C A R O L S I E M M S N, R N, B C, G N P M U S I N C L A I R S C H O O L O F N U R S I N G Q I P M O WHAT S IN A NAME?
|
|
|
- Martha Andrews
- 5 years ago
- Views:
Transcription
1 M D S A N D P R E S S U R E U L C E R S C A R O L S I E M M S N, R N, B C, G N P M U S I N C L A I R S C H O O L O F N U R S I N G Q I P M O WHAT S IN A NAME? 1777: decubitus is the oldest term used 1942 Studies and papers were starting to be published using decubitus 1959 Ischemic ulcers were noted 1975 Bedsores 1980 s Pressure sore 1990 s Pressure Ulcer June 2016 Pressure Injury 1
2 AGE RELATED CHANGES THAT CONTRIBUTE TO PRESSURE ULCER RISK. Thinning of the dermal epidermal junction. Leads to wrinkling, tearing, loss of elasticity, increased skin permeability, & alterations in barrier function of the skin. An altered immune response & decreased dermal vascularity. Causes a greater potential for infection. GOALS OF EDUCATION FOR PRESSURE ULCER RISK PREDICTION AND PREVENTION FOR NURSING HOMES Identify overall goals for the facility & for each resident Outline clearly the role of each team member/position Encourage input from all staff at both the resident level & the facility level Use current standards & sound facility policies to deliver resident specific care Make the care plan the primary resource document for delivering resident specific care 2
3 DEATH AND LAW SUITS Powell found a 129% higher death rate for pts admitted to LTC who developed a pressure ulcer than those who did not. Burd et. al reported a risk of death among geriatric patients who developed a pressure ulcer to be 4 times greater than the norm, & 6 times greater in those whose pressure ulcers did not heal. Estate of Cote: Arizona jury awarded $16.7 million in punitive damages and $2.5 million in Compensatory damage against a SNF Pressure Ulcers are Easy Pickings for Lawsuits: Provider April 2016 pg STATISTICS IN AGED CARE Prevalence Rates: 4.1% to 32.2%: Number of individuals with a PU at a specific point in time Incidence & Facility Acquired Rates: 1.9% to 59% Incidence is the number of new pressure ulcers that develop during a specific time period, such as a year. Significant variations in study methods and methodological rigor limit the value of these data points 3
4 COSTS Latest figures shows the average cost for treating a pressure ulcer is over 1 billion annually and additional $2.2 million in Medicare Hospital Days Cost for treatment $6,000 to $60,000 depending on size and stage Some sources indicate cost per ulcer can be up to $90,000 Wake, W (2010, Summer). Pressure ulcers: What clinicians need to know. The Permanente Journal, 14 (2), NEW DEFINITION BY THE NPUAP Pressure Injury: A pressure injury is localized damage to the skin and/or underlying soft tissue usually over a bony prominence or related to a medical or other device. The injury can present as intact skin or an open ulcer and may be painful. The injury occurs as a result of intense and/or prolonged pressure or pressure in combination with shear. The tolerance of soft tissue for pressure and shear may also be affected by microclimate, nutrition, perfusion, co-morbidities and condition of the soft tissue NPUAP National Pressure Ulcer Advisory Panel





5 CURRENT CMS DEFINITION F686: NOTE: Regardless of the staging system or wound definitions used by the facility, the facility is responsible for completing the MDS utilizing the staging guidelines found in the RAI Manual. PRESSURE ULCER/INJURY A pressure ulcer/injury is localized injury to the skin and/or underlying tissue, usually over a bony prominence, as a result of intense and/or prolonged pressure or pressure in combination with shear. The pressure ulcer/injury can present as intact skin or an open ulcer and may be painful. RAI Manual page M-4 Pressure EXTERNAL FACTORS Friction 5
 2016 Pressure Injury Staging System.")
6 SHEAR Tissue layers slide against each other, disrupts or angulates blood vessels PLANNING FOR CARE The pressure ulcer/injury definitions used in the RAI Manual have been adapted from those recommended by the National Pressure Ulcer Advisory Panel (NPUAP) 2016 Pressure Injury Staging System. An existing pressure ulcer/injury identifies residents at risk for further complications or skin injury. Risk factors described in M0100 should be addressed 6
7 PLANNING FOR CARE For MDS assessment, initial numerical staging of pressure ulcers and the initial numerical staging of ulcers after debridement, or DTI that declares itself, should be coded in terms of what is assessed (seen or palpated, i.e. visible tissue, palpable bone) during the look-back period. Nursing homes may adopt the NPUAP guidelines in their clinical practice and nursing documentation. However, since CMS has adapted the NPUAP guidelines for MDS purposes, the definitions do not perfectly correlate with each stage as described by NPUAP. Therefore, you must code the MDS according to the instructions in this manual. CODING TIPS If an ulcer/injury arises from a combination of factors that are primarily caused by pressure, then the area should be included in this section as a pressure ulcer/injury. If a pressure ulcer is surgically closed with a flap or graft, it should be coded as a surgical wound and not as a pressure ulcer. If the flap or graft fails, continue to code it as a surgical wound until healed 7
8 DIABETICS & CODING TIPS Residents with diabetes mellitus (DM) can have a pressure, venous, arterial, or diabetic neuropathic ulcer. The primary etiology should be considered when coding whether a resident with DM has an ulcer/injury that is caused by pressure or other factors. If a resident with DM has a heel ulcer/injury from pressure and the ulcer/injury is present in the 7-day look-back period, code 1 and proceed to code items in M0300 as appropriate for the pressure ulcer/injury. DIABETICS & CODING TIPS If a resident with DM has an ulcer on the plantar (bottom) surface of the foot closer to the metatarsals and the ulcer is present in the 7-day look-back period, code 0 and proceed to M1040 to code the ulcer as a diabetic foot ulcer. It is not likely that pressure is the primary cause of the resident s ulcer when the ulcer is in this location. 8
9 REVERSE STAGING Pressure ulcers do not heal in a reverse sequence, that is, the body does not replace the types and layers of tissue (e.g., muscle, fat, and dermis) that were lost during pressure ulcer development before they re-epithelialize. Stage 3 and 4 pressure ulcers fill with granulation tissue. This replacement tissue is never as strong as the tissue that was lost and hence is more prone to future breakdown. REVERSE STAGING Clinical standards do not support reverse staging or backstaging as a way to document healing, as it does not accurately characterize what is occurring physiologically as the ulcer heals. For example, over time, even though a Stage 4 pressure ulcer has been healing and contracting such that it is less deep, wide, and long, the tissues that were lost (muscle, fat, dermis) will never be replaced with the same type of tissue. Previous standards using reverse staging or backstaging would have permitted identification of such a pressure ulcer as a Stage 3, then a Stage 2, and so on, when it reached a depth consistent with these stages. Clinical standards now would require that this ulcer continue to be documented as a Stage 4 pressure ulcer until it has completely healed. 9
10 REVERSE STAGING Nursing homes can document the healing of pressure ulcers using descriptive characteristics of the wound (i.e., depth, width, presence or absence of granulation tissue, etc.) or by using a validated pressure ulcer healing tool. Once a pressure ulcer has healed, it is documented as a healed pressure ulcer at its highest numerical stage in this example, a healed Stage 4 pressure ulcer. For care planning purposes, this healed Stage 4 pressure ulcer would remain at increased risk for future breakdown or injury and would require continued monitoring and preventative care. DEFINITIONS EPITHELIAL TISSUE New skin that is light pink and shiny (even in persons with darkly pigmented skin). In Stage 2 pressure ulcers, epithelial tissue is seen in the center and at the edges of the ulcer. In full thickness Stage 3 and 4 pressure ulcers, epithelial tissue advances from the edges of the wound. GRANULATION TISSUE Red tissue with cobblestone or bumpy appearance; bleeds easily when injured. 10


11 ASSESSMENT OF THE PRESSURE ULCER: EPITHELIALIZATION Migration of cells across the top of the wound bed Necessary for wound closure ASSESSMENT OF THE PRESSURE ULCER: GRANULATION TISSUE Pink/red moist tissue that contains new blood vessels and essential components to promote growth. Healthy components of a wound bed, presents like a good beef steak 11

12 SCABS & ESCHAR Scabs & eschar are different both physically & chemically. Eschar is a collection of dead tissue within the wound that is flush with the surface of the wound. A scab is made up of dried blood cells and serum, sits on the top of the skin, & forms over exposed wounds such as wounds with granulating surfaces (like pressure ulcers, lacerations, evulsions, etc.). A scab is evidence of wound healing. A pressure ulcer that was staged as a 2 & now has a scab indicates it is a healing stage 2, & therefore, staging should not change. Eschar characteristics & the level of damage it causes to tissues is what makes it easy to distinguish from a scab. It is extremely important to have staff who are trained in wound assessment & who are able to distinguish scabs from eschar SCAB 12
; tissue consistency (firm or boggy); sensation (pain, itching); and/or a defined area of persistent redness in lightly")
13 Slough Eschar STAGE 1 PRESSURE INJURY An observable, pressure- related alteration of intact skin whose indicators, as compared to an adjacent or opposite area on the body, may include changes in one or more of the following parameters: skin temperature (warmth or coolness); tissue consistency (firm or boggy); sensation (pain, itching); and/or a defined area of persistent redness in lightly pigmented skin, whereas in darker skin tones, the injury may appear with persistent red, blue, or purple hues NON-BLANCHABLE Reddened areas of tissue that do not turn white or pale when pressed firmly with a finger or device. 13
14 14

15 ASSESSMENT STEPS For the purposes of coding, determine that the lesion being assessed is primarily related to pressure and that other conditions have been ruled out. If pressure is not the primary cause, do not code here. Reliance on only one descriptor is inadequate to determine the staging of a pressure injury between Stage 1 and deep tissue injury (see definition of deep tissue injury on page M-24). The descriptors are similar for these two types of injuries (e.g., temperature [warmth or coolness]; tissue consistency [firm or boggy]). 15
16 DEFINITION STAGE 2 PRESSURE ULCER Partial thickness loss of dermis presenting as a shallow open ulcer with a red-pink wound bed, without slough or bruising. May also present as an intact or open/ ruptured blister. The color of the fluid has no impact on how it is coded. 16
17 DEFINITION Examine the area adjacent to or surrounding an intact blister for evidence of tissue damage. If other conditions are ruled out and the tissue adjacent to or surrounding the blister demonstrates signs of tissue damage (e.g., color change, tenderness, bogginess or firmness, warmth or coolness), these characteristics suggest a deep tissue injury (DTI) rather than a Stage 2 pressure ulcer. STEPS FOR ASSESSMENT Most Stage 2 pressure ulcers should heal in a reasonable time frame (e.g., 60 days). If a pressure ulcer fails to show some evidence toward healing within 14 days, the pressure ulcer (including potential complications) and the patient s overall clinical condition should be reassessed. Stage 2 pressure ulcers are often related to friction and/or shearing force, and the care plan should incorporate efforts to limit these forces on the skin and tissues. Stage 2 pressure ulcers may be more likely to heal with treatment than higher stage pressure ulcers. The care plan should include individualized interventions and evidence that the interventions have been monitored and modified as appropriate. 17
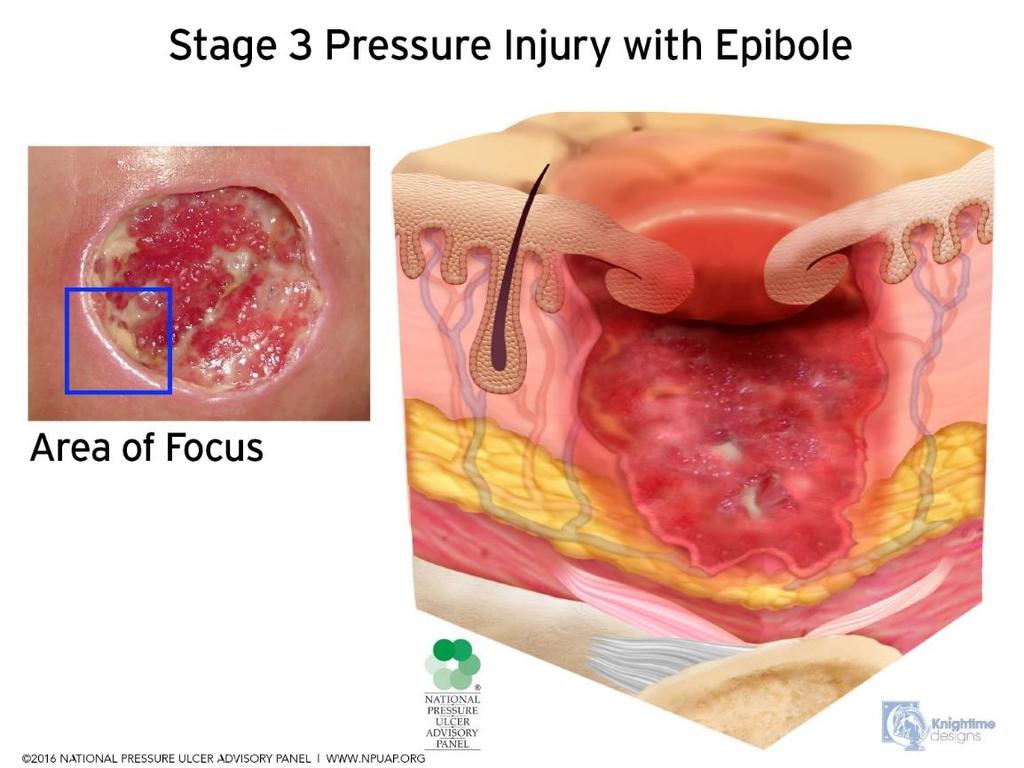
18 STAGE 2: CODING TIPS Stage 2 pressure ulcers by definition have partial thickness loss of the dermis. Granulation tissue, slough, and eschar are not present in Stage 2 pressure ulcers. Do not code skin tears, tape burns, moisture associated skin damage, or excoriation here. When a pressure ulcer presents as an intact blister, examine the adjacent and surrounding area for signs of deep tissue injury. When a deep tissue injury is determined, do not code as a Stage 2. STAGE 3 PRESSURE ULCER: DEFINITION Full thickness tissue loss. Subcutaneous fat may be visible but bone, tendon or muscle is not exposed. Slough may be present but does not obscure the depth of tissue loss. May include undermining or tunneling (see definition of undermining and tunneling on page M-17). Tissue characteristics of pressure ulcers should be considered when determining treatment options and choices. Changes in tissue characteristics over time are indicative of wound healing or degeneration. 18
19 19
20 CODING TIPS FOR STAGE 3 The depth of a Stage 3 pressure ulcer varies by anatomical location. Stage 3 pressure ulcers can be shallow, particularly on areas that do not have subcutaneous tissue, such as the bridge of the nose, ear, occiput, and malleolus. In contrast, areas of significant adiposity can develop extremely deep Stage 3 pressure ulcers. Therefore, observation and assessment of skin folds should be part of overall skin assessment. Do not code moisture-associated skin damage or excoriation here. Bone/tendon/muscle is not visible or directly palpable in a Stage 3 pressure ulcer. DEFINITION: STAGE 4 Full thickness tissue loss with exposed bone, tendon or muscle. Slough or eschar may be present on some parts of the wound bed. Often includes undermining and tunneling. 20
 so that the pressure ulcer is larger at its base than at the skin")
21 DEFINITIONS TUNNELING A passage way of tissue destruction under the skin surface that has an opening at the skin level from the edge of the wound. UNDERMINING The destruction of tissue or ulceration extending under the skin edges (margins) so that the pressure ulcer is larger at its base than at the skin surface. 21
22 CODING TIPS The depth of a Stage 4 pressure ulcer varies by anatomical location. The bridge of the nose, ear, occiput, and malleolus do not have subcutaneous tissue, and these ulcers can be shallow. Stage 4 pressure ulcers can extend into muscle and/or supporting structures (e.g., fascia, tendon, or joint capsule) making osteomyelitis possible. Exposed bone/tendon/muscle is visible or directly palpable. Cartilage serves the same anatomical function as bone. Therefore, pressure ulcers that have exposed cartilage should be classified as a Stage 4 UNSTAGEABLE SLOUGH TISSUE Non-viable yellow, tan, gray, green or brown tissue; usually moist, can be soft, stringy and mucinous in texture. Slough may be adherent to the base of the wound or present in clumps throughout the wound bed. ESCHAR TISSUE Dead or devitalized tissue that is hard or soft in texture; usually black, brown, or tan in color, and may appear scab-like. Necrotic tissue and eschar are usually firmly adherent to the base of the wound and often the sides/ edges of the wound. 22
23 CODING TIPS Pressure ulcers that are covered with slough and/or eschar, and the wound bed cannot be visualized, should be coded as unstageable because the true anatomic depth of soft tissue damage (and therefore stage) cannot be determined. Only until enough slough and/or eschar is removed to expose the anatomic depth of soft tissue damage involved, can the stage of the wound be determined. Stable eschar (i.e., dry, adherent, intact without erythema or fluctuance) on the heels serves as the body s natural (biological) cover and should only be removed after careful clinical consideration, including ruling out ischemia, and consultation with the resident s physician, or nurse practitioner, physician assistant, or clinical nurse specialist if allowable under state licensure laws. 23
24 DEFINITION FLUCTUANCE Used to describe the texture of wound tissue indicative of underlying unexposed fluid. DEEP TISSUE INJURY DEFINITION Purple or maroon area of discolored intact skin due to damage of underlying soft tissue. The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue. 24
25 DEEP TISSUE INJURY ASSESSMENT Examine the area adjacent to, or surrounding, an intact blister for evidence of tissue damage. If the tissue adjacent to, or surrounding, the blister does not show signs of tissue damage (e.g., color change, tenderness, bogginess or firmness, warmth or coolness), do not code as a deep tissue injury. DEEP TISSUE INJURY CODING TIPS Once deep tissue injury has opened to an ulcer, reclassify the ulcer into the appropriate stage. Then code the ulcer for the reclassified stage. Deep tissue injury may be difficult to detect in individuals with dark skin tones. Evolution may be rapid, exposing additional layers of tissue even with optimal treatment. When a lesion due to pressure presents with an intact blister AND the surrounding or adjacent soft tissue does NOT have the characteristics of deep tissue injury, do not code here (see definition of Stage 2 pressure ulcer on page M-12). 25

26 VENOUS AND ARTERIAL ULCERS VENOUS ULCERS Ulcers caused by peripheral venous disease, which most commonly occur proximal to the medial or lateral malleolus, above the inner or outer ankle, or on the lower calf area of the leg. ARTERIAL ULCERS Ulcers caused by peripheral arterial disease, which commonly occur on the tips and tops of the toes, tops of the foot, or distal to the medial malleolus. Venous Insufficiency Ulcer 26


27 Vascular Problems Incompetent venous system of the legs Increased fibrous tissue Hyperpigmentation (Hemosiderin) Chronic stasis dermatitis Increased venous pressure induced by incompetent valves Induces inflammation 27


28 28

29 HEMOSIDERIN DEFINITION An intracellular storage form of iron; the granules consist of an illdefined complex of ferric hydroxides, polysaccharides, and proteins having an iron content of approximately 33% by weight. It appears as a dark yellow-brown pigment. 29
30 ARTERIAL ULCERS Key areas for arterial ulcer development include the distal part of the foot, dorsum or tops of the foot, or tips and tops of the toes Arterial ulcers are often painful and have a pale pink wound bed, necrotic tissue, minimal exudate, and minimal bleeding. ARTERIAL ULCERS CODING TIPS Trophic skin changes (e.g., dry skin, loss of hair growth, muscle atrophy, brittle nails) may also be present. The wound may start with some kind of minor trauma, such as hitting the leg on a wheelchair. The wound does not typically occur over a bony prominence, however, can occur on the tops of the toes. Pressure forces play virtually no role in the development of the ulcer, however, for some residents, pressure may play a part. Ischemia is the major etiology of these ulcers. Lower extremity and foot pulses may be diminished or absent. 30
31 VENOUS ULCERS The wound may start with some kind of minor trauma, such as hitting the leg on a wheelchair. The wound does not typically occur over a bony prominence, and pressure forces play virtually no role in the development of the ulcer. Arterial Ulcer 31
.")
 wound bed, minimal to moderate amounts of yellow fibrinous material, and moderate to large amounts of exudate.")
32 VENOUS ULCERS Key areas for venous ulcer development include the area proximal to the lateral and medial malleolus (e.g., above the inner and outer ankle area). Venous ulcers may or may not be painful and are typically shallow with irregular wound edges, a red granular (e.g., bumpy) wound bed, minimal to moderate amounts of yellow fibrinous material, and moderate to large amounts of exudate. The surrounding tissues may be erythematous or reddened, or appear brown-tinged due to hemosiderin staining. Leg edema may also be present. 32

33 Diabetic Neuropathic Ulcer Characteristically occurs on the foot e.g. at mid-foot, at the ball of the foot over the metatarsal heads, or on the tops of toes with Charcot deformity. Requires that the resident be diagnosed with diabetes mellitus and have peripheral neuropathy. DIABETIC FOOT ULCERS 33


34 Diabetic Neuropathic Ulcer Underlying Condition Diabetic neuropathic ulcer Diabetes Spinal cord injury Hansen s disease Relief of pain with ambulation Parasthesia of extremities 34

35 Characteristics Diabetic Neuropathic Ulcer Wound Bed Variable depth Variable exudate Granulation tissue frequently present Gangrene uncommon, necrotic tissue variable Characteristics Diabetic Neuropathic Ulcer Ulcer edges: well defined Shape: variable Surrounding tissue: normal skin tones, fissuring and/or callus formation Location: Plantar aspect of foot, metatarsal heads, heels 35
.")
36 Perfusion Diabetic Neuropathic Ulcer Pain: diminished sensitivity to touch Peripheral pulses: palpable/present Capillary refill: normal REFERENCES: American Medical Directors Association. Pressure Ulcers in the Long Term Care Setting Clinical Practice Guidelines. Columbia, MD:AMDA Berstrom, N., Demuth, P., & Braden, B. (1987). A clinical trial of the Braden scale for predicting pressure sore risk. Nursing clinics of North America, 22(2), Bergstrom, N, Horn, SD, Rapp, MP, et.al. (2013) Turning for ulcer reduction: a multisite randomized clinical trial in nursing homes. The Journal of the American Geriatrics Society 2013 Oct; 61(10): Lundgren, BJN. (2016) Turning programs hinder a good night s sleep. no2/ Forsberg, T & Jordan, R. FAQ s about support surfaces. 36
37 REFERENCES: National Pressure Ulcer Advisory Panel, European Pressure Ulcer Advisory Panel and Pan Pacific Pressure Injury Alliance. Prevention and Treatment of Pressure Ulcers: Clinical; Practice Guideline. Emily Haesler (Ed.). Cambridge Media, Osborne Park, Western Australia; U.S. Department of Health and Human Services: Agency for Health Care Policy and Research. (1994). Clinical practice guidelines: Pressure ulcer treatment. (AHCPR ). Rockville, MD Guideline for Prevention & Management of Pressure Ulcers. (2010). WOCN. Mount Laurel, NJ 37
SECTION M: SKIN CONDITIONS. M0210: Unhealed Pressure Ulcer(s) Item Rationale
 Item Rationale") SECTION M: SKIN CONDITIONS Intent: The items in this section of the April 1, 2014 release of the LTCH CARE Data Set Version 2.01 document the presence, appearance, and change of pressure ulcers. If warranted
SECTION M: SKIN CONDITIONS Intent: The items in this section of the April 1, 2014 release of the LTCH CARE Data Set Version 2.01 document the presence, appearance, and change of pressure ulcers. If warranted
Pressure Ulcer Staging and Documentation. Carolyn Watts MSN, RN, CWON Vanderbilt Medical Center
 Pressure Ulcer Staging and Documentation Carolyn Watts MSN, RN, CWON Vanderbilt Medical Center Overview of the Pressure Ulcer Problem Scope Over 1 million cases each year, 1 in 4 patients Cost In acute
Pressure Ulcer Staging and Documentation Carolyn Watts MSN, RN, CWON Vanderbilt Medical Center Overview of the Pressure Ulcer Problem Scope Over 1 million cases each year, 1 in 4 patients Cost In acute
Advanced Clinical Solutions. Pressure Ulcer. Carilex Medical Group 1
 Advanced Clinical Solutions Pressure Ulcer Carilex Medical Group 1 Advanced Clinical Solutions Contents About Pressure Ulcer! 2 Stages of Pressure Ulcer! 5 Reference! 7 Carilex Medical Group 1 About Pressure
Advanced Clinical Solutions Pressure Ulcer Carilex Medical Group 1 Advanced Clinical Solutions Contents About Pressure Ulcer! 2 Stages of Pressure Ulcer! 5 Reference! 7 Carilex Medical Group 1 About Pressure
The Importance of Skin Examination. following Spinal Cord Injury
 The Importance of Skin Examination following Spinal Cord Injury An individual who sustains a spinal cord injury (SCI) has a lifetime of increased susceptibility to skin problems, including pressure ulcers
The Importance of Skin Examination following Spinal Cord Injury An individual who sustains a spinal cord injury (SCI) has a lifetime of increased susceptibility to skin problems, including pressure ulcers
Pressure Ulcer Staging. Staging of Wounds are based on the deepest level of tissue damage
 Pressure Ulcer Staging Staging of Wounds are based on the deepest level of tissue damage Pressure Ulcer Staging New Pressure Ulcer Staging Stage I Stage II Stage III Stage IV Unstageable Suspected Deep
Pressure Ulcer Staging Staging of Wounds are based on the deepest level of tissue damage Pressure Ulcer Staging New Pressure Ulcer Staging Stage I Stage II Stage III Stage IV Unstageable Suspected Deep
Acute and Chronic WOUND ASSESSMENT. Wound Assessment OBJECTIVES ITEMS TO CONSIDER
 WOUND ASSESSMENT Acute and Chronic OBJECTIVES Discuss classification systems and testing methods for pressure ulcers, venous, arterial and diabetic wounds List at least five items to be assessed and documented
WOUND ASSESSMENT Acute and Chronic OBJECTIVES Discuss classification systems and testing methods for pressure ulcers, venous, arterial and diabetic wounds List at least five items to be assessed and documented
Objectives. Major Changes to Section M. MDS 3.0 Section M Pressure Ulcers. Risk assessment Introduction of NPUAP guidelines
 MDS 3.0 Section M Pressure Ulcers Moderator: Barbara Baylis Sr. VP of Clinical and Residential Services, Kindred Healthcare Presenter: Glenda Mack, Sr. Director of Clinical Operations, Peoplefirst Rehabilitation
MDS 3.0 Section M Pressure Ulcers Moderator: Barbara Baylis Sr. VP of Clinical and Residential Services, Kindred Healthcare Presenter: Glenda Mack, Sr. Director of Clinical Operations, Peoplefirst Rehabilitation
Pressure Injury Staging Update 2016
 Pressure Injury Staging Update 2016 A Review of the New Changes for Pressure Injury Documentation and Staging Jeanne Terefenko, BSN, RN, CWOCN Ext. 5855 Pressure Ulcer Staging Updates: In April, 2016,
Pressure Injury Staging Update 2016 A Review of the New Changes for Pressure Injury Documentation and Staging Jeanne Terefenko, BSN, RN, CWOCN Ext. 5855 Pressure Ulcer Staging Updates: In April, 2016,
Pressure Injury Definition and Stages
 Program Objective Pressure Injury Definition and Stages Identify the changes to the 2016 NPUAP staging system Changes to the Staging System in 2016 2 Anatomy of the Skin Anatomy of the Skin Largest organ
Program Objective Pressure Injury Definition and Stages Identify the changes to the 2016 NPUAP staging system Changes to the Staging System in 2016 2 Anatomy of the Skin Anatomy of the Skin Largest organ
Bed Sores No More! Pressure Injuries Risk Factors and Updated Staging Methodology. Nicolle Samuels, MSPT, CLT-LANA, CWS, CKTP
 Bed Sores No More! Pressure Injuries Risk Factors and Updated Staging Methodology Nicolle Samuels, MSPT, CLT-LANA, CWS, CKTP Objectives Understand updated definitions as well as staging and classification
Bed Sores No More! Pressure Injuries Risk Factors and Updated Staging Methodology Nicolle Samuels, MSPT, CLT-LANA, CWS, CKTP Objectives Understand updated definitions as well as staging and classification
Uncovering the Pressure Ulcer Coverup Rhonda Kistler RN MS CWON Wound Care Concepts Gentell
 Uncovering the Pressure Ulcer Coverup Rhonda Kistler RN MS CWON Wound Care Concepts Gentell Objectives Identify the stages of pressure ulcer according to the depth of tissue destruction. Discuss the differences
Uncovering the Pressure Ulcer Coverup Rhonda Kistler RN MS CWON Wound Care Concepts Gentell Objectives Identify the stages of pressure ulcer according to the depth of tissue destruction. Discuss the differences
Treat the whole patient, not just the hole in the patient! 3/21/2017 CAN YOU CONNECT THE DOTS?? PHILOSOPHY OBJECTIVES
 CAN YOU CONNECT THE DOTS?? Boone Hospital Wound Healing Center Kimberly Jamison, MD, FACP, FAPWCA, PCWC Kim Mitchell, RN, BSN OBJECTIVES Describe the basic concepts of chronic wound care to ensure an optimal
CAN YOU CONNECT THE DOTS?? Boone Hospital Wound Healing Center Kimberly Jamison, MD, FACP, FAPWCA, PCWC Kim Mitchell, RN, BSN OBJECTIVES Describe the basic concepts of chronic wound care to ensure an optimal
Wound Jeopardy: Name That Wound Session 142 Saturday, September 10 th 2011
 Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
2 Pressure Ulcer or Pressure Injury? (Do you have skin in the game?)
") Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Ann Rambusch, MSN, HCS D, HCS O, RN June 28, 2016 1 Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Understanding NPUAP
Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Ann Rambusch, MSN, HCS D, HCS O, RN June 28, 2016 1 Pressure Ulcer or Pressure Injury? (Do you have skin in the game?) Understanding NPUAP
Recognizing Pressure Injury
 Recognizing Pressure Injury Karen Zulkowski, DNS, RN Hawaii Recorded on March 8, 2017 1 A Little About Myself Executive editor of the Journal of the World Council of Enterostomal Therapists (JWCET) and
Recognizing Pressure Injury Karen Zulkowski, DNS, RN Hawaii Recorded on March 8, 2017 1 A Little About Myself Executive editor of the Journal of the World Council of Enterostomal Therapists (JWCET) and
Assisted Living Resident Assessment (To be used when yes is indicated for skin issues under Section 5 of Assisted Living Resident Assessment)
") Skin Assessment Current open skin areas: Yes No Current pressure ulcer: Yes No A. Stage 1 Ulcers Report based on highest stage of existing ulcers at its worst; do not reverse stage. Number of existing
Skin Assessment Current open skin areas: Yes No Current pressure ulcer: Yes No A. Stage 1 Ulcers Report based on highest stage of existing ulcers at its worst; do not reverse stage. Number of existing
If both a standardized, validated screening tool and an evaluation of clinical factors are utilized, select Response 2.
 (M1300) Pressure Ulcer Assessment: Was this patient assessed for Risk of Developing Pressure Ulcers? 0 - No assessment conducted [Go to M1306 ] 1 - Yes, based on an evaluation of clinical factors (for
(M1300) Pressure Ulcer Assessment: Was this patient assessed for Risk of Developing Pressure Ulcers? 0 - No assessment conducted [Go to M1306 ] 1 - Yes, based on an evaluation of clinical factors (for
Pressure Ulcer. Patient information leaflet. Category I. Category II. Category III. Category IV. Unstageable. Deep Tissue Injury
 Pressure Ulcers Patient information leaflet Pressure Ulcer Category I Category II Category III Category IV Unstageable Deep Tissue Injury Introduction This leaflet is about pressure ulcers and includes
Pressure Ulcers Patient information leaflet Pressure Ulcer Category I Category II Category III Category IV Unstageable Deep Tissue Injury Introduction This leaflet is about pressure ulcers and includes
New Strategies to Improve Assessment, Documentation and Prevention of Pressure Injuries
 New Strategies to Improve Assessment, Documentation and Prevention of Pressure Injuries Janet Cuddigan, PhD, RN, CWCN, FAAN Professor, UNMC College of Nursing Omaha, NE Focus of this Presentation New developments
New Strategies to Improve Assessment, Documentation and Prevention of Pressure Injuries Janet Cuddigan, PhD, RN, CWCN, FAAN Professor, UNMC College of Nursing Omaha, NE Focus of this Presentation New developments
Negative Pressure Wound Therapy
 Origination: 6/29/04 Revised: 8/24/16 Annual Review: 11/10/16 Purpose: To provide Negative Pressure Wound Therapy (wound care treatment) guidelines for the Medical Department staff to reference when making
Origination: 6/29/04 Revised: 8/24/16 Annual Review: 11/10/16 Purpose: To provide Negative Pressure Wound Therapy (wound care treatment) guidelines for the Medical Department staff to reference when making
Teaming Together to Understand Pressure Injuries / (Ulcers): NPUAP Terminology and Staging Clarification
: NPUAP Terminology and Staging Clarification") Teaming Together to Understand Pressure Injuries / (Ulcers): NPUAP Terminology and Staging Clarification We encourage you to share this information with your staff and colleagues by facilitating clinician
Teaming Together to Understand Pressure Injuries / (Ulcers): NPUAP Terminology and Staging Clarification We encourage you to share this information with your staff and colleagues by facilitating clinician
E-learning module: Stages of pressure injuries. Disclaimer
 E-learning module: Stages of pressure injuries 1 Disclaimer Classification of pressure injuries The International Pressure Injury Category System (2009) was developed by:! the National Pressure Ulcer Advisory
E-learning module: Stages of pressure injuries 1 Disclaimer Classification of pressure injuries The International Pressure Injury Category System (2009) was developed by:! the National Pressure Ulcer Advisory
(Words Pressure Wound Video Series and Part II appear on screen with the SCIRE logo at the top right corner.)
") (Words Pressure Wound Video Series and Part II appear on screen with the SCIRE logo at the top right corner.) (Fades to next slide titled Pressure Ulcer Staging. *Video contains Graphic Imagery is noted
(Words Pressure Wound Video Series and Part II appear on screen with the SCIRE logo at the top right corner.) (Fades to next slide titled Pressure Ulcer Staging. *Video contains Graphic Imagery is noted
PRESSURE ULCERS SIMPLIFIED
 10 PRESSURE ULCERS SIMPLIFIED This leaflet is intended to give you information and answers to some question you may have around pressure ulcers PRESSURE ULCERS SIMPLIFIED Pressure ulcer development has
10 PRESSURE ULCERS SIMPLIFIED This leaflet is intended to give you information and answers to some question you may have around pressure ulcers PRESSURE ULCERS SIMPLIFIED Pressure ulcer development has
Wound, Ostomy and Continence Nurses Society s Guidance on OASIS-D Integumentary Items: Best Practice for Clinicians
 Wound, Ostomy and Continence Nurses Society s Guidance on OASIS-D Integumentary Items: Best Practice for Clinicians Table of Contents Table of Contents... 2 Acknowledgments... 3 Introduction... 4 Purpose...
Wound, Ostomy and Continence Nurses Society s Guidance on OASIS-D Integumentary Items: Best Practice for Clinicians Table of Contents Table of Contents... 2 Acknowledgments... 3 Introduction... 4 Purpose...
Successful Wound Management Strategies : An Introduction. Alex Khan, APRN ACNS-BC. Organization of Wound Care Nurses
 Successful Wound Management Strategies : An Introduction Alex Khan, APRN ACNS-BC Organization of Wound Care Nurses www.woundcarenurses.org Goals & Objectives The role and importance of wound care management
Successful Wound Management Strategies : An Introduction Alex Khan, APRN ACNS-BC Organization of Wound Care Nurses www.woundcarenurses.org Goals & Objectives The role and importance of wound care management
Pressure Ulcers ecourse
 Pressure Ulcers ecourse Knowledge Checkup Module 2 Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Knowledge Checkup Module
Pressure Ulcers ecourse Knowledge Checkup Module 2 Handout College of Licensed Practical Nurses of Alberta (Canada) CLPNA.com and StudywithCLPNA.com CLPNA Pressure Ulcers ecourse Knowledge Checkup Module
OASIS NP August 2011: Special Training. OASIS-C Integument Assessment. Rhonda Will, RN, BS, COS-C, HCS-D Assistant Director OASIS Competency Institute
 OASIS NP August 211: Special Training OASIS-C Integument Assessment Rhonda Will, RN, BS, COS-C, HCS-D Assistant Director OASIS Competency Institute 243 King Street, Suite 246 Northampton, MA 16 413-584-53
OASIS NP August 211: Special Training OASIS-C Integument Assessment Rhonda Will, RN, BS, COS-C, HCS-D Assistant Director OASIS Competency Institute 243 King Street, Suite 246 Northampton, MA 16 413-584-53
Wound Care Program for Nursing Assistants-
 Wound Care Program for Nursing Assistants- Wound Cleansing,Types & Presentation Elizabeth DeFeo, RN, WCC, OMS, CWOCN Wound, Ostomy, & Continence Specialist ldefeo@cornerstonevna.org Outline/Agenda At completion
Wound Care Program for Nursing Assistants- Wound Cleansing,Types & Presentation Elizabeth DeFeo, RN, WCC, OMS, CWOCN Wound, Ostomy, & Continence Specialist ldefeo@cornerstonevna.org Outline/Agenda At completion
Wound Care Assessment in the Home Care Setting
 Wound Care Assessment in the Home Care Setting Lynn Peterson, RN, BSN, CWOCN Technical Service Specialist 3M Health Care Wednesday, May 14, 2008 Objectives Describe essential elements of a wound assessment
Wound Care Assessment in the Home Care Setting Lynn Peterson, RN, BSN, CWOCN Technical Service Specialist 3M Health Care Wednesday, May 14, 2008 Objectives Describe essential elements of a wound assessment
Durable Medical Equipment Providers
 August 2009 Provider Bulletin Number 974 Durable Medical Equipment Providers Vacuum Assisted Wound Closure Therapy Negative pressure wound therapy (NPWT) must be requested and supplied by an enrolled durable
August 2009 Provider Bulletin Number 974 Durable Medical Equipment Providers Vacuum Assisted Wound Closure Therapy Negative pressure wound therapy (NPWT) must be requested and supplied by an enrolled durable
Critically Assessing Pressure Injuries
 Critically Assessing Injuries Copyright 2016 Gordian Medical, Inc. dba American Medical Technologies. LeadingAge Indiana presents FACULTY PAMELA SCARBOROUGH PT, DPT, CDE, CWS DIRECTOR OF PUBLIC POLICY
Critically Assessing Injuries Copyright 2016 Gordian Medical, Inc. dba American Medical Technologies. LeadingAge Indiana presents FACULTY PAMELA SCARBOROUGH PT, DPT, CDE, CWS DIRECTOR OF PUBLIC POLICY
Stop The Pressure: Patient Safety and Tissue Viability
 Portsmouth Hospitals NHS Trust Stop The Pressure: Patient Safety and Tissue Viability Alison Cole Claire Brett Karen Oakley Presentation Focus Etiology and cause of a pressure ulcer The impact of pressure
Portsmouth Hospitals NHS Trust Stop The Pressure: Patient Safety and Tissue Viability Alison Cole Claire Brett Karen Oakley Presentation Focus Etiology and cause of a pressure ulcer The impact of pressure
Pathway to excellence. A comprehensive clinical education platform from Smith & Nephew
 Pathway to excellence A comprehensive clinical education platform from Smith & Nephew Pathway to Excellence Support Each year, we train more than 150,000 healthcare professional around the globe. In addition
Pathway to excellence A comprehensive clinical education platform from Smith & Nephew Pathway to Excellence Support Each year, we train more than 150,000 healthcare professional around the globe. In addition
Oregon Health Care Association Presents. F686: Updates on Regulations for Pressure Ulcer/Injury Prevention and Care
 Oregon Health Care Association Presents F686: Updates on Regulations for Pressure Ulcer/Injury Prevention and Care FACULTY: PAMELA SCARBOROUGH PT, DPT, MS, CWS, CEEAA DIRECTOR OF PUBLIC POLICY & EDUCATION
Oregon Health Care Association Presents F686: Updates on Regulations for Pressure Ulcer/Injury Prevention and Care FACULTY: PAMELA SCARBOROUGH PT, DPT, MS, CWS, CEEAA DIRECTOR OF PUBLIC POLICY & EDUCATION
SAMPLE. Home Health Reference Tool For Nurses
 Home Health Reference Tool For Nurses Foundation Management Services, Inc. 2010. All rights reserved. Unauthorized reproduction is strictly prohibited. (10/09) Table of Contents 2 Page Medicare Eligibility
Home Health Reference Tool For Nurses Foundation Management Services, Inc. 2010. All rights reserved. Unauthorized reproduction is strictly prohibited. (10/09) Table of Contents 2 Page Medicare Eligibility
Skin Integrity and Wound Care
 Skin Integrity and Wound Care By Dr. Amer Hasanien & Dr. Ali Saleh Skin Integrity and Wound Care Skin integrity: the presence of normal Skin & Uninterrupted skin layers by wounds. Factors affecting appearance
Skin Integrity and Wound Care By Dr. Amer Hasanien & Dr. Ali Saleh Skin Integrity and Wound Care Skin integrity: the presence of normal Skin & Uninterrupted skin layers by wounds. Factors affecting appearance
CURRENT CONCEPTS IN PRESSURE INJURY PREVENTION AND CARE
 CURRENT CONCEPTS IN PRESSURE INJURY PREVENTION AND CARE JOIE WHITNEY, PHD, RN, CWCN, FAAN PROFESSOR BIOBEHAVIORAL NURSING AND HEALTH SYSTEMS UNIVERSITY OF WASHINGTON HARBORVIEW ENDOWED PROFESSOR IN CRITICAL
CURRENT CONCEPTS IN PRESSURE INJURY PREVENTION AND CARE JOIE WHITNEY, PHD, RN, CWCN, FAAN PROFESSOR BIOBEHAVIORAL NURSING AND HEALTH SYSTEMS UNIVERSITY OF WASHINGTON HARBORVIEW ENDOWED PROFESSOR IN CRITICAL
Spinal Cord Injury Info Sheet An information series produced by the Spinal Cord Program at GF Strong Rehab Centre.
 Spinal Cord Injury Info Sheet An information series produced by the Spinal Cord Program at GF Strong Rehab Centre. What does skin do? 1. It protects you. 2. It provides sensory information. 3. It helps
Spinal Cord Injury Info Sheet An information series produced by the Spinal Cord Program at GF Strong Rehab Centre. What does skin do? 1. It protects you. 2. It provides sensory information. 3. It helps
Team-Centered Wound Care: Making Your Wound Care Safe and Simple Again
 Team-Centered Wound Care: Making Your Wound Care Safe and Simple Again October 4 th, 2017 Ryan P. Dirks PA-C Founder and CEO Road to success Detailed Wound Assessment/Risk Assessment External Support Individualized
Team-Centered Wound Care: Making Your Wound Care Safe and Simple Again October 4 th, 2017 Ryan P. Dirks PA-C Founder and CEO Road to success Detailed Wound Assessment/Risk Assessment External Support Individualized
WOUND MANAGEMENT. A Clinical Perspective. Furqan Alex Khan, APRN ACNS-BC MSN
 WOUND MANAGEMENT A Clinical Perspective Furqan Alex Khan, APRN ACNS-BC MSN alexkhan@prohealthcare.us Ket Harris Davis, APRN FNP-C DNP keturahnp@keturah-hms.com. Objectives Understand types of wounds Discuss
WOUND MANAGEMENT A Clinical Perspective Furqan Alex Khan, APRN ACNS-BC MSN alexkhan@prohealthcare.us Ket Harris Davis, APRN FNP-C DNP keturahnp@keturah-hms.com. Objectives Understand types of wounds Discuss
INSIDE. Stage II pressure ulcers are now
 Spring 2007, Volume 21 National Pressure Ulcer Advisory Panel the NPUAP In this issue President s Message NPUAP Award Honors CAC Member Profile: Healthpoint, Ltd. NPUAP Conferences Milestones Corporate
Spring 2007, Volume 21 National Pressure Ulcer Advisory Panel the NPUAP In this issue President s Message NPUAP Award Honors CAC Member Profile: Healthpoint, Ltd. NPUAP Conferences Milestones Corporate
CARE GUIDE for Pressure Ulcers
 Prevention (1,3) Risk assessment should be performed in both the inpatient and outpatient setting Evaluate for susceptibility for pressure ulcer using a standardized tool such as the Braden Scale The Braden
Prevention (1,3) Risk assessment should be performed in both the inpatient and outpatient setting Evaluate for susceptibility for pressure ulcer using a standardized tool such as the Braden Scale The Braden
Wound Classification. Overview
 Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Excellence in OASIS-C COS-C Prep & OASIS Training
 Excellence in OASIS-C COS-C Prep & OASIS Training Webinar Series - Session 5 April 2, 2014 2:00 3:00PM EST PRESENTER: JOAN L. USHER, BS, RHIA, COS-C, ACE JLU HEALTH RECORD SYSTEMS TEL: (781) 829-9632 FAX:
Excellence in OASIS-C COS-C Prep & OASIS Training Webinar Series - Session 5 April 2, 2014 2:00 3:00PM EST PRESENTER: JOAN L. USHER, BS, RHIA, COS-C, ACE JLU HEALTH RECORD SYSTEMS TEL: (781) 829-9632 FAX:
Frequently Asked Questions about Pressure Injury Staging. February 20, 2018, 1 to 2 pm ET
 Frequently Asked Questions about Pressure February 20, 2018, 1 to 2 pm ET Scott Bolhack, MD, MBA, CMD, CWSP, FACP, FAAP Janet Cuddigan. PhD, RN, CWCN, FAAN Joyce A. Pittman, PhD, ANP-BC, FNP-BC, CWOCN
Frequently Asked Questions about Pressure February 20, 2018, 1 to 2 pm ET Scott Bolhack, MD, MBA, CMD, CWSP, FACP, FAAP Janet Cuddigan. PhD, RN, CWCN, FAAN Joyce A. Pittman, PhD, ANP-BC, FNP-BC, CWOCN
QUICK GUIDE PRESSURE ULCER PREVENTION FOR HEALTHCARE PROFESSIONALS
 QUICK GUIDE PRESSURE ULCER PREVENTION FOR HEALTHCARE PROFESSIONALS This booklet has been produced by Invacare for healthcare professionals working with individuals at risk of developing pressure ulcers.
QUICK GUIDE PRESSURE ULCER PREVENTION FOR HEALTHCARE PROFESSIONALS This booklet has been produced by Invacare for healthcare professionals working with individuals at risk of developing pressure ulcers.
Wound Care per HHVNA Wound Product Formulary
 Venous Ulcers ABI of 0.9-1.2 = normal blood flow An ABI MUST be obtained prior to inititiation of compression therapy. Compression is the Gold Standard of care to promote wound of venous ulcers. Elevation
Venous Ulcers ABI of 0.9-1.2 = normal blood flow An ABI MUST be obtained prior to inititiation of compression therapy. Compression is the Gold Standard of care to promote wound of venous ulcers. Elevation
Definitions and criteria
 Several disciplines are involved in the management of diabetic foot disease and having a common vocabulary is essential for clear communication. Thus, based on a review of the literature, the IWGDF has
Several disciplines are involved in the management of diabetic foot disease and having a common vocabulary is essential for clear communication. Thus, based on a review of the literature, the IWGDF has
Wound Care Evaluation by Kris Dalseg MS PT CWS CLT
 Wound Care Evaluation by Kris Dalseg MS PT CWS CLT This document is intended to describe a standard wound care evaluation for healthcare practitioners. In healthcare, all aspects of our treatment have
Wound Care Evaluation by Kris Dalseg MS PT CWS CLT This document is intended to describe a standard wound care evaluation for healthcare practitioners. In healthcare, all aspects of our treatment have
CRRN Review Course 2017 Skin and Wound Management. Presented by: Jenifer Stevenson BSN, CRRN, CNML
 CRRN Review Course 2017 Skin and Wound Management Presented by: Jenifer Stevenson BSN, CRRN, CNML Disclosure The presenter for this presentation has disclosed no conflict of interest related to this topic.
CRRN Review Course 2017 Skin and Wound Management Presented by: Jenifer Stevenson BSN, CRRN, CNML Disclosure The presenter for this presentation has disclosed no conflict of interest related to this topic.
Ann Leland, APRN, CNP, DNP Instructor, college of surgery
 Ann Leland, APRN, CNP, DNP Instructor, college of surgery leland.ann@mayo.edu 2015 MFMER 3543652-1 Pressure ulcers Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for NPs
Ann Leland, APRN, CNP, DNP Instructor, college of surgery leland.ann@mayo.edu 2015 MFMER 3543652-1 Pressure ulcers Mayo School of Continuous Professional Development 2nd Annual Inpatient Medicine for NPs
DMEPOS: hospital beds, bed accessories, and pressurereducing
 ACTION: Final DATE: 07/02/2018 10:03 AM 5160-10-18 DMEPOS: hospital beds, bed accessories, and pressurereducing support surfaces. (A) Definitions and explanations. (1) "Group 1," "group 2," and "group
ACTION: Final DATE: 07/02/2018 10:03 AM 5160-10-18 DMEPOS: hospital beds, bed accessories, and pressurereducing support surfaces. (A) Definitions and explanations. (1) "Group 1," "group 2," and "group
See Policy CPT/HCPCS CODE section below for any prior authorization requirements
 Effective Date: 7/1/2018 Section: DME Policy No: 377 Medical Officer 7/1/18 Date Technology Assessment Committee Approved Date: 10/10; 10/13; 9/14: 9/15; 4/16 Medical Policy Committee Approved Date: 3/03;
Effective Date: 7/1/2018 Section: DME Policy No: 377 Medical Officer 7/1/18 Date Technology Assessment Committee Approved Date: 10/10; 10/13; 9/14: 9/15; 4/16 Medical Policy Committee Approved Date: 3/03;
ד"ר בוריס פונצ' קי PRESSURE ULCERS
 ד"ר בוריס פונצ' קי 25.12.2013 PRESSURE ULCERS International EPUAP-NPUAP Pressure Ulcer Definition: (European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel, 2010).. is localized
ד"ר בוריס פונצ' קי 25.12.2013 PRESSURE ULCERS International EPUAP-NPUAP Pressure Ulcer Definition: (European Pressure Ulcer Advisory Panel and National Pressure Ulcer Advisory Panel, 2010).. is localized
Chapter 36 & 37. Types of wounds. Skin Tear
 Chapter 36 & 37 Wound Care and Pressure Ulcers Types of wounds A wound is a break in the skin d/t trauma, surgical incision, pressure sore, circulatory ulcers Abrasion, Contusion, Incision, Laceration,
Chapter 36 & 37 Wound Care and Pressure Ulcers Types of wounds A wound is a break in the skin d/t trauma, surgical incision, pressure sore, circulatory ulcers Abrasion, Contusion, Incision, Laceration,
Pressure Ulcer Prevention for OR. Jeanne Knecht RN, CWON Wound/Ostomy Specialist
 Pressure Ulcer Prevention for OR Jeanne Knecht RN, CWON Wound/Ostomy Specialist Benefis Hospital Stats 2009 12 month incident rate 1.90 Benefis Benchmark 3 National Benchmark 5-8 How did we achieve Education
Pressure Ulcer Prevention for OR Jeanne Knecht RN, CWON Wound/Ostomy Specialist Benefis Hospital Stats 2009 12 month incident rate 1.90 Benefis Benchmark 3 National Benchmark 5-8 How did we achieve Education
Address: Left Leg. other: Nails: thick yellow brittle fungus abnormal thick yellow brittle fungus abnormal
 South West Regional Wound Care Toolkit: Interdisciplinary Lower Leg Assessment Form Instructions for use: Competent/ Proficient/ Expert level HCP to complete if lower leg ulcer present or risk of ulcer
South West Regional Wound Care Toolkit: Interdisciplinary Lower Leg Assessment Form Instructions for use: Competent/ Proficient/ Expert level HCP to complete if lower leg ulcer present or risk of ulcer
Determining Wound Diagnosis and Documentation Tips Job Aid
 Determining Wound Diagnosis and Job Aid 1 Coding Is this a traumatic injury from an accident? 800 Codes - Injury Section of the Coding Manual Code by specific site of injury. Only use for accidents or
Determining Wound Diagnosis and Job Aid 1 Coding Is this a traumatic injury from an accident? 800 Codes - Injury Section of the Coding Manual Code by specific site of injury. Only use for accidents or
Objectives. Wisconsin Case Facts. Wounds: The Criminalization of Skin Failure. Lived with aunt for 8 years Aunt s wishes
 Wounds: The Criminalization of Skin Failure Joyce Schank, RN, MSN, ANP, CWOCN, Penn Yan NY Objectives Discuss methods to protect caretakers and clinicians from civil/criminal charges for unavoidable skin
Wounds: The Criminalization of Skin Failure Joyce Schank, RN, MSN, ANP, CWOCN, Penn Yan NY Objectives Discuss methods to protect caretakers and clinicians from civil/criminal charges for unavoidable skin
Consider the possibility of pressure ulcer development
 Douglas Fronzaglia II, DO, MS LECOM Institute for Successful Aging LECOM Institute for Advanced Wound Care and Hyperbaric Medicine Consider the possibility of pressure ulcer development 1 Identify ulcer
Douglas Fronzaglia II, DO, MS LECOM Institute for Successful Aging LECOM Institute for Advanced Wound Care and Hyperbaric Medicine Consider the possibility of pressure ulcer development 1 Identify ulcer
WOCN Document:
 WOCN Document: www.cms.hhs.gov/medicaid/surveycert/080601.pdf OASIS Training Internet site: www.oasistraining.org M0440 Does this patient have a Skin Lesion or an Open Wound? This excludes "OSTOMIES."
WOCN Document: www.cms.hhs.gov/medicaid/surveycert/080601.pdf OASIS Training Internet site: www.oasistraining.org M0440 Does this patient have a Skin Lesion or an Open Wound? This excludes "OSTOMIES."
Coding and Documenting Pressure Injuries and Chronic Ulcers. September 21, 2016
 Coding and Documenting Pressure Injuries and Chronic Ulcers Laurie M. Johnson, MS, RHIA, FAHIMA AHIMA Approved ICD-10-CM/PCS Trainer Director of HIM Consulting Services Panacea Healthcare Solutions, Sandy
Coding and Documenting Pressure Injuries and Chronic Ulcers Laurie M. Johnson, MS, RHIA, FAHIMA AHIMA Approved ICD-10-CM/PCS Trainer Director of HIM Consulting Services Panacea Healthcare Solutions, Sandy
Part 4: OASIS C2 Accuracy
 Part 4: OASIS C2 Accuracy Presented by: Sharon Molinari, RN, HCS D, HCS O For: HealthCare Synergy 1 M2020/M2030 General Rules o If a patient does not have the requisite knowledge of a drug s dose and administration
Part 4: OASIS C2 Accuracy Presented by: Sharon Molinari, RN, HCS D, HCS O For: HealthCare Synergy 1 M2020/M2030 General Rules o If a patient does not have the requisite knowledge of a drug s dose and administration
Topical Oxygen Wound Therapy (MEDICAID)
") Topical Oxygen Wound Therapy (MEDICAID) Last Review Date: September 8, 2017 Number: MG.MM.DM.15C8v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or
Topical Oxygen Wound Therapy (MEDICAID) Last Review Date: September 8, 2017 Number: MG.MM.DM.15C8v2 Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or
Prepared and Presented by: Ms. Sohad Noorsaeed, RN. MSN
 Prepared and Presented by: Ms. Sohad Noorsaeed, RN. MSN Learning Outcomes Upon the completion of Skin integrity lecture, the learners will be able to: 1. Describe factors affecting skin integrity. 2. Identify
Prepared and Presented by: Ms. Sohad Noorsaeed, RN. MSN Learning Outcomes Upon the completion of Skin integrity lecture, the learners will be able to: 1. Describe factors affecting skin integrity. 2. Identify
Wound and Skin Care. What every nurse needs to know! Ruhama Bond, RN. Updated 14 February 2013/ Updated 6/17/13 Updated 10/28/13
 Wound and Skin Care What every nurse needs to know! Ruhama Bond, RN Updated 14 February 2013/ Updated 6/17/13 Updated 10/28/13 Objectives Demonstrate the use of the Braden Scale Pressure Ulcer Risk Assessment
Wound and Skin Care What every nurse needs to know! Ruhama Bond, RN Updated 14 February 2013/ Updated 6/17/13 Updated 10/28/13 Objectives Demonstrate the use of the Braden Scale Pressure Ulcer Risk Assessment
Peripheral Vascular Examination. Dr. Gary Mumaugh Western Physical Assessment
 Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Peripheral Vascular Examination Dr. Gary Mumaugh Western Physical Assessment Competencies 1. Inspection of upper extremity for: size symmetry swelling venous pattern color Texture nail beds Competencies
Saving Face Strategies to reduce skin breakdown during noninvasive ventilation (NIV) for patient care
 for patient care") 1 Saving Face Strategies to reduce skin breakdown during noninvasive ventilation (NIV) for patient care Objectives Define the key factors that can lead to mask-related NIV complications Define ways to
1 Saving Face Strategies to reduce skin breakdown during noninvasive ventilation (NIV) for patient care Objectives Define the key factors that can lead to mask-related NIV complications Define ways to
Rapid Foot Screening
 GP Symposium 2015 Workshop Rapid Foot Screening Ms Chelsea Law, Principal Podiatrist Mr Henry Lee, Podiatrist Ms Ng Jia Lin, Podiatrist Ms Polly Lim, Podiatrist Ms Wong Wan Mun, Podiatrist Mr Yeo Boon
GP Symposium 2015 Workshop Rapid Foot Screening Ms Chelsea Law, Principal Podiatrist Mr Henry Lee, Podiatrist Ms Ng Jia Lin, Podiatrist Ms Polly Lim, Podiatrist Ms Wong Wan Mun, Podiatrist Mr Yeo Boon
Differentiating Incontinence Associated Dermatitis from Category/Stage II Pressure Ulcers
 Differentiating Incontinence Associated Dermatitis from Category/Stage II Pressure Ulcers Suzanne Collins, MS BSN RN CWOCN Mid Atlantic Region Clinical Specialist Mölnlycke Health Care 1 Pre-Test: 1. What
Differentiating Incontinence Associated Dermatitis from Category/Stage II Pressure Ulcers Suzanne Collins, MS BSN RN CWOCN Mid Atlantic Region Clinical Specialist Mölnlycke Health Care 1 Pre-Test: 1. What
Slide 1. Slide 2 Disclosures. Slide 3 Objectives. Karen Rogge Miller, RN, BS, WCC Wound and Ostomy Clinician
 Slide 1 Karen Rogge Miller, RN, BS, WCC Wound and Ostomy Clinician Slide 2 Disclosures Wound and Ostomy RN at St. Vincent Healthcare and Billings Clinic, Billings, MT Former employee of KCI, a division
Slide 1 Karen Rogge Miller, RN, BS, WCC Wound and Ostomy Clinician Slide 2 Disclosures Wound and Ostomy RN at St. Vincent Healthcare and Billings Clinic, Billings, MT Former employee of KCI, a division
Promoting Skin Integrity in End of Life Care. Part 1. Tracey McKenzie Head of Tissue Viability Services TSDFT
 Promoting Skin Integrity in End of Life Care Part 1 Tracey McKenzie Head of Tissue Viability Services TSDFT To Understand the Extrinsic Factors of Pressure Ulcer (PU) development To understand the Intrinsic
Promoting Skin Integrity in End of Life Care Part 1 Tracey McKenzie Head of Tissue Viability Services TSDFT To Understand the Extrinsic Factors of Pressure Ulcer (PU) development To understand the Intrinsic
Lower Extremity Venous Disease (LEVD)
") Lower Extremity Venous Disease (LEVD) Lower Extremity Venous Disease (LEVD) Wounds Etiology Lower extremity venous leg ulcers are caused by chronic venous hypertension. Failure of valves in the veins or
Lower Extremity Venous Disease (LEVD) Lower Extremity Venous Disease (LEVD) Wounds Etiology Lower extremity venous leg ulcers are caused by chronic venous hypertension. Failure of valves in the veins or
Person s Name: ID Number: Date:
 South West Regional Wound Care Program Person s Name: ID Number: Interdisciplinary Diabetic/Neuropathic Foot Assessment Form MEDICAL HISTORY: Question Year diabetes diagnosed: Characteristics of onset
South West Regional Wound Care Program Person s Name: ID Number: Interdisciplinary Diabetic/Neuropathic Foot Assessment Form MEDICAL HISTORY: Question Year diabetes diagnosed: Characteristics of onset
Diabetic Foot Ulcers. Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C. Advanced Practice Nurse / Adult Clinical Nurse Specialist
 Diabetic Foot Ulcers Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C Advanced Practice Nurse / Adult Clinical Nurse Specialist Organization of Wound Care Nurses www.woundcarenurses.org Objectives Identify Diabetic/Neuropathic
Diabetic Foot Ulcers Alex Khan APRN ACNS-BC MSN CWCN CFCN WCN-C Advanced Practice Nurse / Adult Clinical Nurse Specialist Organization of Wound Care Nurses www.woundcarenurses.org Objectives Identify Diabetic/Neuropathic
Venous. Arterial. Neuropathic (e.g. diabetic foot ulcer) Describe Wound Types & Stages of. Pressure Ulcers. Identify Phases of Healing & Wound Care
 Describe Wound Types & Stages of. Pressure Ulcers. Identify Phases of Healing & Wound Care") A dressing the situation at hand Describe Wound Types & Stages of Pressure Ulcers Identify Phases of Healing & Wound Care Goals Clarify Referral Protocol Lacerations- The goal is nearest to complete approximation
A dressing the situation at hand Describe Wound Types & Stages of Pressure Ulcers Identify Phases of Healing & Wound Care Goals Clarify Referral Protocol Lacerations- The goal is nearest to complete approximation
Venous Insufficiency Ulcers. Patient Assessment: Superficial varicosities. Evidence of healed ulcers. Dermatitis. Normal ABI.
 Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Integumentary System (Skin) Unit 6.3 (6 th Edition) Chapter 7.3 (7 th Edition)
 Unit 6.3 (6 th Edition) Chapter 7.3 (7 th Edition)") Integumentary System (Skin) Unit 6.3 (6 th Edition) Chapter 7.3 (7 th Edition) 1 Learning Objectives Identify the major components (anatomy) of skin Differentiate between the two types of skin glands Explain
Integumentary System (Skin) Unit 6.3 (6 th Edition) Chapter 7.3 (7 th Edition) 1 Learning Objectives Identify the major components (anatomy) of skin Differentiate between the two types of skin glands Explain
Preventing Foot Ulcers in the Neuropathic Diabetic Foot. Glossary of Terms
 Preventing Foot Ulcers in the Neuropathic Diabetic Foot Warren Woods, Certified Orthotist, Health Sciences Centre, Rehabilitation Engineering Department What you need to know Glossary of Terms Neuropathic
Preventing Foot Ulcers in the Neuropathic Diabetic Foot Warren Woods, Certified Orthotist, Health Sciences Centre, Rehabilitation Engineering Department What you need to know Glossary of Terms Neuropathic
Assessment & Management of Wounds in primary practice.
 Assessment & Management of Wounds in primary practice. Nutrition Successful wound management depends on appropriate nutritional support. Poor nutrition is recognised as one of the major causes of poor
Assessment & Management of Wounds in primary practice. Nutrition Successful wound management depends on appropriate nutritional support. Poor nutrition is recognised as one of the major causes of poor
Identification Information.
 Section A. Identification Information. A1200. Marital Status. 1. Never married. 2. Married. 3. Widowed. 4. Separated. 5. Divorced. A1300. Optional Resident Items. A. Medical record number: B. Room number:
Section A. Identification Information. A1200. Marital Status. 1. Never married. 2. Married. 3. Widowed. 4. Separated. 5. Divorced. A1300. Optional Resident Items. A. Medical record number: B. Room number:
Welcome to NuMed! Our Commitment: Quality Products, Cost Savings, Exceptional Service
 It s a New Day in Wound Care Welcome to NuMed! Our Commitment: Quality Products, Cost Savings, Exceptional Service NuMed Industries is a manufacturing company that specializes in Advanced Wound Care products.
It s a New Day in Wound Care Welcome to NuMed! Our Commitment: Quality Products, Cost Savings, Exceptional Service NuMed Industries is a manufacturing company that specializes in Advanced Wound Care products.
Pressure Ulcers Memory Aid
 Pressure Ulcers Memory Aid Pocket Guide This pocket guide is intended as a memory aid at the bedside. For more complete information on pressure ulcers, please refer to the Ferris-sponsored Pressure Ulcer
Pressure Ulcers Memory Aid Pocket Guide This pocket guide is intended as a memory aid at the bedside. For more complete information on pressure ulcers, please refer to the Ferris-sponsored Pressure Ulcer
Appropriate Dressing Selection For Treating Wounds
 Appropriate Dressing Selection For Treating Wounds Criteria to Consider for an IDEAL DRESSING Exudate Management Be able to provide for moist wound healing by absorbing exudate or adding moisture Secure
Appropriate Dressing Selection For Treating Wounds Criteria to Consider for an IDEAL DRESSING Exudate Management Be able to provide for moist wound healing by absorbing exudate or adding moisture Secure
The Triangle of Wound Assessment
 The Triangle of Wound Assessment A simple and holistic framework for wound management CPWSC_TOWA_Brochure_210x210_2018.indd 1 10/01/2018 15.13 ? We asked healthcare professionals around the world about
The Triangle of Wound Assessment A simple and holistic framework for wound management CPWSC_TOWA_Brochure_210x210_2018.indd 1 10/01/2018 15.13 ? We asked healthcare professionals around the world about
Leg ulcer assessment and management
 Leg ulceration The views expressed in this presentation are solely those of the presenter and do not necessarily represent the views of Smith & Nephew. Smith & Nephew does not guarantee the accuracy or
Leg ulceration The views expressed in this presentation are solely those of the presenter and do not necessarily represent the views of Smith & Nephew. Smith & Nephew does not guarantee the accuracy or
Advazorb. Hydrophilic foam dressing range
 Advazorb Hydrophilic foam dressing range Advazorb A comprehensive range of patient friendly, absorbent foam dressings Non-adhesive and atraumatic silicone adhesive options Designed to manage exudate whilst
Advazorb Hydrophilic foam dressing range Advazorb A comprehensive range of patient friendly, absorbent foam dressings Non-adhesive and atraumatic silicone adhesive options Designed to manage exudate whilst
Update on Pressure Ulcers: Utilizing an Interdisciplinary Approach to Pressure Ulcer Prevention. Charlene A. Demers GNP-BC, CWOCN
 Update on Pressure Ulcers: Utilizing an Interdisciplinary Approach to Pressure Ulcer Prevention Charlene A. Demers GNP-BC, CWOCN Scope of the Issue Cost $9 billion to $11 billion $20,000-$150,000 per ulcer
Update on Pressure Ulcers: Utilizing an Interdisciplinary Approach to Pressure Ulcer Prevention Charlene A. Demers GNP-BC, CWOCN Scope of the Issue Cost $9 billion to $11 billion $20,000-$150,000 per ulcer
2/11/2016. Palliative Wound Management Workshop. Carolyn Brown BS, MEd, RN, ARM, CWS, FACCWS Carolyn Brown Consulting
 Palliative Wound Management Workshop Be the best that you can be! Carolyn Brown BS, MEd, RN, ARM, CWS, FACCWS Carolyn Brown Consulting 727-348-5856 cbjackwill@gmail.com Learner Objectives After attending
Palliative Wound Management Workshop Be the best that you can be! Carolyn Brown BS, MEd, RN, ARM, CWS, FACCWS Carolyn Brown Consulting 727-348-5856 cbjackwill@gmail.com Learner Objectives After attending
Example. July 2013 Q&A #7. Q & A October 2013 Category 4 Question 5. Q&A October 2013 Category 4 Question 4
 1 July 213 Q&A #7 Q: Define all of the time does pain have to keep patient awake all night long in order to select it? A: At all times means constantly throughout the day and night with little or no relief.
1 July 213 Q&A #7 Q: Define all of the time does pain have to keep patient awake all night long in order to select it? A: At all times means constantly throughout the day and night with little or no relief.
Arterial & Venous Ulcers. A Comprehensive Review Assessment & Management
 Arterial & Venous Ulcers A Comprehensive Review Assessment & Management 1 Objectives Understand Arterial & Venous disease Understand the etiology of lower extremities ulcers Understand assessment of lower
Arterial & Venous Ulcers A Comprehensive Review Assessment & Management 1 Objectives Understand Arterial & Venous disease Understand the etiology of lower extremities ulcers Understand assessment of lower
SKIN INTEGRITY & WOUND CARE
 SKIN INTEGRITY & WOUND CARE Chapter 34 1 skin integrity: intact skin refers to the presence of normal skin layer uninterrupted by wound 2 WOUNDS DISRUPTION IN THE INTEGRITY OF BODY TISSUE CLASSIFIED AS:
SKIN INTEGRITY & WOUND CARE Chapter 34 1 skin integrity: intact skin refers to the presence of normal skin layer uninterrupted by wound 2 WOUNDS DISRUPTION IN THE INTEGRITY OF BODY TISSUE CLASSIFIED AS:
DEEP TISSUE INJURY IN THE BARIATRIC POPULATION DEFINITION HOW IS OVERWEIGHT DEFINED?
 DEEP TISSUE INJURY IN THE BARIATRIC POPULATION James G. Spahn, MD, FACS 1 DEFINITION Bariatrics The field of medicine that offers treatment for the person that is overweight. 2 HOW IS OVERWEIGHT DEFINED?
DEEP TISSUE INJURY IN THE BARIATRIC POPULATION James G. Spahn, MD, FACS 1 DEFINITION Bariatrics The field of medicine that offers treatment for the person that is overweight. 2 HOW IS OVERWEIGHT DEFINED?
Wound Assessment & Management
 Wound Assessment & Management Kim Krog, RN, BScN, CRN(C ) Contributors: Carol Thompson, RN, BScN, CRN(C ) Mary Scarlet, RN, BScN, CRN (C) Objectives Review: Anatomy and physiology of skin Enhance knowledge
Wound Assessment & Management Kim Krog, RN, BScN, CRN(C ) Contributors: Carol Thompson, RN, BScN, CRN(C ) Mary Scarlet, RN, BScN, CRN (C) Objectives Review: Anatomy and physiology of skin Enhance knowledge
Bacterial Burden (Bioburden) The metabolic load imposed by bacteria in tissue.
 The metabolic load imposed by bacteria in tissue.") Glossary Ankle Brachial Index (ABI) Is a numerical figure which indicates a quantifiable pressure index. The pressure index is determined by means of Doppler Ultra Sound. The ABI is obtained by dividing
Glossary Ankle Brachial Index (ABI) Is a numerical figure which indicates a quantifiable pressure index. The pressure index is determined by means of Doppler Ultra Sound. The ABI is obtained by dividing
Essential Elements of Pressure Ulcer Prevention & Management
 All Wales Tissue Viability Nurse Forum Fforwm Nyrsys Hyfywedd Meinwe Cymru Gyfan Essential Elements of Pressure Ulcer Prevention & Management All Wales Guidance for the Prevention & Management of Pressure
All Wales Tissue Viability Nurse Forum Fforwm Nyrsys Hyfywedd Meinwe Cymru Gyfan Essential Elements of Pressure Ulcer Prevention & Management All Wales Guidance for the Prevention & Management of Pressure
Negative Pressure Wound Therapy Pumps
 Negative Pressure Wound Therapy Pumps Adopted from the National Government Services website. For any item to be covered by The Health Plan, it must: 1. Be eligible for a defined Medicare or The Health
Negative Pressure Wound Therapy Pumps Adopted from the National Government Services website. For any item to be covered by The Health Plan, it must: 1. Be eligible for a defined Medicare or The Health
DIABETIC ULCERS V PRESSURE ULCERS SO, WHAT DO YOU CALL IT?
 DIABETIC ULCERS V PRESSURE ULCERS SO, WHAT DO YOU CALL IT? Arthur Stone, DPM Mary Sieggreen, MSN,CNS,NP,CVN Faculty Disclosure Dr. Stone has listed an affiliation with: Advisory Board Member..FXI, Inc.
DIABETIC ULCERS V PRESSURE ULCERS SO, WHAT DO YOU CALL IT? Arthur Stone, DPM Mary Sieggreen, MSN,CNS,NP,CVN Faculty Disclosure Dr. Stone has listed an affiliation with: Advisory Board Member..FXI, Inc.