Management of Chronic Pain in Children. Objectives: Common Myths about Pain. University of Texas Health Science Center at San Antonio, Texas
|
|
|
- Alberta Singleton
- 6 years ago
- Views:
Transcription


1 Management of Chronic Pain in Children I have no disclosures. Glen Medellin, MD Cure sometimes, treat often, comfort always. Hippocrates Objectives: The number of children admitted with chronic pain has increased by 831% from 2004 to Describe the pain pathway and pathophysiology of pain control 2. Recognize and categorize pain in children 3. Develop an individualized pain management plan for children with chronic pain Coffelt T A et al. Pediatrics 2013;132:e422-e by American Academy of Pediatrics Common Myths about Pain Children do not feel pain to the same degree as adults. It is not possible to adequately measure pain in cognitively impaired patients. Physicalmanifestations of pain are more important than self report measurements. Pain does not exist in the absence of detectable tissue damage. Pain without an obvious source is usually psychogenic. Common Myths about Pain The same stimulus produces the same degree of pain in all individuals. Analgesic therapy should not be started until the cause of pain is established. Use of opioids causes all patients to become addicted to them. Aggressive pain management is synonymous with prescribing opioids. 1





2 General Principles of Pain Management Assessment of pain in children must be tailored to the child's developmental stage. The gold standard of pain measurement is patient self report. Trust of health care practitioners is critical to obtaining honest reports of pain from children. Trust is achieved by urgent and effective responses to reports of pain. It is important to ask the child about pain regularly and document and reassess the child's pain following an intervention. Storey P, Knight CF. UNIPAC Eight: The Hospice/Palliative Medicine Approach. The Hospice/Palliative Medicine Approach to Caring for Pediatric Patients. Larchmont, NY: Mary Ann Liebert, Inc; 2003 General Principles of Pain Management Physiologic indicators, such as changes in pulse or blood pressure, may not be reliable indicators of pain in a chronically or critically ill child. Behavioral indicators, such as facial grimacing or crying, are unreliable and may be absent in the presence of chronic pain or critical illness. Children who have pain may use play or sleep as coping mechanisms; these behaviors do not mean the child is free of pain. Storey P, Knight CF. UNIPAC Eight: The Hospice/Palliative Medicine Approach. The Hospice/Palliative Medicine Approach to Caring for Pediatric Patients. Larchmont, NY: Mary Ann Liebert, Inc; 2003 Pain Pathway Transduction Transmission Modulation Perception Gate Control Theory Endogenous ability to reduce or increase the degree of perceived pain Gate located in the dorsal horn of the spinal cord. Acts on signals from the ascending and descending systems and weighs all of the inputs. Can be opened or closed by pharmacologic manipulation, transduction, transmission and modulation, and psychological intervention. 2







3 Pain Assessment Pain assessment is NOT a one time phenomenon. Joint Commission standards: pain is considered d to be the fifth vital sign and should be assessed initially and reassessed on a scheduled and regular basis. Individualized Numeric Rating Scale MILD MODERATE SEVERE Reposition Check tubes/equip Change loction Cuddle/Comfort Tylenol/Ibuprofen Bathe Massage Heating Pad Opioid Distraction ER Opioid increased dose 3




4 Neuropathic Pain Pain due to damaged or dysfunctional nerves Both peripheral and central mechanisms: Changes in the dorsal horn after nerve injury include reorganization Modulation in sensory input Enlargement of the second order neuron s receptive field Alteration in opioid receptivity Central Sensitization Excessive nociceptive nerve signals bombarding the central nervous system from the periphery long term changes occur in the central nervous system persistent amplification of pain signals. Dysfunctional pain Pain and abnormal sensitivity not associated with noxious stimulus, tissue damage, inflammation, or identifiable lesion to the nervous system. Includes fibromyalgia, tension type headaches, migraines, and irritable bowel syndrome. High prevalence of associated co morbid conditions. Dysfunctional Pain Need to help patient understand that persistent pain signals do not indicate ongoing tissue damage. This belief results in fear of movement, physical activity, and the future. It may be necessary to educate the patient that pain does not equal harm and that appropriate physical activity is important. 4

 Irritable bladder Pain Team Treatment is with")
5 Fibromyalgia Patients often believe that medicine has a cure for their problems. For many, accepting that chronic pain can be treated but not necessarily cured is a gradual process. Encouragement to continue to be engaged in life as pain is being managed and not wait for a cure is often necessary. Patients typically present with the following complaints: Chronic widespread muscular pain Chronic fatigue Widespread tenderness (hyperalgesia) Many people with fibromyalgia also experience additional symptoms, such as the following: Morning stiffness Headaches Irritable bowel syndrome Cognitive and memory problems (often called fibro fog ) Irritable bladder Pain Team Treatment is with analgesics and usually includes an antidepressant. Pregabalin has shown to be effective in treating some patients with fibromyalgia. Exercise programs, analgesics, and behavioral therapy. AVOID use of opioids. Anesthesiologists Clergy Complementary and Alternative Medicine Specialists Neurologists Nurses Physical Medicine and Rehabilitation Specialists Physical or Occupational Therapists Psychiatrists Psychologists Social Workers Referral to a Mental Health Professional Suicidal ideation with or without intent or plan Anergia Persistent anhedonia L f tit Loss of appetite Sleep disturbance Anxiety or panic Prolonged difficulty accepting the condition Angry outbursts toward self or others 5
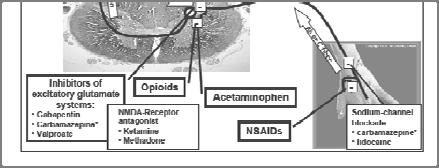
6 WHO Principles for Pharmacological Management Use a two step strategy Dose at regular intervals by the clock Use the appropriate route of administration i i by the mouth Adapt treatment to the individual child by the individual No Pain WHO two step strategy Mild Acetaminophen and ibuprofen are the medicines of choice. Moderate to Severe Morphine is the medicine of choice, although other strong opioids should ldbe considered and made available to ensure an alternative to morphine in case of intolerable sideeffects. Acetaminophen NSAIDS Also known as paracetamol A nonsteroidal anti inflammatory drug with potent antipyretic and analgesic actions but with very weak anti inflammatory inflammatory activity. Lacks the typical actions of NSAIDs, such as antiplatelet activity and gastrotoxicity Can be administered intravenously NSAIDs are particularly good for bone pain and incident pain, or the type of pain that is provoked by activity (e.g., walking). All types of pain may respond to NSAIDs; however, visceral pain is probably less responsive than somatic pain, and neuropathic pain is often unresponsive. Ketorolac and ibuprofen can be given intravenously. Opioids Opioid analgesics are considered to be a mainstay in the treatment of moderate to severe pain that does not respond to non opioids alone, because they: Are effective, Are fairly easy to titrate, Have a favorable risk to benefit ratio. Opioids Opioids can exhibit their analgesic effects by acting on both peripheral and central mu, kappa, and delta opioid receptors. Inhibit the transmission of nociceptive input from theperipheryto to thespinal cord Activate the inhibitory pathways that modulate transmission Alters limbic system activity. May also work peripherally in areas of inflammation 6


7 The Language of Analgesia Opioid vs. Narcotic Medication vs. Drug Addiction Addiction is a chronic neurobiologic disease with genetic, psychosocial, and environmental influences. It is characterized by impaired control over drug use compulsive use continued use despite harm need to use for effects other that pain relief craving Tolerance Process of decreasing effect of a drug over time, requiring increased dose to achieve same level of efficacy Can be evident after a few days of treatment First indication decrease in duration of analgesia, then decrease in analgesic effect Not always the reason for need for dose escalation, should consider differential diagnosis Tolerance Easily overcome by up titrating opioid Should not withhold opioid for fear of producing tolerance or reaching dose beyond which no further analgesia can be achieved Tolerance to non analgesic side effects does occur Physical dependence Physical dependence is a physiologic adaptation that occurs in patients receiving opioid analgesics. Characterized by the development of withdrawal symptoms when a medication is stopped or decreased abruptly Expected in patients receiving opioid analgesics for more than a few days. Withdrawal can be avoided by tapering the dose when discontinuing treatment. 7

.")
8 Pseudoaddiction A term used to describe behavior that appears to be addictive, drug seeking behavior, but is actually an effort to obtain pain relief by a nonaddicted patient who is not receiving adequate analgesia. Opioid Side Effects Constipation Pruritus Sedation Nausea and vomiting Urinary retention Mental clouding Addiction Myoclonus Respiratory depression. Opioid induced Nausea Dopamine blocking agents Prochlorperazine Haloperidol Metoclopramide 5 HT3 receptor antagonists ondansetron Myoclonus Sudden unexpected repetitive, but nonrhythmic jerks of unrelated muscle groups. Treatment approach consists of : opioid idrotation tti if possible suppressed with a number of agents (baclofen, valproic acid, clonazepam, gabapentin). Opioid induced Hyperalgesia Refers to a phenomenon whereby opioid administration results in a lowering of pain threshold, clinically manifested as apparent opioid tolerance, worsening pain despite accelerating opioid doses, and abnormal pain symptoms. 8


9 Respiratory Depression Opioids typically produce a concentrationdependent shift in the carbon dioxide response curve. When this shift becomes great enough, clinical expression of respiratory depression occurs, usually as a decrease in respiratory rate. Usually with clinically appropriate doses, compensation occurs, and respiratory rate does not decline. Coding event In the event of a cardiorespiratory event, a patient s response may be exaggerated due to the presence of opioid concentrations in the bloodstream. Even in the absence of clinical signs, there may still be residual effects on respiratory reserve after tolerance develops, and this must be kept in mind with patients on chronic opioids. Naloxone Overly aggressive administration of naloxone in a patient on chronic opioid therapy can cause severe withdrawal syndrome. Children and patients who weigh less than 40 kg should have 0.1 mg of naloxone diluted in 10 ml of saline to make a 10 mcg/ml solution, given at 0.5 mcg/kg every 2 minutes. Morphine Gold standard for moderate or severe pain Schedule 2 controlled substance Codeine WHO does not recommend its use. US FDA Black Box warning for use after Tonsillectomy ihl ibl b li k i li bl Highly variable metabolism makes it unreliable Up to 30% children poor metabolizers. Some children are ultra rapid metabolizers. Active metabolite is morphine. 9


10 Hydrocodone Only available in combination with acetaminophen or ibuprofen Schedule 3 controlled substance makes it easierto prescribe Preferred over codeine Fentanyl Patch can be used in some cancer and chronic non malignant pain Patches are not for opioid naïve children Sustained release Opioids Children often cannot swallow pills Even lowest dosages of sustained release products may be too high for children High ihrates of gastrostomy tubes in pediatric i palliative care population necessitate liquid formulations Methadone Used in chronic pain Long half life therefore longer time to steady state Should not be used for breakthrough hpain Has NMDA receptor activity Only liquid long acting formulation Tramadol Tramadol is unique in that it has a dual mechanism of action. weak agonist at the mu opioid receptor inhibits reuptake of norepinephrine and serotonin inhibits reuptake of norepinephrine and serotonin Tramadol is typically used for mild to moderate pain WHO does not recommend for children 10




11 Ajuvants Antidepressants amitriptyline, nortriptyline Anticonvulsants valproic acid, phenytoin Anxiolytics benzodiazepines Corticosteroids dexamethasone Anesthetics lidocaine, ketamine Gabapentinoids gabapentin, pregabalin Alpha agonist clonidine, guanfacine SNRI duloxetine Corticosteroids Often used in palliative care, where they have a number of beneficial effects, including pain reduction, improved appetite weight gain antiemetic action mood elevation. Steroids are used in the treatment of neuropathic pain due to cord compression, brachial or lumbosacral plexus invasion, or peripheral nerve infiltration. Anticonvulsants Used for some neuropathic pain conditions to relieve lancinating or stabbing pain. Suppress discharge in pathologically altered neurons, thus inhibiting neural hyperexcitability Tricyclic Antidepressants Useful agents for neuropathic pain, cancer pain, and nonneuropathic pain with certain symptoms (e.g., insomnia, depression, or visceral spasm). Suppress pain signaling through local anestheticlike effects at sodium channels in neural membranes. Inhibit reuptake of norepinephrine, serotonin, and dopamine at synapses, which may increase their analgesic effects, as well as improve mood favorably. Ketamine Acts at the NMDA receptor excitatory glutamatergic receptor present spinal and supraspinal In chronic pain states prolonged nociceptive stimulation causes activation and upregulation of the NMDAR at dorsal horn synapses resulting in enhanced and amplified trafficking of pain signals to the brain (central sensitization). 11





12 Useful Resources WHO guidelines on the pharmacological treatment of persisting pain in children with medical illnesses, int/publications/2012/ _Guidelines.pdf The PainEDU Manual A Pocket Guide to Pain Management,
Choose a category. You will be given the answer. You must give the correct question. Click to begin.
 Instructions for using this template. Remember this is Jeopardy, so where I have written Answer this is the prompt the students will see, and where I have Question should be the student s response. To
Instructions for using this template. Remember this is Jeopardy, so where I have written Answer this is the prompt the students will see, and where I have Question should be the student s response. To
CHAPTER 4 PAIN AND ITS MANAGEMENT
 CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
Acute Pain NETP: SEPTEMBER 2013 COHORT
 Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
Acute Pain NETP: SEPTEMBER 2013 COHORT Pain & Suffering an unpleasant sensory & emotional experience associated with actual or potential tissue damage, or described in terms of such damage International
UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14. Cynthia Kim and Stephen Wilson
 UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14 Cynthia Kim and Stephen Wilson Rules Buzz first and player answers If answer correct, then the player asks teammates if they want to keep
UCSF Pediatric Hospital Medicine Boot Camp Pain Session 6/21/14 Cynthia Kim and Stephen Wilson Rules Buzz first and player answers If answer correct, then the player asks teammates if they want to keep
Pain Assessment & Management. For General Nursing Orientation
 Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
Pain Assessment & Management For General Nursing Orientation April 2012 Overview Definition of pain Barriers to effective pain management Types of pain Objective pain assessment Approaches to management
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS
 POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
POST OPERATIVE PAIN MANAGEMENT: PAIN AND COMPLICATIONS November 9, 2018 Aimee LaMere, CNP Molly McNaughton, CNP Leslie Weide, MSW, LICSW, ACM Disclosures: Conflict of interest statement: We certify that,
10/08/59 PAIN IS THE MOST COMMON TREATABLE SYMPTOM OF CANCER CURRENT EVIDENCE BASED CONCEPTS: MANAGEMENT OF CANCER PAIN PAIN AN UNMET CLINICAL NEED IN
 Pain is a frequent complication of cancer, and is common in many other life-limiting illnesses MANAGEMENT OF CANCER PAIN A/Prof Ghauri Aggarwal FRACP, FAChPM, FFPMANZCA Palliative Medicine Physician Sydney
Pain is a frequent complication of cancer, and is common in many other life-limiting illnesses MANAGEMENT OF CANCER PAIN A/Prof Ghauri Aggarwal FRACP, FAChPM, FFPMANZCA Palliative Medicine Physician Sydney
OPIOIDS AND NON-CANCER PAIN
 Ch05.qxd 1/6/04 4:33 PM Page 77 CHAPTER 5 OPIOIDS AND NON-CANCER PAIN Background 78 Side-effects of opioids 78 Tolerance, physical dependence and addiction 79 Opioid-induced pain 79 Practical issues 80
Ch05.qxd 1/6/04 4:33 PM Page 77 CHAPTER 5 OPIOIDS AND NON-CANCER PAIN Background 78 Side-effects of opioids 78 Tolerance, physical dependence and addiction 79 Opioid-induced pain 79 Practical issues 80
Pain Management Strategies Webinar/Teleconference
 Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Pain Management Strategies Webinar/Teleconference Barry K. Baines, MD April 16, 2009 Objectives Describe the principles of pain management. Identify considerations in the use of opioids. Describe the benefits
Nociceptive Pain. Pathophysiologic Pain. Types of Pain. At Presentation. At Presentation. Nonpharmacologic Therapy. Modulation
 Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
Learning Objectives Effective, Safe Analgesia An Approach to Appropriate Outpatient Chronic Pain Treatment By the end of this presentation, participants will be able to: Identify multiple factors that
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK
 GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
GUIDELINES AND AUDIT IMPLEMENTATION NETWORK General Palliative Care Guidelines The Management of Pain at the End Of Life November 2010 Aim To provide a user friendly, evidence based guide for the management
Narcotic Analgesics. Jacqueline Morgan March 22, 2017
 Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
Narcotic Analgesics Jacqueline Morgan March 22, 2017 Pain Unpleasant sensory and emotional experience with actual or potential tissue damage Universal, complex, subjective experience Number one reason
SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP)
") 9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
9 SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF CHRONIC NON-TERMINAL PAIN (CNTP) SUMMARY OF ARIZONA OPIOID PRESCRIBING GUIDELINES FOR THE TREATMENT OF ACUTE PAIN NONOPIOID TREATMENTS
Neuropathic Pain in Palliative Care
 Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Neuropathic Pain in Palliative Care Neuropathic Pain in Advanced Cancer Affects 40% of patients Multiple concurrent pains are common Often complex pathophysiology with mixed components Nocioceptive Neuropathic
Knock Out Opioid Abuse in New Jersey:
 Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Knock Out Opioid Abuse in New Jersey: A Resource for Safer Prescribing GUIDELINE FOR PRESCRIBING OPIOIDS FOR CHRONIC PAIN IMPROVING PRACTICE THROUGH RECOMMENDATIONS CDC s Guideline for Prescribing Opioids
Pain control in Cancer patients. Dr Ali Shoeibi, Assistant Professor of Neurology
 Pain control in Cancer patients Dr Ali Shoeibi, Assistant Professor of Neurology More than two thirds of patients with advanced cancer experience cancer pain Almost all pain can be controlled to some extent
Pain control in Cancer patients Dr Ali Shoeibi, Assistant Professor of Neurology More than two thirds of patients with advanced cancer experience cancer pain Almost all pain can be controlled to some extent
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES
 NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
NEUROPATHIC CANCER PAIN STANDARDS AND GUIDELINES GENERAL PRINCIPLES Neuropathic pain may be relieved in the majority of patients by multimodal management A careful history and examination are essential.
CHAPTER 4 PAIN AND ITS MANAGEMENT
 CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
CHAPTER 4 PAIN AND ITS MANAGEMENT Pain Definition: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Types of Pain
Spinal Cord Injury Pain. Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018
 Spinal Cord Injury Pain Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018 Objectives At the conclusion of this session, participants should be able to: 1. Understand the difference between nociceptive
Spinal Cord Injury Pain Michael Massey, DO CentraCare Health St Cloud, MN 11/07/2018 Objectives At the conclusion of this session, participants should be able to: 1. Understand the difference between nociceptive
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults
 SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
SCOPING DOCUMENT FOR WHO Treatment Guidelines on pain related to cancer, HIV and other progressive life-threatening illnesses in adults BACKGROUND The justification for developing these guidelines lies
16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces
 16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces Moderators: Kendra Grim, MD, Robert T. Wilder, MD, PhD Institution:
16 year old with Disabling Chest Wall Pain after Thoracoscopic Talc Pleurodesis for Treatment of Recurrent Spontaneous Pneumothoraces Moderators: Kendra Grim, MD, Robert T. Wilder, MD, PhD Institution:
Geriatric Pain Assessment and Management. Robin Arends, DNP, CNP, FNP-BC
 + Geriatric Pain Assessment and Management Robin Arends, DNP, CNP, FNP-BC + Objectives List three reasons why elderly are less likely to report pain. List three barriers to pain management Describe two
+ Geriatric Pain Assessment and Management Robin Arends, DNP, CNP, FNP-BC + Objectives List three reasons why elderly are less likely to report pain. List three barriers to pain management Describe two
Q&A: Opioid Prescribing for Chronic Non-Malignant Pain
 NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
NHS Hastings and Rother Clinical Commissioning Group Chair Dr David Warden Chief Officer Amanda Philpott NHS Eastbourne, Hailsham and Seaford Clinical Commissioning Group Chair Dr Martin Writer Chief Officer
Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN
 Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN Oncology Clinical Nurse Specialist, Senior Research Specialist City of Hope Definition of Pain Pain is an unpleasant sensory and emotional
Managing Pain after Transplant Denice Economou, RN,MN,CHPN,AOCN Oncology Clinical Nurse Specialist, Senior Research Specialist City of Hope Definition of Pain Pain is an unpleasant sensory and emotional
Corporate Medical Policy
 Corporate Medical Policy Intravenous Anesthetics for the Treatment of Chronic Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intravenous_anesthetics_for_the_treatment_of_chronic_pain
Corporate Medical Policy Intravenous Anesthetics for the Treatment of Chronic Pain File Name: Origination: Last CAP Review: Next CAP Review: Last Review: intravenous_anesthetics_for_the_treatment_of_chronic_pain
Pain Management in Older Adults. Mary Shelkey, PhD, ARNP
 Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
Pain Management in Older Adults Mary Shelkey, PhD, ARNP Cause of Death/ Demographic and Social Trends Early 1900s Current Medicine's Focus Comfort Cure Cause of Death Infectious Diseases/ Communicable
PAIN & ANALGESIA. often accompanied by clinical depression. fibromyalgia, chronic fatigue, etc. COX 1, COX 2, and COX 3 (a variant of COX 1)
") Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Pain - subjective experience associated with detection of tissue damage ( nociception ) acute - serves as a warning chronic - nociception gone bad often accompanied by clinical depression fibromyalgia,
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008
 Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Associate Professor Supranee Niruthisard Department of Anesthesiology Faculty of Medicine Chulalongkorn University January 21, 2008 PAIN MECHANISMS Somatic Nociceptive Visceral Inflammatory response sensitizes
Pain management in Paediatric Palliative Care. Dr Jane Nakawesi 14 th August 2017
 Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
Pain management in Paediatric Palliative Care Dr Jane Nakawesi 14 th August 2017 Content Management of pain in children Non pharmacological Pharmacological Exit level outcomes The participants will: Know
1/21/14. Cancer Related Pain: Case-Based Pharmacology. Conflicts of Interest. Learning Objective
 Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Related Pain: Case-Based Pharmacology Jeannine M. Brant, PhD, APRN, AOCN Oncology Clinical Nurse Specialist Nurse Scientist Billings Clinic Conflicts of Interest Jeannine Brant has served on the
Cancer Pain. Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center
 Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
Cancer Pain Suresh K Reddy, MD,FFARCS The University of Texas MD Anderson Cancer Center Prevalence of the Most Common Symptoms in Advanced Cancer (1000 Adults) Symptom % Symptom % Pain 82 Lack of Energy
If Not Opioids then LEAH EDMONDS CSHP OCTOBER 26, 2017
 If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
If Not Opioids then what LEAH EDMONDS CSHP OCTOBER 26, 2017 Disclosure Nothing to disclose Objectives Identify various non-opioid options for the treatment of chronic non cancer pain Choose appropriate
PAIN TERMINOLOGY TABLE
 PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
PAIN TERMINOLOGY TABLE TERM DEFINITION HOW TO USE CLINICALLY Acute Pain Pain that is usually temporary and results from something specific, such as a surgery, an injury, or an infection Addiction A chronic
Learning Objectives. Perioperative goals. Acute Pain in the Chronic Pain Patient for Ambulatory Surgery 9/8/16
 Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Acute Pain in the Chronic Pain Patient for Ambulatory Surgery Danielle Ludwin, MD Associate Professor of Anesthesiology Division of Regional and Orthopedic Anesthesia Columbia University Medical Center
Overview of Essentials of Pain Management. Updated 11/2016
 0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
0 Overview of Essentials of Pain Management Updated 11/2016 1 Overview of Essentials of Pain Management 1. Assess pain intensity on a 0 10 scale in which 0 = no pain at all and 10 = the worst pain imaginable.
Analgesia for Patients with Substance Abuse Disorders. Lisa Jennings CN November 2015
 Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Analgesia for Patients with Substance Abuse Disorders Lisa Jennings CN November 2015 Definitions n Addiction: A pattern of drug use characterised by aberrant drug-taking behaviours & the compulsive use
Cancer patients at End-of-Life: Multidimensional Pain Requiring Multimodal Therapy
 Cancer patients at End-of-Life: Multidimensional Pain Requiring Multimodal Therapy Presented by: Marsha Farrell BSN, RN-BC, CHPN Pathways to Success Conference by the Bay November 12, 2014 Conflict of
Cancer patients at End-of-Life: Multidimensional Pain Requiring Multimodal Therapy Presented by: Marsha Farrell BSN, RN-BC, CHPN Pathways to Success Conference by the Bay November 12, 2014 Conflict of
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I. Mr.D.Raju,M.pharm, Lecturer
 Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Analgesic Drugs PHL-358-PHARMACOLOGY AND THERAPEUTICS-I Mr.D.Raju,M.pharm, Lecturer Mechanisms of Pain and Nociception Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to
Understanding pain and mental illness Impact on management principles
 Understanding pain and mental illness Impact on management principles Chris Alderman Consultant Psychopharmacologist Pain and mental illness - context PAIN MENTAL ILLNESS OTHER FACTORS (personality, history.
Understanding pain and mental illness Impact on management principles Chris Alderman Consultant Psychopharmacologist Pain and mental illness - context PAIN MENTAL ILLNESS OTHER FACTORS (personality, history.
DISCLAIMER: ECHO Nevada emphasizes patient privacy and asks participants to not share ANY Protected Health Information during ECHO clinics.
 DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
DISCLAIMER: Video will be taken at this clinic and potentially used in Project ECHO promotional materials. By attending this clinic, you consent to have your photo taken and allow Project ECHO to use this
Pain and its Treatments. Our Goals: Understand: What is pain and what causes it? 2. What are different types of pain? 3. How do opioid drugs work?
 Pain and its Treatments Cheryl Stucky, Ph.D. Medical College of Wisconsin Our Goals: Understand: 1. What is pain and what causes it? 2. What are different types of pain? 3. How do opioid drugs work? What
Pain and its Treatments Cheryl Stucky, Ph.D. Medical College of Wisconsin Our Goals: Understand: 1. What is pain and what causes it? 2. What are different types of pain? 3. How do opioid drugs work? What
Pain. November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine
 Internal Medicine, Palliative Medicine") Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
Pain November 1, 2006 Dr. Jana Pilkey MD, FRCP(C) Internal Medicine, Palliative Medicine Objectives To be able to define pain To be able to evaluate pain To be able to classify types of pain To learn appropriate
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY
 GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
GUIDELINES ON PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional
Palliative and Hospice Care of the Terminally Ill Introduction
 Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
Palliative and Hospice Care of the Terminally Ill Introduction There has been an increase in life expectancy for men and women of all races to 77.6 years Leading causes of death in older patients are chronic
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment
 an informational booklet for opioid pain treatment") ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
ten questions you might have about tapering (and room for your own) an informational booklet for opioid pain treatment This booklet was created to help you learn about tapering. You probably have lots
Pharmacology of Pain Transmission and Modulation
 Pharmacology of Pain Transmission and Modulation 2 Jürg Schliessbach and Konrad Maurer Nociceptive Nerve Fibers Pain is transmitted to the central nervous system via thinly myelinated Aδ and unmyelinated
Pharmacology of Pain Transmission and Modulation 2 Jürg Schliessbach and Konrad Maurer Nociceptive Nerve Fibers Pain is transmitted to the central nervous system via thinly myelinated Aδ and unmyelinated
MANAGEMENT OF VISCERAL PAIN
 MANAGEMENT OF VISCERAL PAIN William D. Chey, MD, FACG Professor of Medicine University of Michigan 52 year old female with abdominal pain 5 year history of persistent right sided burning/sharp abdominal
MANAGEMENT OF VISCERAL PAIN William D. Chey, MD, FACG Professor of Medicine University of Michigan 52 year old female with abdominal pain 5 year history of persistent right sided burning/sharp abdominal
Acute pain management in opioid tolerant patients. Muhammad Laklouk
 Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Acute pain management in opioid tolerant patients Muhammad Laklouk General principles An adequate review and assessment Provision of effective analgesia (including attenuation of tolerance and hyperalgesia)
Pain. Fears and Facts. What is pain? Factors that Affect People with Pain. Symptom Management
 Symptom Management Pain Pain is an unpleasant physical or emotional experience. While not all cancer patients will experience pain, approximately two thirds of patients will have pain at some point during
Symptom Management Pain Pain is an unpleasant physical or emotional experience. While not all cancer patients will experience pain, approximately two thirds of patients will have pain at some point during
Pain CONCERN. Medicines for long-term pain. Antidepressants
 Pain CONCERN Medicines for long-term pain Antidepressants Many people living with long-term pain (also known as chronic or persistent pain) are worried about using medicines like antidepressants. They
Pain CONCERN Medicines for long-term pain Antidepressants Many people living with long-term pain (also known as chronic or persistent pain) are worried about using medicines like antidepressants. They
The pain of it all. Rod MacLeod MNZM. Hibiscus Hospice, Auckland and University of Auckland
 The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
The pain of it all Rod MacLeod MNZM Hibiscus Hospice, Auckland and University of Auckland Definition of PAIN An unpleasant sensory and emotional experience which we primarily associate with tissue damage
Prescribing drugs of dependence in general practice, Part C
 HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
HO O Prescribing drugs of dependence in general practice, Part C Key recommendations and practice points for management of pain with opioid therapy H H HO N CH3 Acute pain Acute pain is an unpleasant sensory
PAIN MANAGEMENT IN UROLOGY
 24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
24 PAIN MANAGEMENT IN UROLOGY F. Francesca (chairman), P. Bader, D. Echtle, F. Giunta, J. Williams Eur Urol 2003; 44(4):383-389 Introduction Pain is defined as an unpleasant sensory and emotional experience
Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014
 Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014 Overview Types of Pain Physical Examination of Pain Pharmacologic Approach in Pain Management
Practical Pain Management Leah Centanni, MSN, FNP-C, Asst. Clinical Professor CANP Conference March 22, 2014 Overview Types of Pain Physical Examination of Pain Pharmacologic Approach in Pain Management
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE SCOPE
 NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Neuropathic pain pharmacological management: the pharmacological management of neuropathic pain in adults in non-specialist
NATIONAL INSTITUTE FOR HEALTH AND CLINICAL EXCELLENCE 1 Guideline title SCOPE Neuropathic pain pharmacological management: the pharmacological management of neuropathic pain in adults in non-specialist
Rational Polypharmacy
 Rational Polypharmacy Thomas B. Gregory, PharmD, BCPS, CPE, FASPE Disclosures Clinical advisory board: Daiichi Sankyo 1 Introduction Cox Health Ambulatory Pain Clinic Pharmacy Specialist Learning Objectives
Rational Polypharmacy Thomas B. Gregory, PharmD, BCPS, CPE, FASPE Disclosures Clinical advisory board: Daiichi Sankyo 1 Introduction Cox Health Ambulatory Pain Clinic Pharmacy Specialist Learning Objectives
BACKGROUND Measuring renal function :
 A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A GUIDE TO USE OF COMMON PALLIATIVE CARE DRUGS IN RENAL IMPAIRMENT These guidelines bring together information and recommendations from the Palliative Care formulary (PCF5 ) BACKGROUND Measuring renal
A PATIENT GUIDE FOR MANAGING PAIN
 A PATIENT GUIDE FOR MANAGING PAIN PAIN MANAGEMENT Knowing the Facts Pain can be controlled. Pain is common after surgery and with many types of illnesses. Most patients with acute and chronic pain can
A PATIENT GUIDE FOR MANAGING PAIN PAIN MANAGEMENT Knowing the Facts Pain can be controlled. Pain is common after surgery and with many types of illnesses. Most patients with acute and chronic pain can
21 st June BDS BASHD Therapeutics Pain and Analgesia. BASHD Therapeutics Analgesics and Pain Management. Links to other BASHD content
 Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
Volume of Prescribing by Dentists 2011 ( a reminder) BASHD Therapeutics Analgesics and Pain Management Analgesics account for 1 in 80 dental prescriptions made A lot more analgesics will be suggested for
The Fifth Vital Sign.
 Recognizing And Monitoring The Painful Patient Susan Clark, LVT, VTS(ECC) The Fifth Vital Sign. Pain control is part of the accepted standard of care in veterinary medicine. The ability to recognize the
Recognizing And Monitoring The Painful Patient Susan Clark, LVT, VTS(ECC) The Fifth Vital Sign. Pain control is part of the accepted standard of care in veterinary medicine. The ability to recognize the
Palliative Prescribing - Pain
 Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Palliative Prescribing - Pain LAURA BARNFIELD 21/2/17 Aims To understand the classes of painkillers available in palliative care To gain confidence in counselling regarding opiates To gain confidence prescribing
Practical Management Of Osteoporosis
 Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
Practical Management Of Osteoporosis CONFERENCE 2012 Education Centre, Bournemouth.19 November The following companies have given funding towards the cost of this meeting but have no input into the agenda
PART VI: TAPERING OPIOIDS ROBERT JENKINSON MD MARCH 7, 2018
 PART VI: TAPERING OPIOIDS ROBERT JENKINSON MD MARCH 7, 2018 TAPERING OPIOIDS GETTING STARTED ON OPIOIDS IS EASY BUT GETTING PATIENTS OFF IS HARD WE ARE ARE OBLIGED TO TAPER PATIENTS DOWN AND OFF OPIOIDS
PART VI: TAPERING OPIOIDS ROBERT JENKINSON MD MARCH 7, 2018 TAPERING OPIOIDS GETTING STARTED ON OPIOIDS IS EASY BUT GETTING PATIENTS OFF IS HARD WE ARE ARE OBLIGED TO TAPER PATIENTS DOWN AND OFF OPIOIDS
IMPROVING CHRONIC PAIN PATIENTS QUALITY OF LIFE WITH CUTTING EDGE TECHNOLOGY. Jacqueline Weisbein, DO Napa Valley Orthopaedic Medical Group
 IMPROVING CHRONIC PAIN PATIENTS QUALITY OF LIFE WITH CUTTING EDGE TECHNOLOGY Jacqueline Weisbein, DO Napa Valley Orthopaedic Medical Group Who Am I? Avid equestrian Trained in Physical Medicine & Rehabilitation
IMPROVING CHRONIC PAIN PATIENTS QUALITY OF LIFE WITH CUTTING EDGE TECHNOLOGY Jacqueline Weisbein, DO Napa Valley Orthopaedic Medical Group Who Am I? Avid equestrian Trained in Physical Medicine & Rehabilitation
9/30/2017. Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management. Program Objectives. Impact of Poorly Managed Pain
 Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
Case Study: Complete Pain Assessment and Multimodal Approach to Pain Management MARY BETH PARTYKA MSN ADULT NURSE PRACTITIONER ADVOCATE CHRIST MEDICAL CENTER ADULT PAIN SERVICE Program Objectives Identify
PRESCRIBING PRACTICE IN DELIRIUM. John Warburton Critical Care Pharmacist
 PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PRESCRIBING PRACTICE IN DELIRIUM John Warburton Critical Care Pharmacist Learning outcomes Modifiable medication risk factors for delirium An appreciation of contributing factors modifiable with medicines
PAIN MANAGEMENT & MAXIMIZING QUALITY OF LIFE DURING TREATMENT
 PAIN MANAGEMENT & MAXIMIZING QUALITY OF LIFE DURING TREATMENT Brandy Ficek, MD Medical Director of Quality of Life and Palliative Medicine Cancer Treatment Centers of America Rocky Mountain Blood Cancer
PAIN MANAGEMENT & MAXIMIZING QUALITY OF LIFE DURING TREATMENT Brandy Ficek, MD Medical Director of Quality of Life and Palliative Medicine Cancer Treatment Centers of America Rocky Mountain Blood Cancer
Steven Richeimer, M.D.
 Steven Richeimer, M.D. Associate Professor of Anesthesiology & Psychiatry Chief, Division of Pain Medicine Keck School of Medicine, USC Los Angeles, CA 323-442-6202 www.helpforpain.com Pain Light touch
Steven Richeimer, M.D. Associate Professor of Anesthesiology & Psychiatry Chief, Division of Pain Medicine Keck School of Medicine, USC Los Angeles, CA 323-442-6202 www.helpforpain.com Pain Light touch
Prescription Pain Management. University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D
 Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
Prescription Pain Management University of Hawai i Hilo Pre- Nursing Program NURS 203 General Pharmacology Danita 1 Narciso Pharm D 2 Objectives Understand how to preform a pain assessment Know which medications
BASICS OF OPIOID PRESCRIBING 10:30-11:45AM
 PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
PROVIDING QUALITY CARE TO PAIN PATIENTS IN IOWA BASICS OF OPIOID PRESCRIBING 10:30-11:45AM ACPE UAN: 107-000-14-013-L01-P Activity Type: Application-Based 0.125 CEU/1.25hr Learning Objectives for Pharmacists:
New Guidelines for Prescribing Opioids for Chronic Pain
 New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
New Guidelines for Prescribing Opioids for Chronic Pain Andrew Lowe, Pharm.D. CAPA Meeting October 6, 2016 THE EPIDEMIC Chronic Pain and Prescription Opioids 11% of Americans experience daily (chronic)
Inpatient Management of Trauma Related Pain
 Inpatient Management of Trauma Related Pain STOMP Summit September 9, 2016 Ann O Rourke, MD, MPH University of Wisconsin Department of Surgery 1 Our patient Small SDH Intubated Hemopneumothorax with multiple
Inpatient Management of Trauma Related Pain STOMP Summit September 9, 2016 Ann O Rourke, MD, MPH University of Wisconsin Department of Surgery 1 Our patient Small SDH Intubated Hemopneumothorax with multiple
A Pain Management Primer for Pharmacists. Jessica Geiger-Hayes, PharmD, BCPS, CPE Andrea Wetshtein, PharmD, BCPS, CPE
 A Pain Management Primer for Pharmacists Jessica Geiger-Hayes, PharmD, BCPS, CPE Andrea Wetshtein, PharmD, BCPS, CPE Objectives Discuss the differences between somatic, visceral, and neuropathic pain Design
A Pain Management Primer for Pharmacists Jessica Geiger-Hayes, PharmD, BCPS, CPE Andrea Wetshtein, PharmD, BCPS, CPE Objectives Discuss the differences between somatic, visceral, and neuropathic pain Design
Acute Pain Management in the Opioid Tolerant Patient. Objectives. Opioids. The participant will be able to define opioid tolerance
 Acute Pain Management in the Opioid Tolerant Patient Kathleen M. Colfer, MSN, RN-BC Clinical Nurse Specialist Acute Pain Management Service Department of Anesthesiology Thomas Jefferson University Hospital
Acute Pain Management in the Opioid Tolerant Patient Kathleen M. Colfer, MSN, RN-BC Clinical Nurse Specialist Acute Pain Management Service Department of Anesthesiology Thomas Jefferson University Hospital
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST
 PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
PALLIATIVE TREATMENT BY DR. KHRONGKAMOL SIHABAN MEDICAL ONCOLOGIST TREATMENT IN ONCOLOGY Main treatment : surgery Neoadjuvant treatment : RT, CMT Adjuvant treatment : Tx micrometastatic disease -CMT,Targeted
Monte H. Moore, MD. Idaho Physical Medicine and Rehabilitation. Meridian, ID
 Monte H. Moore, MD Idaho Physical Medicine and Rehabilitation Meridian, ID Chronic pain brief review Opiates important things to know Factors in determining whether to use an opiate What to watch for if
Monte H. Moore, MD Idaho Physical Medicine and Rehabilitation Meridian, ID Chronic pain brief review Opiates important things to know Factors in determining whether to use an opiate What to watch for if
HOPE. Considerations. Considerations ISING. Safe Opioid Prescribing Guidelines for ACUTE Non-Malignant Pain
 Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Due to the high level of prescription drug use and abuse in Lake County, these guidelines have been developed to standardize prescribing habits and limit risk of unintended harm when prescribing opioid
Fibromyalgia: Current Trends and Concepts
 Fibromyalgia: Current Trends and Concepts Dr. Brian Kahan Fellow American Academy of Physical Medicine and Rehabilitation Diplomat American Academy of Pain Medicine American College of Rheumatology (ACR)
Fibromyalgia: Current Trends and Concepts Dr. Brian Kahan Fellow American Academy of Physical Medicine and Rehabilitation Diplomat American Academy of Pain Medicine American College of Rheumatology (ACR)
PAIN MANAGEMENT IN CHILDREN
 SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 PAIN MANAGEMENT IN CHILDREN Aziza Shad, MD Ellen Wasserman Chair of Pediatrics Chief, Division of Pediatric Hematology
SIOP PODC Supportive Care Education (ICON 2016) Presentation Date: 23 rd January 2016 PAIN MANAGEMENT IN CHILDREN Aziza Shad, MD Ellen Wasserman Chair of Pediatrics Chief, Division of Pediatric Hematology
Neuropathic Pain Treatment Guidelines
 Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
Neuropathic Pain Treatment Guidelines Background Pain is an unpleasant sensory and emotional experience that can have a significant impact on a person s quality of life, general health, psychological health,
Overview of Neuropathic pain
 Overview of Neuropathic pain Kongkiat Kulkantrakorn,M.D. Neurology division Thammasat University 1 Contents Overview of pain New concepts and mechanism Treatment options New data in management 2 3 Breaking
Overview of Neuropathic pain Kongkiat Kulkantrakorn,M.D. Neurology division Thammasat University 1 Contents Overview of pain New concepts and mechanism Treatment options New data in management 2 3 Breaking
Pain Management: Overview of A Practical Approach
 Pain Management: Overview of A Practical Approach Michael B. Potter, M.D. Department of Family and Community Medicine University of California, San Francisco What is Pain? An unpleasant sensory and emotional
Pain Management: Overview of A Practical Approach Michael B. Potter, M.D. Department of Family and Community Medicine University of California, San Francisco What is Pain? An unpleasant sensory and emotional
Renal Palliative Care Last Days of Life
 Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Renal Palliative Care Last Days of Life Introduction This guideline is an aid to clinical decision-making and good practice for patients with stage 4-5 chronic kidney disease (egfr
Fibromyalgia , The Patient Education Institute, Inc. id Last reviewed: 03/12/2017 1
 Fibromyalgia Introduction Fibromyalgia is a common condition that causes pain and fatigue in the muscles, joints, ligaments and tendons. Fibromyalgia affects about 3 to 6% of people worldwide. Fibromyalgia
Fibromyalgia Introduction Fibromyalgia is a common condition that causes pain and fatigue in the muscles, joints, ligaments and tendons. Fibromyalgia affects about 3 to 6% of people worldwide. Fibromyalgia
PAIN MANAGEMENT COMPETENCY
 PAIN MANAGEMENT COMPETENCY What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is always subjective.
PAIN MANAGEMENT COMPETENCY What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage. Pain is always subjective.
Analgesia in patients with impaired renal function Formulary Guidance
 Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
Analgesia in patients with impaired renal function Formulary Guidance Approved by Trust D&TC: January 2010 Revised March 2017 Contents Paragraph Page 1 Aim 4 2 Introduction 4 3 Assessment of renal function
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE?
 PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
PERIOPERATIVE PAIN MANAGEMENT: WHAT S UP WITH METHADONE? Sandra Z Perkowski, VMD, PhD, DACVAA University of Pennsylvania, School of Veterinary Medicine, Philadelphia, PA Pre-emptive and multimodal use
Pain. Christine Illingworth. Community Nurse St Luke s Hospice 17/5/17
 Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Christine Illingworth Community Nurse St Luke s Hospice 17/5/17 What is pain? Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage Pain is whatever
Pain Pathways. Dr Sameer Gupta Consultant in Anaesthesia and Pain Management, NGH
 Pain Pathways Dr Sameer Gupta Consultant in Anaesthesia and Pain Management, NGH Objective To give you a simplistic and basic concepts of pain pathways to help understand the complex issue of pain Pain
Pain Pathways Dr Sameer Gupta Consultant in Anaesthesia and Pain Management, NGH Objective To give you a simplistic and basic concepts of pain pathways to help understand the complex issue of pain Pain
Pain Management in the Elderly. Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN
 Pain Management in the Elderly Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN Objectives So How Much Do You Really Know? www.geriatricpain.org Geriatric Pain Knowledge Assessment The Geriatric
Pain Management in the Elderly Martha Watson, MS, APRN, GCNS Christie Bowser, RN-BC, RN Objectives So How Much Do You Really Know? www.geriatricpain.org Geriatric Pain Knowledge Assessment The Geriatric
E-Learning Module N: Pharmacological Review
 E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
E-Learning Module N: Pharmacological Review This Module requires the learner to have read Chapter 13 of the Fundamentals Program Guide and the other required readings associated with the topic. Revised:
Treating Pain and Depression
 Treating Pain and Depression Without Getting Depressed Joseph P, Arpaia, MD www.jparpaiamd.com More than 50% of patients with chronic pain also have clinically significant depression. Interestingly that
Treating Pain and Depression Without Getting Depressed Joseph P, Arpaia, MD www.jparpaiamd.com More than 50% of patients with chronic pain also have clinically significant depression. Interestingly that
Non-opioid and adjuvant pain management
 Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
Non-opioid and adjuvant pain management ALLISON JORDAN, MD, HMDC MEDICAL DIRECTOR OF PALLIATIVE CARE SERVICES CHRISTIAN AND ALTON MEMORIAL HOSPITALS ASSOCIATE MEDICAL DIRECTOR, BJC HOSPICE ASSISTANT PROFESSOR
July We hope that our tool will be a useful aid in your efforts to improve pain management in your setting. Sincerely, 7/14
 July 2014 he Knowledge and Attitudes Survey Regarding Pain tool can be used to assess nurses and other professionals in your setting and as a pre and post test evaluation measure for educational programs.
July 2014 he Knowledge and Attitudes Survey Regarding Pain tool can be used to assess nurses and other professionals in your setting and as a pre and post test evaluation measure for educational programs.
Syllabus. Questions may appear on any of the topics below: I. Multidimensional Nature of Pain
 Questions may appear on any of the topics below: I. Multidimensional Nature of Pain Syllabus A. Epidemiology 1. Pain as a public health problem with social, ethical, legal and economic consequences 2.
Questions may appear on any of the topics below: I. Multidimensional Nature of Pain Syllabus A. Epidemiology 1. Pain as a public health problem with social, ethical, legal and economic consequences 2.
Enhanced Community Palliative Support Services. Lynne Ghasemi St Luke s Hospice
 Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Enhanced Community Palliative Support Services Lynne Ghasemi St Luke s Hospice Learning Outcomes Define the different types of pain Describe the process of pain assessment Discuss pharmacological management
Complex Acute Surgical Pain Management. Thomas Baribeault MSN, CRNA
 Complex Acute Surgical Pain Management Thomas Baribeault MSN, CRNA Introduction Anatomy and pathophysiology of acute surgical pain Pharmacology Chronic pain patient Opioid tolerant patient Introduction
Complex Acute Surgical Pain Management Thomas Baribeault MSN, CRNA Introduction Anatomy and pathophysiology of acute surgical pain Pharmacology Chronic pain patient Opioid tolerant patient Introduction
Management of Pain. Agenda: Definitions Pathophysiology Analgesics
 C. Brian Warriner, MD, FRCPC Professor and Past Chair UBC Department of Anesthesiology, Pharmacology and Therapeutics brian.warriner@vch.ca Agenda: Definitions Pathophysiology Analgesics Gases(N 2 O) Opiates
C. Brian Warriner, MD, FRCPC Professor and Past Chair UBC Department of Anesthesiology, Pharmacology and Therapeutics brian.warriner@vch.ca Agenda: Definitions Pathophysiology Analgesics Gases(N 2 O) Opiates