Pain control in Cancer patients. Dr Ali Shoeibi, Assistant Professor of Neurology
|
|
|
- Shauna Manning
- 5 years ago
- Views:
Transcription


1

2 Pain control in Cancer patients Dr Ali Shoeibi, Assistant Professor of Neurology
3 More than two thirds of patients with advanced cancer experience cancer pain Almost all pain can be controlled to some extent with the wide range of available treatments Pain can be classified in nature as: Nociceptive Somatic Visceral Neuropathic
4 Physiological effects of Pain Increased catabolic demands: poor wound healing, weakness, muscle breakdown Decreased limb movement: increased risk of DVT/PE Respiratory effects: shallow breathing, tachypnea, cough suppression increasing risk of pneumonia and atelectasis Increased sodium and water retention (renal) Decreased gastrointestinal mobility Tachycardia and elevated blood pressure

5 Psychological effects of Pain Negative emotions: anxiety, depression Sleep deprivation Existential suffering

6 Immunological effects of Pain Decrease natural killer cell counts Effects on other lymphocytes not yet defined


7 Key principles of the WHO method of cancer pain relief 1. Cancer pain can, and should, be treated 2. Evaluation and treatment of cancer pain are best achieved by a team approach
8 Key principles of the WHO method of cancer pain relief 3. The first steps are to take a detailed history, and to examine the patient carefully, to determine if the pain is: caused by the cancer, related to the cancer, caused by anticancer treatment, or caused by another disorder; part of a specific syndrome; nociceptive, neuropathic, or mixed nociceptive and neuropathic 4. Treatment begins with an explanation and combines physical and psychological approaches, using both nondrug and drug treatments
9 Key principles of the WHO method of cancer pain relief 5. It is useful to have a sequence of specific aims, such as to: 1. increase the hours of pain-free sleep; 2. relieve the pain when the patient is at rest; 3. relieve pain when the patient is standing or active 6. Drugs alone usually give adequate relief from pain caused by cancer, provided that the right drug is administered in the right dose at the right time intervals 7. By mouth : the oral route is the preferred route for analgesics, including morphine
10 Key principles of the WHO method of cancer pain relief 8. By the clock : for persistent pain, drugs should be taken at regular time intervals and not as needed 9. By the ladder : Unless the patient is in severe pain, begin by prescribing a nonopioid drug and adjust the dose, if necessary, to the maximum recommended dose If or when the nonopioid no longer adequately relieves the pain, an opioid drug should be prescribed in addition to the nonopioid If or when the nonopioid for mild to moderate pain (e.g. codeine) no longer adequately relieves the pain, it should be replaced by an opioid for moderate to severe pain (e.g. morphine)
11 Key principles of the WHO method of cancer pain relief 10. For the individual : the right dose of an analgesic is the dose that relieves the pain. The dose of oral morphine may range from as little as 5 mg to more than 1000mg 11. Adjuvant drugs should be prescribed as indicated. For neuropathic pain, a tricyclic antidepressant or an anticonvulsant is the analgesic of choice 12. Attention to detail : it is essential to monitor the patient s response to the treatment to ensure that the patient obtains maximum benefit with as few adverse effects as possible
12 By the mouth the oral route The oral route of analgesic therapy is preferred as: 1. it is simple, acceptable, and relatively cheap 2. Most analgesics, including opioids, have clinically useful oral bioavailability 3. Oral therapy requires little medical intervention and therefore the patient is independent of infrastructure and personnel 4. The delayed absorption after oral administration prolongs the duration of action of most drugs Disadvantages: 1. in the setting of acute (e.g. Incident pain) the later peak time with oral administration may convey disadvantages 2. It may not be the preferred rout in the setting of: vomiting impaired swallow gastrointestinal obstruction malabsorption coma
13 OTHER ROUTES OF DRUG Transdermal: ADMINISTRATION avoids the problem of first pass metabolism Lipid soluble, low molecular weight drugs are more appropriate for this route Absorption is slow, and therapeutic levels can be maintained for many days Compliance is usually good Fentanyl and buprenorphine are available in patch form for transdermal administration
14 OTHER ROUTES OF DRUG ADMINISTRATION The rectal route Advantages: is cheap and requires no specialized skills The rectal veins drain to both the hepatic portal vein and the inferior vena cava, thus some first pass metabolism is avoided analgesia is of more rapid onset and longer duration than that achieved via the oral route Morphine is well absorbed rectally Disadvantages: absorption is often variable Local irritation can occur the variability of drainage makes uptake unpredictable should not be used in patients with diarrhea or fecal incontinence Immunosuppressed patients are at risk of localized infection Administration of opioids via colostomy has been shown not to be useful, probably due to comparatively poor vascularity
15 OTHER ROUTES OF DRUG ADMINISTRATION Parenteral administration Changing from enteral to parenteral administration requires adjustment, usually reduction of dose and frequent reassessment to take into account bioavailability differences resulting from lack of first-pass effect with the parenteral route Subcutaneous bioavailability may be more than 90 percent for most drugs, but depends on: The solubility of the drug, cardiovascular conditions, peripheral perfusion, the injection site, and physical exercise The availability of simple portable syringe pumps has made continuous subcutaneous morphine administration easy and acceptable for the patient who is unable to take oral medication is relatively cheap, requiring little medical input for administration Intramuscular administration is not generally recommended
16 By the clock regular around the clock medication Chronic pain, as occurs in patients with cancer, requires preventative therapy on a regular basis, thus: Avoiding recurrences of pain with unnecessary suffering Avoiding the potential development of chronic pain behavior The dose intervals should be guided by the pharmacokinetics of the drugs utilized, with each successive dose given before the preceding one has worn off Slow or sustained release preparations should be prescribed whenever available, as their use extends dosing intervals and stabilizes plasma concentrations Patients should also be provided with analgesic therapy to use as required or PRN for breakthrough or incident pain. This is also referred to as rescue analgesia
17 By the ladder sequential use of analgesic medication Analgesics are selected according to increasing pain intensity in a sequential approach Inadequate pain relief at one level results in a step up to the next level instead of changing to another drug on the same level In parallel, it encourages the combined use of nonopioid and opioid analgesics with adjuvant or coanalgesic drugs
18 STEP ONE: USE OF NONOPIOIDS For control of pain of mild to moderate intensity Examples within this group include: Paracetamol, dipyrone, traditional nonsteroidal antiinflammatory drugs (NSAID), and the newer COX-2 inhibitors In contrast to opioids, nonopioids do show a ceiling effect to their analgesic action Inadequate pain control by their use at maximum doses makes a move up the ladder necessary, if appropriate adjuvant therapy is already being used and cannot be improved
19 The benefits gained from the first step should be continued, however, even as stronger analgesia is required The combination of NSAIDs and a strong opioid, has been demonstrated to: enhance analgesia and patient satisfaction decrease opioid use without an increase in side effects
20 STEP TWO: USE OF WEAK OPIOIDS the addition of a weak opioid without discontinuation of the nonopioid Examples of drugs within this category include: Codeine phosphate, dextropropoxyphene, dihydrocodeine, and tramadol This second step is currently the subject of a wide-ranging discussion with its use being questioned in terms of: Its pharmacological validity (e.g. low doses of a strong opioid given as an alternative in step two) Its efficacy Tramadol is listed as a step two opioid, although it is better described as an atypical centrally acting analgesic because its mechanism of action combines opioid and monaminergic properties It is effective in both nociceptive and neuropathic pain
21 STEP THREE: USE OF STRONG OPIOIDS When the first two steps fail, a weak opioid is replaced with a strong opioid, again without abandoning the nonopioids and adjuvants a strong opioid should be immediately started in the setting of initial presentation with severe cancer pain Further increases in pain are then counteracted with increasing doses of strong opioid Morphine is the gold standard strong opioid of choice as recommended by the WHO
22 acceptable analgesia can be achieved in over 80 percent by using morphine in combination with a nonopioid analgesic Morphine has no clinically significant ceiling effect to analgesia, allowing large variation in the doses used to achieve pain relief limitations to morphine therapy: the accumulation of active metabolites in renal impairment lack of complete response in some pain types (particularly neuropathic pain) Large interindividual variability in morphine pharmacokinetics requiring careful titration against pain relief
23 other strong oral opioids include: Methadone, oxycodone, and hydromorphone Fentanyl and buprenorphine are also available in sustained release topical delivery systems (patches) Due to accumulation of neurotoxic metabolites, particularly in renal impairment, and its short duration of action, pethidine is not recommended
24 Fears of side effects such as respiratory depression, tolerance, and physical dependence and psychological dependence have led to worldwide underutilization of step 3 Pain acts as a stimulant to counteract any initial respiratory centre depression, while the CNS rapidly becomes tolerant to the depressant effects of opioids over time Therefore, respiratory depression due to opioid treatment of cancer pain almost never occurs the sudden relief of pain by other procedures (e.g. Neurolysis) or spinal cord compression when high doses of opioids, suddenly not counterbalanced by pain, can lead to respiratory depression
25 Because of the common occurrence of nausea and constipation with the use of strong opioids it is advisable to initiate therapy in combination with a regular antiemetic and laxative Nausea often subsides as treatment continues over a few weeks, but treatment for constipation needs to be both continued and aggressive Sedation also will usually subside within a week of stable dosing If sedation or nausea is persistent, rotating to another opioid may be useful, as cross-tolerance between strong opioids is often incomplete Cognitive impairment lasts no longer than a week and patients on stable doses of opioid have no gross change in cognitive abilities Other less frequent side effects of strong opioids are pruritus, urinary retention, and sweating
26 USE OF ADJUVANTS At any step, additional adjuvants and coanalgesic drugs should be added as appropriate for the individual patient Examples of coanalgesic drugs used here include: medications for the treatment of neuropathic pain Bisphosphonates Steroids Many other groups of drugs may be used to treat the adverse effects of analgesics, to enhance pain relief and to treat concomitant psychological disturbances such as insomnia, anxiety, and depression
27 Adjuvants Antidepressants TCAs for neuropathic pain Anticonvulsants Corticosteroids Neuroleptics Alpha 2 agonists Benzodiazepines Antispasmodics Muscle relaxants Systemic/local anesthetics
28 Adjuvants Bone pain Bisphosphonates Calcitonin Pain from malignant bowel obstruction Steroids Octreotide Anticholinergics Practice Points: Choose adjuvant carefully (risk:benefit) Start low and titrate gradually Avoid initiating several adjuvants concurrently
29 Adjuvant Analgesics for neuropathic pain CLASS EXAMPLES Anticonvulsants Antidepressants Local Anesthetics gabapentin, valproate, phenytoin, carbamazepine, clonazepam, topiramate, lamotrigine amitriptyline, desipramine, nortriptyline, paroxetine, citalopram, others mexiletine Corticosteroids dexamethasone, prednisone α-2 Adrenergic Agonists tizanidine NMDA-Receptor Agonists dextromethorphan, ketamine Topicals lidocaine, lidocaine/prilocaine, capsaicin Miscellaneous baclofen, calcitonin
30 Point It is recommended that only one agent from each group be used at one time When one drug fails to provide pain relief, a representative of the next step should be used rather than switching within a group of drugs with similar efficacy and potency However, if one drug results in unacceptable side effects, then it should be replaced by another agent from the same step
31 RESCUE ANALGESICS A short-acting opioid, such as immediate-release morphine, should be available to all cancer patients taking controlled-release preparations to treat pain not covered by their regular medications This is referred to as breakthrough pain or Incident pain Reassessment of the pain and increased doses of controlled release preparation, guided by the amount of rescue analgesia used, will usually be required
32 For the individual Setting realistic and obtainable aims of analgesic therapy clarifies the titration process Aiming for a goal that is too high initially can result in early failure, thereby frustrating the patient and possibly undermining trust in the treating physician In general, titration should be performed only with immediate-release and not with controlled-release preparations
33 Point if a starting opioid dose provides good analgesia, but with excessive sedation, then the subsequent dose should be 50 percent lower If, on the initial dose, pain relief is inadequate after 24 hours, then doses should be increased, based on rescue drug used, but a typical increase would be by 50 percent, with frequent reevaluation at least at 48 and 72 hours
34 Other Interventions Interventional therapies should be considered concurrently with the use of the ladder. It is therefore not appropriate to regard interventional techniques as a final fourth step of the ladder??????? In carefully selected patients with: 1. intractable pain unresponsive to adequately dosed opioids and other therapies 2. With intolerable adverse effects 3. with adequate prognosis use of intraspinal analgesia, particularly involving the use of nonopioids (eg, clonidine) neurolytic celiac plexus block for pancreatic cancer Palliative surgery/kyphoplasty/vertebroplasty
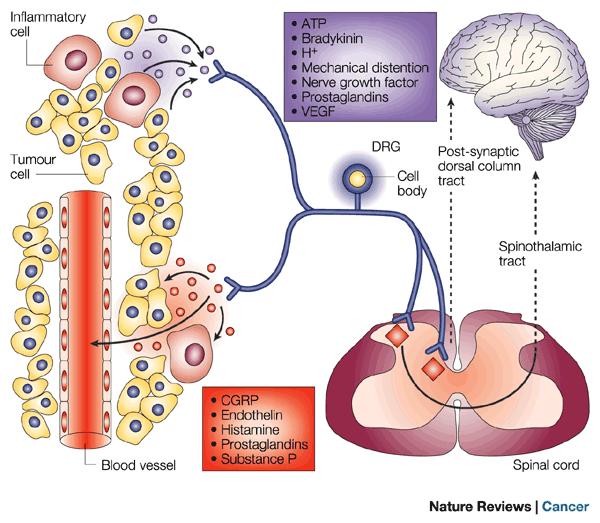
35 Nociceptive Somatic Results from inflammation and stimulation of nociceptors Tumor / Mass effect/musculoskeletal sharp, localized Visceral Is encountered in patients with primary or metastatic tumor infiltration into the viscera, such as the pancreas, liver, gastrointestinal tract, and lung is diffuse and poorly localized, and the pain is often referred to distant, and often superficial, somatic structures Autonomic reflexes, such as nausea and vomiting, may accompany visceral pain
36 Neuropathic Pain at least percent of patients are likely to suffer from neuropathic pain during the course of the disease neuropathic pain presents with complex multiple symptoms which include a combination of positive and negative signs, such as: sensory loss (numbness), spontaneous pain, allodynia, hyperalgesia, and paresthesia Mechanism: compressing or infiltrating nerves/nerve roots/blood supply to nerve Nerve damage from treatments Shooting, sharp, burning, pins & needles Examples: Cranial neuropathies/post-herpetic neuropathies Brachial plexus neuropathies/post-radiation
37 Neuropathic Pain Chemotherapy-induced neuropathies Cisplatin, Oxaliplatin Paclitaxil, Thalidomide Vincristine, Vinblastine Surgical Neuropathies Phantom limb pain Post-mastectomy syndrome Post-thoracotomy syndrome

38 Multiple Pain Mechanisms 1. Nociception 2. Peripheral sensitization 3. Central sensitization 4. Decreased inhibition/structural reorganization
39
40 Nociception Transduction Conduction Transmission Noxious stimulus Modulation primary sensory neuron central neuron
41 Peripheral Sensitization Reduced Transduction Threshold Innocuous/Noxious stimulus Primary hyperalgesia Primary allodynia Inflammation primary sensory neuron central neuron
42 Central Sensitization Increased Pain Responsiveness Noxious stimulus Secondary hyperalgesia and allodynia Irritants Tissue damage Inflammation primary sensory neuron central neuron
43 Pain Intensity Rating Scales Visual Analogue Scale (VAS) No pain Worst pain Numerical Rating Scale No pain Categorical Scale None (0) Mild (1 4) Moderate (5 6) Severe (7 10) 10 Worst pain imaginable




44 Pain Intensity Rating Scales Pain Faces Scale No hurt Hurts just a little bit Hurts a little bit more Hurts even more Hurts a whole lot Hurts as much as you can imagine
45 Quantifying pain In a patient with advanced or terminal illness, asking the patient and believing his/her report is the most appropriate approach for screening for pain (VAS) In a patient with advanced illness, the provider should evaluate for signs of potential pain such as grimacing with touch or movement, moaning, or withdrawing especially with interventions such as turning If an advanced cancer patient has a clear reason for pain or is receiving treatments that would be painful in a conscious individual, providers should treat the patient for pain even if he/she cannot verbalize discomfort
46 Assessment should include evaluating for medical or oncological emergencies Treatable syndromes, including fractures, infections, and obstruction 17% of patients pain is due to adverse effects of cancer treatment, and the burdens and benefits of such treatments should be reconsidered A complete whole patient evaluation also includes assessment for other symptoms and sources of suffering, particularly depression, and stress or family conflict related to the pain
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
Acute Pain NETP: SEPTEMBER 2013 COHORT
 Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
Module 2 Pain Management. Handouts. Pain Is... Please click the links button under the video. You can print and/or save the handouts.
 E L N E C End-of-Life Nursing Education Consortium SuperCore Curriculum Module 2 Pain Management Handouts Please click the links button under the video. You can print and/or save the handouts. Pain Is...
E L N E C End-of-Life Nursing Education Consortium SuperCore Curriculum Module 2 Pain Management Handouts Please click the links button under the video. You can print and/or save the handouts. Pain Is...
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
Pain management in palliative care. Dr. Stepanie Lippett and Sister Karen Davies-Linihan
 Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Pain management in palliative care Dr. Stepanie Lippett and Sister Karen Davies-Linihan contents Concept of total pain Steps in pain management Recognising neuropathic pain WHO analgesic ladder Common
Neuropathic Pain in Palliative Care
 Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain. November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine
 Internal Medicine, Palliative Medicine") Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Pain Assessment & Management. For General Nursing Orientation
 Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN
 Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN Oncology Clinical Nurse Specialist, Senior Research Specialist City of Hope Definition of Pain Pain is an unpleasant sensory and emotional
Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN Oncology Clinical Nurse Specialist, Senior Research Specialist City of Hope Definition of Pain Pain is an unpleasant sensory and emotional
PAIN MANAGEMENT IN UROLOGY
 24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
Cancer Pain. Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center
 Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults
 SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
Non-opioid and adjuvant pain management
 Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
CHAPTER 4 PAIN AND ITS MANAGEMENT
 CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
Enhanced Community Palliative Support Services. Lynne Ghasemi St Luke s Hospice
 Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I. Mr.D.Raju,M.pharm, Lecturer
 Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Pain. Christine Illingworth. Community Nurse St Luke s Hospice 17/5/17
 Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Neuropathic pain pharmacological management: the pharmacological management of neuropathic pain in adults in non-specialist
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Neuropathic pain pharmacological management: the pharmacological management of neuropathic pain in adults in non-specialist
Medications for the Treatment of Neuropathic Pain
 Medications for the Treatment of Neuropathic Pain February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation Neuropathic Pain Pain, paresthesias, and sensory
Medications for the Treatment of Neuropathic Pain February 23, 2011 Jinny Tavee, MD Associate Professor Neurological Institute Cleveland Clinic Foundation Neuropathic Pain Pain, paresthesias, and sensory
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008
 Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Postoperative Pain Management. Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt)
") Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
Postoperative Pain Management Nimmaanrat S, MD, FRCAT, MMed (Pain Mgt) Topics to be Covered Definition Neurobiology Classification Multimodal analgesia Preventive analgesia Step down approach Measurement
10/08/59 PAIN IS THE MOST COMMON TREATABLE SYMPTOM OF CANCER CURRENT EVIDENCE BASED CONCEPTS: MANAGEMENT OF CANCER PAIN PAIN AN UNMET CLINICAL NEED IN
 Pain is a frequent complication of cancer, and is common in many other life-limiting illnesses MANAGEMENT OF CANCER PAIN A/Prof Ghauri Aggarwal FRACP, FAChPM, FFPMANZCA Palliative Medicine Physician Sydney
Pain is a frequent complication of cancer, and is common in many other life-limiting illnesses MANAGEMENT OF CANCER PAIN A/Prof Ghauri Aggarwal FRACP, FAChPM, FFPMANZCA Palliative Medicine Physician Sydney
The pain of it all. Rod MacLeod MNZM. Hibiscus Hospice, Auckland and University of Auckland
 The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
Pain management in Paediatric Palliative Care. Dr Jane Nakawesi 14 th August 2017
 Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT
 1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
1 THE EAPC OPIOID GUIDELINES: PROCESS, RESULTS AND FUTURE DEVELOPMENT Jaegtvolden 4-5 June 2012 14. 12. 2012 2 1 3 WHO ANALGESIC LADDER (1996) NSAID +/- Adjuvant STEP II OPIODS Opids for mild to moderate
Peripheral neuropathy (PN)
") Peripheral neuropathy (PN) damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic:
Peripheral neuropathy (PN) damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic:
21 st June BDS BASHD Therapeutics Pain and Analgesia. BASHD Therapeutics Analgesics and Pain Management. Links to other BASHD content
 Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
Choose a category. You will be given the answer. You must give the correct question. Click to begin.
 Instructions for using this template. Remember this is Jeopardy, so where I have written Answer this is the prompt the students will see, and where I have Question should be the student s response. To
Instructions for using this template. Remember this is Jeopardy, so where I have written Answer this is the prompt the students will see, and where I have Question should be the student s response. To
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14. Cynthia Kim and Stephen Wilson
 UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14 Cynthia Kim and Stephen Wilson Rules Buzz first and player answers If answer correct, then the player asks teammates if they want to keep
UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14 Cynthia Kim and Stephen Wilson Rules Buzz first and player answers If answer correct, then the player asks teammates if they want to keep
The World Health Organization has developed and has widely accepted an algorithm for treatment of cancer pain. This is described as the three-step lad
 Hello. My name is Cynthia Abarado. I m an Advanced Practice Nurse at the Department of Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. I am going to present to you
Hello. My name is Cynthia Abarado. I m an Advanced Practice Nurse at the Department of Genitourinary Medical Oncology at The University of Texas MD Anderson Cancer Center. I am going to present to you
Neuropathic pain (pain due to nerve damage)
") Neuropathic pain (pain due to nerve damage) Clinical Guideline Pain can be nociceptive, neuropathic or mixed. The neuropathic component of pain generally responds poorly to conventional analgesics. Consider
Neuropathic pain (pain due to nerve damage) Clinical Guideline Pain can be nociceptive, neuropathic or mixed. The neuropathic component of pain generally responds poorly to conventional analgesics. Consider
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
sensory nerves, motor nerves, autonomic nerves
 damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic: long term, begins subtly
damage or disease affecting nerves, which may impair sensation, movement, gland or organ function, or other aspects of health, depending on the type of nerve affected o chronic: long term, begins subtly
Analgesics: Management of Pain In the Elderly Handout Package
 Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Analgesics: Management of Pain In the Elderly Handout Package Analgesics: Management of Pain in the Elderly Each patient or resident and their pain problem is unique. A complete assessment should be performed
Berkshire West Area Prescribing Committee Guidance
 Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Guideline Name Berkshire West Area Prescribing Committee Guidance Date of Issue: September 2015 Review Date: September 2017 Date taken to APC: 2 nd September 2015 Date Ratified by GP MOC: Guidelines for
Cancer Pain: A Clinical Overview. Linda A. King, MD Section of Palliative Care and Medical Ethics
 Cancer Pain: A Clinical Overview Linda A. King, MD Section of Palliative Care and Medical Ethics Objectives Define Palliative Care Review prevalence of cancer pain Know barriers to cancer pain management
Cancer Pain: A Clinical Overview Linda A. King, MD Section of Palliative Care and Medical Ethics Objectives Define Palliative Care Review prevalence of cancer pain Know barriers to cancer pain management
Index. Surg Clin N Am 85 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Clin N Am 85 (2005) 393 398 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for chronic pain, in surgical patients, 219 a2 Adrenergic agonists, for neuropathic pain,
Surg Clin N Am 85 (2005) 393 398 Index Note: Page numbers of article titles are in boldface type. A Acetaminophen, for chronic pain, in surgical patients, 219 a2 Adrenergic agonists, for neuropathic pain,
Narcotic Analgesics. Jacqueline Morgan March 22, 2017
 Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
NSG 3008A: PROFESSIONAL NURSING TRANSITION. Objectives NATURE OF PAIN. Pain is key to the survival of an organism
 NSG 3008A: PROFESSIONAL NURSING TRANSITION PAIN MANAGEMENT: STRESS ADAPTATION; CULTURAL DIVERSITY; SUBSTANCE ABUSE AND ETHICAL ISSUES Objectives 1. Describe the physiology of pain and related theories
NSG 3008A: PROFESSIONAL NURSING TRANSITION PAIN MANAGEMENT: STRESS ADAPTATION; CULTURAL DIVERSITY; SUBSTANCE ABUSE AND ETHICAL ISSUES Objectives 1. Describe the physiology of pain and related theories
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Analgesia in patients with impaired renal function Formulary Guidance
 Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
IF I M NOT TREATING WITH OPIOIDS, THEN WHAT AM I SUPPOSED TO USE?
 NON-OPIOID TREATMENT OPTIONS FOR CHRONIC PAIN Alison Knutson, PharmD, BCACP Medication Management Pharmacist Park Nicollet Creekside Clinic Dr. Knutson indicated no potential conflict of interest to this
NON-OPIOID TREATMENT OPTIONS FOR CHRONIC PAIN Alison Knutson, PharmD, BCACP Medication Management Pharmacist Park Nicollet Creekside Clinic Dr. Knutson indicated no potential conflict of interest to this
Pain Management in the
 Pain Management in the Elderly Meri Hix, PharmD, CGP, BCPS Associate Professor of Pharmacy Practice Midwestern University Chicago College of Pharmacy No conflicts of interest to declare Objectives Discuss
Pain Management in the Elderly Meri Hix, PharmD, CGP, BCPS Associate Professor of Pharmacy Practice Midwestern University Chicago College of Pharmacy No conflicts of interest to declare Objectives Discuss
Neuropathic Pain Treatment Guidelines
 Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
Sharon A Stephen, PhD, ARNP, ACHPN. September 23, 2014
 Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
Sharon A Stephen, PhD, ARNP, ACHPN September 23, 2014 Case-based presentation selected to discuss: Pain assessment Barriers to adequate pain relief Pharmacologic interventions Non-Pharmacologic interventions
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
Supportive Care. End of Life Phase
 Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Supportive Care End of Life Phase Guidelines for Health Care Professionals In the care of patients with established renal failure who are in the last days of life References: Chambers E J (2004) End of
Practical Management Of Osteoporosis
 Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS
 GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
GUIDELINES ON THE MANAGEMENT OF PAIN DUE TO CANCER IN ADULTS Bristol Palliative Care Collaborative Contact Numbers: Hospital Specialist Palliative Care Teams: North Bristol 0117 4146392 UH Bristol 0117
Pain Management in the Elderly. Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN
 Pain Management in the Elderly Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN Objectives So How Much Do You Really Know? www.geriatricpain.org Geriatric Pain Knowledge Assessment The Geriatric
Pain Management in the Elderly Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN Objectives So How Much Do You Really Know? www.geriatricpain.org Geriatric Pain Knowledge Assessment The Geriatric
Guidelines for the Management of Chronic Non-Malignant Pain (CNMP) in Primary Care (not including neuropathic pain (NeP).
 in Primary Care (not including neuropathic pain (NeP).") Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
Surrey (East Surrey CCG, Guildford & Waverley CCG, North West Surrey CCG, Surrey Downs CCG & Surrey Heath CCG) North East Hampshire & Farnham CCG and Crawley, Horsham & Mid-Sussex CCG Guidelines for the
PAIN MANAGEMENT COMPETENCY
 PAIN MANAGEMENT COMPETENCY What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is always subjective.
PAIN MANAGEMENT COMPETENCY What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is always subjective.
Pain. Fears and Facts. What is pain? Factors that Affect People with Pain. Symptom Management
 Symptom Management Pain Pain is an unpleasant physical or emotional experience. While not all cancer patients will experience pain, approximately two thirds of patients will have pain at some point during
Symptom Management Pain Pain is an unpleasant physical or emotional experience. While not all cancer patients will experience pain, approximately two thirds of patients will have pain at some point during
Pain Management in Older Adults. Mary Shelkey, PhD, ARNP
 Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
CHAPTER 4 PAIN AND ITS MANAGEMENT
 CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center
 Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Pharmacologic Management of Pain Amber D. Hartman, PharmD Specialty Practice Pharmacist James Cancer Center & Solove Research Institute Ohio State University Medical Center Objectives Identify types of
Non Malignant Pain: Symptom Management
 Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Non Malignant Pain: Symptom Management Renal Care Symposium July 2018 Anica Vasic Pain Management Unit St George Hospital Definitions Prevalence Assessment Treatment Medications Newer agents: tapentadol,
Complicated pain. Dr Stephanie Lippett
 Complicated pain Dr Stephanie Lippett UK incidence & prevalence of cancer pain 1% of UK population are living with cancer at present 70% of cancer patients experience pain 70-90% of patients with advanced
Complicated pain Dr Stephanie Lippett UK incidence & prevalence of cancer pain 1% of UK population are living with cancer at present 70% of cancer patients experience pain 70-90% of patients with advanced
Understanding pain in 5 minutes
 Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Pain Management- PallCare Definition of Pain Pain is what the patient says hurts. Dr Simon Allan Director of Palliative Care Arohanui Hospice An unpleasant sensory and emotional experience associated with
Nociceptive Pain. Pathophysiologic Pain. Types of Pain. At Presentation. At Presentation. Nonpharmacologic Therapy. Modulation
 Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
2018 Learning Outcomes
 I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
I. Pain Physiology and Anatomy (20%) A. Describe the basic anatomy of the nervous system. B. Describe the physiological mechanisms of neuronal function (eg- action potentials). C. Review the nociceptive
Subject: Pain Management (Page 1 of 7)
") Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Subject: Pain Management (Page 1 of 7) Objectives: Managing pain and restoring function are basic goals in helping a patient with chronic non-cancer pain. Federal and state guidelines require that all
Neuropathic Pain. Scott Magnuson, MD Pain Management of North Idaho, PLLC
 Neuropathic Pain Scott Magnuson, MD Pain Management of North Idaho, PLLC Pain is our friend "An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described
Neuropathic Pain Scott Magnuson, MD Pain Management of North Idaho, PLLC Pain is our friend "An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described
FDA hormone replacement therapy Web site 6
 TABLE OF CONTENTS Caring for pain at UIMCC 1-5 FDA hormone replacement therapy Web site 6 P&T Committee Formulary Action - September 2003 6 Caring for pain at UIMCC The International Association for the
TABLE OF CONTENTS Caring for pain at UIMCC 1-5 FDA hormone replacement therapy Web site 6 P&T Committee Formulary Action - September 2003 6 Caring for pain at UIMCC The International Association for the
Pain Management in Hospice and Palliative Care
 Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Pain Management in Hospice and Palliative Care A Case-based Approach JoAnne Nowak, M.D. Merrimack Valley Hospice Revised November 2011 Objectives Use a case study approach to stimulate discussion and illustrate
Management of Pain related to Spinal Cord Lesion
 Management of Pain related to Spinal Cord Lesion A Neurologist s Perspective Vincent Mok, MD Associate Professor Division of Neurology Department of Medicine and Therapeutics The Chinese University of
Management of Pain related to Spinal Cord Lesion A Neurologist s Perspective Vincent Mok, MD Associate Professor Division of Neurology Department of Medicine and Therapeutics The Chinese University of
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation
 Bridging the Gap from Surgery to Rehabilitation") Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Anaesthesia and Pain Management for Endo Exo Femoral Prosthesis (EEFP) Bridging the Gap from Surgery to Rehabilitation Dr Ajay Kumar Senior Lecturer Macquarie and Melbourne University Introduction Amputee
Q&A: Opioid Prescribing for Chronic Non-Malignant Pain
 NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
Pain. Pain and management of pain. Henning Andreas Haga Associate professor Norwegian School of Veterinary Science
 Pain and management of pain Henning Andreas Haga Associate professor Norwegian School of Veterinary Science Pain An unpleasant sensory and emotional experience associated with actual or potential tissue
Pain and management of pain Henning Andreas Haga Associate professor Norwegian School of Veterinary Science Pain An unpleasant sensory and emotional experience associated with actual or potential tissue
Analgesia. This is widely used in palliative care. It has antipyretic and analgesic effects but no anti-
 Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Page 1 of 8 Analgesia The World Health Organisation (WHO, 1990) has devised a model to assist health care professionals in the management of cancer pain. The recommendations include managing pain, by the
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management
 Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Optimizing Your Quality of Life During Cancer Treatment: Pain & Side Effect Management Eric Roeland, MD GI Oncology Palliative Medicine Pancreatic Cancer Patient Tool Belt Chemotherapy Surgery Pain & Symptom
Pharmacotherapy of Pain SUPHAT SUBONGKOT, PHARM.D. BCOP, BCOP CLINICAL PHARMACY DIVISION KHON KAEN UNIVERSITY, THAILAND
 Pharmacotherapy of Pain SUPHAT SUBONGKOT, PHARM.D. BCOP, BCOP CLINICAL PHARMACY DIVISION KHON KAEN UNIVERSITY, THAILAND Therapeutic Strategies for Pain and Disability Pharmacotherapy Rehabilitative approaches
Pharmacotherapy of Pain SUPHAT SUBONGKOT, PHARM.D. BCOP, BCOP CLINICAL PHARMACY DIVISION KHON KAEN UNIVERSITY, THAILAND Therapeutic Strategies for Pain and Disability Pharmacotherapy Rehabilitative approaches
Pancreatic cancer Palliative Care
 Pancreatic cancer Palliative Care Snežana Bošnjak Institute for Oncology and Radiology of Serbia Dept. Supportive Oncology & Pall Care Serbia, Belgrade Pancreatic Cancer: Palliative Care Abdominal / epigastric
Pancreatic cancer Palliative Care Snežana Bošnjak Institute for Oncology and Radiology of Serbia Dept. Supportive Oncology & Pall Care Serbia, Belgrade Pancreatic Cancer: Palliative Care Abdominal / epigastric
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Palliative Care Impact Survey
 September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
September 2018 Contents Introduction...3 Headlines...3 Approach...4 Findings...4 Which guideline are used...4 How and where the guidelines are used...6 Alternative sources of information...7 Use of the
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
Mid Essex Locality Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care
 Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Guideline for Management of Adult Acute and Chronic Non-Cancer Pain in Primary care If possible patients should be assessed using a simple visual analogue scale VAS to determine the most appropriate stage
Spinal Cord Injury Pain. Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018
 Spinal Cord Injury Pain Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018 Objectives At the conclusion of this session, participants should be able to: 1. Understand the difference between nociceptive
Spinal Cord Injury Pain Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018 Objectives At the conclusion of this session, participants should be able to: 1. Understand the difference between nociceptive
Overview of Pain Types and Prevalence
 Pain Resource Nurse Overview of Pain Types and Prevalence Pain Resource Nurse Program Module 1 The Resource Center of the Alliance of State Pain Initiatives University of Wisconsin Board of Regents, 2011
Pain Resource Nurse Overview of Pain Types and Prevalence Pain Resource Nurse Program Module 1 The Resource Center of the Alliance of State Pain Initiatives University of Wisconsin Board of Regents, 2011
PAIN TERMINOLOGY TABLE
 PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly
 Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Mitigating Risks While Optimizing the Benefits of Pharmacologic Agents to Manage Pain in the Elderly Mary Lynn McPherson, PharmD, MDE, MA, BCPS, CPE Professor and Executive Director, Advanced Post-Graduate
Pain management. Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD
 Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Pain management Coleman Palliative Care Conference: February 2016 Josh Baru MD Stacie Levine MD Case #1 61 yo man with history of Stage 3 colon cancer, s/p resection and adjuvant chemotherapy with FOLFOX
Symptom Control in the Community Setting. Dr Andrew Tysoe-Calnon
 Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Symptom Control in the Community Setting Dr Andrew Tysoe-Calnon Lead Consultant t Common symptoms Pain Agitation Shortness of breath Nausea and vomiting Intestinal obstruction Confusion Pain Occurs in
Management of Chronic Pain in Children. Objectives: Common Myths about Pain. University of Texas Health Science Center at San Antonio, Texas
 Management of Chronic Pain in Children I have no disclosures. Glen Medellin, MD Cure sometimes, treat often, comfort always. Hippocrates Objectives: The number of children admitted with chronic pain has
Management of Chronic Pain in Children I have no disclosures. Glen Medellin, MD Cure sometimes, treat often, comfort always. Hippocrates Objectives: The number of children admitted with chronic pain has
Regional Renal Training
 Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
Regional Renal Training Palliative and End of Life Care Dr Clare Kendall North Bristol NHS Trust Advanced Kidney Disease Dialysis/Transplant Conservative Management Deteriorating despite dialysis/failing
BJF Acute Pain Team Formulary Group
 Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Title Analgesia Guidelines for Acute Pain Management (Adults) in BGH Document Type Issue no Clinical guideline Clinical Governance Support Team Use Issue date April 2013 Review date April 2015 Distribution
Understanding pain and mental illness Impact on management principles
 Understanding pain and mental illness Impact on management principles Chris Alderman Consultant Psychopharmacologist Pain and mental illness - context PAIN MENTAL ILLNESS OTHER FACTORS (personality, history.
Understanding pain and mental illness Impact on management principles Chris Alderman Consultant Psychopharmacologist Pain and mental illness - context PAIN MENTAL ILLNESS OTHER FACTORS (personality, history.
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE?
 PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
A Letter From Home February 2016
 More than two thirds of all Americans suffer from multiple, chronic conditions. An estimated 60-70% of people over 65 report at least some persistent pain (Centers for Disease Control and Prevention, 2013).
More than two thirds of all Americans suffer from multiple, chronic conditions. An estimated 60-70% of people over 65 report at least some persistent pain (Centers for Disease Control and Prevention, 2013).
Care in the Last Days of Life
 Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient
Care in the Last Days of Life Introduction This guideline is an aid to clinical decision making and good practice in person-centred care for patients who are deteriorating and at risk of dying. The patient