Achieving Lipid Goals: 2008 Update. Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy
|
|
|
- Erika Higgins
- 6 years ago
- Views:
Transcription
1 Achieving Lipid Goals: 2008 Update Laura Hansen, Pharm.D. Associate Professor, University of Colorado School of Pharmacy


2 Discuss relationship between lipid values and coronary events Evaluate clinical data for aggressive lipid management Describe rationale for combination therapy Explain how to achieve aggressive goals with combination therapy
3

4 17% of US adults have total cholesterol of 240 mg/dl or higher Average total cholesterol in adults is 203 mg/dl > 30% of adults have LDL that exceeds goal 16% of adults over 20 need lifestyle changes 13-46% meet criteria for drug treatment National Center for Health Statistic. Health, United States, 2006 J Gen Intern Med 2006;21: Am Heart J 2005;150:
5 Reduction of CHD risk Reduction of cardiovascular morbidity and mortality Improved survival in pts. with or without CHD Reduced need for procedures (PTCA, CABG) Reduced progression of atherosclerosis Reduction in stroke risk


6 % % by Risk Group % 18% 38% 0 Low Risk High Risk CHD Patients All Subjects Category No CHD No CHD < 2 RF 2 RF LDL Goal < 160 mg/dl <130 mg/dl <100 mg/dl Arch Intern Med 2000;160:
7 LDL < 100 LDL < 70 Patients (%) Total Very High Risk MS DM HTN + low HDL TG>200 + Low HDL 54 Smoking NEPTUNE II = NCEP Evaluation Project Utilizing Novel E-Technology Am J Cardiol 2005;96:
8 Aggressive goals Many patients are never treated Poor adherence Most LDL-C reduction occurs with starting dose of statins Doses are not titrated
9 Evaluate risk of patient Established CHD/CHD risk equivalent Multiple (2+) risk factors Zero-one risk factor Evaluate lipid profile and cholesterol goals Primary target: LDL Circulation 2004;110:
10 Cigarette smoking Hypertension Low HDL-C (<40 mg/dl) Male 45 or Female 55 Family history of premature heart disease (male parent or sibling before 55 or female before 65) Circulation 2004;110:
11 Cardiovascular disease Established coronary and other atherosclerotic vascular disease Carotid artery disease Peripheral arterial disease Atherosclerotic aortic disease Cardiovascular Risk Equivalent Diabetes 10-year risk for CHD > 20% Circulation 2004;110: J Am Coll Cardiol 2006;47:2130-9
12 Risk Assessment Tool for Estimating 10-year Risk of Developing Hard CHD (Myocardial Infarction and Coronary Death) Uses data from the Framingham Heart Study to estimate 10-year risk for hard coronary heart disease outcomes (myocardial infarction and coronary death) Designed to estimate risk in adults aged 20 and older who do not have heart disease or diabetes.
13 Steve is a 48-year-old who was recently diagnosed with high cholesterol. History: smokes 1 ppd, no medications, construction worker, denies any family history of heart disease Lipid profile: Total cholesterol = 215 mg/dl, LDL =160 mg/dl HDL-C = 30 mg/dl, TG=150 mg/dl BP:138/80
14 Risk Category CHD LDL Goal < 100 mg/dl (<70 is reasonable) CRE (10-year risk > 20%) < 100 mg/dl 2+ Risk Factors (10 year risk < 20 %) < 130 mg/dl (<100 is option) 0 1 Risk Factor < 160 mg/dl CRE = CHD Risk Equivalent J Am Coll Cardiol 2006;47: Circulation 2004;110:
15 Category HDL Goals > 40 mg/dl (men) > 50 mg/dl (women) Triglycerides < 150 mg/dl NCEP ATP III HDL > 40 for both genders AHA HDL > 40 for men, > 45 for women ADA HDL > 50 for women
16 Reverse cholesterol transport Reduction of oxidative modification of LDL-C Inhibition of expression of adhesion molecules by cytokine-activated endothelial cells (anti-inflammatory)
17 Reducing LDL from mg/dl baseline to mg/dl with statins reduces CV events 25% 3 out of 4 events occurred despite statin therapy Only 1 in 3 CHD patients is at or below the more liberal current LDL goal of 100 mg/dl. NEJM 2004;350: Int J Clin Pract 2003;57:


18
19 J Am Coll Cardiol 2004;43:
20 J Am Coll Cardiol 2004;43:



21 J Am Coll Cardiol 2004;43:
22 Cholesterol is an essential component of cell membrane and precursor for bile acid, steroid hormone, and vitamin D synthesis. People with naturally low LDL longevity No relationship between on-treatment LDL level and medication adverse effects


23 For every 30 mg/dl change in LDL, relative risk for CHD is changed by about 30%


24 Decreased inflammation ( CRP) Improvement in endothelial dysfunction Decreased incidence of PVD, stroke, dementia, macular degeneration, aortic stenosis, and osteoporosis-related hip and vertebral fractures
25 Blood Biliary C (~1000 mg/day) Liver VLDL IDL LDL Absorption Intestine Excretion Dietary C ( mg/day) Saturated/Trans Fats
26 What does it take to achieve an LDL-C of 70 or 100mg/dl?
 and scheduled for follow-up in 3")
27 Lipid profile: Total cholesterol = 215 mg/dl, LDL =160 mg/dl HDL-C = 30 mg/dl, TG=150 mg/dl Started on TLC (low fat diet and exercise 3 x/wk) and scheduled for follow-up in 3 months.
28 TLC Component LDL-C Low saturated fat/dietary cholesterol 12-15% Viscous fiber (10 25 g/d) 10-15% Plant stanols/sterols (1.5-4 g/d) 10-20% Soy protein (20-30 g/d) 5-7% Policosanol (sugar cane) <10-20% Fish oils (Lovaza, 4-9 g/day) Weight loss (5-10%) TG 25-35%, HDL 9% Variable 120 min/wk exercise HDL 2.5 mg/dl
29
30 Steve has been carefully following the low fat diet and walking or going to gym 3 days per week. Lipid profile LDL =136 mg/dl HDL-C = 34 mg/dl TG=140 mg/dl
31 Agent LDL TG HDL-C Colestipol/Cholestyramine Colesevelam (Welchol) 10-25% 0-12% 3-10% Niacin 10-25% 20-50% 15-35% Fenofibrate (Tricor) Gemfibrozil (Lopid) 10-15% 30-60% 10-30% Ezetimibe (Zetia) 15-23% 7-9% 4-9% Atorvastatin (Lipitor) Fluvastatin (Lescol) Lovastatin (Mevacor, generic) Pravastatin (Pravacol) Rosuvastatin (Crestor) Simvastatin (Zocor, generic) 21-60% 7-30% 5-15%
32 Intensity of initial statin therapy should be sufficient to reach a 30-40% reduction in LDL-C levels Circulation 2004;110:
33 What would his LDL goal be? How would you achieve this goal?
")

34 High dose statin (+ diet and exercise) Combination therapy (+ diet and exercise)
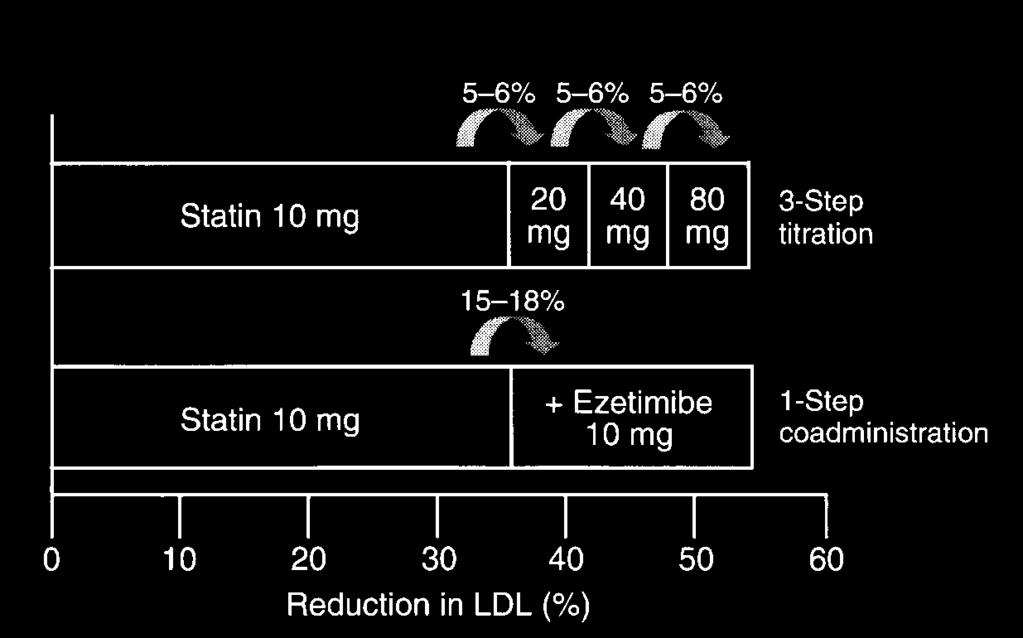
35 Rule of 6 s Still may not reach goal Eur Heart J 2001;3:E11-16.
36 Dose related adverse effects Elevations of LFTs potential for liver toxicity Overall 0.5-2% of patients Appears to be higher rate with higher doses Myopathy Overall % <0.1% progress to rhabdomyolysis Rate does appear to be higher with higher doses Pharmacotherapy 2005;25: Curr Med Res Opin 2001;17:43-50 J Am Coll Cardiol 2002;40:567-72
37 Chronic use of medications known to interact with statins Patients > 80 Thin or frail women Multisystem disease, especially chronic renal failure from diabetes Perioperative Asian Americans (Rosuvastatin) J Am Coll Cardiol 2002;40:


38 Myopathy and rhabdomyolysis are associated with statin therapy (class effect) Elevated creatine kinase (CK) levels may indicate statin-induced muscle damage Muscle weakness or pain without CK elevation may indicate statin-induced muscle damage Myopathy and rhabdomyolysis risk increases with increased statin dose and serum levels Myopathy and rhabdomyolysis risk increases with drug-drug interactions that retard statin metabolism Drugs that can interact to amplify statin related myopathy include gemfibrozil and CYP-3A4 inhibitors Am J Cardiol. 2006;97:69C-76C

39 Monitoring CK levels is recommended only for symptomatic patients Patients on statin therapy do not require routine monitoring of liver function*, renal function, or cognitive function *Note: Liver function monitoring is currently recommended by the regulatory authorities and manufacturers Am J Cardiol. 2006;97:69C-76C
40 Statins can produce muscle pain and weakness, which can very rarely become an important medical problem Serious liver damage due to statins is extremely rare Marketed doses of statins do not have any direct adverse effects on the kidney Statins do not cause peripheral neuropathy and do not impair memory or cognition Am J Cardiol. 2006;97:69C-76C
41 Statin + Niacin Statin + Fibrate Statin + BAS Statin + Stanol/sterol Statin + Ezetimibe Fibrate + Ezetimibe Triple therapy
42 Efficacy HATS: 160 pts with CHD, low HDL, normal LDL Simvastatin (10 mg titrated) + Slo-Niacin 1000 mg BID 90% reduction in CV events over 3 yrs, 0.4% regression of lesions, LDL 42%, HDL 26% Lovastain 40 mg/d-niacin ER 2000 mg/d LDL 47%, TG 41%, HDL 41% Adverse effects 4 of 871 cases of statin-induced rhabdomyolysis were attributed to statin/niacin combo 0.5% with elevated LFTs N Engl J Med 2001;345: Am J Cardiol 2002;89:
43 Efficacy Fenofibrate 300 mg/d + pravastatin 20 mg/d or simvastatin 10 mg/d LDL 28%, TG 41%, HDL 22% Fenofibrate 200 mg/d + atorvastatin 20 mg/d LDL 46%, TG 50%, HDL 22% Safety % overall frequency of muscle damage 9% of rhabdomyolysis cases (statin + gemfibrozil) Pharmacotherapy 2005;25: Diabetes Care 2002;25: Ann Pharmacother 2001;35:
44 Statins Biliary C (~1000 mg/day) Dietary C ( mg/day) Blood Liver VLDL IDL LDL Intestine Saturated/Trans Fats Absorption CAI/ BAS/ Stanol Excretion CAI=cholesterol absorption inhibitor
45 Efficacy Colesevelam 3.6 g/d + simvastatin 10 mg/d LDL by 42% Colesevelam 3.8 g/d + atorvastatin 10 mg/d LDL by 48% Issues Side effects with older BAS rarely get full effect Colesevelam 6 tablets/day Increases in TG Am J Med 2001;110: Atherosclerosis 2001;158:407-16
46 Efficacy Meta analysis of 41 studies of stanol/sterol alone Lowers LDL 10% 2.24 g/d of stanol esters (80% rapeseed oil spread) added to simvastatin mg Lowered LDL an additional 20% Safety No known adverse effects d caloric intake from stanol/sterol spreads (9-27 gm fat) Mayo Clin Proc 2003;78: Arterioscler Thromb Vasc Biol 2000;20:


47 As two separate products statin + ezetimibe (Zetia ) Combination product simvastatin/ezetimibe (Vytorin )
48 % Reduction in LDL-C Atorvastatin Lovastatin Pravastatin Rosuvastatin Simvastatin E10mg+S10mg S* *atorvastatin 80 mg, lovastatin 40mg, pravastatin 40 mg, rosuvastatin 10 mg, simvastatin 80 mg Eur Hear J 2002;4:J9-J18 Circulation 2003;107:
49 EASE: 3030 patients on stable statin dose not at goal, ezetimibe 10 mg/d or placebo Parameter P + Statin E + Statin p value ALT 3X ULN NS AST 3X ULN NS CK 10X ULN w/or w/out symptoms NS ALT, alanine transaminase; AST aspartate transaminase; CK, creatine kinase; ULN, upper limit of normal ACC 53rd Annual Scientific Session; March 2004; New Orleans, LA
50 12 wk trial in 887 patients Drug regimens studied: Placebo Ezetimibe 10 mg qd Simvastatin 10 mg, 20 mg, 40 mg, or 80 mg Ezetimibe/simvastatin (Vytorin) 10/10 mg, 10/20 mg, 10/40 mg, or 10/80 mg Results: Ezetimibe/simvastatin 10/10 mg simvastatin 80 mg ( LDL 46% ) Ezetimibe/simvastatin 10/80 mg LDL 60% Mayo Clinic Proc 2004;79:

51 10/10mg 10mg 20mg 10/40mg 40mg 10/80mg 80mg * * * *Statistically significant Am J Cardiol 2004;93:
52 Eur Heart J 2001;3:E11-16.
53 Percent * p<0.01 Patients reaching LDL-C goal < 70 mg/dl * Atorvastatin dose (mg) Ezetimibe 10 mg/simvastatin dose (mg) 20 * 39 * 57 * 64 Drugs Affecting Lipid Metabolism Meeting 10/2004; Abstract 114.
54 Multinational, randomized, double-blind, trial 10 mg ezetimibe + 80 mg simvastatin vs. simvastatin 80 mg in 720 patients with Heterozygous Familial Hypercholesterolemia (HeFH). Combo 58% drop in LDL vs. 41% for simvastatin Change in carotid artery intima thickness was no different
55 Combo Statin + fenofibrate 145 mg Statin + niacin 1.5g (Niaspan) Statin + colesevelam 3.75 g Statin + sterol 3 tabs/day (CholestaPro) Statin + ezetimibe 10 mg (Zetia) Additiona l LDL Costs / day* Comments 10% $3.33 TG & Lp(a), HDL 10-15% $8.17 Same as above, $3.29 for lovastatin/niacin (Advicor 1000/20) 10-16% $8.60 Potential to TG, 6 tabs 10-20% $4.02 Calories w/spread, no effect on HDL, TG, or Lp(a) 23-26% $5.37 Single pill option (Vytorin, $3.03) * simvastatin 10 mg + dose given of other agent Drugstore.com 1/20/08
56 Additive effects for reducing LDL-C Statin + ezetimibe Statin + ezetimibe or BAS + niacin Additional benefit for reducing very high TG Fibrate + niacin Fibrate or niacin + fish oil Fibrate + niacin + fish oil Am Heart J 2004;148:S9-13
57 Complimentary benefit for mixed dyslipidemias (low HDL-C, high TG, high LDL-C) Statin + niacin or fenofibrate Ezetimibe + fenofibrate or niacin fenofibrate 160 mg + ezetimibe 10 mg LDL 22%, HDL 20%, TG 46% Am Heart J 2004;148:S9-13 J Am Coll Cardiol. 2006;47:
58 Agent LDL TG HDL-C Colestipol/Cholestyramine Colesevelam (Welchol) 10-25% 0-12% 3-10% Niacin 10-25% 20-50% 15-35% Fenofibrate (Tricor) Gemfibrozil (Lopid) 10-15% 30-60% 10-30% Ezetimibe (Zetia) 15-23% 7-9% 4-9% Atorvastatin (Lipitor) Fluvastatin (Lescol) Lovastatin (Mevacor, generic) Pravastatin (Pravacol) Rosuvastatin (Crestor) Simvastatin (Zocor, generic) Ezetimibe/simvastatin (Vytorin) 21-60% 7-30% 5-15% 46-60% 14-35% 6-12%
59 Maintaining dietary and exercise changes Losing weight and keeping it off Adherence and persistence Opportunity for Pharmacist Involvement
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
Pharmaceutical Help to Control Cholesterol
 Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
Pharmaceutical Help to Control Cholesterol Catherine E. Cooke, PharmD, BCPS, PAHM President, PosiHealth, Inc. Clinical Associate Professor, Univ. of Maryland This program has been brought to you by PharmCon
MOLINA HEALTHCARE OF CALIFORNIA
 MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
MOLINA HEALTHCARE OF CALIFORNIA HIGH BLOOD CHOLESTEROL IN ADULTS GUIDELINE Molina Healthcare of California has adopted the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel
STATIN UTILIZATION MANAGEMENT CRITERIA
 STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
STATIN UTILIZATION MANAGEMENT CRITERIA DRUG CLASS: HMG Co-A Reductase Inhibitors & Combinations Agents which require prior review: Advicor (niacin extended-release/lovastatin) Crestor (rosuvastatin)(5mg,10mg,
Non-Statin Lipid-Lowering Agents M Holler - Last updated: 10/2016
 Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
High ( 50%) Restrictions mg 20-40mg PA; TS ⱡ 15 ⱡ
 Restrictions mg 20-40mg PA; TS ⱡ 15 ⱡ") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/16, 5/15, 2/14, 5/12, LOB AFFECTED: Medi-Cal
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/9/2017 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/16, 5/15, 2/14, 5/12, LOB AFFECTED: Medi-Cal
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin
 and Fixed-dose Combination Products Containing a Statin") Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin Final Report Update 5 November 2009 This report reviews information about the comparative
Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin Final Report Update 5 November 2009 This report reviews information about the comparative
Treating Lipids for Prevention of CAD in Women: Matching Therapy to Risk
 TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
TREATING LIPIDS FOR PREVENTION OF CAD IN WOMEN: MATCHING THERAPY TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
It is the policy of health plans affiliated with PA Health & Wellness that Vytorin is medically necessary when the following criteria are met:
 Clinical Policy: Ezetimibe and Simvastatin (Vytorin) Reference Number: PA.CP.PMN.77 Effective Date: 02.01.17 Last Review Date: 07.18 Revision Log Description Ezetimibe/simvastatin (Vytorin ) contains ezetimibe,
Clinical Policy: Ezetimibe and Simvastatin (Vytorin) Reference Number: PA.CP.PMN.77 Effective Date: 02.01.17 Last Review Date: 07.18 Revision Log Description Ezetimibe/simvastatin (Vytorin ) contains ezetimibe,
The new guidelines issued in PRESENTATIONS... Future Outlook: Changing Perspectives on Best Practice
 ... PRESENTATIONS... Future Outlook: Changing Perspectives on Best Practice Based on a presentation by Daniel J. Rader, MD Presentation Summary The guidelines recently released by the National Cholesterol
... PRESENTATIONS... Future Outlook: Changing Perspectives on Best Practice Based on a presentation by Daniel J. Rader, MD Presentation Summary The guidelines recently released by the National Cholesterol
High ( 50%) Restrictions mg 20-40mg Simvastatin (Zocor) 10mg 20-40mg $1.66 Pravastatin (Pravachol) mg $6.
 Restrictions mg 20-40mg Simvastatin (Zocor) 10mg 20-40mg $1.66 Pravastatin (Pravachol) mg $6.") MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/8/2018 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/17, 5/16, 5/15, 2/14, LOB AFFECTED: Medi-Cal
MEDICATION COVERAGE POLICY PHARMACY AND THERAPEUTICS ADVISORY COMMITTEE POLICY: Cholesterol P&T DATE: 5/8/2018 THERAPEUTIC CLASS: Cardiovascular REVIEW HISTORY: 5/17, 5/16, 5/15, 2/14, LOB AFFECTED: Medi-Cal
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Hyperlipidemia: Past and Present. Rebecca Khaimova, PharmD The Brooklyn Hospital Center
 Hyperlipidemia: Past and Present Rebecca Khaimova, PharmD The Brooklyn Hospital Center Rkhaimova@tbh.org Conflicts of Interest None to disclose Learning Objectives for Pharmacist Describe the pathophysiology
Hyperlipidemia: Past and Present Rebecca Khaimova, PharmD The Brooklyn Hospital Center Rkhaimova@tbh.org Conflicts of Interest None to disclose Learning Objectives for Pharmacist Describe the pathophysiology
Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention Center: Rooms 315 & 316
 Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Update on the Treatment of Hyperlipidemia
 Update on the Treatment of Hyperlipidemia Wafaa Abou-Zeineddine, PharmD Medstar Washington Hospital Center Washington Metropolitan Society of Health Systems Pharmacists May 30, 2015 Please MUTE phones
Update on the Treatment of Hyperlipidemia Wafaa Abou-Zeineddine, PharmD Medstar Washington Hospital Center Washington Metropolitan Society of Health Systems Pharmacists May 30, 2015 Please MUTE phones
Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology
 Lipid Management Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology Clinical Director, Lipid Clinics Assistant Professor Division of Cardiovascular Medicine The Ohio State University Wexner
Lipid Management Kavita Sharma, MD Diplomate, American Board of Clinical Lipidology Clinical Director, Lipid Clinics Assistant Professor Division of Cardiovascular Medicine The Ohio State University Wexner
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Statin Therapy Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Statin Therapy Prime Therapeutics will review Prior Authorization requests. Prior Authorization
Statin Therapy Page 1 of 10 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Statin Therapy Prime Therapeutics will review Prior Authorization requests. Prior Authorization
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Cholesterol. Medicines To Help You
 Medicines To Help You Cholesterol Use this guide to help you talk to your doctor, pharmacist, or nurse about your cholesterol medicines. The guide lists all of the FDA-approved products now available to
Medicines To Help You Cholesterol Use this guide to help you talk to your doctor, pharmacist, or nurse about your cholesterol medicines. The guide lists all of the FDA-approved products now available to
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
CHOLESTEROL REDUCING MEDICATIONS. Five Main Categories. 1. Statins 2. Fibrates 3. Resins 4. Niacin 5. Cholesterol absorption inhibitor
 Page 1 of 5 PHA-GEN-002-2004 CHOLESTEROL REDUCING MEDICATIONS Five Main Categories 1. Statins 2. Fibrates 3. Resins 4. Niacin 5. Cholesterol absorption inhibitor Statins Also called HMG-CoA reductase inhibitors
Page 1 of 5 PHA-GEN-002-2004 CHOLESTEROL REDUCING MEDICATIONS Five Main Categories 1. Statins 2. Fibrates 3. Resins 4. Niacin 5. Cholesterol absorption inhibitor Statins Also called HMG-CoA reductase inhibitors
B. Patient has not reached the percentage reduction goal with statin therapy
 Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Dyslipidemia and the Use of Statins. Troy L Randle, DO, FACC, FACOI
 Dyslipidemia and the Use of Statins Troy L Randle, DO, FACC, FACOI Objective: Identify CV risk. Determine what dyslipidemia (dyslipoproteinemia) is Decrease CV risk and optimize lipid levels for your
Dyslipidemia and the Use of Statins Troy L Randle, DO, FACC, FACOI Objective: Identify CV risk. Determine what dyslipidemia (dyslipoproteinemia) is Decrease CV risk and optimize lipid levels for your
Pharmacology Challenges: Managing Statin Myalgia
 Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention Center: Rooms 315 & 316
 Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Ambulatory Care PRN Focus Session New Developments in Hypertension and Dyslipidemia Management Activity No. 0217-0000-11-101-L01-P (Application-Based Activity) Tuesday, October 18 3:30 p.m. 5:30 p.m. Convention
Doctor discussion guide:
 Bring this printout to your next doctor s appointment. It will help you and your doctor work together to set goals for treatment, evaluate the success of your treatment, and reduce your risk of side effects.
Bring this printout to your next doctor s appointment. It will help you and your doctor work together to set goals for treatment, evaluate the success of your treatment, and reduce your risk of side effects.
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
10/1/2008. Therapy? Disclosure Statement
 What s New in Lipid Therapy? Brooke Hudspeth, PharmD Diabetes Care Kroger Pharmacy Disclosure Statement In accordance with policies set forth by the Accreditation Council for Continuing Medical Education
What s New in Lipid Therapy? Brooke Hudspeth, PharmD Diabetes Care Kroger Pharmacy Disclosure Statement In accordance with policies set forth by the Accreditation Council for Continuing Medical Education
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Praluent. Praluent (alirocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.06 Subject: Praluent Page: 1 of 10 Last Review Date: September 20, 2018 Praluent Description Praluent
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.16.08 Subject: Repatha Page: 1 of 8 Last Review Date: September 18, 2015 Repatha Description Repatha
Nearly 62 million people in the. ... REPORTS... New Therapeutic Options in the National Cholesterol Education Program Adult Treatment Panel III
 ... REPORTS... New Therapeutic Options in the National Cholesterol Education Program Adult Treatment Panel III Robert L. Talbert, PharmD Abstract Coronary heart disease (CHD) is a common, costly, and undertreated
... REPORTS... New Therapeutic Options in the National Cholesterol Education Program Adult Treatment Panel III Robert L. Talbert, PharmD Abstract Coronary heart disease (CHD) is a common, costly, and undertreated
DYSLIPIDEMIA PHARMACOLOGY. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D
 DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
DYSLIPIDEMIA PHARMACOLOGY University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita Narciso Pharm D 1 LEARNING OBJECTIVES Know normal cholesterol levels Understand what the role
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Comprehensive Treatment for Dyslipidemias. Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium
 Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
Comprehensive Treatment for Dyslipidemias Eric L. Pacini, MD Oregon Cardiology 2012 Cardiovascular Symposium Primary Prevention 41 y/o healthy male No Medications Normal BP, Glucose and BMI Social History:
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Repatha. Repatha (evolocumab) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.40.08 Subject: Repatha Page: 1 of 8 Last Review Date: December 2, 2016 Repatha Description Repatha (evolocumab)
CARDIOVASCULAR DISEASE WHAT IS IT? WHAT IS THE ROLE OF CHOLESTEROL? HOW CAN WE REDUCE RISK?
 1 CARDIOVASCULAR DISEASE WHAT IS IT? WHAT IS THE ROLE OF CHOLESTEROL? HOW CAN WE REDUCE RISK? Perry J Weinstock, MD, F.A.C.C. Head, Division of Cardiovascular Disease Director of Clinical Cardiology Cooper
1 CARDIOVASCULAR DISEASE WHAT IS IT? WHAT IS THE ROLE OF CHOLESTEROL? HOW CAN WE REDUCE RISK? Perry J Weinstock, MD, F.A.C.C. Head, Division of Cardiovascular Disease Director of Clinical Cardiology Cooper
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
In the Know: Canadian Guidelines for Dyslipidemia, 2003
 In the Know: Canadian Guidelines for Dyslipidemia, 2003 In his reviews of Canadian dyslipidemia guidelines, Dr. Curnew explores the impact of major trials, the assessment and categories of risk, and both
In the Know: Canadian Guidelines for Dyslipidemia, 2003 In his reviews of Canadian dyslipidemia guidelines, Dr. Curnew explores the impact of major trials, the assessment and categories of risk, and both
Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane
 Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane Kostner, 2007 2008 LDL Target depends on your level of Risk Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)
Novel HDL Targeted Therapies: The Search Continues Assoc. Prof. K.Kostner,, Univ. of Qld, Brisbane Kostner, 2007 2008 LDL Target depends on your level of Risk Acute Plaque Rupture ACS (UA/NSTEMI/STEMI)
hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER
 Management of hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER Background on Dyslipidemia in CKD In advanced chronic kidney disease (CKD),
Management of hyperlipidemia in CKD DR MOJGAN MORTAZAVI ASSOCIATE PROFESSOR OF NEPHROLOGY ISFAHAN KIDNEY DISEASES RESEARCH CENTER Background on Dyslipidemia in CKD In advanced chronic kidney disease (CKD),
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Novel Therapeutic Strategies in Lipid Management: Lowering LDL C to Improve Patient Outcomes
 Novel Therapeutic Strategies in Lipid Management: Lowering LDL C to Improve Patient Outcomes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology University of Pennsylvania April 25,
Novel Therapeutic Strategies in Lipid Management: Lowering LDL C to Improve Patient Outcomes Rajat Deo, MD, MTR Assistant Professor of Medicine Division of Cardiology University of Pennsylvania April 25,
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
7 KEYS. to Reduce Cholesterol. By Simeon Margolis, M.D., PH.D. & Roger S. Blumenthal, M.D. and the Editors of Johns Hopkins Health Alerts
 7 KEYS to Reduce Cholesterol By Simeon Margolis, M.D., PH.D. & Roger S. Blumenthal, M.D. and the Editors of Johns Hopkins Health Alerts 7 KEYS 7 Keys to Reduce Cholesterol As many Americans are now aware,
7 KEYS to Reduce Cholesterol By Simeon Margolis, M.D., PH.D. & Roger S. Blumenthal, M.D. and the Editors of Johns Hopkins Health Alerts 7 KEYS 7 Keys to Reduce Cholesterol As many Americans are now aware,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: (Vytorin) Reference Number: CP.PMN.77 Effective Date: 02.01.17 Last Review Date: 02.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Clinical Policy: (Vytorin) Reference Number: CP.PMN.77 Effective Date: 02.01.17 Last Review Date: 02.18 Line of Business: Commercial, Medicaid Revision Log See Important Reminder at the end of this policy
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Hae Sun Suh, B.Pharm., Ph.D. Jason N. Doctor, Ph.D.
 Podium Presentation, May 18, 2009 Comparison of Cardiovascular Event Rates in Subjects with Type II Diabetes Mellitus who Augmented from Statin Monotherapy to Statin Plus Fibrate Combination Therapy with
Podium Presentation, May 18, 2009 Comparison of Cardiovascular Event Rates in Subjects with Type II Diabetes Mellitus who Augmented from Statin Monotherapy to Statin Plus Fibrate Combination Therapy with
Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE)
") Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE) Thomas Dayspring, MD, FACP Clinical Assistant Professor of Medicine University of Medicine and Dentistry
Ezetimibe and SimvastatiN in Hypercholesterolemia EnhANces AtherosClerosis REgression (ENHANCE) Thomas Dayspring, MD, FACP Clinical Assistant Professor of Medicine University of Medicine and Dentistry
Statin Intolerance. Jason Evanchan DO, FACC April 20 th, 2018
 Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Statin Intolerance 2 nd Annual CV Course for Trainees and Early Career Physicians: Current Concepts in the Diagnosis and Management of Coronary Artery Disease Jason Evanchan DO, FACC April 20 th, 2018
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Dyslipidemia and HIV NORTHWEST AIDS EDUCATION AND TRAINING CENTER
 NORTHWEST AIDS EDUCATION AND TRAINING CENTER Dyslipidemia and HIV Heidi Crane, MD, MPH Madison Metabolic Clinic Associate Professor UW Department of Medicine Presentation prepared by: Heidi Crane, MD,
NORTHWEST AIDS EDUCATION AND TRAINING CENTER Dyslipidemia and HIV Heidi Crane, MD, MPH Madison Metabolic Clinic Associate Professor UW Department of Medicine Presentation prepared by: Heidi Crane, MD,
... CPE/CNE QUIZ... CPE/CNE QUESTIONS
 CPE/CNE QUESTIONS Continuing Pharmacy Education Accreditation The Virginia Council on Pharmaceutical Education is approved by the American Council on Pharmaceutical Education as a provider of continuing
CPE/CNE QUESTIONS Continuing Pharmacy Education Accreditation The Virginia Council on Pharmaceutical Education is approved by the American Council on Pharmaceutical Education as a provider of continuing
Dyslipidemia Management - Summary. Adults at any age with the following risk factors should be screened for lipids at any age:
 Dyslipidemia Management - Summary How do I assess Dyslipidemia? Screening of plasma lipids is recommended in adult men 40 and women that are 50 years of age or who are postmenopausal. Adults at any age
Dyslipidemia Management - Summary How do I assess Dyslipidemia? Screening of plasma lipids is recommended in adult men 40 and women that are 50 years of age or who are postmenopausal. Adults at any age
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID?
 Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
See Important Reminder at the end of this policy for important regulatory and legal information.
 Clinical Policy: Reference Number: CP.HNMC.05 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy for important
Clinical Policy: Reference Number: CP.HNMC.05 Effective Date: 11.16.16 Last Review Date: 11.17 Line of Business: Medicaid Medi-Cal Revision Log See Important Reminder at the end of this policy for important
Imbalances in lipid components
 Drugs for Dyslipidemia Vivien Gam, Pharm.D. 1 Dyslipidemia Imbalances in lipid components High total cholesterol High LDL cholesterol Low HDL cholesterol High triglycerides Significant risk factor for
Drugs for Dyslipidemia Vivien Gam, Pharm.D. 1 Dyslipidemia Imbalances in lipid components High total cholesterol High LDL cholesterol Low HDL cholesterol High triglycerides Significant risk factor for
Clinical Practice Guideline
 Clinical Practice Guideline Secondary Prevention for Patients with Coronary and Other Vascular Disease Since the 2001 update of the American Heart Association (AHA)/American College of Cardiology (ACC)
Clinical Practice Guideline Secondary Prevention for Patients with Coronary and Other Vascular Disease Since the 2001 update of the American Heart Association (AHA)/American College of Cardiology (ACC)
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Disclosures. Pediatric Dyslipidemia Casey Elkins, DNP, NP C, CLS, FNLA. Learning Objectives. Atherogenesis. Acceptable Values
 39 th National Conference on Pediatric Health Care Pediatric Dyslipidemia Casey Elkins, DNP, NP C, CLS, FNLA March 19-22, 2018 CHICAGO Disclosures Speakers Bureau Sanofi and Regeneron Learning Objectives
39 th National Conference on Pediatric Health Care Pediatric Dyslipidemia Casey Elkins, DNP, NP C, CLS, FNLA March 19-22, 2018 CHICAGO Disclosures Speakers Bureau Sanofi and Regeneron Learning Objectives
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes
 Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Cardiovascular Risk Reduction and Other Co-Morbidities in Type 2 Diabetes Following this presentation, you will be able to: Describe the relationship between major CV risk factors and CVD outcomes Select
Learning Objectives. Cholesterol and Lipids in Kids: It s a Matter of the Heart. Is Atherosclerosis a Pediatric Disease?
 Scott J. Soifer, MD Professor and Vice Chair Department of Pediatrics University of California, San Francisco UCSF Benioff Children s Hospital Cholesterol and Lipids in Kids: It s a Matter of the Heart
Scott J. Soifer, MD Professor and Vice Chair Department of Pediatrics University of California, San Francisco UCSF Benioff Children s Hospital Cholesterol and Lipids in Kids: It s a Matter of the Heart
Diseases & Conditions
 http://my.clevelandclinic.org Diseases & Conditions About Cholesterol-Lowering Drugs Some people have a genetic predisposition to high blood cholesterol levels. These people may need drug therapy in addition
http://my.clevelandclinic.org Diseases & Conditions About Cholesterol-Lowering Drugs Some people have a genetic predisposition to high blood cholesterol levels. These people may need drug therapy in addition