Sphincter of Oddi Dysfunction: What s the Verdict in 2014?
|
|
|
- Rudolf Marshall
- 5 years ago
- Views:
Transcription

1 SGNA March 2014 Sphincter of Oddi Dysfunction: What s the Verdict in 2014? Evan L. Fogel, M.D. Professor of Clinical Medicine ERCP Fellowship Director Division of Gastroenterology/Hepatology Indiana University Hospital Indianapolis, Indiana
2 Disclosures Consultant: Cook Olympus Boston Scientific
3 Objectives Attendees will: be able to recognize how patients with suspected sphincter of Oddi dysfunction may present in clinical practice; gain an understanding of the appropriate evaluation and management of patients with postcholecystectomy abdominal pain; be able to explain the risks and potential benefits to patients undergoing ERCP with sphincter of Oddi manometry (SOM).
4 OUTLINE sphincter of Oddi dysfunction: definition case presentation manometry outcomes


5 Sphincter of Oddi regulates flow of bile/pancreas enzymes into duodenum maintains sterile intraductal milieu

6 Major Papilla

7 Cannulation Biliary Pancreatic
8 Sphincter of Oddi Dysfunction (SOD) an abnormality of SO contractility it is a benign, noncalculous, relative obstruction to flow of bile or pancreatic juice through the pancreatobiliary junction most common in young women may be manifested clinically by pancreaticobiliary pain, pancreatitis, abnormal LFTs, or abnormal pancreatic enzymes



9 Case: 30-year-old woman with RUQ pain six-month history constant discomfort, rated 2/10, with intermittent attacks of debilitating pain, identical to pain prior to cholecystectomy last year ( wasn t functioning ) pain lasts minutes, radiates to upper back, associated with nausea/vomiting
10 Past medical history: cholecystectomy, otherwise negative Physical exam: upper abdominal tenderness, otherwise unremarkable ER visit: AST 82 (normal < 45), ALT 90 (<40), alkaline phosphatase 150 (<125), bilirubin 0.6 (<1.0), amylase 100 (< 89), lipase 60 (< 51) all return to normal when pain-free CT scan unremarkable normal pancreas and biliary tree

11 referred to a local gastroenterologist EGD normal what is your next step in the diagnostic evaluation of this patient?
12 post-cholecystectomy pain resembling the patient s pre-operative biliary colic occurs in at least 10-20% of patients Here, the pain is similar to gallbladder-type pain, with mildly elevated LFTs, amylase/lipase suggestive of pancreaticobiliary origin
 chronic pancreatitis (scarring/fibrosis) sphincter of Oddi dysfunction")
13 Chronic abdominal pain of pancreaticobiliary origin Consider: structural causes of biliary and pancreatic ductal obstruction (stones, tumors, strictures) chronic pancreatitis (scarring/fibrosis) sphincter of Oddi dysfunction (SOD)
14 Initial evaluation History, physical examination Labs: LFTs, amylase and/or lipase (during an attack of pain) Imaging: ultrasound and/or CT scan
15 Consider MRI/MRCP or endoscopic ultrasound (EUS) if available may detect pathology (stones, sludge, chronic pancreatitis, tumors) not visualized by other modalities
16 MRCP pancreatic duct bile duct


17 MRCP Proceed with ERCP! EUS


18 Chronic Pancreaticobiliary Pain What do I do when the MRCP and EUS are normal?

19 Chronic pancreaticobiliary pain: normal MRCP The residual group of patients has a high frequency of SOD bile duct pancreatic duct
20 SOD Evaluation: Non-Invasive vs Invasive

21 Non-invasive Evaluation cholescintigraphy (nuclear med scan) secretin-mrcp, secretin-eus Not sensitive miss too many cases of SOD Not specific suggest SOD when it isn t there!
22 Diagnostic Evaluation Invasive tests ERCP - provides structural evaluation of the pancreatic duct and bile duct Sphincter of Oddi manometry directly assesses pressure profile of the sphincter of Oddi
23 Indications for SOM 2013 Unexplained, disabling pancreaticobiliary pain LFT and/or pancreatic enzyme abnormalities Idiopathic pancreatitis
24 IU Sphincter of Oddi Manometry (SOM): SOM 5352 pts Abnormal SOM 3520 (65%) Normal/Equivocal SOM 1832 (35%)
25 SOD: Classification Type Biliary/Pancreatic pain abnormal labs duct dilation Objective evidence Some objective evidence No objective evidence I II III + - -
26 OK, we re going to proceed with ERCP / SOM! How do we do it?
27 SOM Procedure Overview requires special equipment requires a cooperative, motionless patient a physician-driven procedure (failed cannulation failed SOM) requires a knowledgeable, skilled endoscopist and an experienced manometrist to perform a successful study requires constant communication and teamwork computer and software program for SOM to view waveform
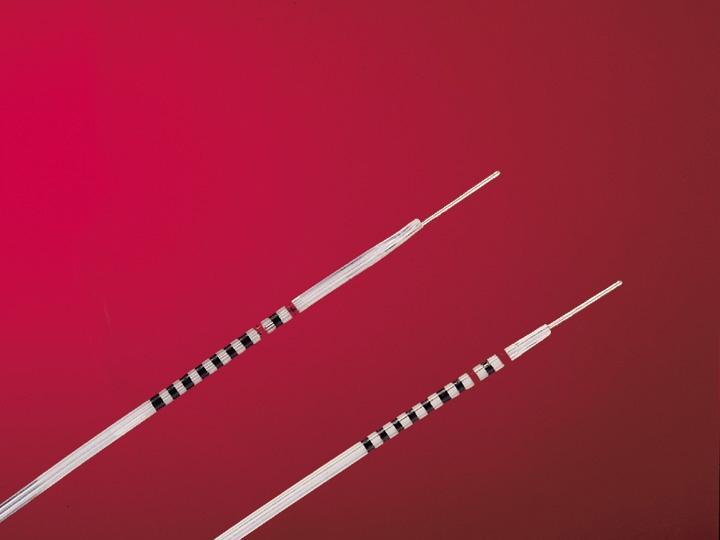
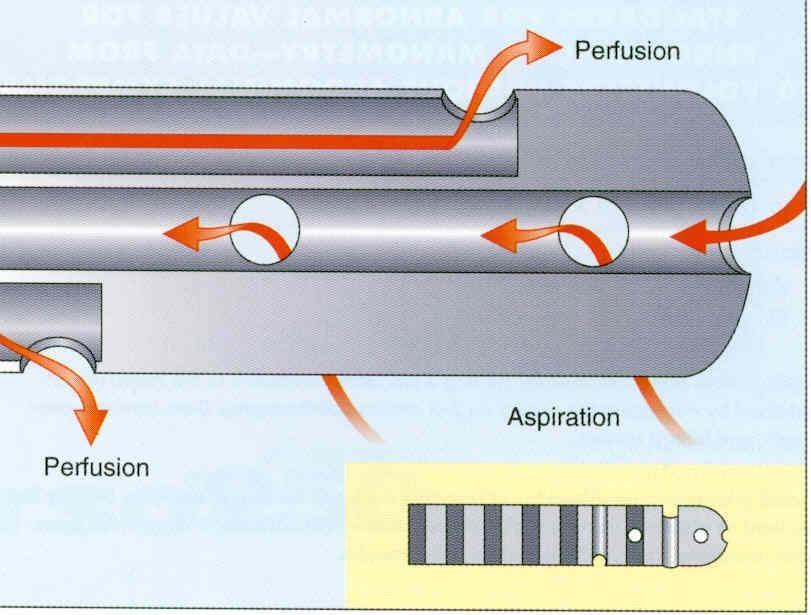
28 EQUIPMENT Water-perfused probe ( Lehman catheter )
29 SOM Procedure the manometry catheter is advanced through the scope to the duodenum -- the duodenal baseline pressure is set to zero the pancreatic/bile duct is cannulated the catheter is withdrawn one band at a time when a high-pressure zone is found, the pressure is recorded for 30 seconds basal pressure must be elevated in both recording leads for a diagnosis of SOD

30 Manometry Tracing
31 Aim of Therapy for SOD: Reduce Resistance to Flow of Bile or Pancreatic Juice Medical Surgical Endoscopic
32 Aim of Therapy for SOD: Reduce Resistance to Flow of Bile or Pancreatic Juice Medical - antispasmodics (smooth muscle relaxants, calcium channel blockers) - PPIs, tricyclic anti-depressants
33 Aim of Therapy for SOD: Reduce Resistance to Flow of Bile or Pancreatic Juice Medical Surgical Endoscopic Sphincterotomy (cutting the muscle) Botulinum toxin injection Dilation Stent
 in SOD?")
34 What is the long-term outcome after biliary sphincterotomy (BES) in SOD?
 12 Thatcher/1987 15 15 (100) 28 Boender/1992 24 18 (77) 12.")
35 Long-term Outcome after BES: Type I SOD Author/year n n Improved (%) Mean follow-up (months) Rosenblatt/ (82) 57.6 Cicala/ (100) 12 Thatcher/ (100) 28 Boender/ (77) 12.5 Sherman/ (82) 24 TOTAL (85) 25.2
36 Long-term Outcome after BES: Type II SOD Author/year n n Improved (%) Mean follow-up (months) Rosenblatt, (73) 57.6 Pereira, (88) 35.1 Cicala, (88) 13 *Toouli, (85) 24 Thatcher, (47) 20 *Geenen, (94) 48 *Sherman, (83) 39.6 Botoman, (60) 36 Wehrmann, (59) 30 Linder, (40) 18.1 Bozkurt, (64) 32.5 TOTAL (70) 36.8 *Randomized controlled trial
37 Long-term Outcome after BES: Type III SOD Author/year n n Improved (%) Mean follow-up (months) Rosenblatt, (28) 57.6 Pereira, (18) 30.2 Wehrmann, (50) 15 *Sherman, (62) 40 Botoman, (55) 36 Wehrmann, (8) 30 Linder, (40) 18 Bozkurt, (33) 36.4 TOTAL (37) 34.7 *RCT
38 Causes for Persistent Symptoms after Biliary Sphincterotomy in SOD Residual or recurrent biliary SOD Pancreatic SOD Chronic pancreatitis Other untreated pancreaticobiliary disease Non-pancreaticobiliary diseases especially gut motility disorders

39 Does the addition of a pancreatic sphincterotomy to biliary sphincterotomy in SOD patients improve outcome?
 Mean follow-up (months)")
 16 Elton,1998 43 31 (72) 36.")
40 Symptomatic Improvement in Pancreatic SOD Patients after Pancreatic Sphincterotomy Author/year n n Improved (%) Mean follow-up (months) Pereira, (54) 30.2 Okolo, (73) 16 Elton, (72) 36.4 Soffer, (64) 13.7 Guelrud, (81) 14.7 TOTAL (71) 23.9
41 Role for ERCP and SOM? 2013 SOD Type ERCP SOM I Yes Not necessary II Yes Highly recommended III Yes Mandatory

42 SOD Approximately 60-80% achieve benefit from sphincterotomy Mostly small, retrospective studies Little prospective data in Type III patients High complications rates (10-20% PEP)
43 NIH State of the Science Conference: ERCP - diagnosis and management of Type III SOD patients are most difficult - invasive procedures should be delayed or avoided if possible the risk of complications exceeds potential benefit in many cases - ERCP with SOM and sphincterotomy should ideally be performed at specific referral centers and in randomized controlled trials.. Cohen GIE 2002


44 Evaluating Predictors & Interventions in Sphincter of Oddi Dysfunction: The EPISOD Trial






45 EPISOD Medical University of South Carolina Indiana University Virginia Mason University of Minnesota Dallas Yale University St. Louis
46 Study Design - a multi-center, randomized, sham-controlled study - designed to assess the value of sphincterotomy as treatment in SOD III - likelihood of finding SOD (by SOM) in these patients approaches 66% -- need 2:1 randomization in favor of treatment - assuming a 30% placebo (sham) response rate, and 60% treatment response rate, 214 subjects required
47 RAPID Score (Recurrent Abdominal Pain Intensity and Disability) modeled after migraine research captures, in past 3 months, days lost due to abdominal pain in 3 domains: work household activities social/leisure activities Durkalski, et al, WJG 2010
48 RAPID score Grade 1: 0-5 days missed (little or no disability) Grade 2: 6-10 days (mild disability) Grade 3: days (moderate disability) Grade 4: >21 days (severe disability) Minimum score for eligibility: 11 days missed
49 Primary outcome sphincterotomy will result in a higher success rate than the sham intervention Success (definition): Grade 1 disability as measured using the RAPID scale at months 9 and 12 post-randomization no referral for possible re-intervention during the follow up period no prescription analgesic use during months 10, 11 and 12 unless prescribed for pain other than abdominal pain (and then no more than 14 days)
50 Secondary Outcomes Is there an association between manometry result and treatment outcome? does addition of a pancreatic sphincterotomy improve outcome in patients with pancreatic sphincter hypertension (PSH)?
51 Primary outcome Treatment Number Success Sphincterotomy (22.0%) Sham (35.6%) p-value 0.03
52 Secondary outcome Treatment Number Success Biliary Sphincterotomy (19.1%) Pancreatic and Biliary (Dual) Sphincterotomy (27.7%) Sham (35.6%)
53 Median change in RAPID (days): Biliary=33 Dual=53 Sham=38
54 Success criteria too strict? Reducing the pain burden by half Treatment Number Success Biliary sphincterotomy (32%) Dual sphincterotomy (45%) Sham (44%)

55 Manometry data Panc and Bil both abnormal 35% P abnormal, B normal 21% P abnormal, B not measured 9% 65% Panc abnormal B abnormal, P normal 11% Both normal 24%
56 Does manometry predict success? Manometry Number Success Pancreas Biliary Biliary sph Dual sph Sham any 137 8/50 (16%) 11/44 + NO! 12/43 (25%) (28%) any /39(18%) 7/29(24%) 7/30(23%) - - or? 52 5/30 (17%) 1/1 12/21 (57%)
57 Potential criticisms Wrong subjects? Wrong definition of success? too strict wrong pain assessment tool (RAPID) Inadequate sphincterotomies?
58 Too strict? Rates higher, but patterns the same with 50% reduction in RAPID 25% reduction in RAPID excluding the narcotics reason using re-intervention only
59 Wrong pain tool? RAPID measured pain-related disability Same results using SF 36 pain scores
60 SF 36 pain assessment Treatment Disability Baseline Months Biliary Pain; Moderate, severe, very severe 88% 44% Work interference; extreme, quite a bit 51% 16% Dual Pain; Moderate, severe, very severe 89% 36% Work interference; extreme, quite a bit 38% 6% Sham Pain; Moderate, severe, very severe 91% 32% Work interference; extreme, quite a bit 31% 10%
61 Conclusions sphincterotomy is not better than a sham procedure in Type III SOD, and manometry is NOT helpful in predicting treatment response these results should eliminate the use of ERCP in these patients, and thereby prevent many attacks of pancreatitis
62 Conclusions Further studies of the source of pain are needed in SOD III, with careful evaluation of other treatment options behavioral and neuromodulator therapies Should we discard the term SOD type III, to divert attention away from the sphincter?
63 Questions Are the results all due to placebo? Was our sham arm (ERCP/manometry/stent) actually therapeutic? Would a no-touch blinded endoscopy have the same effect? Why did sphincterotomy patients do less well? How will GI docs and SOD patients respond? Half the patients did get half better Will patients keep coming? Would the patients do it again? Re-do Type IIIs?

64 Indications for SOM: 2013 Unexplained, disabling pancreaticobiliary pain LFT and/or pancreatic enzyme abnormalities Idiopathic pancreatitis
 Pancreas divisum Stone, Stricture Miscellaneous testing Genetics Empiric cholecystectomy")
65 Defining idiopathic recurrent acute pancreatitis (IRAP) H&P Alcohol Medications Trauma Family history Calcium Triglycerides Liver tests Laboratory Imaging Tumors (PDAC, IPMN) Pancreas divisum Stone, Stricture Miscellaneous testing Genetics Empiric cholecystectomy Microcrystals
66 ERCP for diagnosis and treatment The diagnostic yield of ERCP (ductography alone) ranges from 32-80% Elevated basal sphincter pressure has been reported in 30-65% of patients with idiopathic AP Is this cause or effect? The therapeutic role of sphincterotomy is debated
67 IRAP and SOD: Therapy Results of SOM predict outcome from sphincter ablation limited data no long-term F/U small sample size no randomized controlled trials no outcome data of empiric sphincterotomy without SOM
68 IRAP and SOD: Prospective Randomized Trial Coté et al. Gastro 2012;143:1502-9
69 Enrollment criteria Inclusion Idiopathic recurrent acute pancreatitis (IRAP) two or more episodes ERCP with SOM planned Exclusion Chronic pancreatitis Cross sectional imaging Pancreatogram Pancreas divisum Alternate etiology identified (e.g., CBD stone, mucinous tumor) Inability to perform pancreatic manometry Pregnancy, age < 18, incarceration Inability to provide informed consent


70 Randomization ERCP with pancreatic SOM Elevated ( 40mmHg) basal pancreatic sphincter pressure Normal basal biliary and pancreatic sphincter pressure Biliary sphincterotomy Sham Biliary + Pancreatic sphincterotomy 1:1 Biliary sphincterotomy



71 Study Aims Primary Measure the incidence of recurrent acute pancreatitis (RAP) post-ercp Secondary Interval development of chronic pancreatitis Results and impact of repeat ERCP, if performed
 Screen failure (n=50,")
 Other")

 BES (n=33) DES")
72 Enrollment: 9/1997-8/2011 RAP (n=139) Screen failure (n=50, 36%) Pancreas divisum (n=17) Chronic pancreatitis (n=12) Other (CBD stone, IPMN) (n=21) Preliminary data Elevated pancreatic SOM (n=69, 78%) Normal SOM (n=20, 22%) BES (n=33) DES (n=36) Sham (n=9) BES (n=11)
 Coté et al.")
73 IARP: RCT of biliary sphincterotomy vs biliary+panc sphincterotomy for Pancreatic SOD (f/u 7 years) Coté et al. Gastro 2012
74 Development of chronic pancreatitis Variable Normal SOM Sham (n=9) BES (n=11) P Pancreatic SOD BES (n=33) DES (n=36) P Median followup (months) 85 (72, 108) 36 (22, 73) < (36, 108) 86 (33.5, 108) 0.98 Chronic pancreatitis % % (11.1%) (27.3%) (18.2%) (13.9) %
75 Repeat ERCP during follow-up 43% of patients underwent a repeat ERCP normal SOM (32%) and pancreatic SOD (46%) pancreatic sphincterotomy performed (initial or repeat) in 76% of patients RAP occurred (again) after repeat ERCP in 68%
76 SOD in IRAP pancreatic SOD represents an independent predictor of future AP episodes, but does not necessarily predict the development of CP among patients with pancreatic SOD, pancreatic sphincterotomy affords no added benefit to biliary sphincterotomy alone the role of ANY sphincter therapy remains unclear
77 Conclusions: ERCP in irap among patients with normal SOM, empiric BES may not impact on natural history in all patients with IRAP, the interval development of chronic pancreatitis is notable (16.9%)
78 Conclusion: ERCP and SOM What s the final word in 2014?
79 Role for ERCP and SOM? 2013 SOD Type ERCP SOM I Yes Not necessary II Yes Highly recommended III Yes Mandatory
80 Role for ERCP and SOM? 2014 SOD Type ERCP SOM I Yes Not necessary II Yes Highly recommended III No No
81 SOM in IARP SOD is commonly identified in patients with IARP when detailed endoscopic evaluation is done the best therapy awaits further study at present, the role of sphincter therapy remains unclear

82 2014




83 IU ERCP 83
84 Thank-you!
Sphincter of Oddi Dysfunction: Where do we stand in 2015?
 IU GI Motility Conference August 5, 2015 Sphincter of Oddi Dysfunction: Where do we stand in 2015? Evan L. Fogel, M.D. Professor of Medicine ERCP Fellowship Director Division of Gastroenterology/Hepatology
IU GI Motility Conference August 5, 2015 Sphincter of Oddi Dysfunction: Where do we stand in 2015? Evan L. Fogel, M.D. Professor of Medicine ERCP Fellowship Director Division of Gastroenterology/Hepatology
Sphincter of Oddi dysfunction: SOD after EPISOD, Now what do we do?
 Sphincter of Oddi dysfunction: SOD after EPISOD, Now what do we do? Priya A. Jamidar, M.D., FASGE Professor of Medicine, Director of Endoscopy Yale School Y A L E S CH OO L O F MEDIC IN E February in Connecticut
Sphincter of Oddi dysfunction: SOD after EPISOD, Now what do we do? Priya A. Jamidar, M.D., FASGE Professor of Medicine, Director of Endoscopy Yale School Y A L E S CH OO L O F MEDIC IN E February in Connecticut
Does Sphincter of Oddi Dysfunction Even Exist Anymore?
 Does Sphincter of Oddi Dysfunction Even Exist Anymore? Grace H. Elta, MD, FACG Professor of Medicine University of Michigan Sphincter of Oddi Dysfunction Best studied clinical association: Biliary pain
Does Sphincter of Oddi Dysfunction Even Exist Anymore? Grace H. Elta, MD, FACG Professor of Medicine University of Michigan Sphincter of Oddi Dysfunction Best studied clinical association: Biliary pain
Figure 2: Post-cholecystectomy biliary-like pain
 Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
Figure 2: Post-cholecystectomy biliary-like pain 1 patient with recurrent episodes of pain (not daily), in the epigastrium/right upper quadrant, lasting >30 mins, building to a steady level, interrupting
stents she/he is providing appropriate or inappropriate care?
 Pancreatic Stents Are They Now State of the Art Care? To Help Limit Post ERCP Pancreatitis Glen A. Lehman, M.D. Professor of Medicine and Radiology Division of Gastroenterology/Hepatology Indiana University
Pancreatic Stents Are They Now State of the Art Care? To Help Limit Post ERCP Pancreatitis Glen A. Lehman, M.D. Professor of Medicine and Radiology Division of Gastroenterology/Hepatology Indiana University
Sphincter of Oddi Dysfunction Type III, Manometry and Sphincterotomy: Sham Won, Game Over
 Sphincter of Oddi Dysfunction Type III, Manometry and Sphincterotomy: Sham Won, Game Over C. Mel Wilcox, M.D., M.S.P.H. Professor of Medicine, Surgery and Pediatrics University of Alabama, Birmingham Basil
Sphincter of Oddi Dysfunction Type III, Manometry and Sphincterotomy: Sham Won, Game Over C. Mel Wilcox, M.D., M.S.P.H. Professor of Medicine, Surgery and Pediatrics University of Alabama, Birmingham Basil
Case Report (1) Sphincter of Oddi Dysfunction. Case Report (3) Case Report (2) Case Report (4) Case Report (5)
 Sphincter of Oddi Dysfunction. Case Report (3) Case Report (2) Case Report (4) Case Report (5)") Dr David Westaby Imperial NHS Trust Imperial College Medical School London Case Report (1)! TD 33yr old male! Feb May 2010: Recurrent episodes of abdominal pain! June 2010 Episode severe abdominal pain
Dr David Westaby Imperial NHS Trust Imperial College Medical School London Case Report (1)! TD 33yr old male! Feb May 2010: Recurrent episodes of abdominal pain! June 2010 Episode severe abdominal pain
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine
 Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
Chronic Pancreatitis: When to Scope? Gregory A. Cote, MD, MS Assistant Professor of Medicine Indiana University School of Medicine Endoscopy & Chronic Pancreatitis Diagnosis EUS ERCP Exocrine Function
SPHINCTER OF ODDI DYSFUNCTION (SOD)
") SPHINCTER OF ODDI DYSFUNCTION (SOD) Sphincter of Oddi dysfunction refers to structural or functional disorders involving the biliary sphincter that may result in impedance of bile and pancreatic juice
SPHINCTER OF ODDI DYSFUNCTION (SOD) Sphincter of Oddi dysfunction refers to structural or functional disorders involving the biliary sphincter that may result in impedance of bile and pancreatic juice
7/11/2017. We re gonna help a lot of people today. Biliary/Pancreatic Endoscopy. AGS July 1-2, Kenneth M. Sigman, MD
 Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
Biliary/Pancreatic Endoscopy AGS July 1-2, 2017 Kenneth M. Sigman, MD We re gonna help a lot of people today 1 2 3 4 Cannulation It all starts with cannulation Double Wire Cannulation Difficult cannulations
ERCP and EUS: What s New and What Should We Do?
 ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
ERCP and EUS: What s New and What Should We Do? Rajesh N. Keswani, MD Associate Professor of Medicine Division of Gastroenterology Northwestern University Feinberg School of Medicine EUS/ERCP in 2015 THE
Making ERCP Easy: Tips From A Master
 Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
Making ERCP Easy: Tips From A Master Raj J. Shah, M.D., FASGE Associate Professor of Medicine University of Colorado School of Medicine Co-Director, Endoscopy Director, Pancreaticobiliary Endoscopy Services
The role of ERCP in chronic pancreatitis
 The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
The role of ERCP in chronic pancreatitis Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Results III. Results IV
 Comparing Polyp And Cancer Detection Rate Between Asymptomatic Patients With A Positive Family History Of Colon Cancer Or Polyps And Asymptomatic Patients Of A Similar Age Range Who Have Average Risk Of
Comparing Polyp And Cancer Detection Rate Between Asymptomatic Patients With A Positive Family History Of Colon Cancer Or Polyps And Asymptomatic Patients Of A Similar Age Range Who Have Average Risk Of
Pain a&er cholecystectomy Naviga4ng a clinical minefield
 Pain a&er cholecystectomy Naviga4ng a clinical minefield Peter B Co9on MD, FRCP, FRCS Professor of Medicine Diges4ve Disease Center Medical University of South Carolina 1 Diges4ve Disease Center Pa4ent-
Pain a&er cholecystectomy Naviga4ng a clinical minefield Peter B Co9on MD, FRCP, FRCS Professor of Medicine Diges4ve Disease Center Medical University of South Carolina 1 Diges4ve Disease Center Pa4ent-
Overview. Doumit S. BouHaidar, MD ACG/VGS/ODSGNA Regional Postgraduate Course Copyright American College of Gastroenterology 1
 Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
Doumit S. BouHaidar, MD Associate Professor of Medicine Director, Advanced Therapeutic Endoscopy Virginia Commonwealth University Overview Copyright American College of Gastroenterology 1 Incidence: 4
Acute Pancreatitis. Case: NG. Idiopathic Pancreatitis is Common. Investigation and Management of Idiopathic Acute Recurrent Pancreatitis (IARP)
") BRIGHAM AND WOMENS HOSPITAL Investigation and Management of (IARP) Acute Pancreatitis j Darwin L. Conwell MD, MS Associate Professor of Medicine Harvard Medical School Boston, MA Case: NG 54 year old female
BRIGHAM AND WOMENS HOSPITAL Investigation and Management of (IARP) Acute Pancreatitis j Darwin L. Conwell MD, MS Associate Professor of Medicine Harvard Medical School Boston, MA Case: NG 54 year old female
A patient with an unusual congenital anomaly of the pancreaticobiliary tree
 A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
A patient with an unusual congenital anomaly of the pancreaticobiliary tree Thomas Hocker, HMS IV BIDMC Core Radiology Case Presentation September 17, 2007 Review of Normal Pancreaticobiliary Tract Anatomy
6/17/2016. ERCP in June 26, Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates
 ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
ERCP in 2016 June 26, 2016 Kenneth M. Sigman, M.D. Birmingham Gastroenterology Associates 1 2 3 Diagnostic/Therapeutic ERCP Biliary Obstruction Benign stricture Malignant Stones Ductal injuries Cholangitis
Tools of the Gastroenterologist: Introduction to GI Endoscopy
 Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Tools of the Gastroenterologist: Introduction to GI Endoscopy Objectives Endoscopy Upper endoscopy Colonoscopy Endoscopic retrograde cholangiopancreatography (ERCP) Endoscopic ultrasound (EUS) Endoscopic
Magnetic resonance cholangiopancreatography (MRCP) is an imaging. technique that is able to non-invasively assess bile and pancreatic ducts,
 is an imaging. technique that is able to non-invasively assess bile and pancreatic ducts,") SECRETIN AUGMENTED MRCP Riccardo MANFREDI, MD, MBA, FESGAR Magnetic resonance cholangiopancreatography (MRCP) is an imaging technique that is able to non-invasively assess bile and pancreatic ducts, in
SECRETIN AUGMENTED MRCP Riccardo MANFREDI, MD, MBA, FESGAR Magnetic resonance cholangiopancreatography (MRCP) is an imaging technique that is able to non-invasively assess bile and pancreatic ducts, in
ERCP complications and challenges in their diagnosis and management.
 ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
ERCP complications and challenges in their diagnosis and management. Sandie R Thomson Chair of the Division of Gastroenterology, University of Cape Town ERCP Do I have a good Indication? . Algorithm for
Disclosures. Overview. Case 1. Common Bile Duct Sizes 10/14/2016. General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis
 Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
Disclosures General GI + Advanced Endoscopy: NAFLD/Stones/Pancreatitis 123 Blank Blank, LLC Aldo Maspons, MD Assistant Professor Director of Endoscopy Department of Pediatrics Texas Tech University Health
The campaign on laboratory: focus on Gallstone Disease and ERCP
 The campaign on laboratory: focus on Gallstone Disease and ERCP Mauro Giuliani, MD, Specialist in Visceral Surgery, Vice Head Physician, Surgical Ward, Ospedale Regionale di Locarno Alberto Fasoli, MD,
The campaign on laboratory: focus on Gallstone Disease and ERCP Mauro Giuliani, MD, Specialist in Visceral Surgery, Vice Head Physician, Surgical Ward, Ospedale Regionale di Locarno Alberto Fasoli, MD,
Case 1- B.N. 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids.
 Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
Case 1- B.N 66 yr old F with PMHx of breast cancer s/ p mastectomy, HTN, DM presented with dysphagia to solids and liquids. Reports retching to clear esophagus. Case 1- B.N EGD: Stricture in the distal
The Bile Duct (and Pancreas) and the Physician
 and the Physician") The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
The Bile Duct (and Pancreas) and the Physician Javaid Iqbal Consultant in Gastroenterology and Pancreato-biliary Medicine University Hospital South Manchester Not so common?! Two weeks 38 ERCP s 20 15
GASTROENTEROLOGY ESSENTIALS
 GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
GASTROENTEROLOGY ESSENTIALS Practical Gastroenterology 8/25/2018 Jahnavi Koppala, MBBS Abdullah Abdussalam, MD A 48-year-old male was evaluated for noncardiac chest pain. Treatment with PPI twice daily
Manometry based randomised trial of endoscopic sphincterotomy for sphincter of Oddi dysfunction
 98 GI Surgical Unit, Flinders Medical Centre, Adelaide, Australia J Toouli I C Roberts-Thomson G T P Saccone P Jeans MCox P Anderson C Worthley N Shanks A Craig Department of Gastroenterology, Royal North
98 GI Surgical Unit, Flinders Medical Centre, Adelaide, Australia J Toouli I C Roberts-Thomson G T P Saccone P Jeans MCox P Anderson C Worthley N Shanks A Craig Department of Gastroenterology, Royal North
Endoscopic Ultrasonography Clinical Impact. Giancarlo Caletti. Gastroenterologia Università di Bologna. Caletti
 Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Clinical Impact Giancarlo Gastroenterologia Università di Bologna AUSL di Imola,, Castel S. Pietro Terme (BO) 1982 Indications Diagnosis of Submucosal Tumors (SMT) Staging of Neoplasms Evaluation of Pancreato-Biliary
Treatment of chronic calcific pancreatitis endoscopy versus surgery
 Treatment of chronic calcific pancreatitis endoscopy versus surgery 35 - year old ladypresented to LPC Mumbai with intermittent abdominal pain. Pain was intermittent, colicky, more in epigastrium and periumbilical
Treatment of chronic calcific pancreatitis endoscopy versus surgery 35 - year old ladypresented to LPC Mumbai with intermittent abdominal pain. Pain was intermittent, colicky, more in epigastrium and periumbilical
Chronic pancreatitis is a fibroinflammatory disease of the
 Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
Session 2C: Pancreaticobiliary Disease CHRONIC PANCREATITIS: WHEN TO SCOPE? Gregory A. Coté, MD, MS Chronic pancreatitis is a fibroinflammatory disease of the pancreas that presents with several distinct
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/27/2011 Radiology Quiz of the Week # 35 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 8/27/2011 Radiology Quiz of the Week # 35 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Endoscopic Retrograde Cholangiopancreatography (ERCP)
") Endoscopic Retrograde Cholangiopancreatography (ERCP) Medical Imaging and Treatment of the Bile and Pancreatic Ducts CIE-02718 Understanding ERCP Brochure Update_F.indd 1 7/11/18 9:51 A Minimally Invasive
Endoscopic Retrograde Cholangiopancreatography (ERCP) Medical Imaging and Treatment of the Bile and Pancreatic Ducts CIE-02718 Understanding ERCP Brochure Update_F.indd 1 7/11/18 9:51 A Minimally Invasive
Clinical outcomes and nonendoscopic interventions after minor papilla endotherapy in patients with symptomatic pancreas divisum
 ORIGINAL ARTICLE: Clinical Endoscopy Clinical outcomes and nonendoscopic interventions after minor papilla endotherapy in patients with symptomatic pancreas divisum Lyssa N. Chacko, MD, Yang K. Chen, MD,
ORIGINAL ARTICLE: Clinical Endoscopy Clinical outcomes and nonendoscopic interventions after minor papilla endotherapy in patients with symptomatic pancreas divisum Lyssa N. Chacko, MD, Yang K. Chen, MD,
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital
 in a District General Hospital") Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
Magnetic Resonance Cholangiopancreatography (MRCP) in a District General Hospital Poster No.: C-1790 Congress: ECR 2012 Type: Authors: Scientific Exhibit J. A. Maguire 1, H. Kasem 2, M. Akhtar 2, M. Strauss
sphincter of Oddi dysfunction. Management often involves endoscopic retrograde cholangiopancreatography (ERCP) with manometry and sphincterotomy.
 with manometry and sphincterotomy.") Research Original Investigation Effect of Endoscopic Sphincterotomy for Suspected Sphincter of Oddi Dysfunction on Pain-Related Disability Following Cholecystectomy The EPISOD Randomized Clinical Trial
Research Original Investigation Effect of Endoscopic Sphincterotomy for Suspected Sphincter of Oddi Dysfunction on Pain-Related Disability Following Cholecystectomy The EPISOD Randomized Clinical Trial
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013
 Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Surgical Management of Chronic Pancreatitis VERENA LIU, MD KINGS COUNTY HOSPITAL CENTER SURGERY GRAND ROUNDS 4/1/2013 Case Report 42F with h/o chronic pancreatitis due to alcohol use with chronic upper
Controversies in the management of acute pancreatitis
 Kathmandu University Medical Journal (3) Vol., No. 3, Issue 7, 3-7 Controversies in the management of acute pancreatitis Singh DR 1, Mehta A, Dangol UMS 3 1 Lecturer, Medical Officer, 3 Lecturer, Dept.
Kathmandu University Medical Journal (3) Vol., No. 3, Issue 7, 3-7 Controversies in the management of acute pancreatitis Singh DR 1, Mehta A, Dangol UMS 3 1 Lecturer, Medical Officer, 3 Lecturer, Dept.
Prof. (DR.) MD. ISMAIL PATWARY. MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet
 MD. ISMAIL PATWARY. MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet") Prof. (DR.) MD. ISMAIL PATWARY MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet CHRONIC PANCREATITIS Defined as a progressive inflammatory
Prof. (DR.) MD. ISMAIL PATWARY MBBS, FCPS, MD, FACP, FRCP(Glasgow, Edin) Professor, Dept. of Medicine, Sylhet women s Medical College, Sylhet CHRONIC PANCREATITIS Defined as a progressive inflammatory
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation
 and Endoscopic Ultrasound correlation") Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Pictorial review of Benign Biliary tract abnormality on MRCP/MRI Liver with Endoscopic (including splyglass) and Endoscopic Ultrasound correlation Poster No.: C-2617 Congress: ECR 2015 Type: Educational
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Lutheran Medical Center. Daniel H. Hunt, M.D. June 10 th, 2005
 Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
Lutheran Medical Center Daniel H. Hunt, M.D. June 10 th, 2005 History xx y.o. pt with primary CBD stones s/p ERCP xx months earlier for attempted stone extraction resulting in post ERCP pancreatitis. Patient
SOD (Sphincter of Oddi Dysfunction)
") SOD (Sphincter of Oddi Dysfunction) SOD refers to the mechanical malfunctioning of the Sphincter of Oddi, which is the valve muscle that regulates the flow of bile and pancreatic juice into the duodenum.
SOD (Sphincter of Oddi Dysfunction) SOD refers to the mechanical malfunctioning of the Sphincter of Oddi, which is the valve muscle that regulates the flow of bile and pancreatic juice into the duodenum.
The Pancreas. Basic Anatomy. Endocrine pancreas. Exocrine pancreas. Pancreas vasculature. Islets of Langerhans. Acinar cells Ductal System
 SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
SGNA: Back to Basics Rogelio G. Silva, MD Assistant Clinical Professor of Medicine University of Illinois at Chicago Department of Medicine Division of Gastroenterology Advocate Christ Medical Center GI
Biliary tree dilation - and now what?
 Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Biliary tree dilation - and now what? Poster No.: C-1767 Congress: ECR 2012 Type: Educational Exhibit Authors: I. Ferreira, A. B. Ramos, S. Magalhães, M. Certo; Porto/PT Keywords: Pathology, Diagnostic
Management of Gallbladder Disease
 Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Management of Gallbladder Disease Steven B. Johnson, MD, FACS, FCCM Professor and Chairman, Department of Surgery Program Director, Phoenix Integrated Surgical Residency University of Arizona College of
Abnormal responses to morphine-neostigmine in patients with undefined biliary type pain
 Abnormal responses to morphine-neostigmine in patients with undefined biliary type pain I C ROBERTS-THOMSON AND J TOOULI Gut, 1985, 26, 1367-1372 From the Clinical Research Unit, The Walter and Eliza Hall
Abnormal responses to morphine-neostigmine in patients with undefined biliary type pain I C ROBERTS-THOMSON AND J TOOULI Gut, 1985, 26, 1367-1372 From the Clinical Research Unit, The Walter and Eliza Hall
What Should Be Done with Idiopathic Recurrent Pancreatitis That Remains Idiopathic after Standard Investigation?
 What Should Be Done with Idiopathic Recurrent Pancreatitis That Remains Idiopathic after Standard Investigation? John Baillie Division of Gastroenterology, Duke University Medical Center. Durham, NC, USA
What Should Be Done with Idiopathic Recurrent Pancreatitis That Remains Idiopathic after Standard Investigation? John Baillie Division of Gastroenterology, Duke University Medical Center. Durham, NC, USA
Slide 1. Slide 2. Slide 3 Pancreatic Cancer- Case #1. Endoscopic management of GI malignancy. Endoscopic approaches in GI malignancy- Agenda
 Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Slide 1 A teaching hospital of Harvard Medical School Endoscopic management of GI malignancy Tyler Berzin MD, MS Center for Advanced Endoscopy Division of Gastroenterology Beth Israel Deaconess Medical
Approach to the Biliary Stricture
 Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Approach to the Biliary Stricture ACG Eastern Postgraduate Course Washington DC June 8, 2014 Steven A. Edmundowicz MD FASGE Chief of Endoscopy Division of Gastroenterology Professor of Medicine Disclosures
Anatomical and Functional MRI of the Pancreas
 Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Anatomical and Functional MRI of the Pancreas MA Bali, MD, T Metens, PhD Erasme Hospital Free University of Brussels Belgium mbali@ulb.ac.be Introduction The use of MRI to investigate the pancreas has
Background. RUQ Ultrasound Normal, Recommend Clinical Correlation. Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial
 RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
RUQ Ultrasound Normal, Recommend Clinical Correlation Sohail R. Shah, MD, MSHA, FACS, FAAP Texas Children s Hosptial Background Incidence of pediatric gallbladder disease continues to rise U.S. Pediatric
THE FELLOWSHIP COUNCIL ADVANCED GI SURGERY CURRICULUM FOR FLEXIBLE ENDOSCOPY
 THE FELLOWSHIP COUNCIL ADVANCED GI SURGERY CURRICULUM FOR FLEXIBLE ENDOSCOPY 1. Introduction While general and thoracic surgical training now require basic skills in flexible GI endoscopy, advanced training
THE FELLOWSHIP COUNCIL ADVANCED GI SURGERY CURRICULUM FOR FLEXIBLE ENDOSCOPY 1. Introduction While general and thoracic surgical training now require basic skills in flexible GI endoscopy, advanced training
Original Policy Date 12:2013
 MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
MP 6.01.30 Magnetic Resonance Cholangiopancreatography Medical Policy Section Radiology Is12:2013sue 3:2005 Original Policy Date 12:2013 Last Review Status/Date 12:2013 Return to Medical Policy Index Disclaimer
ERCP / PTC Surgical Laparoscopic vs open Timing and order of approach
 Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Choledocholithiasis Which Approach and When? Lygia Stewart, MD University of California, San Francisco 2010 Naffziger Post-Graduate Course Clinical Manifestations of Choledocholithiasis Asymptomatic (no
Advanced Cannulation Techniques
 Advanced Cannulation Techniques Priya A. Jamidar, M.D., FASGE Professor of Medicine, Director of Endoscopy Yale School Disclosures Consultant to Boston Scientific and Olympus America Cannulation at ERCP
Advanced Cannulation Techniques Priya A. Jamidar, M.D., FASGE Professor of Medicine, Director of Endoscopy Yale School Disclosures Consultant to Boston Scientific and Olympus America Cannulation at ERCP
Together, putting patients first
 The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
The Role of a Gastroenterologist in the Diagnosis and Management of Pancreatic Cancer Sarah Jowett, Consultant Gastroenterologist Bradford Teaching Hospitals Trust Leeds Regional Study Day, 12 September
Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
 Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
Langenbecks Arch Surg (2009) 394:209 213 DOI 10.1007/s00423-008-0330-6 CURRENT CONCEPT IN CLINICAL SURGERY Congenital dilatation of the common bile duct and pancreaticobiliary maljunction clinical implications
CPT COD1NG UPDATES Gastroenterology CPT Advisors
 2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
2014 CPT COD1NG UPDATES Gastroenterology CPT Advisors Joel V. Brill, MD, AGA CPT Advisor Daniel C. DeMarco, MD, ACG CPT Advisor Glenn D. Littenberg, MD, ASGE CPT Advisor The American College of Gastroenterology
The biliary tract transports, stores, and regulates. Functional Gallbladder and Sphincter of Oddi Disorders
 GASTROENTEROLOGY 2006;130:1498 1509 Functional Gallbladder and Sphincter of Oddi Disorders JOSE BEHAR,* ENRICO CORAZZIARI, MOISES GUELRUD, WALTER HOGAN, STUART SHERMAN, and JAMES TOOULI # *Rhode Island
GASTROENTEROLOGY 2006;130:1498 1509 Functional Gallbladder and Sphincter of Oddi Disorders JOSE BEHAR,* ENRICO CORAZZIARI, MOISES GUELRUD, WALTER HOGAN, STUART SHERMAN, and JAMES TOOULI # *Rhode Island
Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico
 Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques Associate Professor
Colangitis Esclerosante Primaria: Manejo Clínico y Endoscópico Andrés Cárdenas, MD, MMSc, PhD, AGAF, FAASLD GI / Liver Unit, Hospital Clinic Institut de Malalties Digestives i Metaboliques Associate Professor
Pediatric PSC A children s tale
 Pediatric PSC A children s tale September 8 th PSC Partners seeking a cure Tamir Miloh Assistant Professor Pediatric Hepatology Mount Sinai Hospital, NY Incidence Primary Sclerosing Cholangitis (PSC) ;
Pediatric PSC A children s tale September 8 th PSC Partners seeking a cure Tamir Miloh Assistant Professor Pediatric Hepatology Mount Sinai Hospital, NY Incidence Primary Sclerosing Cholangitis (PSC) ;
16 April 2010 Resident Teaching Conference. Pancreatitis. W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D.
 16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
16 April 2010 Resident Teaching Conference Pancreatitis W. H. Nealon, M.D., F.A.C.S. J.J. Smith, M.D., D.W.D. Santorini Wirsung anatomy.med.umich.edu/.../ duodenum_ans.html Bud and ductology Ventral pancreatic
In Woong Han 1, O Choel Kwon 1, Min Gu Oh 1, Yoo Shin Choi 2, and Seung Eun Lee 2. Departments of Surgery, Dongguk University College of Medicine 2
 Effect of Rowachol on Prevention of Postcholecystectomy Syndrome after Laparoscopic Cholecystectomy - Prospective multicenter Randomized controlled trial- In Woong Han 1, O Choel Kwon 1, Min Gu Oh 1, Yoo
Effect of Rowachol on Prevention of Postcholecystectomy Syndrome after Laparoscopic Cholecystectomy - Prospective multicenter Randomized controlled trial- In Woong Han 1, O Choel Kwon 1, Min Gu Oh 1, Yoo
Original Article. Rattanasupar A Attasaranya S Ovartlarnporn B ABSTRACT
 74 THAI J GASTROENTEROL 2010 Esophagogastroduodenoscopy (EGD) plus Transabdominal Ultrasound (TUS) for Diagnosed Dyspepsia in Elderly Patients Original Article Esophagogastroduodenoscopy (EGD) plus Transabdominal
74 THAI J GASTROENTEROL 2010 Esophagogastroduodenoscopy (EGD) plus Transabdominal Ultrasound (TUS) for Diagnosed Dyspepsia in Elderly Patients Original Article Esophagogastroduodenoscopy (EGD) plus Transabdominal
Diagnosis of chronic Pancreatitis. Christoph Beglinger, University Hospital Basel, Switzerland
 Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
Diagnosis of chronic Pancreatitis Christoph Beglinger, University Hospital Basel, Switzerland Pancreatitis Pancreas Pancreas - an organ that makes bicarbonate to neutralize gastric acid, enzymes to digest
Principles of ERCP: papilla cannulation, indications/contraindications and risks. Dr. med. Henrik Csaba Horváth PhD
 Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
Principles of ERCP: papilla cannulation, indications/contraindications and risks Dr. med. Henrik Csaba Horváth PhD Evolution of ERCP 1968. 1970s ECPG Endoscopic CholangioPancreatoGraphy Japan 1974 Biliary
Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria
 ORIGINAL ARTICLE Annals of Gastroenterology (2018) 31, 1-6 Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria Ankit Chhoda
ORIGINAL ARTICLE Annals of Gastroenterology (2018) 31, 1-6 Sex-related differences in predicting choledocholithiasis using current American Society of Gastrointestinal Endoscopy risk criteria Ankit Chhoda
Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica
 Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica Authors: Sergio López-Durán, Celia Zaera, Juan Ángel
Title: The endoscopic ultrasound-assisted Rendez-Vous technique for treatment of recurrent pancreatitis due to pancreas divisum and ansa pancreatica Authors: Sergio López-Durán, Celia Zaera, Juan Ángel
Best of UEG week 2017 (Pancreas-biliary)
") Best of UEG week 2017 (Pancreas-biliary) Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Best of UEG week 2017 (Pancreas-biliary) Marianna Arvanitakis Erasme University Hospital, ULB, Brussels, Belgium 10 th Nottingham Endoscopy Masterclass SPEAKER DECLARATIONS This presenter has the following
Management of Gallbladder Disease. Cory Buschmann, MD PGY-5 11/28/2017
 Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Management of Gallbladder Disease Cory Buschmann, MD PGY-5 11/28/2017 Financial disclosures None Content Scope of gallbladder diseases Evaluation H&P Labs Imaging Cholecystectomy vs cholecystostomy Ancillary
Endoscopic treatment of primary sclerosing cholangitis: Is there something new?
 Endoscopic treatment of primary sclerosing cholangitis: Is there something new? Arnaud Lemmers, MD, PhD Gastroenterology Department, Erasme Hospital, ULB, Brussels BASL December 1st 2017 AGENDA Introduction
Endoscopic treatment of primary sclerosing cholangitis: Is there something new? Arnaud Lemmers, MD, PhD Gastroenterology Department, Erasme Hospital, ULB, Brussels BASL December 1st 2017 AGENDA Introduction
Intraductal papillary neoplasms in the bile ducts
 Intraductal papillary neoplasms in the bile ducts Seok Hwa Youn Myunghee Yoon Dong Hoon Shin Kosin University Gospel Hospital Department of general surgery Hepato-biliary-pancreatic division Introduction
Intraductal papillary neoplasms in the bile ducts Seok Hwa Youn Myunghee Yoon Dong Hoon Shin Kosin University Gospel Hospital Department of general surgery Hepato-biliary-pancreatic division Introduction
What Are Gallstones? GALLSTONES. Gallstones are pieces of hard, solid matter that form over time in. the gallbladder of some people.
 What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
What Are Gallstones? Gallstones are pieces of hard, solid matter that form over time in the gallbladder of some people. The gallbladder sits under the liver and stores bile (a key digestive juice ). Gallstones
ENDOSCOPY IN COMPETITION DIAGNOSTICS. Dr. med. Dirk Hartmann Klinikum Ludwigshafen
 Falk Symposium 166 GI Endoscopy Standards and Innovations Mainz, 18. 19. September 2008 ENDOSCOPY IN COMPETITION DIAGNOSTICS Dr. med. Dirk Hartmann Klinikum Ludwigshafen ENDOSCOPY IN COMPETITION Competing
Falk Symposium 166 GI Endoscopy Standards and Innovations Mainz, 18. 19. September 2008 ENDOSCOPY IN COMPETITION DIAGNOSTICS Dr. med. Dirk Hartmann Klinikum Ludwigshafen ENDOSCOPY IN COMPETITION Competing
REFERRAL GUIDELINES: GALLSTONES
 REFERRAL GUIDELINES: GALLSTONES Document Purpose To ensure patients with gallstones disease are managed appropriately in primary/ secondary care Oxford Radcliffe Hospital Surgical Department Surgical Registrar
REFERRAL GUIDELINES: GALLSTONES Document Purpose To ensure patients with gallstones disease are managed appropriately in primary/ secondary care Oxford Radcliffe Hospital Surgical Department Surgical Registrar
Biliary Tree Ultrasound - In a nutshell. Pamela Parker Lead Sonographer
 Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Biliary Tree Ultrasound - In a nutshell Pamela Parker Lead Sonographer Aims Review what we know about the biliary system Common pathologies Pitfalls Reporting tips The Nutshell Background Biliary examinations
Unresolved Issues about Post-ERCP Pancreatitis: An Overview
 Unresolved Issues about Post-ERCP Pancreatitis: An Overview Pier Alberto Testoni Division of Gastroenterology and Gastrointestinal Endoscopy, University Vita-Salute San Raffaele, IRCCS San Raffaele Hospital.
Unresolved Issues about Post-ERCP Pancreatitis: An Overview Pier Alberto Testoni Division of Gastroenterology and Gastrointestinal Endoscopy, University Vita-Salute San Raffaele, IRCCS San Raffaele Hospital.
Pancreatic Benign April 27, 2016
 Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Department of Surgery Pancreatic Benign April 27, 2016 James Choi Dr. Hernandez Objectives Medical Expert: 1. Anatomy and congenital anomalies of the pancreas and pancreatic duct (divisum, annular pancreas
Unusual case of pancreatic ascites and pancreatic pleural effusion following endoscopic retrograde cholangiopancreatography
 Yunen et al. 64 CASE REPORT OPEN ACCESS Unusual case of pancreatic ascites and pancreatic pleural effusion following endoscopic retrograde cholangiopancreatography Rafael Alba Yunen, King Soon Goh, Ugoagha
Yunen et al. 64 CASE REPORT OPEN ACCESS Unusual case of pancreatic ascites and pancreatic pleural effusion following endoscopic retrograde cholangiopancreatography Rafael Alba Yunen, King Soon Goh, Ugoagha
Duration of Pain Is Correlated With Elevation in Liver Function Tests in Patients With Symptomatic Choledocholithiasis
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:1077 1082 Duration of Pain Is Correlated With Elevation in Liver Function Tests in Patients With Symptomatic Choledocholithiasis ALA I. SHARARA, NABIL M.
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2010;8:1077 1082 Duration of Pain Is Correlated With Elevation in Liver Function Tests in Patients With Symptomatic Choledocholithiasis ALA I. SHARARA, NABIL M.
Endoscopy in idiopathic recurrent pancreatitis. Endoscopy for Idiopathic recurrent acute pancreatitis - the truth in between. Markus M.
 1456 Endoscopy for Idiopathic recurrent acute pancreatitis - the truth in between APA 30.10.2013 Miami Markus M. Lerch Medizinische Klinik der königlichen Universität Greifswald 1859 Disclosure: consultancy
1456 Endoscopy for Idiopathic recurrent acute pancreatitis - the truth in between APA 30.10.2013 Miami Markus M. Lerch Medizinische Klinik der königlichen Universität Greifswald 1859 Disclosure: consultancy
Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram
 Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram Assistant Professor, Department of Biotechnoloy, Lady Doak College, Madurai. Acute
Identification of Serum mirnas as prospective Bio-markers for acute and chronic pancreatitis Dr. Jeyaparvathi Somasundaram Assistant Professor, Department of Biotechnoloy, Lady Doak College, Madurai. Acute
Endoscopic Management of the Iatrogenic CBD Injury
 The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
The Liver Week 2014, Jeju, Korea Endoscopic Management of the Iatrogenic CBD Injury Jong Ho Moon, MD, PhD Department of Internal Medicine Soon Chun Hyang University School of Medicine Bucheon/Seoul, KOREA
ACG Clinical Guideline: Management of Acute Pancreatitis
 ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
ACG Clinical Guideline: Management of Acute Pancreatitis Scott Tenner, MD, MPH, FACG 1, John Baillie, MB, ChB, FRCP, FACG 2, John DeWitt, MD, FACG 3 and Santhi Swaroop Vege, MD, FACG 4 1 State University
Outline. Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines
 Guideline Review 4/6/2017. Case Example Background Classification Histology Guidelines") Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
Intraductal Papillary Mucinous Neoplasm (IPMN) Guideline Review The Nurse Practitioner Association New York State Capital Region Teaching Day Matthew Warndorf MD Case Example Background Classification
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer
 What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
What to do and not do before seeking surgical consultation for a patient with suspected pancreatic cancer 9 Th Annual Symposium on Gastrointestinal Cancers, St. Louis University School of Medicine Carlos
Review of idiopathic pancreatitis
 Online Submissions: wjg.wjgnet.com World J Gastroenterol 2007 December 21; 13(47): 6296-6313 World Journal of Gastroenterology ISSN 1007-9327 wjg@wjgnet.com 2007 WJG. All rights reserved. TOPIC HIGHLIGHT
Online Submissions: wjg.wjgnet.com World J Gastroenterol 2007 December 21; 13(47): 6296-6313 World Journal of Gastroenterology ISSN 1007-9327 wjg@wjgnet.com 2007 WJG. All rights reserved. TOPIC HIGHLIGHT
Research Article Safety and Yield of Diagnostic ERCP in Liver Transplant Patients with Abnormal Liver Function Tests
 Diagnostic and erapeutic Endoscopy, Article ID 314927, 5 pages http://dx.doi.org/10.1155/2014/314927 Research Article Safety and Yield of Diagnostic ERCP in Liver Transplant Patients with Abnormal Liver
Diagnostic and erapeutic Endoscopy, Article ID 314927, 5 pages http://dx.doi.org/10.1155/2014/314927 Research Article Safety and Yield of Diagnostic ERCP in Liver Transplant Patients with Abnormal Liver
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS
 Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Intraductal Papillary Mucinous Neoplasms: We Still Have a Way to Go! Francesco M. Serafini, MD, FACS Brooklyn VAMC September 21 st GI Grand Rounds - What is it? - Clinical entity that has emerged from
Risk Factors Associated With Biliary Pancreatitis In Children
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2012 Risk Factors Associated With Biliary Pancreatitis In
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine January 2012 Risk Factors Associated With Biliary Pancreatitis In
Scintigraphy versus manometry in patients with suspected biliary sphincter of Oddi dysfunction
 35 BILIARY DISEASE Scintigraphy versus manometry in patients with suspected biliary sphincter of Oddi dysfunction A G Craig, D Peter, GTPSaccone, P Ziesing, A Wycherley, J Toouli... See end of article
35 BILIARY DISEASE Scintigraphy versus manometry in patients with suspected biliary sphincter of Oddi dysfunction A G Craig, D Peter, GTPSaccone, P Ziesing, A Wycherley, J Toouli... See end of article
Cholangiocarcinoma: Radiologic evaluation and interventions
 November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
November 2014 Cholangiocarcinoma: Radiologic evaluation and interventions Colin Nevins, Harvard Medical School Year III Agenda Initial course and work-up Endoscopic retrograde cholangiopancreatography
Pathophysiology ACUTE PANCREATITIS
 Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis Pathophysiology ACUTE PANCREATITIS BILIARY OBSTRUCTION Duct obstruction in the bile duct, pancreatic duct, or both. Increasing pressure Unregulated activation of digestive enzymes. Inflammation
Pancreatitis is the most common and potentially serious ENDOSCOPY CORNER
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:834 839 ENDOSCOPY CORNER Short 5Fr vs Long 3Fr Pancreatic Stents in Patients at Risk for Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2009;7:834 839 ENDOSCOPY CORNER Short 5Fr vs Long 3Fr Pancreatic Stents in Patients at Risk for Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 10, by Am. Coll. of Gastroenterology ISSN /01/$20.00
 THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 10, 2001 2001 by Am. Coll. of Gastroenterology ISSN 0002-9270/01/$20.00 Published by Elsevier Science Inc. PII S0002-9270(01)02807-6 Can Endoscopic
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 96, No. 10, 2001 2001 by Am. Coll. of Gastroenterology ISSN 0002-9270/01/$20.00 Published by Elsevier Science Inc. PII S0002-9270(01)02807-6 Can Endoscopic
Research Article The Diagnostic Accuracy of Linear Endoscopic Ultrasound for Evaluating Symptoms Suggestive of Common Bile Duct Stones
 Gastroenterology Research and Practice Volume 2016, Article ID 6957235, 5 pages http://dx.doi.org/10.1155/2016/6957235 Research Article The Diagnostic Accuracy of Linear Endoscopic Ultrasound for Evaluating
Gastroenterology Research and Practice Volume 2016, Article ID 6957235, 5 pages http://dx.doi.org/10.1155/2016/6957235 Research Article The Diagnostic Accuracy of Linear Endoscopic Ultrasound for Evaluating
Gallstones Information Leaflet THE DIGESTIVE SYSTEM. Gutscharity.org.uk
 THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about gallstones Gall is an old-fashioned word for bile, a liquid made in the liver and stored in the gall bladder
THE DIGESTIVE SYSTEM http://healthfavo.com/digestive-system-for-kids.html This factsheet is about gallstones Gall is an old-fashioned word for bile, a liquid made in the liver and stored in the gall bladder
What Is Pancreatitis?
 What Is Pancreatitis? Pancreatitis is inflammation (swelling) of the pancreas that is most often caused by gallstones or alcohol abuse. There are other causes that your gastroenterologist will look for,
What Is Pancreatitis? Pancreatitis is inflammation (swelling) of the pancreas that is most often caused by gallstones or alcohol abuse. There are other causes that your gastroenterologist will look for,
Sphincter of Oddi Dysfunction
 Curr Gastroenterol Rep (2010) 12:130 134 DOI 10.1007/s11894-010-0096-1 Sphincter of Oddi Dysfunction John Baillie Published online: 10 March 2010 # Springer Science+Business Media, LLC 2010 Abstract Sphincter
Curr Gastroenterol Rep (2010) 12:130 134 DOI 10.1007/s11894-010-0096-1 Sphincter of Oddi Dysfunction John Baillie Published online: 10 March 2010 # Springer Science+Business Media, LLC 2010 Abstract Sphincter