THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY
|
|
|
- Joleen Jennings
- 6 years ago
- Views:
Transcription
1 THE ESC/EAS LIPID GUIDELINES IN THE ELDERLY Alberico L. Catapano
2 Alberico L. Catapano Potential Conflict Of Interest Prof. Catapano has received honoraria, lecture fees, or research grants from: Abbot, Aegerion, Amgen, AstraZeneca, Bayer, Eli Lilly, Genzyme, Ionis, Kowa, Mediolanum, Meda,Menarini, Merck, Pfizer, Recordati, Regeneron, Sanofi, SigmaTau.
3 LDL-C is a major causal factor for atherosclerotic CVD LDL-C: primary risk factor in CHD and causative for development of coronary atherosclerosis 6 Hypertension 1 Smoking, physical inactivity 1 Prior CV event/manifest atherosclerosis 3 Age, ethnicity, gender, family history/genetic variations 1 Lipid disorders 1 (LDL, HDL, TG ) Increased CV risk Metabolic syndrome 2 Type 2 diabetes 1 High CRP, 4 chronic kidney disease 5 Obesity 1
 Lancet")
4 LDL : a major modifiable cardiovascular risk factor Meta-analysis of 61 prospective studies in the general population (n = 892,237) Lancet 2007;370:
5 Proportional reduction in CHD risk (log scale) Genetic evidence supports LDL-C as a risk factor for CV events 54.5% reduction in CHD risk per 1mmol/L lower LDL-C 30% Genetically lower LDL-C PCSK9 46L rs % ABCG5/8 rs LDLR rs NPC1L1 LDL-C score HMGCR LDL-C score 10% HMGCR rs12916 PCSK9 rs NPC1L1 rs PCSK9 rs HMGCR LDL-C score NPC1L1 LDL-C score LDLR rs Combined NPC1L1 & HMGCR LDL-C score Absolute magnitude of lower LDL-C (mg/dl) Ference et al. J Am Coll Cardiol 2012;60: Ference et al. J Am Coll Cardiol 2015;65:
6 Proportional reduction in CHD risk (log scale) Clinical benefit of lower LDL is determined by absolute exposure to lower LDL 30% 54.5% reduction in CHD risk for each 1mmol/L (38mg/dL) lower LDL-C 20% 10% PCSK9 rs NPC1L1 rs ABCG5/8 rs HMGCR rs12916 LDLR rs PCSK9 rs NPC1L1 LDL-C score HMGCR LDL-C score HMGCR LDL-C score NPC1L1 LDL-C score Genetically lower LDL-C LDLR rs Combined NPC1L1 & HMGCR LDL-C score A to Z GISSI-P SEARCH PCSK9 46L rs Pharmacologically lower LDL-C IMPROVE-IT ALLHAT-LLT 17.2% reduction in CHD risk for each 1mmol/L (38mg/dL) lower LDL-C Lower LDL-C (mg/dl) Ference et al. J Am Coll Cardiol 2015;65:
7 Proportional Reduction in Event Rate (SE) Greater reductions in LDL-C levels are associated with greater reductions in CV event rates 50% 40% 30% 20% CTT-meta-analysis 10% 0% IMPROVE-IT Reduction in LDL-C (mg/dl) CTTC. Lancet 2005;366: CTTC. Lancet 2010;376: Cannon et al. N Engl J Med 2015;372:
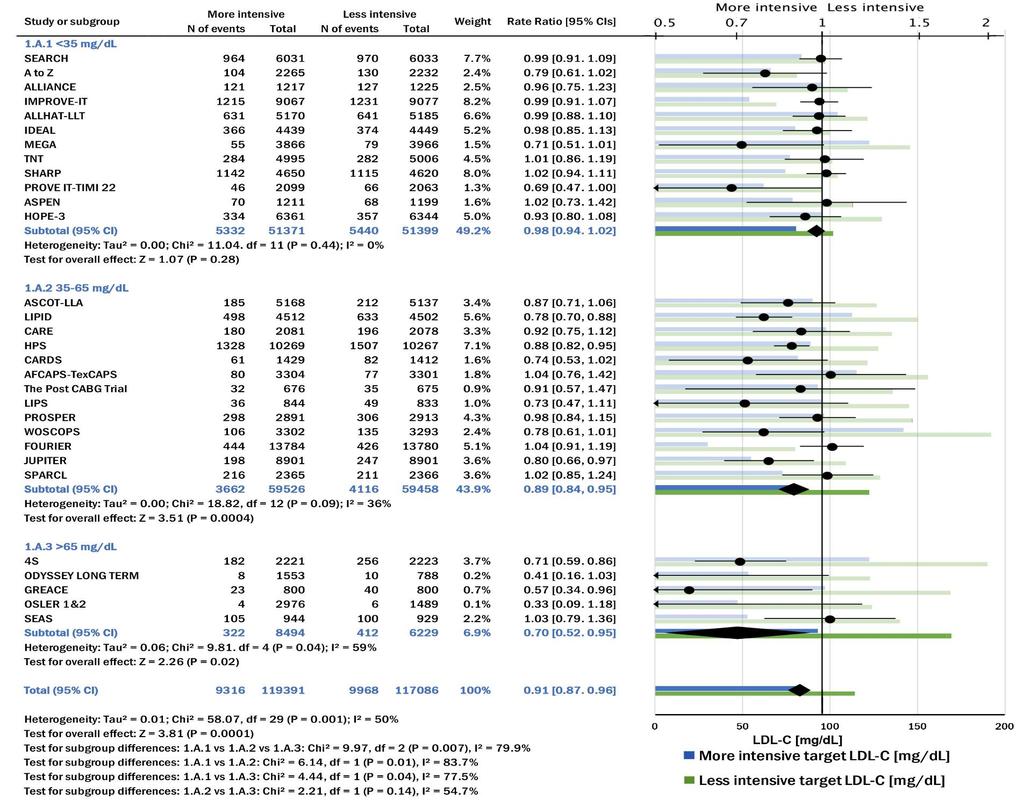
8 Weighted Between-Group Difference in Achieved Low- Density Lipoprotein Cholesterol (LDL-C) Level and Relative Risk for Major Vascular Events for Each Class of Intervention Silverman MG. et al. JAMA. 2016;316:
9 Scatterplot of absolute LDL-C reduction and major vascular event (MVE) relative risk for each trial Silverman MG. et al. JAMA. 2016;316: Supplementary Online Content
10 Effects of lowering LDL cholesterol with statin therapy on cause-specific mortality in metaanalyses of randomised trials of statin therapy Collins R. et al. Lancet 2016 Epub Sep 6
11 Similar proportional reductions in risks of major vascular events per mmol/l LDL cholesterol reduction in randomised trials of statin therapy among people with different presenting characteristics Collins R. et al. Lancet 2016 Epub Sep 6
12 Proportional reductions in risks of major vascular events per mmol/l reduction in LDL cholesterol during each year of scheduled statin treatment, in randomised trials of routine statin therapy versus no routine statin use Collins R. et al. Lancet 2016 Epub Sep 6

13 Predicted absolute reductions in risks of major vascular events (after the first year) by lowering LDL cholesterol with statin therapy for 5 years in people at different levels of absolute risk Collins R. et al. Lancet 2016 Epub Sep 6
14
15 ESC/EAS Guidelines for the management of dyslipidaemias The Task Force of the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR) Task Force Members: A L. Catapano* (Chairperson) (Italy), I Graham* (Chairperson) (Ireland), G De Backer (Belgium), O Wiklund (Sweden), M. J Chapman (France), H Drexel (Austria), A W. Hoes (The Netherlands), C S. Jennings (UK), U Landmesser (Germany), T R. Pedersen (Norway), Ž Reiner (Croatia), G Riccardi (Italy), M-R Taskinen (Finland), L Tokgozoglu (Turkey), W. M. M Verschuren (The Netherlands), Ch Vlachopoulos (Greece), D A. Wood (UK), J L Zamorano (Spain). Additional Contributor: M T Cooney (Ireland)
16 2016 ESC/EAS Guidelines for the management of dyslipidaemias 16 Table of content: -What is cardiovascular disease prevention? -Total cardiovascular risk -Evaluation of laboratory lipid and apolipoprotein parameters -Treatment targets -Lifestyle modifications to improve the plasma lipid profile -Drugs for treatment of hypercholesterolaemia -Drugs for treatment of hypertriglyceridaemia -Drugs affecting high-density lipoprotein-cholesterol -Management of dyslipidaemia in different clinical settings -Monitoring of lipids and enzymes in patients on lipid-lowering therapy -Strategies to encourage adoption of healthy lifestyle changes and adherence to lipid modifying therapies
17 Systolic blood pressure SCORE chart: 10-year risk fatal cardiovascular disease (CVD) in population at high CVD risk Women Men Non-smoker Smoker Age Non-smoker Smoker SCORE % and over 10%-14% 5%-9% 3%-4% 2% 1% <1% 10-year risk of fatal CVD in populations at High CVD risk Cholesterol (mmol/l) mg/dl
18 Systolic blood pressure 18 The risk age concept Women Men SCORE Non-smoker Smoker Age Non-smoker Smoker % and over 10%-14% 5%-9% 3%-4% 2% 1% <1% 10-year risk of fatal CVD in populations at High CVD risk The risk of this 40 year old male smoker with risk factors is the same (3%) as that of a 60 year old man with ideal risk factor levels therefore his risk age is 60 years Cholesterol (mmol/l) mg/dl

19 Risk function without high-density lipoproteincholesterol (HDL-C) for men Non-smoker Age Smoker Without HDL HDL 0.8 HDL 1.0 HDL 1.4 HDL Without HDL HDL 0.8 HDL 1.0 HDL 1.4 HDL Without HDL HDL 0.8 HDL 1.0 HDL 1.4 HDL Without HDL HDL 0.8 HDL 1.0 HDL 1.4 HDL Without HDL HDL 0.8 HDL 1.0 HDL 1.4 HDL Without HDL HDL 0.8 HDL 1.0 HDL 1.4 HDL Without HDL HDL 0.8 HDL 1.0 HDL 1.4 HDL Without HDL HDL 0.8 HDL 1.0 HDL 1.4 HDL Systolic blood pressure (mmhg) Without HDL HDL 0.8 HDL 1.0 HDL 1.4 HDL Total Cholesterol (mmol/l)
20 Risk categories 20 Very high-risk Subjects with any of the following: Documented CVD, clinical or unequivocal on imaging. Documented clinical CVD includes previous AMI, ACS, coronary revascularization and other arterial revascularization procedures, stroke and TIA, aortic aneurysm and PAD. Unequivocally documented CVD on imaging includes significant plaque on coronary angiography or carotid ultrasound. It does NOT include some increase in continuous imaging parameters such as intima media thickness of the carotid artery. DM with target organ damage such as proteinuria or with a major risk factor such as smoking or marked hypercholesterolaemia or marked hypertension. Severe CKD (GFR <30 ml/min/1.73 m 2 ). A calculated SCORE >10%.
21 Risk categories 21 High-risk Subjects with: Markedly elevated single risk factors such as familial dyslipidaemias and severe hypertension. Most other people with diabetes (some young people with type 1 diabetes may be at low or moderate risk). Moderate CKD (GFR ml/min/1.73 m 2 ). A calculated SCORE 5% and < 10% for 10- year risk of fatal CVD. Moderaterisk Low-risk Subjects are considered to be at moderate risk when their SCORE is 1% and < 5% at 10 years. Many middle-aged subjects belong to this risk category. The low risk category applies to individuals with SCORE < 1%
22 ESC/EAS Guidelines for the management of dyslipidaemias Table of content: - What is cardiovascular disease prevention? - Total cardiovascular risk - Evaluation of laboratory lipid and apolipoprotein parameters - Treatment targets - Lifestyle modifications to improve the plasma lipid profile - Drugs for treatment of hypercholesterolaemia - Drugs for treatment of hypertriglyceridaemia - Drugs affecting high-density lipoprotein-cholesterol - Management of dyslipidaemia in different clinical settings - Monitoring of lipids and enzymes in patients on lipid-lowering therapy - Strategies to encourage adoption of healthy lifestyle changes and adherence to lipid modifying therapies
23 23 Lipid analyses as treatment targets Recommendations Class Level Non-HDL-C should be considered as a secondary treatment target. ApoB should be considered as a secondary treatment target, whenavailable. HDL-C is not recommended as a target for treatment. The ratios apob/apoa1 and non-hdl-c/hdl-c are not recommended as targets for treatment. IIa IIa III III B B A B
24 24 Treatment goals for LDL-cholesterol Recommendations Class Level In patients at VERY HIGH CV risk, an LDL-C goal of <1.8 mmol/l (70 mg/dl) or a reduction of at least 50% if the baseline LDL-C is between 1.8 and 3.5 mmol/l (70 and 135 mg/dl) is recommended. In patients at HIGH CV risk, an LDL-C goal of <2.6 mmol/l (100 mg/dl), or a reduction of at least 50% if the baseline LDL- C is between 2.6 and 5.2 mmol/l (100 and 200 mg/dl) is recommended. I I B B In subjects at LOW or MODERATE risk an LDL-C goal of <3.0 mmol/l ( <115 mg/dl) should be considered. IIa C
25 25 Intervention strategies Total CV risk (SCORE) % <70 mg/dl <1.8 mmol/l 70 to <100 mg/dl 1.8 to <2.6 mmol/l LDL-C levels 100 to <155 mg/dl 2.6 to <4.0 mmol/l 155 to <190 mg/dl 4.0 to <4.9 mmol/l <1 Lifestyle advice Lifestyle advice Lifestyle advice Lifestyle advice 190 mg/dl 4.9 mmol/l Lifestyle advice, consider drug if uncontrolled Class/Level I/C I/C I/C I/C IIa/A 1 to <5 Lifestyle advice Lifestyle advice Lifestyle advice, consider drug if uncontrolled Lifestyle advice, consider drug if uncontrolled Lifestyle advice, consider drug if uncontrolled Class/Level I/C I/C IIa/A IIa/A I/A 5 to <10, or high-risk Lifestyle advice Lifestyle advice, consider drug if uncontrolled Lifestyle advice and drug treatment for most Lifestyle advice and drug treatment Lifestyle advice and drug treatment Class/Level IIa/A IIa/A IIa/A I/A I/A 10 or very high-risk Lifestyle advice, consider drug a Lifestyle advice and concomitant drug treatment Lifestyle advice and concomitant drug treatment Lifestyle advice and concomitant drug treatment Lifestyle advice and concomitant drug treatment Class/Level IIa/A IIa/A I/A IA I/A a In patients with myocardial infarction, statin therapy should be considered irrespective of total cholesterol levels.
26 Recommendations for the pharmacological treatment of elevated LDL-cholesterol Prescribe statin up to the highest recommended dose or highest tolerable dose to reach the goal. In the case of statin intolerance, ezetimibe or bile acid sequestrants, or these combined, should be considered. If goal is not reached, statin combination with a cholesterol absorption inhibitor should be considered. If goal is not reached, statin combination with a bile acid sequestrant may be considered. In patients at very high risk, with persistent high LDL- C despite treatment with maximal tolerated statin dose, in combination with ezetimibe or in patients with statin intolerance, a PCSK9 inhibitor may be considered.
27 ESC/EAS Guidelines for the management of dyslipidaemias Table of content: - What is cardiovascular disease prevention? - Total cardiovascular risk - Evaluation of laboratory lipid and apolipoprotein parameters - Treatment targets - Lifestyle modifications to improve the plasma lipid profile - Drugs for treatment of hypercholesterolaemia - Drugs for treatment of hypertriglyceridaemia - Drugs affecting high-density lipoprotein-cholesterol - Management of dyslipidaemia in different clinical settings - Monitoring of lipids and enzymes in patients on lipid-lowering therapy - Strategies to encourage adoption of healthy lifestyle changes and adherence to lipid modifying therapies
28 Treatment of dyslipidaemia in older adults Recommendations Class Level Treatment with statins is recommended for older adults with established CVD in the same way as for younger patients. I A Since older people often have co-morbidities and have altered pharmacokinetics, lipidlowering medication should be started at a lower dose and then titrated with caution to achieve target lipid levels that are the same as in younger subjects. IIa C Statin therapy should be considered in older adults free from CVD, particularly in the presence of hypertension, smoking, diabetes and dyslipidaemia. IIa B

29 Management of dyslipidaemia in women Statin treatment is recommended for primary prevention of CAD in high-risk women. Statins are recommended for secondary prevention in women with the same indications and targets as in men. Lipid-lowering drugs should not be given when pregnancy is planned, during pregnancy or during the breastfeeding period. However, bile acid sequestrants (which are not absorbed) may be considered.
30 Lipid management in patients with moderate to severe chronic kidney disease Recommendations Class Level Patients with stage 3 5 CKD have to be considered at high or very high CV risk. I A The use of statins or statin/ezetimibe combination is indicated in patients with nondialysis-dependent CKD. In patients with dialysis-dependent CKD and free of atherosclerotic CVD, statins should not be initiated. I III A A In patients already on statins, ezetimibe or on a statin/ezetimibe combination at the time of dialysis initiation, these drugs should be continued particularly in patients with CVD. IIa C In adult kidney transplant recipients treatment with statins may be considered. IIb C

31 Tips to aid adherence to multiple drug therapies 1. Agree on rather than dictate a drug regimen to your patient and tailor it to his/her personal lifestyle and needs. 2. Back up verbal instructions with clear written instructions. 3. Simplify the dosing regimen and consider a fixed dose combination pill where available. 4. Perform a regular review of medicines to minimize polypharmacy (or ask the pharmacist to assist). 5. Encourage self-monitoring and use cues and technologies to act as reminders. 6. Provide information on common side effects and discuss management strategies. 7. Involve the partner, other family members or the caregiver in the patient s treatment.
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE
 2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
2016 EUROPEAN GUIDELINES ON CVD PREVENTION IN CLINICAL PRACTICE Massimo F Piepoli, MD, PhD, FESC, Piacenza, Italy on behalf of the 6 th Joint Task Force 2 3 Guidelines still based upon the principles of
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
Is it an era for statin for life?
 Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
Dyslipidemia in women: Who should be treated and how?
 Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March Crowne Plaza, Dublin
 2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
2017 Cardiovascular Summit for Primary Care Thursday 30th & Friday 31st March 2017 - Crowne Plaza, Dublin 2016 ESC Guidelines on Cardiovascular Risk and elevated lipids Carlos Brotons Sardenya Primary
Lipids: new drugs, new trials, new guidelines
 Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
Lipids: new drugs, new trials, new guidelines Milan Gupta, MD, FRCPC, FCCS State of the Heart Co-Chair Associate Clinical Professor of Medicine, McMaster University Assistant Professor of Medicine, University
ESC/EAS Guidelines for the Management of Dyslipidaemias
 ESC/EAS Guidelines for the Management of Dyslipidaemias Professor Željko Reiner, MD, PhD, FRCP(Lond), FESC, FACC University Hospital Center Zagreb School of Medicine, University of Zagreb, Croatia Declaration
ESC/EAS Guidelines for the Management of Dyslipidaemias Professor Željko Reiner, MD, PhD, FRCP(Lond), FESC, FACC University Hospital Center Zagreb School of Medicine, University of Zagreb, Croatia Declaration
Review current guideline recommendations for lipid-lowering therapy
 Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Breakout Session #3 New Paradigms in the Management of Dyslipidemia Review current guideline recommendations for lipid-lowering therapy Dr Meral KAYIKCIOGLU Ege University Medical School, Cardiology Dept,
Landmesser U et al. Eur Heart J 2017; https://doi.org/ /eurheartj/ehx549
 2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
2017 Update of ESC/EAS Task Force on Practical Clinical Guidance for PCSK9 inhibition in Patients with Atherosclerotic Cardiovascular Disease or in Familial Hypercholesterolaemia Cardiovascular Outcomes
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
SIGN 149 Risk estimation and the prevention of cardiovascular disease. Quick Reference Guide July Evidence
 SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
SIGN 149 Risk estimation and the prevention of cardiovascular disease Quick Reference Guide July 2017 Evidence ESTIMATING CARDIOVASCULAR RISK R Individuals with the following risk factors should be considered
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials
 Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
Alirocumab Treatment Effect Did Not Differ Between Patients With and Without Low HDL-C or High Triglyceride Levels in Phase 3 trials G. Kees Hovingh, 1 Richard Ceska, 2 Michael Louie, 3 Pascal Minini,
DYSLIPIDEMIA RECOMMENDATIONS
 DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
DYSLIPIDEMIA RECOMMENDATIONS Α. DIAGNOSIS Recommendation 1 INITIAL LIPID PROFILING (Level of evidence II) It is recommended to GPs and other PHC Physicians to assess the lipid profile {total cholesterol
CVD Risk Assessment. Michal Vrablík Charles University, Prague Czech Republic
 CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
CVD Risk Assessment Michal Vrablík Charles University, Prague Czech Republic What is Risk? A cumulative probability of an event, usually expressed as percentage e.g.: 5 CV events in 00 pts = 5% risk This
Secondary prevention and systems approaches: Lessons from EUROASPIRE and EUROACTION
 Secondary prevention and systems approaches: Lessons from EUROASPIRE and EUROACTION Dr Kornelia Kotseva National Heart & Lung Insitute Imperial College London, UK on behalf of all investigators participating
Secondary prevention and systems approaches: Lessons from EUROASPIRE and EUROACTION Dr Kornelia Kotseva National Heart & Lung Insitute Imperial College London, UK on behalf of all investigators participating
Disclosures. Objectives 2/11/2017
 Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Role of Non-Statin Therapy in CV Risk Reduction James A. Underberg, MD, MS, FACPM, FACP, FASH, FNLA,FASPC Clinical Assistant Professor of Medicine NYU School of Medicine NYU Langone Center for Cardiovascular
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
A Naturally Randomized Trial Comparing the Effect of Genetic Variants that Mimic CETP Inhibitors and Statins on the Risk of Cardiovascular Disease.
 A Naturally Randomized Trial Comparing the Effect of Genetic Variants that Mimic CETP Inhibitors and Statins on the Risk of Cardiovascular Disease. Brian A. Ference MD, MPhil, MSc, John J. P. Kastelein
A Naturally Randomized Trial Comparing the Effect of Genetic Variants that Mimic CETP Inhibitors and Statins on the Risk of Cardiovascular Disease. Brian A. Ference MD, MPhil, MSc, John J. P. Kastelein
Which CVS risk reduction strategy fits better to carotid US findings?
 Which CVS risk reduction strategy fits better to carotid US findings? Dougalis A, Soulaidopoulos S, Cholongitas E, Chalevas P, Vettas Ch, Doumtsis P, Vaitsi K, Diavasti M, Mandala E, Garyfallos A 4th Department
Which CVS risk reduction strategy fits better to carotid US findings? Dougalis A, Soulaidopoulos S, Cholongitas E, Chalevas P, Vettas Ch, Doumtsis P, Vaitsi K, Diavasti M, Mandala E, Garyfallos A 4th Department
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo?
 Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo? Alberto Zambon University of Padova - Italy DISCLOSURE - CONFLICT OF INTEREST Prof. A. Zambon reports having received grants,
Il rischio residuo nella persona con diabete: come individuarlo e come trattarlo? Alberto Zambon University of Padova - Italy DISCLOSURE - CONFLICT OF INTEREST Prof. A. Zambon reports having received grants,
BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS
 BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS Neil R Poulter ICCH, Imperial College London BHIVA: October 10th, 2008 Background CVD is the biggest single killer in the world CVD rates are increasing High
BEST PRACTICE MANAGEMENT: CARDIOVASCULAR RISKS Neil R Poulter ICCH, Imperial College London BHIVA: October 10th, 2008 Background CVD is the biggest single killer in the world CVD rates are increasing High
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies
 1. Evidence from genetic, epidemiologic and clinical studies") Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Low-density lipoproteins cause atherosclerotic cardiovascular disease (ASCVD) 1. Evidence from genetic, epidemiologic and clinical studies A Consensus Statement from the European Atherosclerosis Society
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Supplementary Online Content
 Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
Supplementary Online Content Kavousi M, Leening MJG, Nanchen D, et al. Comparison of application of the ACC/AHA guidelines, Adult Treatment Panel III guidelines, and European Society of Cardiology guidelines
New ESC Guidelines on Cardiovascular Disease Prevention in Clinical Practice. Lipids. Professor Željko Reiner, MD, PhD, FRCP(Lond), FESC, FACC
, FESC, FACC") New ES Guidelines on ardiovascular Disease Prevention in linical Practice Lipids Professor Željko Reiner, MD, PhD, FRP(Lond), FES, FA University Hospital enter Zagreb School of Medicine, University of
New ES Guidelines on ardiovascular Disease Prevention in linical Practice Lipids Professor Željko Reiner, MD, PhD, FRP(Lond), FES, FA University Hospital enter Zagreb School of Medicine, University of
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
LLL Session - Nutrition support in diabetes and dyslipidemia. Dyslipidemia: targeting the management of cardiovascular risk factors. M.
 ESPEN Congress Leipzig 2013 LLL Session - Nutrition support in diabetes and dyslipidemia Dyslipidemia: targeting the management of cardiovascular risk factors M. Leon Sanz (ES) Dyslipidemia: Targeting
ESPEN Congress Leipzig 2013 LLL Session - Nutrition support in diabetes and dyslipidemia Dyslipidemia: targeting the management of cardiovascular risk factors M. Leon Sanz (ES) Dyslipidemia: Targeting
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Cholesterol Treatment Trialists (CTT) Collaborators.
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Cholesterol Treatment Trialists (CTT) Collaborators.
Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD
 Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD Sao Paulo Medical School Sao Paolo, Brazil Subclinical atherosclerosis in CVD risk: Stratification & management Prof.
Subclinical atherosclerosis in CVD: Risk stratification & management Raul Santos, MD Sao Paulo Medical School Sao Paolo, Brazil Subclinical atherosclerosis in CVD risk: Stratification & management Prof.
 Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Five chapters 1. What is CVD prevention 2. Why is CVD prevention needed 3. Who needs CVD prevention 4. How is CVD prevention applied 5. Where should CVD prevention be offered Shorter, more adapted to clinical
Statins ARE Enough For The Prevention of CVD! Professor Kausik Ray Imperial College London, UK
 1 Disclosures Advisory boards PCSK9- Sanofi/ Regeneron, Amgen, Pfizer, Roche, MSD NLI/ SC member for Odyssey- (Sanofi/ Regeneron), Roche Investigator initiated research grant support (Sanofi/Regeneron/
1 Disclosures Advisory boards PCSK9- Sanofi/ Regeneron, Amgen, Pfizer, Roche, MSD NLI/ SC member for Odyssey- (Sanofi/ Regeneron), Roche Investigator initiated research grant support (Sanofi/Regeneron/
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
Think Again About Cholesterol Survey
 ATHEROSCLEROSIS SUPPLEMENTS Atherosclerosis Supplements 20 (2015) 1 5 www.elsevier.com/locate/atherosclerosis Think Again About Cholesterol Survey Alberico L. Catapano a, *, Olov Wiklund b, on behalf of
ATHEROSCLEROSIS SUPPLEMENTS Atherosclerosis Supplements 20 (2015) 1 5 www.elsevier.com/locate/atherosclerosis Think Again About Cholesterol Survey Alberico L. Catapano a, *, Olov Wiklund b, on behalf of
APPENDIX 2F Management of Cholesterol
 Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Patients with established CVD: Coronary heart disease Cerebrovascular disease Peripheral vascular disease APPEDIX 2F Management of Cholesterol Patients at high risk of cardiovascular events: Chronic kidney
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Current guidelines on prevention with a focus on dyslipidemias
 Review Article Current guidelines on prevention with a focus on dyslipidemias Ian M. Graham 1,2, Alberico L. Catapano 3, Nathan D. Wong 4 1 Trinity College Dublin, Dublin, Ireland; 2 Adelaide Health Foundation,
Review Article Current guidelines on prevention with a focus on dyslipidemias Ian M. Graham 1,2, Alberico L. Catapano 3, Nathan D. Wong 4 1 Trinity College Dublin, Dublin, Ireland; 2 Adelaide Health Foundation,
The TNT Trial Is It Time to Shift Our Goals in Clinical
 The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
The TNT Trial Is It Time to Shift Our Goals in Clinical Angioplasty Summit Luncheon Symposium Korea Assoc Prof David Colquhoun 29 April 2005 University of Queensland, Wesley Hospital, Brisbane, Australia
Intercommunale de Santé Publique du Pays de Charleroi, Charleroi, Belgium 2
 Lipid Abnormalities Remain High among Treated Hypertensive Patients with Stable CHD: Results of the Dyslipidemia International Study (DYSIS) II Belgium Michel Guillaume 1, Eric Weber 2, Johan De Sutter
Lipid Abnormalities Remain High among Treated Hypertensive Patients with Stable CHD: Results of the Dyslipidemia International Study (DYSIS) II Belgium Michel Guillaume 1, Eric Weber 2, Johan De Sutter
Guidelines on cardiovascular risk assessment and management
 European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
European Heart Journal Supplements (2005) 7 (Supplement L), L5 L10 doi:10.1093/eurheartj/sui079 Guidelines on cardiovascular risk assessment and management David A. Wood 1,2 * 1 Cardiovascular Medicine
Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both
 Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both Lluís Masana Vascular Medicine and Metabolism Unit. Sant Joan University Hospital. IISPV. CIBERDEM Rovira i Virgili
Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both Lluís Masana Vascular Medicine and Metabolism Unit. Sant Joan University Hospital. IISPV. CIBERDEM Rovira i Virgili
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Inhibition of PCSK9: The Birth of a New Therapy
 Inhibition of PCSK9: The Birth of a New Therapy Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Disclosures Dr. Kastelein
Inhibition of PCSK9: The Birth of a New Therapy Prof. John J.P. Kastelein, MD PhD FESC Dept. of Vascular Medicine Academic Medical Center / University of Amsterdam The Netherlands Disclosures Dr. Kastelein
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Present state and future trends of prevention guidelines
 Present state and future trends of prevention guidelines Professor Željko Reiner MD, PhD, FRCP (Lond), FESC,FACC School of Medicine, University of Zagreb, Croatia History of European guidelines on CVD
Present state and future trends of prevention guidelines Professor Željko Reiner MD, PhD, FRCP (Lond), FESC,FACC School of Medicine, University of Zagreb, Croatia History of European guidelines on CVD
Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia. Prof. Alberto Corsini University of Milan, Italy
 Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia Prof. Alberto Corsini University of Milan, Italy Outline of the presentation State of the art on statin therapy Explore unmet
Farmaci innovativi in ambito cardiovascolare: considerazioni di Farmacologia Prof. Alberto Corsini University of Milan, Italy Outline of the presentation State of the art on statin therapy Explore unmet
surtout qui n est PAS à risque?
 3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
3*25 min et surtout qui n est PAS à risque? 2018 ESC/ESH Hypertension Guidelines 2018 ESC-ESH Guidelines for the Management of Arterial Hypertension 28 th ESH Meeting on Hypertension and Cardiovascular
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations?
 FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
FOURIER: Enough Evidence to Justify Widespread Use? Did It fulfill Its Expectations? CVCT Washington, DC November 3, 2017 Marc S. Sabatine, MD, MPH Chairman, TIMI Study Group Lewis Dexter, MD, Distinguished
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden
 Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Optimizing risk assessment of total cardiovascular risk What are the tools? Lars Rydén Professor Karolinska Institutet Stockholm, Sweden Cardiovascular Disease Prevention (CVD) Three Strategies for CVD
Latest Guidelines for Lipid Management
 Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Latest Guidelines for Lipid Management Goals Recognize the differences between different guidelines Understand the effective strategies to tailor lipid lowering therapies based on evidence and guideline
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Familial hypercholesterolaemia in children and adolescents
 Familial hypercholesterolaemia in children and adolescents Rationale and recommendations for early identification and treatment European Atherosclerosis Society Consensus Panel Slide deck adapted from:
Familial hypercholesterolaemia in children and adolescents Rationale and recommendations for early identification and treatment European Atherosclerosis Society Consensus Panel Slide deck adapted from:
Prevention in Europe
 Prevention in Europe Geneviève Derumeaux Créteil University, France Ian M Graham Trinity College, Dublin ESC: 2016 Lipid guidelines 2016 Joint Prevention Guidelines Cardiovascular disease in Europe Nick
Prevention in Europe Geneviève Derumeaux Créteil University, France Ian M Graham Trinity College, Dublin ESC: 2016 Lipid guidelines 2016 Joint Prevention Guidelines Cardiovascular disease in Europe Nick
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
Models of preventive care in clinical practice to achieve 25 by 25
 Models of preventive care in clinical practice to achieve 25 by 25 Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College
Models of preventive care in clinical practice to achieve 25 by 25 Professor David A Wood Garfield Weston Professor of Cardiovascular Medicine International Centre for Circulatory Health Imperial College
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice
 2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
2016 ESC/EAS Guideline in Dyslipidemias: Impact on Treatment& Clinical Practice Nattawut Wongpraparut, MD, FACP, FACC, FSCAI Associate Professor of Medicine, Division of Cardiology, Department of Medicine
LIPID GUIDELINES: 2015
 LIPID GUIDELINES: 2015 D P Mikhailidis BSc MSc MD FCPP FCP FRSPH FFPM FRCP FRCPath Academic Head Dept. of Clinical Biochemistry (Vascular Disease Prevention Clinics) Royal Free campus University College
LIPID GUIDELINES: 2015 D P Mikhailidis BSc MSc MD FCPP FCP FRSPH FFPM FRCP FRCPath Academic Head Dept. of Clinical Biochemistry (Vascular Disease Prevention Clinics) Royal Free campus University College
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus
 Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Managing Dyslipidemia and ASCVD Risk: Confusion, Controversy Consensus Pamela B. Morris, MD, FACC, FAHA, FASPC, FNLA Chair, ACC Prevention of Cardiovascular Disease Council and Section The Medical University
Current Cholesterol Guidelines and Treatment of Residual Risk COPYRIGHT. J. Peter Oettgen, MD
 Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Current Cholesterol Guidelines and Treatment of Residual Risk J. Peter Oettgen, MD Associate Professor of Medicine Harvard Medical School Director, Preventive Cardiology Beth Israel Deaconess Medical Center
Familial hypercholesterolaemia
 Familial hypercholesterolaemia Jaimini Cegla MRCP FRCPath PhD Consultant in Chemical Pathology and Metabolic Medicine Hammersmith Hospital Lipid Clinic 20 April 2017 An unrecognised, potentially fatal,
Familial hypercholesterolaemia Jaimini Cegla MRCP FRCPath PhD Consultant in Chemical Pathology and Metabolic Medicine Hammersmith Hospital Lipid Clinic 20 April 2017 An unrecognised, potentially fatal,
Key recommendations on antithrombotic and lipid lowering therapy from the 2017 guidelines of the European Society of Cardiology
 Key recommendations on antithrombotic and lipid lowering therapy from the 2017 guidelines of the European Society of Cardiology Univ.-Prof. Dr. med. Christine Espinola-Klein Department of Angiology Center
Key recommendations on antithrombotic and lipid lowering therapy from the 2017 guidelines of the European Society of Cardiology Univ.-Prof. Dr. med. Christine Espinola-Klein Department of Angiology Center
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016
 HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
HYPERLIPIDEMIA IN THE OLDER POPULATION NICOLE SLATER, PHARMD, BCACP AUBURN UNIVERSITY, HARRISON SCHOOL OF PHARMACY JULY 16, 2016 NOTHING TO DISCLOSE I, Nicole Slater, have no actual or potential conflict
Protecting the heart and kidney: implications from the SHARP trial
 Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Cardiology Update, Davos, 2013: Satellite Symposium Protecting the heart and kidney: implications from the SHARP trial Colin Baigent Professor of Epidemiology CTSU, University of Oxford S1 First CTT cycle:
Beyond LDL-Cholesterol
 Biomarkers for Risk Stratification Beyond LDL-Cholesterol Athanasios J.Manolis Director Cardioilogy Dep, Asklepeion Hospital, Athens, Greece Adj. Professor of Medicine, Emory University Atlanta, USA Adj.
Biomarkers for Risk Stratification Beyond LDL-Cholesterol Athanasios J.Manolis Director Cardioilogy Dep, Asklepeion Hospital, Athens, Greece Adj. Professor of Medicine, Emory University Atlanta, USA Adj.
CLINICAL OUTCOME Vs SURROGATE MARKER
 CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
CLINICAL OUTCOME Vs SURROGATE MARKER Statin Real Experience Dr. Mostafa Sherif Senior Medical Manager Pfizer Egypt & Sudan Objective Difference between Clinical outcome and surrogate marker Proper Clinical
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
ESC/EAS GUIDELINES ON MANAGEMENT OF DYSLIPIDEMIAS IN CLINICAL PRACTICE
 ESC/EAS GUIDELINES ON MANAGEMENT OF DYSLIPIDEMIAS IN CLINICAL PRACTICE Professor Željko Reiner, MD, PhD,FRCP(Lond), FESC Director, University Hospital Center Zagreb School of Medicine, University of Zagreb,
ESC/EAS GUIDELINES ON MANAGEMENT OF DYSLIPIDEMIAS IN CLINICAL PRACTICE Professor Željko Reiner, MD, PhD,FRCP(Lond), FESC Director, University Hospital Center Zagreb School of Medicine, University of Zagreb,
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future
 ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
ESC Geoffrey Rose Lecture on Population Sciences Cholesterol and risk: past, present and future Rory Collins BHF Professor of Medicine & Epidemiology Clinical Trial Service Unit & Epidemiological Studies
B. Patient has not reached the percentage reduction goal with statin therapy
 Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
FORTH VALLEY. LIPID LOWERING GUIDELINE v5 2016
 FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
FORTH VALLEY LIPID LOWERING GUIDELINE v5 2016 This guideline applies to people over 16 years of age. This guideline is not intended to serve as a standard of medical care or be applicable in every situation.
The 2012 European Guidelines on Cardiovascular Disease Prevention in Clinical Practice
 The 2012 European Guidelines on Cardiovascular Disease Prevention in Clinical Practice Introduction «meet the Taskforce» Disclosure: no conflicts of interest On behalf of : The 5th Joint European Societies
The 2012 European Guidelines on Cardiovascular Disease Prevention in Clinical Practice Introduction «meet the Taskforce» Disclosure: no conflicts of interest On behalf of : The 5th Joint European Societies
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY. Harvey D White on behalf of The STABILITY Investigators
 STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
AIM HIGH for SATURN and stay SHARP; COURAGE (v1.5)
") AIM HIGH for SATURN and stay SHARP; COURAGE (v1.5) Jacques Genest MD Cardiovascular Research Laboratory McGill University Health Center Disclosure J. Genest MD 2012 Advisory Board, Speaker s Bureau, Consultant,
AIM HIGH for SATURN and stay SHARP; COURAGE (v1.5) Jacques Genest MD Cardiovascular Research Laboratory McGill University Health Center Disclosure J. Genest MD 2012 Advisory Board, Speaker s Bureau, Consultant,
EUROPEAN SURVEY OF CARDIOVASCULAR DISEASE PREVENTION AND DIABETES EUROASPIRE IV. GUY DE BACKER Ghent University,Belgium
 EUROPEAN SURVEY OF CARDIOVASCULAR DISEASE PREVENTION AND DIABETES EUROASPIRE IV GUY DE BACKER Ghent University,Belgium ESC Congress 2012, aug.25-29th, Munich, Germany ESC Congress 2012, aug.25-29th, Munich,
EUROPEAN SURVEY OF CARDIOVASCULAR DISEASE PREVENTION AND DIABETES EUROASPIRE IV GUY DE BACKER Ghent University,Belgium ESC Congress 2012, aug.25-29th, Munich, Germany ESC Congress 2012, aug.25-29th, Munich,
Identification and management of familial hypercholesterolaemia (FH) - An overview
 - An overview") Identification and management of familial hypercholesterolaemia (FH) - An overview National Collaborating Centre for Primary Care and Royal College of General Practitioners NICE Guideline CG 71 (August
Identification and management of familial hypercholesterolaemia (FH) - An overview National Collaborating Centre for Primary Care and Royal College of General Practitioners NICE Guideline CG 71 (August
Cholesterol; what are the future lipid targets?
 Cholesterol; what are the future lipid targets? lipidologist out-of-business in 5-10 years? G.Kees Hovingh dept of vascular medicine, Academic Medical Center g.k.hovingh@amc.uva.nl Disclosure - Consultant
Cholesterol; what are the future lipid targets? lipidologist out-of-business in 5-10 years? G.Kees Hovingh dept of vascular medicine, Academic Medical Center g.k.hovingh@amc.uva.nl Disclosure - Consultant
Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol)
") CLINICAL GUIDELINE Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol) A guideline is intended to assist healthcare professionals in the choice of disease-specific
CLINICAL GUIDELINE Coronary Heart Disease and Stroke, Primary and Secondary Prevention Guidelines (Cholesterol) A guideline is intended to assist healthcare professionals in the choice of disease-specific
NICE QIPP about Lipitor. Robert Trotter. Clinical Effectiveness Consultant
 NICE QIPP about Lipitor Robert Trotter Clinical Effectiveness Consultant LIP2894c Date of preparation: April 2009 Prescribing information for atorvastatin is available on the last slide Roadmap Background
NICE QIPP about Lipitor Robert Trotter Clinical Effectiveness Consultant LIP2894c Date of preparation: April 2009 Prescribing information for atorvastatin is available on the last slide Roadmap Background
the high CVD risk smoker
 Smoking Cessation: population and patients A comprehensive approach to the smoker the high CVD risk smoker Catriona Jennings Cardiovascular Specialist Research Nurse Imperial College London European Society
Smoking Cessation: population and patients A comprehensive approach to the smoker the high CVD risk smoker Catriona Jennings Cardiovascular Specialist Research Nurse Imperial College London European Society
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Deep Dive into Contemporary Cholesterol Management. Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City
 Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
Deep Dive into Contemporary Cholesterol Management Kim Allan Williams, Sr., MD, FACC Pamela B. Morris, MD, FACC 7 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO CONSENSUS IN
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
Cardiovascular Disease Prevention: Current Knowledge, Future Directions
 Cardiovascular Disease Prevention: Current Knowledge, Future Directions Daniel Levy, MD Director, Framingham Heart Study Professor of Medicine, Boston University School of Medicine Editor-in-Chief, Journal
Cardiovascular Disease Prevention: Current Knowledge, Future Directions Daniel Levy, MD Director, Framingham Heart Study Professor of Medicine, Boston University School of Medicine Editor-in-Chief, Journal
Familial Hypercholesterolemia
 Familial Hypercholesterolemia Dr.Ramzi Al-Mohammadi Assistant Professor of Medicine Interventional Cardiologist, Advanced HF and Transplant Consultant Classification of Hyperlipedemia Primary hyperlipedemia:
Familial Hypercholesterolemia Dr.Ramzi Al-Mohammadi Assistant Professor of Medicine Interventional Cardiologist, Advanced HF and Transplant Consultant Classification of Hyperlipedemia Primary hyperlipedemia:
SECONDARY PREVENTION OF CORONARY HEART DISEASE AND ISCHAEMIC STROKE/TIA
 PRIMARY PREVENTION OF CHD AND STROKE IN HIGH RISK PATIENTS Random non fasting test for total cholesterol, HDL cholesterol (TC:HDL ratio) and LFTs If cholesterol > 7.5 mmol/l or LDL C 5mmol/l exclude secondary
PRIMARY PREVENTION OF CHD AND STROKE IN HIGH RISK PATIENTS Random non fasting test for total cholesterol, HDL cholesterol (TC:HDL ratio) and LFTs If cholesterol > 7.5 mmol/l or LDL C 5mmol/l exclude secondary
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES
 ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
ESC GUIDELINES ON DIABETES AND CARDIOVASCULAR DISEASES Pr. Michel KOMAJDA Institute of Cardiology - IHU ICAN Pitie Salpetriere Hospital - University Pierre and Marie Curie, Paris (France) DEFINITION A
The EUROASPIRE surveys: lessons learned in cardiovascular disease prevention
 Brief Report The EUROASPIRE surveys: lessons learned in cardiovascular disease prevention Kornelia Kotseva 1,2 ; on behalf of the EUROASPIRE Investigators 1 National Heart & Lung Institute, Imperial College
Brief Report The EUROASPIRE surveys: lessons learned in cardiovascular disease prevention Kornelia Kotseva 1,2 ; on behalf of the EUROASPIRE Investigators 1 National Heart & Lung Institute, Imperial College
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary