Clostridium difficile Infection (CDI) Guideline Update:
|
|
|
- Lilian Martin
- 5 years ago
- Views:
Transcription
1 Clostridium difficile Infection (CDI) Guideline Update: Understanding the Data Behind the Recommendations Erik R. Dubberke, MD, MSPH A Webinar for HealthTrust Members Professor of Medicine September 24, 2018 Washington University School of Medicine
2 Summary of Key Changes from 2010 Guidelines Epidemiology 027/NAP1/BI strain possibly on the mend Diagnosis Still not completely satisfying Infection prevention and control Nothing really new Too early to know what to do with asymptomatic carriers Treatment Major changes Should result in improved outcomes
 Toxigenic C.")
3 Clostridium difficile Gram positive, spore forming rod Obligate anaerobe Toxin A and Toxin B Required to cause disease (toxigenic) 20% to 30% non-toxigenic C. difficile infection (CDI, formerly CDAD) Toxigenic C. difficile in stool CDI Ubiquitous organism: soil, water, pets, livestock, food, homes of otherwise healthy people, healthy people

4 CDI Epidemiology Best surveillance in US: CDC Emerging Infections Program Seminal paper on CDI published in 2015 Data from 2011 Key findings 147 incident CDI cases / 100,000 persons >450,000 incident cases >29,000 associated deaths More community-onset cases than previously recognized 027 strain: 31% healthcare-associated CDI, 19% community-associated CDI Lessa. NEJM. 2015
5 Declines in 027 since 2011 Incidence (per 100,000) 027: Healthcare associated (%) 027: Community associated (%) % 21% 24% 14% 19% 19% 17% 12% 7%* 8%* *not most common strain
6 Diagnostics Available Test Advantage(s) Disadvantage(s) Toxin testing Toxin Enzyme immunoassay (EIA) Rapid, simple, inexpensive Least sensitive method, assay variability Tissue culture cytotoxicity More sensitive than toxin EIA, associated with outcomes Labor intensive; requires hours for a final result, special equipment; Organism identification Glutamate dehydrogenase (GDH) EIA Rapid, sensitive Non-toxigenic and toxigenic C. difficile detected; Nucleic acid amplification tests (NAAT) (PCR) Rapid, sensitive, detects presence of toxin gene Cost, special equipment, may be too sensitive Stool culture Most sensitive test available when performed appropriately Non-toxigenic and toxigenic C. difficile detected; labor-intensive; requires hours for results
7 Historical Flaws in Diagnostic Literature Interpretation Lack of clinical data Test for CDI does not exist: detect toxin or organism Up to 15% of patients admitted to the hospital are colonized with toxigenic C. difficile Other reasons for diarrhea are often present Enhanced sensitivity for C. difficile detection will increase detection of asymptomatic C. difficile carriage Patients with CDI have more toxin / organism in stool than asymptomatic carriers Lack of appreciation not all toxin detection assays are equal Original EIAs: detect toxin A only Some strains produce only toxin B (as many as 20%) Manufacturer, target(s) and format make a difference Dubberke. AAC. 2015; Peterson, CID. 2007
8 Types of False Positive Tests for CDI Toxigenic C. difficile present but no CDI Concern of more sensitive tests GDH NAAT/PCR Culture Assay result positive but toxigenic C. difficile not present Tests that detect non-toxigenic C. difficile GDH alone Culture alone False positive test

9 Enhanced Sensitivity to Detect C. difficile Decreases Specificity for CDI Including clinically significant diarrhea in gold standard: No impact on sensitivity NAATs 99% Techlab Tox AB II 94% Specificity of NAATs decreased from ~98% to ~89% (p < 0.01) Positive predictive value decreased to ~60% (25% drop) No NAAT (+) / toxin ( ) developed CDIrelated complications Dubberke. JCM. 2011;
10 Largest Assay Comparison To Date Variable Cytotoxicity (CTX) + Number White blood count (SD) CTX -/ NAAT + -/- (CTX+ ) vs. (CTX-/NAAT+) (CTX+) vs. (-/-) 12.4 (8.9) 9.9 (6.6) 10.0 (12.0) <0.001 < Died 72 (16.6%) 30 (9.7%) 349 (8.9%) < (CTX- /NAAT+) vs. (-/-) Planche. Lancet ID. 2013
11 Time to Resolution of Diarrhea Polage. JAMA IM. 2015
12 Guidelines: Diagnosis Clinical question: What is the preferred population for C. difficile testing, and should efforts be made to achieve this target? Patients with unexplained and new-onset 3 unformed stools in 24 hours are the preferred target population for testing for CDI (weak recommendation, very low quality of evidence)
13 Limitations Noted Weak supportive data on definition for clinically significant diarrhea Has changed over time Other conditions / medications can confound Suggest ways to improve patient selection: Clinicians: order tests only on patients likely to have CDI Laboratories: reject specimens that are not soft/liquid (i.e. take the shape of the container) Author Year Definition Tedesco 1974 > 5 loose BM/day Teasley 1983 > 6 loose BM over 36 hours Fekety 1989 Liquid OR >4 BM per day for 3 days Johnson loose or watery BM in 24 hours McDonald. CID. 2018
14 Supportive Evidence for Clinicians Take home messages: Pre-test probability (n) Variable Low (n=72) Medium (n=34) High (n=5) Positive toxin EIAIf clinical judgement 0 used: 365% did not 1 Positive toxigenic culture Negative EIA and empiric treatment Negative EIA and CDI diagnosed in next 30 days need to be tested If we used NAAT, 9 CDI cases vs day mortality Kwon. JCM. 2017
15 Real world Both: weak recommendation, low quality of evidence Ideal world
16 Will Limiting Testing to the Ideal World Limit False Positive NAATs for CDI? 2 years of data: 8,931 testing episodes 8,361 EIA- 570 EIA+ Patients with Clinically significant diarrhea ( 3 diarrheal BM/d or diarrhea plus abdominal pain) No alternate explanation for diarrhea (e.g. laxatives, tube feeds, colostomy, etc.) No recent CDI For EIA-, no treatment for CDI Inpatient
17 EIA- Stools Eligible for culture N=515 (20%) *6% of total EIA- stools* Eligible for Chart Review N=2552 (31%) Total EIA- Stools N=8361 Excluded during chart review N=2037 (80%) Excluded through Medical Informatics queries N=5809 (69%) Reasons for exclusion: Outpatient Unable to determine diarrhea severity Diarrhea not clinically significant Other reason for diarrhea History of CDI Reasons for exclusion: Medical condition associated with diarrhea Laxatives Tube feeds Ostomy Chemo Other infectious etiology History of CDI CDI treatment antibiotics Toxigenic culture positive: N=63 (12.2%)
18 False Positives in Ideal World Testing Scenario Same process for EIA+ specimens 107 (20%) met criteria 170 total that were EIA+ (107) or EIA- / toxigenic culture+ (63) Most EIA- / toxigenic culture+ would be NAAT+ If NAAT used: 63/170 = 37% false positives Similar to what is seen in real world
19 European Recommendations: Importance of Toxin Detection and Clinical Evaluation Crobach. Clin Microbiol Infect. 2016
20 Guidelines: Prevention Antimicrobial stewardship: best intervention available today Contact precautions: prevent transmission of C. difficile from patients with CDI Disinfecting the environment Screening for asymptomatic C. difficile carriers Data not there to support recommendation Needs more study
21 The C. difficile Iceberg CDI 10%-30% Asymptomatic Carriers 70%-90% Courtesy L. Clifford McDonald (note: color changed from original slide)

22 Asymptomatic Carriers Contribute to CDI Clabots: 84% of new acquisitions came from an asymptomatic carrier Lanzas: at least 50% of hospital-onset CDI cases come from asymptomatic carriers Eyre: transmission from as few as 1% of asymptomatic carriers can account for 50% of CDI cases Curry: new hospital-onset CDI 30% from other CDI cases 29% from known asymptomatic carriers (not all patients screened) Clabots. JID. 1992; Lanzas. ICHE. 2011; Eyre PLoS One. 2013; Curry. CID. 2013; McDonald. CID. 2013

23 Screening for Asymptomatic Carriage Issues to keep in mind Single center Recent abstract without significant reduction in CDI Other potential explanations for reductions in CDI More successful than models Lessons learned from MRSA / VRE Cost/expense/person-time to screen Longtin. JAMA IM. 2016; Peterson. ECCMID Abstract 2332; Lanzas. ICHE 2014
24 Guidelines: Treatment
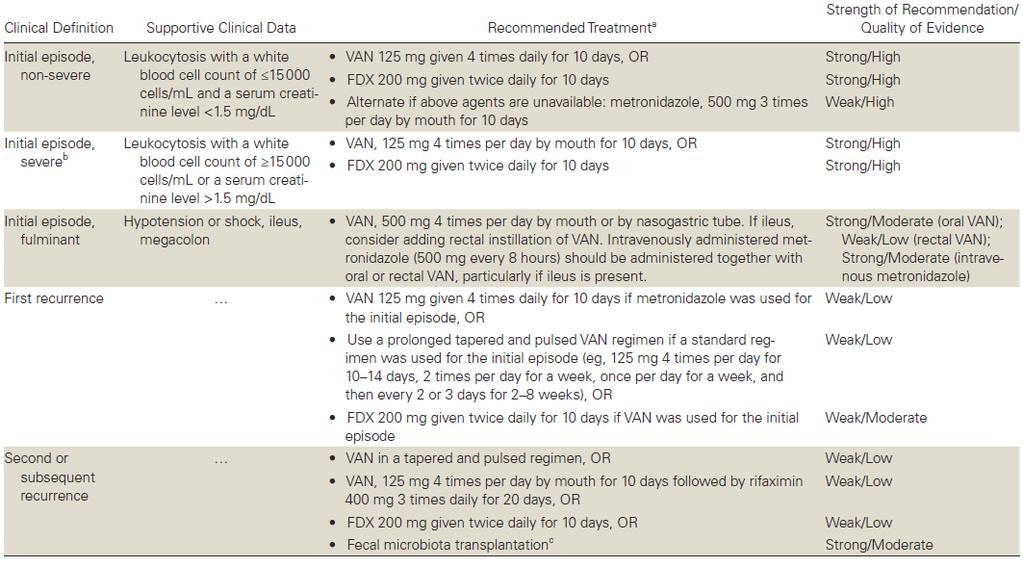
25 Initial episode Clinical Definition Initial episode, non-severe Initial episode, severe Supportive Clinical Data WBC 15,000 cells/ml, serum Cr <1.5 mg/dl Fidaxomicin now firstline agent Initial episode, fulminant WBC >15,000 cells/ml, serum Cr >1.5 mg/dl Hypotension or shock, ileus, megacolon Minor change to serum creatinine cut-off Recommended Treatment (Strength of Recommendation/ Quality of Evidence) VAN 125 mg given 4 times daily for 10 days (Strong/High), OR FDX 200 mg given twice daily for 10 days (Strong/High) Alternate if above agents are unavailable: metronidazole, 500 mg 3 times per day by mouth for 10 days (Weak/High) VAN, 125 mg 4 times per day by mouth for 10 days (Strong/High), OR FDX 200 mg given twice daily for 10 days (Strong/High) VAN, 500 mg 4 times per day by mouth or by nasogastric tube (Strong/Moderate). If ileus, consider adding rectal instillation of VAN. IV metronidazole (500 mg every 8 hours) (Strong/Moderate) should be administered together with oral or rectal VAN (Weak/Low), particularly if ileus is present. Major change: metronidazole is no longer first line agent for non-severe CDI in settings where access to VAN/FDX is not limited


26 Metronidazole Inferior For Severe and Non-Severe CDI **P=0.020, M vs. V Vancomycin superior to metronidazole on multivariable analysis, including controlling for clinical severity (p=0.013) Johnson S, et al. Clin Infect Dis. 2014;59:
27 Fidaxomicin vs. Vancomycin Clinical Outcomes in mitt Populations Novel macrocyclic antimicrobial Narrow spectrum *Lower boundary 97.5% CI. 95% CI. a. Louie TJ, et al. N Engl J Med. 2011;364: ; b. Cornely OA, et al. Lancet Infect Dis. 2012;12: No activity against Gram-negative agents Sparing of Bacteroides sp., Bifidobacterium, clostridial clusters IV and XIV Clinical Outcomes Fidaxomicin, n (%) Vancomycin, n (%) Treatment Difference P Value Clinical cure Louie [a] 253/287 (88.2) Cornely [b] 221/252 (87.8) Recurrence Louie [a] Cornely [b] 39/253 (15.4) 28/221 (12.7) Sustained clinical response * Louie [a] 214/287 (74.6) Cornely [b] 193/252 (76.6) 265/309 (85.8) 223/257 (86.7) 67/265 (25.3) 60/223 (26.9) 198/309 (64.1) 163/257 (63.4) -3.1* -4.9* -9.9 (-16.6 to -2.9) (-21 to -6.8) 10.5 (3.1 to 17.7) 13.2 (5.3 to 21) P =.0005 P =.0002 P =.006 P =.001
28 Recurrence CDI Clinical Definition First recurrence Second or subsequent recurrence Recommended Treatment (Strength of Recommendation/ Quality of Evidence) VAN 125 mg given 4 times daily for 10 days if metronidazole was used for the initial episode (Weak/Low), OR Use a prolonged tapered and pulsed VAN regimen if a standard regimen was used for the initial episode (Weak/Low), OR FDX 200 mg given twice daily for 10 days if VAN was used for the initial Episode (Weak/Moderate) Do not give same regimen a second time VAN in a tapered and pulsed regimen (Weak/Low), OR VAN, 125 mg 4 times per day by mouth for 10 days followed by rifaximin 400 mg 3 times daily for 20 days (Weak/Low), OR FDX 200 mg given twice daily for 10 days (Weak/Low), OR Fecal microbiota transplantation (Strong/Moderate) (appropriate antibiotic treatments for at least 2 recurrences (i.e., 3 CDI episodes) should be tried prior to offering fecal microbiota transplantation) More options provided for second or subsequent recurrence
29 Percent Participants with CDI Recurrence Percent Participants with CDI Recurrence What about Bezlotoxumab? Monoclonal antibody against C. difficile toxin B Administered as single IV infusion in addition to standard of care CDI treatment antibiotics Indication: prevention of recurrent CDI Results not available early enough to be included Age 65 yrs Hx CDI Immunocompromised Severe CDI RT 027/078/244 Bezlo Placebo 0 No risk factors 1 risk factor 1 risk factor 2 risk factors 3 risk factors Bezlo Placebo Gerding. CID. 2018
30 How Can the Microbiology Laboratory Help? CDI prevention multidisciplinary Infection Prevention and Control Antimicrobial Stewardship Program Clinicians Nurses Housekeeping Microbiology laboratory: necessary piece Time to diagnosis of CDI Laboratory-based approaches to minimize false positives Improve antimicrobial prescribing

31 Greatest Risk of Transmission Early Highest risk period for C. difficile transmission Not in contact precautions Sethi. ICHE. 2010
32 Potential Delays to Avoid Mean days from diarrhea onset to Order: 1.4 days Physician awareness Nursing awareness Result: 3.2 days Time from order to collection Frequency of testing Kundrapu. JCM. 2013
33 Minimize False Positive Tests for CDI False positives lead to: Unnecessary antimicrobial use Promotes spread of resistant bacteria Paradoxically may increase risk for CDI once stopped Unnecessary contact precautions Patient anxiety / satisfaction Increase in adverse events Lack of investigation for other causes of diarrhea Diversion of limited resources Masks impact of CDI prevention activities Hospital may lose reimbursement from high CDI rates
34 Interventions to Minimize False Positive Tests DO NOT TEST FORMED STOOLS No diarrhea = No CDI Do not allow test of cure Not predictive of treatment success or risk of recurrent CDI Do not allow automatic repeat testing Most positive tests on repeat testing are false positives Educate nurses and physicians on patient selection for testing Diarrhea: Clinically significant, no other cause: test ASAP (consider contact precautions) Not clinically significant or alternate explanation (i.e. low pre-test probability): do not test Educate on test used at your facility And always remind people: C. difficile test, NOT CDI test
35 Different Testing Strategies and False Positives Hypothetical scenarios Toxin EIA: sensitivity 85%, specificity 97% NAAT: sensitivity 99%, specificity 89% (CDI) GDH: sensitivity 99% (ignore specificity) Test 1,000 patients, 100 with CDI (10% prevalence) Testing strategy True positives Toxin EIA only NAAT only NAAT or GDH (+) then Toxin EIA 84 3 False positives
36 Assist in Antimicrobial Stewardship Improve test utilization related to infections Order of tests in drop down list Most appropriate test first Reflex urine cultures: >10 WBC / high power field Rapid diagnostics MALDI Rapid tests for resistance mechanisms Respiratory multiplex PCRs Barlam. CID. 2016; Sarg. ICHE. 2016; Subramony. J Pediatr. 2016
37 Conclusions: 2017 Guideline Update CDI epidemiology is changing 027 strain may be declining Testing recommendations still with weak supportive data Improve patient selection In most scenarios, toxin testing helpful Antimicrobial stewardship best available CDI prevention intervention Screening for asymptomatic carriage: research for now Major changes to treatment recommendations Metronidazole no longer first-line agent Fidaxomicin is a first-line agent The microbiology lab is a key component to CDI prevention efforts
Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate
 Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate Objectives Summarize the changing epidemiology and demographics of patients at risk for Clostridium
Clostridium Difficile Infection: Applying New Treatment Guidelines and Strategies to Reduce Recurrence Rate Objectives Summarize the changing epidemiology and demographics of patients at risk for Clostridium
Clostridium difficile Infection (CDI) Management Guideline
 Management Guideline") Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Clostridium difficile Infection (CDI) Management Guideline Do not test all patients with loose or watery stools for CDI o CDI is responsible for
Clostridium difficile Infection: Diagnosis and Management
 Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
Clostridium difficile Infection: Diagnosis and Management Brian Viviano D.O. Case study 42 year old female with history of essential hypertension and COPD presents to ED complaining of 24 hours of intractable,
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE
 EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
EDUCATIONAL COMMENTARY CLOSTRIDIUM DIFFICILE UPDATE Educational commentary is provided through our affiliation with the American Society for Clinical Pathology (ASCP). To obtain FREE CME/CMLE credits click
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Stony Brook Adult Clostridium difficile Management Guidelines. Discontinue all unnecessary antibiotics
 Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
Stony Brook Adult Clostridium difficile Management Guidelines Summary: Use of the C Diff Infection (CDI) PowerPlan (Adult) Required Patient with clinical findings suggestive of Clostridium difficile infection
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE
 ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
ENGLISH FOR PROFESSIONAL PURPOSES UNIT 3 HOW TO DEAL WITH CLOSTRIDIUM DIFFICILE The diagnosis of CDI should be based on a combination of clinical and laboratory findings. A case definition for the usual
Modern approach to Clostridium Difficile Infection
 Modern approach to Clostridium Difficile Infection Pseudomembranous Colitis: Principles for diagnosis and treatment Aggelos Stefos Internist, Infectious diseases Specialist Department of Medicine and Research
Modern approach to Clostridium Difficile Infection Pseudomembranous Colitis: Principles for diagnosis and treatment Aggelos Stefos Internist, Infectious diseases Specialist Department of Medicine and Research
Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018
 Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018 Disclosures None Objectives Highlight important changes in the management of Clostridium difficile
Clostridium difficile CRISTINA BAKER, MD, MPH INFECTIOUS DISEASE PARK NICOLLET/HEALTH PARTNERS 11/9/2018 Disclosures None Objectives Highlight important changes in the management of Clostridium difficile
Updated Clostridium difficile Treatment Guidelines
 Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
Updated Clostridium difficile Treatment Guidelines Arielle Arnold, PharmD, BCPS Clinical Pharmacist Saint Alphonsus Regional Medical Center September 29 th, 2018 Disclosures Nothing to disclose Learning
L. Clifford McDonald, MD. Senior Advisor for Science and Integrity September 16, 2015
 Controversies and Current Issues in Diagnosis, Surveillance, and Treatment of Clostridium difficile infeciton L. Clifford McDonald, MD Senior Advisor for Science and Integrity September 16, 2015 Division
Controversies and Current Issues in Diagnosis, Surveillance, and Treatment of Clostridium difficile infeciton L. Clifford McDonald, MD Senior Advisor for Science and Integrity September 16, 2015 Division
Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review
 Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review October 18, 2010 James Kahn and Carolyn Kenney, MSIV Overview Burden of disease associated
Diagnosis, Management, and Prevention of Clostridium difficile infection in Long-Term Care Facilities: A Review October 18, 2010 James Kahn and Carolyn Kenney, MSIV Overview Burden of disease associated
C. Difficile Testing Protocol
 C. Difficile Testing Protocol Caroline Donovan, RN, BSN, ONC- Infection Control Practitioner Abegail Pangan, RN, MSN, CIC- Infection Control Practitioner U.S. NEWS & WORLD REPORT 2017 2018 RANKINGS Acute
C. Difficile Testing Protocol Caroline Donovan, RN, BSN, ONC- Infection Control Practitioner Abegail Pangan, RN, MSN, CIC- Infection Control Practitioner U.S. NEWS & WORLD REPORT 2017 2018 RANKINGS Acute
Clostridium difficile infection surveillance: Applying the case definition
 Clostridium difficile infection surveillance: Applying the case definition PICNet Conference March 3 rd 2016 Presented by: Tara Leigh Donovan, MSc Managing Consultant (Former Epidemiologist) 1 Disclaimer
Clostridium difficile infection surveillance: Applying the case definition PICNet Conference March 3 rd 2016 Presented by: Tara Leigh Donovan, MSc Managing Consultant (Former Epidemiologist) 1 Disclaimer
Case 1. Which of the following would be next appropriate investigation/s regarding the pts diarrhoea?
 Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Case 1 21 yr old HIV +ve, Cd4-100 HAART naïve Profuse diarrhoea for 3/52. Stool MC&S ve Which of the following would be next appropriate investigation/s regarding the pts diarrhoea? Repeat stool MC&S Stool
Clostridium difficile: Can you smell the new updates?
 Clostridium difficile: Can you smell the new updates? Sunish Shah, Pharm.D. PGY-2 Infectious Disease Pharmacy Resident Yale-New Haven Hospital sshah1741@mail.usciences.edu Learning objectives Recognize
Clostridium difficile: Can you smell the new updates? Sunish Shah, Pharm.D. PGY-2 Infectious Disease Pharmacy Resident Yale-New Haven Hospital sshah1741@mail.usciences.edu Learning objectives Recognize
CDI Burden and Pathophysiology
 CDI Burden and Pathophysiology Ciarán P. Kelly, MD Professor of Medicine Harvard Medical School Director Gastroenterology Fellowship Training Director Celiac Center Beth Israel Deaconess Medical Center
CDI Burden and Pathophysiology Ciarán P. Kelly, MD Professor of Medicine Harvard Medical School Director Gastroenterology Fellowship Training Director Celiac Center Beth Israel Deaconess Medical Center
9/18/2018. Clostridium Difficile: Updates on Diagnosis and Treatment. Clostridium difficile Infection (CDI) Clostridium difficile Infection (CDI)
 Clostridium difficile Infection (CDI)") Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
Clostridium Difficile: Updates on Diagnosis and Treatment Elizabeth Hudson, DO, MPH 9/25/18 Antibiotic-associated diarrhea and colitis were well established soon after widespread use of antibiotics In
Clostridium difficile Diagnostic and Clinical Challenges
 Papers in Press. Published December 11, 2015 as doi:10.1373/clinchem.2015.243717 The latest version is at http://hwmaint.clinchem.org/cgi/doi/10.1373/clinchem.2015.243717 Clinical Chemistry 62:2 000 000
Papers in Press. Published December 11, 2015 as doi:10.1373/clinchem.2015.243717 The latest version is at http://hwmaint.clinchem.org/cgi/doi/10.1373/clinchem.2015.243717 Clinical Chemistry 62:2 000 000
Pros and Cons of Alternative Diagnostic Testing Strategies for C. difficile Infection
 Pros and Cons of Alternative Diagnostic Testing Strategies for C. difficile Infection Christopher R. Polage, MD, MAS Associate Professor of Pathology and Infectious Diseases UC Davis Disclosures Test materials
Pros and Cons of Alternative Diagnostic Testing Strategies for C. difficile Infection Christopher R. Polage, MD, MAS Associate Professor of Pathology and Infectious Diseases UC Davis Disclosures Test materials
6/14/2012. Welcome! PRESENTATION OUTLINE CLOSTRIDIUM DIFFICILE PREVENTION. Teaming Up to Prevent Infections! 1) Impact. 2) Testing Recommendations
 Impact. 2) Testing Recommendations") CLOSTRIDIUM DIFFICILE PREVENTION Beth Goodall, RN, BSN Board Certified in Infection Prevention and Control DCH Health System Epidemiology Director Welcome! Teaming Up to Prevent Infections! CLOSTRIDIUM
CLOSTRIDIUM DIFFICILE PREVENTION Beth Goodall, RN, BSN Board Certified in Infection Prevention and Control DCH Health System Epidemiology Director Welcome! Teaming Up to Prevent Infections! CLOSTRIDIUM
Clostridium difficile Infection (CDI)
") 18.09.10 월요집담회 Clostridium difficile Infection (CDI) R4 송주혜 Clostridium difficile infection (CDI) Anaerobic gram (+), spore-forming, toxin(tcda&tcdb)-producing bacillus Transmitted among humans through
18.09.10 월요집담회 Clostridium difficile Infection (CDI) R4 송주혜 Clostridium difficile infection (CDI) Anaerobic gram (+), spore-forming, toxin(tcda&tcdb)-producing bacillus Transmitted among humans through
Clostridium difficile infection (CDI) Week 52 (Ending 30/12/2017)
 Week 52 (Ending 30/12/2017)") Clostridium difficile infection (CDI) Week 52 (Ending 30/12/2017) What is Clostridium difficile? Clostridium difficile is a Gram-positive anaerobic spore forming bacillus. It is ubiquitous in nature and
Clostridium difficile infection (CDI) Week 52 (Ending 30/12/2017) What is Clostridium difficile? Clostridium difficile is a Gram-positive anaerobic spore forming bacillus. It is ubiquitous in nature and
Clostridium difficile: An Overview
 Clostridium difficile: An Overview CDI Webinar July 11, 2017 PUBLIC HEALTH DIVISION Acute and Communicable Disease Prevention Section Outline Background Microbiology Burden Pathogenesis Diagnostic testing
Clostridium difficile: An Overview CDI Webinar July 11, 2017 PUBLIC HEALTH DIVISION Acute and Communicable Disease Prevention Section Outline Background Microbiology Burden Pathogenesis Diagnostic testing
DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest wit
 Potential for conflicts of interest wit") GASTROENTERITIS DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest within this presentation fidaxomicin (which
GASTROENTERITIS DISCLOSURE Relevant relationships with commercial entities Wyeth (received advisory board & speaker honoraria) Potential for conflicts of interest within this presentation fidaxomicin (which
ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Clostridium difficile Infections
 ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Clostridium difficile Infections Christina M. Surawicz, MD 1, Lawrence J. Brandt, MD 2, David G. Binion, MD 3, Ashwin N. Ananthakrishnan,
ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Clostridium difficile Infections Christina M. Surawicz, MD 1, Lawrence J. Brandt, MD 2, David G. Binion, MD 3, Ashwin N. Ananthakrishnan,
Clinical Infectious Diseases IDSA GUIDELINE
 Clinical Infectious Diseases IDSA GUIDELINE Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and
Clinical Infectious Diseases IDSA GUIDELINE Clinical Practice Guidelines for Clostridium difficile Infection in Adults and Children: 2017 Update by the Infectious Diseases Society of America (IDSA) and
Terapia dell infezione da Clostridium difficile. Massimo Coen I Div Mal Inf AO L Sacco
 Terapia dell infezione da Clostridium difficile Massimo Coen I Div Mal Inf AO L Sacco Disease Severity Mild CDI 3 5 BM/day WBC 15,000/mm 3 Defining CDI Disease Severity Mild abdominal pain due to CDI Moderate
Terapia dell infezione da Clostridium difficile Massimo Coen I Div Mal Inf AO L Sacco Disease Severity Mild CDI 3 5 BM/day WBC 15,000/mm 3 Defining CDI Disease Severity Mild abdominal pain due to CDI Moderate
March 3, To: Hospitals, Long Term Care Facilities, and Local Health Departments
 March 3, 2010 To: Hospitals, Long Term Care Facilities, and Local Health Departments From: NYSDOH Bureau of Healthcare Associated Infections HEALTH ADVISORY: GUIDANCE FOR PREVENTION AND CONTROL OF HEALTHCARE
March 3, 2010 To: Hospitals, Long Term Care Facilities, and Local Health Departments From: NYSDOH Bureau of Healthcare Associated Infections HEALTH ADVISORY: GUIDANCE FOR PREVENTION AND CONTROL OF HEALTHCARE
Bezlotoxumab (Zinplava) as Adjunct Treatment for Clostridium difficile. Janel Liane Cala, RPh Medical Center Hospital
 as Adjunct Treatment for Clostridium difficile. Janel Liane Cala, RPh Medical Center Hospital") Bezlotoxumab (Zinplava) as Adjunct Treatment for Clostridium difficile Janel Liane Cala, RPh Medical Center Hospital Objectives Review pathophysiology, risk factors, prevention, and treatment options of
Bezlotoxumab (Zinplava) as Adjunct Treatment for Clostridium difficile Janel Liane Cala, RPh Medical Center Hospital Objectives Review pathophysiology, risk factors, prevention, and treatment options of
Long-Term Care Updates
 Long-Term Care Updates April 2018 By Austin Smith, PharmD Candidate and Lindsay Slowiczek, PharmD is the most common healthcare-acquired infection (HAI) in the United States. 1,2 A 2014 prevalence survey
Long-Term Care Updates April 2018 By Austin Smith, PharmD Candidate and Lindsay Slowiczek, PharmD is the most common healthcare-acquired infection (HAI) in the United States. 1,2 A 2014 prevalence survey
Historical Perspective
 The Diagnosis of C. difficile Infections: Does Molecular Make it More or Less difficile? Stephen M. Brecher Ph.D. VA Boston Health Care System BU School of Medicine The opinions expressed in this presentation
The Diagnosis of C. difficile Infections: Does Molecular Make it More or Less difficile? Stephen M. Brecher Ph.D. VA Boston Health Care System BU School of Medicine The opinions expressed in this presentation
Clostridium Difficile Associated Disease. Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011
 Clostridium Difficile Associated Disease Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011 Introduction Which of the following is more common in community hospitals in the Southeast
Clostridium Difficile Associated Disease Edmund Krasinski, Jr., D.O., F.A.C.G. Southwest Conference on Medicine 2011 Introduction Which of the following is more common in community hospitals in the Southeast
ABSTRACT PURPOSE METHODS
 ABSTRACT PURPOSE The purpose of this study was to characterize the CDI population at this institution according to known risk factors and to examine the effect of appropriate evidence-based treatment selection
ABSTRACT PURPOSE The purpose of this study was to characterize the CDI population at this institution according to known risk factors and to examine the effect of appropriate evidence-based treatment selection
! Macrolide antibacterial. Fidaxomicin (Dificid ) package labeling. Optimer Pharmaceuticals, Inc. May 2011.
 package labeling. Optimer Pharmaceuticals, Inc. May 2011.") Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
Disclosure! I have no conflicts of interest related to this presentation Nina Naeger Murphy, Pharm.D., BCPS Clinical Pharmacy Specialist Infectious Diseases MetroHealth Medical Center Learning Objectives!
A Pharmacist Perspective
 Leveraging Technology to Reduce CDI A Pharmacist Perspective Ed Eiland, Pharm.D., MBA, BCPS (AQ-ID) Clinical Practice and Business Supervisor Huntsville Hospital System Huntsville Hospital 881 licensed
Leveraging Technology to Reduce CDI A Pharmacist Perspective Ed Eiland, Pharm.D., MBA, BCPS (AQ-ID) Clinical Practice and Business Supervisor Huntsville Hospital System Huntsville Hospital 881 licensed
Journey to Decreasing Clostridium Difficile and the Unexpected Twist. Jackie Morton, Infection Prevention Cortney Swiggart, Medication Safety Officer
 Journey to Decreasing Clostridium Difficile and the Unexpected Twist Jackie Morton, Infection Prevention Cortney Swiggart, Medication Safety Officer 4/13/2018 Objectives Discuss the organism and clinical
Journey to Decreasing Clostridium Difficile and the Unexpected Twist Jackie Morton, Infection Prevention Cortney Swiggart, Medication Safety Officer 4/13/2018 Objectives Discuss the organism and clinical
Clostridium Difficile colitismore
 Clostridium Difficile colitismore virulent than ever ECHO- February 18, 2016 Charles Krasner, M.D. UNR School of Medicine Sierra NV Veterans Affairs Hospital Growing problem of pseudomembranous colitis
Clostridium Difficile colitismore virulent than ever ECHO- February 18, 2016 Charles Krasner, M.D. UNR School of Medicine Sierra NV Veterans Affairs Hospital Growing problem of pseudomembranous colitis
C. DIFF QUIK CHEK COMPLETE. Get the complete diagnostic picture with just one test. TAP HERE TO SEE THE NEXT PAGE
 C. DIFF QUIK CHEK COMPLETE Get the complete diagnostic picture with just one test. TAP HERE TO SEE THE PAGE CLINICIAN Would actionable C. difficile test results in less than 30 minutes improve patient
C. DIFF QUIK CHEK COMPLETE Get the complete diagnostic picture with just one test. TAP HERE TO SEE THE PAGE CLINICIAN Would actionable C. difficile test results in less than 30 minutes improve patient
Zinplava. (bezlotoxumab) New Product Slideshow
 New Product Slideshow") Zinplava (bezlotoxumab) New Product Slideshow Introduction Brand name: Zinplava Generic name: Bezlotoxumab Pharmacological class: Human IgG1 monoclonal antibody Strength and Formulation: 25mg/mL; solution
Zinplava (bezlotoxumab) New Product Slideshow Introduction Brand name: Zinplava Generic name: Bezlotoxumab Pharmacological class: Human IgG1 monoclonal antibody Strength and Formulation: 25mg/mL; solution
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013
 Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
Division of GIM Lecture Series Case Presentation David A. Erickson, M.D October 9th, 2013 Financial Disclosures No financial disclosures Objectives Review a case of recurrent Clostridium difficile infection
DUKE ANTIMICROBIAL STEWARDSHIP OUTREACH NETWORK (DASON) Antimicrobial Stewardship News. Volume 3, Number 6, June 2015
 Antimicrobial Stewardship News. Volume 3, Number 6, June 2015") DUKE ANTIMICROBIAL STEWARDSHIP OUTREACH NETWORK (DASON) Antimicrobial Stewardship News Volume 3, Number 6, June 2015 Diagnostic Testing for Clostridium difficile Infection Background Clostridium difficile
DUKE ANTIMICROBIAL STEWARDSHIP OUTREACH NETWORK (DASON) Antimicrobial Stewardship News Volume 3, Number 6, June 2015 Diagnostic Testing for Clostridium difficile Infection Background Clostridium difficile
3/23/2012. Impact of Laboratory Testing on Detection and Treatment of Healthcare Associated Infection: The Case of CDI
 Impact of Laboratory Testing on Detection and Treatment of Healthcare Associated Infection: The Case of CDI L. Clifford McDonald, MD Lance R. Peterson, MD March 27, 2012 1 Potential COI L. Clifford McDonald,
Impact of Laboratory Testing on Detection and Treatment of Healthcare Associated Infection: The Case of CDI L. Clifford McDonald, MD Lance R. Peterson, MD March 27, 2012 1 Potential COI L. Clifford McDonald,
Clostridium Difficile Infection in Adults Treatment and Prevention
 Clostridium Difficile Infection in Adults Treatment and Prevention Definition: Clostridium Difficile colonizes the human intestinal tract after the normal gut flora has been altered by antibiotic therapy
Clostridium Difficile Infection in Adults Treatment and Prevention Definition: Clostridium Difficile colonizes the human intestinal tract after the normal gut flora has been altered by antibiotic therapy
CDI The Impact. Disclosures. Acknowledgments. Objectives and Agenda. What s in the Name? 11/14/2012. Lets Talk Numbers
 Disclosures No conflict of interest to declare Acknowledgments Objectives and Agenda Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA) Guidelines
Disclosures No conflict of interest to declare Acknowledgments Objectives and Agenda Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA) Guidelines
Can We Prevent All Healthcare- Associated Clostridium difficile infections in 10 Years?
 Can We Prevent All Healthcare- Associated Clostridium difficile infections in 10 Years? Curtis Donskey, M.D. Louis Stokes VA Medical Center Cleveland, Ohio Research support: Clorox, EcoLab, GOJO, Merck,
Can We Prevent All Healthcare- Associated Clostridium difficile infections in 10 Years? Curtis Donskey, M.D. Louis Stokes VA Medical Center Cleveland, Ohio Research support: Clorox, EcoLab, GOJO, Merck,
Long-Term Care Updates
 Long-Term Care Updates April 2017 Bezlotoxumab to Prevent Recurrent Infection By Amy Wilson, PharmD and Zara Risoldi Cochrane, PharmD, MS, FASCP Introduction The Gram-positive bacteria is a common cause
Long-Term Care Updates April 2017 Bezlotoxumab to Prevent Recurrent Infection By Amy Wilson, PharmD and Zara Risoldi Cochrane, PharmD, MS, FASCP Introduction The Gram-positive bacteria is a common cause
Clostridium difficile Infection (CDI) Guideline
 Guideline") Clostridium difficile Infection (CDI) Guideline Site Applicability All VCH PHC acute care and residential sites. Practice Level Physicians basic skill Pharmacists basic skill Nurses (RN, LPN, RPN) basic
Clostridium difficile Infection (CDI) Guideline Site Applicability All VCH PHC acute care and residential sites. Practice Level Physicians basic skill Pharmacists basic skill Nurses (RN, LPN, RPN) basic
CLOSTRIDIUM DIFICILE. Negin N Blattman Infectious Diseases Phoenix VA Healthcare System
 CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
CLOSTRIDIUM DIFICILE Negin N Blattman Infectious Diseases Phoenix VA Healthcare System ANTIBIOTIC ASSOCIATED DIARRHEA 1978: C diff first identified 1989-1992: Four large outbreaks in the US caused by J
The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH
 The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH Some history first Clostridium difficile, a spore-forming gram-positive (i.e., thick
The Epidemiology of Clostridium difficile DANIEL SAMAN, DRPH, MPH RESEARCH SCIENTIST ESSENTIA INSTITUTE OF RURAL HEALTH Some history first Clostridium difficile, a spore-forming gram-positive (i.e., thick
New Molecular Diagnostic Assays for Solana Performance Assessment, Workflow Analysis, and Clinical Utility
 New Molecular Diagnostic Assays for Solana Performance Assessment, Workflow Analysis, and Clinical Utility Gerald A. Capraro, Ph.D., D(ABMM) Director, Clinical Microbiology Carolinas Pathology Group Atrium
New Molecular Diagnostic Assays for Solana Performance Assessment, Workflow Analysis, and Clinical Utility Gerald A. Capraro, Ph.D., D(ABMM) Director, Clinical Microbiology Carolinas Pathology Group Atrium
Questions and answers about the laboratory diagnosis of Clostridium difficile infection (CDI)
") Questions and answers about the laboratory diagnosis of Clostridium difficile infection (CDI) The NHS Centre for Evidence based Purchasing (CEP) has published the results of an evaluation of the performance
Questions and answers about the laboratory diagnosis of Clostridium difficile infection (CDI) The NHS Centre for Evidence based Purchasing (CEP) has published the results of an evaluation of the performance
500,000 29,000. New 2015 Data. Lessa et al, N Eng J Med 2015: 34.2% of CDI cases were considered community-acquired
 Cost-effective Treatment of Clostridium difficile Infection in the ICU Kevin W. Garey, PharmD, MS. Professor and Chair University of Houston College of Pharmacy New 2015 Data 500,000 29,000 Lessa et al,
Cost-effective Treatment of Clostridium difficile Infection in the ICU Kevin W. Garey, PharmD, MS. Professor and Chair University of Houston College of Pharmacy New 2015 Data 500,000 29,000 Lessa et al,
Learning Objectives. A Critical Analysis of Recent Fidaxomicin & Nesiritide Trials. Fidaxomicin vs. Vancomycin. Outline 1/3/2012
 Learning Objectives A Critical Analysis of Recent Fidaxomicin & Nesiritide Trials Amy E. Lodolce, PharmD, BCPS Assistant Director, Drug Information Group UIC College of Pharmacy Describe the methods and
Learning Objectives A Critical Analysis of Recent Fidaxomicin & Nesiritide Trials Amy E. Lodolce, PharmD, BCPS Assistant Director, Drug Information Group UIC College of Pharmacy Describe the methods and
Patient presentation
 Update: Clostridium difficile Colitis David H. Kerman, MD Assistant Professor of Clinical Medicine Director, Fellowship Program Division of Gastroenterology University of Miami Miller School of Medicine
Update: Clostridium difficile Colitis David H. Kerman, MD Assistant Professor of Clinical Medicine Director, Fellowship Program Division of Gastroenterology University of Miami Miller School of Medicine
EPIDEMIOLOGY AND PREVENTION OF CLOSTRIDIUM DIFFICILE INFECTION (CDI)
") EPIDEMIOLOGY AND PREVENTION OF CLOSTRIDIUM DIFFICILE INFECTION (CDI) David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics & Epidemiology Associate Chief Medical Offer, UNC Health Care Medical
EPIDEMIOLOGY AND PREVENTION OF CLOSTRIDIUM DIFFICILE INFECTION (CDI) David Jay Weber, M.D., M.P.H. Professor of Medicine, Pediatrics & Epidemiology Associate Chief Medical Offer, UNC Health Care Medical
Clostridium DifficileInfection & Readmissions: An ounce of prevention is worth a pound of cure
 Clostridium DifficileInfection & Readmissions: An ounce of prevention is worth a pound of cure Brian S. Zuckerbraun, MD, FACS Henry T. Bahnson Professor of Surgery University of Pittsburgh Chief, Trauma
Clostridium DifficileInfection & Readmissions: An ounce of prevention is worth a pound of cure Brian S. Zuckerbraun, MD, FACS Henry T. Bahnson Professor of Surgery University of Pittsburgh Chief, Trauma
Ongoing Developments in Management of Clostridium difficile Infection
 Ongoing Developments in Management of Clostridium difficile Infection Infectious Diseases Spring Symposium Creighton University School of Medicine April 28, 2018, Omaha, NB Stuart Johnson, MD Loyola U.
Ongoing Developments in Management of Clostridium difficile Infection Infectious Diseases Spring Symposium Creighton University School of Medicine April 28, 2018, Omaha, NB Stuart Johnson, MD Loyola U.
DETECTION OF TOXIGENIC CLOSTRIDIUM DIFFICILE
 CLINICAL GUIDELINES For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS DETECTION OF TOXIGENIC CLOSTRIDIUM DIFFICILE Policy Number: PDS 021 Effective Date:
CLINICAL GUIDELINES For use with the UnitedHealthcare Laboratory Benefit Management Program, administered by BeaconLBS DETECTION OF TOXIGENIC CLOSTRIDIUM DIFFICILE Policy Number: PDS 021 Effective Date:
Drug Class Update with New Drug Evaluation: Medications for Clostridium difficile Infection
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Updates to pharmacological management in the prevention of recurrent Clostridium difficile
 Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Updates to pharmacological management in the prevention of recurrent Clostridium difficile Julia Shlensky, PharmD PGY2 Internal Medicine Resident September 12, 2017 2017 MFMER slide-1 Clinical Impact Increasing
Los Angeles County Department of Public Health: Your Partner in CDI Prevention
 Los Angeles County Department of Public Health: Your Partner in CDI Prevention Dawn Terashita, MD, MPH Acute Communicable Disease Control Los Angeles County Department of Public Health dterashita@ph.lacounty.gov
Los Angeles County Department of Public Health: Your Partner in CDI Prevention Dawn Terashita, MD, MPH Acute Communicable Disease Control Los Angeles County Department of Public Health dterashita@ph.lacounty.gov
An Oral Fecal Transplant for Lunch?- Frankly Speaking EP 53
 An Oral Fecal Transplant for Lunch?- Frankly Speaking EP 53 Transcript Details This is a transcript of an episode from the podcast series Frankly Speaking accessible at Pri- Med.com. Additional media formats
An Oral Fecal Transplant for Lunch?- Frankly Speaking EP 53 Transcript Details This is a transcript of an episode from the podcast series Frankly Speaking accessible at Pri- Med.com. Additional media formats
Labeled Uses: Treatment of Clostiridum Difficile associated diarrhea (CDAD)
") Brand Name: Dificid Generic Name: fidaxomicin Manufacturer 1,2,3,4,5 : Optimer Pharmaceuticals, Inc. Drug Class 1,2,3,4,5 : Macrolide Antibiotic Uses 1,2,3,4,5 : Labeled Uses: Treatment of Clostiridum
Brand Name: Dificid Generic Name: fidaxomicin Manufacturer 1,2,3,4,5 : Optimer Pharmaceuticals, Inc. Drug Class 1,2,3,4,5 : Macrolide Antibiotic Uses 1,2,3,4,5 : Labeled Uses: Treatment of Clostiridum
Disclosure. Objectives. Assessment Questions. History. Clinical Case 2/27/2015. Clostridium difficile update and new therapies
 Disclosure Clostridium difficile update and new therapies Corey Frederick, PharmD PGY-2 Pharmacy Resident, Infectious Diseases Jackson Memorial Hospital Miami, Florida I do not have a vested interest in
Disclosure Clostridium difficile update and new therapies Corey Frederick, PharmD PGY-2 Pharmacy Resident, Infectious Diseases Jackson Memorial Hospital Miami, Florida I do not have a vested interest in
Update on Clostridium difficile infection.
 Update on Clostridium difficile infection. K. Honein Gastroenterologist, HDF Associate Professor Head of Medicine Department St Joseph University-Beirut. Introduction Gram+anaerobic bacillus responsible
Update on Clostridium difficile infection. K. Honein Gastroenterologist, HDF Associate Professor Head of Medicine Department St Joseph University-Beirut. Introduction Gram+anaerobic bacillus responsible
TITLE OF PRESENTATION
 TITLE OF PRESENTATION Can C. Subtitle difficile of Infection Presentation Rates Be Used to Judge Prevention Success for Hospitals? David P. Calfee, MD, MS Associate Professor of Medicine and Public Health
TITLE OF PRESENTATION Can C. Subtitle difficile of Infection Presentation Rates Be Used to Judge Prevention Success for Hospitals? David P. Calfee, MD, MS Associate Professor of Medicine and Public Health
The incubation period is unknown. However; the onset of clinical disease is typically 5-10 days after initiation of antimicrobial treatment.
 C. DIFFICILE Case definition CONFIRMED CASE A patient is defined as a case if they are one year of age or older AND have one of the following requirements: A laboratory confirmation of a positive toxin
C. DIFFICILE Case definition CONFIRMED CASE A patient is defined as a case if they are one year of age or older AND have one of the following requirements: A laboratory confirmation of a positive toxin
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition Joint Session with ACOFP and Cleveland
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition Joint Session with ACOFP and Cleveland
! MQ is a 44 year old woman that I first saw in Sept ! In MVA in Jan 2003 requiring spinal surgery
 Case MQ is a 44 year old woman that I first saw in Sept 2006 UPDATE ON CLOSTRIDIUM DIFFICILE DISEASE Richard A. Jacobs, M.D.,PhD In MVA in Jan 2003 requiring spinal surgery Subsequently developed fecal
Case MQ is a 44 year old woman that I first saw in Sept 2006 UPDATE ON CLOSTRIDIUM DIFFICILE DISEASE Richard A. Jacobs, M.D.,PhD In MVA in Jan 2003 requiring spinal surgery Subsequently developed fecal
The Bristol Stool Scale and Its Relationship to Clostridium difficile Infection
 JCM Accepts, published online ahead of print on 16 July 2014 J. Clin. Microbiol. doi:10.1128/jcm.01303-14 Copyright 2014, American Society for Microbiology. All Rights Reserved. 1 The Bristol Stool Scale
JCM Accepts, published online ahead of print on 16 July 2014 J. Clin. Microbiol. doi:10.1128/jcm.01303-14 Copyright 2014, American Society for Microbiology. All Rights Reserved. 1 The Bristol Stool Scale
Le infezioni da Clostridium difficile, gravi, ricorrenti e complicate Nicola Petrosillo
 Le infezioni da Clostridium difficile, gravi, ricorrenti e complicate Nicola Petrosillo Istituto Nazionale per le Malattie Infettive «lazzaro Spallanzani», IRCCS-Roma The infectious cycle of transmission
Le infezioni da Clostridium difficile, gravi, ricorrenti e complicate Nicola Petrosillo Istituto Nazionale per le Malattie Infettive «lazzaro Spallanzani», IRCCS-Roma The infectious cycle of transmission
Managing Clostridium Difficile: An Old Bug With
 932 The Red Section see related editorial on page x Managing Clostridium Difficile: An Old Bug With New Tricks Stephen M. Vindigni, MD, MPH 1,2 and Christina M. Surawicz, MD 1 Am J Gastroenterol (2018)
932 The Red Section see related editorial on page x Managing Clostridium Difficile: An Old Bug With New Tricks Stephen M. Vindigni, MD, MPH 1,2 and Christina M. Surawicz, MD 1 Am J Gastroenterol (2018)
Probiotics for Primary Prevention of Clostridium difficile Infection
 Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
Probiotics for Primary Prevention of Clostridium difficile Infection Objectives Review risk factors for Clostridium difficile infection (CDI) Describe guideline recommendations for CDI prevention Discuss
Clostridium difficile Essential information
 Clostridium difficile Essential information Clostridium difficile Origins Clostridium difficile (C. diff) is a Gram positive, spore forming, anaerobic bacterium with a rod structure. It was first identified
Clostridium difficile Essential information Clostridium difficile Origins Clostridium difficile (C. diff) is a Gram positive, spore forming, anaerobic bacterium with a rod structure. It was first identified
C. difficile and ASP Guidelines and Best Practices. Belinda Ostrowsky, MD, MPH, FSHEA, FIDSA February 27 and 28, 2018
 C. difficile and ASP Guidelines and Best Practices Belinda Ostrowsky, MD, MPH, FSHEA, FIDSA February 27 and 28, 2018 Disclosure I have no financial disclosures I have made a recent transition from Montefiore
C. difficile and ASP Guidelines and Best Practices Belinda Ostrowsky, MD, MPH, FSHEA, FIDSA February 27 and 28, 2018 Disclosure I have no financial disclosures I have made a recent transition from Montefiore
Objectives Clostridium difficile Infections, So Many Tests, Which One to Choose?
 Objectives Clostridium difficile Infections, So Many Tests, Which One to Choose? March 9, 0 http://www.slh.wisc.edu/outreach-data/event-detail.php?id=03 Raymond P. Podzorski, Ph.D., D(ABMM) Clinical Microbiologist
Objectives Clostridium difficile Infections, So Many Tests, Which One to Choose? March 9, 0 http://www.slh.wisc.edu/outreach-data/event-detail.php?id=03 Raymond P. Podzorski, Ph.D., D(ABMM) Clinical Microbiologist
L infezione da Clostridium difficile (CDI) Quadri clinici e nuovi approcci terapeutici
 Quadri clinici e nuovi approcci terapeutici") L infezione da Clostridium difficile (CDI) Quadri clinici e nuovi approcci terapeutici Roberto Luzzati SC Malattie Infettive, AOU Trieste Presidente :Prof. Enzo Raise Clinical presentation of infection
L infezione da Clostridium difficile (CDI) Quadri clinici e nuovi approcci terapeutici Roberto Luzzati SC Malattie Infettive, AOU Trieste Presidente :Prof. Enzo Raise Clinical presentation of infection
An APIC Guide 2008 Guide to the Elimination of Clostridium difficile in Healthcare Settings
 An APIC Guide 2008 Guide to the Elimination of Clostridium difficile in Healthcare Settings About APIC APIC s mission is to improve health and patient safety by reducing risks of infection and other adverse
An APIC Guide 2008 Guide to the Elimination of Clostridium difficile in Healthcare Settings About APIC APIC s mission is to improve health and patient safety by reducing risks of infection and other adverse
CLOSTRIDIUM DIFFICILE: IMPROVING DIAGNOSIS AND TREATMENT. Joshua T. Watson, M.D. Lowcountry Gastroenterology Associates
 CLOSTRIDIUM DIFFICILE: IMPROVING DIAGNOSIS AND TREATMENT Joshua T. Watson, M.D. Lowcountry Gastroenterology Associates Learning Objectives Recognize patients who are highest risk for C. diff infections
CLOSTRIDIUM DIFFICILE: IMPROVING DIAGNOSIS AND TREATMENT Joshua T. Watson, M.D. Lowcountry Gastroenterology Associates Learning Objectives Recognize patients who are highest risk for C. diff infections
Nursing Infectious Diseases Topics. David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle
 Nursing Infectious Diseases Topics David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Clostridium difficile Free Access Via Web Source: Cohen SH,
Nursing Infectious Diseases Topics David H. Spach, MD Professor of Medicine Division of Infectious Diseases University of Washington, Seattle Clostridium difficile Free Access Via Web Source: Cohen SH,
Clostridium difficile Asymptomatic Carriers The Hidden Part of the Iceberg?
 Clostridium difficile Asymptomatic Carriers The Hidden Part of the Iceberg? Disclosures Merck Canada, BD Diagnostics, AMD Medical, Canadian Institute for Health Research Merck Canada, Pfizer OBJECTIVES
Clostridium difficile Asymptomatic Carriers The Hidden Part of the Iceberg? Disclosures Merck Canada, BD Diagnostics, AMD Medical, Canadian Institute for Health Research Merck Canada, Pfizer OBJECTIVES
What s New for Clostridium difficile John Lynch MD MPH Harborview Medical Center University of Washington
 What s New for Clostridium difficile 2013 John Lynch MD MPH Harborview Medical Center University of Washington Pathogenic Mechanisms of Diarrhea Toxins: Preformed: S aureus, C perfringens, B cereus Formed
What s New for Clostridium difficile 2013 John Lynch MD MPH Harborview Medical Center University of Washington Pathogenic Mechanisms of Diarrhea Toxins: Preformed: S aureus, C perfringens, B cereus Formed
Clostridium difficile infections: Drug treatment re-evaluated
 Clostridium difficile infections: Drug treatment re-evaluated Kimberly D. Leuthner, PharmD University Medical Center of Southern Nevada August 11, 2016 Random Fact: The human body has 10 13 human cells
Clostridium difficile infections: Drug treatment re-evaluated Kimberly D. Leuthner, PharmD University Medical Center of Southern Nevada August 11, 2016 Random Fact: The human body has 10 13 human cells
Round Robin Highlights of Infection Control Practices
 Round Robin Highlights of Infection Control Practices Arkansas Department of Health Healthcare-Associated Infections Program Staff To Isolate or Not To Isolate: That Is The Question Kelley Garner, MPH,
Round Robin Highlights of Infection Control Practices Arkansas Department of Health Healthcare-Associated Infections Program Staff To Isolate or Not To Isolate: That Is The Question Kelley Garner, MPH,
Understanding C. diff. atomalliance.org/cdifftraining
 Understanding C. diff atomalliance.org/cdifftraining This booklet is a printed guide of the online educational resource atomalliance.org/cdifftraining Target Audience Understanding C. diff This educational
Understanding C. diff atomalliance.org/cdifftraining This booklet is a printed guide of the online educational resource atomalliance.org/cdifftraining Target Audience Understanding C. diff This educational
JMSCR Vol 05 Issue 07 Page July 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i7.15 Rapid Diagnosis of Toxigenic Clostridium
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-0450 DOI: https://dx.doi.org/10.18535/jmscr/v5i7.15 Rapid Diagnosis of Toxigenic Clostridium
Literature Scan: Antibiotics for Clostridium difficile Infection. Month/Year of Review: May 2015 Date of Last Review: April 2012
 Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Copyright 2012 Oregon State University. All Rights Reserved Drug Use Research & Management Program Oregon State University, 500 Summer Street NE, E35 Salem, Oregon 97301-1079 Phone 503-947-5220 Fax 503-947-1119
Does Empirical Clostridium difficile Infection (CDI) Therapy Result in False-Negative CDI Diagnostic Test Results?
 Therapy Result in False-Negative CDI Diagnostic Test Results?") MAJOR ARTICLE Does Empirical Clostridium difficile Infection (CDI) Therapy Result in False-Negative CDI Diagnostic Test Results? Venkata C. K. Sunkesula, 1 Sirisha Kundrapu, 1 Christine Muganda, 3 Ajay
MAJOR ARTICLE Does Empirical Clostridium difficile Infection (CDI) Therapy Result in False-Negative CDI Diagnostic Test Results? Venkata C. K. Sunkesula, 1 Sirisha Kundrapu, 1 Christine Muganda, 3 Ajay
Clostridium difficile
 Clostridium difficile Alex Aspinall MD, PhD, FRCPC Clinical Assistant Professor, University of Calgary Division of Gastroenterology and Hepatology, South Health Campus www.seacourses.com 1 Learning Points
Clostridium difficile Alex Aspinall MD, PhD, FRCPC Clinical Assistant Professor, University of Calgary Division of Gastroenterology and Hepatology, South Health Campus www.seacourses.com 1 Learning Points
C. DIFFICILE UPDATE. Heather Bell, DO Infectious Diseases Physician
 C. DIFFICILE UPDATE Heather Bell, DO Infectious Diseases Physician None to report DISCLOSURE Case review Review IDSA CDI guidelines discuss changes Questions Testing recommendations Treatment recommendations
C. DIFFICILE UPDATE Heather Bell, DO Infectious Diseases Physician None to report DISCLOSURE Case review Review IDSA CDI guidelines discuss changes Questions Testing recommendations Treatment recommendations
Clostridium difficile (C difficile)
") Patient Knowledge and Attitudes About for Clostridium difficile Infection Colin Goodman, MD; Nicholas O Rourke, PharmD; Carla Amundson, MA; and Dimitri Drekonja, MD, MS In a survey of patients with Clostridium
Patient Knowledge and Attitudes About for Clostridium difficile Infection Colin Goodman, MD; Nicholas O Rourke, PharmD; Carla Amundson, MA; and Dimitri Drekonja, MD, MS In a survey of patients with Clostridium
Clostridiodes Difficile Colitis: Update on Guidelines. Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018
 Clostridiodes Difficile Colitis: Update on Guidelines Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018 Outline Overview of CDI Diagnosis of C Difficile- updates Infection Prevention
Clostridiodes Difficile Colitis: Update on Guidelines Jade Le, MD Texas Health Physicians Group No disclosures April 6, 2018 Outline Overview of CDI Diagnosis of C Difficile- updates Infection Prevention
Patient Safety Summit 2014
 Patient Safety Summit 2014 The War on C Diff Mark Mellow, MD + C Diff The Organism Gram + bacillus Anaerobic Spore forming Intestinal flora (up to 35% hospitalized patients, 3% of healthy adults) Leading
Patient Safety Summit 2014 The War on C Diff Mark Mellow, MD + C Diff The Organism Gram + bacillus Anaerobic Spore forming Intestinal flora (up to 35% hospitalized patients, 3% of healthy adults) Leading
Original Article. Infection Control & Hospital Epidemiology (2019), 1 5 doi: /ice
, 1 5 doi: /ice") Infection Control & Hospital Epidemiology (2019), 1 5 doi:10.1017/ice.2018.347 Original Article Healthcare provider diagnostic testing practices for identification of Clostridioides (Clostridium) difficile
Infection Control & Hospital Epidemiology (2019), 1 5 doi:10.1017/ice.2018.347 Original Article Healthcare provider diagnostic testing practices for identification of Clostridioides (Clostridium) difficile
HEALTHCARE- ASSOCIATED INFECTIONS: A FOCUS ON Clostridium difficile
 OBJECTIVES HEALTHCARE- ASSOCIATED INFECTIONS: A FOCUS ON Clostridium difficile Identify and describe the pathophysiology of C. diff. Identify and describe current therapies in treatment of C. diff Identify
OBJECTIVES HEALTHCARE- ASSOCIATED INFECTIONS: A FOCUS ON Clostridium difficile Identify and describe the pathophysiology of C. diff. Identify and describe current therapies in treatment of C. diff Identify
Impact of clinical symptoms on interpretation of diagnostic assays for Clostridium difficile infections
 Washington University School of Medicine Digital Commons@Becker Open Access Publications 2011 Impact of clinical symptoms on interpretation of diagnostic assays for Clostridium difficile infections Erik
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2011 Impact of clinical symptoms on interpretation of diagnostic assays for Clostridium difficile infections Erik
Clinical. Clostridium Difficile: Standard Operating Procedure. Document Control Summary. Contents
 Clinical Clostridium Difficile: Standard Operating Procedure Document Control Summary Status: Version: Author/Title: Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
Clinical Clostridium Difficile: Standard Operating Procedure Document Control Summary Status: Version: Author/Title: Owner/Title: Approved by: Ratified: Related Trust Strategy and/or Strategic Aims Implementation
Clostridioides difficile Infection: What s the BIG Stink?
 Clostridioides difficile Infection: What s the BIG Stink? GLORIA MATHIS, RN, BSN, CIC 29 TH ANNUAL MEDICAL SURGICAL CONFERENCE APRIL 4, 2019 SAN FRANCISCO, CA I am sre my patient has C. diff. I cold smell
Clostridioides difficile Infection: What s the BIG Stink? GLORIA MATHIS, RN, BSN, CIC 29 TH ANNUAL MEDICAL SURGICAL CONFERENCE APRIL 4, 2019 SAN FRANCISCO, CA I am sre my patient has C. diff. I cold smell