Cholesterol Medicines New & Old: What to Use When
|
|
|
- Wendy Scott
- 5 years ago
- Views:
Transcription
1 Cholesterol Medicines New & Old: What to Use When Patrick E. McBride, M.D., M.P.H. Division of Cardiovascular Medicine Preventive Cardiology Program Disclosures McBride no conflicts of interest Outline New lipid guidelines Overview of key points Evidence of statins and PCKS - 9 CVD risk prediction Myalgias Beyond the guidelines Do HDL-C and TG matter? When to use non-statin medications The use of niacin and fish oil
2 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation, American Pharmacists Association, American Society for Preventive Cardiology, Association of Black Cardiologists, Preventive Cardiovascular Nurses Association, and Women Heart: The National Coalition for Women with Heart Disease Guideline Scope Focus on treatment of blood cholesterol to reduce ASCVD risk in adults Emphasize adherence to a heart healthy lifestyle - See lifestyle guidelines Identify individuals most likely to benefit from cholesterol-lowering therapy: statin benefit groups Identify safety issues Advances in the Guidelines 1. Focus is on treatment of LDL-C 2. Treatment is based on risk: not just on LDL-C 3. Risk assessment - evidence to support its use in identifying patients to treat 4. Treatment based on evidence and the intensity of treatment;; no LDL targets
3 Why Not Continue to Treat to Target? 1. Current RCT data do not indicate precise targets 2. Unknown magnitude of additional ASCVD risk reduction with one target compared to another target 3. Unknown rate of additional adverse effects from multidrug therapy used to achieve specific goals 4. Unknown net benefit from treat-to-target approach No LDL Targets or Measurements? No targets does not mean not measuring panel to see if appropriate intensity achieved (hypo-responders) Adherence! < 50% take medicine as prescribed LDL-C <40 mg/dl is too low - lower statin dose Consider adjusting therapy (lifestyle, other) if LDL-C not low enough for risk Statin Benefit Groups Clinical ASCVD (includes stroke and PAD) LDL-C 190 mg/dl w/out secondary cause Primary prevention Diabetes mellitus (DM) and years old: LDL-C mg/dl Primary Prevention: No DM and age years: LDL-C mg/dl, if ASCVD risk 7.5% Requires risk discussion consider statin therapy after lifestyle trial
4 Intensity of Statin Therapy Use evidence-based therapy High risk patients = high intensity Rx 10 year ASCVD risk 7.5% (I, A) Moderate risk = moderate intensity Rx 10 year ASCVD risk 5%-7.5% (IIA, B) Consider if LDL-C > 160 mg/dl, genetic dyslipidemia, family hx of premature heart disease, hscrp> 2 mg/l, CAC >300 or 75 th %tile, ABI 0.9, or high lifetime risk (IIB, C) Primary Prevention: Global Risk Assessment To estimate 10-year / lifetime ASCVD risk New Pooled Cohort Risk Equations White and black, men and women More accurately identifies higher risk individuals for statin therapy Focuses statin therapy on those most likely to benefit Consider not initiating statin therapy in high-risk groups not found to benefit from statins (advanced HF, hemodialysis) Primary Prevention: Statin Therapy Thresholds for initiating statin therapy derived from RCTs Before initiating statin therapy, engage in a discussion of the potential for ASCVD risk reduction benefits, potential for adverse effects, medication interactions, and patient preferences

5 Statins Reduce CVD Risk Cholesterol Treatment Trialists (CTT) Collaborators Prospective meta-analysis of RCTs conducted from 1994 to ,526 subjects in 21 statin vs. control 39,612 subjects in 5 more vs. less intensive Median follow-up = 5.1 years Lancet 2010;;376:167 0 CTT Collaborators Improved CVD outcomes per 39 mg/dl reduction in LDL-C (all p<0.0001) 10% reduction in all-cause mortality 20% reduction in coronary mortality 21% reduction in major CVD events 26% reduction in MI or CHD death 24% reduction in PCI/CABG 15% reduction in stroke Lancet 2010;;376:167 0 CTT Collaborators Subgroups
6 Intensity of Statin Therapy*** *Individual responses to statin therapy varied in RCTs - expected to vary in clinical practice. Simvastatin 80 mg was evaluated in RCTs but is not recommended by the FDA due to the risk of myopathy & rhabdomyolysis Safety RCTs & meta-analyses used to identify important safety considerations Allow estimation of net benefit from statins Expert guidance on management of statinassociated adverse effects, including muscle symptoms Advise use of additional information including pharmacists, manufacturers prescribing information, & drug information centers for complex cases Creatinine Kinase and ALT Baseline/ongoing measures of CK and ALT not needed (Routine CK Class III) Consider if underlying muscle or liver disease or patient at increased risk Family or personal history Concomitant meds that may interact Clinical problems that predispose Measure if patient is symptomatic
7 Management of Mild-Moderate Statin-Associated Myalgias Discontinue statin until sx are evaluated Evaluate the patient for other conditions that might increase the risk for muscle symptoms* Hypothyroidism, kidney/liver disease, rheumatologic disorders (PMR), steroid myopathy, low Vitamin D status, or primary muscle diseases If after 2 months without statin Rx, muscle sx or elevated CK levels do not resolve completely, consider other causes of muscle sx Management of Severe Myalgia or Fatigue on Statin Therapy Promptly discontinue the statin Evaluate for rhabomyolysis CK Creatinine Urine analysis for myoglobinuria Statin Safety - Neurocognitive Meta-analysis of 23,443;; statin exposure 3-25 years No adverse effect of statins on cognition long-term data may support a beneficial role for statins in the prevention of dementia 29% RRR incident dementia (HR 0.71, CI: ) Systematic review Published data do not suggest an adverse effect of statins on cognition But: issues of selection and ascertainment Strength limited, esp. with high intensity statin Swiger KJ, et al. Mayo ClinProc2013;;88:121 Richardson K, et al. Ann Inter n Med 2013;;159:688
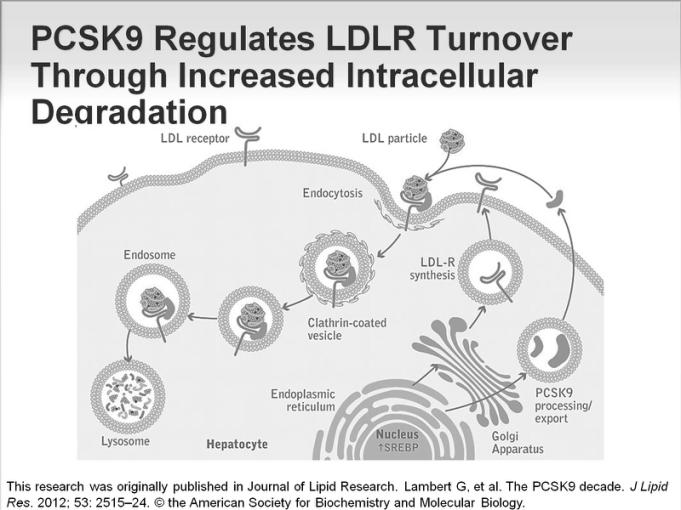
8 IMPROVE-IT Evidence for Ezetimibe RCT: N=18,144 Post-ACS 10 days LDL-C mg/dl ( 100 mg/dl if lipidtx) Standard treatment and interventions Simva 40 mg vs. simva 40/ezetimibe 10 mg QD Increase to simva 80 mg if LDL-C >70 mg/dl >90% power to detect a 9% w/5250 events 1 Endpoint: CV death, MI, hospital admission for UA, coronary revascularization, or stroke Cannon CJ, et al. N Engl J Med 2015;;372:2387 IMPROVE-IT Statin + Ezetimibe: Absolute Benefit 2% Cannon CP et al. N Engl J Med 2015;;372: PCKS-9 Inhibitors Proprotein convertase subtilisin / kexin type 9 Enzyme that modulates LDLR density on hepatocytes (and intestines, kidneys, CNS) Secreted from hepatocytes bindsldlreceptor endocytosis and degradation in lysosomes Inverse relationship between the blood PCSK9 level and LDLR density Inhibition of PCSK9 prevents LDLRdegradation and preserves LDLR recycling to the hepatocyte surface Each receptor normally recycles approximately 150x MAb prevents binding of PCSK-9 to the LDL / LDLR complex greater LDLR density LDL-C clearance
9

10
11 Beyond the Guidelines Low HDL-C Hypertriglyceridemia Combined dyslipidemias Lipoprotein evaluation / treatment No RCTs / recommendations Biomarkers Atherosclerosis imaging Medications for VLDL / TGs / HDL Fibrates (e.g. fenofibrate / gemfibrozil) increase lipoprotein lipase production and decrease VLDL production Niacin (vitamin B3) decreases VLDL production Omega 3 fatty acids e.g. fish oil, flax oil reduce VLDL production Use of Non-Statin Lipid Therapies If TGs >500 mg/dl Fibrates (or niacin or fish oil) Prevent pancreatitis and hepatic steatosis (non-guideline) Consider addition of a non-statin medication Statin intolerance Persistent, less than therapeutic response Assure compliance with meds and lifestyle High-intensity: if LDL <50% or >100 mg/dl Moderate intensity: <30% decrease Use the maximum tolerated dose of statin
12 Use of Non-Statin Lipid Therapies Risk-reduction benefits should outweigh potential for adverse effects Focus on: Clinical ASCVD <75 years of age Baseline LDL-C 190 mg/dl (genetic) Diabetes mellitus, years of age Prefer non-statin cholesterol-lowering medication that reduced ASCVD events in RCTs Use of Non-Statin Lipid Therapies Evidence to support monotherapy with niacin and bile acid resins in individuals with high total or LDL cholesterol (older studies CDP, LRC-CPPT) Evidence for using niacin and fibrates as monotherapy in individuals with high TG and low HDL-C (VA-HIT, HHS) Residual CVD Risk on Statins CV Event Rate (%) S CARE HPS PROVE-IT Control Statin TNT
13 HDL Atherosclerosis Treatment Study (HATS) N = 160 CAD patients HDL-C: women 40 mg/dl, men 35 mg/dl Baseline lipids: TC 199, HDL-C 32, TG 203, LDL-C 127 mg/dl Randomized, 2 x 2 factorial Simvastatin and niacin Antioxidants (C and E, -carotene, selenium) Outcomes after 3 years Brown BG, et al. N Engl J Med. 2001;;345:15 83 HATS: Clinical Endpoints -89% Composite Event Rate (%) * Coronary Death, MI, Stroke, or Revascularization Placebo Simva + niacin Antioxidants S + N + AV Brown BG, et al. N Engl J Med. 2001;;345:15 83 * p=0.003 vs placebo AIM-HIGH N=3,414 men and women with Atherosclerotic vascular disease HDL-C 40 (men);; 50 mg/dl (women) TG mg/dl LDL-C 180 mg/dl Randomized to simvastatin vs. simvastatin + ER niacin 1 endpoint: CHD death, MI, stroke, high-risk ACS, or symptom-driven coronary or cerebral revascularization The AIM-HIGH Investigat ors. N Engl J Med 2011;;365:22 55
14 AIM-HIGH Power: 85% for 25% CVD event reduction with N=850 events ER niacin: 500 mg/d, titrated to 2000 mg/d over 4-8 weeks (open-label run-in) If tolerated 1500 mg/d randomized to maximally tolerated dose of ER niacin or a placebo spiked with 50 mg of IR niacin Simvastatin adjusted during the first 6 months to a LDL-C target of mg/dl Ezetimibe added to reach LDL-C goal The AIM-HIGH Investigat ors. N Engl J Med 2011;;365:22 55 AIM-HIGH After 1 year, ER niacin/statin vs. statin HDL-C (mean 35 mg/dl) by 23% vs. 9% TG (mean 163 mg/dl) by 28% vs. 5% LDL-C (mean 74 mg/dl) by 10% vs. 4% Non-HDL-C from 108 to 90 mg/dl vs. 108 to 102 mg/dl Stopped for futility after a mean of 3 years Primary end point occurred in 282 patients in the niacin group (16.4%) and in 274 patients in the placebo group (16.2%) (HR 1.02;; p=0.79) The AIM-HIGH Investigat ors. N Engl J Med 2011;;365:22 55 AIM-HIGH The AIM-HIGH Investigat ors. N Engl J Med 2011;;365:22 55
15 AIM-HIGH In a subset of patients with the highest TGs ( 198 mg/dl) and lowest HDL-C (<33 mg/dl), ER niacin showed a trend toward benefit (HR 0.74, p = 0.073) Guyton JR, et al. J Am Coll Cardiol 2013;;62:158 0 HPS2-THRIVE Prospective RCT to determine if Niacin + laropiprant prevents CVD events on a background of statin therapy High-risk patients receiving intensive LDLlowering tx N=25,673, aged years old All had ASCVD All on simvastatin 40 mg (+ ezetimibe 10 mg/d, if needed to get TC <135 mg/dl) Randomized to niacin 2 g/d + laropiprant 40 mg/d vs. placebo The HPS2-THRIVE Collabor ative Gr oup. N Engl J Med 2014;;371:203 HPS2-THRIVE After a median of 4 years HDL-C (mean 44 mg/dl) by 6 mg/dl TG (mean 125 mg/dl) by 33 mg/dl LDL-C (mean 63 mg/dl) by 10 mg/dl Niacin-laropiprant had no sig. effect on ASCVD (13.2% vs. 13.7%;; RR 0.96;; p=0.29) Absolute 3.7% increase in serious side effects esp. DM, infection, GI, and myalgia (in China: RR 5.2 vs 1.5 in Europe) The HPS2-THRIVE Collabor ative Gr oup. N Engl J Med 2014;;371:203
16 HPS2-THRIVE The HPS2-THRIVE Collabor ative Gr oup. N Engl J Med 2014;;371: HDL and Niacin Niacin AIM-HIGH: Niacin as add-on to effective statin tx does not reduce events HPS-THRIVE: Supports AIM-HIGH, though risks may be due to laropiprant or niacin Main effect may be LDL-lowering: main use as 2nd line for residual high LDL-C As in AIM-HIGH and ACCORD, the subgroup with TG > 200 mg/dl and HDL < 40 had significant benefit Voight BF, et al. Lancet 2012;; 380: 572 Holmes, MH. Eur Heart J 2014: doi: / eur he ar tj /e ht 57 1 Action to Control CVD Risk in Diabetes (ACCORD) Study N = 5518 w/type II diabetes mellitus Open-label simvastatin RCT fenofibrate 160 mg vs. placebo 1 outcomes = CVD death, non-fatal MI, non-fatal stroke Mean duration 4.7 years Baseline lipids: TC 175, HDL-C 38, TG 162, LDL-C 100 mg/dl N Engl J Med 2010;; 362:1563
17 ACCORD Lipid Changes N Engl J Med 2010;; 362:1563 ACCORD CVD Outcomes + revasc, hosp. CHF N Engl J Med 2010;; 362:1563 ACCORD - Subgroups N Engl J Med 2010;; 362:1563
18 Fish Oil Capsules Omega 3 s Must use total daily dose of 4000 mg of DHA + EPA Divide BID Look at back of label! Many say 1000 mg on front, but low DHA + EPA Cholesterol Medications LDL Statins (best evidence most effective) Ezetimibe Bile Acid Resins PCKS-9 Inhibitors (new, very expensive, limited evidence) Triglycerides / HDL Fibrates Niacin Fish Oil Thank You! Questions?
19 Cholesterol Medications: Sites of Actions Decrease lipoprotein synthesis: Statins (HMG CoA reductase inhibitors) PCKS 9 inhibitors Niacin - Omega 3 s Fibrates - CETP inhibitors Decrease Cholesterol Absorption Ezetimibe Bile acid resins Plant Sterols / Stanol esters Fibers (psyllium, oat bran, etc) Use of Biomarkers and Imaging Apo B, LDL particles, Lp(a): ungraded;; future question hscrp (IIB for primary prevention) Mendelian randomization studies suggest it is a marker and not causal Intermediate/residual risk on statin (not guideline) JUPITER-type patients (not guideline) Ridker BMJ 2011;;342:d54 8 PM et al. N Engl J Med 2008;;359 Use of Imaging ABI, CAC, carotid IMT All IIB, except misgraded carotid IMT (III) No RCT data Future question: how can noninvasive imaging guide treatment? BMJ 2011;;342:d54 8 Stein JH, Tattersall M. J Am Coll Cardiol 2014:63:2301


20 JUPITER RCT of 17,802 healthy individuals Men >50, women >60 years LDL-C <130 mg/dl hscrp >2.0 mg/l Rosuvastatin 20 mg daily vs. placebo Stopped early after 1.9 years Baseline (median) characteristics Age 66 yrs, LDL-C 108 mg/dl BMI 28.3 kg/m 2, 41% Metabolic Syndrome Ridker PM et al. N Engl J Med 2008;;359 JUPITER HPS2-THRIVE The HPS2-THRIVE Collabor ative Gr oup. N Engl J Med 2014;;371:203
21 CTT Collaborators Subgroups Japan EPA Lipid Intervention Study (JELIS) RCT of 18,645 subjects with TC >253 Pravastatin/simvastatin + EPA 1800 mg vs. statin alone (open-label) 1 endpoint: SCD, fatal and non-fatal MI, unstable angina, PCI/CABG Mean follow-up 4.6 years Baseline lipids: HDL-C 59, TG 154, LDL-C 183 mg/dl Lancet 2007;; 369:1090 JELIS LDL-C 25% in both arms;; TG 9 vs 4% (p<0.001) all primary secondary 1 endpoint: 262 (2.8%) EPA vs. 324 (3.5%) controls = 19% RRR;; 0.7% ARR (p=0.011) In those with CAD: 158 (8.7%) EPA vs. 197 (10.7%) controls = 19% RRR;; 2% ARR (p=0.048) Lancet 2007;; 369:1090
 Among subjects with LDL-C <70 mg/dl, HDL-C levels independently predicted CVD events (p=0.03) Barter PJ, et al. N Engl J Med 2007;;357:13 01 Why Do We Have HDL?")
22 Residual CVD Event Rates on Statins are Predicted by HDL-C Levels Post-hoc analysis, TNT RCT of 9770 CHD patients on atorvastatin, 10 or 80 mg Quintiles of HDL-C levels predicted CVD events (p=0.04) Among subjects with LDL-C <70 mg/dl, HDL-C levels independently predicted CVD events (p=0.03) Barter PJ, et al. N Engl J Med 2007;;357:13 01 Why Do We Have HDL? Reverse cholesterol transport unlikely to be selected for until recent increase in CVD deaths Anti-inflammatory effects Host defense and immunity Protection from endotoxin Protection from trypanosomes Low HDL-C Increases CHD Risk, Even if LDL-C is Low: Framingham Heart Study Patient 1 LDL-C 100 HDL-C 25 Patient 2 LDL-C 220 HDL-C 45 CHD Relative Risk HDL-C, mg/dl LDL-C, mg/dl Kwiterovich PO, Am J Cardiol 1998;;82:19Q


23 Triglycerides Controversial as a marker as a cause of CVD risk, because of associations with Obesity Diabetes mellitus Adverse lifestyle habits Inflammation Low HDL-C Small LDL LDL particle excess Mendelian randomization studies do support causal role;; weaker than for LDL-C Miller M, et al. Circulation 2011:123;;229 2 Holmes, MH. Eur Heart J 2014: doi: / eur he ar tj /e ht 57 1 Go D, Nature Genetics 2013:45;; 1345 UW Preventive Cardiology Program Physicians: Lipid, Advanced Hypertension, or Preventive Cardiology Clinics EPIC order or call Exercise Prescription or Nutrition EPIC: Consult to Preventive Cardiology enter request in comments Call:
Lipid Therapy: Statins and Beyond. Ivan Anderson, MD RIHVH Cardiology
 Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Lipid Therapy: Statins and Beyond Ivan Anderson, MD RIHVH Cardiology Outline The cholesterol hypothesis and lipid metabolism The Guidelines 4 Groups that Benefit from Lipid therapy Initiation and monitoring
Cholesterol Treatment Update
 Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Cholesterol Treatment Update Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public Health Disclosure:
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Adult Certified Nurse Practitioner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
Vincent J. Caracciolo, MD FACC FOMA May 2014
 Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Vincent J. Caracciolo, MD FACC FOMA May 2014 Goals of the Guidelines National Heart, lung and Blood Institute ( NHLBI) collaborated with ACC/AHA to develop guidelines a.) assess CV risk, b.) lifestyle
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
2013 Cholesterol Guidelines. Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc.
 2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 Cholesterol Guidelines Anna Broz MSN, RN, CNP, AACC Cer=fied Adult Nurse Prac==oner North Ohio Heart, Inc. Disclosures Speaker Gilead Sciences NHLBI Charge to the Expert Panel Evaluate higher quality
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD
 2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
2013 ACC AHA LIPID GUIDELINE JAY S. FONTE, MD How do you interpret my blood test results? What are our targets for these tests? Before the ACC/AHA Lipid Guidelines A1c:
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Management of Post-transplant hyperlipidemia
 Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
Management of Post-transplant hyperlipidemia B. Gisella Carranza Leon, MD Assistant Professor of Medicine Lipid Clinic - Vanderbilt Heart and Vascular Institute Division of Diabetes, Endocrinology and
4/24/15. AHA/ACC 2013 Guideline Key Points
 Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Review of the ACC/AHA 2013 Guidelines Anita Ralstin, MS, CNS, CNP Next Step Health Consultant, LLC 1! Discuss the rationale for the change in lipid guidelines and how that affects the decision to implement
Lipid Panel Management Refresher Course for the Family Physician
 Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
Lipid Panel Management Refresher Course for the Family Physician Objectives Understand the evidence that was evaluated to develop the 2013 ACC/AHA guidelines Discuss the utility and accuracy of the new
2/10/2016. Perspectives on the 2013 ACC/AHA Cholesterol Guidelines. Disclosures. ATP-III Update 2004
 Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Perspectives on the 2013 ACC/AHA Cholesterol Guidelines Donald M. Lloyd-Jones, MD ScM Senior Associate Dean Chair and Professor of Preventive Medicine Northwestern Feinberg School of Medicine Disclosures
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon
 David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
David Y. Gaitonde, MD, FACP Endocrinology DDEAMC, Fort Gordon I have no actual or potential conflicts of interest in relation to this program or presentation. Raphael School of Athens, 1509-1511 Apply
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Disclosures. Overview 9/30/ ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
2013 ACC/AHA Guidelines on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults 2014 AAHP Fall Seminar Sherry Myatt, PharmD, BCPS Assistant Director of Pharmacy for
How to Handle Statin Intolerance in the High Risk Patient
 How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
How to Handle Statin Intolerance in the High Risk Patient Thomas D. Conley, MD FACC FSCAI Disclosures: None 1 Definition of High Risk Primary Prevention ASCVD Risk Calculator Adults >21 yrs, LDL 190 mg/dl
Lipid Management C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute
 Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Lipid Management 2018 C. Samuel Ledford, MD Interventional Cardiology Chattanooga Heart Institute Disclosures No Financial Disclosures Disclosures I am an Interventional Cardiologist I put STENTS in for
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Approach to Dyslipidemia among diabetic patients
 Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
Approach to Dyslipidemia among diabetic patients Farzad Hadaegh, MD, Professor of Internal Medicine & Endocrinology Prevention of Metabolic Disorders Research Center, Research Institute for Endocrine Sciences
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Hyperlipidemia and Cardiovascular Disease. Kathmandu November 2010 Harold E. Lebovitz, MD, FACE
 Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
Hyperlipidemia and Cardiovascular Disease Kathmandu November 21 Harold E. Lebovitz, MD, FACE Diabetes and Lifetime Risk for CHD Adjusted cummula ative incidence.7.6.5 Men 67% 3%.7.6.5 Women Diabetes No
UPDATES IN LIPID MANAGEMENT
 UPDATES IN LIPID 2017 Cardiovascular Symposium MANAGEMENT SUDHA RAVILLA, MD, DIPLOMATE, ABCL MEDICAL DIRECTOR CLINICAL LIPIDOLOGY TMHPP METABOLIC HEALTH CENTER INTRODUCTION CVD is STILL the No. 1 cause
UPDATES IN LIPID 2017 Cardiovascular Symposium MANAGEMENT SUDHA RAVILLA, MD, DIPLOMATE, ABCL MEDICAL DIRECTOR CLINICAL LIPIDOLOGY TMHPP METABOLIC HEALTH CENTER INTRODUCTION CVD is STILL the No. 1 cause
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Learning Objectives. Patient Case
 Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Joseph Saseen, Pharm.D., FASHP, FCCP, BCPS Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Learning Objectives Identify the 4 patient populations
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Disclosures. Prevention of Heart Disease: The New Guidelines. Summary of Talk. Four guidelines. No relevant disclosures.
 Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Disclosures Prevention of Heart Disease: The New Guidelines No relevant disclosures Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California
Cholesterol Management Roy Gandolfi, MD
 Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
Cholesterol Management 2017 Roy Gandolfi, MD Goals Interpreting cholesterol guidelines Cholesterol treatment in diabetics Statin use and side effects therapy Reporting- Comparison data among physicians
New Cholesterol Guidelines What the LDL are we supposed to do now?!
 New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
New Cholesterol Guidelines What the LDL are we supposed to do now?! Michael D. Shapiro Assistant Professor of Medicine and Radiology Knight Cardiovascular Institute Oregon Health & Science University 2013
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Lipid Management: A Case-Based Approach. Overview. Simple Lipid Therapy Approach. Patients have lipid disorders of:
 Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Lipid Management: A Case-Based Approach Patrick E. McBride, M.D., M.P.H. Professor of Medicine, Cardiovascular Medicine Associate Director, Preventive Cardiology Program UW School of Medicine and Public
Effective Treatment Options With Add-on or Combination Therapy. Christie Ballantyne (USA)
") Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
Effective Treatment Options With Add-on or Combination Therapy Christie Ballantyne (USA) Effective treatment options with add-on or combination therapy Christie M. Ballantyne, MD Center for Cardiovascular
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Prevention of Heart Disease: The New Guidelines
 Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
Prevention of Heart Disease: The New Guidelines Nisha I. Parikh MD MPH Assistant Professor of Medicine Division of Cardiology Department of Medicine University of California San Francisco May 18 th 2015
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman
 Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Making War on Cholesterol with New Weapons: How Low Can We/Should We Go? Shaun Goodman Disclosures Research grant support, speaker/consulting honoraria: Sanofi and Regeneron Including ODYSSEY Outcomes
Confusion about guidelines: How should we treat lipids?
 Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
Confusion about guidelines: How should we treat lipids? Anne Carol Goldberg, MD, FACP, FAHA, FNLA Professor of Medicine Washington University School of Medicine American College of Physicians Missouri
New Guidelines in Dyslipidemia Management
 The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Fourth IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2018 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
Advances in Lipid Management
 Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
Advances in Lipid Management Kavita Sharma, MD Assistant Professor of Medicine, Division of Cardiology Clinical Director of the Lipid Management Clinics, The Ohio State University Wexner Medical Center
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS
 ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
ACC/AHA GUIDELINES ON LIPIDS AND PCSK9 INHIBITORS Ziyad Ghazzal MD, FACC, FSCAI Professor of Medicine Deputy Vice President/Dean Associate Dean for Clinical Affairs American University of Beirut Adjunct
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
MANAGEMENT OF LIPID DISORDERS: WHERE DO WE STAND WITH THE NEW PRACTICE GUIDELINES? Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant financial relationships
Get a Statin or Not? Learning objectives. Presentation overview 4/3/2018. Treatment Strategies in Dyslipidemia Management
 Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Get a Statin or Not? Treatment Strategies in Dyslipidemia Management Michelle Chu, PharmD, BCACP, CDE Assistant Professor of Clinical Pharmacy, USC School of Pharmacy Sahar Dagher, PharmD Virtual Care
Copyright 2017 by Sea Courses Inc.
 Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Diabetes and Lipids Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic, electronic, or
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Lipids What s new? Meera Jain, MD Providence Portland Medical Center
 Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Lipids 2016- What s new? Meera Jain, MD Providence Portland Medical Center 1 Can I trust the ASCVD risk calculator? Do harms outweigh benefits in primary prevention? Is there anything besides a statin?
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Disclosures. Choosing a Statin/New Therapies. Case. How else would you do to treat him? LDL-C Reduction with Different Statin Strategies
 Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Disclosures I have no disclosures relevant to this talk Choosing a Statin/New Therapies Aryan Aiyer, MD Assistant Professor of Medicine University of Pittsburgh School of Medicine UPMC Heart and Vascular
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
New Guidelines in Dyslipidemia Management
 The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
The Third IAS-OSLA Course on Lipid Metabolism and Cardiovascular Risk Muscat, Oman, February 2017 New Guidelines in Dyslipidemia Management Dr. Khalid Al-Waili, MD, FRCPC, DABCL Senior Consultant Medical
An update on lipidology and cardiovascular risk management. Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine
 An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
An update on lipidology and cardiovascular risk management Lipids, Metabolism & Vascular Risk Section - Royal Society of Medicine National and international lipid modification guidelines: A critical appraisal
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2
 2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
2013 ACC/AHA Cholesterol Guidelines JULIE HAMMOND, D.O. PGY-2 MATTHEW PAOLI, D.O. PGY-2 GOALS ACC/AHA as publisher of guidelines Determining which patients are appropriate for statin therapy The treatment
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice
 Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
Lipid Management: The Next Level How Will the New ACC/AHA Guidelines Change My Practice Vera Bittner, MD, MSPH Professor of Medicine Section Head, Preventive Cardiology Medical Director, Cardiac Rehabilitation
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk?
 There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
There are many ways to lower triglycerides in humans: Which are the most relevant for pancreatitis and for CV risk? Michael Davidson M.D. FACC, Diplomate of the American Board of Lipidology Professor,
Pharmacy Drug Class Review
 Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Pharmacy Drug Class Review January 22, 2014 Authored By: Christina Manciocchi, Pharm.D. BCACP Disclaimer: Specific agents may have variations Edited By: Richard J. Kraft, Pharm.D.BCPS NEW CHOLESTEROL GUIDELINES
Treating Hyperlipidemias in Adults. Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC
 Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
Treating Hyperlipidemias in Adults Lisa R. Tannock MD Division of Endocrinology and Molecular Medicine, University of Kentucky Lexington KY VAMC Disclosures Conflicts: None Talk will address off-label
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction
 Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
Considerations and Controversies in the Management of Dyslipidemia for ASCVD Risk Reduction Pamela B. Morris, MD, FACC, FAHA, FASCP, FNLA Chair, ACC Prevention of Cardiovascular Disease Council The Medical
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment?
 What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
What Role do the New PCSK9 Inhibitors Have in Lipid Lowering Treatment? Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director, Prevention Intervention Center University
B. Patient has not reached the percentage reduction goal with statin therapy
 Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Managing Cardiovascular Risk: The Importance of Lowering LDL Cholesterol and Reaching Treatment Goals for LDL Cholesterol The Role of the Pharmacist Learning Objectives 1. Review the role of lipid levels
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go?
 Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Advanced Treatment of LDL: How Low Should You Go? C. Michael White, Pharm.D., FCP, FCCP Professor and Head, Pharmacy Practice, UCONN Co-Director, HOPE Collaborative Group, UCONN/Hartford Hospital Potential
Observations on US CVD Prevention Guidelines. Donald M. Lloyd-Jones, MD ScM FACC FAHA
 Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Observations on US CVD Prevention Guidelines Donald M. Lloyd-Jones, MD ScM FACC FAHA What are Guidelines? Evidence Base for Guidelines Tricoci, JAMA 2009 Evidence Base for Guidelines Tricoci, JAMA 2009
Non-Statin Lipid-Lowering Agents M Holler - Last updated: 10/2016
 Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Drug/Class Cholestyramine (Questran) Bile acid sequestrant Generic? Lipid Effects Y/N (monotherapy) Y LDL : 9% (4 g to 8 ; 21% (16 g to 20 ; 23% to 28% (>20 HDL : 4% to 8% (16 to 24 TG : 11% to 28% (4
Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist
 1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
1 Nicole Ciffone, MS, ANP-C, AACC Clinical Lipid Specialist New Cardiovascular Horizons Multidisciplinary Strategies for Optimal Cardiovascular Care February 7, 2015 2 Objectives After participating in
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Novel PCSK9 Outcomes. in Perspective: Lessons from FOURIER & ODYSSEY LDL-C. ASCVD Risk. Suboptimal Statin Therapy
 LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
LDL-C Novel PCSK9 Outcomes Suboptimal Statin Therapy ASCVD Risk in Perspective: Lessons from FOURIER & ODYSSEY Jennifer G. Robinson, MD, MPH Professor, Departments of Epidemiology & Medicine Director,
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults
 2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation,
2013 ACC/AHA Guideline on the Treatment of Blood Cholesterol to Reduce Atherosclerotic Cardiovascular Risk in Adults Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation,
What do the guidelines say about combination therapy?
 What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
What do the guidelines say about combination therapy? Christie M. Ballantyne, MD Center for Cardiovascular Disease Prevention Methodist DeBakey Heart & Vascular Center Baylor College of Medicine Houston,
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
1980 to 2000: Death rate fell from: 542.9 to 266.8 per 100K men 263.3 to 134.4 per 100K women 341,745 fewer deaths from CHD in 2000 Ford ES, NEJM, 2007 47% from CHD treatments, 44% from risk factor modification
Managing Dyslipidemia in Disclosures. Learning Objectives 03/05/2018. Speaker Disclosures
 Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Managing Dyslipidemia in 2018 Glen J. Pearson, BSc, BScPhm, PharmD, FCSHP, FCCS Professor of Medicine (Cardiology) Co-Director, Cardiac Transplant Clinic; Associate Chair, Health Research Ethics Boards;
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Conflict of Interest Disclosure. Learning Objectives. Learning Objectives. Guidelines. Update on Lifestyle Guidelines
 Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Conflict of Interest Disclosure Updates for the Ambulatory Care Pharmacist: Dyslipidemia and CV Risk Assessment No conflicts of interest to disclose 2014 Updates to the Updates in Ambulatory Care Pharmacy
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes
 Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
Effect of the PCSK9 Inhibitor Evolocumab on Cardiovascular Outcomes MS Sabatine, RP Giugliano, SD Wiviott, FJ Raal, CM Ballantyne, R Somaratne, J Legg, SM Wasserman, R Scott, MJ Koren, and EA Stein for
2/10/2016. Is it Time to Return to Cholesterol Goals for Optimal Patient Management? CON. Disclosures. Stipulations
 Is it Time to Return to Cholesterol Goals for Optimal Patient Management? CON Donald M. Lloyd-Jones MD ScMFACC FAHA Eileen M. FoellProfessor Chair, Dept. of Preventive Medicine Senior Associate Dean Director,
Is it Time to Return to Cholesterol Goals for Optimal Patient Management? CON Donald M. Lloyd-Jones MD ScMFACC FAHA Eileen M. FoellProfessor Chair, Dept. of Preventive Medicine Senior Associate Dean Director,
Case Discussions: Treatment Strategies for High Risk Populations. Most Common Reasons for Referral to the Baylor Lipid Clinic
 Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Case Discussions: Treatment Strategies for High Risk Populations Peter H. Jones MD, FNLA Associate Professor Methodist DeBakey Heart and Vascular Center Baylor College of Medicine Most Common Reasons for
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors
 to PCSK9 Inhibitors") Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
Evolving Concepts on Lipid Management from Ezetimibe (IMPROVE IT) to PCSK9 Inhibitors Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina at Chapel Hill
4 th and Goal To Go How Low Should We Go? :
 4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
4 th and Goal To Go How Low Should We Go? : Evaluating New Lipid Lowering Therapies Catherine Bourg Rebitch, PharmD, BCACP Clinical Associate Professor Disclosure The presenter has nothing to disclose
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID?
 Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Update On Diabetic Dyslipidemia: Who Should Be Treated With A Fibrate After ACCORD-LIPID? Karen Aspry, MD, MS, ABCL, FACC Assistant Clinical Professor of Medicine Warren Alpert Medical School of Brown
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation.
 Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Dyslipidemia: Lots of Good Evidence, Less Good Interpretation. G Michael Allan Evidence & CPD Program, ACFP Associate Professor, Dept of Family, U of A. CFPC CoI Templates: Slide 1 Faculty/Presenter Disclosure
Management of Lipid Levels and Cardiovascular Disease in HIV-Infected Individuals: Just Give Them a Statin?
 Perspective Management of Lipid Levels and Cardiovascular Disease in HIV-Infected Individuals: Just Give Them a Statin? Current guidelines for managing cholesterol to reduce cardiovascular disease (CVD)
Perspective Management of Lipid Levels and Cardiovascular Disease in HIV-Infected Individuals: Just Give Them a Statin? Current guidelines for managing cholesterol to reduce cardiovascular disease (CVD)
Young high risk patients the role of statins Dr. Mohamed Jeilan
 Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
Young high risk patients the role of statins Dr. Mohamed Jeilan KCS Congress: Impact through collaboration CONTACT: Tel. +254 735 833 803 Email: kcardiacs@gmail.com Web: www.kenyacardiacs.org Disclosures
LDL and the Benefits of Statin Therapy
 LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
LDL and the Benefits of Statin Therapy Allan Sniderman McGill University ACC/AHA did not recommend a target-based approach. Right? P 2899 The Expert Panel was unable to find any RCTs that evaluated titration
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making
 Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Dyslipidemia and Combination Therapy: A Framework for Clinical Decision Making Shashank Sinha, MD Pamela B. Morris, MD, FACC 8 October 2016 Mexico City Introduction: Pamela B. Morris, MD, FACC COMING TO
Lipids & Hypertension Update
 Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Lipids & Hypertension Update No financial disclosures Michael W. Cullen, MD, FACC Senior Associate Consultant, Assistant Professor of Medicine Mayo Clinic Department of Cardiovascular Diseases 34 th Annual
Disclosure. A New Partnership. Objectives 03/27/2014. What is the main way you have obtained information about the 2013 ACC/AHA Cholesterol Guideline?
 Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
Disclosure Lindsey Clark, PharmD, BCPS Cardiology-Medicine Pharmacy Specialist University of Cincinnati Medical Center April 10, 2014 I, Lindsey Clark, do not have a financial interest or affiliation with
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Guidelines for Screening and Management of Dyslipidemia
 PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
PIEDMONT ACCESS TO HEALTH SERVICES, INC. Policy Number: 01-09-021 SUBJECT: Guidelines for Screening and Management of Dyslipidemia EFFECTIVE DATE: 04/2008 REVIEWED/REVISED: 04/12/10, 03/17/2011, 4/10/2012,
Lipid Management 2013 Statin Benefit Groups
 Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Clinical Integration Steering Committee Clinical Integration Chronic Disease Management Work Group Lipid Management 2013 Statin Benefit Groups Approved by Board Chair Signature Name (Please Print) Date
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
Prospective Natural-History Study of Coronary Atherosclerosis
 Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything