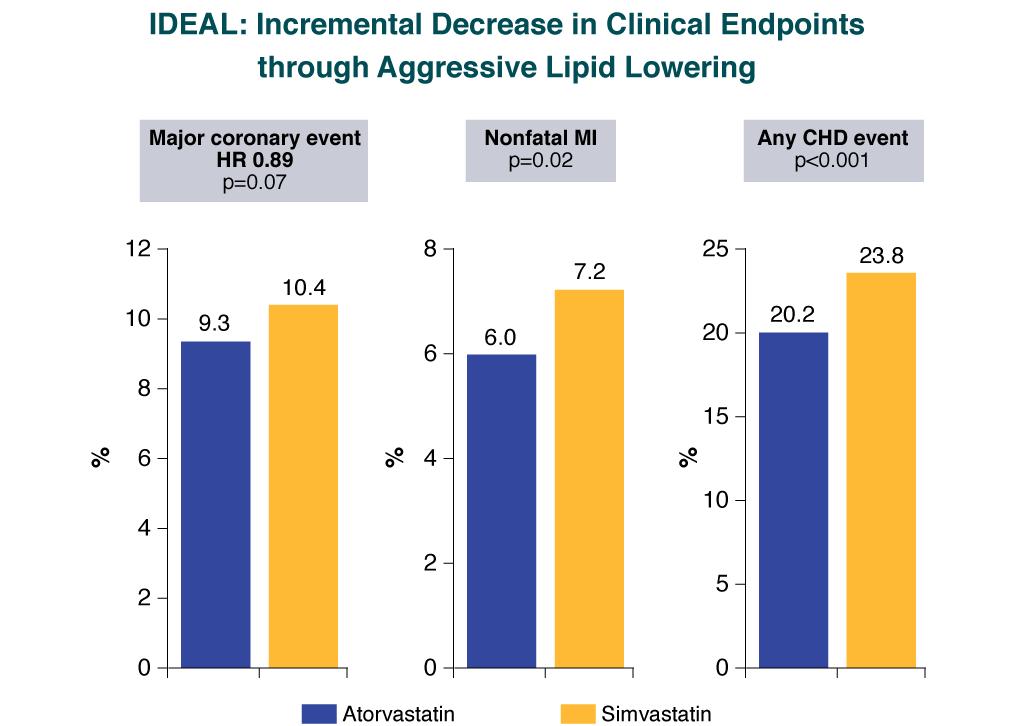
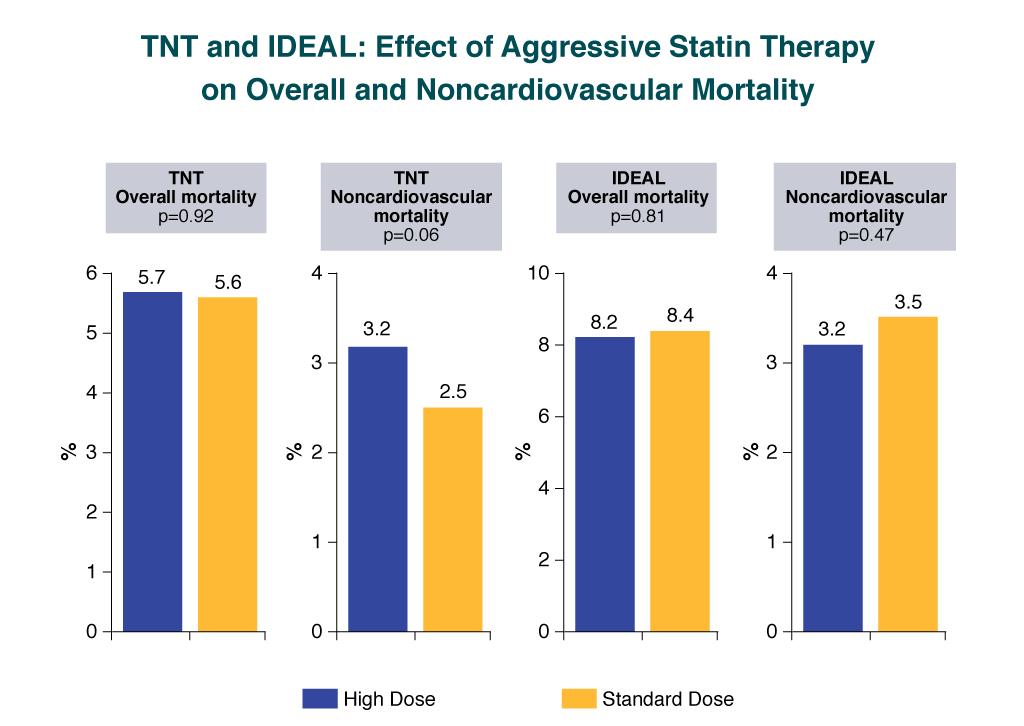
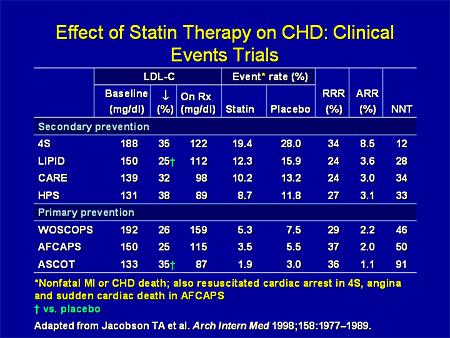
33 TNT (Treating to New Targets) Designed to test the lower is better concept. Intensive lipid-lowering therapy with atorvastatin (80mg vs 10mg) in patients with stable CHD resulted in a 25% CV event risk reduction. No difference between the two treatment groups in overall mortality. LaRosa JC et al. N Engl J Med April ; 352:
34
35
36
37
38 Low-density lipoprotein cholesterol (LDL-C) levels of trials comparing high-dose to standard-dose statin therapy Cannon, C. P. et al. J Am Coll Cardiol 2006;48: Copyright 2006 American College of Cardiology Foundation. Restrictions may apply.
39
40
41 ASTEROID: A study to evaluate the effect of rosuvastatin (40mg) on intravascular ultrasound-derived atheroma burden after 2 years of tx. Resulted in mean LDL-C from 130mg/dL to 60mg/dL and a mean of HDL-C from 43mg/dL to 49mg/dL (15% ). Resulted in significant plaque regression (Reversal). JAMA 2006; 295:
42 Modifications to NCEP ATP III TLC was re-emphasized. Use of the Framingham CAD risk calculator was recommended. Circulation July ; 110:
43 Modifications to NCEP ATP III Risk Category High Risk: CHD,PAD, Carotid vasc. Dx, AAA or CHD risk equivalents (DM or 10-yr CHD risk > 20%) Very High Risk: Above plus having multiple risk factors including DM, tobacco dependence, MetS or severe or poorly controlled risk factors (eg HBP or recent MI, ACS or recurrent CAD symptoms on Tx and CKD. Moderate Risk: Two or more risk factors (10-yr risk < 10%). High Moderate Risk: Two or more risk factors (10-yr risk > 10%). LDL-C Goal < 100mg/dL. Optional goal < 70mg/dL (CAD) Optional goal < 70mg/dL. Strongly Rec < 130mg/dL. Optional goal < 100mg/dL. Circulation July ; 110: ; JACC May ; 47:
44 Safety Analysis of Intensive Tx Among subjects treated with intensive statin therapy following ACS, there were lower rates of clinical events in those patients who achieved LDL-C < 60 mg/dl (or < 40 mg/dl) compared with those in the > mg/dl range. Lipid levels well below the current guidelines were not associated with worse safety outcomes. Therefore, there is no need to reduce statin dosage if the LDL-C levels are below target goal. Circulation 2004;110:III-498. Abstract Comparative safety of atorvastatin 80 mg versus 10 mg derived from analysis of 49 completed trials in 14,236 patients. Am J Cardiol. 2006;97:61-67
45 Very High Risk Patients The updated NCEP III definition of high risk requires established CVD plus: Multiple risk factors (especially diabetes). Severe and poorly controlled risk factors (especially continued cigarette smoking). Multiple risk factors for MetS (especially high TG >200; low HDL-C [< 40mg/dL] i.e. non-hdl-c > 130mg/dL.). Patients with ACS or recurrent anginal symptoms. CKD (Circulation September ; 114: ). GOAL LDL-C: < 70mg/dL GOAL Non-HDL-C: < 100mg/dL
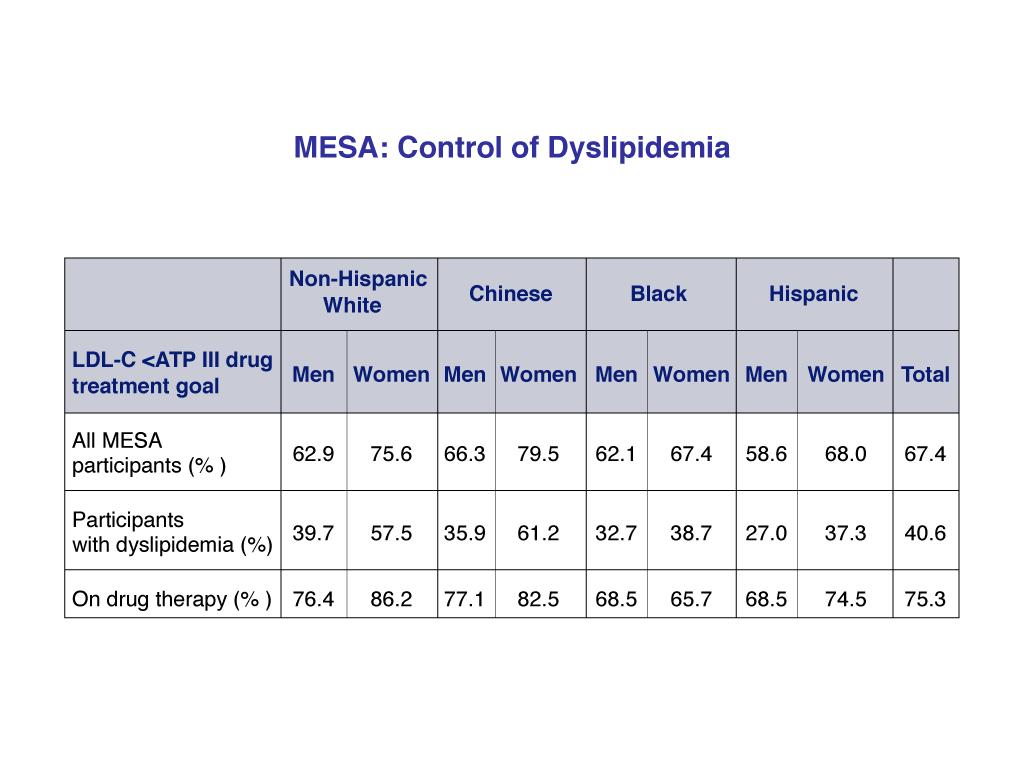
46 The Forgotten Cardiac Risk Factor: Noncompliance With Lipid- Lowering Therapy Before NCEP ATP III Update (2004) and the new secondary prevention guidelines (2006). Will be even more difficult reaching LDL-C goals post update. Goff DC Jr et al. Dyslipidemia prevalence, treatment, and control in the Multi-Ethnic Study of Atherosclerosis (MESA): gender, ethnicity, and coronary artery calcium. Circulation February ;113:
47
48
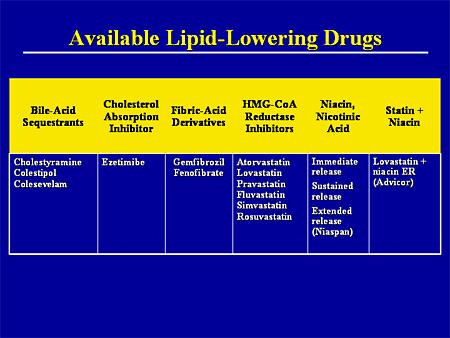
49 Effect of Therapeutic Intervention on Lowering LDL Statins Decrease LDL 18% - 55% Bile Acid Sequestrants Decrease LDL 15% - 30% Fibrates Decrease LDL 5% - 20%
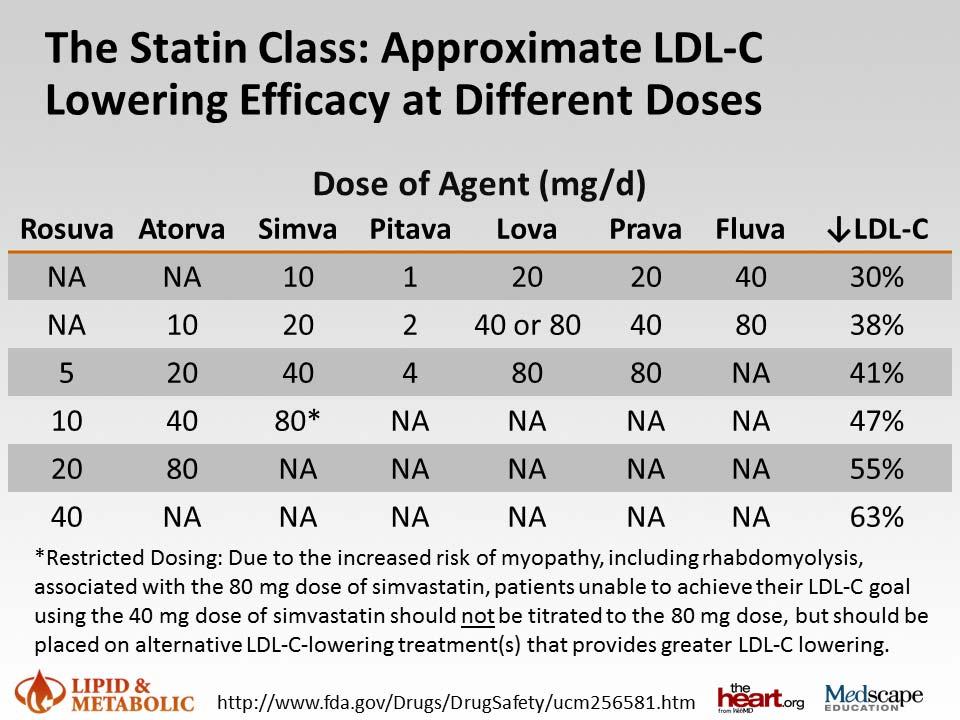
50 Available Statins % LDL-C reduction Pitavastatin (Livalo) 2 mg Rosuvastatin (Crestor) 5mg *Atorvastatin (Lipitor) 10mg 33-39% *Simvastatin (Zocor) 20mg *Lovastatin (Mevocor) 40mg *Pravastatin (Pravacol) 40mg Fluvastatin (Lescol) 80mg * Available in generic form
51
52
53
54
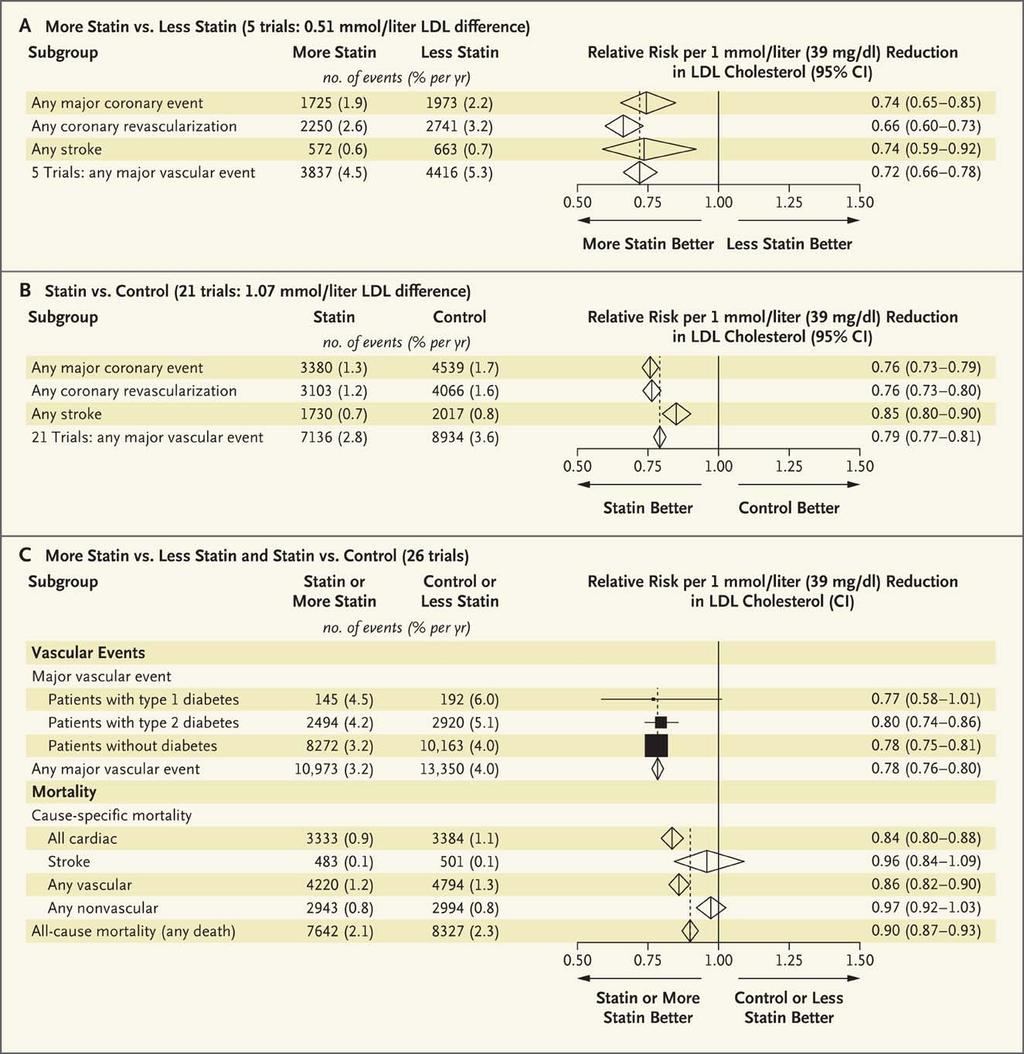
55 Effect of Statins on CV Event Rate According to Reduction in LDL-C Lancet 2010:376: file:///c:/documents%20and%20settings/mario%20maiese/desktop /Statins%20%20Is%20It%20Really%20Time%20to%20Reassess%20Benef its%20and%20risks%20%20%e2%80%94%20nejm_files/nejmp _ f1.jpeg
56
57 Residual Risk: Even with optimal statin treatment: 25-45% reduction in CV events with statins. There is 50% to 60% risk we re not addressing.
58 Residual Risk: Suggests responsibility of other risk factors, such as older age, male sex, hypertension, diabetes, cigarette smoking, and sedentary lifestyle. High-risk patients identified through measurement of lipid values and identification of other risk factors; other lipidbased risk factors include triglycerides, intermediate-density lipoproteins, and very low-density lipoproteins. (apob lipoprotein or LDL-P { particle number}) More sophisticated methods of identifying and addressing risk always being sought; maximal reduction of LDL known to be beneficial; new mechanisms of intervention still being identified, including ways of raising HDL and genetic research to help identify high-risk individuals.
59 Side Effects:
60 The number one side effect of statins is a >25% reduction in heart attacks and strokes.
61 Side Effects: Statins are well tolerated and are believed to have minimal adverse effects. Most common adverse effects are myopathies, elevations of liver enzymes, and very rarely, rhabdomyolysis. Discontinuation or reduction in the dose of statin treatment usually leads to resolution of these side effects.
62 Side Effects: In February 2012, the U.S. Food and Drug Administration (FDA) concluded that serious liver injury with statins is rare and unpredictable in individual patients, and that routine periodic monitoring of liver enzymes does not appear to be effective for detecting or preventing serious liver injury. Therefore, labels were revised to remove the need for routine periodic monitoring of liver enzymes. More recently, the debate has centered on whether use of statins causes cognitive decline, cancer, and/or diabetes mellitus.
63 Statin Benefits Offset Diabetes Risk Ridker P, et al "Cardiovascular benefits and diabetes risks of statin therapy in primary prevention: an analysis from the JUPITER trial" Lancet 2012; 380: Watts G, Ooi E "Balancing the cardiometabolic benefits and risks of statins" Lancet 2012; 380: The cardiovascular benefits of statin treatment for primary prevention outweighed the risk of developing diabetes, even among those at risk for the condition. Statin therapy prevented 134 cardiovascular events or deaths for every 54 cases of new-onset diabetes among participants with at least one risk factor for diabetes. "A major take-home message for the clinician involved in either primary or secondary prevention of cardiovascular disease is that all individuals on a statin who have major risk factors for diabetes, particularly impaired fasting glucose, need to be informed about the risk, monitored regularly for hyperglycemia, and advised to lose weight and take regular physical exercise to mitigate the emergence of diabetes."
64 FDA Alert June Physicians should stop prescribing a new 80-mg dose of simvastatin (Zocor). Do not exceed 10 mg of simvastatin daily with: amiodarone, verapamil or diltiazem. Do not exceed 20 mg of simvastatin daily with: amlodipine or ranolazine. Avoid large quantities of grapefruit juice.
65 Clues for higher risk LDL-C (per NCEP III). non HDL-C ( TC- HDL-C) 30mg/dL higher than LDL-C goal) almost always indicates LDL-P. TG (> 150mg/dL) probably > 100. HDL-C (< 40mg/dL) associated with apob and small LDL-C. VLDL-C ( TG/ 5) > 30mg/dL. TC/HDL-C > 4. TG/ HDL-C >3.8 (women) and > 4 (men) indicates a high chance of small dense LDL-C particles ( LDL-P per NMR LipoProfile)
66 Unlimited Resources If you don t want to bet patients lives on NCEP lipid surrogates get an NMR LipoProfile from LipoScience which measures LDL-P (low density lipoprotein concentration and size which gives you an accurate reflection of apob).. Not proven to decrease risk. NMR LipoProfile can be obtained thru LabCorp (LabCorp form request NMR LipoProfile)
67 No proven benefit of other lipidlowering treatment after statins.
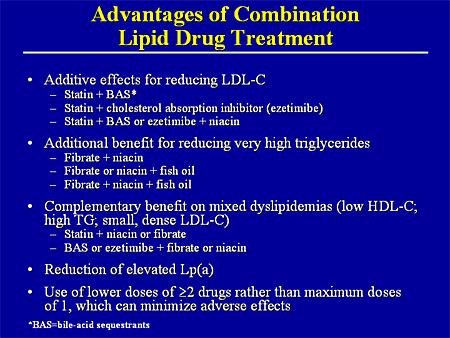
68 Be aggressive with combination therapies after statin at maximum In insulin resistant patients with abnormalities of the TG/HDL-C axis, a statin/ezetimibe/fenofibrate or Lovaza combination would solve the overwhelming majority of lipoprotein abnormalities seen in most patients (getting to LDL-C and non-hdl-c goals (apob surrogate markers) while also HDL-C &/or TG. Niaspan can also improve the numbers.
69 Generics can save millions
70 Cost Saver Message Millions saved by splitting statin tablets. No decrease in benefit. Am J Cardiol 2005; 95:
71 Fenofibrates In combination with statins doesn t interfere with catabolism & is less likely to increase risk of myopathy. Decreases TG and elevates HDL-C. Decreases small, dense LDL-C in favor of larger more buoyant LDL particles. Pleiotropic effects. Decreases cardio CRP.
72
73
74 Summary: Take Home Points Assess and Identify risk. Treat high risk aggressively to specific goals. A statin should be part of the lipid-lowering treatment program. Intensive lipid lowering with high-dose statin therapy provides a significant benefit over standard-dose therapy for preventing predominantly non-fatal cardiovascular events. Always consider safety and cost as part of selection.
75 TLC (Therapeutic Lifestyle Changes) Cornerstone of therapy Diet (South Beach or Med) Exercise (30-60 min 5x/ wk minimum preferably daily ).
76 The Problem: Will power only lasts 3 weeks and in addition it is alcohol soluble..don t have a pill for diet & exercise.
77 Sample Case Male, age 62, overweight, BP 140/90 Original Lipid Panel: TC = 210, HDL-C = 25, LDL-C = 124. TG = 307 Non HDL-C = = 185 FBS 110 Access Risk: CHD Risk calculation Goals of therapy: (Based on NCEP ATP III updated) Primary goal: LDL-C Secondary goal (TG > 200): Non-HDL-C Post Tx Lipid Panel on TriCor 145 mg and Lipitor 20mg TC = 148, HDL-C = 23, LDL-C = 67, TG = 291 Non HDL-C = 125 Treatment: TLC Meds
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Lipoprotein Particle Profile
 Lipoprotein Particle Profile 50% of people at risk for HEART DISEASE are not identified by routine testing. Why is LPP Testing The Most Comprehensive Risk Assessment? u Provides much more accurate cardiovascular
Lipoprotein Particle Profile 50% of people at risk for HEART DISEASE are not identified by routine testing. Why is LPP Testing The Most Comprehensive Risk Assessment? u Provides much more accurate cardiovascular
Changing lipid-lowering guidelines: whom to treat and how low to go
 European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
European Heart Journal Supplements (2005) 7 (Supplement A), A12 A19 doi:10.1093/eurheartj/sui003 Changing lipid-lowering guidelines: whom to treat and how low to go C.M. Ballantyne Section of Atherosclerosis,
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
STATIN UTILIZATION MANAGEMENT CRITERIA
 STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Accelerated atherosclerosis begins years prior to the diagnosis of diabetes
 Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Joslin Diabetes Forum 211: Optimizing Care for the Practicing Clinician Risk for atherosclerosis is 2 4 times greater in patients with diabetes CVD accounts for 65% of diabetic mortality >5% of patients
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID?
 Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Cardiovascular Complications of Diabetes
 VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
VBWG Cardiovascular Complications of Diabetes Nicola Abate, M.D., F.N.L.A. Professor and Chief Division of Endocrinology and Metabolism The University of Texas Medical Branch Galveston, Texas Coronary
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Established Risk Factors for Coronary Heart Disease (CHD)
") Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
Getting Patients to Make Small Lifestyle Changes That Result in SIGNIFICANT Improvements in Health - Prevention of Diabetes and Obesity for Better Health Maureen E. Mays, MD, MS, FACC Director ~ Portland
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Hi Lipidaholics: This week case is a very common lipid disorder, but what are the medications needed to achieve goals of therapy.
 LIPID CASE 251 Treating HDL Size Hi Lipidaholics: This week case is a very common lipid disorder, but what are the medications needed to achieve goals of therapy. I was asked about a 44 year old physically
LIPID CASE 251 Treating HDL Size Hi Lipidaholics: This week case is a very common lipid disorder, but what are the medications needed to achieve goals of therapy. I was asked about a 44 year old physically
Pharmaceutical Help to Control Cholesterol
 Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention Center: Rooms 315 & 316
 Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Case # 278 Should lipoprotein cholesterol assays disappear?
 Case # 278 Should lipoprotein cholesterol assays disappear? Let's get into the case: I was contacted by a provider who states: "I have a 70 year old guy with absolutely no cardiac risk factors except for
Case # 278 Should lipoprotein cholesterol assays disappear? Let's get into the case: I was contacted by a provider who states: "I have a 70 year old guy with absolutely no cardiac risk factors except for
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Comprehensive Treatment for Dyslipidemias. Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium
 Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
Eyes on Korean Data: Lipid Management in Korean DM Patients
 Eyes on Korean Data: Lipid Management in Korean DM Patients ICDM Luncheon Symposium Sung Rae Kim MD PhD Division of Endocrinology and Metabolism The Catholic University of Korea Causes of Death in People
Eyes on Korean Data: Lipid Management in Korean DM Patients ICDM Luncheon Symposium Sung Rae Kim MD PhD Division of Endocrinology and Metabolism The Catholic University of Korea Causes of Death in People
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention Center: Rooms 315 & 316
 Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease
 AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AMERICAN COLLEGE OF ENDOCRINOLOGY Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Writing Committee Chair: Paul S. Jellinger,
AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AMERICAN COLLEGE OF ENDOCRINOLOGY Guidelines for Management of Dyslipidemia and Prevention of Cardiovascular Disease Writing Committee Chair: Paul S. Jellinger,
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients. Copyright. Not for Sale or Commercial Distribution
 CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
Achieving Lipid Goals: 2008 Update. Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy
 Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy Discuss relationship between lipid values and coronary events Evaluate clinical
Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy Discuss relationship between lipid values and coronary events Evaluate clinical
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
What Else Do You Need to Know? Presenter Disclosure Information. Case 1: Cardiovascular Risk Assessment in a 53-Year-Old Man. Learning Objectives
 9: 1:am Understanding Dyslipidemia Testing and Screening: Importance of Lipoprotein Particle Analysis SPEAKER Matthew Sorrentino, MD, FACC Presenter Disclosure Information The following relationships exist
9: 1:am Understanding Dyslipidemia Testing and Screening: Importance of Lipoprotein Particle Analysis SPEAKER Matthew Sorrentino, MD, FACC Presenter Disclosure Information The following relationships exist
Which CVS risk reduction strategy fits better to carotid US findings?
 Which CVS risk reduction strategy fits better to carotid US findings? Dougalis A, Soulaidopoulos S, Cholongitas E, Chalevas P, Vettas Ch, Doumtsis P, Vaitsi K, Diavasti M, Mandala E, Garyfallos A 4th Department
Which CVS risk reduction strategy fits better to carotid US findings? Dougalis A, Soulaidopoulos S, Cholongitas E, Chalevas P, Vettas Ch, Doumtsis P, Vaitsi K, Diavasti M, Mandala E, Garyfallos A 4th Department
Atherosclerotic Disease Risk Score
 Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Atherosclerotic Disease Risk Score Kavita Sharma, MD, FACC Diplomate, American Board of Clinical Lipidology Director of Prevention, Cardiac Rehabilitation and the Lipid Management Clinics September 16,
Best Lipid Treatments
 Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
Best Lipid Treatments Pam R. Taub MD, FACC Director of Step Family Cardiac Rehabilitation and Wellness Center Associate Professor of Medicine UC San Diego Health System Overview of Talk Review of pathogenesis
The New Gold Standard for Lipoprotein Analysis. Advanced Testing for Cardiovascular Risk
 The New Gold Standard for Lipoprotein Analysis Advanced Testing for Cardiovascular Risk Evolution of Lipoprotein Testing The Lipid Panel Total Cholesterol = VLDL + LDL + HDL Evolution of Lipoprotein Testing
The New Gold Standard for Lipoprotein Analysis Advanced Testing for Cardiovascular Risk Evolution of Lipoprotein Testing The Lipid Panel Total Cholesterol = VLDL + LDL + HDL Evolution of Lipoprotein Testing
10/1/2008. Therapy? Disclosure Statement
 What s New in Lipid Therapy? Brooke Hudspeth, PharmD Diabetes Care Kroger Pharmacy Disclosure Statement In accordance with policies set forth by the Accreditation Council for Continuing Medical Education
What s New in Lipid Therapy? Brooke Hudspeth, PharmD Diabetes Care Kroger Pharmacy Disclosure Statement In accordance with policies set forth by the Accreditation Council for Continuing Medical Education
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Qué factores de riesgo lipídicos debemos controlar? En qué medida?
 Qué factores de riesgo lipídicos debemos controlar? En qué medida? Risk category High risk: CHD or CHD risk equivalents (10- year risk >20%) Moderately high risk: two or more risk factors (10-year risk
Qué factores de riesgo lipídicos debemos controlar? En qué medida? Risk category High risk: CHD or CHD risk equivalents (10- year risk >20%) Moderately high risk: two or more risk factors (10-year risk
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
Dyslipidaemia. Is there any new information? Dr. A.R.M. Saifuddin Ekram
 Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Diabetic Dyslipidemia
 Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Diabetic Dyslipidemia Dr R V S N Sarma, M.D., (Internal Medicine), M.Sc., (Canada), Consultant Physician Cardiovascular disease (CVD) is a significant cause of illness, disability, and death among individuals
Metabolic Syndrome. Bill Roberts, M.D., Ph.D. Professor of Pathology University of Utah
 Metabolic Syndrome Bill Roberts, M.D., Ph.D. Professor of Pathology University of Utah Objectives Be able to outline the pathophysiology of the metabolic syndrome Be able to list diagnostic criteria for
Metabolic Syndrome Bill Roberts, M.D., Ph.D. Professor of Pathology University of Utah Objectives Be able to outline the pathophysiology of the metabolic syndrome Be able to list diagnostic criteria for
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Lessons from Recent Atherosclerosis Trials
 Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
High ( 50%) Restrictions mg 20-40mg PA; TS ⱡ 15 ⱡ
 Restrictions mg 20-40mg PA; TS ⱡ 15 ⱡ") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/16, 5/15, 2/14, 5/12, LOB AFFECTED: Medi-Cal
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/16, 5/15, 2/14, 5/12, LOB AFFECTED: Medi-Cal
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Imaging Biomarkers: utilisation for the purposes of registration. EMEA-EFPIA Workshop on Biomarkers 15 December 2006
 Imaging Biomarkers: utilisation for the purposes of registration EMEA-EFPIA Workshop on Biomarkers 15 December 2006 Vascular Imaging Technologies Carotid Ultrasound-IMT IVUS-PAV QCA-% stenosis 2 ICH E
Imaging Biomarkers: utilisation for the purposes of registration EMEA-EFPIA Workshop on Biomarkers 15 December 2006 Vascular Imaging Technologies Carotid Ultrasound-IMT IVUS-PAV QCA-% stenosis 2 ICH E
Hyperlipidemia: Past and Present. Rebecca Khaimova, PharmD The Brooklyn Hospital Center
 Hyperlipidemia: Past and Present Rebecca Khaimova, PharmD The Brooklyn Hospital Center Rkhaimova@tbh.org Conflicts of Interest None to disclose Learning Objectives for Pharmacist Describe the pathophysiology
Hyperlipidemia: Past and Present Rebecca Khaimova, PharmD The Brooklyn Hospital Center Rkhaimova@tbh.org Conflicts of Interest None to disclose Learning Objectives for Pharmacist Describe the pathophysiology
Joshua Shepherd PA-C, MMS, MT (ASCP)
") Joshua Shepherd PA-C, MMS, MT (ASCP) None What is Cholesterol? Why cholesterol is it important? Review the National Cholesterol Education Programs guidelines (NCEP-ATPIII) Discuss New guidelines from the
Joshua Shepherd PA-C, MMS, MT (ASCP) None What is Cholesterol? Why cholesterol is it important? Review the National Cholesterol Education Programs guidelines (NCEP-ATPIII) Discuss New guidelines from the
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology
 Lipid Management Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology Clinical Director, Lipid Clinics Assistant Professor Division of Cardiovascular Medicine The Ohio State University Wexner
Lipid Management Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology Clinical Director, Lipid Clinics Assistant Professor Division of Cardiovascular Medicine The Ohio State University Wexner
LDL How Low can (should) you Go and be Safe
 you Go and be Safe") LDL How Low can (should) you Go and be Safe Edward Shahady MD, FAAFP, ABCL Clinical Professor Family Medicine Medical Director Diabetes Master Clinician Program Definition of Low LDL National Health and
LDL How Low can (should) you Go and be Safe Edward Shahady MD, FAAFP, ABCL Clinical Professor Family Medicine Medical Director Diabetes Master Clinician Program Definition of Low LDL National Health and
Hyperlipidemia. Intern Immersion Block 2015
 Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Hyperlipidemia Intern Immersion Block 2015 Christopher Wong, MD Division of General Internal Medicine University of Washington cjwong@u.washington.edu Welcome! Disclosures: royalties from book sales (not
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
American Osteopathic College of Occupational and Preventive Medicine 2012 Mid-Year Educational Conference St. Petersburg, Florida
 The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
The 21 st Century Paradigm Shift: Prevention Rather Than Intervention for the Treatment of Stable CHD The Economic Burden of Cardiovascular Diseases Basil Margolis MD, FACC, FRCP Director, Preventive Cardiology
Disclosures No relationships (not even to an employer) No off-label uses. Cholesterol Lowering Guidelines: What now?
 No off-label uses. Cholesterol Lowering Guidelines: What now?") Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Disclosures No relationships (not even to an employer) No off-label uses Cholesterol Lowering Guidelines: What now?, FACP 1 2 65-year-old white woman Total cholesterol 175mg/dL HDL 54 mg/dl LDL 96 mg/dl
Risk Factors for Heart Disease
 Risk Factors for Heart Disease Risk Factors we cannot change (Age, Gender, Family History) Risk Factors we can change (modifiable) Smoking Blood pressure Cholesterol Diabetes Inactivity Overweight Stress
Risk Factors for Heart Disease Risk Factors we cannot change (Age, Gender, Family History) Risk Factors we can change (modifiable) Smoking Blood pressure Cholesterol Diabetes Inactivity Overweight Stress
Total risk management of Cardiovascular diseases Nobuhiro Yamada
 Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible
Nobuhiro Yamada The worldwide burden of cardiovascular diseases (WHO) To prevent cardiovascular diseases Beyond LDL Multiple risk factors With common molecular basis The Current Burden of CVD CVD is responsible