SVS AVF Clinical Practice Guidelines Venous Ulcer
|
|
|
- Lora Palmer
- 6 years ago
- Views:
Transcription
1

2 Venous Ulcer SVS AVF Venous Ulcer Clinical Practice Guidelines Task Force Multispecialty committee members Thomas F. O Donnell, Jr., MD (Chair), Marc A. Passman, MD (Vice Chair), William A. Marston, MD, William J. Ennis, DO, Michael Dalsing, MD, Robert L. Kistner, MD, Fedor Lurie, MD, PhD, Peter K. Henke, MD, Monika L. Gloviczki, MD, PhD, BoG. Eklöf, MD, Julianne Stoughton, MD, SesadriRaju, MD, Cynthia K. Shortell, MD, Joseph D. Raffetto, MD, Hugo Partsch, MD Lori C. Pounds, MD, Mary E. Cummings, MD, David L. Gillespie, M.D., Robert B. McLafferty, MD, Mohammad Hassan Murad, MD, Thomas W. Wakefield, MD, Peter Gloviczki, MD Began review process April 2012 Publication August 2014 Journal of Vascular Surgery Supplement Endorsed by: American College of Phlebology Union Internationale de Phlébologie
3 Methodology Target audience - specialists who treat vascular disease and/or wounds. Methodology Subcommittee Structure Clinical Evaluation Wound Care Compression Surgery Ancillary Primary Prevention: Evidence Review Recommendations GRADE strength of recommendation / level of evidence Knowledge and Evaluations Research Unit at the Mayo Clinic, Rochester MN Corroborate proper strength of evidence and quality of evidence for each guideline Commissioned for systematic review: surgery/endovascular and compression
4 Grade 1A Description of Recommendation Strong recommendation, highquality evidence Benefit vs Risk Benefits clearly outweigh risk and burdens, or vice versa Methodological Quality of Supporting Evidence RCTs without important limitations or overwhelming evidence from observational studies Implications Strong recommendation, can apply to most patients in most circumstances without reservation 1B 1C 2A 2B 2C Strong recommendation, moderate quality evidence Strong recommendation, lowquality or very low-quality evidence Weak recommendation, high quality evidence Weak recommendation, moderate-quality evidence Weak recommendation, lowquality or very low-quality evidence Benefits clearly outweigh risk and burdens, or vice versa [BEST PRACTICE] Benefits clearly outweigh risk and burdens, or vice versa Benefits closely balanced with risks and burdens Benefits closely balanced with risks and burdens Uncertainty in the estimates of benefits and risk, and burdens; Risk, benefit, and burdens may be closely balanced RCTs with important limitations (inconsistent results, methodological flaws, indirect, or imprecise) or exceptionally strong evidence from observational studies Observational studies or case series RCTs with important limitations (inconsistent results, methodological flaws, indirect, or imprecise) or exceptionally strong evidence from observational studies Observational studies or case series Strong recommendation, can apply to most patients in most circumstances without reservation Strong recommendation but may change when higher quality evidence becomes available - Recommendation deemed necessary to provide a comprehensive guideline that encompasses all the details RCTs without important needed for providing limitations care for or patients overwhelming with venous ulcers evidence from observational - When there are no comparable alternatives to a studies recommendation, or evidence is lacking - Case series supplemented by the best opinion of a panel of experts Weak recommendation, best action may differ depending on circumstances or patients or societal values Weak recommendation, best action may differ depending on circumstances or patients or societal values Very weak recommendations; Other alternatives may be reasonable
5 Definition Venous Ulcer Guideline 1.1: Venous Leg Ulcer Definition We suggest use of a standard definition of venous ulcer as an open skin lesion of the leg or foot that occurs in an area affected by venous hypertension. [BEST PRACTICE]
6 Anatomy -Pathophysiology Guideline 2.1: Venous Anatomy Nomenclature We recommend use of the International Consensus Committee on Venous Anatomical Terminology for standardized venous anatomy nomenclature. [BEST PRACTICE] Guideline 2.2: Venous Leg Ulcer Pathophysiology We recommend a basic practical knowledge of venous physiology and venous leg ulcer pathophysiology for all practitioners caring for venous leg ulcers. [BEST PRACTICE]
7

8
9 Guideline 3.1: Clinical Evaluation Clinical Evaluation We recommend that for all patients with suspected leg ulcers fitting the definition of venous leg ulcer, clinical evaluation for evidence of chronic venous disease be performed. [BEST PRACTICE]
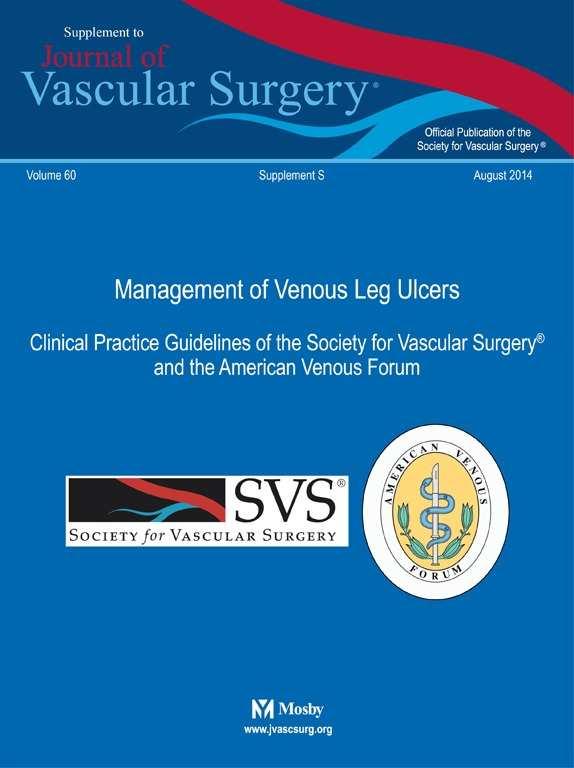
10 Clinical Evaluation Guideline 3.2: Nonvenous Causes Leg Ulcers We recommend identification of medical conditions that affect ulcer healing and other non-venous causes of ulcers. [BEST PRACTICE]
11
12 Clinical Evaluation -Wound Guideline 3.3: Wound Documentation We recommend serial venous leg ulcer wound measurement and documentation. [BEST PRACTICE] Guideline 3.4: Wound Culture We suggest against routine culture of venous leg ulcers and to only obtain wound cultures when clinical evidence of infection is present. [GRADE -2; LEVEL OF EVIDENCE -C] Guideline 3.5: Wound Biopsy We recommend wound biopsy for venous leg ulcers that do not improve with standard wound and compression therapy after 4-6 weeks of treatment and for all ulcers with atypical features. [GRADE -1 ; LEVEL OF EVIDENCE - C]
13 Clinical Evaluation -Arterial Guideline 3.7: Arterial Testing We recommend arterial pulse examination and measurement of ankle brachial index (ABI) on all patients with venous leg ulcer. [GRADE -1; LEVEL OF EVIDENCE -B] Guideline 3.8: Microcirculation Assessment We suggest against routine microcirculation assessment of venous leg ulcers, but suggest selective consideration as an adjunctive assessment for monitoring of advanced wound therapy. [GRADE -2; LEVEL OF EVIDENCE -C]
14 Clinical Evaluation Venous Imaging Guideline 3.9: Venous Duplex Ultrasound We recommend comprehensive venous duplex ultrasound examination of the lower extremity in all patients with suspected venous leg ulcer. [GRADE -1 ; LEVEL OF EVIDENCE -B] Guideline 3.10: Venous Plethysmography We suggest selective use of venous plethysmographyin the evaluation of patients with suspected venous leg ulcer if venous duplex ultrasound does not provided definitive diagnostic information. [GRADE -2; LEVEL OF EVIDENCE -B]
15 Clinical Evaluation Venous Imaging Guideline 3.11: Venous Imaging We suggest selective computed tomography venography, magnetic resonance venography, contrast venography, and/or intravascular ultrasound in patients with suspected venous leg ulceration if additional advanced venous diagnosis is required for thrombotic or non-thrombotic iliac vein obstruction, or for operative planning prior to open or endovenous venous interventions. [GRADE -2; LEVEL OF EVIDENCE - C]
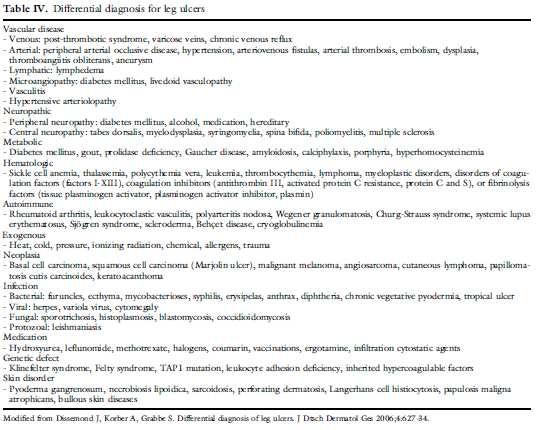
16 Clinical Evaluation Classification Guideline 3.12: Venous Disease Classification We recommend that all patients with venous leg ulcer should be classified based on venous disease classification assessment including clinical CEAP, revised venous clinical severity scoring (VCSS), and venous disease specific quality of life (QOL) assessment. [BEST PRACTICE]
17
18
19
20 Clinical Evaluation Venous Outcomes Guideline 3.13: Venous Procedural Outcome Assessment We recommend venous procedural outcome assessment including reporting of anatomic success, venous hemodyamicsuccess, procedure-related minor and major complications, and impact on venous leg ulcer healing. [BEST PRACTICE]
21 Wound Care -Categories Wound bed preparation Wound cleansers Debridement Surgical debridement Anesthesia for debridement Hydrosurgical debridement Ultrasonic debridement Enzymatic debridement Biologic debridement Nutritional assessment and management Measurement of wound progress Wound infection and bacterial control Wound culture Indications for culture Method of wound culture Management of limb cellulitis Wound colonization and bacterial biofilms Treatment of wound infection Topical antibiotics Systemic antibiotics Primary wound dressings Topical dressing selection Antimicrobials in topical dressings Peri-ulcer skin management Anti-inflammatory dressings Adjunctive wound therapies Indications for adjunctive therapies Split-thickness skin grafting Cellular Therapy Use of cellular therapy Preparation for cellular therapy Frequency of cellular therapy application Negative pressure therapy Electrical stimulation Ultrasound therapy
22 Wound Care -Cleansers Guideline 4.1: Wound Cleansers We suggest that venous leg ulcers be cleansed initially and at each dressing change using a neutral, nonirritating, nontoxic solution, performed with a minimum of chemical or mechanical trauma. [GRADE -2; LEVEL OF EVIDENCE -C]
23 Wound Care -Debridement Guideline 4.2: Debridement We recommend that venous leg ulcers receive thorough debridement at their initial evaluation to remove obvious necrotic tissue, excessive bacterial burden, and cellular burden of dead and senescent cells. [GRADE -1; LEVEL OF EVIDENCE -B] We suggest additional maintenance debridement be performed to maintain the appearance and readiness of the wound bed for healing. [GRADE -2; LEVEL OF EVIDENCE -B] We suggest that the health care provider choose from a number of debridement methods including sharp, enzymatic, mechanical, biological, or autolytic. More than one debridement method may be appropriate. [GRADE -2; LEVEL OF EVIDENCE -B]
24 Wound Care -Debridement Guideline 4.3: Anesthesia for Surgical Debridement We recommend that local anesthesia (topical or local injection) be administered to minimize discomfort associated with surgical venous leg ulcer debridement. In selected cases, regional block or general anesthesia may be required. [GRADE -1; LEVEL OF EVIDENCE -B]
25 Wound Care -Debridement Guideline 4.4: Surgical Debridement We recommend that surgical debridement be performed for venous leg ulcers with slough, non-viable tissue or eschar. Serial wound assessment is important in determining the need for repeat debridement(s). [GRADE -1; LEVEL OF EVIDENCE -B]
26 Wound Care -Debridement Guideline 4.5 Hydrosurgical Debridement We suggest hydrosurgicaldebridement as an alternative to standard surgical debridement of venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -B] Guideline 4.6: Ultrasonic Debridement We suggest against ultrasonic debridement over surgical debridement in the treatment of venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -C]
27 Wound Care -Debridement Guideline 4.7: Enzymatic Debridement We suggest enzymatic debridement of venous leg ulcers when no clinician trained in surgical debridement is available to debride the wound. [GRADE - 2; LEVEL OF EVIDENCE -C] We do not suggest enzymatic debridement over surgical debridement. [GRADE -2; LEVEL OF EVIDENCE -C] Guideline 4.8: Biologic Debridement We suggest larval therapy for venous leg ulcers can be used as an alternative to surgical debridement. [GRADE -2; LEVEL OF EVIDENCE -B]
28 Wound -Infection Guideline 4.9: Management of Limb Cellulitis We recommend that cellulitis (inflammation and infection of the skin and subcutaneous tissue) surrounding the venous leg ulcer be treated with systemic gram-positive antibiotics. [GRADE -1; LEVEL OF EVIDENCE -B] Guideline 4.10: Wound Colonization and Bacterial Biofilms We suggest against systemic antimicrobial treatment of venous leg ulcer colonization or biofilm without clinical evidence of infection. [GRADE -2; LEVEL OF EVIDENCE -C]
29 Wound -Infection Guideline 4.11: Treatment of Wound Infection: We suggest that venous leg ulcers with >1x10 6 CFU/g of tissue and clinical evidence of infection should be treated with antimicrobial therapy. [GRADE -2; LEVEL OF EVIDENCE C] We suggest antimicrobial therapy for virulent or difficult to eradicate bacteria (such as beta hemolytic streptococci, pseudomonas, and resistant staphylococalspecies) at lower levels of CFU/g of tissue. [GRADE -2; LEVEL OF EVIDENCE C] We suggest a combination of mechanical disruption and antibiotic therapy as most likely to be successful in eradicating venous leg ulcer infection. [GRADE -2; LEVEL OF EVIDENCE C]
30 Wound Care -Infection Guideline 4.12: Systemic Antibiotics We recommend that venous leg ulcers with clinical evidence of infection be treated with systemic antibiotics guided by sensitivities performed on wound culture. [GRADE -1; LEVEL OF EVIDENCE -C] Oral antibiotics are preferred initially and the duration of antibiotic therapy should be limited to 2 weeks unless persistent evidence of wound infection is present. [GRADE - 1; LEVEL OF EVIDENCE -C] Guideline 4.13: Topical Antibiotics for Infected Wounds We suggest against using topical antimicrobials agents for the treatment of infected venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE C]
31 Wound Care -Dressings Guideline 4.14: Topical Dressing Selection We suggest applying a topical dressing that will manage venous leg ulcer exudate and maintain a moist warm wound bed. [GRADE -2; LEVEL OF EVIDENCE -C] We suggest selection of a primary wound dressing that will absorb wound exudate produced by the ulcer (alginates, foams) and protect the peri-ulcer skin. [GRADE -2; LEVEL OF EVIDENCE -B]
32 Wound Care -Dressings Guideline 4.15: Topical Dressings Containing Antimicrobials We recommend against the routine use of topical antimicrobial containing dressings in the treatment of non-infected venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -A] Guideline 4.16: Peri-Ulcer Skin Management We suggest application of skin lubricants underneath compression in order to reduce dermatitis that commonly affects peri-ulcer skin. [GRADE -2; LEVEL OF EVIDENCE -C] In severe cases of dermatitis associated with venous leg ulcers, we suggest topical steroids to reduce the development of secondary ulcerations and to reduce the symptoms of dermatitis. [GRADE - 2; LEVEL OF EVIDENCE -C]
33 Wound Care Anti-inflammatory Guideline 4.17: Anti-Inflammatory Therapies We suggest against using anti-inflammatory therapies for the treatment of venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -C]
34 Wound Care Adjuvant Therapy Guideline 4.18: Indications for Adjuvant Therapies We recommend adjuvant wound therapy options for venous leg ulcers that fail to demonstrate improvement after a minimum of 4-6 weeks standard wound therapy. [GRADE -1; LEVEL OF EVIDENCE -B]
35 Wound Care Skin Graft Guideline 4.19: Split Thickness Skin Grafting We suggest against split thickness skin grafting as primary therapy in treatment of venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -B] We suggest split thickness skin grafting with continued compression for selected large venous leg ulcers that have failed to show signs of healing with standard care for 4-6 weeks. [GRADE -2; LEVEL OF EVIDENCE -B]
36 Wound Care Cellular Therapy Guideline 4.20: Cellular Therapy We suggest the use of cultured allogeneic bilayer skin replacements (with both epidermal and dermal layers) to increase the chances for healing patients in patients with difficult to heal venous leg ulcers in addition to compression therapy in patients that have failed to show signs of healing after standard therapy for 4-6 weeks. [GRADE -2; LEVEL OF EVIDENCE -A]
37 Wound Care Cellular Therapy Guideline 4.21: Preparation for Cellular Therapy We suggest a therapeutic trial of appropriate compression and wound bed moisture control prior to application of cellular therapy. [GRADE -2; LEVEL OF EVIDENCE -C] We recommend that prior to the application of a bilayered cellular graft that adequate wound bed preparation be completed including complete removal of slough, debris and any necrotic tissue. [GRADE -1; LEVEL OF EVIDENCE -C] We recommend additional evaluation and management of increased bio-burden levels prior to the application of cellular therapy. [GRADE -1; LEVEL OF EVIDENCE -C]
38 Guideline 4.22: Frequency of Cellular Therapy Application We suggest re-application of cellular therapy as long as the venous leg ulcer continues to respond based on wound documentation. [GRADE -2; LEVEL OF EVIDENCE -C]
39 Wound Care Tissue Substitutes Guideline 4.23: Tissue Matrices, Human Tissues or Other Skin Substitutes We suggest the use of a porcine small intestinal submucosaltissue construct in addition to compression therapy for the treatment of venous leg ulcers that have failed failedto show signs of healing after standard therapy for 4-6 weeks.. [Grade 2; Level of Evidence B]
40 Wound Care Additional Therapy Guideline 4.24: Negative Pressure Therapy We suggest against routine primary use of negative pressure wound therapy for venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -C] Guideline 4.25: Electrical Stimulation We suggest against electrical stimulation therapy for venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -C] Guideline 4.26: Ultrasound Therapy We suggest against routine ultrasound therapy for venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -B]
41 Compression Healing/Recurrence Guideline 5.1: Compression Ulcer Healing In a patient with a venous leg ulcer, we recommend compression therapy over no compression therapy to increase venous leg ulcer healing rate. [GRADE -1; LEVEL OF EVIDENCE -A] Guideline 5.2: Compression Ulcer Recurrence In a patient with a healed venous leg ulcer, we suggest compression therapy to decrease the risk of ulcer recurrence. [GRADE -2; LEVEL OF EVIDENCE -B]
42 Compression Multi-Component Guideline 5.3: Multi-Component Compression Bandage We suggest the use of multi-component compression bandage over single component bandages for the treatment of venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -B]
43 Compression Arterial Insufficiency Guideline 5.4: Compression Arterial Insufficiency In a patient with a venous leg ulcer and underlying arterial disease, we do not suggest compression bandages or stockings if ABI is 0.5 or less or if absolute ankle pressure is less than 60mmHg. [GRADE -2; LEVEL OF EVIDENCE -C]
44 Compression Intermittent Pneumatic Guideline 5.5: Intermittent Pneumatic Compression We suggest using intermittent pneumatic compression (IPC) when other compression options are not available, cannot be used, or have failed to aid in venous leg ulcer healing after prolonged compression therapy. [GRADE - 2; LEVEL OF EVIDENCE -C]
45 Operative / Endovascular -Algorithm Venous Ulcer Diagnostics + reflux obstruction + perforator + superficial similar risk/benefit: Less risk + proximal Rx Endo (open) *** Failed/ not option Reevaluate + Superficial/perforator Deep reflux Valvular reconstruction Rx Endo Failed/ not option Reevaluate + proximal + infrainguinal Bypass unilateral +/- +/+ -/+ Bypass/ endophlebectomy *** clarification: +/+ ulcer treat both, no ulcer treat only superficial similar risk/benefit: Moderate risk Not option/ Reevaluate Bypass bilateral Highest risk
46 Operative / Endovascular -Superficial Guideline 6.1 Superficial Venous Reflux and Active Venous Leg Ulcer Ulcer Healing In a patient with a venous leg ulcer (C6) and incompetent superficial veins that have axial reflux directed to the bed of the ulcer, we suggest ablation of the incompetent veins in addition to standard compressive therapy to improve ulcer healing. [GRADE -2; LEVEL OF EVIDENCE -C] Guideline 6.2 Superficial Venous Reflux and Active Venous Leg Ulcer Prevent Recurrence In a patient with a venous leg ulcer (C6) and incompetent superficial veins that have axial reflux directed to the bed of the ulcer, we recommend ablation of the incompetent veins in addition to standard compressive therapy to prevent recurrence. [GRADE -1; LEVEL OF EVIDENCE-B]
47 Operative / Endovascular -Superficial Guideline 6.3 Superficial Venous Reflux and Healed Venous Leg Ulcer In a patient with a healed venous leg ulcer (C5) and incompetent superficial veins that have axial reflux directed to the bed of the ulcer, we recommend ablation of the incompetent veins in addition to standard compressive therapy to prevent recurrence. [GRADE -1; LEVEL OF EVIDENCE -C] Guideline 6.4: Superficial Venous Reflux with Skin Changes at Risk for Venous Leg Ulcer (C4b): In a patient with skin changes at risk for venous leg ulcer (C4b) and incompetent superficial veins that have axial reflux directed to the bed of the affected skin, we suggest ablation of the incompetent superficial veins in addition to standard compressive therapy to prevent ulceration. [GRADE -2; LEVEL OF EVIDENCE C]
48 Operative / Endovascular -Perforator Guideline 6.5:Combined Superficial / Perforator Venous Reflux With or Without Deep Venous Reflux and Active Venous Leg Ulcer. In a patient with a venous leg ulcer (C6) and incompetent superficial veins that have reflux to the ulcer bed in addition to pathologic perforating veins (outward flow of >500 msecduration, with a diameter of >3.5mm) located beneath or associated with the ulcer bed, we suggest ablation of both the incompetent superficial veins and perforator veins in addition to standard compressive therapy to aid in ulcer healing and prevent recurrence. [GRADE -2; LEVEL OF EVIDENCE -C]
49 Operative / Endovascular -Perforator Guideline 6.6:Combined Superficial and Perforator Venous Reflux With or Without Deep Venous Disease and Skin Changes at Risk for Venous Leg Ulcer (C4b) or Healed Venous Ulcer (C5) In a patient with skin changes at risk for venous leg ulcer (C4b) or healed venous ulcer (C5) and incompetent superficial veins that have reflux to the ulcer bed in addition to pathologic perforating veins (outward flow of >500 msecduration, with a diameter of >3.5mm) located beneath or associated with the healed ulcer bed, we suggest ablation of the incompetent superficial veins to prevent the development or recurrence of a venous leg ulcer. [GRADE -2; LEVEL OF EVIDENCE -C] Treatment of the incompetent perforating veins can be performed simultaneously with correction of axial reflux or can be staged with re-evaluation of perforator veins for persistent incompetence after correction of axial reflux. [GRADE -2; LEVEL OF EVIDENCE -C]
50 Operative / Endovascular -Perforator Guideline 6.7:Pathologic Perforator Venous Reflux in the Absence of Superficial Venous Disease, With or Without Deep Venous Reflux, and a Healed or Active Venous Ulcer: In a patient with isolated pathologic perforator veins (outward flow of >500 msecduration, with a diameter of >3.5mm) located beneath or associated with the healed (C5) or active ulcer (C6) bed regardless of the status of the deep veins, we suggest ablation of the pathologic perforating veins in addition to standard compression therapy to aid in venous ulcer healing and to prevent recurrence. [GRADE -2; LEVEL OF EVIDENCE -C]
51 Operative / Endovascular -Perforator Guideline 6.8: Treatment Alternatives for Pathologic Perforator Veins For those patients who would benefit from pathologic perforator vein ablation, we recommend treatment by percutaneous techniques that include ultrasound guided sclerotherapyor endovenousthermal ablation (radiofrequency or laser) over open venous perforator surgery to eliminate the need for incisions in areas of compromised skin. [GRADE -1; LEVEL OF EVIDENCE -C]
52 Operative / Endovascular -Deep Guideline 6.9:InfrainguinalDeep Venous Obstruction and Skin Changes at Risk for Venous Leg Ulcer (C4b), Healed (C5) or Active (C6) Venous Leg Ulcer In a patient with infrainguinaldeep venous obstruction and skin changes at risk for venous leg ulcer (C4b), healed venous leg ulcer (C5), or active venous leg ulcer (C6), we suggest autogenousvenous bypass or endophlebectomyin addition to standard compression therapy to aid in venous ulcer healing and to prevent recurrence. [GRADE -2; LEVEL OF EVIDENCE -C]
53 Operative / Endovascular -Deep Guideline 6.10:Deep Vein Reflux with Skin Changes at Risk for Venous Leg Ulcer (C4b), Healed (C5) or Active (C6) Venous Leg Ulcer Ligation In a patient with infrainguinaldeep venous reflux and skin changes at risk for venous leg ulcer (C4b), healed venous leg ulcer (C5), or active venous leg ulcer (C6), we suggest against deep vein ligation of the femoral or popliteal veins as a routine treatment. [GRADE -2; LEVEL OF EVIDENCE -C]
54 Operative / Endovascular -Deep Guideline 6.11:Deep Venous Reflux with Skin Changes at Risk for Venous Leg Ulcer (C4b), Healed (C5), or Active (C6) Venous Leg Ulcer Primary Valve Repair In a patient with infrainguinaldeep venous reflux and skin changes at risk for venous leg ulcer (C4b), healed venous leg ulcer (C5), or active venous leg ulcer (C6), we suggest individual valve repair for those who have axial reflux with structurally preserved deep venous valves in addition to standard compression therapy to aid in venous ulcer healing and to prevent recurrence. [GRADE -2; LEVEL OF EVIDENCE -C]
55 Operative / Endovascular -Deep Guideline 6.12:Deep Vein Reflux with Skin Changes at Risk for Venous Leg Ulcer (C4b), Healed (C5) or Active (C6) Venous Leg Ulcer -Valve Transposition or Transplantation In a patient with infrainguinaldeep venous reflux and skin changes at risk for venous leg ulcer (C4b), healed venous leg ulcer (C5), or active venous leg ulcer (C6), we suggest valve transposition or transplantation for those with absence of structurally preserved axial deep venous valve(s) when competent outflow venous pathways are anatomically appropriate for surgical anastomosis in addition to standard compression therapy to aid in venous leg ulcer healing and to prevent recurrence. [GRADE -2; LEVEL OF EVIDENCE -C]
56 Operative / Endovascular -Deep Guideline 6.13: Deep Vein Reflux with Skin Changes at Risk for Venous Leg Ulcer (C4b), Healed (C5), or Active (C6) Venous Leg Ulcer Autogenous Valve Substitute In a patient with infrainguinaldeep venous reflux and skin changes at risk for venous leg ulcer (C4b), healed venous leg ulcer (C5), or active venous leg ulcer (C6), we suggest consideration of autogenousvalve substitutes by surgeons experienced in these techniques to facilitate ulcer healing and to prevent recurrence in those with no other option available in addition to standard compression therapy to aid in venous ulcer healing and to prevent recurrence. [GRADE -2; LEVEL OF EVIDENCE -C]
57 Operative / Endovascular Occlusion Guideline 6.14:Proximal Chronic Total Venous Occlusion / Severe Stenosis with Skin Changes at Risk for Venous Leg Ulcer (C4b), Healed (C5) or Active (C6) Venous Leg Ulcer - Endovascular Repair In a patient with inferior vena cava and/or iliac vein chronic total occlusion or severe stenosis, with or without lower extremity deep venous reflux disease, which is associated with skin changes at risk for venous leg ulcer (C4b), healed venous leg ulcer (C5), or active venous leg ulcer (C6), we recommend venous angioplasty and stent recanalization in addition to standard compression therapy to aid in venous ulcer healing and to prevent recurrence. [GRADE -1; LEVEL OF EVIDENCE -C]
58 Operative / Endovascular Occlusion Guideline 6.15:Proximal Chronic Venous Occlusion / Severe Stenosis (Bilateral) with Recalcitrant Venous Ulcer - Open Repair In a patient with inferior vena cava and/or iliac vein chronic occlusion or severe stenosis, with or without lower extremity deep venous reflux disease, which is associated with a recalcitrant venous leg ulcer and who have failed endovascular treatment, we suggest open surgical bypass using an externally supported eptfegraft in addition to standard compression therapy to aid in venous leg ulcer healing and to prevent recurrence. [GRADE -2; LEVEL OF EVIDENCE -C]
59 Operative / Endovascular Occlusion Guideline 6.16:Unilateral IliofemoralVenous Occlusion / Severe Stenosis With Recalcitrant Venous Ulcer Open Repair: In a patient with unilateral iliofemoralvenous occlusion/severe stenosis with recalcitrant venous leg ulcer who failed attempts at endovascular reconstruction, we suggest open surgical bypass using saphenous vein as a crosspubicbypass (Palma procedure) to aid in venous ulcer healing and to prevent recurrence. A synthetic graft is an alternative in the absence of autogenoustissue. [GRADE -2; LEVEL OF EVIDENCE -C]
60 Operative / Endovascular Occlusion Guideline 6.17:Proximal Chronic Total Venous Occlusion / Severe Stenosis (Bilateral or Unilateral) With Recalcitrant Venous Ulcer Adjunctive arteriovenous fistula: For those patients who would benefit from an open venous bypass, we suggest the addition of an adjunctive arteriovenous fistula (4 to 6 mm in size) as an adjunct to improve inflow into autologous or prosthetic cross over bypasses when the inflow is judged to be poor to aid in venous leg ulcer healing and to prevent recurrence. [GRADE -2; LEVEL OF EVIDENCE -C]
61 Ancillary Measures -Nutrition Guideline 7.1: Nutrition Assessment and Management: We recommend that nutrition assessment be performed in any patient with a venous leg ulcer who has evidence of malnutrition and that nutritional supplementation be provided if malnutrition identified. [BEST PRACTICE]
62 Ancillary Measures -Medications Guideline 7.2: Systemic Drug Therapy For long-standing or large venous leg ulcer we recommend treatment with either pentoxifylline or micronized purified flavonoid fraction used in combination with compression therapy. [GRADE -1; LEVEL OF EVIDENCE B]
63 Ancillary Measures -Physiotherapy Guideline 7.3: Physiotherapy We suggest supervised active exercise to improve muscle pump function and reduce pain and edema in patients with venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -B]
64 Ancillary Measures Lymphatic Guideline 7.4: Manual Lymphatic Drainage We suggest against adjunctive lymphatic drainage for healing of the chronic venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -C]
65 Ancillary Measures -Balneotherapy Guideline 7.5: Balneotherapy We suggest balneotherapyto improve skin trophic changes and quality of life in patients with advance venous disease. [GRADE -2; LEVEL OF EVIDENCE -B]
66 Ancillary Measures -Ultraviolet Guideline 7.6: Ultraviolet light We suggest against using ultraviolet light for the treatment of venous leg ulcers. [GRADE -2; LEVEL OF EVIDENCE -C]
67 Primary Prevention Primary Reflux Guideline 8.1:Primary Prevention - Clinical CEAP C3-4 Primary Venous Disease In patients with Clinical CEAP C 3-4 disease due to primary valvularreflux, we recommend mmhg compression, knee or thigh high. [GRADE -2; LEVEL OF EVIDENCE -C]
68 Primary Prevention Post-Thrombotic Guideline 8.2:Primary Prevention - Clinical CEAP C1-4 Post-Thrombotic Venous Disease In patients with Clinical CEAP C1-4 disease related to prior DVT, we recommend compression, mmhg, knee or thigh high. [GRADE -1; LEVEL OF EVIDENCE -B]
69 Primary Prevention Acute DVT Guideline 8.3. Primary Prevention Acute DVT Treatment As post thrombotic syndrome (PTS) is a common preceding event for venous leg ulcers, we recommend current evidence based therapies for acute DVT treatment. [GRADE -1; LEVEL OF EVIDENCE -B] We suggest use of low molecular weight heparin (LMWH) over vitamin k antagonist therapy of 3 month duration to decrease PTS [GRADE -2; LEVEL OF EVIDENCE -B] We suggest catheter directed thrombolysis in low bleeding risk patients with iliofemoraldvt of duration <14 days [GRADE -2; LEVEL OF EVIDENCE -B]
70 Primary Prevention -Education Guideline 8.4: Primary Prevention Education Measures In patients with C1-4 disease, we suggest patient and family education, regular exercise, leg elevation when at rest, careful skin care, weight control and appropriately fitting foot wear. [BEST PRACTICE]
71 Primary Prevention -Operative Guideline 8.5: Primary Prevention Operative Therapy In patients with asymptomatic C1-2 disease from either primary or secondary causes, we suggest against prophylactic interventional therapies to prevent venous leg ulcer. [GRADE -2; LEVEL OF EVIDENCE -C]
72
New Guideline in venous ulcer treatment: dressing, medication, intervention
 New Guideline in venous ulcer treatment: dressing, medication, intervention Kittipan Rerkasem, FRCS(T), PhD Department of Surgery Faculty of Medicine Chiang Mai University Topic Overview venous ulcer treatment
New Guideline in venous ulcer treatment: dressing, medication, intervention Kittipan Rerkasem, FRCS(T), PhD Department of Surgery Faculty of Medicine Chiang Mai University Topic Overview venous ulcer treatment
Conflict of Interest. None
 Conflict of Interest None American Venous Forum Guidelines on Superficial Venous Disease TOP 10 GUIDELINES 10. We recommend using the CEAP classification to describe chronic venous disorders. (GRADE 1B)
Conflict of Interest None American Venous Forum Guidelines on Superficial Venous Disease TOP 10 GUIDELINES 10. We recommend using the CEAP classification to describe chronic venous disorders. (GRADE 1B)
Venous Ulcers. A Little Basic Science. An Aggressive Prescription to Aid Healing. Why do venous ulcers occur? Ambulatory venous hypertension!
 UCSF Vascular Symposium April 26-28, 2012 San Francisco, California True statements about the management of venous ulcers include: An Aggressive Prescription to Aid Healing Anthony J. Comerota, MD, FACS,
UCSF Vascular Symposium April 26-28, 2012 San Francisco, California True statements about the management of venous ulcers include: An Aggressive Prescription to Aid Healing Anthony J. Comerota, MD, FACS,
Venous Insufficiency Ulcers. Patient Assessment: Superficial varicosities. Evidence of healed ulcers. Dermatitis. Normal ABI.
 Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Venous Insufficiency Ulcers Patient Assessment: Superficial varicosities Evidence of healed ulcers Dermatitis Normal ABI Edema Eczematous skin changes 1. Scaling 2. Pruritus 3. Erythema 4. Vesicles Lipodermatosclerosis
Additional Information S-55
 Additional Information S-55 Network providers are encouraged, but not required to participate in the on-line American Venous Forum Registry (AVR) - The First National Registry for the Treatment of Varicose
Additional Information S-55 Network providers are encouraged, but not required to participate in the on-line American Venous Forum Registry (AVR) - The First National Registry for the Treatment of Varicose
Prevention and Management of Leg Ulcers
 EWMA Educational Development Programme Curriculum Development Project Education Module: Prevention and Management of Leg Ulcers Latest revision: October 2015 ABOUT THE EWMA EDUCATIONAL DEVELOPMENT PROGRAMME
EWMA Educational Development Programme Curriculum Development Project Education Module: Prevention and Management of Leg Ulcers Latest revision: October 2015 ABOUT THE EWMA EDUCATIONAL DEVELOPMENT PROGRAMME
Adjunctive Therapies: The Use of Skin Substitutes and Growth Factors in Venous Leg Ulceration (VLU)
") Adjunctive Therapies: The Use of Skin Substitutes and Growth Factors in Venous Leg Ulceration (VLU) Sami Khan, MD FACS Associate Professor of Surgery Division of Plastic and Reconstructive Surgery SUNY-Stony
Adjunctive Therapies: The Use of Skin Substitutes and Growth Factors in Venous Leg Ulceration (VLU) Sami Khan, MD FACS Associate Professor of Surgery Division of Plastic and Reconstructive Surgery SUNY-Stony
2017 Florida Vascular Society
 Current Management of Venous Leg Ulcers: How to Identify Patients with Correctable Venous Disease and Interventional Procedures to Heal and Prevent Recurrence 2017 Florida Vascular Society Bill Marston
Current Management of Venous Leg Ulcers: How to Identify Patients with Correctable Venous Disease and Interventional Procedures to Heal and Prevent Recurrence 2017 Florida Vascular Society Bill Marston
Venous Leg Ulcers. Care for Patients in All Settings
 Venous Leg Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a venous leg ulcer. The scope of the standard
Venous Leg Ulcers Care for Patients in All Settings Summary This quality standard focuses on care for people who have developed or are at risk of developing a venous leg ulcer. The scope of the standard
Post-Thrombotic Syndrome(PTS) Conservative Treatment Options
 Conservative Treatment Options") Post-Thrombotic Syndrome(PTS) Conservative Treatment Options Dr. S. Kundu Scarborough Hospital-General Division Scarborough Vascular Group Toronto Endovascular Centre The Vein Institute of Toronto Scarborough
Post-Thrombotic Syndrome(PTS) Conservative Treatment Options Dr. S. Kundu Scarborough Hospital-General Division Scarborough Vascular Group Toronto Endovascular Centre The Vein Institute of Toronto Scarborough
Case. Wounds. Fundamentals of Ulcer Care. Dr. Mark Meissner Wound Case Study. Compression and Ulcer Healing Cullum NA, Cochrane Reviews 2001
 Case Wounds Mark H. Meissner, MD University of Washington School of Medicine 65 yr old male physician Recurrent R medial malleolar ulcer over 5 years New R lateral malleolar ulcer Intermittently wearing
Case Wounds Mark H. Meissner, MD University of Washington School of Medicine 65 yr old male physician Recurrent R medial malleolar ulcer over 5 years New R lateral malleolar ulcer Intermittently wearing
Chronic Venous Insufficiency Compression and Beyond
 Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
Disclosure of Conflict of Interest Chronic Venous Insufficiency Compression and Beyond Shawn Amyot, MD, CCFP Fellow of the Canadian Society of Phlebology Ottawa Vein Centre I do not have relevant financial
PUT YOUR BEST FOOT FORWARD
 PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
PUT YOUR BEST FOOT FORWARD Bala Ramanan, MBBS 1 st year vascular surgery fellow Introduction The epidemic of diabetes and ageing of our population ensures critical limb ischemia will continue to grow.
The role of ultrasound duplex in endovenous procedures
 The role of ultrasound duplex in endovenous procedures Neophytos A. Zambas MD, PhD Vascular Surgeon Polyclinic Ygia, Limassol, Cyprus ΚΕΑΕΧ ΚΥΠΡΙΑΚΗ ΕΤΑΙΡΕΙΑ ΑΓΓΕΙΑΚΗΣ ΚΑΙ ΕΝΔΑΓΓΕΙΑΚΗΣ ΧΕΙΡΟΥΡΓΙΚΗΣ Pre
The role of ultrasound duplex in endovenous procedures Neophytos A. Zambas MD, PhD Vascular Surgeon Polyclinic Ygia, Limassol, Cyprus ΚΕΑΕΧ ΚΥΠΡΙΑΚΗ ΕΤΑΙΡΕΙΑ ΑΓΓΕΙΑΚΗΣ ΚΑΙ ΕΝΔΑΓΓΕΙΑΚΗΣ ΧΕΙΡΟΥΡΓΙΚΗΣ Pre
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT
 VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
VASCULAR WOUNDS PATHOPHYSIOLOGY AND MANAGEMENT Lucy Stopher, A/CNS Vascular Surgery ...it is best to think of a wound not as a disease, but rather as a manifestation of disease. Joe McCulloch In order
Physician s Vascular Interpretation Examination Content Outline
 Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Physician s Vascular Interpretation Examination Content Outline (Outline Summary) # Domain Subdomain Percentage 1 2 3 4 5 6 Cerebrovascular Abdominal Peripheral Arterial - Duplex Imaging Peripheral Arterial
Recommendations for Follow-up After Vascular Surgery Arterial Procedures SVS Practice Guidelines
 Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Recommendations for Follow-up After Vascular Surgery Arterial Procedures 2018 SVS Practice Guidelines vsweb.org/svsguidelines About the guidelines Published in the July 2018 issue of Journal of Vascular
Schedule of Benefits. for Professional Fees Vascular Procedures
 Schedule of Benefits for Professional Fees 2018 Vascular Procedures ANASTOMOSIS RULES 820 Arteriovenous anastomosis in arm 1453 Arteriovenous anastomosis, open by basilic vein transposition 1465 Splenorenal
Schedule of Benefits for Professional Fees 2018 Vascular Procedures ANASTOMOSIS RULES 820 Arteriovenous anastomosis in arm 1453 Arteriovenous anastomosis, open by basilic vein transposition 1465 Splenorenal
Morbidity Audit and Logbook Tool SNOMED Board Reporting Terms for SET and IMG Vascular Surgery AMPUTATION AORTA
 SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
SNOMED s for SET and IMG Vascular Surgery AMPUTATION Amputation above-knee Amputation of leg through tibia and fibula Amputation of the foot Amputation of toe Through knee amputation Ray amputation of
Dr Paul Thibault. Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology
 Australasian College of Phlebology") Dr Paul Thibault Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology Prescribing Effective Compression and PTS Dr Paul Thibault Phlebologist, Newcastle,
Dr Paul Thibault Phlebologist & Assistant Editor Phlebology (International Journal) Australasian College of Phlebology Prescribing Effective Compression and PTS Dr Paul Thibault Phlebologist, Newcastle,
Starting with deep venous treatment
 Starting with deep venous treatment Carsten Arnoldussen, MD Interventional Radiologist Maastricht University Medical Centre, Maastricht VieCuri Medical Centre, Venlo The Netherlands Background Maastricht
Starting with deep venous treatment Carsten Arnoldussen, MD Interventional Radiologist Maastricht University Medical Centre, Maastricht VieCuri Medical Centre, Venlo The Netherlands Background Maastricht
Wound Jeopardy: Name That Wound Session 142 Saturday, September 10 th 2011
 Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
Initial Wound Care Consult History Physical Examination Detailed examination of the wound Photographs Cultures Procedures TCOM ABI Debridement Management Decisions A Detailed History and Physical (wound)
Role of free tissue transfer in management of chronic venous ulcer
 Original Article Role of free tissue transfer in management of chronic venous ulcer K. Murali Mohan Reddy, D. Mukunda Reddy Department of Plastic Surgery, Nizams Institute of Medical Sciences, India. Address
Original Article Role of free tissue transfer in management of chronic venous ulcer K. Murali Mohan Reddy, D. Mukunda Reddy Department of Plastic Surgery, Nizams Institute of Medical Sciences, India. Address
Lower Extremity Wound Evaluation and Treatment
 Lower Extremity Wound Evaluation and Treatment Boni-Jo Silbernagel, DPM Describe effective lower extremity wound evaluation and treatment. Discuss changes in theories of treatment in wound care and implications
Lower Extremity Wound Evaluation and Treatment Boni-Jo Silbernagel, DPM Describe effective lower extremity wound evaluation and treatment. Discuss changes in theories of treatment in wound care and implications
ULCERS 1/12/ million diabetics in the US (2012) Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years
 Reamputation Rate 26.7% at 1 year 48.3% at 3 years 60.7% at 5 years") Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
Jay Christensen D.P.M Advanced Foot and Ankle of Wisconsin 2-4% of the population at any given time will have ulcers 0.06-0.20% of the total population Average age of patients 70 years increased as more
How to manage leg ulcers in the elderly
 How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
How to manage leg ulcers in the elderly David Riding Clinical Research Fellow / Specialty Registrar in Vascular Surgery University of Manchester / MFT British Geriatric Society Trainees Meeting 2018 Objectives
Wound Classification. Overview
 Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Overview Jeffrey A. Niezgoda, MD FACHM, MAPWCA, CHWS Review of Initial Wound Care Consultation Rational for Classification Wound Appearance Wound Etiology Management Algorithms Initial Wound Care Consult
Medicare C/D Medical Coverage Policy
 Varicose Vein Treatment Medicare C/D Medical Coverage Policy Origination Date: June 1, 1993 Review Date: February 15, 2017 Next Review: February, 2019 DESCRIPTION OF PROCEDURE OR SERVICE Varicose veins
Varicose Vein Treatment Medicare C/D Medical Coverage Policy Origination Date: June 1, 1993 Review Date: February 15, 2017 Next Review: February, 2019 DESCRIPTION OF PROCEDURE OR SERVICE Varicose veins
Vein Disease Treatment
 MP9241 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated in 2.0, 3.0, 4.0 and 5.0 Additional Information: None Prevea360 Health Plan Medical Policy: Vein disease
MP9241 Covered Service: Yes when meets criteria below Prior Authorization Required: Yes as indicated in 2.0, 3.0, 4.0 and 5.0 Additional Information: None Prevea360 Health Plan Medical Policy: Vein disease
Surgical approach for DVT. Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine
 Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Surgical approach for DVT Seung-Kee Min Division of Vascular Surgery Department of Surgery Seoul National University College of Medicine Treatment Options for Venous Thrombosis Unfractionated heparin &
Perforators: When to Treat and How Best to Do It? Eric Hager, MD September 10, 2015
 Perforators: When to Treat and How Best to Do It? Eric Hager, MD September 10, 2015 Anatomy of Perforating veins Cadaveric studies 1 have shown >60 vein perforating veins from superficial to deep Normal
Perforators: When to Treat and How Best to Do It? Eric Hager, MD September 10, 2015 Anatomy of Perforating veins Cadaveric studies 1 have shown >60 vein perforating veins from superficial to deep Normal
COMMISSIONING POLICY
 Ref No. 1a7.5 COMMISSIONING POLICY Surgery for venous disease of the leg (Varicosities of the Long Saphenous Vein) April 2011 CONTENTS Section Page Summary 2 1. Background 2 2. Criteria for eligibility
Ref No. 1a7.5 COMMISSIONING POLICY Surgery for venous disease of the leg (Varicosities of the Long Saphenous Vein) April 2011 CONTENTS Section Page Summary 2 1. Background 2 2. Criteria for eligibility
Surgical disobliteration of postthrombotic deep veins endophlebectomy is feasible
 Surgical disobliteration of postthrombotic deep veins endophlebectomy is feasible Alessandra Puggioni, MD, a,c Robert L. Kistner, MD, a,b Bo Eklof, MD, PhD, a,b,c and Fedor Lurie, MD, PhD, a,b,c Honolulu,
Surgical disobliteration of postthrombotic deep veins endophlebectomy is feasible Alessandra Puggioni, MD, a,c Robert L. Kistner, MD, a,b Bo Eklof, MD, PhD, a,b,c and Fedor Lurie, MD, PhD, a,b,c Honolulu,
Clinical/Duplex Evaluation of Varicose Veins: Who to Treat?
 Clinical/Duplex Evaluation of Varicose Veins: Who to Treat? Sanjoy Kundu MD, FASA, FCIRSE, FSIR The Vein Institute of Toronto Scarborough Vascular Group Scarborough Vascular Ultrasound Scarborough Vascular
Clinical/Duplex Evaluation of Varicose Veins: Who to Treat? Sanjoy Kundu MD, FASA, FCIRSE, FSIR The Vein Institute of Toronto Scarborough Vascular Group Scarborough Vascular Ultrasound Scarborough Vascular
Complex Iliocaval Reconstruction PNEC. Seattle WA. Bill Marston MD Professor, Div of Vascular Surgery University of N.
 Complex Iliocaval Reconstruction 2017 PNEC. Seattle WA Bill Marston MD Professor, Div of Vascular Surgery University of N. Carolina DISCLOSURES William Marston, MD Consultant/Advisory Board: Veniti, Cardinal
Complex Iliocaval Reconstruction 2017 PNEC. Seattle WA Bill Marston MD Professor, Div of Vascular Surgery University of N. Carolina DISCLOSURES William Marston, MD Consultant/Advisory Board: Veniti, Cardinal
Disclosures. What is a Specialty Vein Clinic? Prevalence of Venous Disease. Management of Venous Disease: an evidence based approach.
 Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
Management of Venous Disease: an evidence based approach Disclosures Ed Boyle, MD Andrew Jones, MD Dr. Ed Boyle and Dr. Andrew Jones disclose Grants/research support: Medtronic, BTG International, Clearflow,
Page 1. Ruling out deep venous obstruction prior to superficial vein treatment. Disclosures. Indications for saphenous vein ablation (SVA)
") 1 Ruling out deep venous obstruction prior to superficial vein treatment Deepak Sudheendra, MD, RPVI Assistant Professor of Clinical Radiology & Surgery Disclosures No financial disclosures Indications
1 Ruling out deep venous obstruction prior to superficial vein treatment Deepak Sudheendra, MD, RPVI Assistant Professor of Clinical Radiology & Surgery Disclosures No financial disclosures Indications
Topical antimicrobials (antiseptics) Iodine, Silver, Honey
 Iodine, Silver, Honey") Topical antimicrobials (antiseptics) Iodine, Silver, Honey Iodine Honey Silver Enzymatic debridement Proteolytic enzyme, also called Proteinase Proteinase breaks the long chainlike molecules of proteins
Topical antimicrobials (antiseptics) Iodine, Silver, Honey Iodine Honey Silver Enzymatic debridement Proteolytic enzyme, also called Proteinase Proteinase breaks the long chainlike molecules of proteins
On Which Criteria Do You Select Your Stent for Ilio-femoral Venous Obstruction? North American Point of View
 On Which Criteria Do You Select Your Stent for Ilio-femoral Venous Obstruction? North American Point of View Peter Gloviczki, MD Ying Huang, MD, PhD Division of Vascular and Endovascular Surgery, Mayo
On Which Criteria Do You Select Your Stent for Ilio-femoral Venous Obstruction? North American Point of View Peter Gloviczki, MD Ying Huang, MD, PhD Division of Vascular and Endovascular Surgery, Mayo
Current Management of Varicose Veins
 Current Management of Varicose Veins Michael J. Heidenreich, MD St. Joseph Mercy Hospital Ann Arbor, MI March 23, 2013 Nothing to disclose History Prevalence Anatomy Risk factors Clinical manifestations
Current Management of Varicose Veins Michael J. Heidenreich, MD St. Joseph Mercy Hospital Ann Arbor, MI March 23, 2013 Nothing to disclose History Prevalence Anatomy Risk factors Clinical manifestations
VENOUS LEG ULCERS (VLU)
") VENOUS LEG ULERS (VLU) REOMMENDTION S Evidence-based gradings Excellent evidence ody of evidence can be trusted to guide practice. Good evidence ody of evidence can be trusted to guide practice in most
VENOUS LEG ULERS (VLU) REOMMENDTION S Evidence-based gradings Excellent evidence ody of evidence can be trusted to guide practice. Good evidence ody of evidence can be trusted to guide practice in most
THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT
 THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT Tara D. Balint, MD FACS Sentara RMH Thursday, June 14, 2018 1 Objectives of treatment for DVT Prevent death from PE Prevent recurrent VTE Prevent post-thrombotic
THERE IS NO ROLE FOR SURGICAL THERAPY FOR DVT Tara D. Balint, MD FACS Sentara RMH Thursday, June 14, 2018 1 Objectives of treatment for DVT Prevent death from PE Prevent recurrent VTE Prevent post-thrombotic
Chronic Venous Insufficiency
 Chronic Venous Insufficiency None Disclosures Lesley Enfinger, MSN,NP-C Chronic Venous Insufficiency Over 24 Million Americans affected by Chronic Venous Insufficiency (CVI) 10 x More Americans suffer
Chronic Venous Insufficiency None Disclosures Lesley Enfinger, MSN,NP-C Chronic Venous Insufficiency Over 24 Million Americans affected by Chronic Venous Insufficiency (CVI) 10 x More Americans suffer
BC Vascular Day. Contents. November 3, Abdominal Aortic Aneurysm 2 3. Peripheral Arterial Disease 4 6. Deep Venous Thrombosis 7 8
 BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
BC Vascular Day Contents Abdominal Aortic Aneurysm 2 3 November 3, 2018 Peripheral Arterial Disease 4 6 Deep Venous Thrombosis 7 8 Abdominal Aortic Aneurysm Conservative Management Risk factor modification
Venous Insufficiency Ulcer
 Disclosure NOTHING Venous Insufficiency Ulcer Venous Insufficiency Ulcer Also know as Venous Stasis Ulcer Ulcerative Venous Reflux Disease Statistics / Clinical Frequency Affects 2-5 % of the population
Disclosure NOTHING Venous Insufficiency Ulcer Venous Insufficiency Ulcer Also know as Venous Stasis Ulcer Ulcerative Venous Reflux Disease Statistics / Clinical Frequency Affects 2-5 % of the population
Debridement within the context of the EWMA s debridement guidelines. Emil Schmidt WCNS SDHB - Otago
 Debridement within the context of the EWMA s debridement guidelines Emil Schmidt WCNS SDHB - Otago EWMA Debridement Document Expert consensus document, 2013 Contents Mechanical debridement options Autolytic
Debridement within the context of the EWMA s debridement guidelines Emil Schmidt WCNS SDHB - Otago EWMA Debridement Document Expert consensus document, 2013 Contents Mechanical debridement options Autolytic
Management of Lower Limb Ulcers. D. NAIK MBChB FRACS DDU
 Management of Lower Limb Ulcers D. NAIK MBChB FRACS DDU Ulcer A defect in the epithelium Ulcer A failure to heal Aetiology of Leg Ulcers Arterial Venous Neuropathic Vasculitic Infectious Neoplastic Lymphoedema
Management of Lower Limb Ulcers D. NAIK MBChB FRACS DDU Ulcer A defect in the epithelium Ulcer A failure to heal Aetiology of Leg Ulcers Arterial Venous Neuropathic Vasculitic Infectious Neoplastic Lymphoedema
A A U
 PVD Venous AUC Rating Sheet 2nd Round 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Median I NI MADM Rating Agree Disagree Upper Extremity Venous Evaluation Table 1. Venous Duplex of the Upper Extremities for Patency
PVD Venous AUC Rating Sheet 2nd Round 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Median I NI MADM Rating Agree Disagree Upper Extremity Venous Evaluation Table 1. Venous Duplex of the Upper Extremities for Patency
Dr Peter Chapman-Smith
 Dr Peter Chapman-Smith Phlebologist NZ Stem Cell Treatment Centre, Whangarei 12:00-12:30 Healing Those Heartsink Leg Ulcers Healing Those Heartsink Leg Ulcers Practice Nurses Presentation GPCME Christchurch
Dr Peter Chapman-Smith Phlebologist NZ Stem Cell Treatment Centre, Whangarei 12:00-12:30 Healing Those Heartsink Leg Ulcers Healing Those Heartsink Leg Ulcers Practice Nurses Presentation GPCME Christchurch
Chronic Venous Disease: A Complex Disorder. A N Nicolaides
 Chronic Venous Disease: A Complex Disorder A N Nicolaides Emeritus Professor of Vascular Surgery, Imperial College, London. Hon. Professor of Surgery, University of Nicosia Medical School, Cyprus Disclosures
Chronic Venous Disease: A Complex Disorder A N Nicolaides Emeritus Professor of Vascular Surgery, Imperial College, London. Hon. Professor of Surgery, University of Nicosia Medical School, Cyprus Disclosures
Thrombectomy, open, arteriovenous fistula without revision, autogenous or nonautogenous dialysis graft (separate procedure)
") Dialysis Vascular Access Coverage, Coding and Reimbursement Overview Hospital Outpatient 2019 Edition All Reimbursement Amounts are Listed at ational Unadjusted Medicare Rates and Do ot Include the 2%
Dialysis Vascular Access Coverage, Coding and Reimbursement Overview Hospital Outpatient 2019 Edition All Reimbursement Amounts are Listed at ational Unadjusted Medicare Rates and Do ot Include the 2%
UNDERSTANDING VEIN PROBLEMS
 UNDERSTANDING VEIN PROBLEMS Varicose Veins, Chronic Venous Insufficiency, and DVT Do You Have a Vein Problem? Have you noticed pain or swelling in your legs? Do your symptoms worsen when you re sitting
UNDERSTANDING VEIN PROBLEMS Varicose Veins, Chronic Venous Insufficiency, and DVT Do You Have a Vein Problem? Have you noticed pain or swelling in your legs? Do your symptoms worsen when you re sitting
Non-Saphenous Vein Treatments. Jessica Ochs PA-C Albert Vein Institute Colorado Springs and Lone Tree, CO
 Non-Saphenous Vein Treatments Jessica Ochs PA-C Albert Vein Institute Colorado Springs and Lone Tree, CO I have no financial disclosures Types of Veins Treated Perforator Veins Tributary Veins Varicose
Non-Saphenous Vein Treatments Jessica Ochs PA-C Albert Vein Institute Colorado Springs and Lone Tree, CO I have no financial disclosures Types of Veins Treated Perforator Veins Tributary Veins Varicose
Complete Evaluation of the Chronic Venous Patient: Recognizing deep venous obstruction. Erin H. Murphy, MD Rane Center
 Complete Evaluation of the Chronic Venous Patient: Recognizing deep venous obstruction Erin H. Murphy, MD Rane Center Disclosure Speaker name: Erin H. Murphy... I have the following potential conflicts
Complete Evaluation of the Chronic Venous Patient: Recognizing deep venous obstruction Erin H. Murphy, MD Rane Center Disclosure Speaker name: Erin H. Murphy... I have the following potential conflicts
The Management of Lower Limb Oedema. Catherine Hammond CNS/CNE 2018
 The Management of Lower Limb Oedema Catherine Hammond CNS/CNE 2018 Causes of oedema Venous stasis Lymphoedema Heart Failure Dependency Liver and kidney failure Medications Cellulitis Low protein Under
The Management of Lower Limb Oedema Catherine Hammond CNS/CNE 2018 Causes of oedema Venous stasis Lymphoedema Heart Failure Dependency Liver and kidney failure Medications Cellulitis Low protein Under
Venous Disease and Leg Ulcers. Edward G Mackay MD St. Petersburg, FL NCVH 2015 Orlando, FL
 Venous Disease and Leg Ulcers Edward G Mackay MD St. Petersburg, FL NCVH 2015 Orlando, FL Disclosures Stocks Endoshape Sapheon Medical Advisory Board BTG, Boston Scientific Venous Leg Ulcer Most common
Venous Disease and Leg Ulcers Edward G Mackay MD St. Petersburg, FL NCVH 2015 Orlando, FL Disclosures Stocks Endoshape Sapheon Medical Advisory Board BTG, Boston Scientific Venous Leg Ulcer Most common
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL Policy Number: MP.066.MH Last Review Date: 11/08/2018 Effective Date: 01/01/2019
 MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers the treatment of Varicose
MedStar Health, Inc. POLICY AND PROCEDURE MANUAL This policy applies to the following lines of business: MedStar Employee (Select) MedStar CareFirst PPO MedStar Health considers the treatment of Varicose
Surgical Options for revascularisation P E T E R S U B R A M A N I A M
 Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
Surgical Options for revascularisation P E T E R S U B R A M A N I A M The goal Treat pain Heal ulcer Preserve limb Preserve life The options Conservative Endovascular Surgical bypass Primary amputation
BC Vascular Surgery Day
 BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
BC Vascular Surgery Day November 4, 2017 1 Table of Contents Abdominal Aortic Aneurysm 3 4 Acute DVT 5 6 Peripheral Arterial Disease 7 9 Varicose Veins 10 11 Diabetic Foot Ulcers 12 13 Carotid Stenosis
Will it heal? How to assess the probability of wound healing
 Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
Will it heal? How to assess the probability of wound healing Richard F. Neville, M.D. Professor of Surgery Chief, Division of Vascular Surgery George Washington University Limb center case 69 yr old male
The evidence for venous interventions is evolving- many patients do actually benefit. Nils Kucher University Hospital Bern Switzerland
 The evidence for venous interventions is evolving- many patients do actually benefit Nils Kucher University Hospital Bern Switzerland Disclosure Speaker name: Nils Kucher X X I have the following potential
The evidence for venous interventions is evolving- many patients do actually benefit Nils Kucher University Hospital Bern Switzerland Disclosure Speaker name: Nils Kucher X X I have the following potential
RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY
 RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY Paul Kramer, MD, FACC, FSCAI Liberty Cardiovascular Specialists Liberty Regional Heart and Vascular Center DISCLOSURES NONE Venous
RECOGNITION AND ENDOVASCULAR TREATMENT OF CHRONIC VENOUS INSUFFICIENCY Paul Kramer, MD, FACC, FSCAI Liberty Cardiovascular Specialists Liberty Regional Heart and Vascular Center DISCLOSURES NONE Venous
DEBRIDEMENT. Professor Donald G. MacLellan Executive Director Health Education & Management Innovations
 DEBRIDEMENT Professor Donald G. MacLellan Executive Director Health Education & Management Innovations DEBRIDEMENT Principles - CSD Methods of Debridement Biopsy options PRINCIPLES OF WOUND MANAGEMENT
DEBRIDEMENT Professor Donald G. MacLellan Executive Director Health Education & Management Innovations DEBRIDEMENT Principles - CSD Methods of Debridement Biopsy options PRINCIPLES OF WOUND MANAGEMENT
How to best approach chronic venous occlusions?
 How to best approach chronic venous occlusions? Prof. Nils Kucher Director Venous Thromboembolism Reseach Group University Hospital Bern nilskucher.com Disclosure Speaker name: Nils Kucher X X I have the
How to best approach chronic venous occlusions? Prof. Nils Kucher Director Venous Thromboembolism Reseach Group University Hospital Bern nilskucher.com Disclosure Speaker name: Nils Kucher X X I have the
Patient assessment and strategy making for endovenous treatment
 Patient assessment and strategy making for endovenous treatment Raghu Kolluri, MD Director Vascular Medicine OhioHealth Riverside Methodist Hospital Columbus, OH Disclosures Current Medtronic Consultant/
Patient assessment and strategy making for endovenous treatment Raghu Kolluri, MD Director Vascular Medicine OhioHealth Riverside Methodist Hospital Columbus, OH Disclosures Current Medtronic Consultant/
Nanogen Aktiv. Naz Wahab MD, FAAFP, FAPWCA Nexderma
 Nanogen Aktiv Naz Wahab MD, FAAFP, FAPWCA Nexderma Patient BM 75 y.o female with a history of Type 2 Diabetes, HTN, Hypercholesterolemia, Renal insufficiency, Chronic back Pain, who had undergone a L3-L4
Nanogen Aktiv Naz Wahab MD, FAAFP, FAPWCA Nexderma Patient BM 75 y.o female with a history of Type 2 Diabetes, HTN, Hypercholesterolemia, Renal insufficiency, Chronic back Pain, who had undergone a L3-L4
Acute and Chronic WOUND ASSESSMENT. Wound Assessment OBJECTIVES ITEMS TO CONSIDER
 WOUND ASSESSMENT Acute and Chronic OBJECTIVES Discuss classification systems and testing methods for pressure ulcers, venous, arterial and diabetic wounds List at least five items to be assessed and documented
WOUND ASSESSMENT Acute and Chronic OBJECTIVES Discuss classification systems and testing methods for pressure ulcers, venous, arterial and diabetic wounds List at least five items to be assessed and documented
Reality TV Managing patients in the real world. Wounds UK Harrogate 2009
 Reality TV Managing patients in the real world Wounds UK Harrogate 2009 Reality TV Managing patients in the real world Brenda M King Nurse Consultant Tissue Viability Sheffield PCT Harrogate 2009 Familiar
Reality TV Managing patients in the real world Wounds UK Harrogate 2009 Reality TV Managing patients in the real world Brenda M King Nurse Consultant Tissue Viability Sheffield PCT Harrogate 2009 Familiar
Determine the patients relative risk of thrombosis. Be confident that you have had a meaningful discussion with the patient.
 Patient Assessment :Venous History, Examination and Introduction to Doppler and PPG Dr Louis Loizou The 11 th Annual Scientific Meeting and Workshops of the Australasian College of Phlebology Tuesday 18
Patient Assessment :Venous History, Examination and Introduction to Doppler and PPG Dr Louis Loizou The 11 th Annual Scientific Meeting and Workshops of the Australasian College of Phlebology Tuesday 18
Date: A. Venous Health History Form. Patient please complete questions Primary Care Physician:
 E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
E S Insurance: 2 nd Insurance: Wait time: Date: A. Venous Health History Form Patient please complete questions 1-12 Patient Name: SSN#: Date of Birth: Primary Care Physician: What is the reason for your
Deep Venous Pathology. Eberhard Rabe Department of Dermatology University of Bonn Germany
 Deep Venous Pathology Eberhard Rabe Department of Dermatology University of Bonn Germany Disclosures None for this presentation Consultant: Sigvaris, EUROCOM Speakers bureau: Bayer Vital, Aspen, Boehringer,
Deep Venous Pathology Eberhard Rabe Department of Dermatology University of Bonn Germany Disclosures None for this presentation Consultant: Sigvaris, EUROCOM Speakers bureau: Bayer Vital, Aspen, Boehringer,
Lower Extremity Venous Disease (LEVD)
") Lower Extremity Venous Disease (LEVD) Lower Extremity Venous Disease (LEVD) Wounds Etiology Lower extremity venous leg ulcers are caused by chronic venous hypertension. Failure of valves in the veins or
Lower Extremity Venous Disease (LEVD) Lower Extremity Venous Disease (LEVD) Wounds Etiology Lower extremity venous leg ulcers are caused by chronic venous hypertension. Failure of valves in the veins or
Management of Post-Thrombotic Syndrome
 Management of Post-Thrombotic Syndrome Thanainit Chotanaphuti Phramongkutklao College of Medicine Bangkok, Thailand President of CAOS Asia President of Thai Hip & Knee Society President of ASEAN Arthroplasty
Management of Post-Thrombotic Syndrome Thanainit Chotanaphuti Phramongkutklao College of Medicine Bangkok, Thailand President of CAOS Asia President of Thai Hip & Knee Society President of ASEAN Arthroplasty
chronic venous disorders, varicose vein, CEAP classification, lipodermatosclerosis, Klippel- Trenaunay syndrome DVT CVD
 Online publication August 27, 2009 chronic venous disorders: CVD CEAP 4 CEAP CVD J Jpn Coll Angiol, 2009, 49: 201 205 chronic venous disorders, varicose vein, CEAP classification, lipodermatosclerosis,
Online publication August 27, 2009 chronic venous disorders: CVD CEAP 4 CEAP CVD J Jpn Coll Angiol, 2009, 49: 201 205 chronic venous disorders, varicose vein, CEAP classification, lipodermatosclerosis,
Efficacy of Velcro Band Devices in Venous and. Mixed Arterio-Venous Patients
 Efficacy of Velcro Band Devices in Venous and Mixed Arterio-Venous Patients T. Noppeney Center for Vascular Diseases: Outpatient Dept. Obere Turnstrasse, Dept. for Vascular Surgery Martha-Maria Hospital
Efficacy of Velcro Band Devices in Venous and Mixed Arterio-Venous Patients T. Noppeney Center for Vascular Diseases: Outpatient Dept. Obere Turnstrasse, Dept. for Vascular Surgery Martha-Maria Hospital
Chronic Iliocaval Venous Occlusive Disease
 none Chronic Iliocaval Venous Occlusive Disease David Rigberg, M.D. Clinical Professor of Surgery Division of Vascular Surgery University of California Los Angeles Chronic Venous Occlusive Disease Chronic
none Chronic Iliocaval Venous Occlusive Disease David Rigberg, M.D. Clinical Professor of Surgery Division of Vascular Surgery University of California Los Angeles Chronic Venous Occlusive Disease Chronic
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2)
") Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Vascular Surgery Rotation Objectives for Junior Residents (PGY-1 and 2) Definition Vascular surgery is the specialty concerned with the diagnosis and management of congenital and acquired diseases of the
Guidelines, Policies and Statements D20 Statement on Peripheral Venous Ultrasound
 Guidelines, Policies and Statements D20 Statement on Peripheral Venous Ultrasound Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Guidelines, Policies and Statements D20 Statement on Peripheral Venous Ultrasound Disclaimer and Copyright The ASUM Standards of Practice Board have made every effort to ensure that this Guideline/Policy/Statement
Foam dressings have frequently
 The practical use of foam dressings Efficient and cost-effective management of excessive exudate continues to challenge clinicians. Foam dressings are commonly used in the management of moderate to heavily
The practical use of foam dressings Efficient and cost-effective management of excessive exudate continues to challenge clinicians. Foam dressings are commonly used in the management of moderate to heavily
Wound Assessment Report
 Wound Assessment Report Single Assessment, Single Wound Mary Taylor Assessment Patient ID MT4367147 Date of Birth 1939-4-18 Left Foot, Sole: Wound A Image taken 16-45-43 Area 1.7cm2 Perimeter 48mm Maximum
Wound Assessment Report Single Assessment, Single Wound Mary Taylor Assessment Patient ID MT4367147 Date of Birth 1939-4-18 Left Foot, Sole: Wound A Image taken 16-45-43 Area 1.7cm2 Perimeter 48mm Maximum
2008 American Medical Association and National Committee for Quality Assurance. All Rights Reserved. CPT Copyright 2007 American Medical Association
 Chronic Wound Care ASPS #1: Use of wound surface culture technique in patients with chronic skin ulcers (overuse measure) This measure may be used as an Accountability measure Clinical Performance Measure
Chronic Wound Care ASPS #1: Use of wound surface culture technique in patients with chronic skin ulcers (overuse measure) This measure may be used as an Accountability measure Clinical Performance Measure
Endo-Thermal Heat Induced Thrombosis (E-HIT)
") Endo-Thermal Heat Induced Thrombosis (E-HIT) Michael Ombrellino MD FACS The Cardiovascular Care Group Clinical Associate Professor of Surgery Rutgers School of Medicine Objectives: What is E-HIT? How do
Endo-Thermal Heat Induced Thrombosis (E-HIT) Michael Ombrellino MD FACS The Cardiovascular Care Group Clinical Associate Professor of Surgery Rutgers School of Medicine Objectives: What is E-HIT? How do
Practical Point in Holistic Diabetic Foot Care 3 March 2016
 Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
Diabetic Foot Ulcer : Vascular Management Practical Point in Holistic Diabetic Foot Care 3 March 2016 Supapong Arworn, MD Division of Vascular and Endovascular Surgery Department of Surgery, Chiang Mai
DISORDERS OF VENOUS SYSTEM
 DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
DISORDERS OF VENOUS SYSTEM Varicose Veins Any dilated, elongated and tortuous vein irrespective of size Varicose veins are common in the superficial veins of the leg which are subject to high pressure
Introduction to Saphenous Vein Ablations: When/Why/How?
 John Ligush, MD SMJH Vascular and Vein Center Introduction to Saphenous Vein Ablations: When/Why/How? Saphenous Vein Ablations: When/Why/How? Venous disease is easy Treatment is straightforward The patients
John Ligush, MD SMJH Vascular and Vein Center Introduction to Saphenous Vein Ablations: When/Why/How? Saphenous Vein Ablations: When/Why/How? Venous disease is easy Treatment is straightforward The patients
Features compression after open and endovascular operation in vascular malformation
 Features compression after open and endovascular operation in vascular malformation Sapelkin Sergey Institute of Surgery named A.V. Vishnevsky, Moscow, Russia 21.10.2017 CIRC Meeting, Grassau AV-malformations:
Features compression after open and endovascular operation in vascular malformation Sapelkin Sergey Institute of Surgery named A.V. Vishnevsky, Moscow, Russia 21.10.2017 CIRC Meeting, Grassau AV-malformations:
Protocols for the evaluation of lower extremity venous reflux: supine, sitting, or standing?
 Protocols for the evaluation of lower extremity venous reflux: supine, sitting, or standing? Susan Whitelaw RVT, RDMS PURPOSE Duplex imaging of the lower extremity veins is performed to assess the deep
Protocols for the evaluation of lower extremity venous reflux: supine, sitting, or standing? Susan Whitelaw RVT, RDMS PURPOSE Duplex imaging of the lower extremity veins is performed to assess the deep
Priorities Forum Statement
 Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
Priorities Forum Statement Number 9 Subject Varicose Vein Surgery Date of decision September 2014 Date refreshed March 2017 Date of review September 2018 Relevant OPCS codes: L841-46, L848-49, L851-53,
Meissner MH, Gloviczki P, Comerota AJ, Dalsing MC, Eklof BG, Gillespie DL, et al. J Vasc Surg. 2012;55:
 Early thrombus removal strategies for acute deep venous thrombosis: Clinical Practice Guidelines of the Society for Vascular Surgery and the American Venous Forum Meissner MH, Gloviczki P, Comerota AJ,
Early thrombus removal strategies for acute deep venous thrombosis: Clinical Practice Guidelines of the Society for Vascular Surgery and the American Venous Forum Meissner MH, Gloviczki P, Comerota AJ,
The Use of Adjunctive Venography and Endovascular Manoeuvres In The Treatment of Saphenous Vein Insufficiency. A Prospective, Multi-centre Study
 The Use of Adjunctive Venography and Endovascular Manoeuvres In The Treatment of Saphenous Vein Insufficiency A Prospective, Multi-centre Study Ramon L. Varcoe, MBBS, MS, FRACS, PhD Associate Professor
The Use of Adjunctive Venography and Endovascular Manoeuvres In The Treatment of Saphenous Vein Insufficiency A Prospective, Multi-centre Study Ramon L. Varcoe, MBBS, MS, FRACS, PhD Associate Professor
2015 ARDMS Physicians Vascular Interpretation Job Task Analysis Summary Report
 P a g e 1 2015 ARDMS Physicians Vascular Interpretation Job Task Analysis Summary Report American Registry for Diagnostic Medical Sonography (ARDMS) P a g e 2 Table of Contents ABOUT THE REPORT... 3 METHODOLOGY...
P a g e 1 2015 ARDMS Physicians Vascular Interpretation Job Task Analysis Summary Report American Registry for Diagnostic Medical Sonography (ARDMS) P a g e 2 Table of Contents ABOUT THE REPORT... 3 METHODOLOGY...
AWMA MODULE ACCREDITATION. Module Three: Assessment and Management of Lower Leg Ulceration
 AWMA MODULE ACCREDITATION Module Three: Assessment and Management of Lower Leg Ulceration Introduction - The Australian Wound Management Association Education & Professional Development Sub Committee-(AWMA
AWMA MODULE ACCREDITATION Module Three: Assessment and Management of Lower Leg Ulceration Introduction - The Australian Wound Management Association Education & Professional Development Sub Committee-(AWMA
National Vascular Registry
 National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
National Vascular Registry Angioplasty Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or
VENOUS SYMPOSIUM: OVERVIEW
 1 VENOUS SYMPOSIUM: OVERVIEW Robert W. Vorhies, M.D., F.A.C.S. Vascular and Endovascular Surgery Endovenous Therapy and Vein Aesthetics Ferrell-Duncan Clinic, Cox Health Systems WHY DO WE CARE? Epidemiology
1 VENOUS SYMPOSIUM: OVERVIEW Robert W. Vorhies, M.D., F.A.C.S. Vascular and Endovascular Surgery Endovenous Therapy and Vein Aesthetics Ferrell-Duncan Clinic, Cox Health Systems WHY DO WE CARE? Epidemiology
Varicose Vein Cyanoacrylate Glue treatment
 The South West s premier independent healthcare and cosmetic clinic Varicose Vein Cyanoacrylate Glue treatment Varicose veins are a sign of underlying venous insufficiency and affect 20 30% of adults.
The South West s premier independent healthcare and cosmetic clinic Varicose Vein Cyanoacrylate Glue treatment Varicose veins are a sign of underlying venous insufficiency and affect 20 30% of adults.
National Vascular Registry
 National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
National Vascular Registry Bypass Patient Details Patient Consent* 2 Not Required If patient not consented: Date consent recorded / / (DD/MM/YYYY) Do not record NHS number, NHS number* name(s) or postcode.
Occasional pain or other discomfort (ie, not restricting regular daily activity)
") Revised Venous Clinical Severity Score Pain : 0 Mild: 1 or other discomfort (ie, aching, heaviness, fatigue, soreness, burning) Occasional pain or other discomfort (ie, not restricting regular daily activity)
Revised Venous Clinical Severity Score Pain : 0 Mild: 1 or other discomfort (ie, aching, heaviness, fatigue, soreness, burning) Occasional pain or other discomfort (ie, not restricting regular daily activity)
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia
 Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Surgery is and Remains the Gold Standard for Limb-Threatening Ischemia Albeir Mousa, MD., FACS.,MPH., MBA Professor of Vascular and Endovascular Surgery West Virginia University Disclosure None What you
Management of Lower Limb Ulcers. D. NAIK MBChB FRACS DDU
 Management of Lower Limb Ulcers D. NAIK MBChB FRACS DDU Ulcer A defect in the epithelium A failure to heal Ulcer Aetiology of Leg Ulcers Venous insufficiency Macrovascular arterial insufficiency Infectious
Management of Lower Limb Ulcers D. NAIK MBChB FRACS DDU Ulcer A defect in the epithelium A failure to heal Ulcer Aetiology of Leg Ulcers Venous insufficiency Macrovascular arterial insufficiency Infectious
Consider the impact of Venous Disease Review elements in the workup and diagnosis of Venous Disease Review treatment considerations
 Gregory Bohn, MD FACS Clinical Symposium on Advances in Skin and Wound Care September 9-12, 2011 Gaylord National Washington, DC Consider the impact of Venous Disease Review elements in the workup and
Gregory Bohn, MD FACS Clinical Symposium on Advances in Skin and Wound Care September 9-12, 2011 Gaylord National Washington, DC Consider the impact of Venous Disease Review elements in the workup and