A rare case of intestinal obstruction due to internal hernia. Dr. Jayanth 3 rd year PG Dept. Of General Surgery
|
|
|
- Paulina Dickerson
- 5 years ago
- Views:
Transcription
1 A rare case of intestinal obstruction due to internal hernia Dr. Jayanth 3 rd year PG Dept. Of General Surgery
2 One of the common cause of acute abdomen May lead to high morbidity and mortality if not treated correctly It can be classified into two types: Dynamic (mechanical) Adynamic
3 Dynamic: where peristalsis is working against a mechanical obstruction. Adynamic: mechanical element is absent - Peristalsis may be absent(paralytic ileus) -May be present in non propulsive form. (mesenteric vascular occlusion or pseudoobstruction)
4 Cause of obstruction DYNAMIC 1.Intraluminal: impacted faeces, foreign bodies, gallstones, Bezoars. 2.Intramural: tumors, inflammatory strictures, 3.Extramural: adhesion, hernias, volvulus, intussusception, tumors
5 Adhesions- 40% Tumors -15% Inflamatory- 15% Hernia-12% Intraluminal-10% Miscellaneous -8%


6
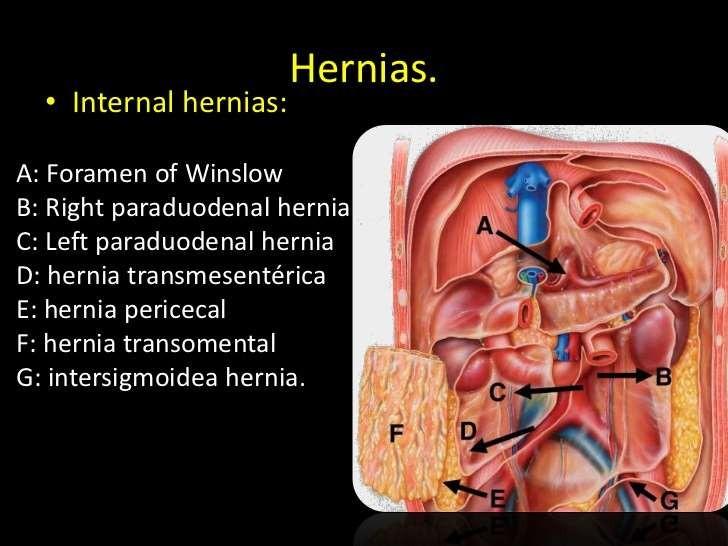
7 Definition Internal hernias are defined by the protrusion of a viscus through a normal or abnormal peritoneal or mesenteric aperture with in the confines of the peritoneal cavity. The hernia orifice is usually a preexisting foramen, recess, and fossa but can be foramen, recess, and fossa where the cause is due to surgery, ischemia, and trauma caused by surgery, ischemia, and trauma.
8
9 Classification Internal hernias are classified as 1. Congenital 2. Acquired
10 In the broad category of internal hernias are several main types, as traditionally described by Meyers, based on location. Using historical data, these consist of Paraduodenal (53%), Pericecal (13%), Foramen of Winslow (8%), Transmesenteric and Transmesocolic (8%), Intersigmoid (6%), Retroanastomotic (5%), 7% described by Meyers included paravesical hernias, which are not true internal hernias
11
12 PARADUODENAL HERNIA
13 Paraduodenal fossae originate as congenital peritoneal anomalies due to failure of mesenteric fusion of parietal peritoneum and an associated abnormal peritoneum along with associated abnormal rotation as the small bowel is imprisoned beneath the developing colon
14 In the classic older literature, paraduodenal hernias were the most common type of internal hernia, accounting for approximately 53% of all cases. Unlike most types of internal hernias, this sub type does have a sex predilection, being found more commonly in men by a ratio of 3:1. There are two main types, left and right, with the former consisting of most (75%) cases.
15 PARADUODENAL HERNIA Pathogenesis: 1)Increased intra abdominal pressure pushes bowel into potential sac 2)Congenital anomaly in development of the peritoneum that arises during midgut rotation

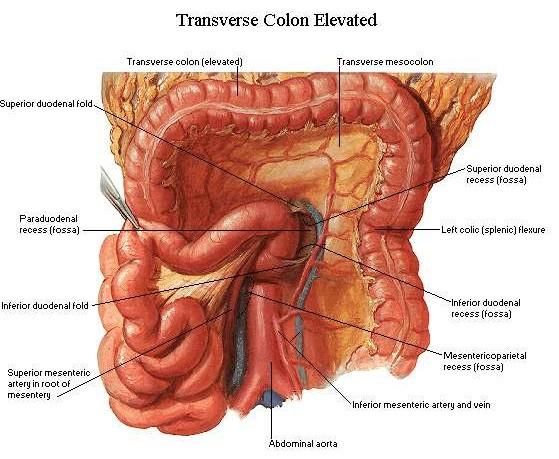
16 Left Paraduodenal hernia Left paraduodenal hernias have an overall incidence of approximately 40% of all internal hernias. They occur when bowel prolapses through Landzert's fossa, an aperture present in approximately 2% of the population. These hernias therefore can be classified as a congenital type, normal aperture subtype.
17 Landzert's fossa is located behind the fourth part of the duodenum and is formed by the lifting up of a peritoneal fold by the inferior mesenteric vein and ascending left colic artery as they run along the lateral side of the fossa. Small-bowel loops prolapse postero inferiorly through the fossa to the left of the fourth part of the duodenum into the left portion of the transverse mesocolon and descending mesocolon.
18 Left Paraduodenal hernia Lt.paraduodenal hernia borders Ant Part of orifice--imv, post part--post abd wall, contains most of small bowel Afferent limb-4th part of duodenum Efferent limb-terminal part of ileum.
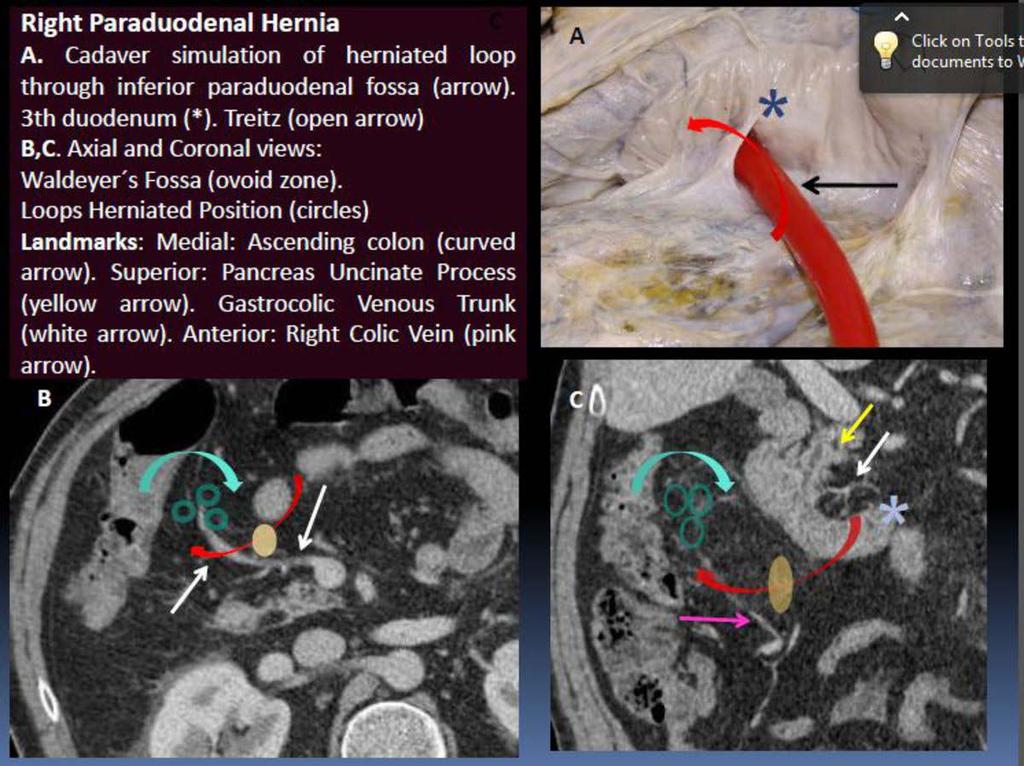
19 Right Paraduodenal hernia Right paraduodenal hernias have an overall incidence of approximately 13% and occur when bowel herniates through Waldeyer s fossa. This normal yet uncommon recess is found in less than 1% of the population. Like left paraduodenal hernias, the right paraduodenal hernia can be classified as congenital type, normal aperture subtype.

20 In these situations, the herniated contents are located in the right half of the transverse mesocolon and behind the ascending mesocolon. This type of hernia occurs more frequently in the setting of nonrotated small bowel. When compared with the left paraduodenal hernias. Those on the right are usually larger and are more often fixed.
21 Pericaecal hernia
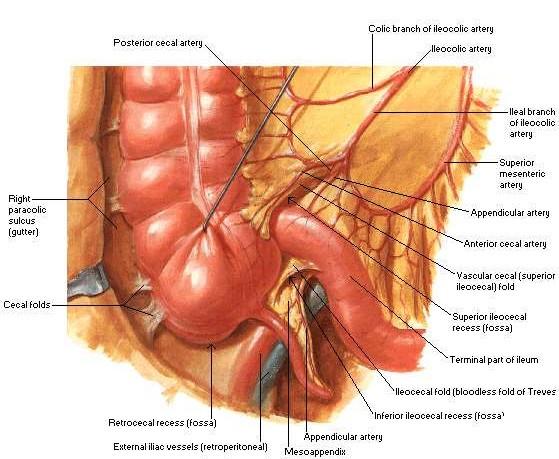
22 Historically, pericecal hernias account for 13% of all internal hernias. The pericecal fossa islocated behind the cecum and ascending colon and is limited by the parietocecal fold outward and the mesentericocecal fold inward. Although there are actually four subtypes (ileocolic, retrocecal,ileocecal, and paracecal) of pericecal hernias, most commonly the herniated loop consists of an ileal segment protruding through a defect in the cecal mesentery and extending into the right paracolic gutter.
23 These hernias can therefore be subcategorized as eith er acquired or congenital defects in the cecal mesentery. Clinically, patients with pericecal hernias present in a similar manner to those with all other types of internal hernias except for the location of pain, which tends to be in the right lower quadrant, so that pericecal hernias are sometimes mistaken for appendiceal abnormalities. A higher incidence of occlusive symptoms with rapid progression to strangulation is also commonly found, with a mortality rate reported to be as high as75%
24 Retrocaecal hernia(hernia of Rieux) Caused by a partial defect of fixation of the right ascending mesocolon (Toldt fascia). In this type of hernia, where the viscera are trapped between the abdominal posterior peritoneum on the dorsal side, the cecum ventrally, and the right ascending mesocolon as the upper limit

25 Transmesentric hernia Protrusion of a loop of bowel through the mesentery of the small bowel, the transverse mesocolon, the sigmoid mesocolon, or the falciform ligament. Congenital-associated with intestinal atresia, or mesenteric ischemia, Acquired-Most TMHs in adults are related to predisposing factors, including previous surgery, abdominal trauma, and peritonitis.

26 TRANSOMENTAL HERNIA Accounts for 1% - 4% of all internal hernias Type I - through the free edge of the Gastric omentum. Type II - through the GCL into the lesser sac Herniation of viscera,typically small bowel, through an opening in the gastrocolic omentum. The ring is formed entirely by the omentum

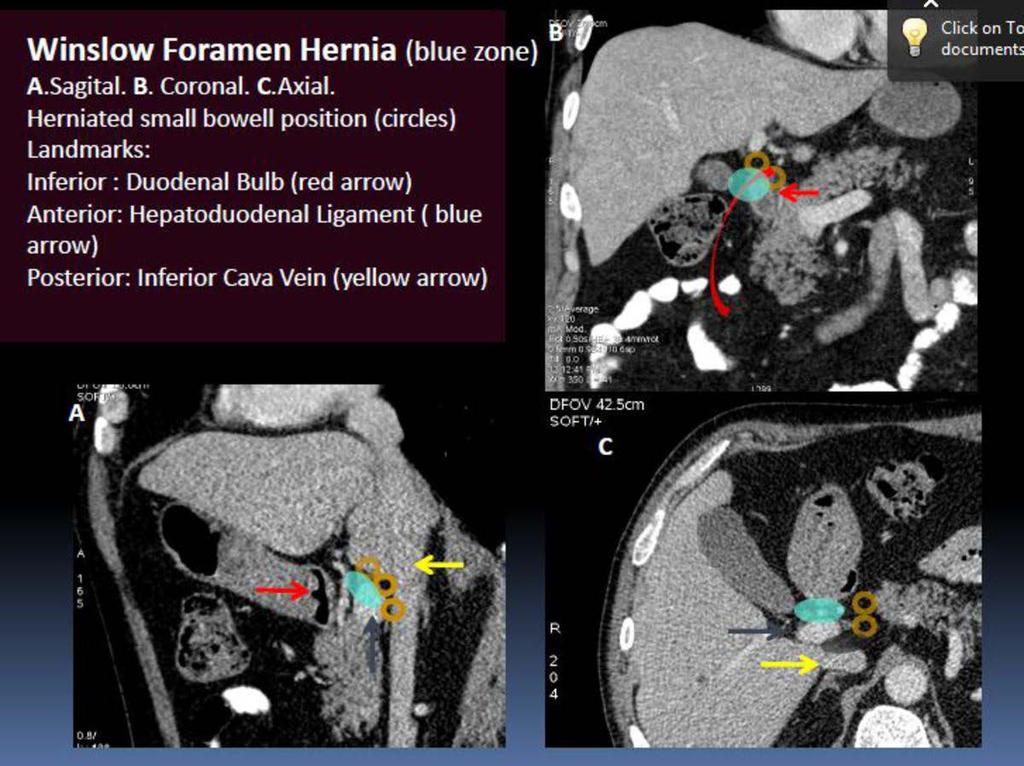
27 Hernia through epiploic foramen (Blandin hernia) 8% of all internal hernias Small bowel most frequently involved (60% ) TI, cecum, ascending colon (25-30% GB, transverse colon, and omental hernias are rare Risk factors: enlarged foramen, excessively mobile gut due to a long mesentery, persistence of the ascending mesocolon, ascending mesocolon that is not fused to the parietal peritoneum
28 Acquired internal hernia Hernia in iatrogenically created defect: 1)open and laparoscopic Roux-en-Y gastric bypass, 2)Billroth II gastrojejunostomy, 3)bilioenteric anastomosis, After the gastric bypass the hernia occur in 3 iatrogenically created space 1) the transverse mesocolon, 2)the divided small bowel mesentery, 3)the Petersen space that is located between the small bowel mesentery of the Roux limb and the transverse mesocolon.
29 Acquired internal hernia 1. The mesocolic defect (arrow A), Mesocolic / transmesenteric hernias occur through iatrogenically created defects in the mesentery. These defects include herniation of an abdominal viscus, usually through the small bowel mesentery or transverse mesocolon. These hernias are common following abdominal surgery, especially Roux-en-Y loop reconstruction

30 2. The Petersen defect (arrow B), Petersen hernias are internal hernias which occur in the potential space posterior to a gastrojejunostomy. This hernia is caused by the herniation of intestinal loops through the defect between the small bowel limbs, the transverse mesocolon and the retroperitoneum, after any type of gastrojejunostomy. 3. The enteroenterostomy defect (arrow C).
31 Symptoms of internal hernia Acute or intermittent small bowl obstruction. Pain, vomiting, distention, obstipation. Rapidly progress into shock if associated with mesenteric ischemia and bowel necrosis.
32 Investigations X ray abdomen CT abdomen CT shows Mesenteric vessels may be stretched, crowded, engorged, and have a whirl sign. Encapsulation or clustering of small bowel loops in peritoneum
33

34 A. Axial MIP view. B. Coronal view. B. Right paraduodenal dilated loops (red arrow) with stretching of gastrocolic venous trunk (white arrow) situated behind to herniated sac. Medial displacement of ascending colon (*)
 located between stomach (with arrow)and pacreatic tail (black arrow). B.")
35 Left Paraduodenal Hernia. A.Hernia sac (open arrow) located between stomach (with arrow)and pacreatic tail (black arrow). B. MIP coronal view. Twisting mesenteric vessels in the core of the herniated loops (red arrow).
36

37 CT Shows: Mesenteric swirl sign
38 Treatment Diagnostic laparoscopy Basic principles of hernia surgery, including reduction of the hernia contents, resection of the hernia sac, restoration of normal bowel anatomy, and repair of the hernia defect. If the orifice is large reduce the hernia If the orifice is narrow and associated with edematous bowel loops the best option is controlled decompression of the distended bowel to avoid the vital structures that pass through.
39
40 High index of clinical suspicion along with prompt surgical management is required in internal hernia in order to avoid a potential abdominal catastrophe. THANK YOU Reference: Shackelford.
Review of Internal Hernias: Radiographic and Clinical Findings
 Radiographic and Clinical Findings of Hernias Gastrointestinal Imaging Review C D E M N E U T R Y L I M C I G O F I N G Lucie C. Martin 1 Elmar M. Merkle William M. Thompson Martin LC, Merkle EM, Thompson
Radiographic and Clinical Findings of Hernias Gastrointestinal Imaging Review C D E M N E U T R Y L I M C I G O F I N G Lucie C. Martin 1 Elmar M. Merkle William M. Thompson Martin LC, Merkle EM, Thompson
The peritoneum. Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website:
 Website:") The peritoneum Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website: http://oluwadiya.com The peritoneum Serous membrane that lines the abdominopelvic cavity and invests the viscera The largest serous membrane
The peritoneum Prof. Oluwadiya KS, MBBS, FMCS(Orthop) Website: http://oluwadiya.com The peritoneum Serous membrane that lines the abdominopelvic cavity and invests the viscera The largest serous membrane
Nordic Forum - Trauma & Emergency Radiology. Bowel Obstruction: Imaging Update
 Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Nordic Forum - Trauma & Emergency Radiology Bowel Obstruction: Imaging Update Borut Marincek Institute of Diagnostic Radiology University Hospital Zurich, Switzerland Acute Abdomen Bowel Obstruction Bowel
Exploring Anatomy: the Human Abdomen
 Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
Exploring Anatomy: the Human Abdomen PERITONEUM AND PERITONEAL CAVITY PERITONEUM The peritoneum is a thin serous membrane that lines the abdominal cavity and covers, in variable amounts, the viscera within
Pathology of Intestinal Obstruction. Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College
 Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Pathology of Intestinal Obstruction Dr. M. Madhavan, MBBS., MD., MIAC, Professor of Pathology Saveetha Medical College Pathology of Intestinal Obstruction Objectives list the causes of intestinal obstruction
Peritoneum: Def. : It is a thin serous membrane that lines the walls of the abdominal and pelvic cavities and clothes the viscera.
 Peritoneum: Def. : It is a thin serous membrane that lines the walls of the abdominal and pelvic cavities and clothes the viscera. Layers of the peritoneum: 1. Outer Layer ( Parietal Peritoneum) : lines
Peritoneum: Def. : It is a thin serous membrane that lines the walls of the abdominal and pelvic cavities and clothes the viscera. Layers of the peritoneum: 1. Outer Layer ( Parietal Peritoneum) : lines
U Lecture Objectives. U Nordic Forum Trauma & Emergency Radiology. Bowel obstruction. U Bowel Obstruction: Etiologies
 Nordic Forum Trauma & Emergency Radiology Lecture Objectives Bowel Obstruction To illustrate the spectrum of acute obstruction of the small and the large bowel To explain how these bowel obstructions may
Nordic Forum Trauma & Emergency Radiology Lecture Objectives Bowel Obstruction To illustrate the spectrum of acute obstruction of the small and the large bowel To explain how these bowel obstructions may
Development of pancreas and Small Intestine. ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama
 Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
Development of pancreas and Small Intestine ANATOMY DEPARTMENT DR.SANAA AL-AlSHAARAWY DR.ESSAM Eldin Salama OBJECTIVES At the end of the lecture, the students should be able to : Describe the development
In the name ofgod. Abdomen 3. Dr. Zahiri
 In the name ofgod Abdomen 3 Dr. Zahiri Peritoneum Peritoneum It is the serous membrane(a type of loose connective tissue and is covered by mesothelium) that lines the abdominal cavity. Extensions of the
In the name ofgod Abdomen 3 Dr. Zahiri Peritoneum Peritoneum It is the serous membrane(a type of loose connective tissue and is covered by mesothelium) that lines the abdominal cavity. Extensions of the
Anatomy of the Large Intestine
 Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
Large intestine Anatomy of the Large Intestine 2 Large Intestine Extends from ileocecal valve to anus Length = 1.5-2.5m = 5 feet Regions Cecum = 2.5-3 inch Appendix= 3-5 inch Colon Ascending= 5 inch Transverse=
Mousa Salah. Dr. Mohammad Al. Mohtasib. 1 P a g e
 8 Mousa Salah Dr. Mohammad Al. Mohtasib 1 P a g e In the previous lecture we talked about the peritoneum, and we said that the peritonium is a serous sac, and it consists of two layers, visceral and parietal.
8 Mousa Salah Dr. Mohammad Al. Mohtasib 1 P a g e In the previous lecture we talked about the peritoneum, and we said that the peritonium is a serous sac, and it consists of two layers, visceral and parietal.
TRANSOMENTAL HERNIATION CAUSING ACUTE INTESTINAL OBSTRUCTION N. Suresh Kumar 1, Rahul Rai 2, P. Kulandai Velu 3
 TRANSOMENTAL HERNIATION CAUSING ACUTE INTESTINAL OBSTRUCTION N. Suresh Kumar 1, Rahul Rai 2, P. Kulandai Velu 3 HOW TO CITE THIS ARTICLE: N. Suresh Kumar, Rahul Rai, P. Kulandai Velu. Transomental Herniation
TRANSOMENTAL HERNIATION CAUSING ACUTE INTESTINAL OBSTRUCTION N. Suresh Kumar 1, Rahul Rai 2, P. Kulandai Velu 3 HOW TO CITE THIS ARTICLE: N. Suresh Kumar, Rahul Rai, P. Kulandai Velu. Transomental Herniation
Midgut. Over its entire length the midgut is supplied by the superior mesenteric artery
 Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
Gi Embryology 3 Midgut the midgut is suspended from the dorsal abdominal wall by a short mesentery and communicates with the yolk sac by way of the vitelline duct or yolk stalk Over its entire length the
An Interesting case of Retrocaecal internal herniation causing Small bowel Obstruction
 Accepted Manuscript An Interesting case of Retrocaecal internal herniation causing Small bowel Obstruction A.O. Rae, Core trainee,year 2 General Surgery, A. Kalyanaraman, SpR in General Surgery, A.E. Ward,
Accepted Manuscript An Interesting case of Retrocaecal internal herniation causing Small bowel Obstruction A.O. Rae, Core trainee,year 2 General Surgery, A. Kalyanaraman, SpR in General Surgery, A.E. Ward,
Case Report Multi-slice computed tomography diagnosis of left paraduodenal hernia in an adult complicated by volvulus: a case report
 Int J Clin Exp Med 2016;9(11):22428-22433 www.ijcem.com /ISSN:1940-5901/IJCEM0036446 Case Report Multi-slice computed tomography diagnosis of left paraduodenal hernia in an adult complicated by volvulus:
Int J Clin Exp Med 2016;9(11):22428-22433 www.ijcem.com /ISSN:1940-5901/IJCEM0036446 Case Report Multi-slice computed tomography diagnosis of left paraduodenal hernia in an adult complicated by volvulus:
Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER
 1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
1 Block 3: DISSECTION 2 CELIAC TRUNK, JEJUNUM/ILEUM, LARGE INTESTINE, DUODENUM, PANCREAS, PORTAL VEIN; MOBILIZATION OF THE LIVER Attempt to complete as much as you can of the dissection explained in the
Case Internal herniation with bowel ischemia after Roux-en-Y gastric bypass surgery.
 Case 14127 Internal herniation with bowel ischemia after Roux-en-Y gastric bypass surgery. Peters B 1, 2, Waked K 3, Vanhoenacker FM 1, 2, 4, Ceulemans J 5, Mespreuve M 2, 4 University Hospital Antwerp,
Case 14127 Internal herniation with bowel ischemia after Roux-en-Y gastric bypass surgery. Peters B 1, 2, Waked K 3, Vanhoenacker FM 1, 2, 4, Ceulemans J 5, Mespreuve M 2, 4 University Hospital Antwerp,
BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS
 BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS External oblique muscle Muscular portion Aponeurotic portion Superficial inguinal ring Lateral (inferior) crus Medial
BLOCK IV: OFFICIAL BODY PARTS LIST FOR ANTERIOR ABDOMINAL WALL AND ABDOMINAL CONTENTS External oblique muscle Muscular portion Aponeurotic portion Superficial inguinal ring Lateral (inferior) crus Medial
Intestinal Obstruction Clinical Presentation & Causes
 Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Intestinal Obstruction Clinical Presentation & Causes V Chidambaram-Nathan Consultant Transplant and General Surgeon Sheffield Kidney Institute Northern General Hospital Intestinal Obstruction One of the
Emergency presentation of hernias of the torso: What your surgeon wants to know.
 Emergency presentation of hernias of the torso: What your surgeon wants to know. Ken F Linnau, MD, MS Emergency Radiology UW Medicine Harborview Medical Center klinnau@uw.edu Nordic Forum 2017 Helsinki,
Emergency presentation of hernias of the torso: What your surgeon wants to know. Ken F Linnau, MD, MS Emergency Radiology UW Medicine Harborview Medical Center klinnau@uw.edu Nordic Forum 2017 Helsinki,
Para-duodenal hernia: a report of five cases and review of literature
 Shadhu et al. BMC Surgery (2018) 18:32 https://doi.org/10.1186/s12893-018-0365-8 CASE REPORT Para-duodenal hernia: a report of five cases and review of literature Kamleshsingh Shadhu 1,2, Dadhija Ramlagun
Shadhu et al. BMC Surgery (2018) 18:32 https://doi.org/10.1186/s12893-018-0365-8 CASE REPORT Para-duodenal hernia: a report of five cases and review of literature Kamleshsingh Shadhu 1,2, Dadhija Ramlagun
Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help. Print this Page Add to my Bookmarks Page 3 of 10
 Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Welcome Kristin Ingstrup [ Logout ] SEARCH Home FAQ Archives ABP Topics NeoReviews.org My Bookmarks CME Information Help Overview Editorial Board My Learning Plan January February March May June July August
Complications after laparoscopic gastric bypass for morbid obesity. Background LGBP. Eirik Hornes Halvorsen, MD, PhD Oslo
 Complications after laparoscopic gastric bypass for morbid obesity Eirik Hornes Halvorsen, MD, PhD Oslo 20.05.2015 Background Ca 3000 patients are surgically treated for morbid obesity in Norway each year.
Complications after laparoscopic gastric bypass for morbid obesity Eirik Hornes Halvorsen, MD, PhD Oslo 20.05.2015 Background Ca 3000 patients are surgically treated for morbid obesity in Norway each year.
Introduction and Definitions
 Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
Bowel obstruction Introduction and Definitions Accounts for 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN
 UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
UNDERSTANDING X-RAYS: ABDOMINAL IMAGING THE ABDOMEN Radiology Enterprises radiologyenterprises@gmail.com www.radiologyenterprises.com STOMACH AND SMALL BOWEL STOMACH AND SMALL BOWEL Swallowed air is a
Development of the Digestive System. W.S. O The University of Hong Kong
 Development of the Digestive System W.S. O The University of Hong Kong Plan for the GI system Then GI system in the abdomen first develops as a tube suspended by dorsal and ventral mesenteries. Blood
Development of the Digestive System W.S. O The University of Hong Kong Plan for the GI system Then GI system in the abdomen first develops as a tube suspended by dorsal and ventral mesenteries. Blood
Embryology of the Midgut and Hind gut
 Embryology of the Midgut and Hind gut Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E-mail: abdulameerh@yahoo.com Abdominal organs www.google.co.uk/search? Development of Duodenum The
Embryology of the Midgut and Hind gut Prof. Abdulameer Al-Nuaimi E-mail: a.al-nuaimi@sheffield.ac.uk E-mail: abdulameerh@yahoo.com Abdominal organs www.google.co.uk/search? Development of Duodenum The
Patient data. Present illness. Past history. Initial Impression
 GS-ER combine meeting 報告者 :R1 王帝皓指導者 :VS 連楚明 100.12.14 Patient data 25 y/o man Visited at 23:22 Chief complain: abd pain since 5:00 pm Triage: III Vital signs: BT: 35.7, PR: 75, RR: 18, BP: 121/70 SpO2:
GS-ER combine meeting 報告者 :R1 王帝皓指導者 :VS 連楚明 100.12.14 Patient data 25 y/o man Visited at 23:22 Chief complain: abd pain since 5:00 pm Triage: III Vital signs: BT: 35.7, PR: 75, RR: 18, BP: 121/70 SpO2:
The embryonic endoderm initially is widely connected with the yolk sac. As a consequence of cephalocaudal and lateral folding, a portion of the
 DIGESTIVE SYSTEM The embryonic endoderm initially is widely connected with the yolk sac. As a consequence of cephalocaudal and lateral folding, a portion of the endoderm-lined yolk sac cavity is incorporated
DIGESTIVE SYSTEM The embryonic endoderm initially is widely connected with the yolk sac. As a consequence of cephalocaudal and lateral folding, a portion of the endoderm-lined yolk sac cavity is incorporated
The abdominal Esophagus, Stomach and the Duodenum. Prof. Oluwadiya KS
 The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
The abdominal Esophagus, Stomach and the Duodenum Prof. Oluwadiya KS www.oluwadiya.com Viscera of the abdomen Abdominal esophagus: Terminal part of the esophagus The stomach Intestines: Small and Large
To describe the liver. To list main structures in porta hepatis.
 GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
GI anatomy Lecture: 6 د. عصام طارق Objectives: To describe the liver. To list main structures in porta hepatis. To define portal system & portosystemic anastomosis. To list parts of biliary system. To
Volvulus of the Gastrointestinal Tract: x-ray and CT imaging
 Volvulus of the Gastrointestinal Tract: x-ray and CT imaging Poster No.: C-0076 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Papadaki, S. Paschalidou, S. GIANNOU ; Rethymno, CR/ 1 2 2 3 1 3
Volvulus of the Gastrointestinal Tract: x-ray and CT imaging Poster No.: C-0076 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Papadaki, S. Paschalidou, S. GIANNOU ; Rethymno, CR/ 1 2 2 3 1 3
Intestinal Obstruction
 By the Name of ALLAH the Most Gracious the Most Merciful Intestinal Obstruction د. أحمد اسامة حسن Specialist in General Surgery and Laparoscopic Surgery To be read in Bailey & Love s Short Practice of
By the Name of ALLAH the Most Gracious the Most Merciful Intestinal Obstruction د. أحمد اسامة حسن Specialist in General Surgery and Laparoscopic Surgery To be read in Bailey & Love s Short Practice of
- Tamara Wahbeh. - Fareed Khdair. 0 P a g e
 -1 - Tamara Wahbeh - - Fareed Khdair 0 P a g e GI Embryology Note: I included everything in the records and slides; anything in the slide not included in this sheet was not mentioned by the doctor during
-1 - Tamara Wahbeh - - Fareed Khdair 0 P a g e GI Embryology Note: I included everything in the records and slides; anything in the slide not included in this sheet was not mentioned by the doctor during
ABDOMEN - GI. Duodenum
 TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
TALA SALEH ABDOMEN - GI Duodenum - Notice the shape of the duodenum, it looks like capital G shape tube which extends from the pyloroduodenal junction to the duodenojejunal junction. - It is 10 inches
Preview from Notesale.co.uk Page 1 of 34
 Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Abdominal viscera and digestive tract Digestive tract Abdominal viscera comprise majority of the alimentary system o Terminal oesophagus, stomach, pancreas, spleen, liver, gallbladder, kidneys, suprarenal
Netter's Anatomy Flash Cards Section 4 List 4 th Edition
 Netter's Anatomy Flash Cards Section 4 List 4 th Edition https://www.memrise.com/course/1577335/ Section 4 Abdomen (31 cards) Plate 4-1 Bony Framework of Abdomen 1.1 Costal cartilages 1.2 Iliac crest 1.3
Netter's Anatomy Flash Cards Section 4 List 4 th Edition https://www.memrise.com/course/1577335/ Section 4 Abdomen (31 cards) Plate 4-1 Bony Framework of Abdomen 1.1 Costal cartilages 1.2 Iliac crest 1.3
Development of the Digestive System. W.S. O School of Biomedical Sciences, University of Hong Kong.
 Development of the Digestive System W.S. O School of Biomedical Sciences, University of Hong Kong. Organization of the GI tract: Foregut (abdominal part) supplied by coeliac trunk; derivatives include
Development of the Digestive System W.S. O School of Biomedical Sciences, University of Hong Kong. Organization of the GI tract: Foregut (abdominal part) supplied by coeliac trunk; derivatives include
Bushra Arafa Zayed & Hanan Jamal. - Dana AF
 - 10 - Bushra Arafa Zayed & Hanan Jamal - Dana AF - Mohammad Al Muhtaseb Notes: This sheet was written in the same order as the slides, and everything in the slides is mentioned in this sheet. Pictures
- 10 - Bushra Arafa Zayed & Hanan Jamal - Dana AF - Mohammad Al Muhtaseb Notes: This sheet was written in the same order as the slides, and everything in the slides is mentioned in this sheet. Pictures
Abdominal radiology 腹部放射線學
 Abdominal radiology 腹部放射線學 台北醫學大學 - 市立萬芳醫院 留偉順 laowilson@hotmail.com The Normal Abdominal Series Chest Supine abdomen Erect abdomen Left lateral decubitus abdomen Learning objectives Understanding normal
Abdominal radiology 腹部放射線學 台北醫學大學 - 市立萬芳醫院 留偉順 laowilson@hotmail.com The Normal Abdominal Series Chest Supine abdomen Erect abdomen Left lateral decubitus abdomen Learning objectives Understanding normal
Lectures of Human Embryology
 Lectures of Human Embryology "Body Cavities & GIT" By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D. "Anatomy and Embryology"
Lectures of Human Embryology "Body Cavities & GIT" By DR. ABDEL-MONEM AWAD HEGAZY M.B. with honor 1983, Dipl."Gynecology and Obstetrics "1989, Master "Anatomy and Embryology" 1994, M.D. "Anatomy and Embryology"
د. عصام طارق. Objectives:
 GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
GI anatomy Lecture: 5 د. عصام طارق Objectives: To describe anatomy of stomach, duodenum & pancreas. To list their main relations. To define their blood & nerve supply. To list their lymph drainage. To
Dr. Zahiri. In the name of God
 Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Dr. Zahiri In the name of God small intestine = small bowel is the part of the gastrointestinal tract Boundaries: Pylorus Ileosecal junction Function: digestion and absorption of food It receives bile
Postgastrectomy Syndromes
 Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
Postgastrectomy Syndromes Postgastrectomy syndromes are iatrogenic conditions that may arise from partial gastrectomies, independent of whether the gastric surgery was initially performed for peptic ulcer
Volvulus characterization in radiology: A review
 Volvulus characterization in radiology: A review Poster No.: C-1677 Congress: ECR 2010 Type: Topic: Educational Exhibit GI Tract Authors: C. Antunes, M. Seco, A. Canelas, C. Ruivo, C. Paulino, F. Cruz,
Volvulus characterization in radiology: A review Poster No.: C-1677 Congress: ECR 2010 Type: Topic: Educational Exhibit GI Tract Authors: C. Antunes, M. Seco, A. Canelas, C. Ruivo, C. Paulino, F. Cruz,
Applied Peritoneal Anatomy - A Pictorial review.
 Applied Peritoneal Anatomy - A Pictorial review. Poster No.: C-1925 Congress: ECR 2011 Type: Educational Exhibit Authors: R. Patel, I. Beal, K. Planche; London/UK Keywords: MR, CT, Anatomy, Abdominal wall,
Applied Peritoneal Anatomy - A Pictorial review. Poster No.: C-1925 Congress: ECR 2011 Type: Educational Exhibit Authors: R. Patel, I. Beal, K. Planche; London/UK Keywords: MR, CT, Anatomy, Abdominal wall,
ANATOMY OF THE SMALL & LARGE INTESTINES. Semester 1, 2011 A. Mwakikunga
 ANATOMY OF THE SMALL & LARGE INTESTINES Semester 1, 2011 A. Mwakikunga LEARNING OBJECTIVES 1. List the parts and anatomical regions of the small and large intestines 2. State anatomical relations of the
ANATOMY OF THE SMALL & LARGE INTESTINES Semester 1, 2011 A. Mwakikunga LEARNING OBJECTIVES 1. List the parts and anatomical regions of the small and large intestines 2. State anatomical relations of the
LECTURE 11 & 12: ABDOMINAL VISCERA ABDOMINAL CONTENTS DIVISION. The location of abdominal viscera is divided into 4 quadrants:
 LECTURE 11 & 12: ABDOMINAL VISCERA ABDOMINAL CONTENTS DIVISION The location of abdominal viscera is divided into 4 quadrants: - horizontal line across the umbilicus divides the upper quadrants from the
LECTURE 11 & 12: ABDOMINAL VISCERA ABDOMINAL CONTENTS DIVISION The location of abdominal viscera is divided into 4 quadrants: - horizontal line across the umbilicus divides the upper quadrants from the
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Proceedings of the American Association of Equine Practitioners - Focus Meeting. Focus on Colic. Indianapolis, IN, USA 2011
 www.ivis.org Proceedings of the American Association of Equine Practitioners - Focus Meeting Focus on Colic Indianapolis, IN, USA 2011 Next Focus Meetings: July 22-24, 2012 - Focus on Hind Limb Lameness
www.ivis.org Proceedings of the American Association of Equine Practitioners - Focus Meeting Focus on Colic Indianapolis, IN, USA 2011 Next Focus Meetings: July 22-24, 2012 - Focus on Hind Limb Lameness
Internal hernias after laparoscopic Roux-en-Y gastric bypass
 The American Journal of Surgery 188 (2004) 796 800 Scientific paper Internal hernias after laparoscopic Roux-en-Y gastric bypass Ernesto Garza, Jr., M.D., Joseph Kuhn, M.D., David Arnold, M.D., William
The American Journal of Surgery 188 (2004) 796 800 Scientific paper Internal hernias after laparoscopic Roux-en-Y gastric bypass Ernesto Garza, Jr., M.D., Joseph Kuhn, M.D., David Arnold, M.D., William
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011
 Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
Christopher Lau Kings County Hospital SUNY Downstate Medical Center February 24, 2011 37 year old male presented with 1 day history of abdominal pain Pain was diffuse but worst in the epigastric area No
The "whirl sign". Diagnostic accuracy for intestinal volvulus.
 The "whirl sign". Diagnostic accuracy for intestinal volvulus. Poster No.: C-0670 Congress: ECR 2014 Type: Scientific Exhibit Authors: M. Pire, M. Marti, A. Borobia, A. Verón; Madrid/ES Keywords: Abdomen,
The "whirl sign". Diagnostic accuracy for intestinal volvulus. Poster No.: C-0670 Congress: ECR 2014 Type: Scientific Exhibit Authors: M. Pire, M. Marti, A. Borobia, A. Verón; Madrid/ES Keywords: Abdomen,
The Physician as Medical Illustrator
 The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
The Physician as Medical Illustrator Francois Luks Arlet Kurkchubasche Division of Pediatric Surgery Wednesday, December 9, 2015 Week 5 A good picture is worth a 1,000 bad ones How to illustrate an operation
Pathology of the Alimentary System Lecture 6 Diseases of intestine
 Systemic Pathology I - VPM 221 Pathology of the Alimentary System Lecture 6 Diseases of intestine Enrique Aburto Fall 2014 VII. Small & Large Intestines Structure & Function Long coiled tube, large surface
Systemic Pathology I - VPM 221 Pathology of the Alimentary System Lecture 6 Diseases of intestine Enrique Aburto Fall 2014 VII. Small & Large Intestines Structure & Function Long coiled tube, large surface
Internal Hernia After Gastric Bypass: Sensitivity and Specificity of Seven CT Signs with Surgical Correlation and Controls
 CT of Hernia After Gastric Bypass Abdominal Imaging Original Research Mark E. Lockhart 1 Franklin N. Tessler 1 Cheri L. Canon 1 J. Kevin Smith 1 Matthew C. Larrison 1 Naomi S. Fineberg 2 Brandon P. Roy
CT of Hernia After Gastric Bypass Abdominal Imaging Original Research Mark E. Lockhart 1 Franklin N. Tessler 1 Cheri L. Canon 1 J. Kevin Smith 1 Matthew C. Larrison 1 Naomi S. Fineberg 2 Brandon P. Roy
The different types of internal hernia after laparoscopic Roux-En-Y gastric by-pass for morbid obesity: MDCT features
 The different types of internal hernia after laparoscopic Roux-En-Y gastric by-pass for morbid obesity: MDCT features Poster No.: C-419 Congress: ECR 2009 Type: Educational Exhibit Topic: Abdominal and
The different types of internal hernia after laparoscopic Roux-En-Y gastric by-pass for morbid obesity: MDCT features Poster No.: C-419 Congress: ECR 2009 Type: Educational Exhibit Topic: Abdominal and
Case Report Intestinal Malrotation: A Rare Cause of Small Intestinal Obstruction
 Case Reports in Surgery, Article ID 453128, 4 pages http://dx.doi.org/10.1155/2014/453128 Case Report Intestinal Malrotation: A Rare Cause of Small Intestinal Obstruction Mesut Sipahi, 1 Kasim Caglayan,
Case Reports in Surgery, Article ID 453128, 4 pages http://dx.doi.org/10.1155/2014/453128 Case Report Intestinal Malrotation: A Rare Cause of Small Intestinal Obstruction Mesut Sipahi, 1 Kasim Caglayan,
Lesser sac: Anatomy and non-neoplastic processes
 Lesser sac: Anatomy and non-neoplastic processes Poster No.: C-0027 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Papadaki, R. Moschona, S. Paschalidou ; Rethymno, CR/ 1 2 2 3 1 3 GR, Rethymno/GR,
Lesser sac: Anatomy and non-neoplastic processes Poster No.: C-0027 Congress: ECR 2013 Type: Educational Exhibit Authors: E. Papadaki, R. Moschona, S. Paschalidou ; Rethymno, CR/ 1 2 2 3 1 3 GR, Rethymno/GR,
Fareed Khdair, MD Assistant Professor Chief, Section of Pediatric Gastroenterology, Hepatology, and Nutrition University of Jordan School of Medicine
 Fareed Khdair, MD Assistant Professor Chief, Section of Pediatric Gastroenterology, Hepatology, and Nutrition University of Jordan School of Medicine Outline Lecture one : Gut formation Foregut: esophagus,
Fareed Khdair, MD Assistant Professor Chief, Section of Pediatric Gastroenterology, Hepatology, and Nutrition University of Jordan School of Medicine Outline Lecture one : Gut formation Foregut: esophagus,
Anatomy of the peritoneum: What for?
 Anatomy of the peritoneum: What for? Poster No.: C-2152 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Lima, R. N. Lucas, C. A. S. Ruano, I. Oliveira, A. Cardoso, Z. Seabra; Lisbon/PT Keywords:
Anatomy of the peritoneum: What for? Poster No.: C-2152 Congress: ECR 2015 Type: Educational Exhibit Authors: M. Lima, R. N. Lucas, C. A. S. Ruano, I. Oliveira, A. Cardoso, Z. Seabra; Lisbon/PT Keywords:
Femoral Triangle and Adductor Canal. Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology
 Femoral Triangle and Adductor Canal Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Femoral Triangle and Adductor Canal Femoral triangle Is a triangular depressed area located in the upper
Femoral Triangle and Adductor Canal Dr. Heba Kalbouneh Associate Professor of Anatomy and Histology Femoral Triangle and Adductor Canal Femoral triangle Is a triangular depressed area located in the upper
Duodenum retroperitoneal
 Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Duodenum retroperitoneal C shaped Initial region out of stomach into small intestine RETROperitoneal viscus Superior 1 st part duodenal cap ; moves upwards and backwards to lie on the R crura medial to
Computed tomography (CT) imaging review of small bowel obstruction
 imaging review of small bowel obstruction") Computed tomography (CT) imaging review of small bowel obstruction Poster No.: C-1602 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract Authors: A. Vousough, D. S. Prasad ; Aberdeen/UK, Leeds/UK
Computed tomography (CT) imaging review of small bowel obstruction Poster No.: C-1602 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract Authors: A. Vousough, D. S. Prasad ; Aberdeen/UK, Leeds/UK
Computed tomography (CT) imaging review of small bowel obstruction
 imaging review of small bowel obstruction") Computed tomography (CT) imaging review of small bowel obstruction Poster No.: C-1602 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract - Small Bowel Authors: A. Vousough, D. S. Prasad ; Aberdeen/UK,
Computed tomography (CT) imaging review of small bowel obstruction Poster No.: C-1602 Congress: ECR 2010 Type: Educational Exhibit Topic: GI Tract - Small Bowel Authors: A. Vousough, D. S. Prasad ; Aberdeen/UK,
Internal hernias: Emergency department radiological dilemma
 www.edoriumjournals.com CASE REPORT OPEN ACCESS PEER REVIEWED Internal hernias: Emergency department radiological dilemma Cigdem Ozpolat, Halil Ibrahim Atalay, Sefer Ozkaya, Musa Adanc, Arzu Denizbasi,
www.edoriumjournals.com CASE REPORT OPEN ACCESS PEER REVIEWED Internal hernias: Emergency department radiological dilemma Cigdem Ozpolat, Halil Ibrahim Atalay, Sefer Ozkaya, Musa Adanc, Arzu Denizbasi,
Case Report Transmesenteric Internal Herniation Leading to Small Bowel Obstruction Postlaparoscopic Radical Nephrectomy
 Hindawi Case Reports in Surgery Volume 2017, Article ID 5128246, 4 pages https://doi.org/10.1155/2017/5128246 Case Report Transmesenteric Internal Herniation Leading to Small Bowel Obstruction Postlaparoscopic
Hindawi Case Reports in Surgery Volume 2017, Article ID 5128246, 4 pages https://doi.org/10.1155/2017/5128246 Case Report Transmesenteric Internal Herniation Leading to Small Bowel Obstruction Postlaparoscopic
International Surgery Strangulated lesser omentum hiatus hernia: a rare case report and a literature review
 International Surgery Strangulated lesser omentum hiatus hernia: a rare case report and a literature review --Manuscript Draft-- Manuscript Number: Full Title: Article Type: Keywords: Corresponding Author:
International Surgery Strangulated lesser omentum hiatus hernia: a rare case report and a literature review --Manuscript Draft-- Manuscript Number: Full Title: Article Type: Keywords: Corresponding Author:
Accessory Glands of Digestive System
 Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Accessory Glands of Digestive System The liver The liver is soft and pliable and occupies the upper part of the abdominal cavity just beneath the diaphragm. The greater part of the liver is situated under
Congenital Internal Hernia Presented with Life Threatening Extensive Small Bowel Strangulation
 pissn: 2234-8646 eissn: 2234-8840 http://dx.doi.org/10.5223/pghn.2013.16.3.190 Pediatric Gastroenterology, Hepatology & Nutrition 2013 September 16(3):190-194 Case Report PGHN Congenital Internal Hernia
pissn: 2234-8646 eissn: 2234-8840 http://dx.doi.org/10.5223/pghn.2013.16.3.190 Pediatric Gastroenterology, Hepatology & Nutrition 2013 September 16(3):190-194 Case Report PGHN Congenital Internal Hernia
The subperitoneal space and peritoneal cavity: basic concepts
 Abdominal Imaging ª The Author(s) 2015. This article is published with open access at Springerlink.com Published online: 26 May 2015 Abdom Imaging (2015) 40:2710 2722 DOI: 10.1007/s00261-015-0429-5 The
Abdominal Imaging ª The Author(s) 2015. This article is published with open access at Springerlink.com Published online: 26 May 2015 Abdom Imaging (2015) 40:2710 2722 DOI: 10.1007/s00261-015-0429-5 The
-Ensherah Mokheemer. -Shatha Al-Jaberi محمد المحتسب- 1 P a g e
 9-9 -Ensherah Mokheemer -Shatha Al-Jaberi محمد المحتسب- 1 P a g e Small intestine has three regions: ( االثني عشر( The duodenum The jejunum The ileum Small intestine Duodenum: -c-shaped -The concavity
9-9 -Ensherah Mokheemer -Shatha Al-Jaberi محمد المحتسب- 1 P a g e Small intestine has three regions: ( االثني عشر( The duodenum The jejunum The ileum Small intestine Duodenum: -c-shaped -The concavity
Adult bowel obstruction with acute abdomen: spectrum of CT findings
 Adult bowel obstruction with acute abdomen: spectrum of CT findings Poster No.: C-1571 Congress: ECR 2013 Type: Educational Exhibit Authors: L. Turturici, G. Gherarducci, F. Bianchi, R. Pascale, M. Tonerini,
Adult bowel obstruction with acute abdomen: spectrum of CT findings Poster No.: C-1571 Congress: ECR 2013 Type: Educational Exhibit Authors: L. Turturici, G. Gherarducci, F. Bianchi, R. Pascale, M. Tonerini,
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3. October 16, 2015
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 16, 2015 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 16, 2015 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
The Whipple Operation Illustrations
 The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
The Whipple Operation Illustrations Fig. 1. Illustration of the sixstep pancreaticoduodenectomy (Whipple operation) as described in a number of recent text books by Dr. Evans. The operation is divided
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3. October 17, 2014
 STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 17, 2014 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
STRUCTURAL BASIS OF MEDICAL PRACTICE EXAMINATION 3 October 17, 2014 PART l. Answer in the space provided. (12 pts) 1. Identify the structures. (2 pts) A. B. A B C. D. C D 2. Identify the structures. (2
Nasogastric tube. Stomach. Pylorus. Duodenum 1. Duodenum 2. Duodenum 3. Duodenum 4
 Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Esophagus Barium Swallow Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach and Duodenum 4 year old Upper GI Nasogastric tube Stomach Pylorus Duodenum 1 Duodenum 2 Duodenum 3 Duodenum 4
Cecal Volvulus: Case Presentation and Review of CT Findings
 August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
August 2011 Cecal Volvulus: Case Presentation and Review of CT Findings Omar Pardesi, Harvard Medical School Year III Our Patient LD: History & Physical HPI: 28 y.o. female presents with diffuse abdominal
Anatomy: Know Your Abdomen
 Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
Anatomy: Know Your Abdomen Glossary Abdomen - part of the body below the thorax (chest cavity); separated by the diaphragm. Anterior - towards the front of the body. For example, the umbilicus is anterior
Peritoneal cavity. Infracolic compartment. Assoc. prof. dr. S. Delchev, MD, PhD
 Peritoneal cavity. Infracolic compartment Assoc. prof. dr. S. Delchev, MD, PhD Infracolic compartment The infracolic compartment lies inferior to the transverse mesocolon and posterior to the greater omentum
Peritoneal cavity. Infracolic compartment Assoc. prof. dr. S. Delchev, MD, PhD Infracolic compartment The infracolic compartment lies inferior to the transverse mesocolon and posterior to the greater omentum
Surgical Anatomy of Hernial Rings. John E. Skandalakis, Stephen W. Gray, John T. Akin. Surgical Clinics of North America, Vol 54, No 6, December 1974.
 Surgical Anatomy of Hernial Rings John E. Skandalakis, Stephen W. Gray, John T. Akin Surgical Clinics of North America, Vol 54, No 6, December 1974. "Where should I cut the ring of the incarcerated or
Surgical Anatomy of Hernial Rings John E. Skandalakis, Stephen W. Gray, John T. Akin Surgical Clinics of North America, Vol 54, No 6, December 1974. "Where should I cut the ring of the incarcerated or
Gastroschisis Sequelae and Management
 Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
Gastroschisis Sequelae and Management Mary Finn Gillian Lieberman, MD Primary Care Radiology Beth Israel Deaconess Medical Center Harvard Medical School April 2014 Outline I. Definition and Epidemiology
THE ORAL CAVITY
 THE ORAL CAVITY WALL OF ABDOMEN (ANTERIOR) The paraumbilical vein drains into the portal vein and then through the liver. This is an important clinical connection. THE ABDOMINAL VISCERA The small
THE ORAL CAVITY WALL OF ABDOMEN (ANTERIOR) The paraumbilical vein drains into the portal vein and then through the liver. This is an important clinical connection. THE ABDOMINAL VISCERA The small
Anatomy of the spleen. Oluwadiya KS
 Anatomy of the spleen Oluwadiya KS www.oluwadiya.com Introduction The spleen is an ovoid, usually purplish, pulpy mass about the size and shape of one's fist. It is the largest lymphoid tissue in the body
Anatomy of the spleen Oluwadiya KS www.oluwadiya.com Introduction The spleen is an ovoid, usually purplish, pulpy mass about the size and shape of one's fist. It is the largest lymphoid tissue in the body
Gastrointestinal Tract. Anatomy of GI Tract. Anatomy of GI Tract. (Effective February 2007) (1%-5%)
 (1%-5%)") Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
Gastrointestinal Tract (Effective February 2007) (1%-5%) Anatomy of GI Tract Esophagus bulls-eye or target EG junction seen on sagittal scan posterior to left lobe of liver and anterior to aorta Anatomy
The Human Body: An Overview of Anatomy. Anatomy. Physiology. Anatomy - Study of internal and external body structures
 C H A P T E R 1 The Human Body: An Orientation An Overview of Anatomy Anatomy The study of the structure of the human body Physiology The study of body function Anatomy - Study of internal and external
C H A P T E R 1 The Human Body: An Orientation An Overview of Anatomy Anatomy The study of the structure of the human body Physiology The study of body function Anatomy - Study of internal and external
Small Plicae Circularis. Short Closely packed together. Sparse, completely absent at distal part Lymphoid Nodule
 Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Intestines Differences Between Jejunum and Ileum Types Jejunum Ileum Color Deeper red Paler pink Calibre Bigger Smaller Thickness of wall Thick and Heavy Thin and Lighter Vascularity Highly vascularised
Anatomy of the SMALL INTESTINE. Dr. Noman Ullah Wazir PMC
 Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
Anatomy of the SMALL INTESTINE Dr. Noman Ullah Wazir PMC SMALL INTESTINE The small intestine, consists of the duodenum, jejunum, and illium. It extends from the pylorus to the ileocecal junction were the
ANATOMY OF THE DIGESTIVE SYSTEM PART II
 ANATOMY OF THE DIGESTIVE SYSTEM PART II 9.12.2014 Kaan Yücel M.D., Ph.D. http://fhs121.org Dr.Kaan Yücel http://fhs121.org Digestive system Part II 1. LIVER The liver is the largest gland in the body and,
ANATOMY OF THE DIGESTIVE SYSTEM PART II 9.12.2014 Kaan Yücel M.D., Ph.D. http://fhs121.org Dr.Kaan Yücel http://fhs121.org Digestive system Part II 1. LIVER The liver is the largest gland in the body and,
Cho Cho* 1, Govani Dhaval 2, Bako Abdulmalik 2, Dhawan Vikram 3 and Patel Ramnik 4
 e - ISSN - 2349-8005 INTERNATIONAL JOURNAL OF ADVANCES IN CASE REPORTS Journal homepage: www.mcmed.us/journal/ijacr POST-OPERATIVE OBSTRUCTED INTERNAL PARACECAL HERNIA THROUGH CONGENITAL MESENTERIC DEFECT
e - ISSN - 2349-8005 INTERNATIONAL JOURNAL OF ADVANCES IN CASE REPORTS Journal homepage: www.mcmed.us/journal/ijacr POST-OPERATIVE OBSTRUCTED INTERNAL PARACECAL HERNIA THROUGH CONGENITAL MESENTERIC DEFECT
General Surgery Service
 General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
General Surgery Service Patient Care Goals and Objectives Stomach/Duodenum and Bariatric assessed for a) Obesity surgery b) Treatment of i) Adenocarcinoma of the stomach ii) GIST iii) Carcinoid 2) Optimize
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus
 A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
A novel plain abdominal radiograph sign to diagnose malrotation with volvulus Nataraja RM 1, Mahomed AA 1* 1. Department of Paediatric Surgery, Royal Alexandra Hospital for Sick Children, Brighton,UK *
The front of the thigh. Dr.Amjad shatarat
 The front of the thigh Femoral triangle (Scarpa s triangle) Is a triangular depressed area located in the upper part of the medial aspect of the thigh immediately below the inguinal ligament. Superiorly:
The front of the thigh Femoral triangle (Scarpa s triangle) Is a triangular depressed area located in the upper part of the medial aspect of the thigh immediately below the inguinal ligament. Superiorly:
Al-Mohtaseb. Saba Alfayoumi. Mo Alfarra
 8 Al-Mohtaseb Saba Alfayoumi Mo Alfarra For the comparison purposes refer to the last page where you can find a table that summarizes them. Enjoy Jejunum and Ileum -They're intraperitoneal and freely mobile
8 Al-Mohtaseb Saba Alfayoumi Mo Alfarra For the comparison purposes refer to the last page where you can find a table that summarizes them. Enjoy Jejunum and Ileum -They're intraperitoneal and freely mobile
DIGESTIVE SYSTEM SURGICAL PROCEDURES December 22, 2015 (effective March 1, 2016) INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 INTESTINES (EXCEPT RECTUM) Asst Surg Anae") December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
December 22, 2015 (effective March 1, 201) INTESTINES (EXCEPT RECTUM) Z513 Hydrostatic - Pneumatic dilatation of colon stricture(s) through colonoscope... 10.50 Z50 Fulguration of first polyp through colonoscope...
Antecolic versus retrocolic alimentary limb in laparoscopic Roux-en-Y gastric bypass: a comparative study
 Surgery for Obesity and Related Diseases 3 (2007) 423 427 Original article Antecolic versus retrocolic alimentary limb in laparoscopic Roux-en-Y gastric bypass: a comparative study Alex Escalona, M.D.
Surgery for Obesity and Related Diseases 3 (2007) 423 427 Original article Antecolic versus retrocolic alimentary limb in laparoscopic Roux-en-Y gastric bypass: a comparative study Alex Escalona, M.D.
SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution,
 SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution, derivatives 4. Hindgut- limits, evolution, derivatives
SUBJECTS 2nd year, 1st semester I. 1. Primitive gut - limits, derivatives 2. Foregut -limits, evolution, derivatives 3. Midgut -limits, evolution, derivatives 4. Hindgut- limits, evolution, derivatives
LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL
 SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
SIGNIFICANCE OF EXTRALUMINAL ABDOMINAL GAS: LOOKING FOR AIR IN ALL THE WRONG PLACES Richard M. Gore, MD North Shore University Health System University of Chicago Evanston, IL SCBT/MR 2012 October 26,
Medical application of transabdominal ultrasound in gastrointestinal diseases
 Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Medical application of transabdominal ultrasound in gastrointestinal diseases Hsiu-Po Wang Department of Emergency Medicine National Taiwan University Hospital Real-time ultrasound has become a standard
Abdominal Assessment
 Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.
Abdominal Assessment Mary Marian, MS,RD,CSO University of AZ, Tucson, AZ Neha Parekh, MS,RD,LD,CNSC Cleveland Clinic, Cleveland, OH Objectives: 1. Outline the steps in performing an abdominal examination.