Superficial Urothelial Cancer in the Prostatic Urethra
|
|
|
- Tamsyn McKenzie
- 5 years ago
- Views:
Transcription
1 Review Article Superficial Bladder Cancer TheScientificWorldJOURNAL (2006) 6, TSW Urology ISSN X; DOI /tsw Superficial Urothelial Cancer in the Prostatic Urethra Ziya Kirkali* and A. Erdem Canda Dokuz Eylul University School of Medicine Department of Urology, Izmir 35340, Turkey Received November 21, 2005; Revised February 6, 2006; Accepted February 10, 2006; Published February 28, 2006 Transitional cell carcinoma (TCC) is a multifocal disease of the urinary tract that can also involve the prostatic urethra (PU). The exact incidence of superficial involvement of the PU in patients with bladder TCC is not well known. Bladder TCC may involve the prostate in 12 40% of the patients and the degree of involvement can include urethral mucosa, ducts, acini, and stroma of the gland, which has been shown to affect the outcome. Risk factors for superficial urothelial cancer in the PU are high-grade, multifocal bladder TCC and presence of carcinoma in situ (CIS) in the bladder. While visible tumors are easy to detect and resect, controversy still exists regarding the optimal technique to identify prostatic involvement by TCC. Prostatic urethral sampling by a transurethral resection biopsy or a cold-cup biopsy, particularly in the high-risk group of bladder cancer patients, has been recommended for detecting prostatic urethral involvement. Management of superficial prostatic involvement by TCC is also unclear. Currently, there is increasing recognition of the value of conservative treatment options with intravesical agents when there is superficial involvement of the PU. Particularly, intravesical bacillus Calmette-Guèrin (BCG) seems to be an effective treatment alternative in the management of superficial involvement of the PU by TCC. Close follow-up by cystoscopy and PU biopsy at 3-month intervals, particularly in intermediate and high-risk patients who respond to intravesical therapy and in whom cystectomy is appropriate, is recommended in order to detect persistent tumor, recurrences, or progression. KEYWORDS: bladder cancer, superficial bladder tumors, prostatic urethral tumor, transitional cell carcinoma INTRODUCTION Transitional cell carcinoma (TCC) is a multifocal disease that can develop anywhere in the entire urinary tract, including the prostatic urethra (PU). The mucosa lining the PU and the prostatic ducts have the same transitional cell lining as the bladder; therefore, TCC can originate from or invade the prostate. The degree of prostatic involvement can include urethral mucosa, ducts, acini, and stroma of the gland, which has been shown to affect the outcome[1]. The exact incidence of superficial involvement of the PU in patients with bladder TCC is not well known and its management is still unclear. In this article, a brief update is presented on superficial urothelial cancer in the PU. *Corresponding author with author. Published by TheScientificWorld;
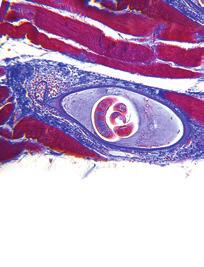
2 DEVELOPMENT Superficial involvement of the PU by TCC is not clearly understood and it appears that there are three possible ways in which TCC can develop in the PU. 1. Extension of the bladder TCC into the PU: Previously developed bladder TCC may extend from the bladder into the PU. 2. Implantation of the TCC cells shed from the bladder TCC on the PU: TCC cells shed from the primary tumor in the bladder can implant in the PU. Although it was suggested that freefloating tumor cells from the bladder tumors may implant at the traumatized sites particularly by instrumentation[2], it has recently been shown in a prospective study that simultaneous transurethral resection (TUR) of the bladder tumor and TUR of the prostate do not negatively affect tumor recurrence at the bladder neck and PU[3]. 3. The impact of carcinogens on the PU: Because the mucosa lining the PU and the prostatic ducts have the same transitional cell lining as in the bladder, carcinogens playing a role in the development of bladder TCC may cause the same process in the PU, leading to the development of primary prostatic TCC. INCIDENCE Primary TCC of the prostatic urothelium is rare, occurring in 1 4% of patients[4], but development of TCC in the PU during follow-up of bladder cancer patients is more common and has been reported in 12 40% of patients[5,6]. The exact incidence of superficial involvement of the PU in patients with bladder TCC is not well known and since PU biopsies have not been done routinely, the incidence of PU involvement might be higher than expected[7]. Prostatic urethral involvement was detected to be 7 43% in the cystoprostatectomy specimens of the patients treated for bladder cancer[8,9,10,11,12]. Mungan et al.[13] reported the incidence of superficial PU involvement as 6.2% in patients with superficial TCC of the bladder. The development of TCC in all celular layers of the prostatic urethral mucosa is considered as carcinoma in situ (CIS) of the PU and its incidence has been reported to be %[14]. Herr and Donat[15] evaluated a series of 186 male, superficial bladder TCC patients with a follow-up of 15 years. Noninvasive prostatic tumor (prostatic urethral and ductal) was detected in 45 patients (24%) and stromal invasion was detected in 27 patients (15%) after a median follow-up of 28 months with survival rates of 82 and 48%, respectively. They concluded that relapse of superficial bladder TCC in the prostate may portend tumor invasion in the bladder, stromal invasion in the prostate, and has a significant impact on survival. RISK FACTORS Multiple and recurrent superficial TCCs of the bladder recur more often than solitary and primary tumors, high-grade tumors more frequently than low-grade tumors, and pt 1 more frequently than pt a neoplasms[16,17]. Prostatic urethral TCC has been detected to be more common in bladder cancer patients with high-grade, multifocal tumors with CIS; therefore, routine sampling of the PU by TUR biopsies have previously been recommended in patients at high risk[18] (Fig. 1). Herr[19] reported on 307 patients with multiple recurrent papillary TCCs and CIS of the bladder who were treated with TUR and intravesical BCG with a median follow-up of 12 years. Tumors were detected in the PU or ducts in 61 out of 251 men (24%) and tumors in the upper urinary tract (UUT) in 78 out of 307 patients (25%). It was concluded that tumor relapse risk is increased in the extravesical sites such as PU and UUT in patients with high-risk superficial bladder tumors. Extravesical tumors were detected during investigation of a positive urine cytology after no tumor was found in the bladder. 2604

3 FIGURE 1. TCC of prostatic urethral epithelium (Hematoxylin-Eosin Stain, 40 ). Recently, Mungan et al.[13] investigated the factors affecting superficial involvement of the PU in patients with superficial bladder TCC. They evaluated the impact of pathological stage, grade, tumor multiplicity, and presence of CIS on mucosal PU involvement in a series of 340 male patients with the diagnosis of primary superficial bladder TCC. In univariate analysis, although tumor stage, grade, and multiplicity were found to be predicting factors, multivariate analysis revealed that only the bladder tumor multiplicity was found to be an independent predictor for superficial PU involvement by TCC. They demonstrated that the risk of superficial PU involvement with multiple tumors was 16 times higher than the risk of the tumor stage and grade[13]. They suggested that patients, particularly those with multiple superficial TCC of the bladder, seem to have an additional increased risk of superficial PU involvement. Several studies have reported that the PU is a common site of recurrence after the use of BCG for bladder TCC[20,21]. Therefore, close surveillance of the PU in conservatively treated patients by cystoscopy and PU biopsy is important. DIAGNOSIS Cystoscopy is the gold standard for detecting urothelial pathologies. Although preoperative cystoscopy was suggested to have a 83% sensitivity and 95% specifity for correctly diagnosing prostatic urethral TCC[22], TCC and even CIS might be present in the normal-appearing PU as isolated tumors[13]. Cystoscopic appearance of CIS is described as an erythematous, patchy, slightly raised, velvety lesion that has the potential for progression[14]. Particularly in patients with an enlarged, friable, and vascular 2605
4 prostate, it might be much more difficult to differentiate prostatic urethral CIS. Therefore, prostatic urethral sampling may be the best method for detecting prostatic urethral involvement by TCC and CIS. Currently, controversy exists regarding the optimal technique to identify prostatic involvement by TCC. TUR biopsy or a cold-cup biopsy of the PU and prostate has been recommended in patients with bladder carcinoma, particularly those at high risk[13,23,24,25]. It was also suggested that prostatic urethral involvement might be present in patients with a positive urinary cytology following a complete response to intravesical therapy for bladder cancer[26]. Therefore, TUR biopsies of the prostate between the 5 and 7 o clock positions along the entire length of the PU was recommended in order to detect prostatic urethral TCC in patients who have positive urinary cytology after complete TUR of bladder tumors or intravesical therapy[27]. Other less-invasive techniques might underestimate the extent of disease in these patients. Sakamoto et al.[7] suggested that TUR biopsy at the 5 and/or 7 o clock position of the verumontanum improves the detection of prostatic duct and acini involvement by TCC in bladder cancer patients. In one study, the significance of cystoscopically normal appearing PU biopsies in patients who underwent cystectomy for invasive bladder cancer was investigated[28]. In this series, 40 men with cystoscopically normal prostatic fossa had negative prostatic biopsies and had orthotopic neobladder substitution. However, TCC involving the prostate was detected histopathologically in 3 out of these 40 patients after the pathological examination was performed. They concluded that TUR biopsy of the PU before cystectomy in patients with cystoscopically normal appearing PU has limited value. Similarly, in another study, the specificity, sensitivity, and positive predictive value of TUR biopsies of the PU for predicting the degree of involvement at cystectomy was low[29]. Matzkin et al.[18] suggested that demonstration of stromal invasion is not also present on TUR biopses of the prostate, showing ductal involvement is difficult. It is claimed that patients with BCG-refractory TCC of the bladder with a poor surgical risk for cystectomy may benefit from continued intravesical therapy without a significant risk of progression[30]. Very close follow-up in order to detect bladder recurrences, as well as prostatic urethral and upper urinary tract involvement, is necessary. The tumor in the PU at endoscopic staging was found to be the only factor associated with understaging and shorter survival in patients who underwent radical cystectomy for high-risk superficial bladder cancer after BCG failure[31]. MANAGEMENT The management of superficial urothelial cancer in the PU is unclear. Currently, there is increasing recognition of the value of conservative treatment options with intravesical agents when there is superficial involvement of the PU[23,32,33]. If TCC involves particularly the mucosa of the PU rather than the ducts or acinar structures, superficial tumor can respond to intravesical agents. Chemotherapeutic agents like Mitomycin C, Adriamycin, Epirubicin, and BCG have been used as intravesical agents in the conservative management of superficial involvement of the PU by TCC. It was suggested that this therapy seems to have a prophylactic effect on tumor reccurrence in the prostate[23,32,33,34,35,36,37]. Among these agents, intravesical BCG seems to be an effective treatment alternative in the management of superficial mucosal PU involvement (Table 1). Because the intravesical agents only contact with the prostatic urothelium during instillation and voiding, the mechanism of action of their effects in treating prostatic TCC is not clear. However, detection of granuloma formation in the post-treatment biopsies of the prostate and occurrence of granulomatous prostatitis after intravesical BCG administration support the effective penetration of BCG in the PU and prostate[23,38]. Moreover, the detection of elevated interleukin 2 and interferon levels after BCG instillation suggests that BCG induces these cytokines, which have antitumor activity[39]. 2606
5 TABLE 1 Complete Response (CR) Rates of Patients with Superficial Prostatic Urethral Involvement by TCC Who were Treated Conservatively by Intravesical Agents Agent Reference CR (%) Mitomycin-C or Adriamycin Solsona et al.[37] 37 Epirubicin Canda et al.[32] 29 BCG Bretton et al.[35] 48 Canda et al.[32] 58 Hillyard et al.[23] 75 Schellhammer et al.[34] 70 Palou et al.[33] 78 Orihuela et al.[36] 87 Low-Grade Superficial Urothelial Cancer in the PU Patients with low-grade superficial involvement of the PU by TCC can be managed conservatively by TUR and chemo/immunotherapy, particularly with BCG[32]. In case of recurrence as low-grade tumors, another TUR and intravesical local treatment with BCG seems to be successful. Meticulous follow-up by cystoscopy and PU biopsy at 3-month intervals, particularly in intermediate and high-risk patients who respond to intravesical BCG therapy and in whom cystectomy is appropriate, can detect persistent tumor, recurrences, or progression[32]. CIS and High-Grade Uurothelial Cancer in the PU The success rates in treating high-grade tumors and CIS of the PU by BCG range from % in the prostate and from 47 72% considering bladder and prostate[14,23,33,34,35]. It is more difficult to treat prostatic CIS or high-grade superficial involvement of the PU by TCC. Palou et al.[33] reported complete response in 14 of 18 patients with CIS of the PU who were treated with intravesical BCG and 3 patients progressed. Successful management of CIS of the prostate by intravesical BCG has also been supported by other authors[23,35]. In a study of 50 patients with prostatic TCC without invasive bladder carcinoma, the 5-year diseasespecific survival rate was 100% (n = 19) in patients with CIS of the PU and prostatic ducts and acini, whereas it was 45% (n = 21) in patients with TCC with stromal invasion[40]. Currently, it is well established that mucosal prostatic urethral involvement by urothelial cancer can be treated effectively with intravesical BCG administration, which is considered as the most effective treatment and prophylaxis for superficial TCC including CIS reducing tumor recurrence, disease progression, and mortality[41]. However, in those patients who fail conservative intravesical treatment with BCG, progression occurs more often in the bladder (40 60%) than in the prostate (20 30%)[42]. Therefore, close surveillance of the urinary tract including the PU in these patients is recommended. Prostatic Ductal Involvement by Urothelial Cancer The management of prostatic ductal involvement by TCC is also debatable. Although some authors recommend a trial of BCG and meticulous follow-up by prostate biopsies in patients with minimal ductal involvement[43], others suggest radical cystoprostatectomy[44]. 2607
6 Bretton et al.[35] reported an 87% complete response rate for prostatic urethral TCC after the treatment with intravesical BCG administration, but only 4 of 23 patients had ductal involvement and none had stromal invasion. Schellhammer et al.[34] stated that TCC involving prostatic urothelium or periurethral ducts is not a contraindication to a trial of intravesical BCG. Others suggest that minimal ductal involvement by TCC does not preclude a trial of BCG and recommended careful follow-up and prostate biopsies[43]. Since prostatic ductal involvement has the potential for invasion, when invasion occurs, radical cystoprostatectomy alone may not be sufficient because of the high risk of metastatic disease. Thus, adjuvant or neoadjuvant chemotherapy may be needed[44]. Martinez-Pineiro et al.[45] compared the efficacy of one-third of the dose vs. standard dose intravesical BCG administration in decreasing the risk of recurrence and progression after TUR in a series of 155 patients with superficial high-risk (stages T1G3 and CIS) bladder TCC. Four patients (6.1%) with CIS were detected to have local extension into the PU and ducts, including 3 (8.3%) treated with the standard dose and 1 (3.4%) treated with the decreased dose BCG. They concluded that threefolddecreased dose and standard dose intravesical BCG are similarly effective in preventing progression in patients with high-risk stages (T1G3 and CIS) of superficial bladder carcinoma, with one-third of the dose BCG having significantly less toxicity[45]. In another study, the degree of TCC extension into the prostate and survival in 76 male patients who underwent radical cystectomy were investigated[12]. The authors detected similar survival rates in patients with prostatic urethral and ductal involvement by TCC without stromal invasion. It is suggested that survival is related with the stage of the primary bladder TCC. In conclusion, superficial involvement of the PU by TCC is not a rare entity and is detected more commonly in bladder cancer patients with high-grade, multifocal tumors and with CIS. Although no prospective study currently exists assessing the value of prostatic urethral sampling in this patient group, taking biopsies from the PU particularly in this high-risk group might be important. In general, it is easy to identify prostatic urethral TCC by cystoscopy, however, it is important to keep in mind that these tumors may be present in the normal-appearing PU. Currently, a trial of intravesical BCG as a conservative treatment option is recommended in patients with superficial involvement of the PU by TCC with close follow-up by cystoscopy and PU biopsy. REFERENCES 1. Pagano, F., Bassi, P., Ferrante, G.L., Piazza, N., Abatangelo, G., Pappagallo, G.L., and Garbeglio, A. (1996) Is pt4a (D1) stage reliable in assessing transitional cell carcinoma involvement of the prostate in patients with concurrent bladder cancer? A necessary distinction for contiguous and noncontiguous involvement. J. Urol. 155, Pode, D., Alon, Y., Horowitz, A.T., Vlodansky, I., and Biran, S. (1986) The mechanism of human bladder tumor implantation in an in vitro model. J. Urol. 136(2), Tsivian, A., Shtricker, A., and Sidi, A.A. (2003) Simultaneous transurethral resection of bladder tumor and benign prostatic hyperplasia: hazardous or a safe timesaver? J. Urol. 170(6 Pt 1), Bates, H.R. (1969) Transitional cell carcinoma of the prostate. J. Urol. 101, Hardeman, S.W. and Soloway, M.S. (1988) Transitional cell carcinoma of the prostate: diagnosis, staging and management. World J. Urol. 6, Freeman, J.A., Esrig, D., Stein, J.P., and Skinner, D.G. (1994) Management of the patient with bladder cancer. Urethral recurrence. Urol. Clin. North Am. 21(4), Sakamoto, N., Tsuneyoshi, M., Naito, S., and Kumazawa, J. (1993) An adequate sampling of the prostate to identify prostatic involvement by urothelial carcinoma in bladder cancer patients. J. Urol. 149, Schellhammer, P.F., Bean, M.A., and Whitmore, W.F., Jr. (1977) Prostatic involvement by transitional cell carcinoma: pathogenesis, patterns and prognosis. J. Urol. 118(3), Wolfe, J.H. and Lloyd-Davies, R.W. (1981) The management of transitional cell carcinoma in the prostate. Br. J. Urol. 53(3), Wood, D.P., Jr., Montie, J.E., Pontes, J.E., VanderBrug Medendorp, S., and Levin, H.S. (1989) Transitional cell carcinoma of the prostate in cystoprostatectomy specimens removed for bladder cancer. J. Urol. 141(2), De Paepe, M.E., Andre, R., and Mahadevia, P. (1990) Urethral involvement in female patients with bladder cancer. A 2608
7 study of 22 cystectomy specimens. Cancer 65(5), Njinou Ngninkeu, B., Lorge, F., Moulin, P., Jamart, J., and Van Cangh, P.J. (2003) Transitional cell carcinoma involving the prostate: a clinicopathological retrospective study of 76 cases. J. Urol. 169(1), Mungan, M.U., Canda, A.E., Tuzel, E., Yorukoglu, K., and Kirkali, Z. (2005) Risk factors for mucosal prostatic urethral involvement in superficial transitional cell carcinoma of the bladder. Eur. Urol. 48, Seemayer, T.A., Knaack, J., Thelmo, W.L., Wang, N.S., and Ahmed, N.M. (1975) Further observations on carcinoma in situ of the urinary bladder: silent but extensive intraprostatic involvement. Cancer 36, Herr, H.W. and Donat, S.M. (1999) Prostatic tumor relapse in patients with superficial bladder tumors: 15-year outcome. J. Urol. 161(6), Soloway, M.S. (1998) Intravesical therapy for bladder cancer. Urol. Clin. North Am. 15, Heney, N.M., Ahmed, S., Flanagan, M.J., Frable, W., Corder, M.P., Hafermann, M.D., and Hawkins, I.R. for the National Bladder Cancer Collaborative Group A (1983) Superficial bladder cancer: progression and recurrence. J. Urol. 130, Matzkin, H., Soloway, M.S., and Hardeman, S. (1991) Transitional cell carcinoma of the prostate. J. Urol. 146, Herr, H.W. (1998) Extravesical tumor relapse in patients with superficial bladder tumors. J. Clin. Oncol. 16(3), Herr, H.W., Pinsky, C.M., Whitmore, W.F., Jr., Sogani, P.C., Oettgen, H.F., and Melamed, M.R. (1986) Long term effect of intravesical bacillus Calmette-Guèrin on flat carcinoma in situ of the bladder. J. Urol. 135(2), Hardeman, S.W., Perry, A., and Soloway, M.S. (1988) Transitional cell carcinoma of the prostate following intravesical therapy for transitional cell carcinoma of the bladder. J. Urol. 140(2), Nixon, R.G., Chang, S.S., Lafleur, B.J., Smith, J.A., and Cookson, M.S. (2002) Carcinoma in situ and tumor multifocality predict the risk of prostatic urethral involvement at radical cystectomy in men with transitional cell carcinoma of the bladder. J. Urol. 167(2 Pt 1), Hillyard, R.W., Ladaga, L., and Schellhammer, P.F. (1988) Superficial transitional cell carcinoma of the bladder associated with mucosal involvement of the prostatic urethra: results of treatment with intravesical bacillus Calmette- Guèrin. J. Urol. 139, Rikken, C.H., van Helsdingen, P.J.R.O., and Kazzaz, B.A. (1987) Are biopsies from the prostatic urethra useful in patients with superficial bladder carcinoma? Br. J. Urol. 59, Wood, D.P., Montie, J.E., Pontes, J.E., and Levin, H.S. (1989) Identification of transitional cell carcinoma of the prostate in bladder cancer patients: a prospective study. J. Urol. 141, Schwalb, M.D., Herr, H.W., Sogani, P.C., Russo, P., Sheinfeld, J., and Fair, W.R. (1994) Positive urinary cytology following a complete response to intravesical bacillus Calmette-Guerin therapy: pattern of recurrence. J. Urol. 152(2 Pt 1), Schwalb, D.M., Herr, H.W., and Fair, W.R. (1993) The management of clinically unconfirmed positive urinary cytology. J. Urol. 150(6), Bulbul, M.A., Wazzan, W., Nasr, R., and Hemady, K. (2001) The value of cystoscopy, prostate biopsy and frozensection urethral biopsy prior to orthotopic neobladder substitution. Can. J. Urol. 8(3), Donat, S.M., Genega, E.M., Herr, H.W., and Reuter, V.E. (2001) Mechanisms of prostatic stromal invasion in patients with bladder cancer: clinical significance. J. Urol. 165, Luciani, L.G., Neulander, E., Murphy, W.M., and Wajsman, Z. (2001) Risk of continued intravesical therapy and delayed cystectomy in BCG-refractory superficial bladder cancer: an investigational approach. Urology 58(3), Huguet, J., Crego, M., Sabate, S., Salvador, J., Palou, J., and Villavicencio, H. (2005) Cystectomy in patients with high risk superficial bladder tumors who fail intravesical BCG therapy: pre-cystectomy prostate involvement as a prognostic factor. Eur. Urol. 48(1), Canda, A.E., Tuzel, E., Mungan, M.U., Yorukoglu, K., and Kirkali, Z. (2004) Conservative management of mucosal prostatic urethral involvement in patients with superficial transitional cell carcinoma of the bladder. Eur. Urol. 45(4), Palou, J., Xavier, B., Laguna, B., Montlleo, M., and Vicente, J. (1996) In situ transitional cell carcinoma involvement of prostatic urethra: bacillus Calmette-Guèrin therapy without previous transurethral resection of the prostate. Urology 57, Schellhammer, P.F., Ladaga, L.E., and Moriarty, R.P. (1995) Intravesical bacillus Calmette-Guèrin for treatment of superficial transitional cell carcinoma of prostatic urethra in association with carcinoma of the bladder. J. Urol. 153, Bretton, P.R., Herr, H.W., Whitmore, W.F., Jr., Badalament, R.A., Kimmel, M., Provet, J., Oettgen, H.F., Melamed, M.R., and Fair, W.R. (1989) Intravesical bacillus Calmette-Guèrin therapy for in situ transitional cell carcinoma involving the prostatic urethra. J. Urol. 141, Orihuela, E., Herr, H.W., and Whitmore, W.F. (1989) Conservative treatment of superficial transitional cell carcinoma of prostatic urethra with intravesical BCG. Urology 34(5), Solsona, E., Iborra, I., Ricos, J.V., Monros, J.L., Dumont, R., Casanova, J., and Calabuig, C. (1991) Recurrence of 2609
8 superficial tumors in prostatic urethra. Eur. Urol. 19, Lamm, D.L., Stogdill, B.J., and Crispen, R.G. (1986) Complications of bacillus Calmette-Guèrin immumotherapy in 1278 patients with bladder cancer. J. Urol. 135, Haaff, E.O., Catalona, W.J., and Ratliff, T.L. (1986) Detection of interleukin 2 in the urine of patients with superficial bladder tumors after treatment with intravesical BCG. J. Urol. 136(4), Cheville, J.C., Dundore, P.A., Bostwick, D.G., Lieber, M.M., Batts, K.P., Sebo, T.J., and Farrow, G.M. (1998) Transitional cell carcinoma of the prostate: clinicopathologic study of 50 cases. Cancer 82(4), Schenkman, E. and Lamm, D.L. (2004) Superficial bladder cancer therapy. TheScientificWorldJOURNAL 4(Suppl 1), Palou, J., Salvador, J., Parada, R., Chéchile, G., Millán, M., and Vicente, J. (2001) Carcinoma in situ of the prostatic urethra: the role of intravesical BCG. Urol. Integr. Invest. 6, Montie, J.E., Wood, D.P., Mendendorp, S.V., Levin, H.S., and Pontes, J.E. (1990) The significance and management of transitional cell carcinoma of the prostate. Semin. Urol. 8(4), Wishnow, K.I. and Ro, J.Y. (1988) Importance of early treatment of transitional cell carcinoma of prostatic ducts. Urology 32(1), Martinez-Pineiro, J.A., Martinez-Pineiro, L., Solsona, E., Rodriguez, R.H., Gomez, J.M., Martin, M.G., Molina, J.R., Collado, A.G., Flores, N., Isorna, S., Pertusa, C., Rabadan, M., Astobieta, A., Camacho, J.E., Arribas, S., Madero, R., Club Urologico Espanol de Tratamiento Oncologico (CUETO) (2005) Has a 3-fold decreased dose of bacillus Calmette-Guerin the same efficacy against recurrences and progression of T1G3 and Tis bladder tumors than the standard dose? Results of a prospective randomized trial. J. Urol. 174(4 Pt 1), This article should be cited as follows: Kirkali, Z. and Canda, A.E. (2006) Superficial urothelial cancer in the prostatic urethra. TSW Urology 1(S2), 1 8. DOI /tswurol











9 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Koji Ichihara Hiroshi Kitamura Naoya Masumori Fumimasa Fukuta Taiji Tsukamoto
 Int J Clin Oncol (2013) 18:75 80 DOI 10.1007/s10147-011-0346-8 ORIGINAL ARTICLE Transurethral prostate biopsy before radical cystectomy remains clinically relevant for decision-making on urethrectomy in
Int J Clin Oncol (2013) 18:75 80 DOI 10.1007/s10147-011-0346-8 ORIGINAL ARTICLE Transurethral prostate biopsy before radical cystectomy remains clinically relevant for decision-making on urethrectomy in
ICUD-EAU International Consultation on Bladder Cancer 2012: Urothelial Carcinoma of the Prostate
 EUROPEAN UROLOGY 63 (2013) 81 87 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review Bladder Cancer ICUD-EAU International Consultation on Bladder Cancer 2012: Urothelial
EUROPEAN UROLOGY 63 (2013) 81 87 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review Bladder Cancer ICUD-EAU International Consultation on Bladder Cancer 2012: Urothelial
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Beware the BCG Failures: A Review of One Institution's Results
 European Urology European Urology 42 (2002) 542±546 Beware the BCG Failures: A Review of One Institution's Results C. Richard W. Lockyer a,*, James E.C. Sedgwick b, David A. Gillatt a a Bristol Urological
European Urology European Urology 42 (2002) 542±546 Beware the BCG Failures: A Review of One Institution's Results C. Richard W. Lockyer a,*, James E.C. Sedgwick b, David A. Gillatt a a Bristol Urological
Multiple factor analysis of metachronous upper urinary tract transitional cell carcinoma after radical cystectomy
 Brazilian Journal of Medical and Biological Research (2007) 40: 979-984 Predictive factors after radical cystectomy ISSN 0100-879X 979 Multiple factor analysis of metachronous upper urinary tract transitional
Brazilian Journal of Medical and Biological Research (2007) 40: 979-984 Predictive factors after radical cystectomy ISSN 0100-879X 979 Multiple factor analysis of metachronous upper urinary tract transitional
Radical Cystectomy Often Too Late? Yes, But...
 european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
european urology 50 (2006) 1129 1138 available at www.sciencedirect.com journal homepage: www.europeanurology.com Editorial 50th Anniversary Radical Cystectomy Often Too Late? Yes, But... Urs E. Studer
Clinical Study of G3 Superficial Bladder Cancer without Concomitant CIS Treated with Conservative Therapy
 Jpn J Clin Oncol 2002;32(11)461 465 Clinical Study of G3 Superficial Bladder Cancer without Concomitant CIS Treated with Conservative Therapy Takashi Saika, Tomoyasu Tsushima, Yasutomo Nasu, Ryoji Arata,
Jpn J Clin Oncol 2002;32(11)461 465 Clinical Study of G3 Superficial Bladder Cancer without Concomitant CIS Treated with Conservative Therapy Takashi Saika, Tomoyasu Tsushima, Yasutomo Nasu, Ryoji Arata,
Maintenance Therapy with Intravesical Bacillus Calmette Guérin in Patients with Intermediate- or High-risk Non-muscle-invasive
 Jpn J Clin Oncol 2013;43(3)305 313 doi:10.1093/jjco/hys225 Advance Access Publication 9 January 2013 Maintenance Therapy with Intravesical Bacillus Calmette Guérin in Patients with Intermediate- or High-risk
Jpn J Clin Oncol 2013;43(3)305 313 doi:10.1093/jjco/hys225 Advance Access Publication 9 January 2013 Maintenance Therapy with Intravesical Bacillus Calmette Guérin in Patients with Intermediate- or High-risk
THE USE OF HALF DOSE BCG FOR INTRAVESICAL IMMUNOTHERAPY IN NON MUSCLE INVASIVE BLADDER CANCER
 THE USE OF HALF DOSE BCG FOR INTRAVESICAL IMMUNOTHERAPY IN NON MUSCLE INVASIVE BLADDER CANCER Mihály Zoltán Attila 1, Rusu Cristian Bogdan 2, Mihály Orsolya Maria 3, Bolboacă Sorana Daniela 4, Bungărdean
THE USE OF HALF DOSE BCG FOR INTRAVESICAL IMMUNOTHERAPY IN NON MUSCLE INVASIVE BLADDER CANCER Mihály Zoltán Attila 1, Rusu Cristian Bogdan 2, Mihály Orsolya Maria 3, Bolboacă Sorana Daniela 4, Bungărdean
The Clinical Impact of the Classification of Carcinoma In Situ on Tumor Recurrence and their Clinical Course in Patients with Bladder Tumor
 Original Article Japanese Journal of Clinical Oncology Advance Access published December 17, 2010 Jpn J Clin Oncol 2010 doi:10.1093/jjco/hyq228 The Clinical Impact of the Classification of Carcinoma In
Original Article Japanese Journal of Clinical Oncology Advance Access published December 17, 2010 Jpn J Clin Oncol 2010 doi:10.1093/jjco/hyq228 The Clinical Impact of the Classification of Carcinoma In
Non Muscle Invasive Bladder Cancer. Primary and Recurrent TCC 4/10/2010. Two major consequences: Strategies: High-Risk NMI TCC
 Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
Intravesical Therapy 2010-When, with What, When to Stop Friday, April 9, 2010 Ralph de VereWhite, MD Director, UC Davis Cancer Center Associate Dean for Cancer Programs Professor, Department of Urolgoy
TCC recurrence within the upper tract urothelium following
 Upper Tract Urothelial Recurrence Following Radical Cystectomy for Transitional Cell Carcinoma of the Bladder: An Analysis of 1,069 Patients With 10-Year Followup Kristin M. Sanderson,* Jie Cai, Gustavo
Upper Tract Urothelial Recurrence Following Radical Cystectomy for Transitional Cell Carcinoma of the Bladder: An Analysis of 1,069 Patients With 10-Year Followup Kristin M. Sanderson,* Jie Cai, Gustavo
Influence of stage discrepancy on outcome in. in patients treated with radical cystectomy.
 Tumori, 96: 699-703, 2010 Influence of stage discrepancy on outcome in patients treated with radical cystectomy Ja Hyeon Ku 1, Kyung Chul Moon 2, Cheol Kwak 1, and Hyeon Hoe Kim 1 1 Department of Urology,
Tumori, 96: 699-703, 2010 Influence of stage discrepancy on outcome in patients treated with radical cystectomy Ja Hyeon Ku 1, Kyung Chul Moon 2, Cheol Kwak 1, and Hyeon Hoe Kim 1 1 Department of Urology,
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D.
 Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of High Grade, T1 Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Patient Risk Profiles: Prognostic Factors of Recurrence and Progression
 european urology supplements 5 (2006) 648 653 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review Patient Risk Profiles: Prognostic Factors of Recurrence and Progression
european urology supplements 5 (2006) 648 653 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review Patient Risk Profiles: Prognostic Factors of Recurrence and Progression
BJUI. Invasive T1 bladder cancer: indications and rationale for radical cystectomy
 2008 The Authors; Journal compilation 2008 BJU International Mini-review Article INVASIVE T1 BLADDER CANCER: INDICATIONS AND RATIONALE FOR RADICAL CYSTECTOMY STEIN and PENSON BJUI BJU INTERNATIONAL Invasive
2008 The Authors; Journal compilation 2008 BJU International Mini-review Article INVASIVE T1 BLADDER CANCER: INDICATIONS AND RATIONALE FOR RADICAL CYSTECTOMY STEIN and PENSON BJUI BJU INTERNATIONAL Invasive
NMIBC. Piotr Jarzemski. Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland
 NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
NMIBC Piotr Jarzemski Department of Urology Jan Biziel University Hospital Bydgoszcz, Poland 71 year old male patient was admitted to the Department of Urology First TURBT - 2 months prior to the hospitalisation.
Management of Superficial Bladder Cancer Douglas S. Scherr, M.D.
 Management of Superficial Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Management of Superficial Bladder Cancer Douglas S. Scherr, M.D. Assistant Professor of Urology Clinical Director, Urologic Oncology Weill Medical College-Cornell University Estimated new cancer cases.
Issues in the Management of High Risk Superficial Bladder Cancer
 Issues in the Management of High Risk Superficial Bladder Cancer MICHAEL A.S. JEWETT DIVISION OF UROLOGY, DEPARTMENT OF SURGICAL ONCOLOGY, PRINCESS MARGARET HOSPITAL & THE UNIVERSITY OF TORONTO 1 Carcinoma
Issues in the Management of High Risk Superficial Bladder Cancer MICHAEL A.S. JEWETT DIVISION OF UROLOGY, DEPARTMENT OF SURGICAL ONCOLOGY, PRINCESS MARGARET HOSPITAL & THE UNIVERSITY OF TORONTO 1 Carcinoma
Clinical significance of immediate urine cytology after transurethral resection of bladder tumor in patients with non-muscle invasive bladder cancer
 International Journal of Urology (2011) 18, 439 443 doi: 10.1111/j.1442-2042.2011.02766.x Original Article: Clinical Investigationiju_2766 439..443 Clinical significance of immediate urine cytology after
International Journal of Urology (2011) 18, 439 443 doi: 10.1111/j.1442-2042.2011.02766.x Original Article: Clinical Investigationiju_2766 439..443 Clinical significance of immediate urine cytology after
models; Kaplan meier curves were also extrapolated for each cohort to compare disease specific and overall survival patterns.
 ; 21 Urological Oncology MUSCULARIS PROPRIA AND UPSTAGING OF ct1 BLADDER CANCER BADALATO ET AL. BJUI Does the presence of muscularis propria on transurethral resection of bladder tumour specimens affect
; 21 Urological Oncology MUSCULARIS PROPRIA AND UPSTAGING OF ct1 BLADDER CANCER BADALATO ET AL. BJUI Does the presence of muscularis propria on transurethral resection of bladder tumour specimens affect
Effectiveness of A Single Immediate Mitomycin C Instillation in Patients with Low Risk Superficial Bladder Cancer: Short and Long-Term Follow-up
 Journal of the Egyptian Nat. Cancer Inst., Vol. 19, No. 2, June: 121-126, 2007 in Patients with Low Risk Superficial Bladder Cancer: Short and Long-Term Follow-up SAMIR EL-GHOBASHY, M.D.; TAREK R. EL-LEITHY,
Journal of the Egyptian Nat. Cancer Inst., Vol. 19, No. 2, June: 121-126, 2007 in Patients with Low Risk Superficial Bladder Cancer: Short and Long-Term Follow-up SAMIR EL-GHOBASHY, M.D.; TAREK R. EL-LEITHY,
Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016
 BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
BLADDER CANCER Joseph H. Williams, MD Idaho Urologic Institute St. Alphonsus Regional Medical Center September 22, 2016 BLADDER CANCER = UROTHELIAL CANCER Antiquated term is Transitional Cell Carcinoma
Role of Re-Resection in Non Muscle-Invasive Bladder Cancer
 Review Special Issue: Bladder Cancer TheScientificWorldJOURNAL (2011) 11, 283 288 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2011.29 Role of Re-Resection in Non Muscle-Invasive Bladder Cancer Harry W.
Review Special Issue: Bladder Cancer TheScientificWorldJOURNAL (2011) 11, 283 288 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2011.29 Role of Re-Resection in Non Muscle-Invasive Bladder Cancer Harry W.
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
The value of EORTC risk tables in evaluating recurrent non muscle invasive bladder cancer in everyday practice
 48 Original Paper UROLOGICAL ONCOLOGY The value of EORTC risk tables in evaluating recurrent non muscle invasive bladder cancer in everyday practice Rafał Walczak, Krzysztof Bar 2, Janusz Walczak Department
48 Original Paper UROLOGICAL ONCOLOGY The value of EORTC risk tables in evaluating recurrent non muscle invasive bladder cancer in everyday practice Rafał Walczak, Krzysztof Bar 2, Janusz Walczak Department
Management of High-Risk Non-Muscle Invasive Bladder Cancer. Seth P. Lerner, MD, FACS
 Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
Management of High-Risk Non-Muscle Invasive Bladder Cancer Seth P. Lerner, MD, FACS Professor of Urology, Beth and Dave Swalm Chair in Urologic Oncology, Scott Department of Urology, Baylor College of
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
 A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
A Personal History NIH CWRU U of TN U of Miami Animal Model for Bladder Cancer Carcinogen induced FANFT Three Models Primary tumors individual tumors, simulates clinical scenario of locally advanced cancer
Controversies in the management of Non-muscle invasive bladder cancer
 Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Controversies in the management of Non-muscle invasive bladder cancer Sia Daneshmand, MD Associate Professor of Urology (Clinical Scholar) Director of Urologic Oncology Director of Clinical Research Urologic
Radiochemotherapy after Transurethral Resection is an Effective Treatment Method in T1G3 Bladder Cancer
 Radiochemotherapy after Transurethral Resection is an Effective Treatment Method in T1G3 Bladder Cancer Z. AKÇETIN 1, J. TODOROV 1, E. TÜZEL 1, D.G. ENGEHAUSEN 1, F.S. KRAUSE 1, R. SAUER 2, K.M. SCHROTT
Radiochemotherapy after Transurethral Resection is an Effective Treatment Method in T1G3 Bladder Cancer Z. AKÇETIN 1, J. TODOROV 1, E. TÜZEL 1, D.G. ENGEHAUSEN 1, F.S. KRAUSE 1, R. SAUER 2, K.M. SCHROTT
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
EAU GUIDELINES ON NON-MUSCLE INVASIVE (TaT1, CIS) BLADDER CANCER
 BLADDER CANCER") EU GUIDELINES ON NON-MUSLE INVSIVE (TaT1, IS) LDDER NER (Limited text update March 2017) M. abjuk (hair), M. urger (Vice-hair), E. ompérat, P. Gontero,.H. Mostafid, J. Palou,.W.G. van Rhijn, M. Rouprêt,
EU GUIDELINES ON NON-MUSLE INVSIVE (TaT1, IS) LDDER NER (Limited text update March 2017) M. abjuk (hair), M. urger (Vice-hair), E. ompérat, P. Gontero,.H. Mostafid, J. Palou,.W.G. van Rhijn, M. Rouprêt,
Haijun Zhou, Jae Y Ro, Luan D Truong, Alberto G Ayala, Steven S Shen
 Am J Clin Exp Urol 2014;2(2):156-160 www.ajceu.us /ISSN:2330-1910/AJCEU0000048 Original Article Intraoperative frozen section evaluation of ureteral and urethral margins: studies of 203 consecutive radical
Am J Clin Exp Urol 2014;2(2):156-160 www.ajceu.us /ISSN:2330-1910/AJCEU0000048 Original Article Intraoperative frozen section evaluation of ureteral and urethral margins: studies of 203 consecutive radical
Urological Oncology INTRODUCTION. M Hammad Ather, Masooma Zaidi
 Urological Oncology Predicting Recurrence and Progression in Non-Muscle- Invasive Bladder Cancer Using European Organization of Research and Treatment of Cancer Risk Tables M Hammad Ather, Masooma Zaidi
Urological Oncology Predicting Recurrence and Progression in Non-Muscle- Invasive Bladder Cancer Using European Organization of Research and Treatment of Cancer Risk Tables M Hammad Ather, Masooma Zaidi
Renal Pelvis Squamous Cell Carcinoma and Renal Cell Carcinoma in a Tuberculous Kidney
 Case Study TheScientificWorldJOURNAL (2004) 4, 965 968 ISSN 1537-744X; DOI 10.1100/tsw.2004.196 Renal Pelvis Squamous Cell Carcinoma and Renal Cell Carcinoma in a Tuberculous Kidney M. Al-Assiri 1, M.F.
Case Study TheScientificWorldJOURNAL (2004) 4, 965 968 ISSN 1537-744X; DOI 10.1100/tsw.2004.196 Renal Pelvis Squamous Cell Carcinoma and Renal Cell Carcinoma in a Tuberculous Kidney M. Al-Assiri 1, M.F.
Partial Cystectomy for Invasive Bladder Cancer
 European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
European Urology Supplements European Urology Supplements 4 (2005) 67 71 Partial Cystectomy for Invasive Bladder Cancer Gerald H. Mickisch* Center of Operative Urology Bremen, Academic Hospital Bremen
The Impact of Blue Light Cystoscopy with Hexaminolevulinate (HAL) on Progression of Bladder Cancer ANewAnalysis
 on Progression of Bladder Cancer ANewAnalysis") Bladder Cancer 2 (2016) 273 278 DOI 10.3233/BLC-160048 IOS Press Research Report 273 The Impact of Blue Light Cystoscopy with Hexaminolevulinate (HAL) on Progression of Bladder Cancer ANewAnalysis Ashish
Bladder Cancer 2 (2016) 273 278 DOI 10.3233/BLC-160048 IOS Press Research Report 273 The Impact of Blue Light Cystoscopy with Hexaminolevulinate (HAL) on Progression of Bladder Cancer ANewAnalysis Ashish
Citation International journal of urology (2. Right which has been published in final f
 Title Novel constant-pressure irrigation of renal pelvic tumors after ipsila Nakamura, Kenji; Terada, Naoki; Sug Author(s) Toshinori; Matsui, Yoshiyuki; Imamu Kazutoshi; Kamba, Tomomi; Yoshimura Citation
Title Novel constant-pressure irrigation of renal pelvic tumors after ipsila Nakamura, Kenji; Terada, Naoki; Sug Author(s) Toshinori; Matsui, Yoshiyuki; Imamu Kazutoshi; Kamba, Tomomi; Yoshimura Citation
Reviewing Immunotherapy for Bladder Carcinoma In Situ
 Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Reviewing Immunotherapy for Bladder Carcinoma In Situ Samir Bidnur Dept of Urologic Sciences, Grand Rounds March 1 st, 2017 Checkpoint Inhibition and Bladder Cancer, an evolving story with immunotherapy
Guidelines on Non-muscle invasive Bladder Cancer (TaT1 and CIS)
") Guidelines on Non-muscle invasive Bladder Cancer (TaT1 and CIS) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt European Association of Urology 2011 TABLE OF CONTENTS
Guidelines on Non-muscle invasive Bladder Cancer (TaT1 and CIS) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt European Association of Urology 2011 TABLE OF CONTENTS
Efficacy and Safety of Bacille Calmette-Guérin Immunotherapy in Superficial Bladder Cancer
 S86 Efficacy and Safety of Bacille Calmette-Guérin Immunotherapy in Superficial Bladder Cancer Donald L. Lamm Department of Urology, West Virginia University, Morgantown In the United States, bladder cancer
S86 Efficacy and Safety of Bacille Calmette-Guérin Immunotherapy in Superficial Bladder Cancer Donald L. Lamm Department of Urology, West Virginia University, Morgantown In the United States, bladder cancer
SUPERFICIAL BLADDER CANCER MANAGEMENT
 A CME Webcast/TELECONFERENCE Case by Case: CRITICAL ISSUES IN SUPERFICIAL BLADDER CANCER MANAGEMENT An Interactive Case Format with Instant Audience Polling APRIL-MAY 2005 CME Program Slide Book Sponsored
A CME Webcast/TELECONFERENCE Case by Case: CRITICAL ISSUES IN SUPERFICIAL BLADDER CANCER MANAGEMENT An Interactive Case Format with Instant Audience Polling APRIL-MAY 2005 CME Program Slide Book Sponsored
The Effects of Intravesical Chemoimmunotherapy with Gemcitabine and Bacillus Calmette Guérin in Superficial Bladder Cancer: a Preliminary Study
 The Journal of International Medical Research 2009; 37: 1823 1830 The Effects of Intravesical Chemoimmunotherapy with Gemcitabine and Bacillus Calmette Guérin in Superficial Bladder Cancer: a Preliminary
The Journal of International Medical Research 2009; 37: 1823 1830 The Effects of Intravesical Chemoimmunotherapy with Gemcitabine and Bacillus Calmette Guérin in Superficial Bladder Cancer: a Preliminary
Bladder Cancer Guidelines
 Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
Bladder Cancer Guidelines Agreed by Urology CSG: October 2011 Review Date: September 2013 Bladder Cancer 1. Referral Guidelines The following patients should be considered as potentially having bladder
INTRAVESICAL THERAPY AND FOLLOW-UP OF SUPERFICIAL TRANSITIONAL CELL CARCINOMA OF THE BLADDER
 Clinical Urology Brazilian Journal of Urology Official Journal of the Brazilian Society of Urology Vol. 26 (3): 242-249, May - June, 2000 INTRAVESICAL THERAPY AND FOLLOW-UP OF SUPERFICIAL TRANSITIONAL
Clinical Urology Brazilian Journal of Urology Official Journal of the Brazilian Society of Urology Vol. 26 (3): 242-249, May - June, 2000 INTRAVESICAL THERAPY AND FOLLOW-UP OF SUPERFICIAL TRANSITIONAL
Prognosis of Muscle-Invasive Bladder Cancer: Difference between Primary and ProgressiveTumours and Implications fortherapy
 European Urology European Urology 45 (2004) 292 296 Prognosis of Muscle-Invasive Bladder Cancer: Difference between Primary and ProgressiveTumours and Implications fortherapy Barthold Ph. Schrier a, Maarten
European Urology European Urology 45 (2004) 292 296 Prognosis of Muscle-Invasive Bladder Cancer: Difference between Primary and ProgressiveTumours and Implications fortherapy Barthold Ph. Schrier a, Maarten
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Urological Oncology. Dae Hyeon Kwon, Phil Hyun Song, Hyun Tae Kim.
 www.kjurology.org http://dx.doi.org/10.4111/kju.2012.53.7.457 Urological Oncology Multivariate Analysis of the Prognostic Significance of Resection Weight after Transurethral Resection of Bladder Tumor
www.kjurology.org http://dx.doi.org/10.4111/kju.2012.53.7.457 Urological Oncology Multivariate Analysis of the Prognostic Significance of Resection Weight after Transurethral Resection of Bladder Tumor
 Case Presentation 58 year old male with recent history of hematuria, for which he underwent cystoscopy. A 1.5 cm papillary tumor was found in the left lateral wall of the bladder. Pictures of case Case
Case Presentation 58 year old male with recent history of hematuria, for which he underwent cystoscopy. A 1.5 cm papillary tumor was found in the left lateral wall of the bladder. Pictures of case Case
BLADDER CANCER: PATIENT INFORMATION
 BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
BLADDER CANCER: PATIENT INFORMATION The bladder is the balloon like organ located in the pelvis that stores and empties urine. Urine is produced by the kidneys, is conducted to the bladder by the ureters,
Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer Center Contemporary Experience
 International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
International Scholarly Research Notices, Article ID 702653, 6 pages http://dx.doi.org/10.1155/2014/702653 Research Article Partial Cystectomy after Neoadjuvant Chemotherapy: Memorial Sloan Kettering Cancer
The Predictors of Local Recurrence after Radical Cystectomy in Patients with Invasive Bladder Cancer
 The Predictors of Local Recurrence after Radical Cystectomy in Patients with Invasive Bladder Cancer Hiroki Ide, Eiji Kikuchi, Akira Miyajima, Ken Nakagawa, Takashi Ohigashi, Jun Nakashima and Mototsugu
The Predictors of Local Recurrence after Radical Cystectomy in Patients with Invasive Bladder Cancer Hiroki Ide, Eiji Kikuchi, Akira Miyajima, Ken Nakagawa, Takashi Ohigashi, Jun Nakashima and Mototsugu
Neo-adjuvant chemotherapy and bladder preservation in locally advanced transitional cell carcinoma of the bladder
 Annals of Oncology : -5. 999. 999 Klimer Academic Publishers. Printed in the Netherlands. Original article Neo-adjuvant chemotherapy and bladder preservation in locally advanced transitional cell carcinoma
Annals of Oncology : -5. 999. 999 Klimer Academic Publishers. Printed in the Netherlands. Original article Neo-adjuvant chemotherapy and bladder preservation in locally advanced transitional cell carcinoma
Kyung Won Seo, Byung Hoon Kim, Choal Hee Park, Chun Il Kim, Hyuk Soo Chang
 www.kjurology.org DOI:.4/kju..5..65 Urological Oncology The Efficacy of the EORTC Scoring System and Risk Tables for the Prediction of Recurrence and Progression of Non-Muscle-Invasive Bladder Cancer after
www.kjurology.org DOI:.4/kju..5..65 Urological Oncology The Efficacy of the EORTC Scoring System and Risk Tables for the Prediction of Recurrence and Progression of Non-Muscle-Invasive Bladder Cancer after
Management of Difficult Cases of Non-Muscle Invasive Bladder Cancer
 Management of Difficult Cases of Non-Muscle Invasive Bladder Cancer 1 Bladder Cancer Recurrence is common Progression is uncommon Progression is more important than recurrence There are indicators of recurrence
Management of Difficult Cases of Non-Muscle Invasive Bladder Cancer 1 Bladder Cancer Recurrence is common Progression is uncommon Progression is more important than recurrence There are indicators of recurrence
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of electrically-stimulated intravesical chemotherapy for superficial bladder
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of electrically-stimulated intravesical chemotherapy for superficial bladder
Mixed low and high grade non muscle invasive bladder cancer: a histological subtype with favorable outcome
 DOI 10.1007/s00345-014-1383-5 Original Article Mixed low and high grade non muscle invasive bladder cancer: a histological subtype with favorable outcome Tina Schubert Matthew R. Danzig Srinath Kotamarti
DOI 10.1007/s00345-014-1383-5 Original Article Mixed low and high grade non muscle invasive bladder cancer: a histological subtype with favorable outcome Tina Schubert Matthew R. Danzig Srinath Kotamarti
BJUI. The value of bladder mapping and prostatic urethra biopsies for detection of carcinoma in situ (CIS)
") BJUI BJU INTERNATIONAL The value of bladder mapping and prostatic urethra biopsies for detection of carcinoma in situ (CIS) Sigurdur Gudj ó nsson *, Mats Bl ä ckberg, Gunilla Chebil, Staffan Jahnson, Hans
BJUI BJU INTERNATIONAL The value of bladder mapping and prostatic urethra biopsies for detection of carcinoma in situ (CIS) Sigurdur Gudj ó nsson *, Mats Bl ä ckberg, Gunilla Chebil, Staffan Jahnson, Hans
Clinical Study Ureteroscopic Laser Treatment of Upper Urinary Tract Urothelial Cell Carcinomas: Can a Tumour Free Status Be Achieved?
 Advances in Urology Volume 2013, Article ID 429585, 4 pages http://dx.doi.org/10.1155/2013/429585 Clinical Study Ureteroscopic Laser Treatment of Upper Urinary Tract Urothelial Cell Carcinomas: Can a Tumour
Advances in Urology Volume 2013, Article ID 429585, 4 pages http://dx.doi.org/10.1155/2013/429585 Clinical Study Ureteroscopic Laser Treatment of Upper Urinary Tract Urothelial Cell Carcinomas: Can a Tumour
Contents of Online Supporting Information. etable 1. Study characteristics for trials of intravesical therapy vs. TURBT alone
 Contents of Online Supporting Information etable 1. Study characteristics for trials of intravesical therapy vs. TURBT alone etable 2. Study characteristics of head to head trials of intravesical therapy
Contents of Online Supporting Information etable 1. Study characteristics for trials of intravesical therapy vs. TURBT alone etable 2. Study characteristics of head to head trials of intravesical therapy
Intravesical gemcitabine in combination with mitomycin C as salvage treatment in recurrent non-muscle-invasive bladder cancer
 Intravesical gemcitabine in combination with mitomycin C as salvage treatment in recurrent non-muscle-invasive bladder cancer Patrick A. Cockerill, John J. Knoedler, Igor Frank, Robert Tarrell and Robert
Intravesical gemcitabine in combination with mitomycin C as salvage treatment in recurrent non-muscle-invasive bladder cancer Patrick A. Cockerill, John J. Knoedler, Igor Frank, Robert Tarrell and Robert
Transitional Cell Carcinoma of the Upper Ureter Metastatic to the Thoracic Spine Presenting as a Spinal Cord Compression
 Case Study TheScientificWorldJOURNAL (2008) 8, 223 227 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2008.43 Transitional Cell Carcinoma of the Upper Ureter Metastatic to the Thoracic Spine Presenting as
Case Study TheScientificWorldJOURNAL (2008) 8, 223 227 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2008.43 Transitional Cell Carcinoma of the Upper Ureter Metastatic to the Thoracic Spine Presenting as
PDF hosted at the Radboud Repository of the Radboud University Nijmegen
 PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/21069
PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/21069
Protocol for BCG + maintenance, Donald L. Lamm, MD Last Updated Friday, 14 November 2008
 Protocol for BCG + maintenance, Donald L. Lamm, MD Last Updated Friday, 14 November 2008 {niftybox width=180px,float=right,textalign=left} update on the protocol: from Dr. Lamm's site: It is also true
Protocol for BCG + maintenance, Donald L. Lamm, MD Last Updated Friday, 14 November 2008 {niftybox width=180px,float=right,textalign=left} update on the protocol: from Dr. Lamm's site: It is also true
TREATMENT OF PATIENTS WITH SUPERFICIAL BLADDER CANCER STRATIFIED BY RISK GROUPS TREATED WITH LYOPHILIZED MOREAU-RIO DE JANEIRO BCG STRAIN
 Clinical Urology International Braz J Urol Official Journal of the Brazilian Society of Urology Vol. 28 (5): 426-436, September - October, 2002 TREATMENT OF PATIENTS WITH SUPERFICIAL BLADDER CANCER STRATIFIED
Clinical Urology International Braz J Urol Official Journal of the Brazilian Society of Urology Vol. 28 (5): 426-436, September - October, 2002 TREATMENT OF PATIENTS WITH SUPERFICIAL BLADDER CANCER STRATIFIED
Incidence and predictors of understaging in patients with clinical T1 urothelial carcinoma undergoing radical cystectomy
 Incidence and predictors of understaging in patients with clinical T1 urothelial carcinoma undergoing radical cystectomy Jacob T. Ark*, Kirk A. Keegan*, Daniel A. Barocas*, Todd M. Morgan*, Matthew J.
Incidence and predictors of understaging in patients with clinical T1 urothelial carcinoma undergoing radical cystectomy Jacob T. Ark*, Kirk A. Keegan*, Daniel A. Barocas*, Todd M. Morgan*, Matthew J.
The Prognostic Importance of Prostate-Specific Antigen in Monitoring Patients Undergoing Maximum Androgen Blockage for Metastatic Prostate Cancer
 Research Article TheScientificWorldJOURNAL (005) 5, 8 4 ISSN 57-744X; DOI 0.00/tsw.005.9 The Prognostic Importance of Prostate-Specific Antigen in Monitoring Patients Undergoing Maximum Androgen Blockage
Research Article TheScientificWorldJOURNAL (005) 5, 8 4 ISSN 57-744X; DOI 0.00/tsw.005.9 The Prognostic Importance of Prostate-Specific Antigen in Monitoring Patients Undergoing Maximum Androgen Blockage
Long term follow-up in patients with initially diagnosed low grade Ta non-muscle invasive bladder tumors: tumor recurrence and worsening progression
 Kobayashi et al. BMC Urology 2014, 14:5 RESEARCH ARTICLE Open Access Long term follow-up in patients with initially diagnosed low grade Ta non-muscle invasive bladder tumors: tumor recurrence and worsening
Kobayashi et al. BMC Urology 2014, 14:5 RESEARCH ARTICLE Open Access Long term follow-up in patients with initially diagnosed low grade Ta non-muscle invasive bladder tumors: tumor recurrence and worsening
T1HG Bladder Cancer What is the Best Therapy?
 T1HG Bladder Cancer What is the Best Therapy? Ashish M. Kamat, MD, MBBS, FACS Professor of Urology Director, Urologic Oncology Fellowship Guidelines for T1HG Bladder Cancer AUA Recommendation: BCG induction
T1HG Bladder Cancer What is the Best Therapy? Ashish M. Kamat, MD, MBBS, FACS Professor of Urology Director, Urologic Oncology Fellowship Guidelines for T1HG Bladder Cancer AUA Recommendation: BCG induction
The pathology of bladder cancer
 1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
The Efficacy of Adjuvant Chemotherapy for Locally Advanced Upper Tract Urothelial Cell Carcinoma
 Ivyspring International Publisher Research Paper 686 Journal of Cancer 2013; 4(8): 686-690. doi: 10.7150/jca.7326 The Efficacy of Adjuvant Chemotherapy for Locally Advanced Upper Tract Urothelial Cell
Ivyspring International Publisher Research Paper 686 Journal of Cancer 2013; 4(8): 686-690. doi: 10.7150/jca.7326 The Efficacy of Adjuvant Chemotherapy for Locally Advanced Upper Tract Urothelial Cell
The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
 30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach
 Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Non-Muscle-Invasive Bladder Cancer Last Updated Friday, 14 November 2008
 Non-Muscle-Invasive Bladder Cancer Last Updated Friday, 14 November 2008 Bladder Cancer WebCafé {niftybox width=180px,float=right,textalign=left} Online article, 2007, discussing the controversies of treating
Non-Muscle-Invasive Bladder Cancer Last Updated Friday, 14 November 2008 Bladder Cancer WebCafé {niftybox width=180px,float=right,textalign=left} Online article, 2007, discussing the controversies of treating
Metachronous anterior urethral metastasis of prostatic ductal adenocarcinoma
 http://dx.doi.org/10.7180/kmj.2016.31.1.66 KMJ Case Report Metachronous anterior urethral metastasis of prostatic ductal adenocarcinoma Jeong Hyun Oh 1, Taek Sang Kim 1, Hyun Yul Rhew 1, Bong Kwon Chun
http://dx.doi.org/10.7180/kmj.2016.31.1.66 KMJ Case Report Metachronous anterior urethral metastasis of prostatic ductal adenocarcinoma Jeong Hyun Oh 1, Taek Sang Kim 1, Hyun Yul Rhew 1, Bong Kwon Chun
UC San Francisco UC San Francisco Previously Published Works
 UC San Francisco UC San Francisco Previously Published Works Title Multi-institutional analysis of sequential intravesical gemcitabine and mitomycin C chemotherapy for non-muscle invasive bladder cancer
UC San Francisco UC San Francisco Previously Published Works Title Multi-institutional analysis of sequential intravesical gemcitabine and mitomycin C chemotherapy for non-muscle invasive bladder cancer
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Bladder Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Intravesical Gemcitabine for High Risk, Nonmuscle Invasive Bladder Cancer after Bacillus Calmette-Guerin Treatment Failure
 Intravesical Gemcitabine for High Risk, Nonmuscle Invasive Bladder Cancer after Bacillus Calmette-Guerin Treatment Failure Itay A. Sternberg, Guido Dalbagni,* Ling Y. Chen, Sherri M. Donat, Bernard H.
Intravesical Gemcitabine for High Risk, Nonmuscle Invasive Bladder Cancer after Bacillus Calmette-Guerin Treatment Failure Itay A. Sternberg, Guido Dalbagni,* Ling Y. Chen, Sherri M. Donat, Bernard H.
Cystoscopy in children presenting with hematuria should not be overlooked
 Ped Urol Case Rep 2015; 2(3):7-11 DOI: 10.14534/PUCR.2015310303 PUCR Ped Urol Case Rep PEDIATRIC UROLOGY CASE REPORTS ISSN: 2148 2969 Journal homepage: http://www.pediatricurologycasereports.com Cystoscopy
Ped Urol Case Rep 2015; 2(3):7-11 DOI: 10.14534/PUCR.2015310303 PUCR Ped Urol Case Rep PEDIATRIC UROLOGY CASE REPORTS ISSN: 2148 2969 Journal homepage: http://www.pediatricurologycasereports.com Cystoscopy
The clinical epidemiology of superficial bladder cancer
 Br. J. Cancer (1993), 67, 86-812 '." Macmillan Press Ltd., 1993 Br. J. Cancer (1993), 67, 86-812 1993 The clinical epidemiology of superficial bladder cancer L.A.L.M. Kiemeneyl2, J.A. Witjes3, A.L.M. Verbeekl2,
Br. J. Cancer (1993), 67, 86-812 '." Macmillan Press Ltd., 1993 Br. J. Cancer (1993), 67, 86-812 1993 The clinical epidemiology of superficial bladder cancer L.A.L.M. Kiemeneyl2, J.A. Witjes3, A.L.M. Verbeekl2,
CUA guidelines on the management of non-muscle invasive bladder cancer
 Original cua guidelines research CUA guidelines on the management of non-muscle invasive bladder cancer Wassim Kassouf, MD, CM, FRCSC; * Samer L. Traboulsi, MD; * Girish S. Kulkarni, MD, FRCSC; Rodney
Original cua guidelines research CUA guidelines on the management of non-muscle invasive bladder cancer Wassim Kassouf, MD, CM, FRCSC; * Samer L. Traboulsi, MD; * Girish S. Kulkarni, MD, FRCSC; Rodney
Incidental Prostate Cancer in Patients with Bladder Urothelial Carcinoma: Comprehensive Analysis of 1,476 Radical Cystoprostatectomy Specimens
 Incidental Prostate Cancer in Patients with Bladder Urothelial Carcinoma: Comprehensive Analysis of 1,476 Radical Cystoprostatectomy Specimens Harman Maxim Bruins,* Hooman Djaladat,* Hamed Ahmadi, Andy
Incidental Prostate Cancer in Patients with Bladder Urothelial Carcinoma: Comprehensive Analysis of 1,476 Radical Cystoprostatectomy Specimens Harman Maxim Bruins,* Hooman Djaladat,* Hamed Ahmadi, Andy
Pharmacologyonline 3: (2006)
") INTRAVESICAL MISTLETOE EXTRACT FOR ADJUVANT TREATMENT OF SUPERFICIAL URINARY BLADDER CANCER P. Bühler 1, C. Leiber 1, M. Lucht 2, P. Wolf 1, U. Wetterauer 1, U. Elsässer-Beile 1 1 Department of Urology,
INTRAVESICAL MISTLETOE EXTRACT FOR ADJUVANT TREATMENT OF SUPERFICIAL URINARY BLADDER CANCER P. Bühler 1, C. Leiber 1, M. Lucht 2, P. Wolf 1, U. Wetterauer 1, U. Elsässer-Beile 1 1 Department of Urology,
Urethral recurrence after cystectomy: current preventative measures, diagnosis and management
 Urethral recurrence after cystectomy: current preventative measures, diagnosis and management Yvonne Chan*, Patrick Fisher*, Derya Tilki* and Christopher P.Evans* *Department of Urology, Medical Center,
Urethral recurrence after cystectomy: current preventative measures, diagnosis and management Yvonne Chan*, Patrick Fisher*, Derya Tilki* and Christopher P.Evans* *Department of Urology, Medical Center,
european urology 52 (2007)
") european urology 52 (2007) 1123 1130 available at www.sciencedirect.com journal homepage: www.europeanurology.com Urothelial Cancer Long-Term Intravesical Adjuvant Chemotherapy Further Reduces Recurrence
european urology 52 (2007) 1123 1130 available at www.sciencedirect.com journal homepage: www.europeanurology.com Urothelial Cancer Long-Term Intravesical Adjuvant Chemotherapy Further Reduces Recurrence
Bladder-Sparing Treatment of Invasive Bladder Cancer
 Several alternatives to radical cystectomy for muscle-invasive bladder cancer have been studied. None, however, are reliably superior to operative treatment. Sidi Bou Said,Tunisia, 1999. Courtesy of J.
Several alternatives to radical cystectomy for muscle-invasive bladder cancer have been studied. None, however, are reliably superior to operative treatment. Sidi Bou Said,Tunisia, 1999. Courtesy of J.
Organ-sparing treatment of invasive transitional cell bladder carcinoma
 Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
Journal of BUON 7: 241-245, 2002 2002 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Organ-sparing treatment of invasive transitional cell bladder carcinoma C. Damyanov, B. Tsingilev,
The Role of Bacillus Calmette-Guérin in the Treatment of Non Muscle-Invasive Bladder Cancer
 EUROPEAN UROLOGY 57 (2010) 410 429 available at www.sciencedirect.com journal homepage: www.europeanurology.com Collaborative Review Bladder Cancer The Role of Bacillus Calmette-Guérin in the Treatment
EUROPEAN UROLOGY 57 (2010) 410 429 available at www.sciencedirect.com journal homepage: www.europeanurology.com Collaborative Review Bladder Cancer The Role of Bacillus Calmette-Guérin in the Treatment
Bilateral Segmental Testicular Infarction
 Case Study TheScientificWorldJOURNAL (2007) 7, 779 783 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2007.146 Bilateral Segmental Testicular Infarction Aaron Bayne 1, Brad Koslin 2, and Siamak Daneshmand
Case Study TheScientificWorldJOURNAL (2007) 7, 779 783 TSW Urology ISSN 1537-744X; DOI 10.1100/tsw.2007.146 Bilateral Segmental Testicular Infarction Aaron Bayne 1, Brad Koslin 2, and Siamak Daneshmand
Disease Speci c Survival as Endpoint of Outcome for Bladder Cancer Patients Following Radical Cystectomy
 European Urology European Urology 41 2002) 440±448 Disease Speci c Survival as Endpoint of Outcome for Bladder Cancer Patients Following Radical Cystectomy JuÈrgen E. Gschwend a,b,*, Philipp Dahm c, WilliamR.
European Urology European Urology 41 2002) 440±448 Disease Speci c Survival as Endpoint of Outcome for Bladder Cancer Patients Following Radical Cystectomy JuÈrgen E. Gschwend a,b,*, Philipp Dahm c, WilliamR.
Case by Case: Critical Issues in Superficial Bladder Cancer Management 5/24/05 13:46 1
 Case by Case: Critical Issues in Superficial Bladder Cancer Management 5/24/05 13:46 1 Case Study 1 A 22-year-old man with a history of gross total painless hematuria: two times in two months, both after
Case by Case: Critical Issues in Superficial Bladder Cancer Management 5/24/05 13:46 1 Case Study 1 A 22-year-old man with a history of gross total painless hematuria: two times in two months, both after
Improving Patient Outcomes: Optimal BCG Treatment Regimen to Prevent Progression in Superficial Bladder Cancer
 european urology supplements 5 (2006) 654 659 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review Improving Patient Outcomes: Optimal BCG Treatment Regimen to Prevent Progression
european urology supplements 5 (2006) 654 659 available at www.sciencedirect.com journal homepage: www.europeanurology.com Review Improving Patient Outcomes: Optimal BCG Treatment Regimen to Prevent Progression
Clinical significance of random bladder biopsy in primary T1 bladder cancer
 MOLECULAR AND CLINICAL ONCOLOGY 8: 665-670, 2018 Clinical significance of random bladder biopsy in primary T1 bladder cancer MASAFUMI OTSUKA 1, SATORU TAGUCHI 1, TOHRU NAKAGAWA 1, TEPPEI MORIKAWA 2, SHIGEKATSU
MOLECULAR AND CLINICAL ONCOLOGY 8: 665-670, 2018 Clinical significance of random bladder biopsy in primary T1 bladder cancer MASAFUMI OTSUKA 1, SATORU TAGUCHI 1, TOHRU NAKAGAWA 1, TEPPEI MORIKAWA 2, SHIGEKATSU
/05/ /0 Vol. 174, 86 92, July 2005 THE JOURNAL OF UROLOGY. Printed in U.S.A. Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION
 0022-5347/05/1741-0086/0 Vol. 174, 86 92, July 2005 THE JOURNAL OF UROLOGY Printed in U.S.A. Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000162059.64886.1c BACILLUS CALMETTE-GUERIN
0022-5347/05/1741-0086/0 Vol. 174, 86 92, July 2005 THE JOURNAL OF UROLOGY Printed in U.S.A. Copyright 2005 by AMERICAN UROLOGICAL ASSOCIATION DOI: 10.1097/01.ju.0000162059.64886.1c BACILLUS CALMETTE-GUERIN
Ivyspring International Publisher. Introduction. Journal of Cancer 2017, Vol. 8. Abstract
 2885 Ivyspring International Publisher Research Paper Journal of Cancer 2017; 8(15): 2885-2891. doi: 10.7150/jca.20003 Papillary Urothelial Neoplasm of Low Malignant Potential (PUNLMP) After Initial TUR-BT:
2885 Ivyspring International Publisher Research Paper Journal of Cancer 2017; 8(15): 2885-2891. doi: 10.7150/jca.20003 Papillary Urothelial Neoplasm of Low Malignant Potential (PUNLMP) After Initial TUR-BT:
Q&A. Fabulous Prizes. Collecting Cancer Data: Bladder, Renal Pelvis, and Ureter 5/2/13. NAACCR Webinar Series
 Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data Bladder & Renal Pelvis NAACCR 2012 2013 Webinar Series Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Original Article APMC-276
 Original Article APMC-276 The Clinical Value of Immediate Second Transurethral Resection in Patients with High Grade Non-Muscle Inasive Bladder Cancer (HG-NMIBC) Syed Saleem Abbas Jafri, Zafar Iqbal Khan
Original Article APMC-276 The Clinical Value of Immediate Second Transurethral Resection in Patients with High Grade Non-Muscle Inasive Bladder Cancer (HG-NMIBC) Syed Saleem Abbas Jafri, Zafar Iqbal Khan
Radical Cystectomy in the Treatment of Bladder Cancer: Oncological Outcome and Survival Predictors
 ORIGINAL ARTICLE Radical Cystectomy in the Treatment of Bladder Cancer: Oncological Outcome and Survival Predictors Chen-Hsun Ho, 1,2 Chao-Yuan Huang, 1 Wei-Chou Lin, 3 Shih-Chieh Chueh, 1 Yeong-Shiau
ORIGINAL ARTICLE Radical Cystectomy in the Treatment of Bladder Cancer: Oncological Outcome and Survival Predictors Chen-Hsun Ho, 1,2 Chao-Yuan Huang, 1 Wei-Chou Lin, 3 Shih-Chieh Chueh, 1 Yeong-Shiau