Objec ves To discuss the process of formulation of guidelines and how this may differ among professional societies 5/14/15
|
|
|
- Jeffrey Martin
- 6 years ago
- Views:
Transcription

1 Kellie McLain, NP- C, CLS Medical University of South Carolina Cardiology Division Seinsheimer Cardiovascular Prevention and Lipid Program May 29 th, 2015 Objecves To discuss the process of formulation of guidelines and how this may differ among professional societies To provide an overview of the development, recommendations, confusions and controversies concerning the new 2013 ACC/AHA Treatment of Blood Cholesterol Guideline for ASCVD Prevention To discuss difficult lipid management case studies using current recommendations and novel lipid lowering medications. 1

2 A Year of Controversy in Guideline Development 2013 ACC/AHA Cholesterol Guidelines 2013 ACC/AHA ASCVD Risk Assessment Algorithm not JNC 8 Panel BP Guidelines Guidelines for the Management of LDL- related ASCVD Risk Significant etiologic role of low density lipoprotein in the pathogenesis of atherosclerotic cardiovascular disease Plethora of guidelines with sometimes discordant or overlapping recommendations can lead to confusion among providers, media, patients General population Special populations 2
:196-206. doi:10.1016/j.jacc.2014.05.")
3 Comparison of Clinical Guidelines for the Management of Risks Related to LDL in ASCVD J Am Coll Cardiol. 2014;64(2): doi: /j.jacc A Change in Strategy 3
4 2013: ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atheroscleroc Cardiovascular Risk in Adults Content/Scope: Addresses only a limited number of clinical questions (3) and does not provide comprehensive recommendations for management of dyslipidemias What is the evidence for LDL- C and non- HDL- C goals for secondary prevention of ASCVD? (19 RCTs) What is the evidence for LDL- C and non- HDL- C goals for primary prevention of ASCVD? (6 RCTs) What is the impact on lipid levels, effectiveness, and safety of specific lipid- lowering drugs in general and in selected subgroups? Succinct summary of evidence for each recommendation DOI: /01.cir a Crical Queson 1: Secondary Prevenon Publicaons screened 4D (diabetics, atorva 20 mg v. placebo: hemodialysis pts, n=1255) *A- Z (ACS, early v. delayed, simva 40 to 80 mg v. placebo to simva 20 mg, n=2265) ACCORD (diabetics, fenofibrate v. placebo on background simva mg, n=5518) ALLIANCE (CHD, usual care v. atorva 80 mg, n=2442) ASPEN (2006, T2DM+CAD baseline LDL- C 114 mg/dl, atorva 10 mg v. placebo, n=2410) AURORA (hemodialysis, rosuva 10 mg v. placebo, n=2776) CARE (MI, prava 40 mg v. placebo, n=4159) CORONA (Class II- IV ischemic syshf age >60 yrs, rosuva 10 mg v. placebo, n=5011) *GREACE (Greece CHD, usual care v. atorva titrated to LDL- C < 100 mg/dl, n=1600) HATS (CHD, simva+niacin v. placebo, n=160) HPS (UK CVD or DM, simva 40 mg v. placebo, n=20,536) IDEAL (MI, atorva 80 mg v. simva 20 mg, n=8888) LIPID (ACS, prava 40 mg v. placebo, n=9014) LIPS (s/p PCI, fluva 80 mg v. placebo, n=1677) MIRACL (ACS, atorva 80 mg v. placebo, n=3086) MUSHASHI- AMI (Japan, acute MI, any statin v. no statin, n=486) PROVE- IT (ACD, atorva 80 mg v. prava 40 mg, n=4132) SPARCL (CVA or TIA, atorva 80 mg v. placebo, n=4731) TNT (CHD, LDL<130 mg/dl, atorva 80 mg v. atorva 10 mg, n=10,001) 4
5 Crical Queson 2: Primary Prevenon Publicaons screened Publications Screened 1958 Included 20 Excluded 1938 Final total for review of CQ2: 6 RCTs Good quality 7 Fair quality 12 Poor quality 1 Total ABSTRACTED 19 Crical Queson 2: Primary Prevenon Publicaons screened AFCAPS/TexCAPS (pts. with average LDL- C levels 150 mg/dl, lova mg v. placebo, n=6605) ASPEN (diabetics, atorva 10 mg v. placebo, n=2410) AURORA (hemodialysis, rosuva 10 mg v. placebo, n=2776) CARDS (T2DM LDL- C 160 mg/dl, atorva 10 mg v. placebo, n=2838) JUPITER (hs- CRP >2 mg/dl, LDL- C <130 mg/dl, rosuva 20 mg v. placebo, n=17,802) MEGA (Japan LDL- C 157 mg/dl, prava mg v. diet alone, n=7832) 5
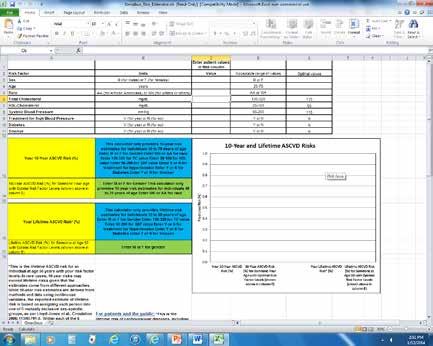
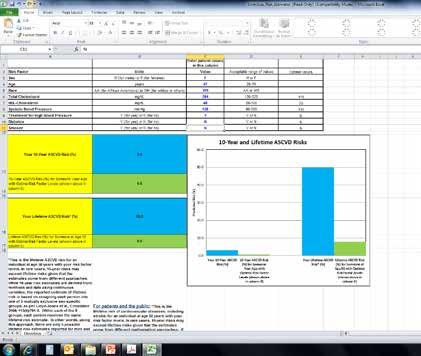
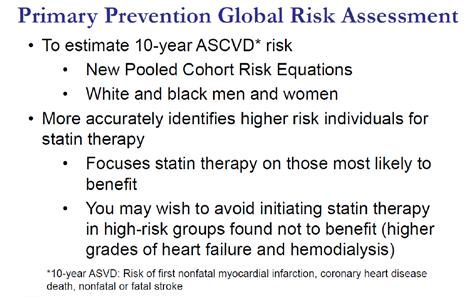
6 Crical Queson 3: Efficacy and Safety Publicaons screened Publications Screened 2911 Included 59 Excluded 2852 Good quality 10 Fair quality 25 Poor quality 24 Total ABSTRACTED 35 Meta-analyses used for statin efficacy and safety included data from additional studies. 2013: ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atheroscleroc Cardiovascular Risk in Adults New GLOBAL risk assessment tool: CV Risk Calculator based on the Pooled Cohort Equations Derived from large, diverse, community- based cohorts that are generally representative of US population of whites and AA (ARIC, CHS, CARDIA, Framingham original and FOS) 10- year risk of first hard ASCVD event (nonfatal MI, CHD death, fatal or nonfatal stroke) DOI: /01.cir a DOI: / 01.cir

7 DOI: /01.cir a DOI: / 01.cir DOI: /01.cir a DOI: / 01.cir

8 DOI: /01.cir a DOI: / 01.cir DOI: /01.cir a DOI: / 01.cir
9 2013: ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atheroscleroc Cardiovascular Risk in Adults Provides race- and sex- specific estimates of 10- year risk Should be used in non- Hispanic whites and non- Hispanic African Americans between the ages of years of age Also provides lifetime risk for persons yr who are not at high short- term risk Recommended optional RF or screening tests: primary LDL- C >160 mg/dl, family history premature ASCVD, hs- CRP >2 mg/l, CAC >300 Agatston or >75 th percentile, ABI <0.9, elevated lifetime risk DOI: /01.cir a DOI: / 01.cir : ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atheroscleroc Cardiovascular Risk in Adults Novel new approach to the management of LDL- related ASCVD risk No RCTs available in which ALL patients were titrated to a specific LDL- C goal <70 or <100 mg/dl in primary or secondary prevention Determined that data are inadequate to identify specific lipoprotein targets of therapy Panel makes no recommendation for or against LDL- C or non- HDL- C targets for primary or secondary ASCVD prevention DOI: /01.cir a DOI: / 01.cir
 Individuals with clinical ASCVD 2) Individuals with primary elevations of LDL- C >190 mg/dl 3) Individuals 4-75 yrs.")
10 2013: ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atheroscleroc Cardiovascular Risk in Adults Identified four groups of patients with most extensive evidence of benefit of statin therapy for ASCVD prevention 1) Individuals with clinical ASCVD 2) Individuals with primary elevations of LDL- C >190 mg/dl 3) Individuals 4-75 yrs. of age with diabetes and LDL- C mg/dl 4) Individuals without ASCVD or diabetes, yrs. of age, with LDL- C mg/dl and an estimated 10- year ASCVD risk of >7.5% by the Pooled Risk Equations DOI: /01.cir a DOI: / 01.cir
11 2013: ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atheroscleroc Cardiovascular Risk in Adults For each risk group an intensity of statin therapy is specified: moderate- or high- intensity Low- intensity statins are recommended only in patients with history of/at risk for adverse drug effects Quantitative comparison of statin risks and benefits Did not find evidence to support targets of therapy No dose titration recommended Monitoring of LDL- C to assess compliance and response to therapy DOI: /01.cir a DOI: / 01.cir : ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atheroscleroc Cardiovascular Risk in Adults Non- statin therapies did not provide ASCVD risk reduction benefits or safety profiles comparable to statin therapy (IMPROVE- IT) Insufficient evidence to make recommendations in Class II- IV heart failure or hemodialysis DOI: /01.cir a DOI: / 01.cir
 mg Rosuvastatin (5**) 10* mg Simvastatin 20*- 40* mg")
12 High-, moderate, and low- intensity stan therapy used in clinical trials High- intensity statin Moderate- intensity therapy statin therapy Daily dose lowers LDL- C on average, by approximately >50% Atorvastatin 40*- 80* mg Rosuvastatin 20*- 40** mg Daily dose lowers LDL- C on average, by approximately 30 to <50% Atorvastatin 10* (20**) mg Rosuvastatin (5**) 10* mg Simvastatin 20*- 40* mg Pravastatin 40* (80**) mg Lovastatin 40* mg Fluvastatin XL 80** mg Fluvastatin 40 mg BID* Pitavastatin 2-4** mg *Statins demonstrated reduction in major CVD events **FDA approved doses not tested in clinical trials Low- intensity statin therapy Daily dose lowers LDL- C on average by approximately <30% Simvastatin 10** mg Pravastatin 10*- 20* mg Lovastatin 20* mg Fluvastatin 20**- 40** mg Pitavastatin 1** mg DOI: /01.cir a DOI: / 01.cir
13 13
14 Monitoring Stan Therapy Initial fasting lipid panel Second panel 4-12 weeks later to determine adherence to therapy Every 3-12 months as clinically indicated Monitoring Stan Therapy Insufficient response to statin therapy Reinforce medication adherence Reinforce adherence to intensive lifestyle changes Exclude secondary causes of hyperlipidemia 14
15 Monitoring Stan Therapy Insufficient response to statin therapy Reinforce medication adherence Reinforce adherence to intense lifestyle changes Exclude secondary causes to dyslipidemia Secondary Causes of Dyslipidemia Secondary Causes- (most common) Diet Drugs Diseases Disorders and altered states of metabolism Elevated LDL- C Saturated or trans fat, weight gain or anorexia Diuretics, cyclosporine, glucocorticoids, amiodarone Biliary obstruction, nephrotic syndrome Hypothyroid, obesity, pregnancy Elevated TG Weight gain, very low- fat diets, high refined carbs, excess ETOH Oral estrogens, glucocorticoids, BAS, protease inhibitors, anabolic steroids, sirolimus, raloxifene, tamoxifen, thiazides, BB(not carvedilol) Nephrotic syndrome, Chronic renal failure, lipodystrophies Diabetes(PC), hypothyroid, obesity, pregnancy 15
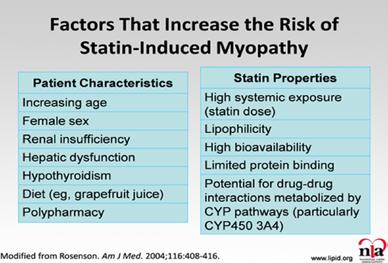
16 Monitoring Stan Therapy Higher risk individuals with suboptimal response May consider addition of non- statin therapy if potential risk- reduction benefits outweigh potential adverse effects Preference should be given to drugs shown to reduce ASCVD events in RCTs Statin- intolerant patients May consider addition of non- statin therapy if potential risk- reduction benefits outweigh potential adverse effects Preference should be given to drugs shown to reduce ASCVD events in RCT Stan Safety Recommendaons Consider reduction of statin intensity Multiple comorbidities, impaired renal or hepatic function Previous statin adverse effects, muscle disorders, Unexplained ALT >3 times ULN Concomitant use of drugs affecting statin metabolism >75 yrs of age History of hemorrhagic stroke Asian ancestry 16
17 Stan Safety Recommendaons Do not routinely measure CK Reasonable to measure CK at baseline if individual at increased risk for muscle events or on therapy with muscle symptoms Measure ALT prior to initiation of statin therapy Reasonable to measure LFTs if symptoms of hepatotoxicity May consider decreasing statin dose if 2 consecutive LDL- C <40 mg/dl Do not use simvastatin 80 mg Monitor for new onset diabetes per ADA guidelines Obtain baseline history of current or previous history of muscle symptoms Change, Controversy, Confusion, Concern, Chaos? What is similar? LDL- C remains the lipoprotein of interest Very high- risk patients with FH and/or LDL- C >190 mg/dl are candidates for high- intensity statin therapy In FH combination therapy may be considered (ezetimibe, BAS, niacin, lomitapide, mipomersen, LDL apheresis) Diabetics are a high- risk group: however, intensity of therapy is now based on 10- year risk of hard ASCVD by the Pooled Risk Equations Monitoring of LDL- C, but for adherence rather than goal of therapy 17
18 Change, Controversy, Confusion, Concern, Chaos? What is different? Limited scope of current guideline 3 critical questions Fire and forget vs treat to target, lowest is best, treat level of ASCVD risk, lifetime risk Abandonment of LDL- C and non- HDL- C goals Limited monitoring of LDL- C Limited guidance <40 or >75 yrs. of age Treatment in special populations Limited discussion of management of complex patients New Pooled Risk Equations/CV Risk Calculator work in progress to validate in other populations with varying levels of risk DOI: /01.cir a DOI: / 01.cir Misconcepons What is the meaning of the panel s determination that there is inadequate evidence that lowering of LDL- C to a specific target lowers ASCVD risk? LDL- C is not important Lipid therapy is not beneficial LDL- C is not relevant in ASCVD It s all about statins, not LDL- C Reluctance to initiate therapy, discontinuation of statins DOI: /01.cir a DOI: / 01.cir
19 Misconcepons With primary focus on statins, patients with more complex dyslipidemias, statin intolerance, FH may discontinue combination regimens. Physicians reluctant to prescribe non- statin therapies in appropriate patients. Challenges Large patient population who are possible candidates for statin therapy (non- diabetics, no clinical ASCVD) require calculation of ASCVD risk by the new Pooled Risk Equations. Will providers incorporate this into busy daily practice? 19

20 ACC/AHA and collaborating societies will begin updating these guidelines in 2014 Key Points 20
 Case Study: Statin intolerant Alternate therapy, weekly dosing, non- statin therapy")
21 Key Points (cont.) Case Study: Statin intolerant Alternate therapy, weekly dosing, non- statin therapy Primary prevention Alternate risk evaluation Secondary Prevention LDL- P 21
22 Stan Intolerant: 22


23 Lipo/hydrophilicity lipophilicity Log P Simvastatin Lovastatin Atorvastatin Fluvastatin Pitavastatin hydrophilicity Pravastatin Rosuvastatin 23
, rosuvastatin, pravachol, lovastatin, fluvastatin all with myalgias.")
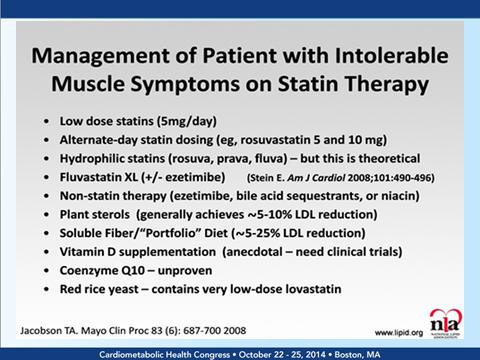
24 1. Case Study: SI RW 63 yo AAM with CAD, s/p CABG, AFIB, Kidney TX, DM, PVD, Htn, OSA on cpap presented on gemfibrozil 600mg bid. TG 578, HDL 25 Previous zocor 80mg/myalgias- termed Statin Intolerant - Gemfibrozil, RD, 4g O3 Tried atorvastatin(daily/weekly), rosuvastatin, pravachol, lovastatin, fluvastatin all with myalgias. Vit D low- replaced. Pitavastatin What would be next option? 1. Case Study: SI Rosuvastatin 5mg 3x week, vit D replaced/supplement Kidney and liver- nl or slightly elevated transaminases Last visit 3-15 TC 131, HDL 40, LDL 75, TG 78 Lipophilic statins easily penetrate muscle cells, hydrophilic statins penetrate at a lesser extent. 24

25 2. Case Study: Primary Prevenon MS 48 yo WM with HTN, asthma referred by wife(rn) for high cholesterol. Highest LDL 158, TG 285. No DM, thyroid, kidney/liver. FH premature CAD in father at 51 with MI and 2V CABG, deceased at 55 MI. 11 Siblings. BP well controlled. Past intolerance to pravastatin, on simva 10mg, no complaints. Losartan 50mg. Labs 6/13 LDL 135, HDL 37, TG245, TC 221, FG 119, liver nl What next? 25

26 2. Case Study: PP Obtained calcium score Total calcium score of 150, which is at the 97th percentile for age and race matched controls. This means that 97% of people of this age, race, and gender have less calcium than was detected in this CT scan What would be next step? 2. Case Study: PP Started on atorvastatin 20. Developed myalgias. Initiated rosuvastatin 10mg- tolerating well. Started couch to 5K. RD. FU 3 mo. Most recent labs: LDL 65, HDL 44, TG 123, TC 134, AST/ALT nl, FG 97 Continues to tolerate rosuvastatin 10mg. 26

27 3. Case Study: Secondary Prevenon SC 69 yo WM with CAD, s/p mult PCI s, dyslipidemia. Rf by cardiologist for lipid optimization/low HDL Initial labs TC 140, HDL 39, LDL 73, TG 140, on atorvastatin 80mg, ASA 81, toprol xl 50,multi vit. What would be your next step? 3. Case Study: Secondary Prevenon Discuss exercise (rehab), eating habits- refer to RD, low HDL- C, routine lipids ok Check LDL- P number(ideal high risk <700) LDL- P 1929, HDL- P 29.1?? 27
28 3. Case Study: Secondary Prevenon *Options* lifestyle He was started on ezetimibe 10mg and encouraged to change diet (LC) and keep up exercising. FU 3-4 months. Fasting labs at FU LDL- C 55, HDL 42, TG158, TC130 LDL- P 1489 HDL- P tolerating meds without myalgias. No diet or exercise change. Next? 3. Case Study: Secondary Prevenon FU 4 months after met with exercise physiologist and signed up for cardiac gym membership. Decided to change eating habits. Lost 8 lbs LDL- P 984! HDL- P 32.7 LDL- c 52, HDL 45, TG 110, TC 119 Continues with exercise efforts and lower carb eating. 28

29 Quesons? 29
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Major recommendations for statin therapy for ASCVD prevention
 2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
2013 A/AHA Guidelines holesterol Rx to Reduce ASVD Risk in Adults Major recommendations for statin therapy for ASVD prevention *% in LDL can be used as indication of response & adherence to Rx but is not
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines
 Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
Update on Cholesterol Management: The 2013 ACC/AHA Guidelines Ola Akinboboye MD MPH MBA Medical Director, Queens Heart institute Rosedale. Associate Professor of Clinical Medicine, Weill Medical College
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Vincent J. Caracciolo, MD FACC FOMA May 2014
 Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Sanger Heart & Vascular Institute Symposium 2015
 Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Sanger Heart & Vascular Institute Symposium 2015 Cardiovascular Update For Primary Care Physicians William E. Downey, MD FACC FSCAI Medical Director, Interventional Cardiology Sanger Heart & Vascular Institute
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Conflicts of interest. What's the Skinny on the Lipid Guidelines? Key Differences. Are you applying the new ACC/AHA Lipid guidelines in your practice?
 Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Conflicts of interest What's the Skinny on the Lipid Guidelines? The presenter has no relevant conflicts of interest to disclose. Kathleen Vest, PharmD, CDE, BCACP At the end of this presentation, pharmacist
Acute Coronary Syndromes (ACS)
") Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Sally A. Arif, Pharm.D., BCPS (AQ Cardiology) Assistant Professor of Pharmacy Practice Midwestern University, Chicago College of Pharmacy Cardiology Clinical Specialist, Rush University Medical Center
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
Assessment and Primary Prevention of CAD. Tuan D. Nguyen, M.D. Non-Invasive Cardiology Seton Heart Institute
 Assessment and Primary Prevention of CAD Tuan D. Nguyen, M.D. Non-Invasive Cardiology Seton Heart Institute Objectives Identify risk factors for CV disease Identify populations that likely benefit from
Assessment and Primary Prevention of CAD Tuan D. Nguyen, M.D. Non-Invasive Cardiology Seton Heart Institute Objectives Identify risk factors for CV disease Identify populations that likely benefit from
9/3/ AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis. Disclosure
 2013 AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis Robert Gleeson MD Preven5ve Cardiology and Lipid Management Froedtert and The Medical College of Wisconsin Disclosure
2013 AHA/ACC Lipid Guidelines on the Treatment of Cholesterol to Reduce Atherosclerosis Robert Gleeson MD Preven5ve Cardiology and Lipid Management Froedtert and The Medical College of Wisconsin Disclosure
PREV E E V N E TI T O I N
 PREVENTION OF ATHEROSCLEROTIC CARDIOVASCULAR DISEASE SHANE JOHNSON,, PHARM. D. OBJECTIVES 1. Define atherosclerotic cardiovascular disease(s) and describe the disease progression. 2. Identify three independent
PREVENTION OF ATHEROSCLEROTIC CARDIOVASCULAR DISEASE SHANE JOHNSON,, PHARM. D. OBJECTIVES 1. Define atherosclerotic cardiovascular disease(s) and describe the disease progression. 2. Identify three independent
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Implementation of CV Risk and. Dyslipidemia Guidelines. Impact on Americans 11/25/2014. Summary Implementing new. Dyslipidemia Guidelines
 Summary Implementing new Dyslipidemia Guidelines Implementation of CV Risk and Dyslipidemia Guidelines Ronald D. Scott, MD Regional KPSC CVD Co-Lead Family Medicine and Lipidology, WLA ASCVD (Atherosclerotic
Summary Implementing new Dyslipidemia Guidelines Implementation of CV Risk and Dyslipidemia Guidelines Ronald D. Scott, MD Regional KPSC CVD Co-Lead Family Medicine and Lipidology, WLA ASCVD (Atherosclerotic
Disclosure. A New Partnership. Objectives 03/27/2014. What is the main way you have obtained information about the 2013 ACC/AHA Cholesterol Guideline?
 Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies
 A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
A New Age of Dyslipidemia Treatment: Role of Non- Statin Therapies BRODY MAACK, PHARMD, BCACP, CTTS Objectives 1. Review current guidelines regarding use of statin medications in the treatment and prevention
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
LAMIS (Livalo in AMI Study)
") JCR 2018. 12. 8 LAMIS (Livalo in AMI Study) Young Joon Hong Division of Cardiology, Chonnam National University Hospital Gwangju, Korea Trend of hypercholesterolemia in Korea < Prevalence of hypercholesterolemia
JCR 2018. 12. 8 LAMIS (Livalo in AMI Study) Young Joon Hong Division of Cardiology, Chonnam National University Hospital Gwangju, Korea Trend of hypercholesterolemia in Korea < Prevalence of hypercholesterolemia
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Assessing atherosclerotic risk for long term preventive treatment
 Assessing atherosclerotic risk for long term preventive treatment Donald A. Smith, MD, MPH Endocrinologist, Clinical Lipidologist Associate Professor of Medicine and Preventive Medicine Icahn School of
Assessing atherosclerotic risk for long term preventive treatment Donald A. Smith, MD, MPH Endocrinologist, Clinical Lipidologist Associate Professor of Medicine and Preventive Medicine Icahn School of
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
NEW GUIDELINES FOR CHOLESTEROL
 NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
NEW GUIDELINES FOR CHOLESTEROL NEW CHOLESTEROL GUIDELINES 2013 Recently updated guidelines for the treatment of high blood cholesterol levels is a major update since 2002. The news media have trumpeted
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Long-Term Complications of Diabetes Mellitus Macrovascular Complication
 Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
Long-Term Complications of Diabetes Mellitus Macrovascular Complication Sung Hee Choi MD, PhD Professor, Seoul National University College of Medicine, SNUBH, Bundang Hospital Diabetes = CVD equivalent
2013 Cholesterol Guidelines: Clarity and Controversy
 2013 Cholesterol Guidelines: Clarity and Controversy Sco9 J Deron DO, FACC Diplomate American Board Clinical Lipidology 2013 Cholesterol Guidelines: Background ATP III last updated 2004 2008 NHLBI started
2013 Cholesterol Guidelines: Clarity and Controversy Sco9 J Deron DO, FACC Diplomate American Board Clinical Lipidology 2013 Cholesterol Guidelines: Background ATP III last updated 2004 2008 NHLBI started
Targeting Lipids Strategies for Patients with Cardiometabolic Risk
 Targeting Lipids Strategies for Patients with Cardiometabolic Risk Faculty Disclosure David G. Carmouche, MD Director, Center for Cardiovascular Disease Prevention Baton Rouge Clinic ASH Specialist in
Targeting Lipids Strategies for Patients with Cardiometabolic Risk Faculty Disclosure David G. Carmouche, MD Director, Center for Cardiovascular Disease Prevention Baton Rouge Clinic ASH Specialist in
Update on the Treatment of Hyperlipidemia
 Update on the Treatment of Hyperlipidemia Wafaa Abou-Zeineddine, PharmD Medstar Washington Hospital Center Washington Metropolitan Society of Health Systems Pharmacists May 30, 2015 Please MUTE phones
Update on the Treatment of Hyperlipidemia Wafaa Abou-Zeineddine, PharmD Medstar Washington Hospital Center Washington Metropolitan Society of Health Systems Pharmacists May 30, 2015 Please MUTE phones
9/18/2017 DISCLOSURES. Consultant: RubiconMD. Research: Amgen, NHLBI OUTLINE OBJECTIVES. Review current CV risk assessment tools.
 UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018
 Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
Diabetes: Use of Adjunctive Therapy ACEs, ARBs, ASA & STATINs --Oh My! Veronica J. Brady, PhD, FNP-BC, BC-ADM, CDE Project ECHO April 19, 2018 Points to Ponder ASCVD is the leading cause of morbidity
10/4/2016. Similarities between the ACC/AHA Guidelines and the NLA Recommendations
 Lipid Management CoxHealth Heart and Vascular Summit Oct 15, 2016 DISCLOSURES I have no potential conflicts of interest and nothing relevant to this lecture to disclose Learning Objectives Develop an evidence-based
Lipid Management CoxHealth Heart and Vascular Summit Oct 15, 2016 DISCLOSURES I have no potential conflicts of interest and nothing relevant to this lecture to disclose Learning Objectives Develop an evidence-based
Objectives. Having completed the learning activities, the participant will be able to: Dyslipidemia: The latest treatment recommendations
 Objectives Dyslipidemia: The latest treatment recommendations Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC President, Fitzgerald Health Education Associates, Inc. North Andover, MA
Objectives Dyslipidemia: The latest treatment recommendations Margaret A. Fitzgerald, DNP, FNP-BC, NP-C, FAANP, CSP, FAAN, DCC President, Fitzgerald Health Education Associates, Inc. North Andover, MA
Treatment of Cholesterol in 2018: Time to Level Up. Most Important Slide. Three Things Learned that Will be Applied
 Treatment of Cholesterol in 2018: Time to Level Up 1. Most Important Slide Three Things Learned that Will be Applied 2. 3. 2013 Top Ten Points 1. Expert committee. Evidence used. 2. Four groups identified
Treatment of Cholesterol in 2018: Time to Level Up 1. Most Important Slide Three Things Learned that Will be Applied 2. 3. 2013 Top Ten Points 1. Expert committee. Evidence used. 2. Four groups identified
LDL and the Benefits of Statin Therapy
 LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
Pharmacology Challenges: Managing Statin Myalgia
 Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Clinical Case: RM is a 50 year-old African American woman with a past medical history of type diabetes, dyslipidemia, hypertension and peripheral arterial disease. She had been prescribed simvastatin 80
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake?
 Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake? Brian G. Choi, MD, MBA, FACC Associate Professor of Medicine Co-Director, Advanced Cardiac Imaging November 14, 2014 Washington, DC Disclosures
Hypertension Guidelines: JNC- Late, JNC- 8, or JNC- Fake? Brian G. Choi, MD, MBA, FACC Associate Professor of Medicine Co-Director, Advanced Cardiac Imaging November 14, 2014 Washington, DC Disclosures
Clinical Policy: Lomitapide (Juxtapid) Reference Number: ERX.SPA.170 Effective Date:
 Reference Number: ERX.SPA.170 Effective Date:") Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Juxtapid) Reference Number: ERX.SPA.170 Effective Date: 01.11.17 Last Review Date: 11.17 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk
 Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
Case Studies The Role of Non-Statin Therapies for LDL-C Lowering in the Management of ASCVD Risk Kim K. Birtcher, PharmD, MS, AACC Clinical Professor University of Houston College of Pharmacy Houston,
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes
 When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
When Statins Aren t Enough: Appropriate Therapies for High-Risk Patients with Diabetes Kim K. Birtcher, MS, PharmD, AACC, FNLA, CLS, BCPS (AQ-Cardiology), CDE Clinical Professor University of Houston College
Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients
 Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients Joe Anderson, PharmD, PhC, BCPS James Nawarskas, PharmD, PhC, BCPS Gretchen Ray, PharmD, PhC, BCACP University of
Applying the Intricacies of the New Hypertension and Lipid Guidelines to Your Patients Joe Anderson, PharmD, PhC, BCPS James Nawarskas, PharmD, PhC, BCPS Gretchen Ray, PharmD, PhC, BCACP University of
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
Lipids: Translating Studies into Practice. WD04: Cortney Joneikis, MD, MS Bob Gleeson, MD Jeff Whittle, MD, MPH
 Lipids: Translating Studies into Practice WD04: Cortney Joneikis, MD, MS Bob Gleeson, MD Jeff Whittle, MD, MPH Discussants: Bob Gleeson, MD Assistant Professor of Medicine, General Internal Medicine Medical
Lipids: Translating Studies into Practice WD04: Cortney Joneikis, MD, MS Bob Gleeson, MD Jeff Whittle, MD, MPH Discussants: Bob Gleeson, MD Assistant Professor of Medicine, General Internal Medicine Medical
Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin
 and Fixed-dose Combination Products Containing a Statin") Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin Final Report Update 5 November 2009 This report reviews information about the comparative
Drug Class Review HMG-CoA Reductase Inhibitors (Statins) and Fixed-dose Combination Products Containing a Statin Final Report Update 5 November 2009 This report reviews information about the comparative
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Clinical Policy: Mipomersen (Kynamro) Reference Number: ERX.SPA.171 Effective Date:
 Reference Number: ERX.SPA.171 Effective Date:") Clinical Policy: (Kynamro) Reference Number: ERX.SPA.171 Effective Date: 01.11.17 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
Clinical Policy: (Kynamro) Reference Number: ERX.SPA.171 Effective Date: 01.11.17 Last Review Date: 08.18 Revision Log See Important Reminder at the end of this policy for important regulatory and legal
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
UPDATES IN LIPID MANAGEMENT
 UPDATES IN LIPID 2017 Cardiovascular Symposium MANAGEMENT SUDHA RAVILLA, MD, DIPLOMATE, ABCL MEDICAL DIRECTOR CLINICAL LIPIDOLOGY TMHPP METABOLIC HEALTH CENTER INTRODUCTION CVD is STILL the No. 1 cause
UPDATES IN LIPID 2017 Cardiovascular Symposium MANAGEMENT SUDHA RAVILLA, MD, DIPLOMATE, ABCL MEDICAL DIRECTOR CLINICAL LIPIDOLOGY TMHPP METABOLIC HEALTH CENTER INTRODUCTION CVD is STILL the No. 1 cause
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Lipid Guidelines Who, What, and How Low. Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute
 Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Lipid Guidelines Who, What, and How Low Anita Ralstin, MS, CNP Next Step Health Consultant, LLC New Mexico Heart Institute Disclosures! None Objectives! List factors used in screening for dyslipidemia
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
CPE Session 7. Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction
 CPE Session 7 Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction Saturday, April 25, 2015 ACPE UAN 0128-0000-15-027-L01-P 1.0
CPE Session 7 Update on Clinical Practice Guidelines and Best Evidence in the Management of Hyperlipidemia and Cardiovascular Risk Reduction Saturday, April 25, 2015 ACPE UAN 0128-0000-15-027-L01-P 1.0
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Dyslipedemia New Guidelines
 Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy
Dyslipedemia New Guidelines New ACC/AHA Prevention Guidelines on Blood Cholesterol November 12, 2013 Mohammed M Abd El Ghany Professor of Cardiology Cairo Universlty 1 1 0 Cholesterol Management Pharmacotherapy