Integrating Pain Metrics into Oncologic Clinical and Regulatory Decision-Making. Charles Cleeland MD Anderson Cancer Center
|
|
|
- Lynette Pitts
- 6 years ago
- Views:
Transcription

1 Integrating Pain Metrics into Oncologic Clinical and Regulatory Decision-Making Charles Cleeland MD Anderson Cancer Center
2 Panelists Charles Cleeland, Department Chair, Department of Symptom Research, MD Anderson Cancer Center Carole Baas, Advocate, Physical Sciences in Oncology, NCI Laurie Burke, Assoc. Director for Study Endpoints and Labeling Development, Office of New Drugs, CDER, FDA Ann O Mara, Head of Palliative Care Research, Community Oncology and Prevention Trials Research Group, NCI Martin Zagari, Global Health Economics Head, Amgen
3 Panel Topic Introduction Pain is a disabling consequence of cancer and of some cancer treatments Pain can be best measured by self-report of patients (a patient reported outcome) Inclusion of effects of treatment on pain and other symptoms provides critical information about the patient s experience in clinical trials
4 Prevalence of Pain In Cancer Review of 41 Studies After curative treatment, 33% During anticancer treatment: 59% With advanced/metastatic disease, 64% Pooled prevalence of pain was >50% in all cancer types More than one-third graded their pain as moderate or severe. van den Beuken-van Everdingen Ann Oncol. 2007
5 Current Cancer Pain Management Most disease-related pain can be controlled with opioids, BUT at a cost in side effects Treatment-related pain more difficult to control (especially that caused by nerve damage) Agents that prevent/reduce pain targeted at mechanisms of pain production of potentially great benefit opioid sparing
6 Pain Benefit in Cancer The pain benefit of a treatment is related to both the reduction of pain severity/impact the time of overall survival spent with no or lower severity pain.
7 Activities Impaired by Increasing Pain relate walk walk enjoy work enjoy sleep active mood work enjoy sleep active mood work enjoy sleep active mood work enjoy sleep active mood work enjoy > > > > worst pain rating > > > > Cleeland & Wang
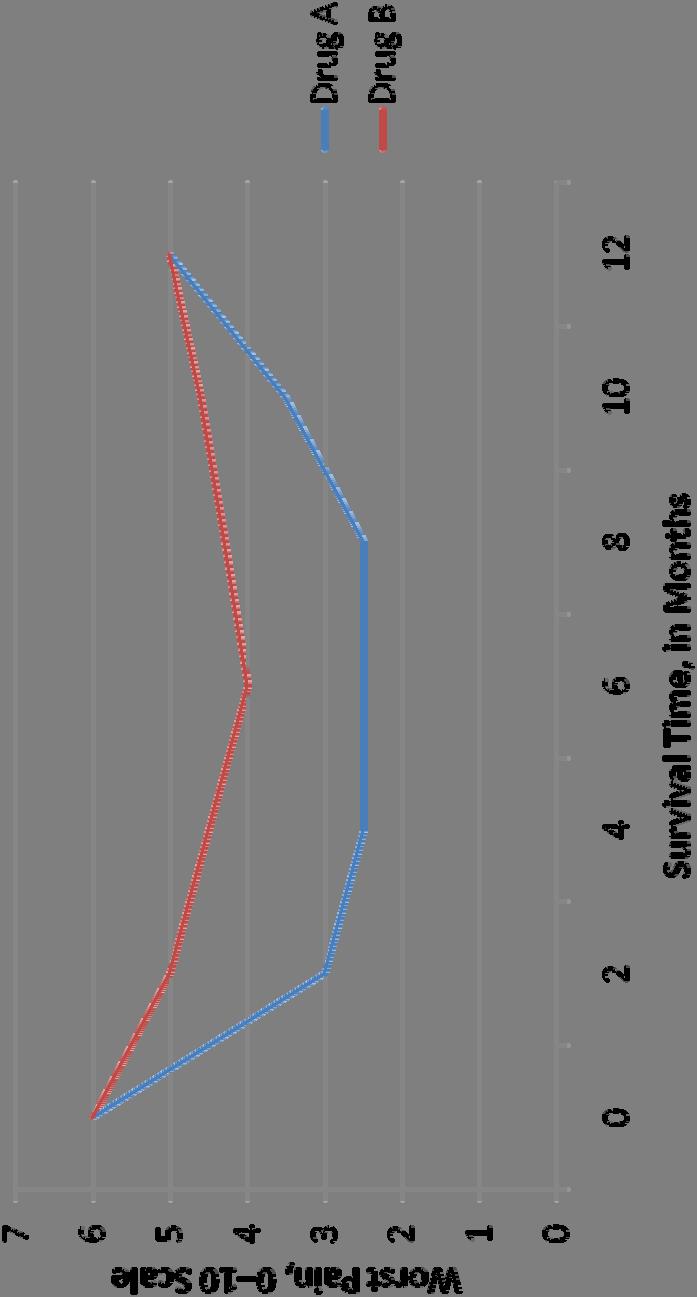
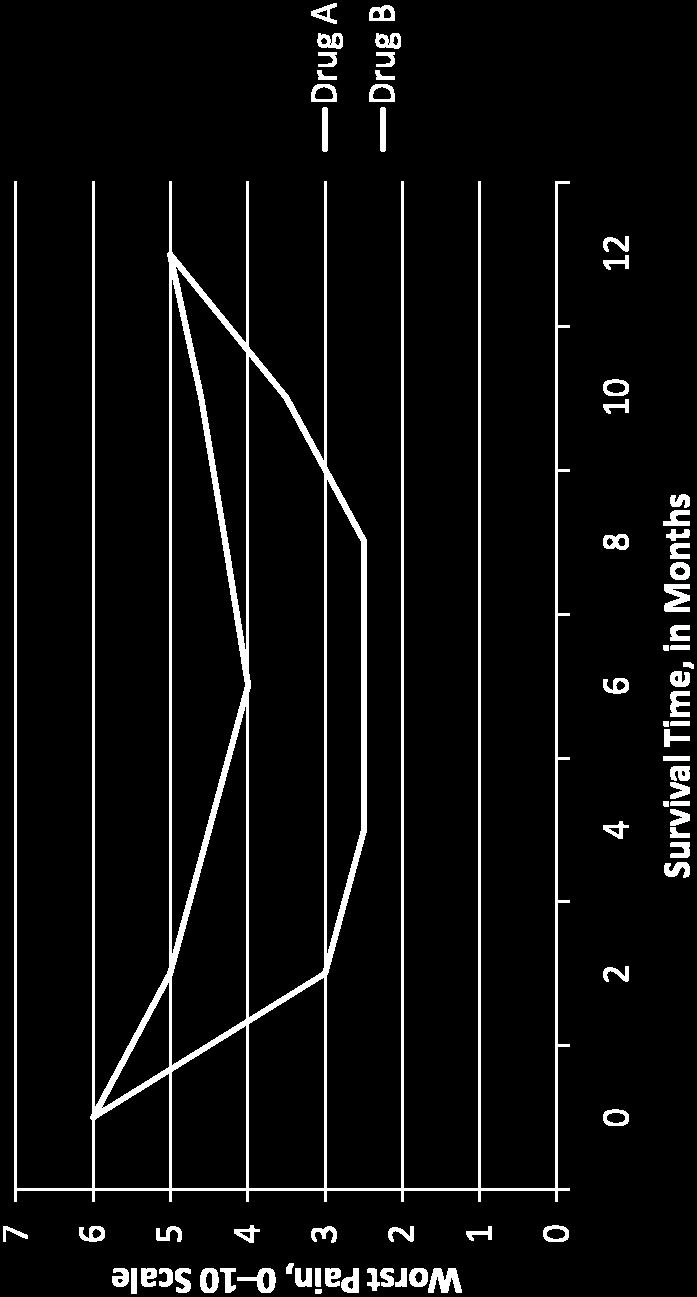
8 Pain Palliation as Benefit

9 Pain Prevention as Benefit
10 Challenges for Implementation Why or why not do sponsors include pain? Is pain a primary or secondary endpoint? How do palliation and progression endpoints differ? How to incorporate effects of analgesics in endpoints? How to separate effects of agent on pain and tumor burden?
11 NCI Perspective Ann O Mara, PhD, RN Head, Palliative Care Research Division of Cancer Prevention, NCI
12 RTOG 9714: Short vs. Long-Course for Palliation of Painful Bone Metastasis 8 Gy vs. 30 Gy Breast or prostate cancer Endpoints: pain and narcotic relief 898 patients Stratified by # of painful sites, treatment site, initial worse pain score, use of bisphosphonates
13 Endpoint Evaluation At 3 months after radiation therapy: Worst pain score on Brief Pain Inventory Use of any narcotic pain medication Complete response: no pain, no narcotics Partial response: Pain score <2 at baseline Stable response: Pain +/- 1 Progression: Pain >2
14 Results No difference between 2 arms: Complete, partial, stable or progression of pain Use of narcotics Pathologic fracture incidence
15 Other Symptoms Early stage prostate cancer What is the effect of different radiation approaches (external beam, brachytherapy, protons, fractionated stereotactic radiotherapy) on symptoms (urinary, bowel, erectile dysfunction)?
16 Integrating Pain Metrics into Oncologic Clinical and Regulatory Decision-Making Martin Zagari, MD Amgen
17 Contemporary Drug Development Reality and Symptom Endpoints Drug development costs continue to escalate, research productivity is down, and payment for future innovative product increasingly uncertain Designing increasingly complex trials is not the primary challenge (industry and FDA are used to complexity) The measurement of pain or symptoms is imperfect, path to labeling and meaning of results often unclear, and risk perceived as high Can t be done in time for phase 3; Unforeseen benefit in ph 2 Reluctance to allocate alpha for uncertain results Hard regulatory requirements and trial must haves are (of course) prioritized first Downside outweighs upside (efficacy requirements are very high but safety labeling is increasingly broad and inclusive)
18 What Would Stimulate More Pain and Symptom Research Interest? Ability to qualify instruments (or more instruments qualified) More Pathways to Labeling or Provider Access to Pain Outcome Results ( Appropriate but Attainable ) Consistency in Interpretation (and understanding) of Results by DACs, Medical Review Divisions, and SEALD Guidance from FDA on Oncology-Related Pain Assessment Methodology Development and Qualification of Enabling Technologies
19 Could Labeling Provide More Clinical and Outcomes Information? Can we accelerate instrument qualification (C-PATH as a path)? After a drug is shown to have an effect, are noteworthy secondary pain findings as important as safety results in helping physicians and patients make a balanced riskbenefit decision? Could there be a US equivalent of the Pharmacodynamic section of the European SmPC* where noteworthy trial results (including pain or other outcomes) are considered for listing even if alpha is not allocated? *Summary of Product Characteristics
20 Can We Reduce Uncertainty in the Review Process? How do we reach agreement on a meaningful difference for a secondary pain outcome (i.e. what do we power for)? Sponsors and FDA may not agree on a meaningful change Is it necessary to spend alpha or are some pain differences important enough to be self evident? What are they? Does a secondary cancer pain treatment effect need to be as large as might be required for an analgesic? Are advisory committees and other review groups well versed enough in assessment of these outcomes?
21 Could FDA Develop Guidance for Oncology- Specific Pain Measurement and Analysis? Could industry and FDA develop endpoints for analgesia-sparing, or conventions for adjusting pain results for analgesia use? Can standards be agreed (or shared) for: Acceptable drop out rate and missing data handling Event-driven assessment and modeling (e.g. time varying techniques) Non-inferiority margin for additive (supportive) treatments
22 How can Technology be Deployed More Effectively? Real-time, mobile devices could allow for collection of vastly more pain or functional impact information but costs and qualification in time for cancer trials is a challenge (many tumor types) What would it take to create a cross-oncology platform? Is there an opportunity for functional endpoints such as Patient Activity Monitoring (PAM)? When are smart mobile devices ready for prime time?
23 Type of compound Potential benefit Instruments Trial Scenarios Scenario 1 Scenario 2 Scenario 3 Anti neoplastic NME with new MOA Pain palliation in addition to treatment of mcrpc Similar MOA with similar survival Similar survival in mcrpc but decreased painful neuropathy Pain molecule Would qualification be required for both palliation and reduction in progression? Novel pain modifying agent may decrease time to cancer pain progression when added to second line Analgesia use and treatment benefit How much reduction in pain is meaningful? How much reduction in analgesia is meaningful? How is onset defined? Time to analgesic use? Interaction of analgesia with pain? Endpoint Composite pain and analgesia? Time to pain or analgesia use? AUC, vs worst pain? Alpha Rescue Technology Is there ever a magnitude of benefit where pre-specification would not be required for labeling? Are some preferred technologies emerging that enable richer patient input? Would non-inferiority be required and would it vary with pain effect? How would one approach rescue for pain?
24 Integrating Pain Metrics into Oncologic Clinical and Regulatory Decision-Making Carole Baas, PhD Patient Advocate
25 In cancer patients, pain is one of the most feared and burdensome symptoms. van den Beuken-van Everdingen. Ann Oncol. 2007
26 Pain occurs in approximately one quarter of patients with newly diagnosed malignancies, one third of patients undergoing treatment, and three quarters of patients with advanced disease, and is one of the symptoms patients fear most. Swarm R, et al. Adult Cancer Pain. J Natl Compr Canc Netw. 2010
27 Despite the clear WHO recommendations, cancer pain is still a major problem. The increasing number of cancer survivors who live to an advanced age means that it is of paramount importance to reduce the prevalence of pain at all stages of the disease process. van den Beuken-van Everdingen. Ann Oncol. 2007
28 Why Pain Management in Patients with Metastatic Cancer? Pain is usually what gets patients with advanced cancer to the doctor Pain is usually associated with poor quality of life Physical pain is associated with psychological pain and spiritual pain Other symptoms are diagnosed and causes of the pain are identified Control of pain will help patients focus on getting their cancer under control
; advanced prostate cancer. CT scans and bone scan indicate extensive and aggressive cancer in hips, spinal region and shoulders.")
29 Case Study and Pain Management 1 A 58 year old African American male is presented to the multidisciplinary prostate cancer clinic with a PSA of His biopsy results were Gleason score of 10 (T4); advanced prostate cancer. CT scans and bone scan indicate extensive and aggressive cancer in hips, spinal region and shoulders. Arrives in wheelchair and is physically unable to stand due to a tremendous amount of back and hip pain.
30 Pain Management & Quality of Life Patient was given a hormone injection (3 month LUPRON) to halt the onset of the cancer Patient also was scheduled for treatments with ZOMETA and EBRT (external beam radiation therapy) Patient returned to clinic in one month with reduced PSA score and walked into clinic with the use of walking cane (still unsteady) Patient and family reported significant reduction in pain and subsequently patient was able to resume walking Patient quality of life improved with pain management
 and Lenalidomide (Revlimid) Now at Year 5: Experiencing progressive neuropathy in feet and")
31 Case Study and Pain Management 2 55 year old man is diagnosed with Stage 1 multiple myeloma Treated with steroids, chemotherapy, thalidomide and bone marrow transplant Relapsed 1 year later, treated with the corticosteroid dexamethasone (Decadron) and Lenalidomide (Revlimid) Now at Year 5: Experiencing progressive neuropathy in feet and hands
32 Pain Management & Quality of Life Patient has numbness in hands and feet Patient is a critical care physician: Working is who I am and what I do. I m not ready to quit. I don t want to lose function, particularly in my hands. Treatment-induced neuropathy has had a significant impact on patient s quality of life and ability to function and work There s a gap in practitioners understanding of the real treatment course. They understand the disease but not the side effects of treatment.
33 Oncology patients are interested in: achieving clinically meaningful beneficial effects on disease-related symptoms ability to carry out normal activities overall survival Fleming TR, Rothmann MD, Lu HL. J Clin Oncol. 2009
34 pain management is not only for end-of-life care There is a new population of patients who have essentially been cured or who can expect long-term survival but have been left with serious pain issues as a result of treatment. Sherman C. Oncology Nurse Advisor 2010
Hypofractionated RT in Cervix Cancer. Anuja Jhingran, MD
 Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
Hypofractionated RT in Cervix Cancer Anuja Jhingran, MD Hypofractionated RT in Cervix Cancer: Clinicaltrials.gov 919 cervix trials 134 hypofractionated RT trials Prostate, breast, NSCLC, GBM 0 cervix trials
AllinaHealthSystems 1
 2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
2018 Dimensions in Oncology Genitourinary Cancer Disclosures I have no financial or commercial relationships relevant to this presentation. Matthew O Shaughnessy, MD, PhD Director of Urologic Oncology
Radiotherapy symptoms control in bone mets. Francesco Cellini GemelliART. Ernesto Maranzano,MD. Session 5: Symptoms management
 Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Session 5: Symptoms management Radiotherapy symptoms control in bone mets Francesco Cellini GemelliART Ernesto Maranzano,MD Director of Oncology Department Chief of Radiation Oncology Centre S. Maria Hospital
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Rhona McMenemin Consultant in Clinical Oncology The
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer
 Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Incorporating New Agents into the Treatment Paradigm for Prostate Cancer Dr. Celestia S. Higano FACP, Professor, Medicine and Urology, Uni. of Washington Member, Fred Hutchinson Cancer Research Center
Patient Engagement to Get The Question Right
 Patient Engagement to Get The Question Right Minnie Reddy PATIENTS Program Advisor; Member of Mount Lebanon Baptist Church C. Daniel Mullins, PhD Professor and Chair PHSR Dept, UM School of Pharmacy PATIENTS
Patient Engagement to Get The Question Right Minnie Reddy PATIENTS Program Advisor; Member of Mount Lebanon Baptist Church C. Daniel Mullins, PhD Professor and Chair PHSR Dept, UM School of Pharmacy PATIENTS
The Role of Radiotherapy in Metastatic Breast Cancer. Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health
 The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
The Role of Radiotherapy in Metastatic Breast Cancer Shilpen Patel MD, FACRO Associate Professor Departments of Radiation Oncology and Global Health Indications for Palliative Pain Control Radiation Bone
DRAFT FOR CONSULTATION. Clinical Commissioning Policy Proposition: Palliative radiotherapy for bone pain
 Clinical Commissioning Policy Proposition: Palliative radiotherapy for bone pain Information Reader Box (IRB) to be inserted on inside front cover for documents of 6 pages and over, with Publications Gateway
Clinical Commissioning Policy Proposition: Palliative radiotherapy for bone pain Information Reader Box (IRB) to be inserted on inside front cover for documents of 6 pages and over, with Publications Gateway
Clinical Commissioning Policy Proposition: Proton Beam Therapy for Cancer of the Prostate
 Clinical Commissioning Policy Proposition: Proton Beam Therapy for Cancer of the Prostate Reference: NHS England B01X09 First published: March 2016 Prepared by NHS England Specialised Services Clinical
Clinical Commissioning Policy Proposition: Proton Beam Therapy for Cancer of the Prostate Reference: NHS England B01X09 First published: March 2016 Prepared by NHS England Specialised Services Clinical
Clinical Case Conference
 Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
Clinical Case Conference Palliative radiation therapy for bone metastasis Jeff Burkeen, MD, PGY2 7/20/2015 1 Overview Epidemiology Pathophysiology Common presentations and symptoms Imaging Surgery Radiation
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 11 th May 2017 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk Clinical
Managing Bone Pain in Metastatic Disease. Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018
 Managing Bone Pain in Metastatic Disease Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018 None Disclosures Managing Bone Pain in Metastatic Disease This lecture will
Managing Bone Pain in Metastatic Disease Rachel Schacht PA-C Medical Oncology and Hematology Associates Presented on 11/2/2018 None Disclosures Managing Bone Pain in Metastatic Disease This lecture will
Prostate Cancer Incidence
 Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
Prostate Cancer: Prevention, Screening and Treatment Philip Kantoff MD Dana-Farber Cancer Institute Professor of fmedicine i Harvard Medical School Prostate Cancer Incidence # of patients 350,000 New Cases
NCCN Framework for resource stratification of cervical cancer treatment
 NCCN Framework for resource stratification of cervical cancer treatment Wui-Jin Koh, MD SCCA/University of Washington/Fred Hutchinson Cancer Research Center Benjamin Greer, MD SCCA/UW/FHCRC Nadeem Abu-Rustum,
NCCN Framework for resource stratification of cervical cancer treatment Wui-Jin Koh, MD SCCA/University of Washington/Fred Hutchinson Cancer Research Center Benjamin Greer, MD SCCA/UW/FHCRC Nadeem Abu-Rustum,
IOM Workshop: Achieving Value in Cancer Care: ASCO s Top 5 and Beyond Lowell E. Schnipper, M.D.
 IOM Workshop: Achieving Value in Cancer Care: ASCO s Top 5 and Beyond Lowell E. Schnipper, M.D. Expenditures Cancer Care: 2010 Initial dx, continuing care, last phase Costs of Cancer Care: breast, colorectal,
IOM Workshop: Achieving Value in Cancer Care: ASCO s Top 5 and Beyond Lowell E. Schnipper, M.D. Expenditures Cancer Care: 2010 Initial dx, continuing care, last phase Costs of Cancer Care: breast, colorectal,
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
This LCD recognizes these two distinct treatment approaches and is specific to treatment delivery:
 National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: 77371, 77372, 77373 LCD ID Number: L33410 J-N FL Responsible
National Imaging Associates, Inc. Clinical guidelines STEREOTACTIC RADIOSURGERY (SRS) AND STEREOTACTIC BODY RADIATION THERAPY (SBRT) CPT4 Codes: 77371, 77372, 77373 LCD ID Number: L33410 J-N FL Responsible
PSA Screening and Prostate Cancer. Rishi Modh, MD
 PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
PSA Screening and Prostate Cancer Rishi Modh, MD ABOUT ME From Tampa Bay Went to Berkeley Prep University of Miami for Undergraduate - 4 years University of Miami for Medical School - 4 Years University
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer
 Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Pelvic palliative radiotherapy for gynecological cancers present state of knowledge and pending research questions to answer Esten S. Nakken MD PhD Division of Cancer Medicine Oslo University Hospital
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
Stereotactic Ablative Radiotherapy for Prostate Cancer
 Stereotactic Ablative Radiotherapy for Prostate Cancer Laurie Cuttino, MD Associate Professor of Radiation Oncology VCU Massey Cancer Center Director of Radiation Oncology Sarah Cannon Cancer Center at
Stereotactic Ablative Radiotherapy for Prostate Cancer Laurie Cuttino, MD Associate Professor of Radiation Oncology VCU Massey Cancer Center Director of Radiation Oncology Sarah Cannon Cancer Center at
Advances and Challenges in Radiation Protection of Patients Modern Radiotherapy. Risk Acceptability
 Advances and Challenges in Radiation Protection of Patients Modern Radiotherapy Risk Acceptability Versailles, France December 2-4, 2009 Fred A. Mettler Jr. M.,D., M.P.H. New Mexico Federal Regional Medical
Advances and Challenges in Radiation Protection of Patients Modern Radiotherapy Risk Acceptability Versailles, France December 2-4, 2009 Fred A. Mettler Jr. M.,D., M.P.H. New Mexico Federal Regional Medical
New Approaches to Survivor Health Care
 New Approaches to Survivor Health Care May 14, 2007 Survivorship Care Models Mary S. McCabe, RN Ms. McCabe is the Director of the Cancer Survivorship Program at Memorial Sloan-Kettering Cancer Center.
New Approaches to Survivor Health Care May 14, 2007 Survivorship Care Models Mary S. McCabe, RN Ms. McCabe is the Director of the Cancer Survivorship Program at Memorial Sloan-Kettering Cancer Center.
Clinical oncology workforce: the case for expansion Faculty of Clinical Oncology
 www.rcr.ac.uk Clinical oncology workforce: the case for expansion Faculty of Clinical Oncology www.rcr.ac.uk Contents Foreword 2 1. Background information 3 What do clinical oncologists do? 3 Why is the
www.rcr.ac.uk Clinical oncology workforce: the case for expansion Faculty of Clinical Oncology www.rcr.ac.uk Contents Foreword 2 1. Background information 3 What do clinical oncologists do? 3 Why is the
Bone metastases of solid tumors Diagnosis and management by
 Bone metastases of solid tumors Diagnosis and management by Dr/RASHA M Abd el Motagaly oncology consultant Nasser institute adult oncology unit 3/27/2010 1 Goals 1- Know the multitude of problem of bone
Bone metastases of solid tumors Diagnosis and management by Dr/RASHA M Abd el Motagaly oncology consultant Nasser institute adult oncology unit 3/27/2010 1 Goals 1- Know the multitude of problem of bone
ISSUE BRIEF Conference on Clinical Cancer Research November 2011
 ISSUE BRIEF Conference on Clinical Cancer Research November 2011 PANEL 3 Symptom Measurement in Clinical Trials Ethan Basch, Associate Attending Physician, Memorial Sloan-Kettering Cancer Center Lori Minasian,
ISSUE BRIEF Conference on Clinical Cancer Research November 2011 PANEL 3 Symptom Measurement in Clinical Trials Ethan Basch, Associate Attending Physician, Memorial Sloan-Kettering Cancer Center Lori Minasian,
The Latest is the Greatest. Future Directions in the Management of Patients with Bone Metastases from Breast Cancer
 City Wide Medical Oncology Rounds Friday Sept. 21 st, 2007 The Latest is the Greatest Future Directions in the Management of Patients with Bone Metastases from Breast Cancer Mark Clemons Head, Breast Medical
City Wide Medical Oncology Rounds Friday Sept. 21 st, 2007 The Latest is the Greatest Future Directions in the Management of Patients with Bone Metastases from Breast Cancer Mark Clemons Head, Breast Medical
Louisa Fleure. Advanced Prostate Cancer Clinical Nurse Specialist. Guys and St Thomas NHS Trust
 Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
Louisa Fleure Advanced Prostate Cancer Clinical Nurse Specialist Guys and St Thomas NHS Trust The classification of advanced prostate cancer The incidence of patients presenting with, or developing advanced
OVERALL CLINICAL BENEFIT
 pcodr systematic review but were excluded from the review because they were retrospective case series. perc confirmed that the inclusion and exclusion criteria of the systematic review were appropriate
pcodr systematic review but were excluded from the review because they were retrospective case series. perc confirmed that the inclusion and exclusion criteria of the systematic review were appropriate
Palliative radiotherapy in lung cancer
 New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
New concepts and insights regarding the role of radiation therapy in metastatic disease Umberto Ricardi University of Turin Department of Oncology Radiation Oncology Palliative radiotherapy in lung cancer
Framework for Defining Evidentiary Standards for Biomarker Qualification: Minimal Residual Disease (MRD) in Multiple Myeloma (MM)
 in Multiple Myeloma (MM)") Framework for Defining Evidentiary Standards for Biomarker Qualification: Minimal Residual Disease (MRD) in Multiple Myeloma (MM) MRD in Multiple Myeloma Team Biomarker Qualification Workshop Framework
Framework for Defining Evidentiary Standards for Biomarker Qualification: Minimal Residual Disease (MRD) in Multiple Myeloma (MM) MRD in Multiple Myeloma Team Biomarker Qualification Workshop Framework
Isotopes and Palliative Radiotherapy for bone metastases
 Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
The management and treatment options for secondary bone disease. Dr Jason Lester Clinical Oncologist Velindre Cancer Centre
 The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
The management and treatment options for secondary bone disease Dr Jason Lester Clinical Oncologist Velindre Cancer Centre Aims Overview of bone metastases management in castrate-refractory prostate cancer
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 brentuximab. Given that the median survival of Hodgkin lymphoma patients who relapse after ASCT is approximately two years, perc considered that the manufacturer had substantially overestimated the incremental
brentuximab. Given that the median survival of Hodgkin lymphoma patients who relapse after ASCT is approximately two years, perc considered that the manufacturer had substantially overestimated the incremental
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION
 FINAL RECOMMENDATION") pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
pcodr EXPERT REVIEW COMMITTEE (perc) FINAL RECOMMENDATION The pan-canadian Oncology Drug Review (pcodr) was established by Canada s provincial and territorial Ministries of Health (with the exception of
Ακτινοθεραπευτική Ογκολογία & Παθολογική Ογκολογία
 Office or other outpatient visit for the evaluation and management of a new patient, which requires these 3 key components: A problem focused history; A problem focused examination; Straightforward medical
Office or other outpatient visit for the evaluation and management of a new patient, which requires these 3 key components: A problem focused history; A problem focused examination; Straightforward medical
Delivering the best of both worlds effective, high-dose treatment with minimal side effects
 Delivering the best of both worlds effective, high-dose treatment with minimal side effects New Treatment, New Hope A cancer diagnosis changes your life. It can leave you unsure of the best plan of action.
Delivering the best of both worlds effective, high-dose treatment with minimal side effects New Treatment, New Hope A cancer diagnosis changes your life. It can leave you unsure of the best plan of action.
EVIDENCE IN BRIEF OVERALL CLINICAL BENEFIT
 large impact on cost-effectiveness. perc discussed that one of the main factors affecting the costeffectiveness estimates was the survival estimates used in the economic model. In reviewing the clinical
large impact on cost-effectiveness. perc discussed that one of the main factors affecting the costeffectiveness estimates was the survival estimates used in the economic model. In reviewing the clinical
Caring for Survivors. Nancy Houlihan, RN, MA, AOCN. Cancer Survivorship Program
 Caring for Survivors Nancy Houlihan, RN, MA, AOCN Cancer Survivorship Program Survivors Growing numbers of survivors Convergance of ageing population and numbers surviving cancer Greatest number are over
Caring for Survivors Nancy Houlihan, RN, MA, AOCN Cancer Survivorship Program Survivors Growing numbers of survivors Convergance of ageing population and numbers surviving cancer Greatest number are over
Metastatic Spinal Cord Compression
 Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
Metastatic Spinal Cord Compression Dr Zacharias Tasigiannopoulos Clinical Oncologist Colney centre Department of Oncology Norwich, UK Introduction 2-5% of cancer patients have an episode of MSCC Initial
Early Integration of Palliative Care
 Early Integration of Palliative Care Dr. Camilla Zimmermann Head, Palliative Care Program University Health Network Toronto November 1, 2014 www.fpon.ca Early Integration of Palliative Care: Evidence and
Early Integration of Palliative Care Dr. Camilla Zimmermann Head, Palliative Care Program University Health Network Toronto November 1, 2014 www.fpon.ca Early Integration of Palliative Care: Evidence and
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Prostate Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE. Proposed Health Technology Appraisal
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Radium-223 chloride for the treatment of bone metastases in castrate resistant prostate cancer Draft scope Draft
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE Proposed Health Technology Appraisal Radium-223 chloride for the treatment of bone metastases in castrate resistant prostate cancer Draft scope Draft
RADIONUCLIDE THERAPY FOR PALLIATION OF PAIN FROM BONY METASTASES
 RADIONUCLIDE THERAPY FOR PALLIATION OF PAIN FROM BONY METASTASES Overview and Topics to Be Covered Reviews the use of radionuclide therapy in nuclear medicine for palliation of pain due to bony metastases.
RADIONUCLIDE THERAPY FOR PALLIATION OF PAIN FROM BONY METASTASES Overview and Topics to Be Covered Reviews the use of radionuclide therapy in nuclear medicine for palliation of pain due to bony metastases.
Future Directions in Prostate Cancer: The Case for Protons. John J. Coen, MD Helen & Harry Gray Cancer Center
 Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Future Directions in Prostate Cancer: The Case for Protons John J. Coen, MD Helen & Harry Gray Cancer Center November 14, 2012 Protons and prostate cancer Early proton experience at the MGH The case for
Management of castrate resistant disease: after first line hormone therapy fails
 Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Management of castrate resistant disease: after first line hormone therapy fails Rob Jones Consultant in Medical Oncology Beatson Cancer Centre Glasgow Relevant Disclosure I have received research support
Your Guide to Prostate Cancer
 Your Guide to Prostate Cancer If you face a diagnosis of prostate cancer, what s next? We can help. A prostate cancer diagnosis can be overwhelming. The good news is that while prostate cancer can be serious,
Your Guide to Prostate Cancer If you face a diagnosis of prostate cancer, what s next? We can help. A prostate cancer diagnosis can be overwhelming. The good news is that while prostate cancer can be serious,
Denosumab (AMG 162) for bone metastases from solid tumours and multiple myeloma
 for bone metastases from solid tumours and multiple myeloma") Denosumab (AMG 162) for bone metastases from solid tumours and multiple myeloma September 2008 This technology summary is based on information available at the time of research and a limited literature
Denosumab (AMG 162) for bone metastases from solid tumours and multiple myeloma September 2008 This technology summary is based on information available at the time of research and a limited literature
18-Oct-16. Take home messages. An update for GPs on modern radiation therapy & hormones for prostate cancer. Session plan
 An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
An update for GPs on modern radiation therapy & hormones for prostate cancer A/Prof Jeremy Millar Director Radiation Oncology, Alfred Health Clinical lead Prostate Cancer Outcomes Registry, Monash University
Questions and Answers About Breast Cancer, Bone Metastases, & Treatment-Related Bone Loss. A Publication of The Bone and Cancer Foundation
 Questions and Answers About Breast Cancer, Bone Metastases, & Treatment-Related Bone Loss A Publication of The Bone and Cancer Foundation Contents This publication includes important information about
Questions and Answers About Breast Cancer, Bone Metastases, & Treatment-Related Bone Loss A Publication of The Bone and Cancer Foundation Contents This publication includes important information about
one patient advocacy group (Myeloma Canada) the submitter (Cancer Care Ontario Hematology Disease Site Group) the manufacturer (Janssen Inc.
 the submitter (Cancer Care Ontario Hematology Disease Site Group) the manufacturer (Janssen Inc.") perc noted that the pcodr Economic Guidance Panel s estimates of the use of bortezomib in both pre- ASCT and post-asct settings when compared with standard induction therapy and observation-only maintenance
perc noted that the pcodr Economic Guidance Panel s estimates of the use of bortezomib in both pre- ASCT and post-asct settings when compared with standard induction therapy and observation-only maintenance
Prostatectomy as salvage therapy. Cases. Paul Cathcart - Guy s & St Thomas NHS Trust, London
 Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Prostatectomy as salvage therapy Cases Paul Cathcart - Guy s & St Thomas NHS Trust, London Attributes of brachytherapy appeal to young men who place high utility on genitourinary function At risk of
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia
 Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
Does RT favor RP in long term Quality of Life? Juanita Crook MD FRCPC Professor of Radiation Oncology University of British Columbia Disclosures Advisory Board/honoraria: Varian Advisory Board: Breast
perc deliberated upon: a pcodr systematic review other literature in the Clinical Guidance Report providing clinical context
 require close monitoring. perc noted that induction therapy is generally administered in-hospital while consolidation therapy is administered on an out-patient basis. Because of the potential for serious
require close monitoring. perc noted that induction therapy is generally administered in-hospital while consolidation therapy is administered on an out-patient basis. Because of the potential for serious
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
The Rise, Fall, and Rise Again of Proton Therapy or Never count out a well-financed therapy
 The Rise, Fall, and Rise Again of Proton Therapy or Never count out a well-financed therapy Anthony Zietman MD Shipley Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School
The Rise, Fall, and Rise Again of Proton Therapy or Never count out a well-financed therapy Anthony Zietman MD Shipley Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School
Comparison of Futility Monitoring Methods Using RTOG Clinical Trials. Q. Ed Zhang, PhD
 Comparison of Futility Monitoring Methods Using RTOG Clinical Trials Q. Ed Zhang, PhD 1 Futility Monitoring Definition: Monitoring for early determination that trial results will not be in favor of H 1
Comparison of Futility Monitoring Methods Using RTOG Clinical Trials Q. Ed Zhang, PhD 1 Futility Monitoring Definition: Monitoring for early determination that trial results will not be in favor of H 1
Table 1 Standards and items to set up a PCU: general requirements and critical mass
 Table 1 Standards and items to set up a PCU: general requirements and critical mass General requirements and European Prostate Cancer Units are structures managing sufficient volumes of patients with on-site
Table 1 Standards and items to set up a PCU: general requirements and critical mass General requirements and European Prostate Cancer Units are structures managing sufficient volumes of patients with on-site
Medical Treatments for Prostate Cancer
 Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
Medical Treatments for Prostate Cancer Ian F Tannock MD, PhD Daniel E Bergsagel Professor of Medical Oncology, Princess Margaret Hospital and University of Toronto March 17, 2005 Brampton 1 A hypothetical
Lung Cancer Radiotherapy
 Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Lung Cancer Radiotherapy Indications, Outcomes, and Impact on Survivorship Care Malcolm Mattes, MD Assistant Professor WVU Department of Radiation Oncology When people think about radiation, they think
Isotopes and Palliative Radiotherapy for bone metastases
 Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
Isotopes and Palliative Radiotherapy for bone metastases Rationale for Bone-seeking Isotope Therapies in Prostate Cancer > 90% of patients with advanced prostate cancer have bone metastases which can be
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY
 BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
BIOCHEMICAL RECURRENCE POST RADICAL PROSTATECTOMY AZHAN BIN YUSOFF AZHAN BIN YUSOFF 2013 SCENARIO A 66 year old man underwent Robotic Radical Prostatectomy for a T1c Gleason 4+4, PSA 15 ng/ml prostate
Radiotherapy physics & Equipments
 Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
Radiotherapy physics & Equipments RAD 481 Lecture s Title: An Overview of Radiation Therapy for Health Care Professionals Dr. Mohammed Emam Vision :IMC aspires to be a leader in applied medical sciences,
ISSUE BRIEF Conference on Clinical Cancer Research November 2014
 ISSUE BRIEF Conference on Clinical Cancer Research November 2014 Introduction Considerations for Summary Review of Supplemental NDA/BLA Submissions in Oncology Rachel Sherman, Principal, Drug and Biological
ISSUE BRIEF Conference on Clinical Cancer Research November 2014 Introduction Considerations for Summary Review of Supplemental NDA/BLA Submissions in Oncology Rachel Sherman, Principal, Drug and Biological
Challenging Cases. With Q&A Panel
 Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
Challenging Cases With Q&A Panel Case Studies Index Patient #1 Jeffrey Wieder, MD Case # 1 72 year old healthy male with mild HTN Early 2011: Preop bone scan and pelvic CT = no mets Radical prostatectomy
FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS
 Tel: +27-21-9494060 Fax: +27-21-9494112 E-mail: leon.gouws@cancercare.co.za FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS 1. EXTERNAL BEAM RADIATION... 2 2. PLANNING OF TREATMENT... 2 3. DELIVERY
Tel: +27-21-9494060 Fax: +27-21-9494112 E-mail: leon.gouws@cancercare.co.za FEE RULES RADIATION ONCOLOGY FEE SCHEDULE CONTENTS 1. EXTERNAL BEAM RADIATION... 2 2. PLANNING OF TREATMENT... 2 3. DELIVERY
FOR PATIENTS DIAGNOSED WITH EARLY-STAGE PROSTATE CANCER. Discover a test that can help you on your treatment journey
 FOR PATIENTS DIAGNOSED WITH EARLY-STAGE PROSTATE CANCER Discover a test that can help you on your treatment journey Jim G. Oncotype DX GPS patient navigating prostate cancer since 2014 Not all prostate
FOR PATIENTS DIAGNOSED WITH EARLY-STAGE PROSTATE CANCER Discover a test that can help you on your treatment journey Jim G. Oncotype DX GPS patient navigating prostate cancer since 2014 Not all prostate
Overview of Radiotherapy for Clinically Localized Prostate Cancer
 Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Session 16A Invited lectures: Prostate - H&N. Overview of Radiotherapy for Clinically Localized Prostate Cancer Mack Roach III, MD Department of Radiation Oncology UCSF Helen Diller Family Comprehensive
Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018)
 Test Content Outline (Effective 2018)") Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018) I. Coordination of Care - 26% A. Breast health, screening, early detection, risk assessment and reduction 1. Issues related to
Certified Breast Care Nurse (CBCN ) Test Content Outline (Effective 2018) I. Coordination of Care - 26% A. Breast health, screening, early detection, risk assessment and reduction 1. Issues related to
New research in prostate brachytherapy
 New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
New research in prostate brachytherapy Dr Ann Henry Associate Professor in Clinical Oncology University of Leeds and Leeds Cancer Centre PIVOTAL boost opening 2017 To evaluate - The benefits of pelvic
Otis W. Brawley, MD, MACP, FASCO, FACE
 Otis W. Brawley, MD, MACP, FASCO, FACE Chief Medical and Scientific Officer American Cancer Society Professor of Hematology, Medical Oncology, Medicine and Epidemiology Emory University Atlanta, Georgia
Otis W. Brawley, MD, MACP, FASCO, FACE Chief Medical and Scientific Officer American Cancer Society Professor of Hematology, Medical Oncology, Medicine and Epidemiology Emory University Atlanta, Georgia
Performance Outcome Measures: A Regulatory Perspective
 Performance Outcome Measures: A Regulatory Perspective International Society for Pharmacoeconomics and Outcomes Research (ISPOR) May 18, 2015 Ashley F. Slagle, MS, PhD Study Endpoints and Labeling Development
Performance Outcome Measures: A Regulatory Perspective International Society for Pharmacoeconomics and Outcomes Research (ISPOR) May 18, 2015 Ashley F. Slagle, MS, PhD Study Endpoints and Labeling Development
Transformational cancer centre design supports the implementation of disruptive technologies
 European Healthcare Design 2018 Transformational cancer centre design supports the implementation of disruptive technologies Catherine Zeliotis 11 th June navigating change in healthcare design Bow River,
European Healthcare Design 2018 Transformational cancer centre design supports the implementation of disruptive technologies Catherine Zeliotis 11 th June navigating change in healthcare design Bow River,
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
Can you bring these to the attention of the committee when it meets. I hope to be there, and will gladly talk the committee trough them.
 L Jeremy Powell NICE By Email 17 th Aug 2011 Dear Jeremy, Thank you for the opportunity to contribute to this TA. I have forwarded to NICE the necessary paperwork including our comment form. I have a number
L Jeremy Powell NICE By Email 17 th Aug 2011 Dear Jeremy, Thank you for the opportunity to contribute to this TA. I have forwarded to NICE the necessary paperwork including our comment form. I have a number
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE
 Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
Prostate Cancer UK Best Practice Pathway: ACTIVE SURVEILLANCE Low risk localised PSA < 10 ng/ml and Gleason score 6, and clinical stage T1 - T2a Intermediate risk localised PSA 10-20 ng/ml, or Gleason
X, Y and Z of Prostate Cancer
 X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
X, Y and Z of Prostate Cancer Dr Tony Michele Medical Oncologist Prostate cancer Epidemiology Current EUA (et al) guidelines on Advanced Prostate Cancer Current clinical management in specific scenarios
SYNOPSIS PROTOCOL N UC-0107/1602
 SYNOPSIS PROTOCOL N UC-0107/1602 A) TRIAL IDENTIFICATION SPONSOR PROTOCOL CODE NUMBER: UC-0107/1602 VERSION (NR & DATE): 0.1, MARCH 2016 TRIAL TITLE: Extracranial Stereotactic Body Radiation Therapy (SBRT)
SYNOPSIS PROTOCOL N UC-0107/1602 A) TRIAL IDENTIFICATION SPONSOR PROTOCOL CODE NUMBER: UC-0107/1602 VERSION (NR & DATE): 0.1, MARCH 2016 TRIAL TITLE: Extracranial Stereotactic Body Radiation Therapy (SBRT)
Use of radiation to kill diseased cells. Cancer is the disease that is almost always treated when using radiation.
 Radiation Therapy Use of radiation to kill diseased cells. Cancer is the disease that is almost always treated when using radiation. One person in three will develop some form of cancer in their lifetime.
Radiation Therapy Use of radiation to kill diseased cells. Cancer is the disease that is almost always treated when using radiation. One person in three will develop some form of cancer in their lifetime.
8/2/2018. Acknowlegements: TCP SPINE. Disclosures
 A Presentation for the AAPM Annual meeting, Aug 2, 2018 Nashville, TN Stereotactic Radiosurgery for Spinal Metastases: Tumor Control Probability Analyses and Recommended Reporting Standards for Future
A Presentation for the AAPM Annual meeting, Aug 2, 2018 Nashville, TN Stereotactic Radiosurgery for Spinal Metastases: Tumor Control Probability Analyses and Recommended Reporting Standards for Future
Page 1. Helical (Spiral) Tomotherapy. UW Helical Tomotherapy Unit. Helical (Spiral) Tomotherapy. MVCT of an Anesthetized Dog with a Sinus Tumor
 Tomotherapy. UW Helical Tomotherapy Unit. Helical (Spiral) Tomotherapy. MVCT of an Anesthetized Dog with a Sinus Tumor") Helical (Spiral) Tomotherapy Novel Clinical Applications of IMRT Linac Ring Gantry CT Detector X-Ray Fan Beam Binary Multileaf Collimator Binary MLC Leaves James S Welsh, MS, MD Department of Human Oncology
Helical (Spiral) Tomotherapy Novel Clinical Applications of IMRT Linac Ring Gantry CT Detector X-Ray Fan Beam Binary Multileaf Collimator Binary MLC Leaves James S Welsh, MS, MD Department of Human Oncology
MSCC CARE PATHWAYS & CASE STUDIES. By Michael Balloch Spine CNS
 MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
MSCC CARE PATHWAYS & CASE STUDIES By Michael Balloch Spine CNS Aims To be familiar with the routes of MSCC prentaion How the guidelines work in practice Routes of presentation Generic intervention Managing
ANZUP SURVEILLANCE RECOMMENDATIONS FOR METASTATIC TESTICULAR CANCER POST-CHEMOTHERAPY
 ANZUP SURVEILLANCE RECOMMENDATIONS FOR METASTATIC TESTICULAR CANCER POST-CHEMOTHERAPY Note: These surveillance recommendations are provided as recommendations only. Clinicians should take into account
ANZUP SURVEILLANCE RECOMMENDATIONS FOR METASTATIC TESTICULAR CANCER POST-CHEMOTHERAPY Note: These surveillance recommendations are provided as recommendations only. Clinicians should take into account
Date Modified: May 29, Clinical Quality Measures for PQRS
 Date Modified: May 29, 2014 Clinical Quality s for PQRS # Domain Type Denominator Numerator Denominator Exclusions/Exceptions Rationale QCDR-1 QCDR-2 Patient Safety 102 Efficiency and Cost Reduction QCDR-3
Date Modified: May 29, 2014 Clinical Quality s for PQRS # Domain Type Denominator Numerator Denominator Exclusions/Exceptions Rationale QCDR-1 QCDR-2 Patient Safety 102 Efficiency and Cost Reduction QCDR-3
Advanced Prostate Cancer. November Jose W. Avitia, M.D
 Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
Advanced Prostate Cancer November 4 2017 Jose W. Avitia, M.D In 2017 161,000 new cases of prostate cancer diagnosed in US, mostly with elevated PSA 5-10% will present with metastatic disease In 2017: 26,000
NICE BULLETIN Diagnosis & treatment of prostate cancer
 Diagnosis & treatment of prostate cancer NICE provided the content for this booklet which is independent of any company or product advertised Diagnosis and treatment of prostate cancer Introduction In
Diagnosis & treatment of prostate cancer NICE provided the content for this booklet which is independent of any company or product advertised Diagnosis and treatment of prostate cancer Introduction In
Initial Hormone Therapy
 Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
Initial Hormone Therapy Alan Horwich Institute of Cancer Research and Royal Marsden Hospital, London, UK Alan.Horwich@icr.ac.uk MANAGEMENT OF PROSTATE CANCER Treatment windows Subclinical Localised PSA
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 /
 METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
METASTATIC PROSTATE CANCER MANAGEMENT K I R U B E L T E F E R A M. D. T R I H E A LT H C A N C E R I N S T I T U T E 0 1 / 3 1 / 2 0 1 8 Prostate Cancer- Statistics Most common cancer in men after a skin
The Selenium and Vitamin E Prevention Trial
 The largest-ever-prostate cancer prevention trial is now underway. The study will include a total of 32,400 men and is sponsored by the National Cancer Institute and a network of researchers known as the
The largest-ever-prostate cancer prevention trial is now underway. The study will include a total of 32,400 men and is sponsored by the National Cancer Institute and a network of researchers known as the
ASCO Publishes "Top Five" List of Opportunities to Improve Quality and Value in Cancer Care
 Published on ASCO (https://www.asco.org) Home > ASCO Publishes "Top Five" List of Opportunities to Improve Quality and Value in Cancer Care ASCO Publishes "Top Five" List of Opportunities to Improve Quality
Published on ASCO (https://www.asco.org) Home > ASCO Publishes "Top Five" List of Opportunities to Improve Quality and Value in Cancer Care ASCO Publishes "Top Five" List of Opportunities to Improve Quality
Metastatic Disease of the Proximal Femur
 CASE REPORT Metastatic Disease of the Proximal Femur WI Faisham, M.Med{Ortho)*, W Zulmi, M.S{Ortho)*, B M Biswal, MBBS** 'Department of Orthopaedic, "Department of Oncology and Radiotherapy, School of
CASE REPORT Metastatic Disease of the Proximal Femur WI Faisham, M.Med{Ortho)*, W Zulmi, M.S{Ortho)*, B M Biswal, MBBS** 'Department of Orthopaedic, "Department of Oncology and Radiotherapy, School of
Radiation Therapy for Prostate Cancer. Resident Dept of Urology General Surgery Grand Round November 24, 2008
 Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Radiation Therapy for Prostate Cancer Amy Hou,, MD Resident Dept of Urology General Surgery Grand Round November 24, 2008 External Beam Radiation Advances Improving Therapy Generation of linear accelerators
Multiple Sclerosis. What is multiple sclerosis? What is the cause? What are the symptoms?
 What is multiple sclerosis? Multiple Sclerosis Multiple sclerosis (MS) is a disease of the central nervous system (the brain and spinal cord). Many people with multiple sclerosis are only mildly affected
What is multiple sclerosis? Multiple Sclerosis Multiple sclerosis (MS) is a disease of the central nervous system (the brain and spinal cord). Many people with multiple sclerosis are only mildly affected
Panel One: Alternative Trial Designs Based on Tumor Genetics/Pathway Characteristics
 Panel One: Alternative Trial Designs Based on Tumor Genetics/Pathway Characteristics Alternative Trial Designs Based on Tumor Genetics and/or Pathway Characteristics Instead of Histology George D. Demetri,
Panel One: Alternative Trial Designs Based on Tumor Genetics/Pathway Characteristics Alternative Trial Designs Based on Tumor Genetics and/or Pathway Characteristics Instead of Histology George D. Demetri,
Impact of pre-treatment symptoms on survival after palliative radiotherapy An improved model to predict prognosis?
 Impact of pre-treatment symptoms on survival after palliative radiotherapy An improved model to predict prognosis? Thomas André Ankill Kämpe 30.05.2016 MED 3950,-5 year thesis Profesjonsstudiet i medisin
Impact of pre-treatment symptoms on survival after palliative radiotherapy An improved model to predict prognosis? Thomas André Ankill Kämpe 30.05.2016 MED 3950,-5 year thesis Profesjonsstudiet i medisin
Recognition & Treatment of Malignant Spinal Cord Compression Study Day
 Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
Recognition & Treatment of Malignant Spinal Cord Compression Study Day 16 th October 2014 Dr Bernie Foran Consultant Clinical Oncologist & Honorary Senior Lecturer Weston Park Hospital Outline of Talk
FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE. Geoffrey S. Ibbott, Ph.D. June 20, 2017
 FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE Geoffrey S. Ibbott, Ph.D. June 20, 2017 1 DISCLOSURES My institution holds Strategic Partnership Research Agreements with Varian, Elekta, and Philips
FROM ICARO1 TO ICARO2: THE MEDICAL PHYSICS PERSPECTIVE Geoffrey S. Ibbott, Ph.D. June 20, 2017 1 DISCLOSURES My institution holds Strategic Partnership Research Agreements with Varian, Elekta, and Philips
Update on Management of Malignant Spinal Cord Compression. Heino Hugel Consultant in Palliative Medicine University Hospital Aintree
 Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
Update on Management of Malignant Spinal Cord Compression Heino Hugel Consultant in Palliative Medicine University Hospital Aintree Current Guidelines The symptoms of MSCC may be subtle and therefore careful
BY PEGGY EASTMAN BETHESDA, MD A multidisciplinary panel of independent experts has concluded in a draft statement that
 Advertisement Wolters Kluwer Health Logo Login Register Subscribe etoc Help Enter Keywords Search Advanced Search Saved Searches HomePrevious IssuesBlogsCollectionsCEPodcastsInfo & Services Home > Blogs
Advertisement Wolters Kluwer Health Logo Login Register Subscribe etoc Help Enter Keywords Search Advanced Search Saved Searches HomePrevious IssuesBlogsCollectionsCEPodcastsInfo & Services Home > Blogs
Bringing prostate cancer education to regional and rural Australian communities
 Bringing prostate cancer education to regional and rural Australian communities Julie Sykes 1, Lisa Fodero 2, Nick Brook 3, Rachel Jenkin 4 1 Prostate Cancer Foundation of Australia; 2 Health Consult;
Bringing prostate cancer education to regional and rural Australian communities Julie Sykes 1, Lisa Fodero 2, Nick Brook 3, Rachel Jenkin 4 1 Prostate Cancer Foundation of Australia; 2 Health Consult;